Evidence Based Practice - 118er
Evidence Based Practice - 118er
Evidence Based Practice - 118er

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
GIMBE ®<br />
<strong>Evidence</strong> <strong>Based</strong> <strong>Practice</strong><br />
Gabriele Manzi<br />
Azienda U.S.L. di Bologna
GIMBE ®<br />
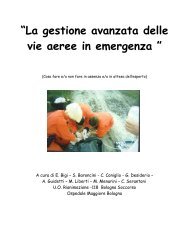
DOING<br />
THINGS<br />
CHEAPER<br />
The Evolution of Health Care<br />
DOING<br />
THINGS<br />
BETTER<br />
DOING<br />
THINGS<br />
RIGHT<br />
Efficiency Effectiveness<br />
DOING<br />
THE<br />
RIGHT<br />
THINGS<br />
DOING<br />
THE<br />
RIGHT<br />
THINGS<br />
RIGHT<br />
Quality<br />
Improvement<br />
1970s 1980s 1990s 21st Century
GIMBE ®<br />
<strong>Evidence</strong> <strong>Based</strong> Medicine<br />
L’EBM costituisce un approccio alla pratica clinica<br />
dove le decisioni cliniche risultano<br />
dall'integrazione tra l'esperienza del medico e<br />
l'utilizzo conscenzioso, esplitico e giudizioso delle<br />
migliori evidenze scientifiche disponibili, mediate<br />
dalle preferenze del paziente.<br />
David Sackett
GIMBE ®<br />
<strong>Evidence</strong> <strong>Based</strong> Medicine<br />
What it is and what it isn’t<br />
Research<br />
evidence<br />
Clinical<br />
expertise<br />
Patient<br />
preferences<br />
Sackett et al, BMJ 1996
GIMBE ®<br />
Patients’ preferences<br />
and actions<br />
Clinical state and<br />
circumstances<br />
<strong>Evidence</strong> <strong>Based</strong> Medicine<br />
What it is and what it isn’t<br />
Clinical<br />
expertise<br />
Research<br />
evidence<br />
Modificato da Haynes RB et al, BMJ 2002<br />
Health Care<br />
Resurces
GIMBE ®<br />
E.B. Pharmacy E.B. Midwifery<br />
EBM EBPH<br />
EBN<br />
<strong>Evidence</strong> <strong>Based</strong> <strong>Practice</strong><br />
<strong>Evidence</strong> <strong>Based</strong> Health Care<br />
Clinical Governance
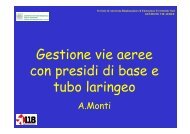
ANATOMIA DELL’INFORMAZIONE<br />
DELL INFORMAZIONE<br />
RICERCA<br />
PRIMARIA<br />
• Studi<br />
Osservazionali<br />
• Studi<br />
Sperimentali<br />
GIMBE ®<br />
BIOMEDICA<br />
RICERCA<br />
SECONDARIA<br />
• Revisioni<br />
Sistematiche<br />
• Linee Guida<br />
• Analisi<br />
economiche<br />
• Analisi decisionali<br />
Distorsione dei risultati<br />
FONTI<br />
TERZIARIE<br />
• Revisioni<br />
tradizionali<br />
• Trattati<br />
• Editoriali<br />
• Parere degli<br />
esperti
GIMBE ®<br />
I principi dell’evidence dell evidence<br />
based practice
GIMBE ®<br />
PREREQUISITI<br />
Componente essenziale: attitudine ad<br />
avvertire il bisogno di informazione<br />
Componente tecnica: abilità pratiche per<br />
effettuare le ricerche e valutare<br />
criticamente<br />
Giudizio clinico: pesare, valutare e<br />
integrare le evidenze nel processo<br />
decisionale.<br />
Cartabellotta A. Rec Prog Med 2002
GIMBE ®<br />
Come prendiamo le decisioni nella pratica<br />
professionale?<br />
• Scegliere tra due interventi assistenziali (quale<br />
medicazione posizionare),<br />
• Decidere la tipologia di paziente su cui<br />
intraprendere un intervento (su quali pazienti<br />
applico le strategie di prevenzione delle lesioni<br />
da decubito),<br />
• La tempistica delle prestazioni (ogni quanto<br />
realizzare la medicazione di un CVC)<br />
• Cosa e come comunicare con i pazienti e le loro<br />
famiglie (comunicare il rischio di caduta),<br />
• Come organizzare l’assistenza (modalità di<br />
consegna)<br />
• …
GIMBE ®<br />
Come prendiamo le decisioni nella pratica<br />
professionale?<br />
• Insegnamento scolastico<br />
• Tradizioni/abitudini di reparto<br />
• Esperienza<br />
• Autoreferenzialità<br />
• Prescrizioni di …<br />
• Libri, riviste, …<br />
• …
GIMBE ®<br />
Le conseguenze di ciò<br />
Difformità della pratica<br />
Erogazione di prestazioni non ottimali<br />
Scarsa crescita professionale<br />
Esposizione dei pazienti a rischi non<br />
necessari<br />
Determinazione di costi non giustificati<br />
…
GIMBE ®<br />
Un esempio:<br />
da “Le basi scientifiche dell’assistenza infermieristica” di Paola di Giulio<br />
Prostatecmia<br />
radicale<br />
Due giorni<br />
prima<br />
Giorno prima<br />
Giorno<br />
dell’intervento<br />
Clinica Urologica Divisione Urologia<br />
Dieta senza scorie<br />
* 3 per 2 cp Humatin<br />
* 2 buste Selg (e/o Isocolan)<br />
Dieta<br />
* Pranzo senza scorie Cena<br />
liquida; 3 per 2 cp Humatin<br />
Clisma con Neomicina 1%<br />
Tricotomia ampia (dai capezzoli<br />
fino a metà coscia)<br />
Doccia con betadine<br />
Digiuno dalla mezzanotte<br />
Digiuno totale<br />
Clisma ore 6.00 con neomicina 1%<br />
Doccia con Betadine<br />
Antibiotico profilassi<br />
Purgante<br />
Tricotomia xifopubica e scrotale<br />
Digiuno dalla mezzanotte<br />
Calze antiembolo<br />
Doccia con betadine<br />
-
GIMBE ®<br />
…una considerazione<br />
“Meno del 20 % di ciò che i medici fanno ogni<br />
giorno possiede almeno uno studio clinico ben<br />
disegnato a sostegno della sua utilità.”<br />
Cochrane A.L. ” Effectiveness and Efficiency. Random reflection on Health.<br />
Service” Nuffield Provincial hospital trust, London, 1972.<br />
E quello che fanno gli infermieri?
GIMBE ®<br />
Le origini dell’evidence dell evidence<br />
based practice
GIMBE ®<br />
Archibald L. Cochrane<br />
(1909-1988)
GIMBE ®<br />
<strong>Evidence</strong>-based Medicine: la storia 1972<br />
Archibald L. Cochrane, un epidemiologo inglese,<br />
sosteneva che i risultati della ricerca avevano un<br />
impatto molto limitato sulla pratica clinica.<br />
“E’ causa di grande preoccupazione constatare come<br />
la professione medica non abbia saputo organizzare<br />
un sistema in grado di rendere disponibili, e<br />
costantemente aggiornate, delle revisioni critiche<br />
sugli effetti dell'assistenza sanitaria".<br />
In altre parole Cochrane, suggeriva di rendere<br />
disponibili a tutti i pazienti solo gli interventi sanitari di<br />
documentata efficacia.
GIMBE ®<br />
<strong>Evidence</strong>-based Medicine: la storia 1986<br />
L'attenzione di Sackett e coll. si sposta<br />
progressivamente da “come leggere la<br />
letteratura biomedica” a “come utilizzare la<br />
letteratura biomedica per risolvere i problemi<br />
clinici”.<br />
David Sackett
GIMBE ®<br />
<strong>Evidence</strong> <strong>Based</strong> Nursing
GIMBE ®<br />
<strong>Evidence</strong> = Evidenza ?<br />
In Italiano<br />
– È evidenza qualsiasi cosa che sia palese e<br />
chiara, per la quale non è necessaria<br />
qualsiasi ulteriore dimostrazione.<br />
In Inglese<br />
– È evidenza qualsiasi cosa che ha provato la<br />
propria validità mediante il metodo scientifico.<br />
È evidenza ciò che è stato dimostrato.<br />
Evidenza = Prova di efficacia ?
GIMBE ®<br />
<strong>Evidence</strong>-<strong>Based</strong> Nursing (EBN)<br />
Processo per mezzo del quale le infermiere e<br />
gli infermieri assumono le decisioni cliniche<br />
utilizzando le migliori ricerche disponibili, la loro<br />
esperienza clinica e le preferenze del paziente,<br />
in un contesto di risorse disponibili.<br />
Di Censo A, Cullum N, Ciliska D.<br />
“Implementing evidence based nursing: some misconceptions”<br />
<strong>Evidence</strong> <strong>Based</strong> Nursing 1998; 1:38-40
GIMBE ®<br />
<strong>Evidence</strong>-<strong>Based</strong> Nursing (EBN)<br />
Opinion <strong>Based</strong> Nursing – O.B.N.<br />
<strong>Evidence</strong> <strong>Based</strong> Nursing – E.B.N.
GIMBE ®<br />
A<br />
t<br />
t<br />
i<br />
v<br />
i<br />
t<br />
à<br />
c<br />
l<br />
i<br />
n<br />
i<br />
c<br />
a<br />
Perché la ricerca<br />
• Individuare gli ambiti dove c’è variabilità<br />
• Dove c’è variabilità, c’è incertezza<br />
• Incertezza = area dove è necessario<br />
fare chiarezza<br />
• Per fare chiarezza bisogna attivare la<br />
ricerca<br />
• La ricerca è il motore che produce<br />
conoscenza quale riferimento per<br />
guidare la pratica professionale<br />
Paolo Chiari - Centro Studi EBN<br />
S.Orsola-Malpighi - Bologna
GIMBE ®<br />
Quando la ricerca e quando l’EBN<br />
Quando abbiamo un dubbio ricorrere<br />
all’EBN, prima di pensare alla conduzione di<br />
uno studio, è senz’altro una precauzione<br />
che può farci risparmiare molto tempo ed<br />
energie a patto che non siamo nell’area<br />
grigia.
GIMBE ®<br />
Il processo dell’EBN<br />
Avere chiaro rispetto ad un problema<br />
assistenziale cosa voglio cercare, perché, e<br />
quali risultati devo andare a misurare (aree<br />
di incertezza)<br />
Porre le proprie domande alle banche dati,<br />
ricercando quelle che sono le conoscenze<br />
scientifiche disponibili<br />
Valutare criticamente i risultati<br />
Applicazione delle conoscenze acquisite al<br />
problema originario
GIMBE ®<br />
EBN – Strumento & Processo<br />
Selezionare un aspetto del proprio lavoro da<br />
mettere in discussione (bisogno di informazione)<br />
Trasformare il bisogno di informazione in quesiti<br />
clinici ben definiti<br />
Ricercare con la massima efficienza, attraverso le<br />
fonti bibliografiche ed elettroniche le migliori<br />
evidenze disponibili<br />
Valutare criticamente le evidenze trovate, la loro<br />
validità ed applicabilità<br />
Diffondere ed integrare le evidenze trovate<br />
Miglioramento continuo della pratica professionale
GIMBE ®<br />
I limiti dell’<strong>Evidence</strong><br />
dell <strong>Evidence</strong><br />
<strong>Based</strong> <strong>Practice</strong>
GIMBE ®<br />
I limiti della EBM<br />
Esistenza di “zone grigie”:<br />
Zone in cui vi è incertezza sull’efficacia.<br />
EBM si basa sulle migliori evidenze<br />
“disponibili”, non sulle migliori evidenze<br />
“possibili”.
Le “aree grigie”: lo spazio dell’opinion based<br />
Interventi<br />
efficaci Area grigia<br />
Copyright © 1996-2007 - GIMBE ®<br />
GIMBE ®<br />
RICERCA<br />
PRATICA CLINICA<br />
EBP<br />
Interventi<br />
inefficaci
GIMBE ®<br />
I limiti dell’EBP nella realtà italiana<br />
Necessità di acquisire nuove competenze<br />
Mancanza di tempo<br />
Scarsa attitudine a mettere in discussione le proprie<br />
conoscenze e a generare quesiti clinicoassistenziali.<br />
Barriere linguistiche<br />
Limitata diffusione/accesso agli strumenti informatici<br />
(computer, internet)<br />
Scarsa familiarità informatica<br />
Resistenza al cambiamento<br />
Scarsa disponibilità di riviste
GIMBE ®<br />
Le caratteristiche della<br />
letteratura biomedica
Copyright © 1996-2007 - GIMBE ®<br />
GIMBE ®<br />
The Ascent of <strong>Evidence</strong><br />
(and the exhaustion of man)<br />
Clarke M.J. BMJ 1998
GIMBE ®<br />
Le caratteristiche dell’informazione<br />
biomedica<br />
Crescita esponenziale:<br />
circa 2.000.000 di articoli pubblicati ogni<br />
anno in oltre 20.000 riviste<br />
sino a 400.000 citazioni aggiunte<br />
annualmente au MEDLINE
GIMBE ®<br />
Le caratteristiche dell’informazione<br />
biomedica<br />
Obsolescenza:<br />
Progresso scientifico e tecnologico.<br />
Ritardo nella disseminazione ed utilizzazione delle<br />
conoscenze.<br />
Frammentazione:<br />
Articoli che trattano lo stesso argomento sono<br />
pubblicati in riviste ed annate diverse.<br />
Basso rapporto segnale/rumore:<br />
La maggior parte della produzione scientifica è<br />
irrilevante per la pratica clinica.
GIMBE ®<br />
WARNING !!!<br />
Trials are conducted and published without a systematic<br />
review of existing evidence, meaning that trials are<br />
conducted unnecessarily or don't address the most<br />
important questions<br />
Results are selectively published with positive results<br />
emphasised or published more than once, and negative<br />
results are ignored<br />
Trials favourable to sponsors are published in major<br />
journals, and unfavourable trials are not published at all<br />
or are published in minor journals<br />
Smith R, Roberts I. Patient Safety Requires a New Way to Publish Clinical Trials. PLoS Clinical Trials (2006)1(1)
GIMBE ®<br />
WARNING !!!<br />
Una ricerca effettuata su 3.600 ricercatori e 4.000<br />
borsisti ha dimostrato che:<br />
0,3% ha inventato o falsificato dati<br />
6% non ha pubblicato dati che erano in contrasto con le<br />
sue ricerche precedenti<br />
15,5% ha cambiato il disegno della ricerca per<br />
accontentare lo sponsor<br />
4,7% ha pubblicato più volte gli stessi risultati<br />
15,3% non ha utilizzato tutti i risultati ottenuti<br />
Nature 2005; 435: 718-9
GIMBE ®<br />
Fasi del processo:<br />
EBN<br />
Conversione del bisogno di informazione in<br />
quesiti clinici ben definiti.<br />
Ricerca con la massima efficienza delle migliori<br />
evidenze disponibili.<br />
Valutazione della loro validità ed applicabilità<br />
clinica.<br />
Integrazione delle evidenze nella pratica clinica.<br />
Rivalutazione continua della propria performance<br />
professionale.
GIMBE ®<br />
Approcci di ricerca<br />
Cercare attivamente nelle banche dati<br />
rispetto ad un quesito formulato<br />
(SEARCHING).<br />
Consultare periodicamente alcune<br />
riviste per individuare novità sui temi di<br />
abituale interesse (SCANNING).
sorveglianza<br />
GIMBE ®<br />
Gestione dell’informazione<br />
SCANNING<br />
SEARCHING<br />
cerco ciò che<br />
mi serve
GIMBE ®<br />
SCANNING<br />
Seleziono alcune riviste e le leggo in modo<br />
regolare<br />
•che cosa trovo?<br />
– abstract<br />
– full text<br />
•problemi<br />
– time consuming<br />
– aspecificità
GIMBE ®<br />
SEARCHING<br />
• Risorse primarie<br />
– B.D. generali: Medline, Embase, …<br />
– B.D. specialistiche: Cinhal, Pedro,<br />
Joanna Briggs, …<br />
• Risorse secondarie:informazioni predigerite<br />
– B.D. revisione sistematiche: Cochrane<br />
library, Joanna Briggs, …<br />
– B.D. linee guida: New Zeland guideline<br />
group, Sign, National Guideline<br />
Clearinghouse, …
GIMBE ®<br />
IL QUESITO<br />
ovvero<br />
Come definire un quesito clinico che ci permetta di<br />
ricercare la risposta nella letteratura
GIMBE ®<br />
Focalizzando la domanda si:<br />
chiarisce l’obiettivo della ricerca<br />
facilita l’utilizzo di regole<br />
appropriate nella scelta dei titoli e<br />
dei riassunti degli articoli che sono<br />
stati individuati
GIMBE ®<br />
FORMULARE DOMANDE PERTINENTI<br />
ALLE QUALI SIA POSSIBILE<br />
RISPONDERE
GIMBE ®<br />
I quesiti clinico-assistenziali<br />
appartengono a due categorie principali<br />
Background<br />
Modificato da: Guyatt GH, et al. AMA Press, 2001<br />
Conoscenza, esperienza<br />
Foreground
GIMBE ®<br />
Perché Perch ci interessa questa distinzione?<br />
Per orientare diversamente la ricerca<br />
Background questions<br />
Sono i quesiti di base che vengono formulati nelle situazioni in cui<br />
l'argomento è poco, o per nulla, conosciuto.<br />
E' un "bisogno di informazione" caratteristico del giovane professionista.<br />
Il professionista esperto, peraltro, formula quesiti di base quando la<br />
malattia/condizione/tecnologia è:<br />
– estranea al proprio settore professionale/specialistico<br />
– di recente introduzione (tecnologia) o descrizione (malattia)<br />
–rara<br />
Verso linee guida
GIMBE ®<br />
Perché Perch ci interessa questa distinzione?<br />
Per orientare diversamente la ricerca<br />
Foreground questions<br />
Sono quesiti specifici, generalmente formulati dal<br />
professionista esperto.<br />
Verso la letteratura secondaria: Revisioni sistematiche<br />
Verso la letteratura primaria: Medline, Cinahl, Embase
Quando nasce un quesito di<br />
foreground?<br />
Categoria Quesito ed esempio<br />
Eziologia/Rischio<br />
Diagnosi<br />
Prognosi<br />
Trattamento<br />
Copyright © 1996-2007 - GIMBE ®<br />
GIMBE ®<br />
Qual'è la responsabilità eziologica del fattore di rischio X nell'insorgenza della malattia Y?<br />
L'utilizzo del telefono cellulare aumenta il rischio di neoplasia cerebrale?<br />
Qual'è l’accuratezza del test diagnostico X (rispetto al gold-standard Y) nella diagnosi<br />
della malattia Z?<br />
Qual'è l'accuratezza diagnostica della risonanza magnetica nucleare nei pazienti con<br />
sospetta lesione del menisco?<br />
Qual'è la storia naturale della malattia X e la potenza dei fattori prognostici?<br />
In un paziente con neurite ottica, quali sotto i fattori prognostici (favorevoli e sfavorevoli)<br />
che condizionano l'evoluzione in sclerosi multipla?<br />
Qual'è l'efficacia del trattamento X (preventivo, terapeutico o riabilitativo), rispetto al<br />
trattamento Y, nella malattia Z?<br />
In un paziente con osteoartrosi in trattamento cronico con FANS (malattia/condizione),<br />
l'omeprazolo (intervento), rispetto al misoprostolo (confronto) è in grado di prevenire<br />
l'ulcera da FANS sintomatica e le sue complicanze (evento)?
GIMBE ®<br />
Quesito di foreground<br />
formulare il quesito in modo preciso ed<br />
articolato (es PICOM)<br />
P patient<br />
I intervention<br />
C comparison<br />
O outcome<br />
M metodology
GIMBE ®<br />
Esempio di ricerca<br />
Punto di partenza: quesito in forma<br />
“narrativa”:<br />
“Il saccarosio può essere impiegato come<br />
analgesico per i neonati che devono essere<br />
sottoposti a procedure dolorose<br />
(es.: puntura del calcagno …)?”
GIMBE ®<br />
Trasformazione con PICOM<br />
Patient: neonati da sottoporre a procedure<br />
dolorose.<br />
Intervention: analgesia con saccarosio.<br />
Comparison: altri trattamenti non farmacologici<br />
(“pacifiers”, ecc.).<br />
Outcome: ridotta percezione del dolore da parte<br />
del neonato.<br />
Metodology: Randomized Controlled Trial
GIMBE ®<br />
PER OGNI DOMANDA UN DISEGNO<br />
EZIOLOGIA<br />
PROGNOSI<br />
DIAGNOSI<br />
TRATTAMENTO<br />
QUESITO DISEGNO DELLO STUDIO<br />
• COORTE<br />
• CASO CONTROLLO<br />
• REVISIONI SISTEMATICHE<br />
• STUDI LONGITUDINALI DI COORTE<br />
(SENZA COORTE CONCORRENTE)<br />
• STUDI TRASVERSALI DI CONFRONTO<br />
INDIPENDENTE E CIECO CON IL GOLD<br />
STANDARD DIAGNOSTICO<br />
• REVISIONI SISTEMATICHE<br />
• RCT<br />
• REVISIONI SISTEMATICHE
GIMBE ®<br />
Paziente<br />
o<br />
problema<br />
Quesito di foreground<br />
Chiedersi:<br />
“come descriverei un gruppo di pazienti<br />
simili al mio?”<br />
Bilanciare la precisione con la brevità
GIMBE ®<br />
Intervento<br />
o<br />
esposizione<br />
(una causa, un<br />
fattore prognostico,<br />
un trattamento)<br />
Quesito di foreground<br />
Chiedersi<br />
“Quale intervento principale/fattore di<br />
rischio sto prendendo in<br />
considerazione?”<br />
Essere specifici
GIMBE ®<br />
Intervento di<br />
controllo<br />
(se necessario<br />
e/o possibile)<br />
Quesito di foreground<br />
Chiedersi<br />
“Qual’è la principale alternativa da<br />
comparare all’intervento prescelto?”<br />
Essere specifici
GIMBE ®<br />
Outcome<br />
Quesito di foreground<br />
Chiedersi<br />
“Che cosa spero di ottenere?”<br />
o<br />
“Che cosa questo intervento può<br />
realmente produrre?”<br />
Essere specifici
GIMBE ®<br />
Metodology<br />
Quesito di foreground<br />
Chiedersi<br />
“Quale disegno di studio costituisce<br />
il gold standard per il mio quesito?”
GIMBE ®<br />
Perché è importante chiarire bene il<br />
quesito?<br />
Per due motivi fondamentali:<br />
– dal quesito vengono estratte le parole chiave<br />
che useremo nella ricerca.<br />
– dalla chiara espressione del quesito possiamo<br />
definire i criteri di inclusione o di esclusione,<br />
tra i quali capire quale tipo di studio dobbiamo<br />
cercare.
GIMBE ®<br />
Esercitazione del quesito: diagnosi<br />
Lavori come infermiere all’interno di un ambulatorio<br />
di assistenza di base. Usi abitualmente diversi<br />
strumenti validati per la diagnosi di depressione.<br />
Una collega ti parla di uno strumento analogo, ma<br />
composto da due sole domande, che secondo lei è<br />
efficace per la individuazione della depressione<br />
maggiore ed il cui uso, essendo così semplice,<br />
permetterebbe di risparmiare molto tempo. Decidi<br />
quindi di compiere una ricerca su diversi strumenti<br />
per la diagnosi di depressione e sulle loro proprietà.
GIMBE ®<br />
Esercitazione del quesito<br />
Popolazione Intervento Comparazione Outcome<br />
In pazienti<br />
con sospetta<br />
depressione<br />
L’uso di<br />
uno<br />
strumento<br />
a due<br />
domande<br />
Rispetto ad<br />
altri strumenti<br />
validati<br />
Che livello<br />
di<br />
accuratezza<br />
permette?
GIMBE ®<br />
Esercitazione del quesito: prognosi<br />
Stai assistendo una paziente di 28 anni che è appena<br />
stata sottoposta a dilatazione e curettage dopo aborto<br />
spontaneo. Era di 10 settimane ed era alla sua prima<br />
gravidanza. In un incontro di team, uno dei tuoi<br />
colleghi ricorda vagamente di aver letto un articolo<br />
inerente la depressione dopo l’aborto. Decidi di<br />
compiere una ricerca per verificare se nella tua<br />
paziente sono riscontrabili i fattori prognostici di severa<br />
e prolungata depressione.
