Toxicidade do fluoreto - Faculdade de Odontologia de Piracicaba
Toxicidade do fluoreto - Faculdade de Odontologia de Piracicaba
Toxicidade do fluoreto - Faculdade de Odontologia de Piracicaba

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Toxicida<strong>de</strong></strong> <strong>do</strong> flúor
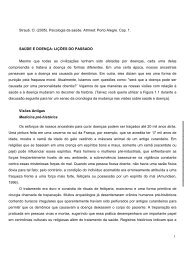
Concentração <strong>de</strong> F no plasma em função <strong>do</strong><br />
tempo após a ingestão<br />
[F] plasma<br />
horas
Utilização ina<strong>de</strong>quada <strong>do</strong> flúor<br />
<strong>Toxicida<strong>de</strong></strong> Aguda<br />
<strong>Toxicida<strong>de</strong></strong> Crônica<br />
náusea<br />
vômito<br />
parada cardíaca<br />
morte<br />
DOSE = 5,0 mg F/Kg<br />
DPT
• Náusea, vômito, <strong>do</strong>r ab<strong>do</strong>minal alguns minutos após a<br />
ingestão<br />
<strong>Toxicida<strong>de</strong></strong> aguda<br />
• Sintomas não específicos: hipersalivação, diarréia, <strong>do</strong>r <strong>de</strong><br />
cabeça, suor frio ou convulsões<br />
• Fraqueza geral, espasmo das extremida<strong>de</strong>s e tetania<br />
• Declínio das concentrações plasmáticas <strong>de</strong> Ca e aumento<br />
das concentrações <strong>de</strong> K<br />
• Queda da pressão, <strong>de</strong>pressão respiratória, aci<strong>do</strong>se<br />
respiratória, arritmia cardíaca<br />
• Morte após algumas horas, precedida por extrema<br />
<strong>de</strong>sorientação ou coma<br />
Fejerskov, O.; Ekstrand, J; Burt, B.A. (eds.) Fluori<strong>de</strong> in Dentistry. 2.ed., 1996
Casos <strong>de</strong> intoxicação aguda<br />
inseticida NaF 90% na refeição <strong>do</strong><br />
hospital<br />
200 comprimi<strong>do</strong>s NaF (suplementos)<br />
ingeri<strong>do</strong>s por uma criança<br />
ATF com gel 33% NaF (145.000 ppm F)<br />
Aci<strong>de</strong>ntes: utilização ina<strong>de</strong>quada <strong>de</strong> produtos<br />
fluoreta<strong>do</strong>s!
Suplementos <strong>de</strong> F<br />
<strong>Toxicida<strong>de</strong></strong> aguda<br />
• Local: Áustria<br />
• Menino <strong>de</strong> 3 anos – peso <strong>de</strong> 12,5 kg<br />
• Produto: comprimi<strong>do</strong> <strong>de</strong> 1,0 mg F<br />
• Causa: ingestão <strong>de</strong> 200 comprimi<strong>do</strong>s<br />
• Dose: 16 mg F/kg peso<br />
• Tempo <strong>de</strong> morte: 7 h após ingestão<br />
EICHLER et al. Int. J. Clin. Pharmacol. Ther. Toxicol., 20:334-8, 1982
Intoxicação aguda letal em<br />
consultório<br />
• Local: Maceió, AL, 12/07/87<br />
• Vítima: menino <strong>de</strong> 3 anos<br />
• Produto: Fluor<strong>de</strong>nt (33% <strong>de</strong> NaF)<br />
• Causa: Uso in<strong>de</strong>vi<strong>do</strong> e <strong>de</strong>sconheci<strong>do</strong><br />
sobre a segurança <strong>do</strong> flúor<br />
• Dose: 15-30 mg F/kg ()<br />
• Tempo <strong>de</strong> morte: 4 h após ingestão<br />
Gazeta Alagoas, 08/89
<strong>Toxicida<strong>de</strong></strong> da solução <strong>de</strong> NaF 10%<br />
1 copinho 10 mL = 450 mg F<br />
DPT = 5 mg F/ kg<br />
450 mg F = 90 kg<br />
5 mg F/ kg<br />
Trata-se <strong>de</strong> Dose<br />
Provavelmente Tóxica para<br />
uma pessoa <strong>de</strong> 90 kg !!!<br />
Criança <strong>de</strong> 30 kg:<br />
450 mg F = 15 mg F/ kg<br />
30 kg<br />
Trata-se<br />
<strong>de</strong> uma <strong>do</strong>se 3x<br />
maior que a DPT !
