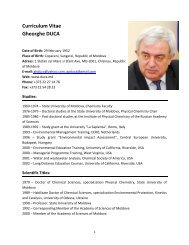
232Buletinul AŞMaveau ca scop i<strong>de</strong>ntificarea microorganismelor cu rol<strong>de</strong> agent etiologic, însă un astfel <strong>de</strong> agent cauzal nua fost găsit. Pe parcursul ultimului <strong>de</strong>ceniu, căutărilese reorientează în direcţia studierii microorganismelorintestinale nepatogene obligatorii şi tranzitorii. Înprezent este acumulată o bază impunătoare <strong>de</strong> doveziîn favoarea rolului patogenetic primordial al florei intestinaleîn BII [29]. Cele mai convingătoare dovezivizând rolul primordial al microorganismelor intestinaleîn <strong>de</strong>zvoltarea BII au fost oferite <strong>de</strong> cercetărileexperimentale. La majoritatea mo<strong>de</strong>lelor experimentale,indiferent <strong>de</strong> acţiunea patogenă, a lipsit inflamaţiaintestinală cronică, dacă animalul a fost plasat şimenţinut în condiţii sterile. Suplimentarea ambianţeiacestor animale cu floră normală a condus la <strong>de</strong>zvoltareacolitei în termene scurte. Aceste rezultate aucontribuit la apariţia şi acceptarea paradigmei „nu-sbacterii – nu-i colită”. Se presupune că anumiţi antigeniai florei intestinale sunt triggerii casca<strong>de</strong>i <strong>de</strong> reacţiiimunologice, rezultante prin colită la indivizii cususceptibilitate genetică. Însă antigenii-triggerii, încazul existenţei acestora, încă nu au fost i<strong>de</strong>ntificaţi.Efectul terapeutic al probioticelor asupra evoluţieiBII este un argument în favoarea rolulului patogenetical disbiozei în aceste afecţiuni. Prin trialuriclince controlate au fost <strong>de</strong>monstrate efecte terapeuticefavorabile în CU prin administrarea probioticelor[30]. Totodată, în contextul BII se cunoaşte <strong>de</strong>sprerolul protectiv nu doar al florei intestinale obligatorii,dar şi al unor paraziţi intestinali. Spre exemplu, unadintre publicaţiile recente ale grupului <strong>de</strong> cercetătoridin Germania [31] relatează o asociere între invazia<strong>de</strong> helminţi şi riscul scăzut <strong>de</strong> <strong>de</strong>zvoltare a BC. Înopinia unor savanţi, helmintozele contribuie la menţinereaactivităţii imunităţii înnăscute şi dobândite,astfel prevenind <strong>de</strong>vierea reacţiilor imunologice îndirecţia reactivităţii patologice [32]. Au fost publicateprimele rezultate <strong>de</strong>spre eficacitatea tratamentului cuhelminţi atât în CU, cât şi în BC [34].Acumularea datelor referitor la reducerea riscului<strong>de</strong> <strong>de</strong>zvoltare a BII la persoanele cu helmintoze, parazitozeşi alte infecţii intestinale, concomitent cu dateleepi<strong>de</strong>miologice (răspândirea minimală a BII concomitentcu răspândirea înaltă a invaziilor cu helminţiîn Africa, Asia <strong>de</strong> Sud şi Asia <strong>de</strong> Sud-Est) a condus laapariţia „ipotezei igienice” în etiopatogenia BII [34].De pe poziţiile acestei ipoteze, minimizarea expuneriila acţiunea cronică a diverselor microorganisme cutransmisie intestinală, mai ales în perioada copilăriei(condiţii <strong>de</strong> trai cu standar<strong>de</strong> igienice înalte), conducela scă<strong>de</strong>rea toleranţei sistemului imun al intestinuluişi, consecutiv, la <strong>de</strong>zvoltarea locală a inflamaţiei. Inflamaţiaîn aceste cazuri se datorează activităţii floreipatogene, dar şi a celei condiţionat-patogene şi nepatogene.Cu toate că „ipoteza igienică” nu este susţinutăunanim <strong>de</strong> experţi, totuşi, este mare probabilitateacă factorii <strong>de</strong> mediu participă în <strong>de</strong>zvoltarea BII.Rolul factorilor <strong>de</strong> mediu. La factorii <strong>de</strong> ambianţă,probabil implicaţi sau cu impact <strong>de</strong>monstratasupra BII, se referă factorii igienici: calitatea apeipotabile, existenţa sistemului centralizat <strong>de</strong> canalizare,a apei cal<strong>de</strong>, calitatea prelucrării alimentelor, păstrareaalimentelor în condiţii <strong>de</strong> frigi<strong>de</strong>r şi congelator,numărul membrilor familiei, disponibilitatea <strong>de</strong> dormitoareindividuale şi alţi factori habituali [1]. Opiniaunor savanţi <strong>de</strong>spre nivelul înalt al normelor igieniceca factor <strong>de</strong> risc pentru BII este susţinută indirect şi<strong>de</strong> cercetările epi<strong>de</strong>miologice.Există numeroase publicaţii ştiinţifice consacrateasocierilor posibile dintre BII şi particularităţile <strong>de</strong>alimentaţie. Dieta săracă în fibre alimentare, dar cuconţinut exagerat <strong>de</strong> hidrocarburi rafinate, grăsimi <strong>de</strong>origine animală, margarină, fast foods a fost propusăca factor <strong>de</strong> risc pentru BII. Indicii <strong>de</strong> morbiditate încreştere a BII în zonele anterior „favorabile” (Europa<strong>de</strong> Est, Asia) pot avea explicaţia „acci<strong>de</strong>ntalizării”dietei, alimentaţia tradiţională fiind substituită <strong>de</strong>cea caracteristică societăţilor occi<strong>de</strong>ntale. Cu toatecă există multe cercetări rezultatele cărora sugereazăexistenţa asocierilor între particularităţile <strong>de</strong> alimentaţieşi BII, totuşi, până în prezent nu au fost oferitedovezi convingătoare a implicării directe în patogenezaCU sau BC a factorilor dietetici. În opinia luiRussel şi coautorii [35], riscurile alimentare sunt <strong>de</strong>terminatemai puţin <strong>de</strong> factorii dietetici, dar prepon<strong>de</strong>rent<strong>de</strong> alţi factori ce caracterizează modul <strong>de</strong> viaţăocci<strong>de</strong>ntal (“mo<strong>de</strong>rn lifestyle”).SusceptibilitategeneticGena 1Gena 2Gena 3MicrofloraintestinalBacteria 1Bacteria 2Bacteria 3RspunsulimunRspunsimun 1Rspunsimun 2Rspunsimun 3Variantaclinico-evolutivBII 1, evoluieuoarBII 2, evoluieseverBII 3,stenozareFigura 2. Interacţiunile dintre factori patogenetici[37].A fost studiat şi impactul fumatului asupra diverselorforme <strong>de</strong> BII. Fumatul sporeşte riscul apariţieiBC şi agravează evoluţia acesteia, fumătorii mai<strong>de</strong>s necesită tratament steroid şi imunosupresiv, darşi intervenţii chirurgicale, obţinându-se rezultate terapeuticemai slabe; renunţarea la fumat amelioreazăevoluţia bolii [36]. În cazul CU situaţia este inversă:fumatul sca<strong>de</strong> riscul <strong>de</strong>zvoltării bolii, amelioreazăevoluţia, reduce riscul colonectomiei; renunţarea lafumat în CU agravează evoluţia bolii şi prognosticul.
