FÓRMULAS INFANTIS ESPECIAIS Uma relação de ... - Nestlé
FÓRMULAS INFANTIS ESPECIAIS Uma relação de ... - Nestlé
FÓRMULAS INFANTIS ESPECIAIS Uma relação de ... - Nestlé

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
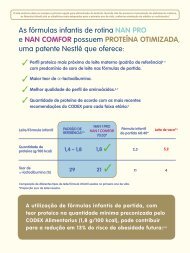
Material <strong>de</strong>stinado exclusivamente ao profissional <strong>de</strong> saú<strong>de</strong>.Proibida a distribuição a consumidores.A solução para cada situação.<strong>Nestlé</strong>Nutrition.Lí<strong>de</strong>r mundialem NutriçãoInfantil.<strong>FÓRMULAS</strong> <strong>INFANTIS</strong> <strong>ESPECIAIS</strong><strong>Uma</strong> <strong>relação</strong> <strong>de</strong> confiançaexige soluções que sejamcomprovadamente seguras.Na ausência do leite materno, a fórmula infantil é o substituto a<strong>de</strong>quado para a alimentação <strong>de</strong> lactentes no primeiro ano <strong>de</strong> vida. 45Acesse o nosso site e obtenha mais informações: www.nestle.com.br/nutricaoinfantilServiço <strong>de</strong> Atendimento Nutrição Infantil ao Profissional <strong>de</strong> Saú<strong>de</strong>0800-7701599NOTA IMPORTANTE:AS GESTANTES E NUTRIZES PRECISAM SER INFORMADAS QUE O LEITE MATERNO É O IDEAL PARA O LACTENTE, CONSTITUINDO-SE A MELHOR NUTRIÇÃO E PROTEÇÃO PARA ESTASCRIANÇAS. A MÃE DEVE SER ORIENTADA QUANTO À IMPORTÂNCIA DE UMA DIETA EQUILIBRADA NESTE PERÍODO E QUANTO À MANEIRA DE SE PREPARAR PARA O ALEITAMENTOAO SEIO ATÉ OS DOIS ANOS DE IDADE DA CRIANÇA OU MAIS. O USO DE MAMADEIRAS, BICOS E CHUPETAS DEVE SER DESENCORAJADO, POIS PODE TRAZER EFEITOS NEGATIVOSSOBRE O ALEITAMENTO NATURAL. A MÃE DEVE SER PREVENIDA QUANTO À DIFICULDADE DE VOLTAR A AMAMENTAR SEU FILHO UMA VEZ ABANDONADO O ALEITAMENTO AO SEIO.ANTES DE SER RECOMENDADO O USO DE UM SUBSTITUTO DO LEITE MATERNO, DEVEM SER CONSIDERADAS AS CIRCUNSTÂNCIAS FAMILIARES E O CUSTO ENVOLVIDO. A MÃE DEVEESTAR CIENTE DAS IMPLICAÇÕES ECONÔMICAS E SOCIAIS DO NÃO ALEITAMENTO AO SEIO – PARA UM RECÉM-NASCIDO ALIMENTADO EXCLUSIVAMENTE COM MAMADEIRA SERÁNECESSÁRIA MAIS DE UMA LATA POR SEMANA. DEVE-SE LEMBRAR À MÃE QUE O LEITE MATERNO NÃO É SOMENTE O MELHOR, MAS TAMBÉM O MAIS ECONÔMICO ALIMENTOPARA O LACTENTE. CASO VENHA A SER TOMADA A DECISÃO DE INTRODUZIR A ALIMENTAÇÃO POR MAMADEIRA É IMPORTANTE QUE SEJAM FORNECIDAS INSTRUÇÕES SOBREOS MÉTODOS CORRETOS DE PREPARO COM HIGIENE RESSALTANDO-SE QUE O USO DE MAMADEIRA E ÁGUA NÃO FERVIDAS E DILUIÇÃO INCORRETA PODEM CAUSAR DOENÇAS.OMS – CÓDIGO INTERNACIONAL DE COMERCIALIZAÇÃO DE SUBSTITUTOS DO LEITE MATERNO. WHA 34:22, MAIO DE 1981. PORTARIA Nº 2.051 – MS DE 08 DE NOVEMBRODE 2001, RESOLUÇÃO Nº 222 – ANVISA – MS DE 05 DE AGOSTO DE 2002 E LEI 11.265/06 DE 04.01.2006 – PRESIDÊNCIA DA REPÚBLICA – REGULAMENTAM A COMERCIALIZAÇÃODE ALIMENTOS PARA LACTENTES E CRIANÇAS DE PRIMEIRA INFÂNCIA E TAMBÉM A DE PRODUTOS DE PUERICULTURA CORRELATOS.