Doses provavelmente tóxicas <strong>de</strong> flúor<br />
para uma criança <strong>de</strong> 20 Kg<br />
Méto<strong>do</strong>/ Concentração<br />
Comprimi<strong>do</strong> 2,21 mg NaF<br />
Dentifrício/1000 ppm F<br />
Gel 1,23%<br />
Verniz NaF 2,26%<br />
Solução NaF 0,05%<br />
Solução NaF 0,2%<br />
Solução NaF 2%<br />
Equivale a<br />
1 mg F/comp.<br />
1 mg F/g<br />
12,3 mg F/g<br />
22,6 mg F/g<br />
0,225 mg F/mL<br />
0,9 mg F/mL<br />
9 mg F/mL<br />
DPT<br />
100 comp.<br />
100 g<br />
8,1 g<br />
4,4 mL<br />
444 mL<br />
111 mL<br />
11 mL
Aplicação tópica <strong>de</strong> F profissional
ATF e toxicida<strong>de</strong> aguda<br />
Dose em relação<br />
mg F / Kg<br />
Aplica<strong>do</strong> (Mol<strong>de</strong>ira) 2,7<br />
Ingeri<strong>do</strong> (cuspir 1 min.) 0,7<br />
DPT = 5,0 mg F/Kg<br />
Anais da SBPqO, 48, 1989
ATF gel FFA: 1,23% F -<br />
• Associação com mal-estar gástrico (náuseas e<br />
vômitos): cerca <strong>de</strong> 25% <strong>do</strong> gel é ingeri<strong>do</strong><br />
• Medidas <strong>de</strong> precaução:<br />
– colocar pouco gel na mol<strong>de</strong>ira<br />
– paciente na posição vertical<br />
– utilizar suga<strong>do</strong>r<br />
– recomendar ao paciente cuspir exaustivamente
Tratamento <strong>de</strong> intoxicação aguda<br />
• Até 5 mg F/ kg:<br />
– cálcio via oral (leite) ou hidróxi<strong>do</strong> <strong>de</strong> alumínio<br />
– observação<br />
• Acima <strong>de</strong> 5 mg F/ kg:<br />
– induzir vômito<br />
– hidróxi<strong>do</strong> <strong>de</strong> alumínio via oral<br />
– cálcio via oral (leite, gluconato <strong>de</strong> cálcio)<br />
– internação hospitalar imediata, para observação<br />
Intoxicação aguda pela Ingestão <strong>de</strong> Fluoreto. In: Emergências Médicas em<br />
O<strong>do</strong>ntologia, 2002, p. 131-8.
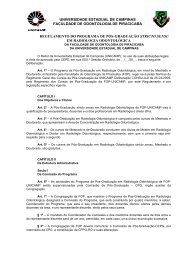
Absorção X pH gástrico<br />
[ F ]<br />
plasma<br />
ATF gel<br />
Al(OH)<br />
*<br />
3<br />
t<br />
* AntiAci<strong>do</strong> (Pepsamar)<br />
Rosalen & Cury, 1992
Tratamento <strong>de</strong> intoxicação aguda<br />
• Acima <strong>de</strong> 15 mg F/ kg:<br />
– internação hospitalar imediata<br />
– enquanto aguarda socorro, induzir vômito com<br />
eméticos; adicionalmente, ministrar hidróxi<strong>do</strong> <strong>de</strong><br />
alumínio ou cálcio via oral<br />
– em ambiente hospitalar:<br />
• monitoramento cardíaco<br />
• Ca ++ en<strong>do</strong>venoso<br />
• glicose e soro bicarbonata<strong>do</strong><br />
• medidas <strong>de</strong> suporte para prevenção <strong>de</strong> colapso<br />
respiratório e cardiovascular<br />
Intoxicação aguda pela Ingestão <strong>de</strong> Fluoreto. In: Emergências Médicas em<br />
O<strong>do</strong>ntologia, 2002, p. 131-8.