GIMBE ®<br />
Esercitazione del quesito: prognosi<br />
Popolazione Intervento Comparazione<br />
In una<br />
paziente sana<br />
che ha<br />
recentemente<br />
subito un<br />
aborto<br />
L’individuazione<br />
di<br />
quali fattori<br />
prognostici<br />
Outcome<br />
Consente<br />
di<br />
individuare<br />
uno stato<br />
depressivo<br />
non<br />
fisiologico
GIMBE ®<br />
Esercitazione del quesito: terapia<br />
Lavori come infermiere scolastico e visiti<br />
quotidianamente molti bambini delle scuole elementari<br />
e medie (di età compresa tra i 5 ed i 13 anni). È<br />
inverno, per cui sono molto diffusi influenza e<br />
raffreddore. Una delle insegnanti ti ferma nell’atrio<br />
della scuola e ti chiede un consiglio per la sua<br />
bambina di 10 anni che è raffreddata. L’insegnante ha<br />
sentito dire che lo zinco in compresse può aiutare ad<br />
alleviare i sintomi del raffreddore: ti chiede se è<br />
realmente efficace e se è opportuno darlo ai bambini.
GIMBE ®<br />
Esercitazione del quesito: terapia<br />
Popolazione Intervento Comparazione<br />
Nei bambini L’assunzio-<br />
con<br />
raffreddore<br />
ne di<br />
compresse<br />
di zinco<br />
?<br />
Outcome<br />
Sono<br />
efficaci e<br />
sicure per<br />
alleviare i<br />
sintomi del<br />
raffreddore?
GIMBE ®<br />
Esercitazione del quesito: eziologia<br />
Sei un infermiere territoriale. Una tua paziente è<br />
una donna di 29 anni che ha assunto contraccettivi<br />
orali negli ultimi 6 anni. Ti telefona per chiederti un<br />
consiglio: è molto in ansia dopo avere letto che<br />
l’assunzione degli estroprogestinici aumenta il<br />
rischio di malattie cardiovascolari. Lei non ha mai<br />
fumato, è in buona salute e non ci sono casi di<br />
malattie cardiache nella sua famiglia. Chiede di<br />
vederti per discutere se è il caso di sospendere<br />
l’assunzione della pillola e passare all’uso di un altro<br />
metodo anticoncezionale. Nel prepararti all’incontro<br />
decidi di eseguire una ricerca.
GIMBE ®<br />
Esercitazione del quesito: eziologia<br />
Popolazione Intervento Comparazione<br />
Nelle donne<br />
in età fertile<br />
L’assunzione<br />
di<br />
contraccettivi<br />
orali a base<br />
di<br />
estroprogesti<br />
nici<br />
Rispetto ad<br />
altri metodi<br />
contraccett<br />
ivi non<br />
estroproge<br />
stinici<br />
Outcome<br />
Aumenta il<br />
rischio di<br />
insorgenza di<br />
malattie<br />
cardiovascolari?
GIMBE ®<br />
THE END<br />
GIMBE ®
GIMBE ®<br />
<strong>Evidence</strong> <strong>Based</strong> <strong>Practice</strong><br />
Gabriele Manzi<br />
Azienda U.S.L. di Bologna
GIMBE ®<br />
Architettura della<br />
ricerca clinica<br />
Studi Epidemiologici
ANATOMIA DELL’INFORMAZIONE<br />
DELL INFORMAZIONE<br />
RICERCA<br />
PRIMARIA<br />
• Studi<br />
Osservazionali<br />
• Studi<br />
Sperimentali<br />
GIMBE ®<br />
BIOMEDICA<br />
RICERCA<br />
SECONDARIA<br />
• Revisioni<br />
Sistematiche<br />
• Linee Guida<br />
• Analisi<br />
economiche<br />
• Analisi decisionali<br />
Distorsione dei risultati<br />
FONTI<br />
TERZIARIE<br />
• Revisioni<br />
tradizionali<br />
• Trattati<br />
• Editoriali<br />
• Parere degli<br />
esperti
The 6S hierarchy of<br />
pre-appraised pre appraised evidence<br />
Computerized decision support systems<br />
<strong>Evidence</strong> based clinical practice guideline / textbooks<br />
<strong>Evidence</strong> based abstraction jourmal<br />
Systematic reviews<br />
<strong>Evidence</strong> based abstraction jourmal<br />
Original jourmal articles<br />
DiCenso A, Bayley L, Haynes RB. Evid. <strong>Based</strong> Nurs. 2009;12;99-101
GIMBE ®<br />
<strong>Evidence</strong><br />
Non<br />
evidence<br />
Ricerca sanitaria<br />
Randomized<br />
Controlled<br />
Studies<br />
Cohort Studies<br />
Case Control Studies<br />
Case Series<br />
Case Reports<br />
Ideas, Editorials, Opinions<br />
Animal research<br />
In vitro (‘test ( test tube’) tube ) research<br />
Systematic Review<br />
Mega Trial
GIMBE ®<br />
Architettura della ricerca clinica<br />
• Studi osservazionali<br />
–descrittivi<br />
• case report<br />
• case series
GIMBE ®<br />
Architettura della ricerca clinica<br />
• Studi osservazionali<br />
– Analitici<br />
• Studi caso controllo<br />
• Studi di coorte<br />
–Con coorte parallela<br />
»Prospettici<br />
–Senza coorte parallela<br />
»Prospettici retrospettivi<br />
• Studi trasversali/cross sectional
GIMBE ®<br />
EZIOLOGIA<br />
PROGNOSI<br />
DIAGNOSI<br />
TRATTAMENTO<br />
Quali sono?<br />
QUESITO DISEGNO DELLO STUDIO<br />
COORTE<br />
CASO CONTROLLO<br />
REVISIONI SISTEMATICHE<br />
STUDI LONGITUDINALI DI COORTE<br />
(SENZA COORTE CONCORRENTE)<br />
STUDI TRASVERSALI DI CONFRONTO<br />
INDIPENDENTE E CIECO CON IL GOLD<br />
STANDARD DIAGNOSTICO<br />
REVISIONI SISTEMATICHE<br />
RCT<br />
REVISIONI SISTEMATICHE<br />
Per ogni domanda un disegno
GIMBE ®<br />
Studi che verificano l’eziologia<br />
• Es: vogliamo verificare se avere un indice<br />
di massa corporea basso (BMI)<br />
(esposizione) è un fattore di rischio per le<br />
lesioni da decubito (esito).
GIMBE ®<br />
Come posso rispondere a questa<br />
domanda?<br />
Attraverso tre disegni di studio:<br />
studi trasvesrale/cross sectional<br />
studi caso controllo<br />
studi di coorte
Studio che raccoglie informazioni relative<br />
all’esposizione ai fattori di rischio ed ai loro esiti<br />
(positivi o negativi) NELLO STESSO<br />
MOMENTO e sullo stesso paziente.<br />
GIMBE ®<br />
Studio Cross Sectional
GIMBE ®<br />
Studio Cross Sectional<br />
Sono studi che rilevando i dati in un<br />
preciso momento realizzano la fotografia<br />
del fenomeno.<br />
Attraverso questi studi si rileva la<br />
PREVALENZA di una patologia, ossia<br />
l’insieme di tutti i casi esistenti in un<br />
determinato momento, in una determinata<br />
popolazione.
Sono studi retrospettivi che partendo dalla<br />
presenza, o meno, dell’esito (endpoint)<br />
raccolgono informazioni relative<br />
all’esposizione ai fattori di rischio.<br />
GIMBE ®<br />
Fattori di<br />
rischio<br />
Studio Caso-Controllo<br />
Oggi<br />
End point sì<br />
End point no
Sono studi prospettici che partendo<br />
dall’esposizione ai fattori di rischio o meno,<br />
verificano se insorge l’esito.<br />
GIMBE ®<br />
Oggi<br />
Fattori di<br />
rischio sì<br />
Fattori di<br />
rischio no<br />
Studio di Coorte<br />
End point
esposti<br />
non esposti<br />
esposti<br />
non esposti<br />
Studi osservazionali analitici<br />
CASI<br />
CONTROLLI<br />
CASO-CONTROLLO<br />
Soggetti<br />
dello studio<br />
direzione dell’osservazione<br />
ESPOSTI<br />
NON ESPOSTI<br />
outcome +<br />
outcome -<br />
outcome +<br />
outcome -<br />
COORTE PROSPETTICA
GIMBE ®<br />
Cosa ci serve sapere per<br />
leggere gli studi<br />
osservazionali?<br />
Dove può essere<br />
l’errore/imbroglio?
GIMBE ®<br />
Individuare i bias<br />
In uno studio il termine bias si riferisce a<br />
qualsiasi errore sistematico che porti ad<br />
una stima errata dell’associazione tra<br />
l’esposizione e l’esito.<br />
In uno studio osservazionale i puù<br />
frequenti bias che possiamo incontrare<br />
sono:<br />
– Information bias<br />
– Recall bias (studi caso controllo)<br />
– Selection bias<br />
– Fattori di confondimento
Information bias/misclassification – si realizza<br />
tutte le volte in cui il paziente è posto nel<br />
gruppo sbagliato a causa della errata<br />
rilevazione del parametro considerato (es.<br />
misurazione errata di peso ed altezza e<br />
collocazione erronea nel gruppo sbagliato).<br />
GIMBE ®<br />
Information bias
GIMBE ®<br />
Information bias<br />
Esso si riduce in due modi:<br />
– Utilizzando misure di rilevazione oggettive.<br />
– Facendo in modo che chi effettua la<br />
rilevazione dell’esposizione non sia a<br />
conoscenza dell’esito (studio caso controllo) e<br />
che chi rileva l’esito non sia a conoscenza<br />
della condizione di esposizione all’agente<br />
indagato (studio di coorte).
GIMBE ®<br />
Recall bias<br />
E’ proprio degli studi caso controllo e si<br />
verifica a causa dell’errato ricordo dei<br />
soggetti coinvolti nello studio.
GIMBE ®<br />
Esempio :<br />
confronto tra<br />
quanto riferito dai<br />
pazienti e quanto<br />
rilevato dalla<br />
documentazione<br />
clinica.<br />
Coloro che non hanno<br />
sviluppato ldp hanno un<br />
ricordo meno accurato e<br />
più positivo rispetto la<br />
durata della propria<br />
degenza (in realtà 13<br />
anziché 10 hanno avuto<br />
degenze >10 gg).
Questo tipo di bias<br />
modifica in modo<br />
consistente i risultati<br />
della associazione,<br />
spostandola<br />
dall’ipotesi nulla!<br />
GIMBE ®<br />
Esempio:<br />
confronto tra<br />
quanto riferito dai<br />
pazienti e quanto<br />
rilevato dalla<br />
documentazione<br />
clinica.
GIMBE ®<br />
Selection bias<br />
I soggetti selezionati devono essere identici ad<br />
eccezione dell’esposizione all’agente eziologico.<br />
Quando questo non si realizza siamo in presenza<br />
del SELECTION BIAS.<br />
In uno studio caso controllo, in cui si parte da due<br />
gruppi con e senza l’esito, cosa accadrebbe se si<br />
fossero scelte solo persone non esposte al reale<br />
agente eziologico?<br />
In uno studio di coorte, l’allocazione alla condizione<br />
di esposizione si riferisce allo sviluppo dell’esito (o<br />
nei due gruppi ci sono altre differenze non<br />
considerate)?
GIMBE ®<br />
Follow up<br />
Negli studi di coorte i soggetti inclusi nei<br />
gruppi devono essere seguiti per un<br />
periodo di tempo sufficientemente lungo.<br />
Cosa accadrebbe se il follow up fosse<br />
troppo breve, o in esso fossero persi molti<br />
soggetti?<br />
Una perdita nel follow up superiore al 20%<br />
compromette i risultati dello studio.
GIMBE ®<br />
Se nel compimento di uno studio è stato<br />
effettuato un bias i suoi risultati possono<br />
essere definitivamente compromessi.<br />
Gli studi di coorte da questo punto di vista<br />
sono più sicuri per qul che riguarda<br />
l’information bias o il recall bias, ma non<br />
sempre sono realizzabili (condizioni rare o<br />
a lentissimo decorso).
GIMBE ®<br />
Errors in epidemiological studies<br />
Error<br />
Random error (chance)<br />
Study size<br />
Systematic error (bias)<br />
Rothman, 2002
GIMBE ®<br />
Fattori di confondimento<br />
Esiste una relazione tra l’assunzione di<br />
caffè e l’insorgenza del tumore del<br />
polmone?
GIMBE ®<br />
Fattori di confondimento<br />
I fattori di confondimento sono le variabili<br />
associate sia all’esposizione, sia all’esito,<br />
che potrebbero spiegare qualsiasi<br />
relazione osservata tra questi due fattori.<br />
Esposizione Esito<br />
Fattore di<br />
confondimento
GIMBE ®<br />
Fattori di confondimento<br />
Al contrario dei bias, i fattori di<br />
confondimento possono essere corretti<br />
cercando di escludere dal campione<br />
coloro che possono recarli con sé.<br />
Purtroppo però i fattori di confondimento<br />
sono numerosi, per cui è difficile escluderli<br />
completamente dagli studi (e non è detto<br />
che possano essere identificati).
GIMBE ®<br />
Fattori di confondimento<br />
Per ridurre l’effetto delle variabili di<br />
confondimento esistono diverse tecniche<br />
in fase di campionamento o in fase di<br />
analisi.
GIMBE ®<br />
Accorgimenti in fase di<br />
campionamento<br />
Esclusione dei soggetti che presentano variabili<br />
di confondimento.<br />
Matching negli studi caso controllo, che consiste<br />
nell’introdurre nel gruppo di controllo persone<br />
con le stesse variabili di confondimento presenti<br />
nel gruppo dei casi.<br />
Stratificazione, che consiste nell’esaminare<br />
l’associazione in modo separato nei diversi<br />
gruppi.
GIMBE ®<br />
GIMBE ® GIMBE<br />
Accorgimenti in fase di analisi<br />
Regressione.<br />
Si tratta di un’elaborazione statistica che<br />
ricalcola le associazioni tenendo conto<br />
dell’effetto delle variabili di<br />
confondimento.<br />
Centro Studi EBN - Bologna
GIMBE ®<br />
Esempio<br />
Esiste una relazione tra il sesso maschile<br />
e l’insorgenza delle lesioni da decubito?<br />
Lo studio di Margolis e al, rispetto al<br />
genere maschile e le lesioni da decubito,<br />
presenta un rischio relativo non adattato<br />
pari a 0,78, (CI 95% 0,70-0,88), quindi per<br />
gli uomini esisterebbe il 22% in meno di<br />
rischio di sviluppare lesioni da decubito.
GIMBE ®<br />
Esempio<br />
Tuttavia, considerando i fattori potenziali<br />
di confondimento, quali l’età e le<br />
patologie concomitanti, il rischio relativo<br />
diventa 1,01 (CI 95% 0,89-1,15).<br />
Quindi, cosa si può concludere?
GIMBE ®<br />
Misure di associazione<br />
• Negli studi sulle cause, vogliamo<br />
conoscere la relazione tra alcuni fattori di<br />
rischio dei pazienti (le esposizioni) e una<br />
particolare condizione o patologia (l’esito).<br />
• La relazione tra i fattori di rischio e gli esiti<br />
viene generalmente presentata come<br />
rischio relativo, negli studi di coorte, o<br />
come odds ratio negli studi caso controllo.
GIMBE ®<br />
Tabellare i dati<br />
Evento Sì Evento No<br />
Gruppo E a + b<br />
a b<br />
Gruppo C c + d<br />
L’odds ratio (OR)<br />
a/b<br />
OR = ----------c/d<br />
c d<br />
a + c b + d<br />
Rischio Relativo (RR)<br />
a<br />
EER ---------a<br />
+ b<br />
RR = ------------ = ------------c<br />
CER ---------c<br />
+ d
Esempio ipotetico<br />
Rischio Relativo (RR) a<br />
EER ----------- 0,073<br />
a + b<br />
RR = ------------ = --------------- = ----------- = 1,37<br />
c<br />
CER ---------- 0,053<br />
c + d<br />
GIMBE ®<br />
Un risk ratio di 1,37<br />
indica che le persone<br />
con un BMI basso<br />
hanno un rischio di<br />
1,37 volte maggiore (o<br />
del 37%) di<br />
presentare l’esito,<br />
rispetto a quelli con<br />
elevato BMI.
Odds Ratio (OR)<br />
Esempio ipotetico<br />
a/b 0,078<br />
OR = ------------ = ----------------- = 1,39<br />
c/d 0,056<br />
GIMBE ®<br />
Un odds ratio di 1,39<br />
indica che le persone<br />
con un BMI basso<br />
hanno una probabilità<br />
di 1,39 volte maggiore<br />
(o del 39%) di<br />
presentare l’esito,<br />
rispetto a quelli con<br />
elevato BMI.
GIMBE ®<br />
Misure di associazione<br />
• Il RR si utilizza negli studi di coorte.<br />
• L’OR si utilizza negli studi caso controllo.<br />
• Non è tanto importante capire quando<br />
bisogna usare l’uno o l’altro, ma sapere<br />
che cosa indicano.
GIMBE ®<br />
Interpretazione<br />
• RR/OR1 – l’esposizione favorisce<br />
l’insorgenza del danno<br />
• RR/OR=1 – l’esposizione non produce<br />
effetti
GIMBE ®<br />
Intervallo di confidenza (IC)
Si verifica quando i parametri di associazione<br />
(RR o OR) assumono valore uguale a 1 o<br />
quando l’intervallo di confidenza comprende<br />
il valore 1.<br />
GIMBE ®<br />
Ipotesi nulla
GIMBE ®<br />
I risultati sono validi?<br />
Per valutare la validità di uno studio<br />
sull’eziologia (danno) di una particolare<br />
condizione, abbiamo bisogno di valutare<br />
quanto abbiano influito, sui risultati dello<br />
studio, 3 fattori:<br />
il caso<br />
i bias<br />
i fattori di<br />
confondimento
GIMBE ®<br />
Test di significatività statistica<br />
… lo zampino del caso<br />
Oltre a verificare i valori delle misure di<br />
associazione, e del loro IC, occorre<br />
osservare il valore assunto da “p”, che<br />
ci dice quale sia la significatività<br />
statistica dei risultati ottenuti.
GIMBE ®<br />
Significatività statistica
GIMBE ®<br />
Per ogni quesito un disegno di<br />
EZIOLOGIA<br />
PROGNOSI<br />
DIAGNOSI<br />
TERAPIA<br />
studio ideale<br />
QUESITO DISEGNO DELLO STUDIO<br />
COORTE<br />
CASO CONTROLLO<br />
REVISIONI SISTEMATICHE<br />
STUDI LONGITUDINALI DI COORTE<br />
(SENZA COORTE CONCORRENTE)<br />
STUDI TRASVERSALI DI CONFRONTO<br />
INDIPENDENTE E CIECO CON IL GOLD<br />
STANDARD DIAGNOSTICO<br />
REVISIONI SISTEMATICHE<br />
RCT<br />
REVISIONI SISTEMATICHE
GIMBE ®<br />
<strong>Evidence</strong><br />
Non<br />
evidence<br />
Ricerca sanitaria<br />
Randomized<br />
Controlled<br />
Studies<br />
Cohort Studies<br />
Case Control Studies<br />
Case Series<br />
Case Reports<br />
Ideas, Editorials, Opinions<br />
Animal research<br />
In vitro (‘test ( test tube’) tube ) research<br />
Systematic Review<br />
Mega Trial
GIMBE ®<br />
Architettura della ricerca clinica<br />
• Studi sperimentali<br />
– Non controllati<br />
– Controllati<br />
• Non randomizzati<br />
• Randomizzati
GIMBE ®<br />
Popolazione e campione<br />
Il campione viene definito individuando<br />
criteri di inclusione e di esclusione. Essi<br />
sono utilizzati per selezionare il campione<br />
dall’insieme di tutte le unità.
GIMBE ®<br />
Campione<br />
Il campione deve essere corrispondente<br />
alle caratteristiche definite dal ricercatore<br />
e deve essere rappresentativo in termini<br />
quali-quantitativi della popolazione.<br />
Solo in questo modo sarà possibile trarre<br />
inferenze (generalizzazioni) sulle<br />
popolazione dallo studio effettuato su una<br />
piccola parte di essa.
GIMBE ®<br />
Campione<br />
Un campione statisticamente<br />
rappresentativo deve essere<br />
sufficientemente numeroso, omogeneo e<br />
scelto a caso.
GIMBE ®<br />
Campionamento casuale<br />
Per ottenere delle informazioni attendibili su una<br />
popolazione utilizzando un campione, è<br />
necessario che il campione sia ottenuto in modo<br />
casuale.<br />
Perché un campione possa essere considerato<br />
casuale, è indispensabile che ogni membro della<br />
popolazione in oggetto abbia la stessa<br />
probabilità di essere selezionato.<br />
Un campione non casuale non dà alcun<br />
affidamento: in altre parole tutte le inferenze da<br />
esso tratte non sono da prendersi sul serio.
GIMBE ®<br />
Campionamento casuale<br />
Al fine di realizzare un campionamento<br />
casuale occorre ricorrere alla<br />
randomizzazione.<br />
Essa può essere realizzata in diversi modi:<br />
– Randomizzazione semplice<br />
– Randomizzazione stratificata<br />
– Randomizzazione a grappolo<br />
– Randomizzazione sistematica
GIMBE ®<br />
Architettura della ricerca clinica<br />
• Studi sperimentali<br />
– Non controllati<br />
– Controllati<br />
• Non randomizzati<br />
• Randomizzati
GIMBE ®<br />
Trial Randomizzati Controllati<br />
Campione<br />
di<br />
popolazione<br />
Randomizzazione<br />
Esposizione<br />
Gruppo<br />
sperimentale<br />
Gruppo<br />
controllo<br />
Direzione della raccolta dati<br />
Esposizione<br />
Outcome<br />
Outcome<br />
No outcome<br />
Outcome<br />
No outcome
GIMBE ®<br />
Anatomia<br />
dell’RCT<br />
Gruppo Sperimentale<br />
Gruppo di Controllo<br />
Outcome<br />
No<br />
Outcome<br />
Outcome<br />
No<br />
Outcome
GIMBE ®<br />
La cecità per vedere bene<br />
Singolo cieco: solo il soggetto sotto sperimentazione non<br />
sa quale trattamento sta ricevendo<br />
Doppio cieco: sia il soggetto sotto sperimentazione che<br />
gli sperimentatori non sanno quale trattamento si<br />
assume/somministra<br />
Doppio simulato: metodica utilizzata per mantenere la<br />
cecità quando si confrontano farmaci somministrati per<br />
vie diverse tra di loro<br />
In aperto: sperimentazione senza cecità. Accettabile<br />
quando si confrontano terapie diverse e/o complesse
GIMBE ®<br />
La cecità per vedere bene<br />
Non conoscere il trattamento che si riceve (paziente)<br />
o che si somministra (sperimentatore) impedisce di<br />
essere influenzati dalle aspettative che si hanno<br />
rispetto al trattamento<br />
Altrettanto importante è essere ciechi nella<br />
valutazione dei risultati della sperimentazione,<br />
soprattutto se gli end-points sono sfumati o di difficle<br />
interpretazione (triplo cieco)
Trial Randomizzati Controllati<br />
I RCTs rappresentano lo standard sperimentale per valutare<br />
l'efficacia dei trattamenti, grazie alla loro capacità di<br />
minimizzare i bias rispetto ad altri disegni sperimentali<br />
L'elemento che contraddistingue i RCTs è l'assegnazione<br />
casuale dei pazienti al trattamento da sperimentare o al<br />
trattamento di controllo, attraverso le procedure di<br />
randomizzazione.<br />
Questa assicura che tutti i fattori prognostici - sia noti che non<br />
conosciuti - vengono equamente distribuiti nei due gruppi di<br />
pazienti, tra i quali l’unica differenza risulta essere l’intervento<br />
terapeutico in studio.<br />
GIMBE ®
Trial Randomizzati Controllati<br />
Se lo studio è condotto ed analizzato in maniera adeguata,<br />
l’eventuale differenza di esiti tra i due gruppi può essere<br />
attribuita all’effetto del trattamento in studio.<br />
Esistono alcune condizioni per cui i RCTs non costituiscono il<br />
miglior disegno sperimentale:<br />
- storia naturale delle malattie studi di coorte<br />
- eziologia, fattori di rischio studi di coorte, studi casocontrollo<br />
- accuratezza diagnostica studi trasversali<br />
GIMBE ®
GIMBE ®<br />
Fasi degli studi sui<br />
farmaci<br />
Da dove nascono gli RCTs
GIMBE ®<br />
Fasi degli studi farmacologici<br />
• Nella fase I viene definita la massima dose<br />
tollerata e gli effetti tossici di un nuovo<br />
farmaco già sperimentato in laboratorio su<br />
animali (si svolgono pochi pazienti,
GIMBE ®<br />
Fasi degli studi farmacologici<br />
• La fase III rappresenta i tipici effettivi trials,<br />
in quanto si cerca di comparare il nuovo<br />
farmaco con un farmaco esistente o un<br />
intervento ritenuto efficace.<br />
• La fase IV riguarda gli studi che cercano di<br />
monitorare gli effetti indesiderati di un<br />
nuovo farmaco dopo che è stato<br />
approvato per il marketing.
GIMBE ®<br />
Necessità di ricorrere<br />
agli RCTs<br />
Ma è proprio indispensabile<br />
confrontare i risultati di due<br />
gruppi?
GIMBE ®<br />
Trial non controllati<br />
Il trattamento sperimentale viene<br />
assegnato a tutti i pazienti eleggibili<br />
consecutivamente osservati. Sono ad<br />
esempio le serie di casi o gli studi di fase I<br />
e II.
