Bijlage bij richtlijn Cervixcarcinoom, hoofdstuk Algemeen - Oncoline
Bijlage bij richtlijn Cervixcarcinoom, hoofdstuk Algemeen - Oncoline
Bijlage bij richtlijn Cervixcarcinoom, hoofdstuk Algemeen - Oncoline

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
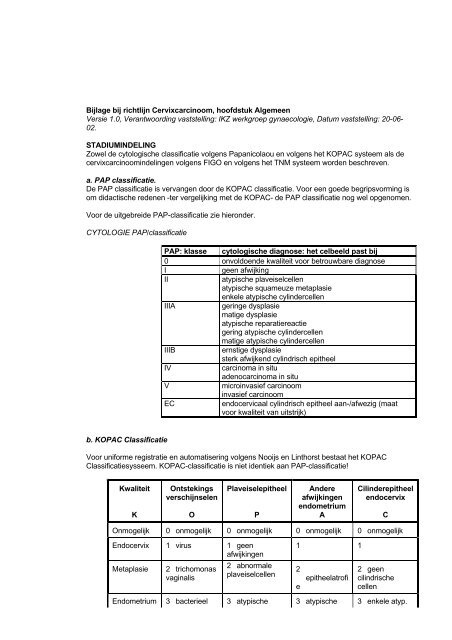
<strong>Bijlage</strong> <strong>bij</strong> <strong>richtlijn</strong> <strong>Cervixcarcinoom</strong>, <strong>hoofdstuk</strong> <strong>Algemeen</strong>Versie 1.0, Verantwoording vaststelling: IKZ werkgroep gynaecologie, Datum vaststelling: 20-06-02.STADIUMINDELINGZowel de cytologische classificatie volgens Papanicolaou en volgens het KOPAC systeem als decervixcarcinoomindelingen volgens FIGO en volgens het TNM systeem worden beschreven.a. PAP classificatie.De PAP classificatie is vervangen door de KOPAC classificatie. Voor een goede begripsvorming isom didactische redenen -ter vergelijking met de KOPAC- de PAP classificatie nog wel opgenomen.Voor de uitgebreide PAP-classificatie zie hieronder.CYTOLOGIE PAP/classificatiePAP: klasse cytologische diagnose: het celbeeld past <strong>bij</strong>0 onvoldoende kwaliteit voor betrouwbare diagnoseIgeen afwijkingIIatypische plaveiselcellenatypische squameuze metaplasieenkele atypische cylindercellenIIIAgeringe dysplasiematige dysplasieatypische reparatiereactiegering atypische cylindercellenmatige atypische cylindercellenIIIBernstige dysplasiesterk afwijkend cylindrisch epitheelIVcarcinoma in situadenocarcinoma in situVmicroinvasief carcinoominvasief carcinoomECendocervicaal cylindrisch epitheel aan-/afwezig (maatvoor kwaliteit van uitstrijk)b. KOPAC ClassificatieVoor uniforme registratie en automatisering volgens Nooijs en Linthorst bestaat het KOPACClassificatiesysseem. KOPAC-classificatie is niet identiek aan PAP-classificatie!KwaliteitKOntstekingsverschijnselenOPlaveiselepitheelPAndereafwijkingenendometriumACilinderepitheelendocervixCOnmogelijk 0 onmogelijk 0 onmogelijk 0 onmogelijk 0 onmogelijkEndocervix 1 virus 1 geenafwijkingenMetaplasie2 trichomonasvaginalis2 abnormaleplaveiselcellen1 12eepitheelatrofi2 geencilindrischecellenEndometrium 3 bacterieel 3 atypische 3 atypische 3 enkele atyp.