Uso<br />
a<strong>de</strong>qua<strong>do</strong><br />
<strong>do</strong> flúor
Fluorose<br />
Cárie <strong>de</strong>ntal
Utilização ina<strong>de</strong>quada <strong>do</strong> flúor<br />
<strong>Toxicida<strong>de</strong></strong> Aguda<br />
<strong>Toxicida<strong>de</strong></strong> Crônica<br />
náusea<br />
vômito<br />
parada cardíaca<br />
morte<br />
DOSE = 5,0 mg F/Kg<br />
DPT<br />
Fluorose Dental<br />
DOSE = 0,07 mg F/Kg<br />
Limite Superior<br />
Fluorose Esquelética<br />
DOSE = 0,7 mg F/Kg
Composição química <strong>do</strong><br />
esmalte<br />
Composição<br />
Esmalte<br />
Inorgânica 95<br />
Orgânica 2<br />
Água 3<br />
MJÖR; FEJERSKOV, 1990
Mineralização <strong>do</strong> esmalte <strong>de</strong>ntal<br />
ameloblasto<br />
ameloblasto<br />
matriz proteica<br />
(25% proteínas)<br />
matriz proteica (25% proteínas)<br />
mineralização<br />
(95% Mineral<br />
Porosida<strong>de</strong><br />
OPACIDADE
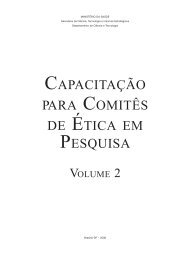
Microscopia <strong>de</strong> luz polarizada<br />
Esmalte normal<br />
Esmalte com fluorose
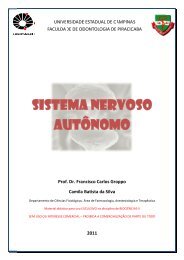
Fluorose<br />
• Perío<strong>do</strong> crítico para o acometimento <strong>do</strong>s<br />
incisivos centrais superiores 20 aos<br />
30 meses<br />
FEJERSKOV, O.; EKSTRAND, J.; BURT, B.A. Fluori<strong>de</strong> in <strong>de</strong>ntistry, 1996
0,03 ppm F 0,7 ppm F<br />
1,6 ppm F 2,5 ppm F
Fluorose <strong>de</strong>ntal<br />
• Aumento da prevalência nos países <strong>de</strong>senvolvi<strong>do</strong>s<br />
• Causan<strong>do</strong> expectativa nos em <strong>de</strong>senvolvimento que tem<br />
prevenção centrada no uso <strong>de</strong> <strong>fluoreto</strong><br />
Lima & cury, rev saú<strong>de</strong> pública 35(6), 2001<br />
“É o único efeito colateral conheci<strong>do</strong><br />
associa<strong>do</strong> a exposição sistêmica a<br />
baixas <strong>do</strong>se <strong>de</strong> <strong>fluoreto</strong>”<br />
EKSTRAND, 1989
Fluorose em crianças <strong>de</strong> 12 anos no<br />
esta<strong>do</strong> <strong>de</strong> São Paulo, 2002<br />
10% 2% 1% 0%<br />
10%<br />
Normal<br />
Questionável<br />
Muito leve<br />
Leve<br />
Mo<strong>de</strong>rada<br />
Severa<br />
77%
Community Dent Oral Epi<strong>de</strong>miol. 2004 Apr;32<br />
Suppl 1:9-18.<br />
A review of fluorosis in the European Union: prevalence, risk factors and<br />
aesthetic issues.<br />
Whelton HP, Ketley CE, McSweeney F, O'Mullane DM.<br />
Fluori<strong>de</strong> has played a key role in caries prevention for the past 50 years<br />
but excessive ingestion of fluori<strong>de</strong> during tooth <strong>de</strong>velopment may lead<br />
to <strong>de</strong>ntal fluorosis. Throughout Europe many vehicles have been, and are<br />
currently, employed for optimal fluori<strong>de</strong> <strong>de</strong>livery including drinking water,<br />
toothpaste, fluori<strong>de</strong> supplements, salt and milk..<br />
Overall the evi<strong>de</strong>nce would<br />
appear to indicate, however, that diffuse enamel opacities are more prevalent in<br />
fluoridated than in nonfluoridated communities and that their prevalence at the<br />
very mild level may be increasing. In addition to fluoridated drinking water, risk<br />
factors for fluorosis inclu<strong>de</strong> inadvertent ingestion of fluori<strong>de</strong> toothpaste and<br />
the inappropriate use of fluori<strong>de</strong> supplements. The risk is of aesthetic concern<br />
primarily during the period of enamel <strong>de</strong>velopment of the permanent central<br />
incisors, although this largely appears to be a cosmetic rather than a public-<br />
health issue.<br />
Furthermore, a importância estética da fluorose precisa<br />
ser <strong>de</strong>terminada em maiores <strong>de</strong>talhes em cada país in<br />
the light of each country's respective risk factors and <strong>de</strong>ntal<br />
health policies.