A solução paracada situação.Esteja seguroda sua escolhaNAN A.R.: LACTENTES COM REGURGITAÇÃO• Eficaz na redução dos episódios <strong>de</strong> regurgitação. 28-30• Por ser espessada com amido, não interfere na absorção <strong>de</strong> nutrientese é menos suscetível à fermentação e à diarréia. 31-33• Fórmula com tecnologia exclusiva no uso <strong>de</strong> amido pré-gelatinizado, o que dispensao espessamento excessivo e conseqüente ingestão elevada <strong>de</strong> ar e da própria fórmula. 33PRE NAN e FM 85: PARA O RECÉM-NASCIDO PREMATURONAN SEM LACTOSE: INTOLERÂNCIA À LACTOSE• Maiores quantida<strong>de</strong>s <strong>de</strong> energia, necessárias ao rápido crescimento. 1• Proteína do soro <strong>de</strong> leite, proporcionando ótima digestibilida<strong>de</strong> 2,3e a<strong>de</strong>quado perfil <strong>de</strong> aminoácidos. 4-6• Cálcio <strong>de</strong> alta biodisponibilida<strong>de</strong>, 7-9 essencial para a a<strong>de</strong>quadamineralização óssea.Especializadopara prematuros.Fórmula <strong>de</strong> nutrientes paraser acrescida ao leite materno,para recém-nascidos <strong>de</strong> alto risco.• Malto<strong>de</strong>xtrina como fonte <strong>de</strong> carboidrato, favorecendo o processo absortivopor lactentes que sofrem <strong>de</strong> diarréia. 34• Baixa osmolalida<strong>de</strong>, contribuindo para a melhora da diarréia osmótica. 35• Nucleotí<strong>de</strong>os, contribuindo para a rápida recuperação das vilosida<strong>de</strong>se da mucosa intestinal. 36-38NAN H.A.: REDUÇÃO DO RISCO DE DOENÇAS ALÉRGICASNAN SOY: ALERGIA ÀS PROTEÍNAS DO LEITE DE VACA IgE MEDIADA 39• Proteína do soro <strong>de</strong> leite parcialmente hidrolisada: redução do risco<strong>de</strong> alergia 10-12 e promoção da tolerância oral. 13• DHA e ARA modulam a resposta inflamatória 14-16 e contribuem para aredução dos sintomas alérgicos. 17,18• Nutrientes com efeito bifidogênico proporcionam uma microbiota intestinalsaudável e conseqüentemente mais proteção ao lactente. 19,20• 100% proteína isolada <strong>de</strong> soja com adição <strong>de</strong> L-metionina,sendo <strong>de</strong> a<strong>de</strong>quada digestibilida<strong>de</strong> e <strong>de</strong> alto valor biológico. 40• Isenta <strong>de</strong> sacarose. Malto<strong>de</strong>xtrina como fonte <strong>de</strong> carboidrato, reduzindoo risco <strong>de</strong> fermentação intestinal quando comparada à sacarose. 40NAN COMFORT: LACTENTES COM CONSTIPAÇÃOALFARÉ: ALERGIA ÀS PROTEÍNAS DO LEITE DE VACA 39• A adição <strong>de</strong> prebióticos em Fórmulas Infantis proporciona fezes maismacias e mais freqüentes. 21-24• O uso <strong>de</strong> quantida<strong>de</strong> a<strong>de</strong>quada <strong>de</strong> prebióticos (4g/litro) minimiza o risco<strong>de</strong> perda hídrica e <strong>de</strong> fezes líquidas. 23-27• Única Fórmula à base <strong>de</strong> proteína do soro <strong>de</strong> leite extensamente hidrolisada(80% peptí<strong>de</strong>os e 20% aminoácidos), apresentando melhor valor nutricional. 41,42• Com adição <strong>de</strong> nucleotí<strong>de</strong>os que proporcionam rápida recuperaçãodas vilosida<strong>de</strong>s e da mucosa intestinal. 36-38• Com LC-PUFAS (DHA e GLA) que contribuem para a modulaçãoda resposta inflamatória. 14-16