Ştiinţe MedicaleIndiferent <strong>de</strong> rezultatele studiilor, fumatul nu va fi recomandatbolnavilor cu CU, <strong>de</strong>oarece efectul asuprabolii se nivelează <strong>de</strong> acţiunea nefavorabilă asupra sistemelorcardiovascular şi respirator.Totalizând cele expuse, putem presupune că factorii<strong>de</strong> mediu, asociaţi cu BII, posibil, îşi exercită acţiuneaprin intermediul florei intestinale (spre exemplu,particularităţile alimentaţiei, factorii igienici etc.)şi al sistemului imun, iar <strong>de</strong>reglările florei intestinaleşi ale statutului imun la persoanele cu susceptibilitategenetică conduc spre apariţia inflamaţiei cronice înintestin.Concluzii. Interacţiunile dintre susceptibilitateagenetică, caracterul atacului antigenic al microfloreiintestinale şi caracterul răspunsului imun la aceastăagresiune antigenică sunt mecanisme complexeşi necesită studiere în continuare. În mod schematicaceste legături sunt reprezentate în figura 2. Caracterulşi particularităţile acestor interacţiuni, probabil,<strong>de</strong>termină nu doar apariţia BII, dar şi fenotipul bolii,exprimat prin varianta clinico-evolutivă.Bibliografie selectivă1. Lakatos P. Environmental factors affecting infl ammatorybowel disease: have we ma<strong>de</strong> progress? In: Dig.Dis., 2009, 27(3), p. 215-225.2. Kaser A., Zeissig S., Blumberg R. Genes and environment:how will our concepts on the pathophysiologyof IBD <strong>de</strong>velop in the future? In: Dig. Dis., 2010, 28(3), p.395-405.3. Fiocchi C. The multifactorial pathogenesis of IBD.Inflam. bowel disease – Diagnostic and therapeutic strategies.Falk Symposium 154. Moscow, 2006, p. 21-22.4. Kirsner J.B., Spencer J.A. Family occurrence ofulcerative colitis, regional enteritis, and ileocolitis. In:Ann. Intern. Med., 1963,; 59, p. 133-144.5. Jewell D.P. Genetic basis of infl ammatory boweldisease. Inflammation in the intestinal tract: pathogenesisand treatment. Falk symp. 169, 2009, Kiev, p. 17-19.6. Hugot J.P., Laurent-Puig P, Gower-Roussean C. etal. Mapping of a susceptibility locus for Crohn’s disease onchromosome 16. In: Nature, 1996; 379(6), p. 821-822.7. Hugot J.P., Chamaillard M., Zouali H. et al. Associationof NOD2 leucine-rich repeat variants with susceptibilityto Crohn’s disease. In: Nature, 2001, 411(4), p.599-603.8. Ogura Y., Inohara N., Benito A. et al. NOD2, aNOD1-Apaf-1 family member that is restricted to monocytesand activates NF-kB. In: J. Biol. Chem., 2001, 276,p. 4812-4818.9. Duer R.H. Genome-wi<strong>de</strong> association studies heralda new era of rapid discoveries in inflammatory bowel diseaseresearch. In: Gastroenterol., 2007, 132, p. 2045-2062.10. Cho J.H., Weaver C.T. The genetics of infl ammatorybowel disease. In: Gastroenterol. 2007, 133, p. 1327-1339.11. Satsangi J., Parkes M., Louis E. et al. Two stagegenome-wi<strong>de</strong> search in infl ammatory bowel disease provi<strong>de</strong>sevi<strong>de</strong>nce for susceptibility loci on chromosomes 3, 7and 12. In: Nat. Genet., 1996, 14, p. 199-202.23312. Perri F., Annese V., Pieroli A. et al. HLA antigensand pANCA <strong>de</strong>fi ne ulcerative colitis as a genetically heterogeneousdisor<strong>de</strong>r. In: Ital. J. Gastroenterol. Hepatol.,1998, 30(1), p. 56-61.13. Lei<strong>de</strong>nius M.N.K., Koskimies S.A., KellokumpuI.H., Hockerstedt