Municípios<br />
ppm F<br />
Cor<strong>de</strong>irópolis, SP<br />
n =24<br />
*<strong>Piracicaba</strong>, SP<br />
n = 57<br />
0,03 ± 0,01<br />
0,64 ± 0,01<br />
(0,02 – 0,04)<br />
(0,61<br />
– 0,66)<br />
Assistência, SP<br />
n = 43<br />
Rafael Arruda, CE<br />
n = 47<br />
1,10 ± 0,49<br />
1,22 ±0,66<br />
(0,07 – 1,57)<br />
(0,33 – 2,55)<br />
*Rev Saú<strong>de</strong> Pub 36(6) 2002<br />
Bezerra <strong>de</strong> Menezes et al. 2001
Satisfação com seus <strong>de</strong>ntes <br />
70<br />
Sim<br />
Não<br />
Não Sabe<br />
Porcentagem (%)<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
Cor<strong>de</strong>irópolis <strong>Piracicaba</strong><br />
Assistência<br />
Rafael Arruda<br />
Não Fluoretada Ótima 2x Ótima 3x Ótima
Meios <strong>de</strong> usar flúor associa<strong>do</strong>s com<br />
risco <strong>de</strong> fluorose <strong>de</strong>ntal<br />
1- Diretamente<br />
• Flúor da água<br />
• Suplementos <strong>de</strong> flúor<br />
2- Indiretamente<br />
• Dentifrício fluoreta<strong>do</strong><br />
As principais fontes <strong>de</strong> <strong>fluoreto</strong> associadas ao aumento da prevalência<br />
da fluorose <strong>de</strong>ntal são água, suplementos, <strong>de</strong>ntifrícios e alimentos<br />
industrializa<strong>do</strong>s infantis consumi<strong>do</strong>s antes <strong>do</strong>s seis anos <strong>de</strong> ida<strong>de</strong>.<br />
Mascarenhas, 2000
Uso <strong>de</strong> Flúor no SUS-SP SP e Risco <strong>de</strong> Cárie<br />
RSS-95, <strong>de</strong> 27/06/20002000<br />
1- PRÉ-NATAL<br />
“Não se justifica por não causar nenhum benefício”<br />
2- PÓS-NATAL<br />
• Saú<strong>de</strong> Pública : Não recomenda<strong>do</strong><br />
• Individual : Prescrição Limitada<br />
www.sau<strong>de</strong>.sp.gov.br<br />
Narvai et al. Uso <strong>de</strong> produtos fluora<strong>do</strong>s conforme o risco<strong>de</strong> cárie. Rev APCD<br />
56(2), 2002
Temperatura x ingestão <strong>de</strong> H 2 O F x <strong>do</strong>se<br />
Fórmula <strong>de</strong> Galagan & Vermillion<br />
Litros/ Kg = - 0,0025 + 0,0004 x Média Máx Temp. (ºF)<br />
Dose Limite = 0,07 mg F/Kg
Dose <strong>de</strong> <strong>fluoreto</strong> a que crianças <strong>de</strong> 20 a 30 meses<br />
são expostas (mgF/kg peso/dia)<br />
Comunida<strong>de</strong><br />
Dieta<br />
Dentifrício<br />
Dieta + <strong>de</strong>ntifrício<br />
Ibiá (MG)<br />
0,027 ± 0,013 A,a<br />
0,061 ± 0,045 A,b<br />
0,088 ± 0,049 A<br />
(0,022 - 0,031)<br />
(0,046 - 0,077)<br />
(0,071 - 0,105)<br />
<strong>Piracicaba</strong> (SP)<br />
0,040 ± 0,009 B,a<br />
0,052 ± 0,019 A,b<br />
0,090 ± 0,022 A<br />
(0,037 - 0,042)<br />
(0,046 - 0,058)<br />
(0,083 - 0,097)<br />
Média ± d.p.; (intervalo <strong>de</strong> confiança-95%)<br />