GIMBE ®<br />
Trial non controllati<br />
In assenza del gruppo di controllo, i<br />
benefici del trattamento sperimentale<br />
vengono misurati confrontando i risultati<br />
ottenuti al decorso della malattia non<br />
trattata (o trattata con terapia standard).<br />
I benefici del trattamento sperimentale<br />
vengono misurati riportando i benefici<br />
assoluti del trattamento (ad es. il 98% dei<br />
pazienti con polmonite trattati con<br />
l’antibiotico X è guarito)
GIMBE ®<br />
Pazienti eleggibili<br />
Trial non controllati<br />
Esposizione:<br />
Intervento<br />
sperimentale<br />
Follow up<br />
Outcome
GIMBE ®<br />
Trial non controllati<br />
• Principali fonti bias sono:<br />
- variabilità prognostica e di decorso della<br />
malattia.<br />
- effetto placebo.<br />
- aspettative ottimistiche del medico e del<br />
paziente.
L’effetto totale del trattamento è la somma<br />
del miglioramento spontaneo, delle risposte<br />
aspecifiche e della risposta specifica<br />
Copyright © 1996-2007 - GIMBE ®<br />
GIMBE ®<br />
Effetto reale del trattamento<br />
Effetto placebo<br />
Aspettative ottimistiche<br />
Effetto Hawthorne<br />
Miglioramento spontaneo
Effetto Effetto reale reale del del trattamento trattamento<br />
Dipende dai benefici o dai danni indotti dal<br />
trattamento in uso, può essere influenzato<br />
anche dalla storia naturale della malattia che<br />
porterà il paziente a migliorare o peggiorare<br />
comunque<br />
GIMBE ®
Induce il paziente a stare meglio per la<br />
consapevolezza di essere trattato<br />
L’effetto placebo può essere maggiore se il<br />
paziente ha fiducia nel medico o nella<br />
struttura sanitaria a cui si rivolge o se ha<br />
grande speranza che il nuovo trattamento<br />
sia efficace<br />
GIMBE ®<br />
Effetto placebo
Le aspettative ottimistiche del medico<br />
derivano dalla sua fiducia nel trattamento<br />
che sta sperimentando e che lo inducono a<br />
interpretare ottimisticamente i risultati<br />
terapeutici accentuando l’effetto placebo<br />
GIMBE ®<br />
Apettative ottimistiche
Induce il paziente a stare meglio per la<br />
consapevolezza di essere parte di uno<br />
studio<br />
GIMBE ®<br />
Effetto Hawthorne
In una certa epoca storica hanno prodotto<br />
evidenze inconfutabili per trattamento<br />
drammatica efficacia in condizioni ad esito<br />
invariabilmente fatale/sfavorele:<br />
GIMBE ®<br />
Trial non controllati<br />
– insulina nel coma diabetico.<br />
– penicillina nella polmonite pneumococcica (o<br />
nella endocardite batterica).<br />
– vitamina B12 nell’anemia perniciosa.<br />
– appendicectomia nell’appendicite acuta.
GIMBE ®<br />
Trial non controllati<br />
Oggi si utilizzano per:<br />
– efficacia del nuovo trattamento<br />
drammaticamente evidente in osservazioni<br />
iniziali.<br />
– patologie a decorso sfavorevole (arresto<br />
cardiaco, epatite fulminante, …).<br />
– patologie rare.<br />
– studi di fase I e II.<br />
– assenza di trattamenti alternativi di confronto.<br />
– presupposti fisiopatologici convincenti.<br />
Byar DP. NEJM 1990; 323: 1343
GIMBE ®<br />
Trial non controllati<br />
• Smith GC, Jill JP.<br />
Parachute use to prevent death and major<br />
trauma related to gravitational challenge:<br />
systematic review of randomised<br />
controlled trials. BMJ, Dec 2003; 327:<br />
1459 - 1461.
GIMBE ®<br />
Parachutes reduce the risk of injury<br />
after gravitational challenge, but their<br />
effectiveness has not been proved<br />
with randomized contolled trials.<br />
As with many interventions intended to prevent ill<br />
health, the effectiveness of parachutes has not been<br />
subjected to rigorous evaluation by using randomised<br />
controlled trials.<br />
Advocates of evidence based medicine have criticised<br />
the adoption of interventions evaluated by using only<br />
observational data.<br />
We think that everyone might benefit if the most<br />
radical protagonists of evidence based medicine<br />
organised and participated in a double blind,<br />
randomised, placebo controlled, crossover trial of the<br />
parachute.
GIMBE ®<br />
Mega-Trial<br />
• Sempre più frequenti<br />
• Dimensione del campione > 1.000 - > 10.000<br />
• Multicentrici >100 - > 1.000<br />
• Criteri di inclusione larghi<br />
• Disegno semplice, registrati solo dati essenziali<br />
• End points non equivocabili (es: mortalità)<br />
• Grande potenza statistica: possono evidenziare<br />
differenze di efficacia minime fra i trattamenti a<br />
confronto.<br />
Topol EJ & Califf RM. Br Heart J 1992; 68: 348
Magnesio nell’infarto miocardico<br />
Razionale: variazione nell’andamento di patologie cardiache in funzione<br />
della quantità di magnesio nell’acqua<br />
Studi su animali hanno mostrato l’attività antiaritmica, antiaggregante e<br />
coronarodilatatrice del magnesio<br />
Piccoli trials positivi sull’uso del magnesio nell’infarto<br />
Una review informale dei risultati ha mostrato una riduzione della<br />
mortalità da IMA (infarto acuto del miocardio)<br />
Una meta-analisi formale su 1300 pazienti con un totale di 78 decessi<br />
ha mostrato una riduzione del 55% nel rischio di morte (p=0.001)<br />
Studio LIMIT-1 su 100 paz. - diminuzione delle aritmie (1986)<br />
Studio LIMIT-2 su 2300 paz. - diminuzione dell’incidenza di insuff.<br />
ventricolare sinistra (1994)<br />
GIMBE ®<br />
Dai trial clinici ai mega-trial
GIMBE ®<br />
58.050 pazienti entro 24 ore dall’infarto in 1086 ospedali<br />
- captopril per 1 mese vs placebo<br />
- nitoderivati per un mese vs placebo<br />
- magnesio solfato IV 24 h vs controllo<br />
Risultati<br />
Il mega-trial ISIS-4 (1995)<br />
Il captopril previene 5 morti su 1000, i nitroderivati e il<br />
magnesio sono inefficaci
GIMBE ®<br />
Lancet, 1995 Mar 18;345(8951):669-85.
Trial controllati non randomizzati<br />
Sono caratterizzati dalla presenza di un gruppo<br />
di pazienti di controllo, i cui esiti vengono<br />
confrontati con quelli del gruppo dei pazienti<br />
trattati<br />
L'assegnazione dei pazienti all'uno o all'altro<br />
gruppo avviene con una delle seguenti<br />
procedure:<br />
‐ controlli paralleli (contemporanei)<br />
‐ controlli storici<br />
‐ controlli da banche dati<br />
GIMBE ®
I limiti comuni a tutti i CCTs sono:<br />
• lo sbilanciamento dei fattori prognostici tra i due<br />
gruppi di pazienti<br />
• la tendenza ad assegnare al trattamento<br />
sperimentale i pazienti a prognosi più favorevole<br />
• la sovrastima dell'efficacia del trattamento<br />
sperimentale, accentuata nelle CCTs con controlli<br />
storici dal miglioramento delle condizioni assistenziali<br />
Per tali ragioni le CCTs, non dovrebbero più occupare<br />
alcun ruolo nella moderna ricerca clinica (vedi Consort<br />
Statement II)<br />
Costituiscono a tutti gli effetti una frode scientifica<br />
Copyright © - GIMBE ®
GIMBE ®<br />
Cosa dobbiamo sapere<br />
quando leggiamo gli<br />
RCT<br />
Dove può essere<br />
l’imbroglio?
GIMBE ®<br />
Bias negli RCTs<br />
• Benchè costituiscano gli studi più rigorosi,<br />
in essi la presenza di errori sistematici<br />
(bias), compromette la credibilità e<br />
l’autorevolezza dei risultati.<br />
• I più comuni bias possono essere:<br />
– bias di selezione<br />
– bias di accertamento<br />
– bias di violazione del protocollo<br />
– bias di pubblicazione<br />
– bias temporali
GIMBE ®<br />
Selection bias<br />
• Accade quando gli outcome di uno studio<br />
sono influenzati dalle differenze<br />
sistematiche (reali e non casuali) dei due<br />
gruppi di studio, che dipendono dalle<br />
modalità con cui le persone sono state<br />
selezionate a partecipare al trial o con cui<br />
sono state assegnate ai due gruppi.<br />
• La prevenzione di questo tipo di bias si<br />
realizza con una corretta<br />
randomizzazione.
GIMBE ®<br />
Selection bias<br />
• Se uno studio è realmente randomizzato,<br />
l’allocazione ai gruppi non può essere<br />
influenzata dai ricercatori o dai<br />
partecipanti allo studio.<br />
• Con la randomizzazione a tutti i<br />
partecipanti dello studio sono date le<br />
stesse opportunità di essere assegnati ad<br />
ognuno dei gruppi di studio.
GIMBE ®<br />
Ascertainment bias<br />
• Questo tipo di bias accade quando i risultati o le<br />
conclusioni di un trial sono distorte dalla conoscenza<br />
relativa all’intervento a cui ogni partecipante è stato<br />
sottoposto. Questo tipo di errore può essere<br />
determinato da chi eroga l’intervento, dai soggetti<br />
studiati, dai ricercatori che valutano o analizzano gli<br />
outcome e coloro che scrivono l’articolo descrivente<br />
il trial.<br />
• Il miglior modo per evitare questo bias è mantenere<br />
le persone, coinvolte nello studio, non a conoscenza<br />
dell’identità dell’intervento il più a lungo possibile,<br />
realizzando quella che è detta CECITA’.
GIMBE ®<br />
Bias di violazione di protocollo<br />
Lost to follow‐up (persi al follow up)<br />
Withdrawal (sospendono il trattamento)<br />
Crossover (passano all’altro gruppo)
GIMBE ®<br />
Bias di violazione di protocollo<br />
Tutti i pazienti randomizzati devono essere<br />
inclusi nell’analisi alla fine dello studio (sia i<br />
persi al follow‐up, sia quelli che hanno sospeso<br />
il trattamento)<br />
Ciascun paziente deve essere analizzato nel<br />
gruppo originale di randomizzazione, anche se<br />
poi ha ricevuto il trattamento dell’altro braccio<br />
(cross‐over)
GIMBE ®<br />
Bias di violazione di protocollo<br />
• Ciò si giustifica con il fatto che, se il<br />
trattamento procura effetti indesiderati tali<br />
da non consentire al soggetto di seguire<br />
correttamente la terapia, considerare il suo<br />
esito negativo nel gruppo di controllo, ne<br />
accrescerebbe l’efficacia.<br />
• Questo tipo di elaborazione dei dati si<br />
chiama analisi secondo “intention to treat”.
GIMBE ®<br />
Follow up<br />
• Ogni paziente reclutato dovrebbe essere<br />
considerato fino alla fine, ma purtroppo<br />
non è sempre così, a causa, ad esempio<br />
del ritiro del pz dallo studio.<br />
• L’abbandono degli studi non avviene per<br />
caso. Addirittura esso potrebbe essere<br />
determinato dal trattamento stesso.<br />
• Per questo quando il numero dei persi al<br />
follow up non è uguale nei due gruppi, è<br />
legittimo nutrire qualche sospetto.
GIMBE ®<br />
Follow up<br />
• Dato che studiare solo coloro che sono rimasti<br />
nello studio può portare a sovrastimare<br />
l’efficacia del trattamento, gli autori dello studio<br />
devono riportare nelle conclusioni tutti coloro<br />
che erano stati reclutati, assegnando ai<br />
soggetti persi del gruppo di trattamento l’esito<br />
peggiore ed ai soggetti persi del gruppo di<br />
controllo l’esito migliore.<br />
• In questo caso il rischio è di sottostimare<br />
l’efficacia del trattamento, il che è sicuramente<br />
più accettabile del contrario.
Il limite tollerabile di persi durante il follow up è<br />
del 20%: difficilmente uno studio che ha<br />
dimostrato l’efficacia del trattamento, rimane<br />
tale attribuendo un esito negativo a più del<br />
20% dei pazienti.<br />
GIMBE ®<br />
Follow up
GIMBE ®<br />
Publication bias<br />
• Alcune evidenze dimostrano la probabilità<br />
di trovare pubblicato uno studio, non è<br />
casuale ma dipende dalla direzione e dalla<br />
forza dei risultati della ricerca, per cui i<br />
lavori con risultati statisticamente<br />
significativi (positivi) sono pubblicati con<br />
maggiore facilità rispetto a quelli con<br />
risultati non significativi.<br />
• Questa tendenza, che appare favorire i<br />
trials con risultati positivi, è stata chiamata<br />
pubblication bias.
GIMBE ®<br />
Publication bias<br />
Uno studio randomizzato sulla lorcainide<br />
(antiaritmico di classe I), dove si osservava un<br />
aumento di morti fra i pazienti trattati, non<br />
venne pubblicato per 13 anni.<br />
Negli anni 80 questi farmaci causarono fra<br />
20.000 e 70.000 morti premature negli USA<br />
Tonks, BMJ dicembre 1999
GIMBE ®<br />
Publication bias<br />
Lo studio VIGOR che ha promosso il VIOXX è<br />
stato pubblicato nel novembre 2000 sul New<br />
England Journal of Medicine<br />
Bombardier C. et al. “Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with<br />
rheumatoid arthritis.” VIGOR Study Group. N Engl J Med. 2000 Nov 23;343(21):1520-8<br />
Nel dicembre 2005 il NEJM informa i lettori<br />
che gli autori dello studio VIGOR avevano<br />
manipolato i dati dei risultati della ricerca<br />
omettendo casi di gravi effetti avversi<br />
Gregory D. et al. “Expression of Concern: Bombardier et al., ‘Comparison of Upper Gastrointestinal Toxicity of<br />
Refecoxib and Naproxen in Patients with Rheumatoid Arthritis’ N Engl J Med 2000 Nov 23;343(21):1520-8”<br />
N Engl J Med. 2005 Dec 29;353(26):2813-4.
GIMBE ®<br />
Publication bias
GIMBE ®<br />
Publication bias<br />
Dal 1999 al 2004 il VIOXX ha indotto negli<br />
USA circa 38.000 decessi supplementari<br />
(Lancet 2005)<br />
Stima per i paesi industrializzati: 140-160.000<br />
decessi supplementari
GIMBE ®<br />
Publication bias<br />
Nel maggio del 2006 il Wall Street Journal<br />
informa che l’editore del NEJM era già a<br />
conoscenza nell’agosto 2001 della<br />
manipolazione.<br />
La ditta produttrice del VIOXX (Merck) aveva<br />
acquistato nel novembre 2000 per la campagna<br />
pubblicitaria 900.000 ristampe dell’articolo del<br />
NEJM per circa 700-830.000 $<br />
Il profitto per il NEJM si aggirava intorno ai<br />
500.000$ Smith R. “Lapses at the new England journal of medicine.” J R Soc Med. 2006 Aug;99(8):380-2
GIMBE ®<br />
Bias temporali – Time lag bias<br />
• Questo tipo di errore accade in quanto la velocità di<br />
pubblicazione dipende dalla direzione e dalla forza<br />
dei risultati del trial. In generale sembra che uno<br />
studio con risultati negativi impieghi il doppio del<br />
tempo per essere pubblicato rispetto ad uno con<br />
risultati positivi.<br />
• Inoltre possono passare anni dal momento in cui lo<br />
studio è stato completato a quello in cui è<br />
pubblicato, tanto che il tempo per realizzalo sembra<br />
uguale a quello necessario per pubblicarlo e ciò<br />
riguarda allo stesso modo gli studi grandi e gli studi<br />
piccoli.
Possiamo quindi fidarci della<br />
generalizzabilità degli RCTs?<br />
In letteratura sono segnalati alcuni aspetti che<br />
devono portarci a considerare gli RCTs<br />
sempre con spirito critico. In particolare<br />
sono segnalati:<br />
GIMBE ®<br />
– Popolazioni estremanente selezionate<br />
(Gurwitz JH. Jama 1992).<br />
– Competenza, motivazioni e condizioni<br />
organizzativo-assistenziali ideali (Grilli R. Et<br />
al, Il Pensiero Scientifico Editore,1995).
GIMBE ®<br />
Possiamo quindi fidarci della<br />
generalizzabilità degli RCTs?<br />
– Risultati “medi” che non prevedono la risposta<br />
nel paziente individuale (Rothweel PM.<br />
Lancet 1995).<br />
– End point misurati (surrogati vs clinicamente<br />
significativi) (Fleming TR,et al. Ann.Inter.Med.<br />
1996).<br />
– Misure utilizzate per riportare i risultati<br />
(relative vs assolute) (Bobbio M, et al. Lancet<br />
1994).
Clinicamente rilevanti - comprendono, oltre la mortalità, tutti gli<br />
eventi clinici morbosi che possono essere rilevati nella storia<br />
naturale/post-terapeutica di una malattia<br />
Surrogati – sono variabili anatomico-fisiologico-metaboliche<br />
misurate con test di laboratorio/strumentali<br />
Hard - di sicura determinazione, per la verifica dei quali l’errore è<br />
minimo (mortalità)<br />
Soft - possono essere influenzati da imprecisioni o soggettività<br />
(es. miglioramento di un quadro sintomatologico, lettura di un<br />
ECG/Rx)<br />
GIMBE ®<br />
End point
GIMBE ®<br />
Trattamento End point surrogato<br />
Encainide, Flecainide,<br />
Moricizina: extrasistolia<br />
ventricolare post-IMA (1)<br />
Milrinone: insufficienza<br />
eardiaca (2)<br />
NaF: osteoporosi (2)<br />
End point<br />
End point<br />
rilevante<br />
extrasistolia mortalità<br />
portata circolatoria mortalità<br />
densità minerale<br />
ossea<br />
incidenza<br />
fratture<br />
(1) Epstein AE & al. JAMA 1993; 270:2451<br />
(2) Da: Fleming TR & al Ann Intern Med 1996;125:605
GIMBE ®<br />
Misure di efficacia negli<br />
RCTs
GIMBE ®<br />
Misure di efficacia<br />
Nella lettura degli studi troveremo indicate<br />
diverse misure di efficacia.<br />
La comprensione del loro significato,<br />
l’interpretazione del loro valore e della loro<br />
precisione ci servono per capire la forza e<br />
la direzione della associazione che vi è tra<br />
trattamento e outcome (e quindi di capire<br />
se l’intervento è efficace e in che misura).
GIMBE ®<br />
Esempi<br />
o<br />
Cullen l, et al. Nebulized lidocaine decrease the discomfort of nasogastric<br />
tube insertion: a randomized, doubleblind trial. Ann Emerg Med 2004; 44:<br />
131-7.<br />
La somministrazione di lidocaina nebulizzata prima dell’inserimento<br />
del sondino naso gastrico riduce il disagio del paziente?<br />
P: Adulti da sottoporre a posizionamento del SNG in pronto<br />
soccorso.<br />
I: nebulizzazione di lidocaina nella narice da utilizzare.<br />
C: nebulizzazione di soluzione fisiologica.<br />
O: disagio misurato attraverso una scala visuale analogica (misura<br />
continua), difficoltà di inserimento del sondino (misura continua),<br />
complicanze (sanguinamento, vomito, impossibilità di passaggio,<br />
dispnea – misure discrete).
GIMBE ®<br />
Esempi<br />
o<br />
Outcome Lidocaina Placebo<br />
Disagio riferito<br />
(media dei<br />
punteggi della<br />
scala visuale<br />
analogica)<br />
Difficoltà<br />
percepita<br />
dall’infermiere<br />
nell’inserimento<br />
del SNG<br />
Sanguinamento<br />
nasale<br />
Differenza<br />
(IC 95%)<br />
37.7 59.3 26.6 (5.3 a 38.0)<br />
2 2 0 (-1 a 1)<br />
17% 0 17% (3,5-31)<br />
Vomito 10% 0 10%(-0,7-21)
Il primo passaggio per capire le diverse misure di<br />
efficacia consiste nel tabellare i dati.<br />
GIMBE ®<br />
Misure di efficacia per gli esisti discreti<br />
Evento Sì Evento No<br />
Gruppo S a + b<br />
a b<br />
Gruppo C c + d<br />
c d<br />
a + c b + d
GIMBE ®<br />
Misure di efficacia per gli esisti discreti<br />
Experimental Event Rate<br />
- Frequenza (o rischio)<br />
nel gruppo<br />
sperimentale<br />
a<br />
EER =<br />
a + b<br />
Control Event Rate -<br />
Frequenza (o rischio) nel<br />
gruppo di controllo<br />
c<br />
CER =<br />
c + d<br />
La EER ci dice con che<br />
frequenza l’evento<br />
indesiderato<br />
si è verificato<br />
nel gruppo sperimentale<br />
La CER ci dice con che<br />
frequenza l’evento<br />
indesiderato<br />
si è verificato<br />
nel gruppo sperimentale
Rischio Relativo / RR<br />
EER<br />
RR = =<br />
GIMBE ®<br />
Misure di efficacia per gli esisti discreti<br />
CER<br />
a<br />
a + b<br />
c<br />
c + d<br />
Dal rapporto tra EER e CER<br />
individuiamo il rischio relativo<br />
che ci dice qual è il rischio di<br />
manifestare l’evento negativo<br />
nel gruppo sperimentale rispetto<br />
a quello del gruppo di controllo.<br />
Se l’intervento ha un effetto<br />
benefico<br />
RR1<br />
Se non c’è differenza<br />
RR=1
GIMBE ®<br />
Misure di efficacia per gli esisti discreti<br />
OR =<br />
Odds ratio / OR<br />
a/b<br />
c/d<br />
A volte per motivi statistici<br />
anziché essere calcolato il RR<br />
troviamo indicato l’odds ratio<br />
che non confronta le<br />
frequenze<br />
(rischio) degli eventi,<br />
ma le loro probabilità.<br />
se l’intervento ha un effetto<br />
benefico<br />
OR1<br />
Se non c’è differenza<br />
OR=1
GIMBE ®<br />
Il difetto di RR e OR<br />
Sia il RR che l’OR sono misure della forza<br />
dell’associazione tra trattamento ed esito<br />
RELATIVE. Esse, cioè, non ci danno<br />
espressione della importanza clinica degli<br />
eventi nei due gruppi.<br />
Per questo motivo, per comprendere la<br />
rilevanza clinica degli effetti, vengono<br />
calcolate altre misure di efficacia.
GIMBE ®<br />
Misure di efficacia per gli esisti discreti<br />
Riduzione Assoluta del<br />
Rischio<br />
ARR = CER _ EER<br />
Riduzione Relativa del<br />
Rischio<br />
ARR<br />
RRR =<br />
CER<br />
La riduzione del rischio<br />
assoluto ci dà l’esatta<br />
espressione<br />
di quanto si riduca la frequenza<br />
degli eventi negativi con<br />
il trattamento<br />
sperimentato.<br />
La riduzione del rischio<br />
relativo dice con che<br />
proporzione diminuisce<br />
il rischio con<br />
il trattamento sperimentato.
GIMBE ®<br />
I difetti di RRR e ARR<br />
La RRR è di nuovo una misura relativa,<br />
che non ci dà idea della frequenza, e<br />
quindi dell’importanza, dell’evento<br />
negativo.<br />
Al contrario ARR è proprio espressione di<br />
questa misura, ma essendo un numero<br />
decimale non è facile da ricordare.<br />
Per questo motivo la misura che rende al<br />
meglio l’importanza clinica<br />
dell’associazione tra trattamento ed<br />
outcome è il NNT.
GIMBE ®<br />
Misure di efficacia per gli esisti discreti<br />
Number Needed to Treat<br />
1<br />
NNT =<br />
ARR<br />
Il numero dei pazienti da<br />
trattare ci dice il numero di<br />
quante persone è necessario<br />
trattare per evitare un<br />
evento negativo. Si tratta di<br />
un valore espresso con<br />
numeri interi (e quindi è più<br />
facile da ricordare)<br />
tanto più è piccolo tanto<br />
maggiore è l’efficacia clinica<br />
del trattamento.<br />
Tanto più è grande<br />
tanto più è modesta l’efficacia<br />
del trattamento.
GIMBE ®<br />
Un esempio reale<br />
Trivedi DP, Doll R, Khaw KT. Effect of four montly oral<br />
vitamin D3 supplementation on fracutres and mortality in<br />
men and women living in the community: randomised<br />
double blind controlled trial. BMJ 2003; 326:469-72.<br />
La somministrazione di un integratore di Vitamina D3 per<br />
via orale riduce l’incidenza di fratture negli anziani (65-<br />
85) residenti al domicilio?<br />
P: anziani residenti al domicilio.<br />
I: somministrazione di un integratore di Vit D3.<br />
C: somministrazione di un placebo.<br />
O: Incidenza di fratture e mortalità da tutte le cause.