K.A.V. HLA antigens in ulcerative colitisand primary sclerosing cholangitis. In: Acta Path. Microbiol.Immunol. Scandinavica, 1995, 103 (7-8), p. 519-524.14. Masuda H., Nakamura Y., Tanaka T., Hayakawa S.Distinct relationship between HLA-DR genes and intractabilityof ulcerative colitis. In: J. Gastroenterol., 1994, 89,p. 1957-1962.15. Cassinotti A., Birin<strong>de</strong>lli S., Clerici M. et al. HLAand autoimmune digestive disease: a clinically orientedreview for gastroenterologist. In: Am. J. Gastroenterol.,2009, 104, p. 195-217.16. Fiocchi C., Susceptibility Genes and overallpathogenesis of infl ammatory bowel disease: where do westand? In: Dig. Dis., 2009, 27(3), p. 226-235.17. Schreiber S., Clinical implications of genetic fi ndingsin infl ammatory bowel disease. In: Inflammation inthe intestinal tract. Falk symposium 169, Kiev, 2009, p.18-19.18. Fowler E.V., Doecke J., Simms L.A. et al., AT-G16L1 T300A shows strong association with disease subgroupsin a larg Australian IBD population: further supportfor signifi cant disease heterogeneity. In: Am. J. Gastroenterol.,2008, 103, p. 2519-2526.19. Quinton J.F., Sendid B., Reumax D. et al., Anti-Saccharomyces cerevisiae mannan antibodies combinedwith antineutrophil cytoplasmic autoantibodies in infl ammatorybowel disease: prevalence and diagnostic role. In:Gut, 1998, 42, p. 788-791.20. Marcelletti J., Moskowitz D., Stempak J et al.,Anti-microbial antibody markers as prognostic indicatorsof infl ammatory bowel disease course. In: Gastroenterol.,2005, 128 (suppl. 4), A 305.21. Altstock R., Shtevi A., Karban A. et al., ImprovedIBD diagnosis via ELISA <strong>de</strong>tecting novel antibodies:ACCA, ALCA and AMCA. In: Gastroenterol., 2005, 128(suppl. 4), A 303.22. Schwarz S., Ammirati M. et al., I<strong>de</strong>ntifi cation ofin<strong>de</strong>terminate colitis using PANCA and ASCA. In: Gastroenterol.,2000, 118 (suppl.2), A 1891.23. Dotan I., New serologic markers for infl ammatorybowel disease diagnosis. In: Dig. Dis., 2010, 28(3), p. 418-23.24. Genunche-Dumitrescu A., Mitrut P., Ba<strong>de</strong>a D.,Ba<strong>de</strong>a M., The serum level of cytokines (IL-1, IL-6) andTNF-alfa in patients with infl ammatory bowel disease. In:Mechanisms of intestinal inflammation. Falk Workshop.Dres<strong>de</strong>n, 2007, p. A 14.25. Atreya R., Neurath M.F., Chemokines in infl ammatorybowel disease. In: Dig. Dis., 2010, 28(3), p. 386-394.26. Zeitz M., Immunoregulation: Crohn’s diseaseversus ulcerative colitis. In: Inflammatory bowel disease– Diagnostic and therapeutic strategies. Falk Symposium154. Moscow, 2006, p. 25-26.27. Deretic V., Links between autophagy, innate immunity,infl ammation and Crohn’s disease. In: Dig. Dis.,2009, 27(3), p. 246-251.28. Rioux J.D., Xavier R.J., Taylor K.D. et al., Genome-wi<strong>de</strong>association study i<strong>de</strong>ntifi es new susceptibility
- Page 1 and 2:
Ştiinţe Medicale1ACADEMIA DE ȘTI
- Page 3 and 4:
3S U M A R СОДЕРЖАНИЕ S U
- Page 5 and 6:
5Ion Balica. Destrucţiile pulmonar
- Page 7 and 8:
7Mihail Borş, Victor Cojocaru, Vir
- Page 9 and 10:
9Veronica Gonţa, Zinaida Alexa,Nat
- Page 11 and 12:
11Angela Peltec. Bine-cunoscută vs
- Page 13 and 14:
Ştiinţe MedicaleUn prim pas în r
- Page 15 and 16:
Ştiinţe Medicale15Dacă în anul
- Page 17 and 18:
Ştiinţe Medicale17SĂNĂTATE PUBL
