Zetia - Express Scripts
Zetia - Express Scripts
Zetia - Express Scripts
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
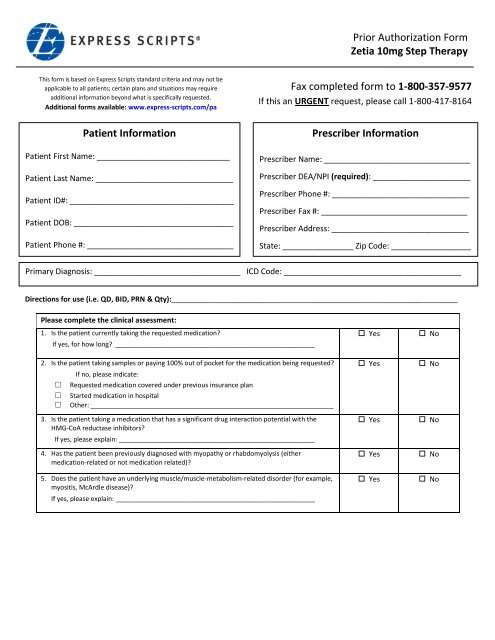
Prior Authorization Form<strong>Zetia</strong> 10mg Step TherapyThis form is based on <strong>Express</strong> <strong>Scripts</strong> standard criteria and may not beapplicable to all patients; certain plans and situations may requireadditional information beyond what is specifically requested.Additional forms available: www.express-scripts.com/paPatient InformationPatient First Name: ______________________________Patient Last Name: _______________________________Patient ID#: _____________________________________Patient DOB: ____________________________________Patient Phone #: _________________________________Fax completed form to 1-800-357-9577If this an URGENT request, please call 1-800-417-8164Prescriber InformationPrescriber Name: _________________________________Prescriber DEA/NPI (required): ______________________Prescriber Phone #: _______________________________Prescriber Fax #: _________________________________Prescriber Address: _______________________________State: ________________ Zip Code: __________________Primary Diagnosis: _________________________________ ICD Code: ________________________________________Directions for use (i.e. QD, BID, PRN & Qty):_______________________________________________________________________Please complete the clinical assessment:1. Is the patient currently taking the requested medication?If yes, for how long? _______________________________________________________2. Is the patient taking samples or paying 100% out of pocket for the medication being requested?□□□If no, please indicate:Requested medication covered under previous insurance planStarted medication in hospitalOther: ___________________________________________________________________3. Is the patient taking a medication that has a significant drug interaction potential with theHMG-CoA reductase inhibitors?If yes, please explain: ______________________________________________________4. Has the patient been previously diagnosed with myopathy or rhabdomyolysis (eithermedication-related or not medication related)?5. Does the patient have an underlying muscle/muscle-metabolism-related disorder (for example,myositis, McArdle disease)?If yes, please explain: _______________________________________________________ Yes Yes Yes Yes Yes No No No No No