Fórmula InfantilEspecialAnti-RegurgitaçãoBenefícios obtidos pela cuidadosaadição <strong>de</strong> amido pré-gelatinizado:• NAN A.R. tem adição <strong>de</strong> amido, que ofereceeficácia comprovada na redução dos episódios<strong>de</strong> regurgitação. 28-30• Na ausência do leite materno, NAN A.R. é uma FórmulaInfantil nutricionalmente completa e balanceada, quecontribui para o a<strong>de</strong>quado crescimento e <strong>de</strong>senvolvimentodo lactente e um risco menor <strong>de</strong> obesida<strong>de</strong>, quandocomparada às fórmulas espessadas caseiramente. 43% <strong>de</strong> lactentes com regurgitaçõesmo<strong>de</strong>radas ou graves10090807060504030201000 7 14 Dias• Não interfere na absorção <strong>de</strong> nutrientes como cálcio,ferro e zinco. 31-33Fórmula controleFórmula espessada com amidoFigura 1: Evolução da regurgitação em lactentes entre 1 e 4 meses <strong>de</strong> ida<strong>de</strong> com uso<strong>de</strong> fórmula espessada com amido fórmula não espessada por duas semanas. 30• Espessada com amido, que é menos suscetível à fermentaçãono cólon, reduzindo o risco <strong>de</strong> dor abdominal, cólica e diarréia. 33Viscosida<strong>de</strong> na medida certa,mais segurança.A mistura <strong>de</strong> amido presente em NAN A.R. é pré-gelatinizadae ao entrar em contato com o pH ácido do estômagogelatiniza, proporcionando o efeito anti-regurgitação:• Viscosida<strong>de</strong> i<strong>de</strong>al.VômitoRegurgitaçãoRGEEntradado estômago• Melhor escoamento da Fórmula.• Evita a prática ina<strong>de</strong>quada <strong>de</strong> cortar o bico da mama<strong>de</strong>irae o conseqüente consumo elevado <strong>de</strong> ar e da própriaFórmula Infantil. 33Em contato com o ácido clorídrico,NAN A.R. gelatiniza, proporcionandoo espessamento da Fórmulae o efeito anti-regurgitante.Imagem meramente ilustrativa
Dicas para o atendimentodo lactente com regurgitação:As atuais recomendações terapêuticas no manejoda regurgitação iniciam-se com a orientação dos pais. 44Referências bibliográficas1. ESPGAN Committee on Nutrition. Nutrition and feeding of preterm infants.Committee on Nutrition of the Preterm Infant. Acta Paediatr 1987;336:1-14. 2. Billeaud C, Guillet J, Sandler B. Gastric emptyingin infants with or without gastroesophageal reflux according to the type of milk. Eur J Clin Nutr 1990; 44:577-83. 3. Tolia V, Lin CH, Kuhns LR. Gastric emptying using three different formulas in infantswith gastroesophageal reflux. J Pediatr Gastroenterol Nutr 1992;15:297-301. 4. Rassin DK, et al. Milk protein quantity and quality in low-birthweight infants. II. Effects on selected aliphatic amino acidsin plasma and urine. Pediatrics 1977;59:407-22. 5. Rassin DK, et al. Milk protein quantity and quality in low-birthweight infants. IV. Effects on tyrosine and phenylalanine in plasma and urine. Pediatrics1977;90:356-60. 6. Goldman HI, et al. Late effects of early dietary protein intake on low-birth-weight infants. J Pediatr 1974;85:764-9. 7. Schuette SA, Knowles JB. Intestinal absorption of Ca(H2PO4)2and Ca citrate compared by two methods. Am J Clin Nutr 1988;47:884-888. 