Médias seguidas por letras distintas diferem significantemente (p
Fluorose em crianças <strong>de</strong> 12 anos no esta<strong>do</strong> <strong>de</strong><br />
São Paulo, 2002, <strong>de</strong> acor<strong>do</strong> com a fluoretação da<br />
água <strong>de</strong> abastecimento público<br />
% <strong>de</strong> crianças<br />
15<br />
12<br />
9<br />
6<br />
3<br />
Fluorose muito leve<br />
Fluorose leve<br />
Fluorose mo<strong>de</strong>rada<br />
Fluorose severa<br />
0<br />
Água não fluoretada<br />
Água fluoretada<br />
Cida<strong>de</strong>s
Acta O<strong>do</strong>ntol Scand. 1999 Oct;57<br />
57(5):247-56<br />
"Risk periods" associated with the <strong>de</strong>velopment of <strong>de</strong>ntal fluorosis in<br />
maxillary permanent central incisors: a meta-analysis.<br />
Bardsen A.<br />
This systematic review of the <strong>de</strong>ntal literature (1966-98) concerns risk periods<br />
associated with <strong>de</strong>ntal fluorosis in the maxillary permanent central incisors. A<br />
literature search was organized through the MedLine and the ISI databases. In<br />
addition, one unpublished paper (in manuscript) was obtained, as well as one<br />
paper published before 1966. However, out of 143 catches, only 10 studies were<br />
inclu<strong>de</strong>d in this review. The meta-analysis<br />
analysis now revealed an overall OR of 5.83<br />
(95% CI; 2.83-11.94) for long periods of fluori<strong>de</strong> exposure (>2 out of the first 4<br />
years) versus shorter periods of exposure (
Catani et al. Relação entre níveis <strong>de</strong> <strong>fluoreto</strong> na água<br />
<strong>de</strong> abastecimento público e fluorose <strong>de</strong>ntal.<br />
Rev Saú<strong>de</strong> Publica; 41:732-9, 2007<br />
RESULTADOS: A prevalência <strong>de</strong> fluorose no município com<br />
teores<br />
oscilantes<br />
<strong>de</strong><br />
flúor<br />
na<br />
água<br />
foi<br />
<strong>de</strong> 31,4% e no<br />
município com teores homogêneos foi <strong>de</strong> 79,9%. Entretanto,<br />
em ambos os municípios prevaleceu o grau muito leve <strong>de</strong><br />
fluorose. A prevalência <strong>de</strong> fluorose foi associada com o<br />
município com teores <strong>de</strong> flúor homogêneos na água [OR<br />
=8,33, 95% IC: 5,15-13,45] e não possuir automóvel [OR=2,10<br />
10,<br />
95% IC: 1,27<br />
27-3,49<br />
49].<br />
CONCLUSÃO: Embora a prevalência <strong>de</strong> fluorose tenha<br />
si<strong>do</strong> maior nas crianças <strong>do</strong> município que possuía<br />
melhor controle da concentração ótima <strong>de</strong> <strong>fluoreto</strong> na<br />
água, esta não afetou a estética <strong>de</strong>ntal <strong>do</strong>s<br />
comprometi<strong>do</strong>s.