- Page 19 and 20:
Ştiinţe MedicaleFinlandei în Uni
- Page 21 and 22:
Ştiinţe MedicaleTabelul 1Componen
- Page 23 and 24:
Ştiinţe Medicaleeficacităţii in
- Page 25 and 26:
Ştiinţe MedicaleLes sources d’i
- Page 27 and 28:
Ştiinţe Medicalea chetuielilor î
- Page 29 and 30:
Ştiinţe Medicalenontransmissibile
- Page 31 and 32:
Ştiinţe Medicaleохранени
- Page 33 and 34:
Ştiinţe Medicaleски, при о
- Page 35 and 36:
Ştiinţe Medicale35жизнь, а
- Page 37 and 38:
Ştiinţe Medicale”старые
- Page 39 and 40:
Ştiinţe Medicale39Tabelul 2Analiz
- Page 41 and 42:
Ştiinţe Medicale(p
- Page 43 and 44:
Ştiinţe MedicaleVârsta medie a p
- Page 45 and 46:
Ştiinţe Medicaledul chirurgical a
- Page 47 and 48:
Ştiinţe Medicaleminuat la 1 săpt
- Page 49 and 50:
Ştiinţe Medicale2006 în secţia
- Page 51 and 52:
Ştiinţe Medicale51de ventricul st
- Page 53 and 54:
Ştiinţe Medicalefunctional ischem
- Page 55 and 56:
Ştiinţe Medicale551. Trombectomia
- Page 57 and 58:
Ştiinţe Medicaletecţia miocardic
- Page 59 and 60:
Ştiinţe Medicalecu sânge, el tot
- Page 61 and 62:
Ştiinţe Medicalere ale valvei, da
- Page 63 and 64:
Ştiinţe Medicaleticul de DSV cu s
- Page 65 and 66:
Ştiinţe Medicale8. Sidi D. Maladi
- Page 67 and 68:
Ştiinţe Medicale67reconstructivă
- Page 69 and 70:
Ştiinţe Medicale69dă la întreba
- Page 71 and 72:
Ştiinţe Medicaleţesuturi, în ac
- Page 73 and 74:
Ştiinţe Medicalebilizarea ţesutu
- Page 75 and 76:
Ştiinţe Medicalerac. Cardiovasc.
- Page 77 and 78:
Ştiinţe Medicale77tanil 1-2 mkg/k
- Page 79 and 80:
Ştiinţe MedicaleThe technique of
- Page 81 and 82:
Ştiinţe Medicale81Indicaţia prin
- Page 83 and 84:
Ştiinţe MedicaleConcluzii1. Atitu
- Page 85 and 86:
Ştiinţe Medicale1. Examene radiol
- Page 87 and 88:
Ştiinţe Medicale6. Dallemagne B.,
- Page 89 and 90:
Ştiinţe Medicalede datele noastre
- Page 91 and 92:
Ştiinţe Medicale3. Dual Mesh; 4.
- Page 93 and 94:
Ştiinţe Medicale93Figura 1. Repar
- Page 95 and 96:
Ştiinţe Medicalefaptul că utiliz
- Page 97 and 98:
Ştiinţe MedicaleLimfom non-Hodgki
- Page 99 and 100:
Ştiinţe Medicale99strumentale sau
- Page 101 and 102:
Ştiinţe Medicale6. David J.K., Bo
- Page 103 and 104:
Ştiinţe Medicale103la debutul bol
- Page 105 and 106:
Ştiinţe Medicale105DIALIZA ŞI TR
- Page 107 and 108:
Ştiinţe Medicale14. Weinberger H.
- Page 109 and 110:
Ştiinţe MedicaleFigura 3. Durata
- Page 111 and 112:
Ştiinţe Medicaleas the threshold
- Page 113 and 114:
Ştiinţe Medicale6. Basha J., Dewi
- Page 115 and 116:
Ştiinţe Medicaleconstituie 46%. C
- Page 117 and 118:
Ştiinţe Medicale15. Klotz T., Sac
- Page 119 and 120:
Ştiinţe Medicaleucocitar s-a depi
- Page 121 and 122:
Ştiinţe Medicale2010, în secţia
- Page 123 and 124:
Ştiinţe Medicaleoperaţi deschis,
- Page 125 and 126:
Ştiinţe Medicalemm Hg versus valo
- Page 127 and 128:
Ştiinţe Medicaleдавление,
- Page 129 and 130:
Ştiinţe Medicale129Dimensiunile c
- Page 131 and 132:
Ştiinţe Medicale(ESWL) etc. Litot
- Page 133 and 134:
Ştiinţe Medicalerata de succes a
- Page 135 and 136:
Ştiinţe Medicale135ORLCHISTUL BRA
- Page 137 and 138:
Ştiinţe Medicaleces in adult case
- Page 139 and 140:
Ştiinţe Medicalea fost ablaţia c
- Page 141 and 142:
Ştiinţe MedicaleMaterial şi meto
- Page 143 and 144:
Ştiinţe MedicaleMETODE DE MIRINGO
- Page 145 and 146:
Ştiinţe Medicale145PRIMA EXPERIEN
- Page 147 and 148:
Ştiinţe Medicalepostoperatorie.