Gruppo<br />
intervento<br />
Trattamento<br />
sperimentale<br />
Trattamento<br />
controllo<br />
Frattura Non<br />
frattura<br />
N. Tot.<br />
119 1226 1345<br />
149 1192 1341<br />
Riduzione relativa del<br />
rischio = di quanto si<br />
riduce il rischio nel gruppo<br />
sperimentale?<br />
Riduzione assoluta del<br />
rischio = differenza (%) fra<br />
controllo e sperimentale<br />
Rischio Relativo Riduzione Assoluta del Rischio<br />
EER 0,088<br />
RR = = = 0,8 ARR= CER - EER= 0,11 – 0,088 = 0,022<br />
CER 0,11<br />
Riduzione Relativa del Rischio Number Needed to Treat<br />
ARR 0,022 1 1<br />
RRR = = = 20% NNT = = = 44<br />
CER 0,11 ARR 0,022<br />
GIMBE ®
GIMBE ®<br />
Un esempio reale<br />
RCT a doppio cieco della durata di 5 anni sulla riduzione del rischio di<br />
malattie coronariche con la somministrazione di gemfibrozil.<br />
Pazienti arruolati: 4081<br />
gruppo sperimentale (gemfibrozil) 2051 pz.<br />
gruppo controllo (placebo) 2030 pz.<br />
HELSINKI HEART STUDY<br />
New England Journal of Medicine 1987;<br />
317:1237-45<br />
gruppo sperimentale eventi cardiaci 56<br />
morti 45<br />
gruppo controllo eventi cardiaci 84<br />
morti 42<br />
Calcolare RR, ARR, RRR, NNT
GIMBE ®<br />
Spesso i risultati degli studi clinici sono presentati<br />
in termini di riduzione relativa del rischio (RRR)<br />
espressa come percentuale. RRR èun indicatore<br />
che, se non completato da ulteriori elementi, può<br />
enfatizzare l’efficacia di un trattamento, in<br />
particolare può far credere che il risultato sia più<br />
rilevante del reale nella pratica medica.
GIMBE ®<br />
Studio A: 10.000 pazienti per gruppo; EER= 0,1 (10%); CER=0,2<br />
(20%); RRR= 0,5 (50%)<br />
Studio B: 10.000 pazienti per gruppo; EER= 0,01 (1%); CER=0,02<br />
(2%); RRR= 0,5 (50%)<br />
Studio C: 10.000 pazienti per gruppo; EER= 0,001 (0,1%); CER=0,002<br />
(0,2%); RRR= 0,5 (50%)<br />
ARR<br />
Studio A: 0,1 (10%); Studio B: 0,01 (1%); Studio C: 0,001 (0,1%)<br />
NNT<br />
Studio A: 10 soggetti; Studio B: 100 soggetti; Studio C: 1000<br />
soggetti
GIMBE ®<br />
La curva gaussiana
GIMBE ®<br />
Intervallo di confidenza (IC)<br />
Quando valutiamo l’efficacia di un<br />
trattamento, oltre ad osservare il valore<br />
della misura di efficacia, dobbiamo<br />
valutarne la sua precisione.<br />
Ciò si effettua considerando l’intervallo di<br />
confidenza (IC).
L’intervallo di confidenza (IC) fornisce la<br />
misura della precisione dei risultati di una<br />
ricerca, così da poter trarre deduzioni sulla<br />
popolazione da cui sono tratti quei pazienti.<br />
Per convenzione si è stabilito che la<br />
precisione dell’intervallo di confidenza sia al<br />
95%, lasciando sempre un piccolo - 5% -<br />
margine di errore dovuto al caso.<br />
GIMBE ®<br />
Intervallo di confidenza (IC)
Stima l’intervallo dei valori all’interno del<br />
quale, con una probabilità del 95%,<br />
partendo dal risultato conseguito nel<br />
campione, cade il reale valore della<br />
popolazione studiata.<br />
L’IC si fonda sull’idea che lo stesso studio,<br />
condotto su differenti campioni di pazienti,<br />
non porterebbe a risultati identici, ma questi<br />
sarebbero distribuiti intorno al risultato vero<br />
che resta sconosciuto.<br />
GIMBE ®<br />
Intervallo di confidenza (IC)
GIMBE ®<br />
Intervallo di confidenza (IC)<br />
In particolare dobbiamo verificare:<br />
– Quanto è ampio l’intervallo di confidenza.<br />
– Che i suoi limiti non vadano oltre il valore che<br />
conferma l’ipotesi nulla (assenza di<br />
associazione).
GIMBE ®<br />
Intervallo di confidenza (IC)<br />
Tanto più è ampio l’intervallo di confidenza, tanto<br />
meno precisa è la stima dell’associazione tra fattori<br />
di rischio e condizione (e meno dobbiamo fidarci del<br />
risultato dello studio).<br />
L’ampiezza dell’IC è inversamente proporzionale<br />
alla dimensione del campione (se sono stati inclusi<br />
pochi soggetti il risultato ottenuto è<br />
necessariamente poco preciso).
GIMBE ®<br />
Ipotesi nulla<br />
Coloro che eseguono lo studio mirano a<br />
dimostrare l’esistenza di una relazione tra<br />
il trattamento ed il miglioramento<br />
dell’outcome, cercando di dimostrare<br />
l’inesistenza dell’ipotesi nulla.<br />
L’ipotesi nulla sussiste tutte le volte in cui<br />
non vi è alcuna relazione tra il<br />
miglioramento dell’esito ed il trattamento<br />
studiato.
GIMBE ®<br />
Ipotesi nulla - H0 Ipotesi alternativa - H1<br />
Non esiste una reale<br />
differenza tra le variabili<br />
studiate: le differenze<br />
osservate sono dovute<br />
la caso.<br />
Ipotesi nulla<br />
Le differenze osservate<br />
sono troppo grandi per<br />
essere dovute al caso.
GIMBE ®<br />
Ipotesi nulla<br />
Come faccio a verificare che l’ipotesi nulla<br />
si è verificata o meno?<br />
Attraverso l’esame dei valori delle misure<br />
di efficacia, che non devono esprimere<br />
specifici valori.
GIMBE ®<br />
Ipotesi nulla nei parametri discreti<br />
Parametro Valore nullo<br />
RRR, RR, OR 1<br />
ARR 0<br />
NNT Infinito<br />
ARR non deve essere 0, perché<br />
significherebbe che il beneficio<br />
ottenuto in termini di riduzione<br />
assoluta del rischio è 0, nel qual caso<br />
NNT diventerebbe un valore tendente<br />
ad infinito.<br />
Se questo valore<br />
è 1, il rischio o la<br />
probabilità di<br />
incorrere<br />
nell’evento<br />
avverso sono<br />
Uguali, sia che<br />
si faccia il<br />
trattamento o meno
GIMBE ®<br />
Ipotesi nulla nei parametri continui<br />
Nel caso in cui lo studio misuri parametri<br />
continui, mediante la dimostrazione della<br />
differenza della media, essa non deve<br />
essere 0.
GIMBE ®<br />
Significatività statistica<br />
Oltre a verificare i valori delle misure di<br />
efficacia, e del loro IC, vi è anche un altro<br />
parametro che occorre osservare che ci<br />
dice quale sia la significatività statistica dei<br />
risultati ottenuti.<br />
Si tratta del test di significatività che<br />
attribuisce il valore ad una variabile detta<br />
“p”.
GIMBE ®<br />
Significatività statistica<br />
Il valore di “p” misura la probabilità che la<br />
associazione osservata possa essere<br />
dovuta a fluttuazioni casuali, ossia alla<br />
possibile variabilità tra campioni, e possa<br />
quindi non corrispondere a fenomeni reali.<br />
Quanto deve essere il valore di “p” per<br />
poter escludere l’ipotesi nulla?
GIMBE ®<br />
Significatività statistica<br />
Viene deciso dei ricercatori che indicano il<br />
livello di significatività statistica stabilito.<br />
Il livello di significatività per convenzione è<br />
0,05. Si conclude cioè che una differenza non<br />
è dovuta al caso se “p” è uguale o inferiore a<br />
0,05.<br />
Nel caso i ricercatori vogliano darsi una<br />
maggiore rigorosità statistica possono portare<br />
tale valore soglia a 0,01.
GIMBE ®<br />
Significatività statistica<br />
È chiaro quindi che<br />
– "Significativo" non è sinonimo di "importante“<br />
– "Significativo" = difficilmente dovuto al puro<br />
caso.
La significatività statistica non è l’unico criterio utile per<br />
decidere se utilizzare i risultati di uno studio. La<br />
significatività statistica dipende dalla numerosità del<br />
campione e dall’entità dell’efficacia del trattamento<br />
(differenze degli esiti). Differenze clinicamente<br />
irrilevanti possono divenire statisticamente significative<br />
se le dimensioni dei campioni sono sufficientemente<br />
grandi. Al contrario, differenze clinicamente rilevanti<br />
possono essere statisticamente non significative se i<br />
campioni sono troppo piccoli (in gergo statistico, se lo<br />
studio manca di potenza statistica).<br />
GIMBE ®<br />
Significatività statistica
GIMBE ®<br />
Randomized Controlled<br />
Trials - Critical Appraisal<br />
Come si valutano i Trial<br />
Randomizzati Controllati.
Durante la lettura di una pubblicazione si<br />
devono trovare informazioni sufficienti,<br />
presentate chiaramente e coerentemente,<br />
affinché si possa decidere, in base alle<br />
evidenze fornite dagli autori, se le<br />
conclusioni a cui arrivano sono logiche e<br />
credibili.<br />
GIMBE ®<br />
Critical appraisal
GIMBE ®<br />
Critical appraisal<br />
1. Validità interna<br />
2. Rilevanza clinica<br />
3. Applicabilità<br />
4. Consistenza
E’ diretta funzione del rigore metodologico seguito dai<br />
ricercatori nelle fasi di:<br />
pianificazione e conduzione dello studio<br />
analisi dei risultati<br />
La validità interna ha l’obiettivo di minimizzare i bias<br />
che possono “distorcere” la validità interna della ricerca<br />
I criteri di validità interna variano con il disegno dello<br />
studio correlato agli obiettivi (eziologia, diagnosi,<br />
prognosi, trattamento)<br />
GIMBE ®<br />
Validità interna
GIMBE ®<br />
Validità interna<br />
A. I risultati dello studio sono validi?<br />
Domande preliminari<br />
Lo studio si basa su una domanda di ricerca<br />
chiaramente formulata?<br />
– Una domanda di ricerca è chiaramente formulata se sono<br />
indicati la popolazione studiata, l’intervento erogato,<br />
l’outcome considerato<br />
Gli autori hanno utilizzato il tipo giusto di<br />
studio?<br />
– Deve esserci coerenza tra il disegno dello studio ed il<br />
quesito.<br />
Vale la pena continuare?
GIMBE ®<br />
Validità interna<br />
A. I risultati dello studio sono validi?<br />
Domande specifiche<br />
L’assegnazione dei pazienti al trattamento è<br />
randomizzato?<br />
– I migliori metodi di randomizzazione sono<br />
quelli realizzati con il computer o con le<br />
tabelle dei numeri random; sistemi più deboli<br />
sono rappresentati dalla assegnazione<br />
alternata, secondo l’ordine di arrivo o del<br />
giorno, settimana o mese. Se non c’è stata randomizzazione<br />
si può anche lasciare perdere<br />
l’articolo in esame.
GIMBE ®<br />
Validità interna<br />
Tutti i pazienti ammessi a partecipare allo studio<br />
sono stati considerati in modo appropriato nella<br />
formulazione delle conclusioni?<br />
– La percentuale dei pazienti persi al follow up<br />
non può essere superiore al 20%.<br />
– L’analisi dei risultati deve essere effettuata<br />
secondo l’intention to treat.
GIMBE ®<br />
Validità interna<br />
Vi era cecità rispetto al trattamento? A che livelli?<br />
– Considera che questo non è sempre<br />
possibile, ma valuta se sono stati compiuti<br />
tutti gli sforzi per assicurare la cecità. In<br />
generale coloro che analizzano i dati<br />
possono sempre non essere resi a<br />
conoscenza a che gruppo si riferiscono i<br />
dati che stanno analizzando.
GIMBE ®<br />
Validità interna<br />
I gruppi erano simili all’inizio dello studio?<br />
– Valuta l’eventuale presenza di fattori di<br />
confondimento che possono avere influito<br />
sugli esiti.<br />
Al di là dell’intervento sperimentale i<br />
partecipanti sono stati assistiti nello stesso<br />
modo?<br />
– Ad esempio verifica se sono stati valutati agli<br />
stessi intervalli.
GIMBE ®<br />
Critical appraisal<br />
1. Validità interna<br />
2. Rilevanza clinica<br />
3. Applicabilità<br />
4. Consistenza
GIMBE ®<br />
Rilevanza clinica<br />
Misura, oltre la significatività statistica, l’entità e la<br />
precisione dei risultati dello studio<br />
Corrisponde alla fase di analisi dei risultati<br />
Gli elementi che influenzano la rilevanza clinica sono<br />
diversi per gli studi di:<br />
• trattamento<br />
• diagnosi<br />
• eziologia e prognosi
Studi di eziologia e prognosi<br />
‐ Rilevanza clinica del danno o fattore prognostico<br />
‐ RR (studi di coorte), OR (studi caso‐controllo)<br />
‐ Ampiezza limiti di confidenza<br />
Copyright © - GIMBE ®<br />
Rilevanza clinica
GIMBE ®<br />
Rilevanza clinica<br />
Studi su trattamenti<br />
‐ Rilevanza clinica dell’end‐point (surrogato vs<br />
significativo)<br />
‐ NNT<br />
‐ Ampiezza limiti di confidenza
GIMBE ®<br />
B. Quali sono i risultati?<br />
Rilevanza clinica<br />
Quanto è grande l’effetto del trattamento?<br />
– Verificare che i parametri di efficacia non<br />
corrispondano al valore dell’ipotesi nulla.<br />
– Quanto precisa è la stima dell’effetto del<br />
trattamento?<br />
– Valutare gli intervalli di confidenza ed il valore<br />
di “p”.
GIMBE ®<br />
Critical appraisal<br />
1. Validità interna<br />
2. Rilevanza clinica<br />
3. Applicabilità<br />
4. Consistenza
E’ il grado con cui i risultati dello studio possono essere<br />
applicati al paziente individuale<br />
GIMBE ®<br />
Applicabilità<br />
Sinonimi: validità esterna, generalizzabilità<br />
E’ condizionata da:<br />
criteri di selezione dei pazienti: inclusione, esclusione<br />
setting assistenziale: aspetti strutturali‐organizzativi,<br />
tecnologie, “competence” professionale<br />
descrizione accurata e completa delle modalità di<br />
erogazione degli interventi sanitari
GIMBE ®<br />
Applicabilità<br />
C. Il risultato potrà aiutarti a livello locale?<br />
I risultati possono essere applicati alla<br />
popolazione locale?<br />
– Considera se i pazienti considerati nel trial<br />
sono così diversi da quelli da te assistiti.
Explanatory<br />
RCTs<br />
Ideal<br />
condition<br />
GIMBE ®<br />
Internal validity<br />
(efficacy)<br />
Generalizzability<br />
(effectiveness)<br />
Pragmatic<br />
RCTs<br />
Routine<br />
clinical practice
GIMBE ®<br />
Critical appraisal<br />
1. Validità interna<br />
2. Rilevanza clinica<br />
3. Applicabilità<br />
4. Consistenza
GIMBE ®<br />
Consistenza<br />
Si riferisce al fatto che i risultati di uno studio vengano<br />
confermati da altri studi<br />
Sinonimi: riproducibilità della ricerca<br />
Lo strumento ideale per verificare la consistenza della<br />
ricerca è rappresentato dalle revisioni sistematiche con<br />
meta‐analisi di più studi<br />
N.B. Il bias di pubblicazione, oltre a sovrastimare<br />
l’efficacia dei trattamenti, influenza la consistenza della<br />
ricerca
Mortality in the placebo and beta-blocker groups of 22 RCTs<br />
GIMBE ®<br />
Brophy JM, et al. Ann Intern Med 200
Lo studio è valido?<br />
I risultati dello studio sono<br />
clinicamente rilevanti?<br />
I risultati dello studio sono<br />
applicabili?<br />
GIMBE ®<br />
sì<br />
sì<br />
sì<br />
Best evidence for patients<br />
no<br />
no<br />
no<br />
Presenza di bias che<br />
compromettono la validità dei<br />
risultati<br />
Risultati validi, ma irrilevanti: end<br />
points surrogati, NNT elevato, ampi<br />
limiti di confidenza<br />
Risultati validi e clinicamente<br />
rilevanti, ma non applicabili nel mio<br />
contesto assistenziale
GIMBE ®<br />
THE END<br />
GIMBE ®
GIMBE ®<br />
<strong>Evidence</strong> <strong>Based</strong> <strong>Practice</strong><br />
Gabriele Manzi<br />
Azienda U.S.L. di Bologna
GIMBE ®<br />
Clinical state, setting<br />
and circumstances<br />
Research<br />
evidence<br />
Clinical<br />
expertise<br />
Patient<br />
preferences<br />
Health care<br />
resources<br />
Modificato da Haynes RB et al ACP J Club. 2002; 136:A11-14.
“…E’ causa di grande preoccupazione constatare<br />
come la professione medica non abbia saputo<br />
organizzare un sistema in grado di rendere<br />
disponibili e costantemente aggiornate, revisioni<br />
critiche sugli effetti dell’assistenza sanitaria”<br />
GIMBE ®<br />
Archibald Cochrane, 1972
ANATOMIA DELL’INFORMAZIONE<br />
DELL INFORMAZIONE<br />
RICERCA<br />
PRIMARIA<br />
• Studi<br />
Osservazionali<br />
• Studi<br />
Sperimentali<br />
GIMBE ®<br />
BIOMEDICA<br />
RICERCA<br />
SECONDARIA<br />
• Revisioni<br />
Sistematiche<br />
• Linee Guida<br />
• Analisi<br />
economiche<br />
• Analisi decisionali<br />
Distorsione dei risultati<br />
FONTI<br />
TERZIARIE<br />
• Revisioni<br />
tradizionali<br />
• Trattati<br />
• Editoriali<br />
• Parere degli<br />
esperti
GIMBE ®<br />
Reviews<br />
Hanno lo scopo di rendere più<br />
“maneggevole” una enorme quantità di<br />
informazioni<br />
• revisioni tradizionali<br />
• revisioni sistematiche
Le revisioni tradizionali, oltre ad avere obiettivi<br />
molto ampi, non sono basate su una ricerca<br />
sistematica delle evidenze disponibili, ma su una loro<br />
selezione legata a diversi fattori: reperibilità,<br />
accessibilità linguistica, sintonia con le idee<br />
dell’autore<br />
Nelle revisioni sistematiche esiste un protocollo<br />
che definisce un preciso obiettivo e descrive fonti e<br />
metodi utilizzati per ricercare, selezionare e<br />
sintetizzare gli studi primari.<br />
GIMBE ®<br />
Narrative reviews vs Systematic reviews<br />
Cartabellotta A. Rec Prog Med 1998
GIMBE ®<br />
Narrative reviews<br />
Paragonabile al capitolo di un libro<br />
Non esplicitato il metodo di selezione,<br />
sintesi e interpretazione delle evidenze<br />
Impossibilità di fare una valutazione<br />
critica<br />
Obiettivi molto ampi<br />
Spesso fatte su commissione
GIMBE ®<br />
Systematic reviews<br />
E’ una ricerca scientifica vera e propria<br />
Esplicitato il protocollo metodologico<br />
Possibilità di fare una valutazione critica<br />
(definizione di obiettivi, fonti, criteri…)<br />
Sintesi dei risultati spesso fatta con<br />
metodo meta analitico
GIMBE ®<br />
Narrative vs Systematic Review<br />
Caratteristica Revisione<br />
narrativa<br />
Domande Molto vasta<br />
Revisione<br />
sistematica<br />
Focalizzate su problemi<br />
clinici<br />
Risorse e ricerca Non specificate Complete ed esplicite<br />
Selezione Non specificate Basato su criteri espliciti<br />
Critical appraisal Variabile Rigoroso<br />
Sistesi Qualitativa<br />
Qualitativa/quantitativa<br />
*meta-analisis
GIMBE ®<br />
Systematic reviews<br />
E’ uno strumento capace di risolvere alcuni<br />
problemi legati alla ricerca e alla<br />
interpretazione delle migliori evidenze<br />
Ha un ruolo sempre crescente per la pratica<br />
clinica,<br />
per la formazione permanente,<br />
per le decisioni di politica sanitaria
Processo di sviluppo delle RS<br />
Nel loro approccio, i ricercatori, usano<br />
metodi che sono pianificati e documentati<br />
in un protocollo di revisione sistematica<br />
Il protocollo di revisione sistematica<br />
assicura che la revisione sia condotta con<br />
lo stesso rigore che ci si aspetta da una<br />
ricerca<br />
GIMBE ®<br />
Systematic reviews
GIMBE ®<br />
Systematic reviews<br />
Componenti essenziali del processo<br />
Definizione del quesito<br />
Strategia di ricerca<br />
Definizione dei criteri di<br />
inclusione/esclusione<br />
Valutazione qualità degli studi<br />
Estrapolazione dei dati<br />
Analisi dei dati
GIMBE ®
E’ un momento fondamentale del processo<br />
di una revisione sistematica<br />
Deve definire i partecipanti, gli interventi da<br />
valutare, gli esiti da misurare<br />
Quesiti poco chiari e troppo generici<br />
portano a revisioni di qualità scadente<br />
GIMBE ®<br />
Quesito
GIMBE ®
GIMBE ®<br />
Definizione dei criteri di<br />
inclusione/esclusione<br />
Devono essere sempre definiti prima di<br />
iniziare la ricerca degli studi in<br />
letteratura<br />
Devono riflettere direttamente il quesito<br />
della ricerca (partecipanti, interventi,<br />
risultati)<br />
Devono indicare che tipo di studi<br />
verranno selezionati
GIMBE ®
GIMBE ®<br />
Elementi per la strategia di ricerca<br />
Database<br />
Ricerca manuale<br />
Ricerca bibliografica<br />
Contatti con i ricercatori<br />
Ricerca di letteratura non pubblicata
GIMBE ®<br />
Elementi per la strategia di ricerca<br />
Lo scopo è di identificare quanti più studi<br />
ragionevolmente possibili sull’argomento;<br />
Anche i lavori non pubblicati devono essere<br />
richiesti per aiutare a minimizzare i rischi di<br />
pubblicazione. Le riviste tendono ad<br />
accettare e pubblicare più facilmente le<br />
ricerche che dimostrano un esito positivo.<br />
Includere, quando è possibile, anche le<br />
pubblicazioni non in inglese
GIMBE ®
GIMBE ®<br />
Valutazione della qualità degli studi<br />
Una RS di buona qualità dipende soprattutto<br />
dalla qualità degli studi inclusi<br />
La valutazione dello studio deve essere<br />
condotta sulla metodologia della ricerca<br />
utilizzata per condurre lo studio stesso<br />
Esistono numerosi strumenti per effettuare<br />
una valutazione critica<br />
Va definito il metodo usato per la<br />
valutazione e per l’analisi delle informazioni<br />
per farli conoscere ai fruitori della RS
GIMBE ®
GIMBE ®<br />
Sintesi degli studi<br />
Definizione dei risultati importanti per le<br />
proprie necessità<br />
Estrapolare i dati nel modo più accurato<br />
possibile, tale che siano di facile utilizzo<br />
quando si affronta l’analisi dei dati stessi<br />
Creare uno strumento (es. una griglia)<br />
dove registrare le informazioni che<br />
servono, relative ad ogni studio incluso<br />
nella RS
GIMBE ®
GIMBE ®<br />
Sintesi dei dati<br />
L’obiettivo di una revisione sistematica è di<br />
riassumere i risultati di differenti studi per<br />
ottenere una valutazione totale dell’efficacia<br />
di un intervento o di un trattamento.<br />
Per un buon livello qualitativo, l’analisi dei<br />
dati va definita nel protocollo della RS.
Sintesi dei dati<br />
L’obiettivo di una revisione sistematica è di<br />
riassumere i risultati di differenti studi per<br />
ottenere una valutazione totale dell’efficacia<br />
di un intervento o di un trattamento.
GIMBE ®<br />
Sintesi dei dati<br />
I dati di una revisione si possono analizzare<br />
in modi differenti: se quantitativi si prestano<br />
al metodo statistico della meta-analisi, se<br />
qualitativi possono essere presentati in<br />
forma narrativa<br />
In entrambi i casi è opportuno definire a<br />
priori la metodologia che si intende seguire
GIMBE ®
GIMBE ®<br />
Systematic reviews critical appraisal<br />
La RS presenta un quesito ben definito?<br />
(partecipanti, interventi, outcomes)<br />
E’ stato fatto un lavoro sostanziale per la<br />
ricerca della letteratura? (database appropriati,<br />
key words adeguate, letteratura non pubblicata)<br />
E’ stata data una corretta e chiara definizione<br />
dei criteri di inclusione/esclusione? Questi sono<br />
adeguati?