1,2<br />
1,0<br />
0,8<br />
µg F total/g<br />
µg F solúvel/g<br />
Água fluoretada<br />
2,5<br />
2<br />
µg F total/g<br />
µg F solúvel/g<br />
Água fluoretada<br />
µg F/g<br />
0,6<br />
0,4<br />
0,2<br />
Água <strong>de</strong>stilada e<br />
<strong>de</strong>ionizada<br />
µg F/g<br />
1,5<br />
1<br />
0,5<br />
Água <strong>de</strong>stilada e<br />
<strong>de</strong>ionizada<br />
0<br />
TioJoão<br />
Prato<br />
Fino<br />
Camil<br />
ARROZ<br />
TioJoão<br />
Prato<br />
Fino<br />
Camil<br />
0<br />
Broto<br />
legal<br />
Grão <strong>de</strong><br />
Campo<br />
Vence<strong>do</strong>r<br />
FEIJÃO<br />
Broto<br />
legal<br />
Grão <strong>de</strong><br />
Campo<br />
Vence<strong>do</strong>r<br />
Casarin; Lima; Cury. Anais da SBPqO, 2002<br />
Casarin; Lima; Cury. Anais da SBPqO, 2002<br />
RESULTADOS: A concentração <strong>de</strong> <strong>fluoreto</strong> encontrada nos grãos <strong>de</strong> arroz<br />
e feijão foi baixa, mas sua concentração aumentou <strong>de</strong> 100-200<br />
vezes<br />
após cozimento em água fluoretada, e mesmo assim, foi menor que a<br />
encontrada em alguns alimentos industrializa<strong>do</strong>s.<br />
Uma refeição com arroz-feijão preparada com água fluoretada seria<br />
responsável por 29% da <strong>do</strong>se limite <strong>de</strong> ingestão <strong>de</strong> <strong>fluoreto</strong> em termos <strong>de</strong><br />
uma fluorose aceitável, enquanto que a contribuição <strong>de</strong> alguns alimentos<br />
industrializa<strong>do</strong>s atingiria 45%.<br />
Casarin et al., Rev Saú<strong>de</strong> Pública 41(4) 2007
Uso<br />
a<strong>de</strong>qua<strong>do</strong><br />
<strong>do</strong> flúor
1 lata/dia: 2 x superior à <strong>do</strong>se limite<br />
diária para criança <strong>de</strong> 12 Kg<br />
Hayacibara et al., Rev Saú<strong>de</strong> Pública, 2004
• 0,4 mg F/unida<strong>de</strong><br />
• 2 Tabletes = Dose limite fluorose <strong>de</strong>ntal - 10 Kg
Dentifrício fluoreta<strong>do</strong> e efeito sistêmico<br />
Estu<strong>do</strong>s<br />
mg F/kg/dia<br />
Local<br />
Lima & Cury, 1998* 0,052052 Creche, <strong>Piracicaba</strong><br />
Paiva & Cury, 1998**<br />
0,061061 Domiciliar, Ibiá<br />
n =39*;32**<br />
Ida<strong>de</strong> = 20-30<br />
meses<br />
1. Crianças que já escovam os <strong>de</strong>ntes com <strong>de</strong>ntifrício<br />
fluoreta<strong>do</strong> estão sen<strong>do</strong> submetidas a uma <strong>do</strong>se <strong>de</strong><br />
flúor que contraindicaria uma suplementação<br />
2. Po<strong>de</strong>rá haver sobre<strong>do</strong>se com água fluoretada<br />
Paiva, Lima e Cury. Community Dent Oral Epi<strong>de</strong>miol, 31(3) 2003
Risco <strong>de</strong> fluorose <strong>de</strong>ntal pelo uso <strong>de</strong><br />
<strong>de</strong>ntifrício fluoreta<strong>do</strong><br />
1- É esperada uma prevalência <strong>de</strong> fluorose<br />
<strong>de</strong>ntal <strong>de</strong> até 28%;<br />
2- A menor prevalência seria explicada:<br />
- Superestimação na frequência <strong>de</strong> escovação<br />
- Nem to<strong>do</strong> flúor ingeri<strong>do</strong> é absorvi<strong>do</strong><br />
Fejerskov et al, 1996
Absorção <strong>de</strong> <strong>fluoreto</strong> ingeri<strong>do</strong> a partir <strong>de</strong><br />
<strong>de</strong>ntifrício com 1100 ppm F em jejum ou 15 min<br />
após as refeições<br />
Refeição<br />
% absorção<br />
Jejum 100<br />
Café da manhã 71<br />
Almoço 61<br />
Cury, Del Fiol, Tenuta, Rosalen. Journal of Dental Research, 2005
Biodisponibilida<strong>de</strong> <strong>do</strong> <strong>fluoreto</strong> ingeri<strong>do</strong> a partir <strong>de</strong><br />