FIGOstagesTNMcategoriesT0No evidence of primary tumourTis 0 Carcinoma in situ (preinvasive carcinoma)T1ICervical carcinoma confined to uterus(extension to corpus should be disregarded)T1aIAInvasive carcinoma diagnosed only bymicroscopy. All macroscopically visible lesions– even with superficial invasion - areT1b/Stage IBT1a1T1a2IA1IA2Stromal invasion no greater than 3.0 mm indepth and 7.0 mm or less in horizontal spreadStromal invasion more than 3.0 mm and notmore than 5.0 mm with a horizontal spread7.0 mm or lessNote: the depth of invasion should not bemore than 5 mm taken from the base of theepithelium, either surface or glandular, fromwhich it originates. The depth of invasion isdefined as the measurement of the tumourfrom the epithelial-stromal junction of theadjacent most superficial epithelial papilla tothe deepest point of invasion. Vascular spaceinvolvement, venous or lymphatic, does notaffect classification.T1bIBClinically visible lesion confined to the cervixor microscopic lesion greater than T1a2/IA2T1b1T1b2IB1IB2Clinically visible lesion 4.0 cm or less ingreatest dimensionClinically visible lesion more than 4 cm ingreatest dimensionT2IITumour invades beyond uterus but not topelvic wall or to lower third of the vaginaT3T2aT2bT3aT3bIIIIIAIIBIIIAIIIBWithout parametrial invasionWith parametrial invasionTumour extends to pelvic wall and/or involveslower third of vagina and/or causeshydronephrosis of non-functioning kidneyTumour involves lower third of vagina, noextension to pelvic wallTumour extends to pelvic wall and/or causes
T1aDiagnosed only by microscopyIAT1a1Depth < 3 mm, horizontal spread < 7 mmIA1T1bT1b1T1b2Depth > 3 and ≤ 5 mm, horizontal spread 4 cmIBIA21B11B2T2Beyond uterus but not pelvic wall or lowerthird vaginaIIT2aT2bNo parametriumParametriumIIAIIBT3Lower third vagina / pelvic wall /hydronephrosisIIIT3aT3bLower third vaginaPelvic wall / hydronephrosisIIIAIIIBT4Mucosa of bladder / rectum; beyond truepelvisIVAM1 Distant metastasis IVBBjjlage <strong>bij</strong> <strong>richtlijn</strong> <strong>Cervixcarcinoom</strong>, <strong>hoofdstuk</strong> ScreeningVersie 1.0, Verantwoording vaststelling: IKZ werkgroep gynaecologie, Datum vaststelling: 20-06-02.HERHALINGSADVIEZEN CERVIXUITSTRIJKEN"KLASSE" PAP (herhalings)ADVIESVERVOLGADVIESKOPAC P1, A1-A2, C1KOPAC P2-P3, C3KOPAC P4, C4-C5KOPAC P5PAP 1PAP 2PAP 3APAP 3A5 jaar½ jaar½ jaargynaecoloognormaalafwijkend6 maandengynaecoloognormaal 6 maandenafwijkend gynaecoloogna behandeling na 6-6-12 maandenna géénbehandeling na 6-6 maandenna behandeling na 6-6-12 mnd
KOPAC P6, C6P7, C7KOPAC P9, C9PAP 3BPAP 4PAP 5gynaecolooggynaecoloogna géénbehandelingna 6-6 maandenna behandeling na 6-6-12 maandenna géénbehandeling na 6-6 maandenna behandeling na 6-6-12 maandenKOPAC B2PAP 1cf. KOPAC-uitslagvolgens bovenstaand protocol; <strong>bij</strong>persisterende B2 verwijzing gynaecoloogKOPAC B3PAP 0na 6 wekenvolgens bovenstaand protocol; <strong>bij</strong>persisterende B3 verwijzing gynaecoloogDe aard van het onderzoek zal afhankelijk zijn van de gedetailleerde KOPAC-uitslag.