- Page 149 and 150:
Ştiinţe Medicale149donat. Mastoci
- Page 151 and 152:
Ştiinţe Medicale151OFTALMOLOGIEPA
- Page 153 and 154:
Ştiinţe MedicaleCapsulorexis circ
- Page 155 and 156:
Ştiinţe Medicalerecesie muscular
- Page 157 and 158:
Ştiinţe Medicalebismus in adults-
- Page 159 and 160:
Ştiinţe Medicaleîşi va demonstr
- Page 161 and 162:
Ştiinţe Medicalene receptors, and
- Page 163 and 164:
Ştiinţe MedicaleHipotensiune 37 9
- Page 165 and 166:
Ştiinţe MedicaleTratamentul medic
- Page 167 and 168:
Ştiinţe MedicaleРезюмеМе
- Page 169 and 170:
Ştiinţe Medicale169Tabelul 3Valor
- Page 171 and 172:
Ştiinţe Medicale171apare tromboza
- Page 173 and 174:
Ştiinţe MedicaleTNF, IL6, IL1 şi
- Page 175 and 176:
Ştiinţe MedicaleDatele obţinute
- Page 177 and 178:
Ştiinţe MedicalePrincipalele tipu
- Page 179 and 180:
Ştiinţe MedicaleANESTEZIA REGIONA
- Page 181 and 182: Ştiinţe Medicaleretrobulbar a fos
- Page 183 and 184: Ştiinţe Medicale183terapie sau î
- Page 185 and 186: Ştiinţe MedicaleSEDAREA MONITORIZ
- Page 187 and 188: Ştiinţe Medicalefără a ne teme
- Page 189 and 190: Ştiinţe Medicale189TERAPIE. STUDI
- Page 191 and 192: Ştiinţe MedicaleExaminarea organe
- Page 193 and 194: Ştiinţe Medicaleobiectivelor stud
- Page 195 and 196: Ştiinţe MedicaleBibliografie sele
- Page 197 and 198: Ştiinţe MedicaleConcluzii:1) Afec
- Page 199 and 200: Ştiinţe Medicalea relevat o creş
- Page 201 and 202: Ştiinţe Medicalede pacienţi, din
- Page 203 and 204: Ştiinţe Medicaleantele poliarticu
- Page 205 and 206: Ştiinţe Medicale7 mm/h. Valoarea
- Page 207 and 208: Ştiinţe Medicale207p < 0.05primar
- Page 209 and 210: Ştiinţe Medicale4. Rudwaleit M.,
- Page 211 and 212: Ştiinţe Medicaleonat valorile nor
- Page 213 and 214: Ştiinţe MedicaleFitness, Arthriti
- Page 215 and 216: Ştiinţe Medicaleterapie este foar
- Page 217 and 218: Ştiinţe Medicaleca inductor al r
- Page 219 and 220: Ştiinţe Medicaleи чувстви
- Page 221 and 222: Ştiinţe Medicale221(de 4-5 ori ma
- Page 223 and 224: Ştiinţe Medicale13. Sperberg K.,
- Page 225 and 226: Ştiinţe Medicale225GASTROENTEROLO
- Page 227 and 228: Ştiinţe Medicale227Remisiune comp
- Page 229 and 230: Ştiinţe Medicalecolitis in remiss
- Page 231: Ştiinţe Medicale• un grup nou -
- Page 235 and 236: Ştiinţe MedicaleRezultatele obţi
- Page 237 and 238: Ştiinţe Medicale2. Bianco A.C., S
- Page 239 and 240: Ştiinţe Medicaleciroză Child-Pug
- Page 241 and 242: Ştiinţe Medicale241menstrual estr
- Page 243 and 244: Ştiinţe Medicalecu gradul disfunc
- Page 245 and 246: Ştiinţe Medicalecineticii transam
- Page 247 and 248: Ştiinţe Medicale247NEFROLOGIEEVAL
- Page 249 and 250: Ştiinţe Medicaleteracţiunea cu f
- Page 251 and 252: Ştiinţe Medicalevilor la tratamen
- Page 253 and 254: Ştiinţe Medicalediafi ltration. I