<strong>de</strong>ntifrícios, <strong>de</strong> acor<strong>do</strong> com a refeição prévia<br />
100%<br />
80%<br />
60%<br />
Jejum<br />
Café manhã<br />
Almoço<br />
40%<br />
20%<br />
0%<br />
1100 µg F/g 550 µg F/g<br />
Dentifrícios<br />
Cury, Del Fiol, Tenuta, Rosalen. Journal of Dental Research, 2005
Medidas para reduzir a ingestão total<br />
<strong>de</strong> flúor satisfazen<strong>do</strong> o limite*<br />
<br />
<br />
<br />
reduzir a concentração <strong>de</strong> F na água<br />
(0,3 ppm)<br />
reduzir a concentração <strong>de</strong> F nos<br />
<strong>de</strong>ntifrícios (500-600<br />
ppm)<br />
utilizar pequena quantida<strong>de</strong> <strong>de</strong><br />
<strong>de</strong>ntifrício (0,3 g)<br />
*0,07 mg F/dia/Kg peso corporal<br />
Paiva, Lima e Cury. Community Dent Oral Epi<strong>de</strong>miol, 31(3) 2003
Cárie <strong>de</strong>ntal (CPO-D) em crianças <strong>de</strong> 12 anos no<br />
esta<strong>do</strong> <strong>de</strong> São Paulo, 2002, <strong>de</strong> acor<strong>do</strong> com a<br />
fluoretação da água <strong>de</strong> abastecimento público
J Can Dent Assoc. 2003 May;69(5):286-91.<br />
An update on fluori<strong>de</strong>s and fluorosis.<br />
Levy SM.<br />
College of Dentistry, University of Iowa, Preventive and Community<br />
Dentistry, Iowa City, Iowa 52242, USA.<br />
Decisions concerning use of fluori<strong>de</strong> in its many forms for caries<br />
prevention are more complicated now than in the past because of the<br />
need to balance these benefits with the risks of <strong>de</strong>ntal fluorosis. This<br />
article reviews pertinent literature concerning <strong>de</strong>ntal fluorosis<br />
(<strong>de</strong>finition, appearance, prevalence), pre- and post-eruptive use of<br />
fluori<strong>de</strong>, esthetic perceptions of <strong>de</strong>ntal fluorosis, fluori<strong>de</strong> levels of<br />
beverages and foods, the Iowa Fluori<strong>de</strong> Study, and the U.S. Centers for<br />
Disease Control and Prevention's "Recommendations for Using<br />
Fluori<strong>de</strong> to Prevent and Control Dental Caries in the United States.”<br />
Water fluoridation and use of fluori<strong>de</strong> <strong>de</strong>ntifrice are the<br />
most efficient and cost-effective ways to prevent <strong>de</strong>ntal<br />
caries; other modalities should be targeted toward high-risk<br />
individuals.
Lesão <strong>de</strong> cárie produzida in vitro<br />
Controle<br />
280 ppm F<br />
(simulan<strong>do</strong> diluição <strong>de</strong> <strong>de</strong>ntifrício<br />
<strong>de</strong> 1100 ppm F com saliva)
Caries Res. 2003 Mar-Apr;37(2):85-92.<br />
Systematic review of studies comparing the anti-caries<br />
efficacy of children's toothpaste containing 600 ppm of<br />
fluori<strong>de</strong> or less with high fluori<strong>de</strong> toothpastes of 1,000<br />
ppm or above.<br />
Ammari AB, Bloch-Zupan A, Ashley PF.<br />
Results of the meta-analysis were statistically significant (p = 0.002<br />
and 0.0005) and in favour of the control group (1,000 ppm). DFS<br />
increments in the 250-ppm group were 0.6-0.7 greater than the<br />
1,000-ppm group. 500 PPM: Only two studies were in this category,<br />
and one of them failed to present the baseline caries levels, so a<br />
meta-analysis was not carried out. CONCLUSIONS: 250 ppm fluori<strong>de</strong><br />
<strong>de</strong>ntifrice was not as effective in caries prevention in permanent<br />
<strong>de</strong>ntition as <strong>de</strong>ntifrice containing 1,000 ppm F or more.<br />
More studies have to be carried out to test the anticaries<br />
efficacy of 500 against 1,000 ppm and above.