GIMBE ®<br />
Systematic reviews critical appraisal<br />
E’ stata valutata dagli autori la qualità degli<br />
studi inclusi nella RS?<br />
Gli autori forniscono sufficienti informazioni<br />
sui singoli studi? (progetto di ricerca,<br />
dimensione del campione, descrizione<br />
dell’intervento, risultati ottenuti)<br />
Gli studi sono stati assemblati in modo<br />
appropriato? (test di eterogeneità)
GIMBE ®<br />
Meta-analisi<br />
Metodo per combinare i risultati di più studi<br />
indipendenti in modo da poter calcolare un<br />
valore statistico riassuntivo totale (cumula<br />
insieme più studi per ottenere un risultato<br />
unico)<br />
Consente una stima più precisa dell’efficacia di<br />
un trattamento<br />
La validità di una MA dipende anche dalla<br />
qualità della RS su cui si basa
Systematic review analisi metodologica<br />
GIMBE ®<br />
Meta – analisi analisi statistica
GIMBE ®<br />
Revisioni sistematiche<br />
(qualitative)<br />
***<br />
Revisioni sistematiche<br />
(quantitative)<br />
Meta – analisi<br />
(non sistematiche)
E’ utilizzata nei casi di incertezza nella valutazione<br />
di efficacia di un trattamento<br />
quando i risultati dei singoli studi non sono univoci<br />
quando singoli studi sono effettuati su un campione di<br />
pazienti numericamente scarso (poco affidabili)<br />
GIMBE ®<br />
Meta-analisi<br />
LA COMBINAZIONE DEI DATI DIMINUISCE<br />
L’IMPRECISIONE DEI RISULTATI DEI SINGOLI STUDI
GIMBE ®<br />
Antmann EM, et al. JAMA 1992
GIMBE ®
GIMBE ®<br />
The<br />
Cochrane Library
GIMBE ®<br />
Cochrane Collaboration<br />
Nel 1993 nasce la fondazione Cochrane<br />
Collaboration, un network internazionale con<br />
l’obiettico di “preparare, aggiornare e disseminare<br />
revisioni sistematiche degli studi clinici controllati<br />
sugli effetti dell’assistenza sanitaria e, laddove<br />
non disponibili studi clinici controllati, revisioni<br />
sistematiche delle evidenze comunque esistenti.”<br />
Chalmers I., 1993
• Rappresenta la prima fonte di consultazione se il<br />
“bisogno d’informazione” riguarda l’efficacia dei<br />
trattamenti<br />
Cochrane Library<br />
• Tuttavia:<br />
- il n° totale di revisioni sistematiche (RS) è<br />
ancora modesto (poco più di 1.800 ripetto alle<br />
30-35 mila previste)<br />
- la maggior parte di RS riguarda 5-6 specialità<br />
cliniche<br />
- molte RS non sono conclusive (aree grigie)<br />
GIMBE ®
GIMBE ®<br />
Cochrane Library<br />
Rappresenta la prima fonte di consultazione se<br />
il “bisogno d’informazione” riguarda l’efficacia<br />
dei trattamenti<br />
Nonostante sia la fonte di elezione dispone di<br />
un numero di revisioni sistematiche ancora<br />
limitato (circa 4200 vs 35000 previste)<br />
Molte RS in essa contenute riguardano un<br />
numero esiguo di specialità cliniche<br />
molte RS non sono conclusive (aree grigie)
GIMBE ®<br />
Cochrane Database of Systematic Reviews<br />
(CDRS)<br />
È il database principale:<br />
raccoglie le revisioni sistematiche realizzate dai<br />
gruppi di revisione Cochrane (circa 4200)<br />
raccoglie i protocolli di quelle in corso di<br />
realizzazione (circa 1900)<br />
abstracts delle revisioni e titoli dei protocolli sono<br />
disponibili gratuitamente on-line.
Contiene circa 12.000 abstract di revisioni<br />
sistematiche pubblicate in letteratura e valutate<br />
criticamente a cura del NHS Centre for Review and<br />
Dissemination.<br />
Accessibile gratuitamente on-line<br />
GIMBE ®<br />
Database of Abstract of Reviews of<br />
Effectiveness - (DARE)
E’ un registro creato dopo una ricerca manuale delle<br />
riviste pubblicate dal 1945 ad oggi per identificare<br />
tutti i RCTs pubblicati; include più di 608.000 RCTs<br />
(molti non indicizzati nelle banche dati tradizionali)<br />
GIMBE ®<br />
Cochrane Controlled Trial Register<br />
(CCTR)
GIMBE ®<br />
altre risorse<br />
The Cochrane Methodology Register (CMR)<br />
Health Technology Assessment Database<br />
NHS Economic Evaluation Database
www.evidencebasednursing.it<br />
GIMBE ®
BACKGROUND<br />
Cos’è il TIA o come<br />
si assiste il paziente<br />
con TIA<br />
GIMBE ®<br />
LG<br />
Mappa della ricerca<br />
QUESITO<br />
TESTO o<br />
E-BOOK!<br />
FOREGROUND - PICO<br />
E’ meglio posizionare il<br />
paziente con Braden
GIMBE ®<br />
Studi Primari<br />
QUESITO<br />
Mappa della ricerca<br />
Revisioni sistematiche<br />
E’ un trattamento? Trial randomizzto e controllato<br />
Ricerca una causa? Studio di coorte o Caso controllo<br />
Vuole conoscere una prognosi? Studio di coorte<br />
Vuole valutare un test Studio di sensibilità<br />
diagnostico? e specificità
GIMBE ®<br />
THE END<br />
GIMBE ®
GIMBE ®<br />
<strong>Evidence</strong> <strong>Based</strong> <strong>Practice</strong><br />
Gabriele Manzi<br />
Azienda U.S.L. di Bologna
GIMBE ®<br />
Cosa sono le evidenze<br />
scientifiche?<br />
Conoscenze che derivano dalle prove di efficacia,<br />
ossia dalle sperimentazioni cliniche.<br />
Esse permettono l’acquisizione di nuove<br />
informazioni partendo dal dato empirico derivante<br />
da esse.<br />
Non è evidenza ciò che è<br />
esplicito, ma ciò che è<br />
dimostrato.
GIMBE ®<br />
Obiettivi di un sistema sanitario<br />
impossibilitato a soddisfare tutte le<br />
domande di salute<br />
Garantire un livello omogeneo di assistenza su obiettivi<br />
prioritari di prevenzione, diagnosi, terapia, riabilitazione<br />
Utilizzare criteri scientifici, oggettivi, riproducibili per<br />
decidere come impiegare le risorse economiche.<br />
Cartabellotta, 1998
GIMBE ®<br />
Come è arrivata l’EBHC<br />
in Italia?<br />
•PSN 1998-2000<br />
•DLGs 229/99
GIMBE ®<br />
Il PSN 1998-2000<br />
Il Piano Sanitario Nazionale 1998-<br />
2000 definisce i livelli di assistenza<br />
alla luce di principi ispiratori del<br />
Servizio Sanitario Nazionale.
GIMBE ®<br />
Principi ispiratori del SSN<br />
Principio dell'efficacia e<br />
dell'appropriatezza degli<br />
interventi:<br />
le risorse devono essere indirizzate verso le<br />
prestazioni la cui efficacia é riconosciuta in<br />
base alle evidenze scientifiche e verso i<br />
soggetti che maggiormente ne possono trarre<br />
beneficio.
GIMBE ®<br />
Appropriatezza<br />
Appropriatezza clinica<br />
Misura in cui un particolare intervento è sia<br />
efficace sia indicato per la persona che lo<br />
riceve.<br />
- benefici > effetti negativi e disagi<br />
- benefici/danni > con = costi<br />
- è relativa solo alla fase decisionale
GIMBE ®<br />
Appropriatezza<br />
Appropriatezza organizzativa<br />
o generica<br />
Misura in cui un intervento viene erogato al<br />
livello più gradito all’utente e/o meno costoso<br />
(ad es. domicilio, ambulatorio, day-hospital,<br />
ricovero)<br />
PSN 1998-2000<br />
appropriatezza = efficacia
GIMBE ®<br />
Coordinato dall’Istituto Superiore di Sanità in<br />
collaborazione con l’ASL 6 di Livorno, l'Agenzia di sanità<br />
pubblica della regione Lazio, CeVEAS di Modena<br />
e il Centro Cochrane Italiano.<br />
http://www.snlg-iss.it/
GIMBE ®<br />
Linee Guida<br />
Raccomandazioni di comportamento clinico,<br />
prodotte attraverso un metodo sistematico di<br />
revisione della letteratura, che informano tutti gli<br />
attori di un sistema sanitario (professionisti,<br />
manager, utenti) sulle modalità più appropriate<br />
per la gestione di presentazioni cliniche e<br />
malattie.
GIMBE ®<br />
Contesto Locale<br />
Insieme delle variabili (strutturali, organizzative,<br />
tecnologiche, professionali) in grado di<br />
condizionare l’applicazione locale di singole<br />
raccomandazioni delle LG.
GIMBE ®<br />
Percorso Assistenziale*<br />
• Strumento finalizzato all’implementazione delle LG<br />
• In relazione al contesto locale il PA:<br />
- adatta le raccomandazioni delle LG<br />
- definisce:<br />
- procedure (how)<br />
- professionisti (who)<br />
- setting (where)<br />
- tempistiche (when)<br />
• In altri termini: PA= LG + CL<br />
* da preferire a “percorso diagnostico-terapeutico”, termine più riduttivo
GIMBE ®<br />
Processo (assistenziale)<br />
• Rappresenta l’unità elementare del PA (costituito<br />
da N processi)<br />
• In funzione del numero di strutture e di<br />
professionisti coinvolti nella sua erogazione il<br />
processo può essere:<br />
- molto semplice, talora sino ad identificarsi con<br />
la procedura (vedi)<br />
- estremamente complesso<br />
• L’appropriatezza dei processi è correlata al<br />
grado di aderenza alle raccomandazioni cliniche.
GIMBE ®<br />
Procedura (operativa)<br />
• Sequenza di azioni tecnico-operative attraverso cui il<br />
professionista eroga gli interventi assistenziali.<br />
• Rappresenta l’unità elementare del processo (costituito<br />
da N procedure)<br />
• Può essere molto semplice (cateterismo vescicale) o<br />
estremamente complessa (chirurgia dell’aorta<br />
addominale).<br />
• La conformità della procedura dovrebbe essere<br />
definita da standard di competence professionale<br />
(accreditamento?)<br />
• Sinomini: istruzione operativa
GIMBE ®<br />
A B C D<br />
Percorso assistenziale<br />
Processo<br />
Procedura operativa
GIMBE ®<br />
Protocollo<br />
• Può indicare, indifferentemente, un processo o una<br />
procedura.<br />
• Nella letteratura giuridica il termine protocollo viene<br />
interpretato come “vincolante” (mandatory) per i<br />
professionisti.<br />
• Questo termine, in disuso nella letteratura internazionale,<br />
dovrebbe essere limitato, anche per i potenziali rischi<br />
medico-legali.
GIMBE ®<br />
Linee Guida<br />
Basate sull’evidenza Non basate sull’evidenza
GIMBE ®<br />
Le non evidence based guide line erano diffuse<br />
soprattutto qualche anno fa, erano fatte in casa<br />
(senza l’ausilio di revisioni sistematiche) ed avevano<br />
come risultato quello di validare i comportamenti già<br />
in atto.
GIMBE ®<br />
Le evidence based guide line si caratterizzano per:<br />
la multidisciplinarietà multidisciplinariet del gruppo responsabile<br />
della produzione della linea guida<br />
la valutazione sistematica delle prove scientifiche<br />
disponibili<br />
formulate<br />
quale base per le raccomandazioni<br />
la classificazione delle raccomandazioni in base<br />
alla qualità delle prove scientifiche che le<br />
sostengono<br />
Grilli et al, Lancet 2000
GIMBE ®<br />
Requisiti per lo sviluppo e<br />
l’applicabilità di una EBGL<br />
• Deve dichiarare la qualità delle informazioni<br />
utilizzate (livello livello di evidenza) evidenza e<br />
l’importanza/rilevanza/fattibilità/priorità della loro<br />
implementazione (forza forza delle<br />
raccomandazioni).<br />
raccomandazioni<br />
• Deve essere prodotta attraverso un processo<br />
multidisciplinare (cittadini/pazienti): ciò migliora<br />
la qualità delle linee guida e favorisce la sua<br />
adozione nella pratica.
GIMBE ®<br />
Requisiti per lo sviluppo e<br />
l’applicabilità di una EBGL<br />
• Deve esplicitare le alternative di trattamento e<br />
i loro effetti sugli esiti.<br />
• Deve essere flessibile e adattabile alle<br />
mutevoli condizioni locali.<br />
• Nel produrre una linea guida dovrebbero essere<br />
esplicitati i possibili indicatori di monitoraggio<br />
utili a valutarne l’effettiva applicazione.
GIMBE ®<br />
Requisiti per lo sviluppo e<br />
l’applicabilità di una EBGL<br />
• Una linea guida dovrebbe essere aggiornata<br />
con regolarità regolarit per evitare che le<br />
raccomandazioni divengano obsolete.<br />
• Una linea guida deve essere chiara, chiara dotata di<br />
una struttura semplice e di un linguaggio<br />
comprensibile, esplicitando in modo<br />
inequivocabile i punti ritenuti fondamentali e le<br />
aree di incertezza.
GIMBE ®<br />
Technology Assessment<br />
Le tecnologie sanitarie sono l’insieme delle risorse<br />
materiali e delle conoscenze indispensabili per<br />
l’erogazione delle prestazioni sanitarie.<br />
La valutazione delle tecnologie sanitarie<br />
(technology assessment) consiste nella<br />
valutazione di benefici, rischi e costi (clinici,<br />
sociali, economici, di sistema) del trasferimento<br />
delle tecnologie sanitarie nella pratica clinica.
GIMBE ®<br />
Technology Assessment<br />
Si pone ad un livello di complessità superiore<br />
occupandosi non solo di aspetti clinici, ma anche<br />
organizzativi, gestionali, economici e sociali.<br />
Mira fornire ad amministratori e decisori della<br />
sanità le informazioni necessarie per fare scelte<br />
appropriate sul piano dell’efficienza allocativa.
GIMBE ®
GIMBE ®<br />
Chi produce linee guida?<br />
• Agenzie internazionali<br />
• Agenzie nazionali<br />
• Agenzie governative<br />
• Agenzie regionali<br />
• Aziende sanitarie
GIMBE ®<br />
Perché?<br />
variabilità degli interventi professionali;<br />
esigenza di confronto tra attori diversi con<br />
differenti punti di vista (amministratori, pazienti,<br />
operatori);<br />
crescente complessità ed aumentata insorgenza<br />
di obsolescenza delle tecnologie sanitarie;<br />
aumentate aspettative da parte della popolazione.
GIMBE ®<br />
Aspetti legali<br />
Le linee guida riassumono in modo sistematico<br />
le migliori modalità assistenziali, attualmente<br />
riconosciute, relative ad una patologia o<br />
condizione.<br />
Esse vengono assunte come “regole d’arte” e<br />
nelle controversie giudiziarie costituiscono il<br />
criterio per valutare la correttezza tecnica della<br />
condotta del professionista sanitario nella cura<br />
del paziente.
GIMBE ®<br />
GIMBE ®<br />
Aspetti legali<br />
La dottrina medico-legale, pur affermando che<br />
per valutare la condotta professionale dei<br />
professionisti si deve fare riferimento anche a<br />
questi documenti, nella stesura vigente<br />
sottolinea correttamente “il valore relativo” delle<br />
linee guida “per i singoli casi”.
GIMBE ®<br />
Aspetti legali<br />
Le linee guida, infatti, fanno riferimento a un<br />
paziente astratto, non a “quel particolare<br />
paziente” che il professionista deve in concreto<br />
curare, con la sua complessità clinica e la sua<br />
specificità patologica.
GIMBE ®<br />
Aspetti legali<br />
La diligenza deve essere valutata in relazione<br />
alle circostanze concrete nelle quali il<br />
professionista si è trovato a operare e, quindi, la<br />
giurisprudenza riconosce al sanitario pur sempre<br />
uno spazio di discrezionalità tecnica nella scelta<br />
del metodo di cura da proporre al singolo<br />
paziente, purché fondata correttamente su dati<br />
oggettivi riscontrati durante il processo di cura.
GIMBE ®<br />
Aspetti legali<br />
In definitiva il professionista nella sua pratica<br />
clinica deve confrontarsi con il contenuto di una<br />
linea guida che, se correttamente elaborata e<br />
aggiornata, può contenere le “regole dell’arte”<br />
astrattamente applicabili. Peraltro la<br />
responsabilità della scelta del trattamento da<br />
praticare compete al professionista che ha in<br />
cura il paziente e, quindi, spetta al sanitario<br />
verificare se nel caso di specie si deve seguire<br />
l’indicazione contenuta nella linea guida ovvero è<br />
opportuno discostarsene a ragion veduta.
GIMBE ®<br />
Aspetti legali<br />
Le linee guida non sono infatti vincolanti per<br />
legge e, quindi, non sussiste alcun obbligo di<br />
automatica applicazione.<br />
Le linee guida, se correttamente interpretate, non<br />
deresponsabilizzano quindi il professionista, ma<br />
rendono invece più evidente il suo dovere di<br />
motivare e documentare le scelte dei<br />
comportamenti di cura.
GIMBE ®<br />
Aspetti legali<br />
E’ opportuno infine ricordare che la<br />
responsabilità professionale presuppone<br />
l’accertamento non solo della colpa, ma anche<br />
della sussistenza del rapporto di causalità tra<br />
comportamento del sanitario ed evento dannoso<br />
per il paziente.
GIMBE ®
GIMBE ®<br />
Livello delle prove<br />
Il livello delle prove (LdP) indica che la<br />
raccomandazione è derivata da studi pianificati<br />
e condotti in modo tale da produrre informazioni<br />
valide e prive di errori sistematici.
GIMBE ®<br />
Livello delle prove<br />
Complessivamente, quindi, si può affermare che<br />
l’LdP dipende da:<br />
appropriatezza del disegno di studio utilizzato<br />
(qualità metodologica a priori);<br />
rigore e qualità di conduzione e analisi dello studio<br />
(controllo dell’errore sistematico);<br />
dimensione dell’effetto clinico/epidemiologico<br />
misurato (controllo dell’errore casuale);<br />
appropriatezza e rilevanza degli indicatori di esito<br />
utilizzati (rilevanza clinico-epidemiologica).
GIMBE ®<br />
Forza delle raccomandazioni<br />
La forza della raccomandazione (FdR) si<br />
riferisce alla probabilità che l’applicazione nella<br />
pratica di una raccomandazione determini un<br />
miglioramento dello stato di salute della<br />
popolazione.
GIMBE ®<br />
Forza delle raccomandazioni<br />
Livello delle evidenze<br />
Forza delle raccomandazioni
GIMBE ®
GIMBE ®
GIMBE ®<br />
Ceveas
GIMBE ®<br />
Ceveas
Più volte sono state prodotte per consenso,<br />
attraverso una riunione di un gruppo di esperti nel<br />
corso di un convegno per discutere e concordare<br />
quale sia il comportamento ottimale da tenere per<br />
affrontare un determinato problema.<br />
GIMBE ®<br />
Come nasce una LG
GIMBE ®<br />
Questo processo presenta molti limiti:<br />
non sempre l’opinione degli esperti riflette lo<br />
stato delle conoscenze mediche!<br />
l’analisi della letteratura scientifica potrebbe<br />
non essere eseguita in modo sistematico!<br />
le conclusioni a cui si arriva possono non<br />
essere valide da un punto di vista scientifico!
GIMBE ®<br />
Consenso informale<br />
Gli esperti si confrontano nel corso di una o più<br />
discussioni non strutturate e infine arrivano a un<br />
consenso sulle raccomandazioni.<br />
Questo tipo di consenso viene definito informale in<br />
quanto i criteri di scelta non sono fissati a priori e<br />
le raccomandazioni espresse possono riflettere<br />
l’opinione dei più esperti o di coloro che hanno<br />
maggiore autorevolezza o potere.<br />
E’ il metodo più semplice, pratico e utilizzato, ma è<br />
anche quello scientificamente meno valido.
GIMBE ®<br />
Consenso formale<br />
Il confronto in questo caso è più strutturato, in<br />
modo che tutte le posizioni espresse all’interno del<br />
gruppo possano essere rappresentate e discusse.<br />
Il metodo più noto è il Metodo” Delphi”: a tutti i<br />
partecipanti viene inviato un questionario con le<br />
domande principali sulle quali si vuole trovare un<br />
consenso.<br />
I partecipanti rispondono e si arriva via via a<br />
discutere le risposte-comportamenti più<br />
raccomandati.
GIMBE ®<br />
Metodo Rand<br />
Ideato dalla Rand Corporation negli anni Ottanta,<br />
prevede gruppi di 10-11 esperti che vengono chiamati<br />
a definire i criteri di utilizzo appropriato di una<br />
procedura o di un trattamento, avendo come<br />
riferimento non il paziente medio, ma specifiche<br />
categorie di pazienti.<br />
Il suo limite è che nonostante si combinino le opinioni<br />
degli esperti con le indicazioni della letteratura, la<br />
valutazione resta sempre soggettiva.<br />
E’ difficile coinvolgere più figure professionali, con<br />
diverso potere.