8. Hanning RM, Mitchell MK, Atkinson SA. In vitro solubility of calcium glycerophosphate versus conventional mineral saltsin pediatric parenteral nutrition solutions. J Pediatr Gastroenterol Nutr 1989;9:67-72. 9. Hanning RM, Atkinson AS, Whyte RK. Efficacy of calcium glycerophosphate vs conventional minerals salts fortotal parenteral nutrition in low-birth-weight infants: a randomized clinical trial. Am J Clin Nutr 1991;54:903-908. 10. Baumgartner M et al. Controlled trials investigating the use of one partiallyhydrolysed whey formula for dietary prevention of atopic manifestation until 60 months of age: An overview using meta-analytical techniques. Nut Res 1998;18:1425-42. 11. Von Berg A, et al. The effectRegurgitação e/ouvômitos recorrentesFluxograma <strong>de</strong> <strong>de</strong>cisão terapêuticaof hydrolysed cow’s milk formula for prevention in the first year of life: the German Infant Nutritional Intervention Study, a randomized double-bind trial. J Allergy Clin Immunol 2003;111:533-40.12. Von Berg A, Filipiak-Pittroff B, Krämer U, Link E, Bollrath C, Brockow I, Koletzko S, Grübl A, Heinrich J, Wichmann HE, Bauer CP, Reinhardt D, Ber<strong>de</strong>l D; GINI plus study group. Preventive effect ofhydrolyzed infant formulas persists until age 6 years: long-term results from the German Infant Nutritional Intervention Study (GINI). J Allergy Clin Immunol. 2008 Jun;121(6):1442-7. 13. Fritsche Ret al Induction of systemic immunologic tolerance to beta-lactoglobulin by oral administration of a whey protein hydrolysate. J Allergy Clin Immunol 1997;100(2):266-73. 14. Cal<strong>de</strong>r PC. PolyunsaturatedHistória e examefísico <strong>de</strong>talhadosfatty acids, inflammation, and immunity. Lipids 2001;36:1007-24. 15. Prescott SL, Cal<strong>de</strong>r PC. N-3 polyunsaturated fatty acids and allergic disease. Curr Opin Cli Nutr Metab Care 2004;7:123-9.16. Nafstad P, Nystad W, Magnus P, Jaakkola JJ. Asthma and allergic rhinitis at 4 years of age in relation to fish consumption in infancy. J asthma 2003;40:343-348. 17. Mihrshahi S, Peat JK, MarksGB, et al. Eighteen-month outcomes of house dust mite avoidance and dietary fatty acid modification in the childhood Asthma Prevention Study (CAPS). J Allergy Clin Immunol 2003;111:162-168.Há sinais <strong>de</strong> riscoou <strong>de</strong> DRGESimAmpliar a investigaçãopara DRGE18. Peat JK, et al. Three years outcomes of dietary fatty acid modification and house dust mite reduction in the Childhood Asthma Prevention Study. J Allerg Clin Immunol 2004;114(4):807-813.19. Walker WA. Role of nutrients and bacterial colonization in the <strong>de</strong>velopment of intestinal host <strong>de</strong>fense. J Pediatr Gastroenterol Nutr. 2000;30 Suppl 2:S2-7. 20. Cummings JH, Antoine JM, Azpiroz F,NãoConsi<strong>de</strong>rar como RGEfisiológicoMEDIDAS DIETÉTICASBour<strong>de</strong>t-Sicard R, Brandtzaeg P, Cal<strong>de</strong>r PC, Gibson GR, Guarner F, Isolauri E, Pannemans D, Shortt C, Tuijtelaars S, Watzl B. PASSCLAIM--gut health and immunity. Eur J Nutr. 2004 Jun;43 Suppl 2:II118-II173. 18. 21. Vivatvakin B, Mahayosnond A,Theamboonlert A, Steenhout P, Conus N. Effects of a Whey predominant starter formula containing LcPufas (DHA/ARA) and Oligosacchari<strong>de</strong>s (GOS/FOS) ongastrointestinal comfort in infants. Abstract accept to apresentation in Asia Pacific Congress of Pediatrics ,Shanghai ,October 14-18 ,2009. 