Disponibilida<strong>de</strong> <strong>de</strong> F na saliva até 60 min após a<br />
escovação com <strong>de</strong>ntifrícios fluoreta<strong>do</strong>s, seguida<br />
ou não <strong>de</strong> um enxágue com água (Média ± EP)<br />
300.0<br />
ASC [F] salivar<br />
250.0<br />
200.0<br />
150.0<br />
100.0<br />
50.0<br />
a<br />
b<br />
b<br />
c<br />
0.0<br />
500 µg F/g<br />
com enxágue<br />
500 µg F/g<br />
sem enxágue<br />
1100 µg F/g<br />
com enxágue<br />
1100 µg F/g<br />
sem enxágue<br />
Zamataro, Tenuta, Cury. Eur Arch Paed Dent, 2008
Eficácia anti-cárie <strong>de</strong> <strong>de</strong>ntifrícios fluoreta<strong>do</strong>s <strong>de</strong><br />
acor<strong>do</strong> com a ativida<strong>de</strong> <strong>de</strong> cárie <strong>do</strong> paciente<br />
Incremento <strong>de</strong> lesões após 1 ano<br />
6.0<br />
5.0<br />
4.0<br />
3.0<br />
2.0<br />
1.0<br />
0.0<br />
-1.0<br />
-2.0<br />
-3.0<br />
Cárie-inativos<br />
Cárie-ativos<br />
500 ppm<br />
1100 ppm<br />
*<br />
• Região <strong>de</strong> água não fluoretada<br />
Lima, Ribeiro, Tenuta, Cury. Caries Res, 2008
Redução da [ F ]<br />
em <strong>de</strong>ntifrícios<br />
•1100 ppm F <strong>de</strong>ntifrício<br />
•crianças com 13,2 kg<br />
•57% ingestão<br />
•0,51 g <strong>de</strong>ntifrício<br />
•2,2 escovações ao dia<br />
• Dose <strong>de</strong>vi<strong>do</strong> ao <strong>de</strong>ntifrício = DDe = 0,05 mg F/ kg (0,007 a 0,185)<br />
• Dose <strong>de</strong>vi<strong>do</strong> à dieta = DDi = 0,04 mg F/ kg (0,017 a 0,074)<br />
• Dose total = DT = 0,09 mg F/ kg (0,041 a 0,223)<br />
LIMA & CURY, Rev Saú<strong>de</strong> Publica USP,2001<br />
SE FOSSE UTILIZADO DENTIFRÍCIO COM 550 ppm F:<br />
EM MÉDIA<br />
DDe = 0,025 mg F/ kg<br />
(+ DDi = 0,04 mg F/kg)<br />
DT = 0,065 mg F/ kg<br />
PARA CASOS EXTREMOS<br />
DDe = 0,09<br />
(+ DDi = 0,04 mg F/ kg)<br />
DT = 0,13 mg F/ kg
Risco <strong>de</strong> fluorose <strong>de</strong>ntal<br />
“Assim, julgamos oportuno que para regiões <strong>de</strong> água<br />
fluoretada haja uma advertência <strong>de</strong> que crianças<br />
menores <strong>de</strong> 6 anos utilizem uma pequena quantida<strong>de</strong> <strong>de</strong><br />
pasta por escovação.”<br />
Cury, J.A. Rev gaúcha o<strong>do</strong>ntol,1986<br />
“Se fosse utiliza<strong>do</strong> 0,3 g <strong>de</strong> <strong>de</strong>ntifrício por escovação<br />
resolveria o problema inclusive <strong>do</strong>s que ingerem maior<br />
quantida<strong>de</strong> <strong>de</strong> pasta.”<br />
Lima, Y.B.O.; Cury, J.A. Rev saú<strong>de</strong> pública USP, 2001
1,0 g 0,3 g 0,15 g
0,11 g<br />
Villena & Cury. In: O<strong>do</strong>ntopediatria na 1 a Infância, 1998
Biodisponibilida<strong>de</strong> <strong>de</strong> F no plasma <strong>de</strong> acor<strong>do</strong> com o mo<strong>do</strong><br />
<strong>de</strong> enxágüe da cavida<strong>de</strong> bucal após o uso <strong>de</strong> <strong>de</strong>ntifrícios<br />
100<br />
% biodisponibilida<strong>de</strong><br />
80<br />
60<br />
40<br />
20<br />
0<br />
Ingestão <strong>do</strong> <strong>de</strong>ntifrício<br />
Expectoração<br />
apenas, sem enxágüe<br />
Enxágue por 1 min com 5<br />
mL <strong>de</strong> água mistura<strong>do</strong> à<br />
espuma e expectoração<br />
Sjögren et al., 1994