Prevede momenti di discussione e verifica delle<br />
informazioni disponibili sui diversi aspetti di una<br />
tecnologia sanitaria, in modo da definire lo stato<br />
dell’arte e produrre raccomandazioni per la pratica<br />
clinica.<br />
GIMBE ®<br />
Consensus Conference
GIMBE ®<br />
NICE<br />
National Institute of Clinical Excellence<br />
http://www.nice.org.uk<br />
Organizzazione creata dal governo inglese<br />
all’interno del suo servizio sanitario nazionale<br />
Valuta l’efficacia degli interventi medici,<br />
rappresentati da farmaci, dispositivi medici,<br />
procedure fisioterapiche e chirurgiche allo scopo<br />
di orientare una corretta utilizzazione delle<br />
risorse da parte del National Health Service<br />
inglese<br />
Produce linee guida cliniche e rapporti di<br />
valutazione tecnologica
GIMBE ®<br />
THE END<br />
GIMBE ®
1 Department of<br />
Gastroenterology, G B Pant<br />
Hospital, New Delhi, India<br />
2 Department of Hepatology,<br />
Institute of Liver & Biliary<br />
Sciences (ILBS), New Delhi,<br />
India<br />
Correspondence to<br />
Dr S K Sarin, Department of<br />
Gastroenterology, G B Pant<br />
Hospital, 201 Academic Block,<br />
New Delhi 110002, India;<br />
shivsarin@gmail.com<br />
Revised 1 February 2010<br />
Accepted 7 February 2010<br />
Endoscopic cyanoacrylate injection versus b-blocker<br />
for secondary prophylaxis of gastric variceal bleed:<br />
a randomised controlled trial<br />
Smruti Ranjan Mishra, 1 Barjesh Chander Sharma, 1 Ashish Kumar, 2<br />
Shiv Kumar Sarin 1,2<br />
ABSTRACT<br />
Background and aims Bleeding from gastric varices is<br />
often severe and difficult to manage. Endoscopic<br />
injection of gastric varices with cyanoacrylate is effective<br />
in prevention of rebleeding. The efficacy of b-blockers in<br />
secondary prophylaxis of gastric variceal bleed has not<br />
been well studied. A comparison of the efficacy of bblocker<br />
treatment and cyanoacrylate injection for the<br />
prevention of gastric variceal rebleeding was carried out.<br />
Methods Patients with gastro-oesophageal varices type<br />
2 (GOV2) with eradicated oesophageal varices or<br />
isolated gastric varices type 1 (IGV1) who had bled from<br />
gastric varices were randomised to cyanoacrylate<br />
injection (n¼33) or b-blocker treatment (n¼34).<br />
Baseline and follow-up upper gastrointestinal endoscopy<br />
and hepatic venous pressure gradient (HVPG)<br />
measurements were performed. Primary end points were<br />
gastric variceal rebleeding or death.<br />
Results The probability of gastric variceal rebleeding<br />
rate in the cyanoacrylate group was significantly lower<br />
than in the b-blocker group (15% vs 55%, p¼0.004) and<br />
the mortality rate was lower (3% vs 25%, p¼0.026)<br />
during a median follow-up of 26 months. The median<br />
baseline and follow-up HVPG in the cyanoacrylate group<br />
were 15 (10e23) and 17 (11e24) mm Hg (p¼0.001)<br />
and for the b-blocker group 14 (11e24) and 13<br />
(8e25) mm Hg (p¼0.003). While no patient showed<br />
reduction of HVPG in the cyanoacrylate group, in the bblocker<br />
group 12 of 28 (42%) patients were responders,<br />
of which 5 (41% of responders) bled. On multivariate<br />
analysis, treatment method, portal hypertensive<br />
gastropathy and size of the gastric varix >20 mm<br />
independently correlated with gastric variceal rebleeding.<br />
Gastric variceal rebleeding independently correlated with<br />
mortality.<br />
Conclusions Cyanoacrylate injection is more effective<br />
than b-blocker treatment for the prevention of gastric<br />
variceal rebleeding and improving survival.<br />
Clinical trial number NCT00888784.<br />
INTRODUCTION<br />
Gastric varices (GVs) are less common than oesophageal<br />
varices, occurring in w20% of patients<br />
with portal hypertension. 1 GVs bleed less<br />
frequently than oesophageal varices 1 ; however<br />
bleeding tends to be more severe, requires more<br />
transfusions and has a higher mortality rate than<br />
oesophageal variceal bleeding. 1e3 After control of<br />
acute bleeding, GVs have a high rebleeding rate<br />
(34e89%) and treatment options to prevent<br />
rebleeding are not optimised. 2 4 5 The frequency<br />
Significance of this study<br />
Stomach<br />
What is already known about this subject?<br />
< The efficacy of b-blockers in secondary prophylaxis<br />
of gastric variceal bleeding has not been<br />
well studied.<br />
< Endoscopic injection of cyanoacrylate has been<br />
proven to be effective in the prevention of<br />
gastric variceal rebleeding.<br />
< b-Blockers have been recommended empirically<br />
for prophylaxis of gastric variceal bleeding<br />
without proof.<br />
What are the new findings?<br />
< The probability of rebleeding from large gastrooesophageal<br />
varices type 2 (GOV2) or isolated<br />
gastric varices type 1 (IGV1) was significantly<br />
lower in the cyanoacrylate group (15%)<br />
compared with the b-blocker group (55%).<br />
< The majority of patients with such gastric<br />
varices have baseline HVPG >12 mm Hg.<br />
< Cyanoacrylate injection increases the hepatic<br />
venous pressure gradient (HVPG), and b-blocker<br />
decreases HVPG significantly on follow-up.<br />
< Mortality in patients treated with a b-blocker is<br />
higher than with cyanoacrylate injection.<br />
How might it impact on clinical practice in the<br />
foreseeable future?<br />
< Endoscopic injection of cyanoacrylate should be<br />
used to prevent rebleeding from large GOV2 and<br />
IGV1 and improve survival.<br />
< b-Blockers are not effective in prevention of<br />
rebleeding from such gastric varices, although<br />
they decrease HVPG in these patients.<br />
and severity of bleeding from GVs depends on their<br />
location (figure 1). GVs could be associated with<br />
oesophageal varices (gastro-oesophageal varices<br />
type 1 along the lesser curve, or type 2 (GOV2),<br />
along the fundus) or are present in isolation<br />
(isolated gastric varix type 1 (IGV1), in the fundus<br />
or at ectopic sites in the stomach or the first part of<br />
the duodenum (isolated gastric varix type 2)). 1<br />
b-Blockers have been reported to reduce the risk<br />
of rebleeding of oesophageal varices by w40% and<br />
risk of death by 20%. 6e11 A small open-label trial of<br />
b-blocker and nitrate treatment in patients with<br />
GVs reported no significant benefit for rebleeding or<br />
survival, but there was a trend towards lower<br />
rebleeding. 12 Endoscopic injection of cyanoacrylate<br />
Gut 2010;59:729e735. doi:10.1136/gut.2009.192039 729
Stomach<br />
Figure 1 Classification of gastric varices.<br />
has been proven to be effective in the prevention of GV<br />
rebleeding. 13e17 However, cyanoacrylate injection is associated<br />
with a risk of cerebral or pulmonary embolism and damage to<br />
the endoscope. 18<br />
Results on the long-term efficacy of gastric variceal obturation<br />
with cyanoacrylate injection are variable, with eradication rates<br />
between 50% and 100% and a rebleeding rate of 23e50%, with<br />
the majority occurring in the first year. 13 16 19e21 Due to the high<br />
rate of primary haemostasis and lower rebleeding rate, GV<br />
obturation with cyanoacrylate injection is used as the first-line<br />
treatment for bleeding GVs and secondary prophylaxis of GV<br />
bleed.<br />
For patients who have bled from IGV1 or GOV2, N-butylcyanoacrylate,<br />
transjugular intrahepatic portosystemic shunt<br />
(TIPS) or b-blockers have been recommended. 22 Endoscopic<br />
injection of thrombin has also been tried for secondary<br />
prophylaxis of bleeding from GVs. 23e26 b-Blockers have been<br />
recommended empirically for GVs since they have been found to<br />
be quite effective in patients who have bled from oesophageal<br />
varices. However, there is no randomised controlled trial available<br />
comparing b-blocker treatment with endoscopic cyanoacrylate<br />
injection for prevention of rebleeding from GVs. We conducted<br />
a randomised controlled trial to study the efficacy of endoscopic<br />
cyanoacrylate injection versus b-blockers in the prevention of<br />
gastric variceal (GOV2 or IGV1) rebleeding and improvement in<br />
survival. We also investigated the predictors of rebleeding and<br />
mortality in patients who had previously bled from GVs.<br />
Patients and methods<br />
Patients with portal hypertension with upper gastrointestinal<br />
bleed were assessed. All consecutive patients with cirrhosis with<br />
GVs (GOV2 with eradicated oesophageal varices or IGV1)<br />
admitted to our hospital from August 2006 to March 2009 were<br />
enrolled. The study was approved by our institutional review<br />
board, and written informed consent was obtained from all<br />
patients. Parents gave the written consent for children. Patients<br />
who had bled from GOV2 or IGV1 were included. The exclusion<br />
criteria were non-cirrhotic portal hypertension, presence of<br />
oesophageal varices, contraindications to b-blockers and cyanoacrylate<br />
injection, patients already on b-blockers, past history of<br />
cyanoacrylate injection or sclerotherapy for GVs or GV ligation,<br />
TIPS, balloon-occluded retrograde transvenous obliteration<br />
(BRTO), balloon-occluded endoscopic injection sclerotherapy,<br />
shunt operation, undetermined origin of bleeding, hepatic<br />
encephalopathy grade III/IV, hepatorenal syndrome, hepatocellular<br />
carcinoma, presence of deep jaundice (serum bilirubin<br />
>10 mg/dl), cardiorespiratory failure, age >75 years, pregnancy<br />
or patients who did not give informed consent.<br />
After assessing eligibility with initial endoscopy and subsequently<br />
obtaining informed consent patients were randomised,<br />
using a sealed envelope technique, to receive cyanoacrylate<br />
injection (Nectacryl, Nectar Laboratories, Medak, India) or bblocker<br />
(propranolol). The allocation sequence remained with<br />
the statistician and the sequence remained concealed from the<br />
investigators until the intervention was assigned. The doctors<br />
who evaluated the outcomes were blinded to group assignment.<br />
According to the Baveno IV consensus on portal hypertension, 22<br />
secondary prophylaxis starts from the sixth day of acute variceal<br />
bleed. For patients presenting with acute GV bleeding, an<br />
emergency endoscopy was done and, if the bleeding was found<br />
to be from GOV2 or IGV1, one cyanoacrylate injection was<br />
given to control acute GV haemorrhage (not with the intention<br />
of obliterating the GV). The patients were randomised and the<br />
follow-up started from day 6 after occurrence of acute bleeding.<br />
None of the patients presenting with acute GV bleeding received<br />
b-blocker or endoscopic treatment for secondary prophylaxis<br />
from day 0 till day 6. Patients with a previous bleed were<br />
randomised after control endoscopy. For patients randomised to<br />
the propranolol group, control endoscopy was completed and<br />
propranolol was started on the same day. For patients randomised<br />
to the cyanoacrylate group, a second endoscopy with<br />
cyanoacrylate injection was performed on the same day. In<br />
patients with a history of past bleeding, the follow-up started<br />
immediately after randomisation. The follow-up period was<br />
terminated at 3 months after enrolment of the last patient.<br />
Upper gastrointestinal endoscopy was done to determine the<br />
variceal status at baseline and repeated at 3 month intervals or<br />
during rebleeding. The size of the GV, recurrence of oesophageal<br />
varices and portal hypertensive gastropathy (PHG) were<br />
recorded. An attempt was made to localise the source of bleeding<br />
at the time of emergency endoscopy. The size of the GV was<br />
calculated by a zebra guide wire with markings made at 5 mm<br />
intervals, and we classified the fundal varix as small (20 mm). The colour of the GV<br />
was observed as red or blue. The recent signs of haemorrhage<br />
over the GV were the presence of a clot or blackish spot localised<br />
over the GV. 1 The presence or absence of oesophageal varices and<br />
PHG were also evaluated. Concurrence of two independent<br />
observers was required before characterising the type of GV and<br />
its size. Rebleeding from GVs was managed with a cyanoacrylate<br />
injection in the b-blocker group and TIPS or surgery in the<br />
cyanoacrylate group.<br />
The primary end points of the study were rebleeding from<br />
GVs or death. The actuarial probability of rebleeding from GVs<br />
and mortality were calculated. Secondary end points were<br />
increase or decrease in the size of GVs, appearance of new<br />
oesophageal varices and appearance or worsening of PHG and<br />
complications.<br />
The diagnosis of cirrhosis was based on clinical, biochemical,<br />
radiological and histological findings. Ultrasonography of the<br />
abdomen with Doppler of splenoportal axis, CT angiography or<br />
magnetic resonance (MR) angiography was done to diagnose<br />
730 Gut 2010;59:729e735. doi:10.1136/gut.2009.192039
cirrhosis and assess spontaneous shunts. Model for end-stage<br />
liver disease (MELD) and ChildeTurcotteePugh (CTP) scores<br />
were calculated at baseline and serial intervals.<br />
Technique of cyanoacrylate injection<br />
Endoscopic injection was performed intravariceally using<br />
a therapeutic endoscope and a transparent Teflon injector, with<br />
a6e8 mm long, 21-gauge needle, with N-butyl-2-cyanoacrylate.<br />
The cyanoacrylate was injected without dilution with lipiodol.<br />
The maximum amount of cyanoacrylate injected per site was<br />
2 ml, and the total amount of cyanoacrylate required to obliterate<br />
the GVs completely was recorded. An attempt was made<br />
to obturate the GVs completely at one session by injecting<br />
cyanoacrylate at multiple sites. If a second session was required,<br />
it was done within a week of the initial session. The injected GV<br />
was palpated using the hub of the injector with the needle<br />
retracted to look for solidification and obliteration of the GV. If<br />
the GV was not completely obturated, cyanoacrylate was reinjected<br />
till the whole GV became solidified.<br />
b-Blocker treatment<br />
Propranolol was started at a dose of 20 mg twice daily. The dose<br />
was increased every alternate day by 20 mg to achieve target<br />
a heart rate of 55/min or to the maximal dose of 360 mg/day if<br />
the medication was well tolerated and the systolic blood pressure<br />
was >90 mm Hg. On the occurrence of intolerable adverse<br />
effects, systolic blood pressure
Stomach<br />
treatment. Upper gastrointestinal endoscopy performed after<br />
a median period of 7 (4e15) days showed maroon-black spots<br />
(n¼26), a nipple (n¼9) on GVs and only large GVs (n¼14)<br />
without other obvious source of bleeding.<br />
Baseline characteristics of both groups of patients were<br />
comparable (table 1). The median follow-up period was 26<br />
(range 3e34) months in both the groups. The most common<br />
aetiology of cirrhosis was alcohol or cryptogenic (table 1). Four<br />
patients in the b-blocker and six patients in the cyanoacrylate<br />
group had IGV1; the rest of the patients had GOV2. The size,<br />
colour of GVs and PHG between the two groups were similar<br />
(table 1). MR portovenography and Doppler ultrasound<br />
demonstrated spontaneous lienorenal shunt in the cyanoacrylate<br />
group (n¼8) and in the b-blocker group (n¼11).<br />
Gastric variceal obturation<br />
Endoscopic intervention could be performed with 100% technical<br />
success. Complete obturation of GVs was achieved in all.<br />
The mean number of sessions required to achieve obliteration<br />
was 1.760.4 (range 1e2). The mean volume of cyanoacrylate<br />
required was 6.061.7 (range 3e9) ml. Mean time to obturation<br />
was 2.060.6 (range 1e3) days.<br />
b-Blocker treatment<br />
All patients were compliant to b-blocker treatment. The mean<br />
daily dose was 160 (range 80e320) mg. The median time<br />
interval to achieve the desired heart rate was 15 (range 5e20)<br />
days, and during this period no patient bled from GVs.<br />
Gastric variceal rebleeding<br />
Over a median follow-up period of 26 (3e34) months, in the<br />
cyanoacrylate group 3 (9%) (GOV2 (n¼2), IGV1 (n¼1)) patients<br />
bled, in contrast to 15 (44%) (GOV2 (n¼12), IGV1 (n¼3)) in the<br />
b-blocker group. The probability of GV rebleeding was significantly<br />
lower in the cyanoacrylate group (15%) compared with<br />
Table 1 Baseline characteristics of study group patients<br />
the b-blocker group (55%) (p¼0.004, log rank 8.466, figure 3A).<br />
The difference was also significant in the frequency of bleeding<br />
over a median follow-up period of 26 months from GOV2<br />
between the two groups (p¼0.005) (table 2). Of 34 patients in<br />
the b-blocker group 15 had rebleed, and cyanoacrylate injection<br />
was used to control rebleeding in 13 patients. In two patients,<br />
bleeding from GVs was torrential and cyanoacrylate injection<br />
could not be performed, and they were subjected to surgery. Of<br />
33 patients in the cyanoacrylate group, two patients had<br />
a rebleed and were managed by surgery.<br />
Size of gastric varix<br />
Over a median follow-up period of 26 (3e34) months in the<br />
cyanoacrylate group all patients had a decrease in GV size<br />
(table 2) and the median size of GVs decreased from w25<br />
(10e35) to w5 (0e10) mm (p
Figure 3 Probability of freedom from gastric variceal rebleeding (A)<br />
and survival (B) in the cyanoacrylate and b-blocker group.<br />
patient the hepatic vein could not be cannulated). Follow-up<br />
HVPG was measured in 23 patients in the cyanoacrylate group<br />
(three patients refused HVPG measurement and in one patient<br />
the hepatic vein could not be cannulated) and in 28 patients in<br />
the b-blocker group. Median baseline HVPG was 15 (10e23)<br />
mm Hg and follow-up HVPG was 17 (11e24) mm Hg in the<br />
cyanoacrylate group. The increase in HVPG on follow-up in the<br />
cyanoacrylate group was significant (p¼0.001). The median<br />
baseline HVPG was 14 (11e24) mm Hg and follow-up HVPG<br />
was 13 (8e25) mm Hg in the b-blocker group. The decrease in<br />
Table 2 Results of treatment in the cyanoacrylate and b-blocker groups<br />
HVPG on follow-up in the b-blocker group was significant<br />
(p¼0.003). In the cyanoacrylate group, 22 of 27 (81%) patients<br />
had HVPG >12 mm Hg at baseline and 22 of 23 (91%) patients<br />
had HVPG >12 mm Hg on follow-up. In the b-blocker group, 24<br />
of 28 (85%) patients had HVPG >12 mm Hg at baseline and 18<br />
of 28 (64%) patients had HVPG >12 mm Hg on follow-up.<br />
Response to treatment and rebleeding<br />
In the cyanoacrylate group, none of the patients responded to<br />
treatment in the form of reduction in HVPG. In the b-blocker<br />
group, 12 of the 28 (42%) patients were responders. However, 5<br />
(41%) responders bled during follow-up. Of the non-responders,<br />
2 of 23 (8%) patients in the cyanoacrylate group and 8 of 16<br />
(50%) patients in the b-blocker group bled. In responders, the<br />
median baseline HVPG was 16 (12e22) mm Hg and the followup<br />
HVPG was 12 (8e16) mm Hg. A >20% reduction in HVPG<br />
was achieved in 12 of 28 (42%) patients in the b-blocker group.<br />
In non-responders in the b-blocker group, the median baseline<br />
HVPG was 14 (11e24) mm Hg and the follow-up HVPG was<br />
13.5 (10e25) mm Hg. Of the responders who bled, one had<br />
IGV1 and the other four had GOV2. Those responders who did<br />
not bleed had a mean decrease in HVPG from baseline of 30% in<br />
comparison with a 22% decrease in those who bled. In patients<br />
with IGV1, the baseline median HVPG was 13 (11e17) mm Hg<br />
and in patients with GOV2 the baseline median HVPG was 14<br />
(10e24) mm Hg.<br />
Since all the patients were bleeders, it was interesting to note<br />
that patients with spontaneous shunt (n¼21) at baseline had<br />
a lower median HVPG (13 (10e15) mm Hg) than patients<br />
without spontaneous shunt (n¼43) (18 (13e24) mm Hg<br />
(p¼0.001)). Thus, the HVPG levels which predict the likelihood<br />
of rebleeding in patients with or without shunt are 13 and<br />
18 mm Hg, respectively. In patients with spontaneous shunt, 6<br />
of 21 (28%) patients had a HVPG value of 12 mm<br />
Hg. Overall, 20% of patients who bled had a HVPG
Stomach<br />
cyanoacrylate and 2 (6%) patients in the b-blocker group<br />
developed spontaneous bacterial peritonitis, and improved on<br />
treatment (table 2). Four patients in the b-blocker group developed<br />
headache and generalised weakness which was controlled<br />
with dose reduction, and after 2e3 weeks the desired dose was<br />
achieved. No serious adverse effects were noticed which required<br />
stoppage of b-blocker.<br />
Mortality<br />
Over a median follow-up period of 26 (3e34) months, a significant<br />
difference in the overall mortality was observed between the<br />
cyanoacrylate (n¼1, 3%) and the b-blocker (n¼8, 25%) group<br />
(p¼0.016, log rank¼5.808, figure 3B). Of 15 patients with<br />
rebleeding in the b-blocker group, treated with cyanoacrylate<br />
injection, 6 (19%) patients died in comparison with none in three<br />
of 33 patients in the cyanoacrylate group (p¼0.024) who were<br />
managed with surgery at the time of rebleeding. In the b-blocker<br />
group, one patient died of hepatic encephalopathy and one patient<br />
died of spontaneous bacterial peritonitis and hepatorenal<br />
syndrome. In the cyanoacrylate group, one patient died of hepatic<br />
encephalopathy. The cumulative 2-year survival rate was 90% in<br />
the cyanoacrylate group and 52% in the b-blocker group. In the<br />
b-blocker group, only one patient died among responders<br />
compared with seven patients among non-responders (p¼0.077).<br />
Predictors of GV rebleed and mortality<br />
On univariate analysis, the variables which influenced GV<br />
rebleeding were size of the GV >20 mm, a red or black spot over<br />
the GV, blue colour of the GV, presence of PHG, international<br />
normalised ratio (INR) $1.6, serum creatinine >1 mg/dl, CTP<br />
score $9, MELD score $17 and the treatment method. On<br />
multivariate analysis, the treatment method (p¼0.006), PHG<br />
(p¼0.029) and size of the GV >20 mm (p¼0.002) independently<br />
correlated with GV rebleeding. Variables which influence<br />
survival on univariate analysis included GV rebleeding, presence<br />
of PHG, CTP $9, MELD score $17 and the treatment method.<br />
On multivariate analysis, GV rebleeding (p¼0.003) independently<br />
correlated with mortality.<br />
DISCUSSION<br />
The results of this large prospective randomised controlled<br />
clinical trial comparing the efficacy of cyanoacrylate and<br />
b-blocker treatmjent clearly demonstrate that endoscopic injection<br />
of cyanoacrylate is significantly more effective than bblocker<br />
treatment for the prevention of rebleeding from GVs.<br />
Small studies have reported that drug treatment is effective in<br />
the prevention of GV rebleeding after successful endoscopic<br />
injection of the bleeding varix with tissue adhesives. 12 28 A small<br />
open-label trial of b-blocker and nitrate treatment reported no<br />
significant benefit in terms of risk of rebleeding or survival. 12<br />
This study had several limitations such as a small sample size,<br />
retrospective analysis, fixed and low doses of drug and lack of<br />
haemodynamic monitoring. In another study, Evrard et al<br />
randomised patients to receive 160 mg/day of propranolol<br />
(n¼20) or histoacryl injection (n¼21) for secondary prophylaxis<br />
of gastro-oesophageal variceal bleed. 28 The rebleeding and<br />
mortality rates were similar in the b-blocker and endoscopic<br />
treatment groups, with a higher complication rate in the latter<br />
(10% vs 47%). This study had limitations of early termination<br />
due to increased complications in the histoacryl arm, no<br />
haemodynamic monitoring and inclusion of patients with coexisting<br />
oesophageal varices. In fact, all patients had oesophageal<br />
varices, and 17 had GVs (12 with GOV1 and 5 with GOV2).<br />
The median baseline HVPG was 14.5 (10e24) mm Hg. Of 55<br />
patients with bleeding from gastric varices, 16% had baseline<br />
HVPG
lipiodol use, limiting the total volume per injection and by<br />
proper monitoring, no embolic complication was observed in our<br />
study population. Dilution of cyanoacrylate with lipiodol delays<br />
solidification by 15e20 s, thus increasing the chances of distal<br />
embolisation. In the undiluted form, it solidifies within 5e7 s,<br />
and thus the chances of distal embolisation become almost<br />
negligible. However, with undiluted cyanoacrylate injection,<br />
there is a risk of needle impaction in GVs at the time of<br />
injection. 39<br />
b-Blocker treatment was well tolerated and none of our<br />
patients required withdrawal of treatment. In the cyanoacrylate<br />
group, 21% of patients had appearance of new oesophageal<br />
varices in comparison with 11% in the b-blocker group, although<br />
none of the patients bled from oesophageal varices. The<br />
frequency of PHG in both the groups was similar (24% vs 21%).<br />
Survival in the cyanoacrylate group was better because of<br />
a low frequency of rebleeding compared with the b-blocker<br />
group. In both the groups, differences in mortality were due to<br />
rebleed-related deaths. However, mortality due to other causes<br />
(not rebleed related) was similar in both the groups. More<br />
favourable survival in our patients could be due to close followup<br />
during the study period and the fact that w50% of the<br />
patients with cirrhosis in both the groups were Child A and B.<br />
The stronger aspects of our trial are that it was a randomised<br />
controlled study and had a large sample size, a longer follow-up<br />
period and a minimal drop-out rate. The weaker aspect of this<br />
study is inclusion of only a selective patient group with IGV1<br />
and GOV2 types of GVs. The applicability of the present study<br />
is related only to patients with bleeding GVs of GOV2 and IGV1<br />
types. GVs of GOV2 and IGV1 types are more common, and<br />
associated with more frequent and more severe bleeds with<br />
higher mortality rates as compared with other types of gastric<br />
varices. 1<br />
In conclusion, the results of our study clearly demonstrate<br />
that cyanoacrylate injection is more effective in the prevention<br />
of rebleeding from GVs and improving patient survival as<br />
compared with b-blocker treatment. Propranolol is not effective<br />
in preventing gastric variceal rebleeding despite reduction in<br />
HVPG.<br />
Competing interests None.<br />
Patient consent Obtained.<br />
Ethics approval This study was conducted with the approval of the MAMC Ethical<br />
Committee, New Delhi.<br />