22. Costalos C, Kapiki A, Apostolou M, Papathoma E. Theeffect of a prebiotic supplemented formula on growth and stool microbiology of term infants Early Hum Dev. 2008 Jan;84(1):45-9. 23. Agostoni C, Axelsson I, Goulet O et al. Prebiotic oligossacchari<strong>de</strong>sModificado <strong>de</strong> Van<strong>de</strong>nplas et al. 2009 44• Orientação dos pais• Educação postural• Fracionamento da dieta• Consi<strong>de</strong>rar uso <strong>de</strong> FI espessadaMelhora dossintomase/ou resolução por volta<strong>de</strong> 12 meses?SimCriança saudávelNão• Fórmulas infantis espessadas, no casoda ausência do leite materno.• Fracionamento: alimentos ingeridosem menor volume por refeição.Ampliar a investigaçãopara DRGEin dietetic products for infants: A commentary by the ESPGHAN Committee on Nutrition. J Pediatr 2004;39:465-473. 24. Moro G, Minoli I, Mosca M, Fanaro S, Jelinek J, Stahl B, Boehm G. Dosage-relatedbifidogenic effects of galacto- and fructooligosacchari<strong>de</strong>s in formula-fed term infants. J Pediatr Gastroenterol Nutr. 2002 Mar;34(3):291-5. 25. Scientific Committee on Food (2001). Statement on the use ofresistant short chain carbohydrates (oligofructose and oligogalactose) in infant formulae and in follow-on formulae, expressed on 26 September 2001. 26. Scientific Committee on Food (2001).Additional statement on the use of resistant short chain carbohydrates (oligofructosyl-saccharose and oligogalactosyl-lactose) in infant formulae and in follow-on formulae, expressed on 13 December 2001.27. Veitl V, et al. Akzeptanz, Toleranz und Wirksamkeit von milupa Comformil bei Säuglingen mit kleineren Ernährungs- und Verdauungsproblemen. J Ernährungsmed 2000;2:14-20. 28. Chevallier B, GrunbergJ, Rives JJ, Van Egroo LD, Fichot MC Évaluation <strong>de</strong> la tolérance et <strong>de</strong> l’efficacité dún lait épaissi à l’amidon <strong>de</strong> maïs chez les nourrissons présentant <strong>de</strong>s régurgitations simples. Annales <strong>de</strong> Pédiatrie1998;45:509-515. 29. Infante D, Tormo R, Clinical study of the dietary treatment of regurgitation with a thickened infant formula. Clinical trial with Nidina AR. In Nidina AR ensayos clinicos PulsoEdiciones, SA, Nestle Espana SA 1998;4-11. 30. Valver<strong>de</strong> A, et al. Clinical trial with Nidina AR. In Nidina AR ensayos clinicos Pulso Ediciones, SA, Nestle Espana SA 1998;14-28. 31. Bosscher D, MichelineVCB, Van Cauwenbergh R, et al. Availabilities of calcium, iron, and zinc from dairy infant formulas is affected by soluble dietary fibers and modified starch fractions. Basic Nutrition Investigation2003;19:641-645. 32. Bosscher D, Micheline VCB, Kristien VD. Thickening infant formula with digestible and indigestible carboydrate: availability of calcium, iron, and zinc in vitro. J Pediatr GastroenterolNutr 2000;30(4):373-378. 33. Van<strong>de</strong>nplas Y. Nutritional Management of Regurgitation in Infants. Journal of the American College of Nutrition 1998;17(4):308-316. 34. Lebenthal E, et al. Corn syrupsugars: in vitro and in vivo digestibility and clinical intolerance in acute diarrhoea in infancy. J Pediatr. 