- plaveiselepitheel afwijkend:colposcopie- plaveiselepitheel afwijkend zonder overzicht van squamo-columnar junction (scj):colposcopie evt. aangevuld met endocervicale curettage (ECC)- endocervicaal epitheel afwijkend:colposcopie (+biopten) en ECC- <strong>bij</strong> andere afwijkingen, bv. endometrium tijdens of na de menopauze afwijkend:zie <strong>richtlijn</strong> endometriumcarcinoom<strong>Bijlage</strong> <strong>bij</strong> <strong>richtlijn</strong> <strong>Cervixcarcinoom</strong>, <strong>hoofdstuk</strong> BehandelingVersie 1.0, Verantwoording vaststelling: IKZ werkgroep gynaecologie, Datum vaststelling: 20-06-02.OVERZICHT CIN AFWIJKINGEN EN CARCINOOMHISTOLOGIEColposcopischebioptenLichte en matigedysplasie(CIN I en II)Ernstige dysplasie enCarcinoma in situ(CIN III)Microinvasiefcarcinoom(invasie < 3 mm;< 7 mm breedte)AdviezenGeen symptomen:1. afwachten 6 maanden2. 2.herhaling uitstrijkje(colposcopie optioneel)Wèl symptomen +ectocervicale afwijkingen→ Therapie→ Therapie→ TherapieTherapieWeefselbehoudende therapie:- exconisatie- diathermische lusexcisieWeefselbeschadigende therapie:- cryochirurgie- lasertherapie- exconisatie- diatheramische lusexcisie(- uterusextirpatie)- uterusextirpatie (therapie vanvoorkeur)- exconisatie of ruime lusexcisie(<strong>bij</strong> kinderwens)- (radiotherapie <strong>bij</strong>
stadium Ia1Invasief carcinoom(>3mm)FIGO stadium Ia2-Ib1FIGO-stadium IIa(met tumordiameter≤4cm)FIGO stadium Ib2FIGO stadium IIa(met tumordiameter >4 cm)FIGO Stadium III-Iva→ TherapieVóóronderzoek:inspectie, bimanueel toucheronder narcose,evt. recto-cystoscopie, X-thorax, IVP en/of Echoabdomen,CT-scan abdomen en kleinebekken→ TherapieVóóronderzoek: inspectie,bimanueel onderzoek ondernarcose, evt. rectocystoscopie,X-thorax, IVPen/of ECHO abdomen, CTscanabdomen en kleinebekken, evt. MRI kleinebekken.contraïndicatie voor anderetherapie)Chirurgie:-radicale operatiepre-menopauzaalovaria in situ laten (optioneel)Radiotherapie:- op indicatie postoperatieveradio- en/of chemotherapie (<strong>bij</strong>irradicale ingreep of positievepelvische lymfklieren)- primaire gecombineerderadio/chemotherapie )<strong>bij</strong>contraindicatie voor chirurgischetherapie)Chemotherapie:- niet standaard, enkel intrialverbandStandaard gecombineerderadio/chemotherapie (cisplatinum).Radiotherapie in combinatie metdiepe hyperthermie <strong>bij</strong>contraïndicatie voor cis-platinumChemotherapie: niet standaard,enkel in trial-verband, of evt. alsinductie <strong>bij</strong> para-aortalekliermetastasen.<strong>Bijlage</strong> <strong>bij</strong> <strong>richtlijn</strong> <strong>Cervixcarcinoom</strong>, <strong>hoofdstuk</strong> Follow-upVersie 1.0, Verantwoording vaststelling: IKZ werkgroep gynaecologie, Datum vaststelling: 20-06-02.FOLLOW-UPIngestelde therapie Onderzoek FrequentieExconisatieDiathermischelusexcisieUterusextirpatiePremaligne afwijkingen: Dysplasieën of carcinoma in situAnamneseCervixuitstrijkjes1e keer: na 6 maanden2e keer: na 12 maanden3e keer: na 24 maandenFollow-up alleen voorResearchConisatie of ruimelusexcisieUterusextirpatieMicroinvasief carcinoomAnamneseSpeculumonderzoek met evt. uitstrijkjeRectovaginaal toucher1e jaar: 1x/3 maanden2e jaar: 1x/4 maanden3e - 5e jaar : 1x/6 maanden
RadiotherapieRadicale chirurgieRadiotherapieInfiltrerend carcinoom (> Ia1)Anamnese:• mictie, defaecatie, vaginaalbloedverlies, lage rugpijnLichamelijk onderzoek:• speculumonderzoek, rectovag.toucher, onderzoek abdomen, Inn.supraclaviculair, perifeer oedeemIdem