Provenance and peer review Not commissioned; externally peer reviewed.<br />
REFERENCES<br />
1. Sarin SK, Lahoti D, Saxena SP, et al. Prevalence, classification and natural history of<br />
gastric varices: a long-term follow-up study in 568 portal hypertension patients.<br />
Hepatology 1992;16:1343e9.<br />
2. Trudeau W, Prindiville T. Endoscopic injection sclerosis in bleeding gastric varices.<br />
Gastrointest Endosc 1986;32:264e8.<br />
3. Thakeb F, Salem SA, Abdallah M, et al. Endoscopic diagnosis of gastric varices.<br />
Endoscopy 1994;26:287e91.<br />
4. Bretagne JF, Dudicourt JC, Morisot D, et al. Is endoscopic variceal sclerotherapy<br />
effective for the treatment of gastric varices? [abstract]. Dig Dis Sci 1986;31:505S.<br />
5. Sarin SK. Long-term follow-up of gastric variceal sclerotherapy: an eleven-year<br />
experience. Gastrointest Endosc 1997;46:8e14.<br />
6. Lebrec D. Pharmacological treatment of portal hypertension: hemodynamic effects<br />
and prevention of bleeding. Pharmacol Ther 1994;61:65e107.<br />
7. Hayes PC, Davis JM, Lewis JA, et al. Meta-analysis of value of propranolol in<br />
prevention of variceal haemorrhage. Lancet 1990;336:153e6.<br />
8. Lin HC, Soubrane O, Lebrec O. Prevention of portal hypertension and portosystemic<br />
shunts by early chronic administration of clonidine in conscious portal vein-stenosed<br />
rats. Hepatology 1991;14:325e30.<br />
9. Sarin SK, Groszmann RJ, Mosca PG, et al. Propranolol ameliorates the development<br />
of portal-systemic shunting in a chronic murine schistosomiasis model of portal<br />
hypertension. J Clin Invest 1991;87:1032e6.<br />
Stomach<br />
10. Ideo G, Bellati G, Fesce E, et al. Nadolol can prevent the first gastrointestinal<br />
bleeding in cirrhotics: a prospective, randomized study. Hepatology 1988;8:6e9.<br />
11. The Italian Multicenter Project for Propranolol in Prevention of Bleeding.<br />
Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients.<br />
Final report of a multicenter randomized trial. J Hepatol 1989;9:75e83.<br />
12. Wu CY, Yeh HZ, Chen GH. Pharmacologic efficacy in gastric variceal<br />
rebleeding and survival: including multivariate analysis. J Clin Gastroenterol<br />
2002;35:127e32.<br />
13. Lo GH, Lai KH, Cheng JS, et al. A prospective, randomized trial of butyl<br />
cyanoacrylate injection versus band ligation in the management of bleeding gastric<br />
varices. Hepatology 2001;33:1060e4.<br />
14. Soehendra N, Nam VC, Grimm H, et al. Endoscopic obliteration of large<br />
esophagogastric varices with bucrylate. Endoscopy 1986;18:25e6.<br />
15. Ramond MJ, Valla D, Mosnier JF, et al. Successful endoscopic obliteration of<br />
gastric varices with butyl cyanoacrylate. Hepatology 1989;10:488e93.<br />
16. Huang YH, Yeh HZ, Chen GH, et al. Endoscopic treatment of bleeding gastric varices<br />
by N-butyl-2-cyanoacrylate (Histoacryl) injection: long-term efficacy and safety.<br />
Gastrointest Endosc 2000;52:160e7.<br />
17. Binmoeller KF, Soehendra N. “Superglue”: the answer to variceal bleeding and<br />
fundal varices? Endoscopy 1995;27:392e6.<br />
18. Ryan BM, Stockbrugger RW, Ryan JM. A pathophysiologic, gastroenterologic, and<br />
radiologic approach to the management of gastric varices. Gastroenterology<br />
2004;126:1175e89.<br />
19. Sarin SK, Jain AK, Jain M, et al. A randomized controlled trial of cyanoacrylate<br />
versus alcohol injection in patients with isolated fundic varices. Am J Gastroenterol<br />
2002;97:1010e15.<br />
20. Akahoshi T, Hashizume M, Shimabukuro R, et al. Long-term results of endoscopic<br />
histoacryl injection sclerotherapy for gastric variceal bleeding: a 10-year experience.<br />
Surgery 2002;131:S176e81.<br />
21. Kim JW, Baik SK, Kim KH, et al. Effect of endoscopic sclerotherapy using N-butyl-<br />
2-cyanoacrylate in patients with gastric variceal bleeding. Korean J Hepatol<br />
2006;12:394e403.<br />
22. de Franchis R. Evolving consensus in portal hypertension report of the Baveno<br />
IV consensus workshop on methodology of diagnosis and therapy in portal<br />
hypertension. J Hepatol 2005;43:167e76.<br />
23. Ramesh J, Limdi JK, Sharma V, et al. The use of thrombin injections in the<br />
management of bleeding gastric varices: a single center experience. Gastrointest<br />
Endosc 2008;68:877e82.<br />
24. Yang WL, Tripathi D, Therapondos G, et al. Endoscopic use of human thrombin in<br />
bleeding gastric varices. Am J Gastroenterol 2002;97:1381e5.<br />
25. Datta D, Vlavianos P, Alisa A, et al. Use of fibrin glue (beriplast) in the management<br />
of bleeding gastric varices. Endoscopy 2003;35:675e8.<br />
26. Tripathi D, Hayes PC. Endoscopic therapy for bleeding gastric varices: to clot or<br />
glue? Gastrointest Endosc 2008;68:883e6.<br />
27. Wadhawan M, Dubey S, Sharma BC, et al. Hepatic venous pressure gradient in<br />
cirrhosis: correlation with the size of varices, bleeding, ascites, and Child’s status.<br />
Dig Dis Sci 2006;51:2264e9.<br />
28. Evrard S, Dumonceau JM, Delhaye M, et al. Endoscopic histoacryl obliteration vs.<br />
propranolol in the prevention of esophagogastric variceal rebleeding: a randomized<br />
trial. Endoscopy 2003;35:729e35.<br />
29. Tripathi D, Therapondos G, Jackson E, et al. The role of the transjugular intrahepatic<br />
portosystemic stent shunt (TIPSS) in the management of bleeding gastric varices:<br />
clinical and haemodynamic correlations. Gut 2002;51:270e4.<br />
30. Watanabe K, Kimura K, Matsutani S, et al. Portal hemodynamics in patients with<br />
gastric varices. A study in 230 patients with esophageal and/or gastric varices using<br />
portal vein catheterization. Gastroenterology 1988;95:434e40.<br />
31. Matsumoto A, Hamamoto N, Nomura T, et al. Balloon-occluded retrograde<br />
transvenous obliteration of high-risk gastric fundal varices. Am J Gastroenterol<br />
1999;94:643e9.<br />
32. Hong CH, Kim HJ, Park JH. Treatment of patients with gastric variceal hemorrhage:<br />
endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occluded retrograde<br />
transvenous obliteration. J Gastroenterol Hepatol 2009;24:372e8.<br />
33. Lo GH, Liang HL, Chen WC, et al. A prospective, randomized controlled trial of<br />
transjugular intrahepatic portosystemic shunt vs. cyanoacrylate injection in the<br />
prevention of gastric variceal rebleeding. Endoscopy 2007;39:679e85.<br />
34. Marques P, Maluf-Filho F, Kumar A, et al. Long-term outcomes of acute gastric<br />
variceal bleeding in 48 patients following treatment with cyanoacrylate. Dig Dis Sci<br />
2008;53:544e50.<br />
35. Tripathi D, Ferguson JW, Therapondos G, et al. Review article: recent advances<br />
in the management of bleeding gastric varices. Aliment Pharmacol Ther<br />
2006;24:1e17.<br />
36. Tan PC, Hou MC, Lin HC, et al. A randomized trial of endoscopic treatment of acute<br />
gastric variceal hemorrhage: N-butyl-2-cyanoacrylate injection versus band ligation.<br />
Hepatology 2006;43:690e7.<br />
37. Hwang SS, Kim HH, Park SH, et al. N-butyl-2-cyanoacrylate pulmonary embolism<br />
after endoscopic injection sclerotherapy for gastric variceal bleeding. J Comput Assist<br />
Tomogr 2001;25:16e22.<br />
38. Yoshida H, Onda M, Tajiri T, et al. Endoscopic findings of bleeding esophagogastric<br />
varices. Hepatogastroenterology 2002;49:1287e9.<br />
39. Bhasin DK, Sharma BC, Prasad H, et al. Endoscopic removal of sclerotherapy needle<br />
from gastric varix after N-butyl-2-cyanoacrylate injection. Gastrointest Endosc<br />
2000;51:497e8.<br />
Gut 2010;59:729e735. doi:10.1136/gut.2009.192039 735
Stretching to prevent or reduce muscle soreness after<br />
exercise (Review)<br />
Herbert RD, de Noronha M<br />
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library<br />
2008, Issue 4<br />
http://www.thecochranelibrary.com<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
T A B L E O F C O N T E N T S<br />
HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1<br />
ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1<br />
PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2<br />
BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2<br />
OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3<br />
METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3<br />
RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5<br />
DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7<br />
AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8<br />
ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8<br />
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9<br />
CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11<br />
DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19<br />
Analysis 1.1. Comparison 1 Pre-exercise stretching, Outcome 1 Soreness on day 0.5 (assessed 6-17 hours post-exercise). 20<br />
Analysis 1.2. Comparison 1 Pre-exercise stretching, Outcome 2 Soreness on day 1 (assessed 18-29 hours post-exercise). 21<br />
Analysis 1.3. Comparison 1 Pre-exercise stretching, Outcome 3 Soreness on day 1.5 (assessed 30-41 hours post-exercise). 21<br />
Analysis 1.4. Comparison 1 Pre-exercise stretching, Outcome 4 Soreness on day 2 (assessed 42-53 hours post-exercise). 22<br />
Analysis 1.5. Comparison 1 Pre-exercise stretching, Outcome 5 Soreness on day 2.5 (assessed 54-65 hours post-exercise). 22<br />
Analysis 1.6. Comparison 1 Pre-exercise stretching, Outcome 6 Soreness on day 3 (assessed 66-77 hours post-exercise). 23<br />
Analysis 2.1. Comparison 2 Post-exercise stretching, Outcome 1 Soreness on day 0.5 (assessed 6-17 hours post-exercise). 23<br />
Analysis 2.2. Comparison 2 Post-exercise stretching, Outcome 2 Soreness on day 1 (assessed 18-29 hours post-exercise). 24<br />
Analysis 2.3. Comparison 2 Post-exercise stretching, Outcome 3 Soreness on day 1.5 (assessed 30-41 hours post-exercise). 24<br />
Analysis 2.4. Comparison 2 Post-exercise stretching, Outcome 4 Soreness on day 2 (assessed 42-53 hours post-exercise). 25<br />
Analysis 2.5. Comparison 2 Post-exercise stretching, Outcome 5 Soreness on day 2.5 (assessed 54-65 hours post-exercise). 25<br />
Analysis 2.6. Comparison 2 Post-exercise stretching, Outcome 6 Soreness on day 3 (assessed 66-77 hours post-exercise).<br />
Analysis 3.1. Comparison 3 Either pre- or post-exercise stretching, Outcome 1 Soreness on day 0.5 (assessed 6-17 hours<br />
26<br />
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26<br />
Analysis 3.2. Comparison 3 Either pre- or post-exercise stretching, Outcome 2 Soreness on day 1 (assessed 18-29 hours<br />
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27<br />
Analysis 3.3. Comparison 3 Either pre- or post-exercise stretching, Outcome 3 Soreness on day 1.5 (assessed 30-41 hours<br />
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27<br />
Analysis 3.4. Comparison 3 Either pre- or post-exercise stretching, Outcome 4 Soreness on day 2 (assessed 42-53 hours<br />
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28<br />
Analysis 3.5. Comparison 3 Either pre- or post-exercise stretching, Outcome 5 Soreness on day 2.5 (assessed 54-65 hours<br />
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29<br />
Analysis 3.6. Comparison 3 Either pre- or post-exercise stretching, Outcome 6 Soreness on day 3 (assessed 66-77 hours<br />
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29<br />
APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29<br />
WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30<br />
HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31<br />
CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31<br />
DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31<br />
SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31<br />
INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
i
[Intervention Review]<br />
Stretching to prevent or reduce muscle soreness after<br />
exercise<br />
Robert D Herbert 1 , Marcos de Noronha 2<br />
1 The George Institute for International Health, Camperdown, Australia. 2 School of Physiotherapy, University of Sydney, Lidcombe,<br />
Australia<br />
Contact address: Robert D Herbert, The George Institute for International Health, PO Box M201, Missendown Road, Camperdown,<br />
New South Wales, 2050, Australia. rherbert@george.org.au.<br />
Editorial group: Cochrane Bone, Joint and Muscle Trauma Group.<br />
Publication status and date: Edited (no change to conclusions), published in Issue 4, 2008.<br />
Review content assessed as up-to-date: 15 August 2006.<br />
Citation: Herbert RD, de Noronha M. Stretching to prevent or reduce muscle soreness after exercise. Cochrane Database of Systematic<br />
Reviews 2007, Issue 4. Art. No.: CD004577. DOI: 10.1002/14651858.CD004577.pub2.<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
Background<br />
A B S T R A C T<br />
Many people stretch before or after (or both) engaging in athletic activity. Usually the purpose is to reduce risk of injury, reduce soreness<br />
after exercise, or enhance athletic performance.<br />
Objectives<br />
The aim of this review was to determine effects of stretching before or after exercise on the development of post-exercise muscle soreness.<br />
Search strategy<br />
We searched the Cochrane Bone, Joint and Muscle Trauma Group Specialised Register (to April 2006), the Cochrane Central Register<br />
of Controlled Trials (The Cochrane Library 2006, Issue 2), MEDLINE (1966 to May 2006), EMBASE (1988 to May 2006), CINAHL<br />
(1982 to May 2006), SPORTDiscus (1949 to May 2006), PEDro (to May 2006) and reference lists of articles.<br />
Selection criteria<br />
Eligible studies were randomised or quasi-randomised studies of any pre-or post-exercise stretching technique designed to prevent or<br />
treat delayed-onset muscle soreness (DOMS), provided the stretching was conducted soon before or soon after exercise. To be eligible<br />
studies must have assessed muscle soreness or tenderness.<br />
Data collection and analysis<br />
Methodological quality of the studies was assessed using the Cochrane Bone, Joint and Muscle Trauma Group’s methodological quality<br />
assessment tool. Estimates of effects of stretching were converted to a common 100-point scale. Outcomes were pooled in a fixed-effect<br />
meta-analysis.<br />
Main results<br />
Of the 10 included studies, nine were carried out in laboratory settings using standardised exercise protocols and one involved postexercise<br />
stretching in footballers. All participants were young healthy adults. Three studies examined the effects of stretching before<br />
exercise and seven studies investigated the effects of stretching after exercise. Two studies, both of stretching after exercise, involved<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
1
epeated stretching sessions at intervals of greater than two hours. The duration of stretching applied in a single session ranged from<br />
40 to 600 seconds.<br />
All studies were small (between 10 and 30 participants received the stretch condition) and of questionable quality.<br />
The effects of stretching reported in individual studies were very small and there was a high degree of consistency of results across<br />
studies. The pooled estimate showed that pre-exercise stretching reduced soreness one day after exercise by, on average, 0.5 points on a<br />
100-point scale (95% CI -11.3 to 10.3; 3 studies). Post-exercise stretching reduced soreness one day after exercise by, on average, 1.0<br />
points on a 100-point scale (95% CI -6.9 to 4.8; 4 studies). Similar effects were evident between half a day and three days after exercise.<br />
Authors’ conclusions<br />
The evidence derived from mainly laboratory-based studies of stretching indicate that muscle stretching does not reduce delayed-onset<br />
muscle soreness in young healthy adults.<br />
P L A I N L A N G U A G E S U M M A R Y<br />
Stretching to prevent or reduce muscle soreness after exercise<br />
Many people stretch prior to or after engaging in physical activities such as sport. Usually the purpose is to reduce the risk of injury,<br />
reduce soreness after exercise, or enhance athletic performance.<br />
The review located 10 relevant randomised trials looking at the effect of stretching before or after physical activity on muscle soreness.<br />
The trials were mostly small and of questionable quality. Nine were conducted in laboratories using standardised exercises. Only one<br />
study examined the effect of stretching on muscle soreness after sport. Three of the studies examined the effects of stretching before<br />
physical activity and seven examined effects of stretching after physical activity.<br />
The 10 studies produced very consistent findings. They showed there was minimal or no effect on the muscle soreness experienced<br />
between half a day and three days after the physical activity. Effects of stretching on effect on other outcomes such as injury and<br />
performance were not examined in this review.<br />
B A C K G R O U N D<br />
Many people stretch before or after (or before and after) engaging<br />
in athletic activity. Usually the purpose is to reduce the risk of<br />
injury, reduce soreness after exercise, or enhance athletic performance<br />
(Cross 1999; de Vries 1961; Gleim 1990; Gleim 1997).<br />
This review focuses on the effects of muscle stretching on muscle<br />
soreness. Another Cochrane review (Yeung 2003) has examined<br />
whether stretching prevents injury, and several non-Cochrane systematic<br />
reviews have examined whether stretching prevents muscle<br />
soreness or injury, or enhances performance (Herbert 2002;<br />
Shrier 2004; Thacker 2004; Weldon 2003).<br />
The muscle soreness that is the focus of this review is sometimes<br />
called delayed-onset muscle soreness to differentiate it from soreness<br />
that occurs as muscle fatigue, or immediately after muscles<br />
have been fatigued. Delayed-onset muscle soreness (hereafter re-<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
ferred to simply as muscle soreness) is usually caused by unaccustomed<br />
exercise, particularly exercise that requires primarily eccentric<br />
muscle contraction. Eccentric contractions occur when the<br />
muscle lengthens as it contracts. Typically the soreness arises within<br />
the first day after exercise and peaks in intensity at around 48<br />
hours (Balnave 1993; Bobbert 1986; Wessel 1994). The soreness<br />
is usually associated with tenderness and may be associated with<br />
swelling (Bobbert 1986; Wessel 1994).<br />
The series of events that ultimately cause muscle soreness are only<br />
partly understood. The initial event is probably mechanical disruption<br />
of sarcomeres (contractile units within muscle fibres; Proske<br />
2001). This causes swelling of damaged muscle fibres and initiates<br />
an inflammatory response, which could excite nociceptors (receptors<br />
capable of transmitting information about pain; Lieber 2002).<br />
2
Muscle soreness is usually only experienced when the muscle contracts<br />
or is stretched. This indicates that, while swelling of muscle<br />
fibres and inflammation may be necessary for muscle soreness to<br />
occur, swelling and inflammation are not sufficient to cause soreness<br />
on their own. Muscle soreness is exacerbated by vibration over<br />
the belly of the muscle, and pressure thresholds increase when large<br />
diameter afferents are blocked (large diameter afferents are nerve<br />
cells that conduct information about touch and limb position),<br />
indicating that excitation of large diameter muscle afferents, probably<br />
primary spindle afferents from stretch receptors in muscles,<br />
is involved in generating the sensation of soreness (Weerakkody<br />
2001).<br />
The practice of stretching to prevent muscle soreness was encouraged<br />
by early investigators of muscle soreness who thought that<br />
unaccustomed exercise caused muscle spasm (de Vries 1961). Muscle<br />
spasm was believed to impede blood flow to the muscle, causing<br />
ischaemic pain and further spasm. Stretching the muscle was<br />
thought to restore blood flow to the muscle and interrupt the painspasm-pain<br />
cycle. The muscle spasm theory of muscle soreness has<br />
since been discredited (Bobbert 1986), but the practice of stretching<br />
persists.<br />
Typically people who stretch to prevent muscle soreness do so prior<br />
to exercise, but some people stretch after exercise. Usually each atrisk<br />
muscle is stretched for between 15 seconds and 2 minutes,<br />
once or several times. Some proponents of stretching recommend<br />
applying a sustained stretch to the relaxed muscle (de Vries 1961;<br />
this is called static stretching), but others recommend more elaborate<br />
techniques such as the ’contract-relax-agonist contract’ technique<br />
(Feland 2001). This technique and related techniques (collectively<br />
called proprioceptive neuromuscular facilitation (PNF)<br />
techniques) involve contracting the muscle strongly before applying<br />
a stretch.<br />
O B J E C T I V E S<br />
This review aims to determine the effect of stretching before or<br />
after exercise on the development of post-exercise muscle soreness.<br />
M E T H O D S<br />
Criteria for considering studies for this review<br />
Types of studies<br />
We considered any randomised or quasi-randomised (method of<br />
allocating participants to a treatment that is not strictly random<br />
e.g. by date of birth, hospital record number and alternation)<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
clinical trials of pre-or post-exercise stretching techniques designed<br />
to prevent or treat delayed-onset muscle soreness.<br />
Types of participants<br />
Trials involving participants of any age group, and of either sex.<br />
Types of interventions<br />
Any pre-or post-exercise stretching technique designed to prevent<br />
or treat delayed-onset muscle soreness, provided the stretching was<br />
conducted soon before or soon after exercise of any type.<br />
Types of outcome measures<br />
Measures of muscle soreness (pain) or tenderness (pain on palpation<br />
of the muscle).<br />
Search methods for identification of studies<br />
We searched the Cochrane Bone, Joint and Muscle Trauma Group<br />
Specialised Register (12 April 2006), the Cochrane Central Register<br />
of Controlled Trials (The Cochrane Library 2006, Issue 2)<br />
(see Appendix 1), MEDLINE (OVID WEB; 1966 to 16 May<br />
2006), EMBASE (OVID WEB; 1988 to 16 May 2006), CINAHL<br />
(OVID WEB; 1982 to 16 May 2006), SPORTDiscus (OVID<br />
WEB; 1949 to 16 May 2006), PEDro - Physiotherapy <strong>Evidence</strong><br />
Database (www.pedro.fhs.usyd.edu.au/accessed 16 May 2006)<br />
and reference lists of articles.<br />
In MEDLINE (OVID WEB) the subject-specific search in<br />
Appendix 2 was used. As it was anticipated that only a small<br />
number of references would be identified, the results were not<br />
combined with a trial search strategy. This strategy was modified<br />
slightly for use in the other OVID databases.<br />
In PEDro, two searches were conducted (see Appendix 3).<br />
Data collection and analysis<br />
Selection of trials<br />
The two authors screened search results for potentially eligible<br />
studies. When titles and abstracts suggested a study was potentially<br />
eligible for inclusion a paper copy of the report was obtained. Disagreements<br />
between the two people regarding a study’s eligibility<br />
were resolved by discussion or, where necessary, by a third person.<br />
Assessment of methodological quality<br />
The methodological quality of the studies was assessed using the<br />
Cochrane Bone, Joint and Muscle Trauma Group quality assessment<br />
tool (Table 1). Two people independently assessed study<br />
quality in this way. Disagreements were resolved by discussion.<br />
Where necessary, a third person was consulted. It was anticipated<br />
that several of the included studies would be laboratory-based studies<br />
which were unlikely to describe elements thought important<br />
3
in clinical trials. These studies may appear methodologically weak<br />
when assessed with a tool designed for clinical trials. Nonetheless<br />
it was thought useful to document the degree to which they conform<br />
with best practice clinical trial design.<br />
Table 1. Bone, Joint and Muscle Trauma Group methodological quality assessment tool<br />
Item Criterion<br />
A Was the assigned treatment adequately concealed prior to allocation?<br />
2 = clearly yes (method did not allow disclosure of assignment).<br />
1 = not sure (small but possible chance of disclosure of assignment or unclear).<br />
0 = clearly no (quasi-randomised or open list/tables).<br />
B Were the outcomes of patients/participants who withdrew described and included in the analysis (intention to treat)?<br />
2 = withdrawals well described and accounted for in analysis.<br />
1 = withdrawals described and analysis not possible.<br />
0 = no mention, inadequate mention, or obvious differences and no adjustment.<br />
C Were the outcome assessors blinded to treatment status?<br />
2 = effective action taken to blind assessors.<br />
1 = small or moderate chance of unblinding of assessors.<br />
0 = not mentioned or not possible.<br />
D Were the treatment and control group comparable at entry?<br />
2 = good comparability of groups, or confounding adjusted for in analysis.<br />
1 = confounding small; mentioned but not adjusted for.<br />
0 = large potential for confounding, or not discussed.<br />
E Were the participants blind to assignment status after allocation?<br />
2 = effective action taken to blind participants.<br />
1 = small or moderate chance of unblinding of participants.<br />
0 = not possible, or not mentioned (unless double-blind), or possible but not done.<br />
F Were the treatment providers blind to assignment status?<br />
2 = effective action taken to blind treatment providers.<br />
1 = small or moderate chance of unblinding of treatment providers.<br />
0 = not possible, or not mentioned (unless double-blind), or possible but not done.<br />
G Were care programmes, other than the trial options, identical?<br />
2 = care programmes clearly identical.<br />
1 = clear but trivial differences.<br />
0 = not mentioned or clear and important differences in care programmes.<br />
H Were the inclusion and exclusion criteria clearly defined?<br />
2 = clearly defined.<br />
1 = inadequately defined.<br />
0 = not defined.<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
4
Table 1. Bone, Joint and Muscle Trauma Group methodological quality assessment tool (Continued)<br />
I Were the interventions clearly defined? (This item was optional)<br />
2 = clearly defined interventions are applied with a standardised protocol.<br />
1 = clearly defined interventions are applied but the application protocol is not standardised.<br />
0 = intervention and/or application protocol are poorly or not defined.<br />
J Were the outcome measures used clearly defined? (by outcome)<br />
2 = clearly defined.<br />
1 = inadequately defined.<br />
0 = not defined.<br />