1983;103:29-34. 35. Leite AZG, Santos PZ, Feferbaum R. Fórmulas. In: Feferbaum R, Falcão MC.Nutrição do recém-nascido. Editora Atheneu 280-299. 2003. 36. Uauy R, Stringel G, Thomas R, Quan R. Effect of dietary nucleosi<strong>de</strong>s on growth and maturation of the <strong>de</strong>veloping gut in the rat. J PediatrGastroenterol Nutr 1990;10:497-503. 37. Nunez MC, Ayudarte MV, Morales D, Suarez MD, Gil A. Effect of dietary nucleoti<strong>de</strong>s on intestinal repair in rats with experimental chronic diarrhea. JPEN JParenter Enteral Nutr 1990;14:598-604. 38. Ortega MA, Nunez MC, Gil A, Sanchez-Pozo A. Dietary nucleoti<strong>de</strong>s accelerate intestinal recovery after food <strong>de</strong>privation in old rats. J Nutr 1995;125:1413-1418.As orientações relacionadas a como preparar a mama<strong>de</strong>ira po<strong>de</strong>rão facilitar o dia-a-diados pais <strong>de</strong> lactentes com regurgitação e, conseqüentemente, a maior a<strong>de</strong>sãoàs orientações dadas pelo Pediatra.A mama<strong>de</strong>ira <strong>de</strong>verá ser preparada da seguinte forma: <strong>de</strong>speje meta<strong>de</strong> da quantida<strong>de</strong><strong>de</strong> água morna previamente fervida. Adicione a quantida<strong>de</strong> <strong>de</strong> pó. Complete com o restanteda água, tampe a mama<strong>de</strong>ira e agite bem até que o pó se dissolva completamente.39. Sole D, Silva LR, Rosário Filho N, Sarni ROS, et al. Consenso Brasileiro sobre Alergia Alimentar. Revista Brasileira <strong>de</strong> Alergia e Imunopatologia 2008;31(2):65-90. 40. Lopez FA, Juzwiak CR. O uso<strong>de</strong> Fórmulas Infantis após o <strong>de</strong>smame. Temas <strong>de</strong> Pediatria n° 74. 2003. 41. Maire JC, Jarret A, Vuichoud J, Moënnoz D. protein nutritional quality of a new therapeutic formula (THERA-11A) –Comparison with ALFARE and two competitor products. R&D Report N° RE-SR960100 30.09.1996. 42. Oggero R, Cagliero T, Spinello M, Bertolone D, Cali M, Biasetti S. Post-enteric refeeding in theinfant. Evaluation and comparison of the effectiveness of several diet therapeutic foods. Minerva Pediatr. 31-10-1985;37:787-794. 43. Penna FJ, et al. Comparação entre uma fórmula infantilpré-espessada e fórmula <strong>de</strong> espessamento caseiro no tratamento do refluxo gastroesofágico. J Pediatr 2003;79(1):49. 44. Van<strong>de</strong>nplas Y, Rudolph CD Van<strong>de</strong>nplas Y, Rudolph CD,Di Lorenzo C, Hassall E, Liptak G, Mazur L, Sondheimer J, Staiano A, Thomson M, Veereman-Wauters G, Wenzl TG; Co-Chairs:; Committee Members:. PediatricGastroesophageal Reflux Clinical Practice Gui<strong>de</strong>lines: Joint Recommendations of the North American Society of Pediatric Gastroenterology, Hepatology, andNutrition and the European Society of Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr. 2009;49:498-547.45. Socieda<strong>de</strong> Brasileira <strong>de</strong> Pediatria. Departamento <strong>de</strong> Nutrologia. Manual <strong>de</strong> orientação para alimentação do lactente,do pré-escolar, do escolar, do adolescente e na escola. São Paulo: Socieda<strong>de</strong> Brasileira <strong>de</strong> Pediatria.Departamento <strong>de</strong> Nutrologia, 2008. 2ª edição. 120p.