- Page 255 and 256: Ştiinţe Medicale255Tabelul 1Difer
- Page 257 and 258: Ştiinţe Medicale5. Lohman T., Kel
- Page 259 and 260: Ştiinţe MedicaleLa pacienţii cu
- Page 261 and 262: Ştiinţe MedicaleINTERRELAŢIILEDI
- Page 263 and 264: Ştiinţe Medicale5. Jespersen B.,
- Page 265 and 266: Ştiinţe Medicalevârstnic este ad
- Page 267 and 268: Ştiinţe Medicale267ALERGOLOGIEREZ
- Page 269 and 270: Ştiinţe MedicaleRezultate şi dis
- Page 271 and 272: Ştiinţe Medicale după începutul
- Page 273 and 274: Ştiinţe Medicale273PULMONOLOGIEAS
- Page 275 and 276: Ştiinţe Medicale3. Blot F., Rayna
- Page 277 and 278: Ştiinţe Medicale277unilor prepond
- Page 279 and 280: Ştiinţe MedicalePacientul s-a pre
- Page 281 and 282: Ştiinţe Medicaleby the abnormal a
- Page 283 and 284:
Ştiinţe Medicaleprima dată ca o
- Page 285 and 286:
Ştiinţe Medicale285CARDIOLOGIECUM
- Page 287 and 288:
Ştiinţe Medicale287Mediile ajusta
- Page 289 and 290:
Ştiinţe Medicalein the European P
- Page 291 and 292:
Ştiinţe Medicaletoda imunoferment
- Page 293 and 294:
Ştiinţe Medicalediovascular înal
- Page 295 and 296:
Ştiinţe Medicale295DIVERSESTRESUL
- Page 297 and 298:
Ştiinţe MedicaleLa fel şi procen
- Page 299 and 300:
Ştiinţe Medicale• sectorul dat
- Page 301 and 302:
Ştiinţe MedicaleStudiul a fost ef
- Page 303 and 304:
Ştiinţe MedicaleА.И. Неспе
- Page 305 and 306:
Ştiinţe Medicalecazul colonului a
- Page 307 and 308:
Ştiinţe Medicalepentru oncologi l
- Page 309 and 310:
Ştiinţe Medicaleof non-radiated r
- Page 311 and 312:
Ştiinţe Medicale311corpului stră
- Page 313 and 314:
Ştiinţe MedicaleBibliografie sele
- Page 315 and 316:
Ştiinţe MedicaleMetodele radiolog
- Page 317 and 318:
Ştiinţe MedicaleРезюмеНа
- Page 319 and 320:
Ştiinţe Medicaleculare este impos
- Page 321 and 322:
Ştiinţe Medicaleîn regim multipo
- Page 323 and 324:
Ştiinţe Medicaledepistat 20 (24,1
- Page 325 and 326:
Ştiinţe MedicaleCVP, %Diametrul v
- Page 327 and 328:
Ştiinţe Medicaletraţia muşchilo
- Page 329 and 330:
Ştiinţe Medicale329stazei venoase
- Page 331 and 332:
Ştiinţe Medicaleсопрoтивл
- Page 333 and 334:
Ştiinţe Medicale333Figura 3. a -
- Page 335 and 336:
Ştiinţe Medicalecare se caracteri
- Page 337 and 338:
Ştiinţe Medicale9. Tseng Y., Lee
- Page 339 and 340:
Ştiinţe MedicaleН. А. Петр
- Page 341 and 342:
Ştiinţe Medicale341Indici studia
- Page 343 and 344:
Ştiinţe MedicaleРезюмеПр
- Page 345 and 346:
Ştiinţe MedicaleWELL-KNOWN VERSUS
- Page 347 and 348:
Ştiinţe Medicalein cardiovascular
- Page 349 and 350:
Ştiinţe MedicaleDuctul pancreatic
- Page 351 and 352:
Ştiinţe MedicaleCel mai complex s
- Page 353 and 354:
Ştiinţe Medicalepompă devine nes
- Page 355 and 356:
Ştiinţe Medicale355ANIVERSĂRISav
- Page 357 and 358:
Ştiinţe Medicalecilor de urgenţ
- Page 359 and 360:
Ştiinţe Medicale359Lista fondator