K Were diagnostic tests used in outcome assessment clinically useful? (by outcome)<br />
2 = optimal.<br />
1 = adequate.<br />
0 = not defined, not adequate.<br />
L Was the surveillance active, and of clinically appropriate duration?<br />
2 = active surveillance and appropriate duration.<br />
1 = active surveillance, but inadequate duration.<br />
0 = surveillance not active or not defined.<br />
Data extraction<br />
Soreness or tenderness data from stretch and comparison groups<br />
were extracted from study reports using a pro forma. This was<br />
done by the authors; again, disagreements were resolved by discussion<br />
or a third person. It was expected that some studies would<br />
report soreness data and some would report tenderness data. Some<br />
studies reported raw scores, whereas others report change scores<br />
or covariance-adjusted scores. It was also expected that outcomes<br />
would usually be measured at a series of times following exercise.<br />
Where available, data were extracted for each of a series of 12-hour<br />
intervals following exercise (6-17 hours, 18-29 hours, 30-41 hours,<br />
etc). Only one outcome was recorded from each study for each<br />
time. Where multiple outcomes were available, soreness data was<br />
preferred to tenderness data. Covariate-adjusted data were most<br />
preferred, then change scores, then raw scores. Where within-subject<br />
studies (studies in which participants’ limbs were allocated to<br />
stretch and control conditions) or cross-over studies (studies in<br />
which each participant was sequentially exposed to both stretch<br />
and control conditions) did not provide estimates of the variance<br />
of differences between conditions or of the correlations between<br />
outcomes under the two conditions being compared (Elbourne<br />
2002) the variance of the difference between conditions was estimated<br />
by assuming the data were independent.<br />
Analysis<br />
Pain and tenderness data were typically reported on 100 mm visual<br />
analogue scales or 10 point scales. To facilitate pooling, data were<br />
converted to a common 100-point scale. The effect of stretching<br />
was estimated from each study using the difference between<br />
mean pain levels in stretch and comparison groups. Where there<br />
was apparent qualitative homogeneity in participants, interventions<br />
and outcome measures, meta-analysis was considered. Metaanalysis<br />
was conducted using the RevMan Analysis program in<br />
Review Manager (RevMan 2003). The effects of stretching was<br />
described as a weighted mean difference. Data were inspected for<br />
statistical heterogeneity. As there was no evidence of heterogeneity<br />
of effect (Cochran Q, P < 0.1; Fleiss 1993), a fixed-effect model<br />
was used to pool findings across studies. Effects of pre- and postexercise<br />
stretching were initially estimated separately but, as there<br />
was no evidence of heterogeneity, they were combined in a secondary<br />
analysis. A post-hoc analysis was conducted to obtain separate<br />
estimates from laboratory-based studies and the one community-based<br />
study. An additional post-hoc analysis was conducted<br />
to obtain separate estimates from studies of static stretch and the<br />
one study that used another method of stretching.<br />
R E S U L T S<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
5
Description of studies<br />
See: Characteristics of included studies; Characteristics of excluded<br />
studies.<br />
The search retrieved 25 potentially eligible studies of which 10<br />
were included (Buroker 1989; Dawson 2005; Gulick 1996; High<br />
1989; Johansson 1999; Maxwell 1988; McGlynn 1979; Terry<br />
1985; Wessel 1994a; Wessel 1994b). The titles or abstracts of a<br />
further four papers appeared potentially eligible but could not be<br />
retrieved (Costa 1997; Buckenmeyer 1998; Lin 1999; Lu 1992)<br />
and still await assessment.<br />
Included studies<br />
Participants of all included studies were young healthy adults (age<br />
less than 40 years or mean age less than 26 years); no studies investigated<br />
effects of stretching on muscle soreness in children or<br />
middle-aged or older adults. All but one of the studies were carried<br />
out in laboratory settings and involved standardised exercise.<br />
The exception (Dawson 2005) investigated the effect of post-game<br />
stretching on muscle soreness in Australian rules football players.<br />
Three studies examined the effect of stretching before exercise (<br />
High 1989; Johansson 1999; Wessel 1994a); the remaining seven<br />
studies investigated the effects of stretching after exercise. The<br />
stretch was of the knee extensor muscles (Buroker 1989; High<br />
1989; Maxwell 1988; Terry 1985), hamstring muscles (Johansson<br />
1999; Wessel 1994a; Wessel 1994b), ankle plantarflexor muscles (<br />
Buroker 1989), wrist extensor muscles (Gulick 1996), elbow flexor<br />
muscles (McGlynn 1979), or “legs and back” muscles (Dawson<br />
2005). All but one of the studies examined the effects of static<br />
stretching; one study examined the effects of a PNF technique<br />
(“hold-relax”; Terry 1985). Two studies, both of stretching after<br />
exercise, involved repeated stretching sessions (Buroker 1989: 12<br />
sessions; McGlynn 1979: 5 sessions). The duration of stretching<br />
applied in a single session ranged from 40 seconds (Terry 1985)<br />
to 600 seconds (Gulick 1996), with a median of 390 seconds.<br />
In six studies (Buroker 1989; Dawson 2005; Gulick 1996; High<br />
1989; Maxwell 1988; McGlynn 1979) participants were randomly<br />
allocated to stretch and control conditions. One of these (Dawson<br />
2005) was a cross-over study in which each subject experienced<br />
both the stretch and control conditions. The remaining four studies<br />
(Johansson 1999; Terry 1985; Wessel 1994a; Wessel 1994b)<br />
stratified by participant and randomised legs to stretch and control<br />
conditions. Thus five studies (the single cross-over study and<br />
Table 2. Quality of trials. Rows correspond to those in Table 01<br />
Buroker<br />
1989<br />
Dawson<br />
2005<br />
Gulick<br />
1996<br />
High<br />
1989<br />
Johansson<br />
1999<br />
the four studies that compared right and left legs) provided paired<br />
comparisons. In all but two of these sufficient data were supplied<br />
to take account of the paired nature of the data. In the studies<br />
by Wessell and Wan (Wessel 1994a; Wessel 1994b) the estimates<br />
from an analysis which accounted for the paired nature of the data<br />
were less precise (Wessel 1994a) or had similar precision (Wessel<br />
1994b) to estimates obtained by ignoring the paired nature of the<br />
data, so the data were treated as if they were independent. Data<br />
from the other two studies (Dawson 2005; Johansson 1999) were<br />
treated as independent. See ’Characteristics of included studies’<br />
for further details.<br />
One study (Gulick 1996) reported only pooled data from all<br />
groups and another (Maxwell 1988) did not provide any data<br />
that could be used to calculate precison. (Both studies concluded<br />
stretching had no effect.) Consequently these studies did not contribute<br />
to the meta-analysis.<br />
Excluded studies<br />
Eleven studies were excluded (see ’Characteristics of excluded studies’).<br />
Risk of bias in included studies<br />
Table 2 summarises the methodological quality assessments. The<br />
reviewers were not always able to agree on how particular items<br />
were rated; these items are marked as “No consensus” in Table<br />
2. All included studies were apparently randomised. None of the<br />
studies described if the allocation schedule was concealed. There<br />
was no blinding in any studies: this is because it is difficult or<br />
impossible in studies of stretching to blind the person supervising<br />
the stretching exercises and the person doing the stretches and, as<br />
the outcome (soreness) must be self-reported, the assessor cannot<br />
be blinded. None of the studies clearly indicated that analysis was<br />
by intention to treat and in one study (Dawson 2005) analysis<br />
was explicitly not by intention to treat. Only one study explicitly<br />
reported completeness of follow up (Dawson 2005 reported data<br />
were available for 31 of 34 player-conditions), although two further<br />
studies (High 1989; Terry 1985) provided data that implied<br />
follow up was complete. It is likely that follow up was complete<br />
or nearly complete in most or all studies because the follow-up<br />
period was very short (three days or less) and outcome measures<br />
were not onerous.<br />
Maxwell<br />
1988<br />
McGlynn<br />
1979<br />
Terry<br />
1985<br />
Wessel<br />
1994a<br />
1 0 1 1 1 1 1 1 1 1<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
Wessel<br />
1994b<br />
6
Table 2. Quality of trials. Rows correspond to those in Table 01 (Continued)<br />
0 0 0 0 No<br />
consensus<br />
0 0 0 0 0<br />
0 0 0 0 0 0 0 0 0 0<br />
0 2 0 0 0 0 0 0 2 2<br />
0 0 0 0 0 0 0 0 0 0<br />
0 0 0 0 0 0 0 0 0 0<br />
2 2 2 2 2 2 2 2 2 2<br />
2 0 No<br />
consensus<br />
1 2 0 2 2 0 0<br />
2 1 2 2 2 2 2 2 2 2<br />
2 2 2 2 2 2 2 2 2 2<br />
2 2 2 2 2 2 2 2 2 2<br />
2 2 2 2 2 2 2 2 2 2<br />
Effects of interventions<br />
One study (Gulick 1996) reported only pooled data from all<br />
groups and another (Maxwell 1988) did not provide any data that<br />
could be used to calculate precision. Consequently these studies<br />
did not contribute to the meta-analysis. (Both studies concluded<br />
stretching had no effect.) The following results are based on data<br />
from the remaining studies.<br />
The mean effects of stretching reported in individual studies were<br />
too small to be of clinical relevance. There was a remarkable degree<br />
of consistency (homogeneity) of results across studies (I 2 for<br />
all pooled estimates was 0%). The pooled estimate was that preexercise<br />
stretching reduced soreness one day after exercise by, on<br />
average, 0.5 points on a 100-point scale (95% CI -11.3 to 10.3; 3<br />
studies; Analysis 01.02). Post-exercise stretching reduced soreness<br />
one day after exercise by, on average, 1.0 points on a 100-point<br />
scale (95% CI -6.9 to 4.8; 4 studies; Analysis 02.02). Similar effects<br />
were evident between half a day and three days after exercise.<br />
As there was no sign of statistical heterogeneity we pooled the preexercise<br />
and post-exercise studies. The pooled estimates are that<br />
pre- and post-exercise stretching reduces soreness, on average, by<br />
0.9 points on a 100-point scale at one day (95% CI -6.1 to 4.2; 7<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
studies; Analysis 03.02), increases soreness by 1.0 points on a 100point<br />
scale at two days (95% CI -4.1 to 6.2; 7 studies; Analysis<br />
03.04) and decreases soreness by 0.3 points on a 100-point scale<br />
at three days (95% CI -6.8 to 6.2; 5 studies; Analysis 03.06).<br />
Similar estimates of effects were obtained in the only study that<br />
tested PNF stretching. Terry 1985 showed the effect of PNF<br />
stretching was to reduce soreness by 1.1 points on a 100-point<br />
scale at both one and two days after exercise (95% CIs of -13.0<br />
to 10.8; and -13.3 to 11.1 respectively). Also similar effects were<br />
obtained in the one study of stretching after sport. Dawson 2005<br />
showed that stretching increased muscle soreness by 3.0 points on<br />
a 100-point scale (95% CI -7.1 to 13.1) at 15 hours and by 4.0<br />
points (95% CI -5.2 to 13.2) at 48 hours after an Australian rule<br />
football match.<br />
D I S C U S S I O N<br />
The evidence from randomised studies indicates that stretching<br />
soon before or soon after exercise does not lessen muscle soreness<br />
on subsequent days.<br />
7
This conclusion is based on studies that rate poorly on conventional<br />
scales of study quality. None of the reviewed studies explicitly<br />
concealed allocation, none were blinded, and none explicitly<br />
analysed by intention to treat. Nonetheless there are some reasons<br />
to believe that the findings may not be seriously biased: First, there<br />
is a high degree of consistency across studies in estimates of the<br />
effect of stretching. Also, biases due to non-concealment, lack of<br />
blinding and failure to analyse by intention to treat typically produce<br />
exaggerated effects (Chalmers 1983; Colditz 1989; Moher<br />
1998; Schulz 1995), yet this review found consistent evidence of<br />
near-zero effects. The high degree of consistency of estimates across<br />
studies suggests that alternative weightings (based, for example,<br />
on different approaches to estimating precision from studies that<br />
used within-subject designs) would produce very similar pooled<br />
estimates of effects.<br />
All but one of the eligible studies were laboratory-based studies.<br />
These studies assessed whether supervised stretching reduced<br />
the soreness produced by standardised exercise involving eccentric<br />
contractions of a particular muscle group. Such studies can be<br />
considered to have an “explanatory” orientation because they tell<br />
us about what the effects of stretching could be when administered<br />
under ideal conditions. It might have been expected that the<br />
effects of stretching would be smaller in community settings. In<br />
community settings, unlike the laboratory settings of these studies,<br />
stretching is not usually supervised, so it may be carried out<br />
sub-optimally. Also, the everyday experience of muscle soreness<br />
may be of soreness in many muscle groups, and it may be difficult<br />
to effectively stretch all of the muscle groups that might become<br />
sore. These considerations suggest the effects of stretching<br />
might be smaller in community settings than in laboratory settings.<br />
However the estimates from nine laboratory-based studies<br />
and one community-based study suggest there are similar (nearzero)<br />
effects in both settings.<br />
The practice of stretching before or after exercise may have been<br />
arisen because of the mistaken belief, prevalent in the 1960s and<br />
1970s, that muscle soreness was due to muscle spasm (de Vries<br />
1961). This view has since been discredited (Bobbert 1986). Contemporary<br />
beliefs about the mechanisms of muscle soreness do<br />
not suggest any means by which stretching before or after exercise<br />
could reduce the soreness that follows that exercise session. However<br />
if, as has been proposed, muscle soreness is due to excessive<br />
elongation of some sarcomeres within muscle fibres (Proske 2001),<br />
it is conceivable that any intervention which increased the number<br />
of sarcomeres in series in muscle fibres, or which increased the<br />
length or compliance of tendons, could reduce sarcomere strains<br />
and lessen muscle damage associated with unaccustomed eccentric<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
muscle contractions. This suggests the possibility that stretching<br />
may be more effective for people who have very short muscles, or<br />
if the stretching is repeated for weeks or months or years. To date,<br />
however, randomised trials have only examined the short-term effects<br />
of one or a few sessions of stretching, and no randomised<br />
trials have specifically investigated interactions between effects of<br />
stretching and flexibility.<br />
The best available evidence indicates stretching does not reduce<br />
muscle soreness. However there are other justifications for stretching.<br />
Some evidence suggests that once muscle soreness has developed<br />
stretching may provide a transient relief of soreness (Reisman<br />
2005): some people stretch to reduce risk of injury, others stretch<br />
to enhance athletic or sporting performance, and yet others stretch<br />
because it gives them a sense of well-being. The current review<br />
does not provide any evidence of an effect or otherwise of stretching<br />
on risk of injury, performance or well-being.<br />
A U T H O R S ’ C O N C L U S I O N S<br />
Implications for practice<br />
The available evidence from randomised trials carried out mainly<br />
in laboratory settings consistently suggests that stretching before<br />
or after exercise does not prevent muscle soreness in young healthy<br />
adults.<br />
Implications for research<br />
Arguably the findings of this review are clear enough that further<br />
research into the effects of stretching on muscle soreness is not<br />
necessary. We see some merit in this view. However, in our opinion<br />
it would be useful to conduct further trials of the effects of longerterm<br />
stretching programs, in community-based populations and<br />
for people with reduced flexibility.<br />
A C K N O W L E D G E M E N T S<br />
This review is based on an earlier “non-Cochrane” review conducted<br />
by Rob Herbert and Michael Gabriel and published in<br />
2002 (Herbert RD, Gabriel M. BMJ 2002;325(7362):468-72).<br />
Through that earlier work Michael Gabriel indirectly contributed<br />
to the current review. His contribution is gratefully acknowledged.<br />
The authors thank Helen Handoll, Vicki Livingstone, Janet Wale,<br />
Gisela Sole and Lindsey Shaw for helpful comments on the review,<br />
and Lisa Harvey for assistance with data extraction.<br />
8
References to studies included in this review<br />
Buroker 1989 {published data only}<br />
Buroker KC, Schwane JA. Does postexercise static stretching<br />
alleviate delayed muscle soreness?. Physician and Sportsmedicine<br />
1989;17(6):65–83.<br />
Dawson 2005 {published data only}<br />
Dawson B, Gow S, Modra S, Bishop D, Stewart G. Effects of<br />
immediate post-game recovery procedures on muscle soreness,<br />
power and flexibility levels over the next 48 hours. Journal of<br />
Science and Medicine in Sport 2005;8(2):210–21.<br />
Gulick 1996 {published data only}<br />
Gulick DT, Kimura IF, Sitler M, Paolone A, Kelly JD. Various<br />
treatment techniques on signs and symptoms of delayed onset<br />
muscle soreness. Journal of Athletic Training 1996;31(2):145–52.<br />
High 1989 {published data only}<br />
High DM, Howley ET, Franks BD. The effects of static stretching<br />
and warm-up on prevention of delayed-onset muscle soreness.<br />
Research Quarterly for Exercise and Sport 1989;60(4):357–61.<br />
Johansson 1999 {published data only}<br />
Johansson PH, Lindström L, Sundelin G, Lindström B. The effects<br />
of preexercise stretching on muscular soreness, tenderness and force<br />
loss following heavy eccentric exercise. Scandinavian Journal of<br />
Medicine and Science in Sports 1999;9(4):219–25.<br />
Maxwell 1988 {published data only}<br />
Maxwell S, Kohn S, Watson A, Balnave RJ. Is stretching effective in<br />
the prevention of or amelioration of delayed-onset muscle soreness?.<br />
In: Torode M editor(s). The athlete maximising participation and<br />
minimising risk. Sydney: Cumberland College of Health Sciences,<br />
1988:109–18.<br />
McGlynn 1979 {published data only}<br />
McGlynn GH, Laughlin NT, Rowe V. Effect of electromyographic<br />
feedback and static stretching on artificially induced muscle<br />
soreness. American Journal of Physical Medicine 1979;58(3):139–48.<br />
Terry 1985 {published data only}<br />
∗ Terry L. Stretching and muscle soreness. An investigation into the<br />
effects of hold-relax stretch on delayed post-exercise soreness in the<br />
quadriceps muscle - a pilot study [thesis]. Adelaide (Australia): South<br />
Australian Institute of Technology, 1985.<br />
Terry L. Stretching and muscle soreness: an investigation into the<br />
effects of a hold-relax stretch on delayed post-exercise soreness in<br />
the quadriceps muscle: a pilot study [abstract]. Australian Journal of<br />
Physiotherapy Australian Journal of Physiotherapy 1987;33(1):69.<br />
Wessel 1994a {published data only}<br />
Wessel J, Wan A. Effect of stretching on the intensity of delayedonset<br />
muscle soreness. Clinical Journal of Sport Medicine 1994;4(2):<br />
83–7.<br />
Wessel 1994b {published data only}<br />
Wessel J, Wan A. Effect of stretching on the intensity of delayedonset<br />
muscle soreness. Clinical Journal of Sport Medicine 1994;4(2):<br />
83–7.<br />
References to studies excluded from this review<br />
R E F E R E N C E S<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
Abraham 1977 {published data only}<br />
Abraham WM. Factors in delayed muscle soreness. Medicine and<br />
Science in Sports 1997;9(1):11–20.<br />
Bale 1991 {published data only}<br />
Bale P, James H. Massage, warmdown and rest as recuperative<br />
measures after short term intense exercise. Physiotherapy in Sport<br />
1991;13(2):4–7.<br />
de Vries 1966 {published data only}<br />
de Vries HA. Quantitative electromyographic investigation of the<br />
spasm theory of muscle pain. American Journal of Physical Medicine<br />
1966;45(3):119–34.<br />
Jayaraman 2004 {published data only}<br />
Jayaraman RC, Reid RW, Foley JM, Prior BM, Dudley GA,<br />
Weingand KW, et al.MRI evaluation of topical heat and static<br />
stretching as therapeutic modalities for the treatment of eccentric<br />
exercise-induced muscle damage. European Journal of Applied<br />
Physiology 2004;93(1-2):30–8.<br />
Lightfoot 1997 {published data only}<br />
Lightfoot JT, Char D, McDermott J, Goya C. Immediate<br />
postexercise massage does not attenuate delayed onset muscle<br />
soreness. Journal of Strength and Conditioning Research 1997;11:<br />
119–24.<br />
Lund 1998 {published data only}<br />
Lund H, Vestergaard-Poulsen, Kanstrup I-L, Sejrsen P. The effect of<br />
passive stretching on delayed onset muscle soreness, and other<br />
detrimental effects following exercise. Scandinavian Journal of<br />
Medicine and Science in Sports 1998;8:216–21.<br />
Prentice 1982 {published data only}<br />
Prentice WE. Electromyographic analysis of the effectiveness of<br />
heat or cold and stretching for inducing relaxation in injured<br />
muscle. Journal of Orthopaedic and Sports Physical Therapy 1982;3<br />
(3):133–40.<br />
Rahnama 2005 {published data only}<br />
Rahnama N. Rahmani-Nia F. Ebrahim K. The isolated and<br />
combined effects of selected physical activity and ibuprofen on<br />
delayed-onset muscle soreness. Journal of Sports Sciences 2005;23<br />
(8):843–850.<br />
Reilly 2002 {published data only}<br />
Reilly T, Rigby M. Effect of an active warm-down following<br />
competitive soccer. In: Spinks W, Reilly T, Murphy A editor(s).<br />
Science and Football IV. Proceedings of the 4th World Congress of<br />
Science and Football; 1999 Feb 22-26; Sydney, NSW. London:<br />
Routledge, 2002:226–9.<br />
Rodenburg 1994 {published data only}<br />
Rodenburg JB, Steenbeek, Schiereck P, Bar PR. Warm-up,<br />
stretching and massage diminish harmful effects of eccentric<br />
exercise. International Journal of Sports Medicine 1994;15(7):414–9.<br />
Smith 1993 {published data only}<br />
Smith LL, Brunetz MH, Chenier TC, McCammon MR, Houmard<br />
JA, Franklin ME, et al.The effects of static and ballistic stretching<br />
on delayed onset muscle soreness. Research Quarterly for Exercise<br />
and Sport 1993;1:103–7.<br />
9
References to studies awaiting assessment<br />
Buckenmeyer 1998 {published data only}<br />
Buckenmeyer P, Kokkinidis E. Machairidou M, Tsamourtas A. The<br />
effect of static stretching and cryotherapy on the recovery of<br />
delayed muscle soreness [Greek]. Exercise & Society Journal of Sport<br />
Science (Komotini) 1998;(19):45–53.<br />
Costa 1997 {published data only}<br />
Costa MC, Cabral JG, Muniz GMA, Silva EF, Silva MG, Duarte<br />
JAR, et al.Effects of stretching after exercise on some indirect<br />
markers muscle damage. 9th European Congress on Sports<br />
Medicine; 1997 Sept 23-26; Porto, Portugal. 1997:1.<br />
Lin 1999 {published data only}<br />
Lin WH. The effects of massage, stretch and meloxicam on delayed<br />
onset muscle soreness [Masters thesis]. Taiwan: National College of<br />
Physical Education and Sports Taoyuan, 1999.<br />
Lu 1992 {published data only}<br />
∗ Lu D, Fan JY, Qu Z. An immuno-electron microscopic study of<br />
the effect of acupuncture and static stretch on contractile structural<br />
alteration of skeletal muscle after strenuous exercise. Sport Science<br />
(Beijing) 1992;12(6):47–51.<br />
Lu D, Fan JY, Qu Z. An immuno-electron microscopic study of the<br />
effect of acupuncture and static stretch on ultrastructural alteration<br />
of M-line of skeletal muscle after strenuous exercise. Sports Science<br />
(Beijing) 1992;12(6):52–9.<br />
Lu D, Fan JY, Qu Z. An immuno-electron microscopic study of the<br />
effect of acupuncture and static stretch on ultrastructural alteration<br />
of Z-band in human skeletal muscle after strenuous exercise. Sports<br />
Science (Beijing) 1992;12(6):60–5.<br />
Additional references<br />
Balnave 1993<br />
Balnave CD, Thomson MW. Effect of training on eccentric<br />
exercise-induced muscle damage. Journal of Applied Physiology<br />
1993;75(4):1545–51.<br />
Bobbert 1986<br />
Bobbert MF, Hollander AP, Huijing PA. Factors in delayed onset<br />
muscle sorenesss of man. Medicine and Science in Sports and Exercise<br />
1986;18(1):75–81.<br />
Chalmers 1983<br />
Chalmers TC, Celano P, Sacks HS, Smith H. Bias in treatment<br />
assignment in controlled clinical trials. New England Journal of<br />
Medicine 1983;309(22):1358–61.<br />
Colditz 1989<br />
Colditz GA, Miller JN, Mosteller F. How study design affects<br />
outcomes in comparisons of therapy. I: Medical. Statistics in<br />
Medicine 1989;8(4):441–54.<br />
Cross 1999<br />
Cross KM, Worrell TW. Effects of a static stretching program on<br />
the incidence of lower extremity musculotendinous strains. Journal<br />
of Athletic Training 1999;34:11–4.<br />
de Vries 1961<br />
de Vries HA. Prevention of muscular distress after exercise. Research<br />
Quarterly 1961;32:177–85.<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
Elbourne 2002<br />
Elbourne DR, Altman DG, Higgins JPT, Curtin F, Worthington<br />
HV, Vail A. Meta-analyses involving cross-over trials:<br />
methodological issues. International Journal of Epidemiology 2002;<br />
31(1):140–9.<br />
Feland 2001<br />
Feland JB, Myrer JW, Merrill RM. Acute changes in hamstring<br />
flexibility: PNF versus static stretch in senior athletes. Physical<br />
Therapy in Sport 2001;2(4):186–93.<br />
Fleiss 1993<br />
Fleiss JL. The statistical basis of meta-analysis. Statistical Methods in<br />
Medical Research 1993;2:121–45.<br />
Gleim 1990<br />
Gleim GW, Stachenfeld NS, Nicholas JA. The influence of<br />
flexibility on the economy of walking and jogging. Journal of<br />
Orthopedic Research 1990;8:814–23.<br />
Gleim 1997<br />
Gleim GW, McHugh MP. Flexibility and its effects on sports injury<br />
and performance. Sports Medicine 1997;24:289–99.<br />
Lieber 2002<br />
Lieber RL, Friden J. Morphologic and mechanical basis of delayedonset<br />
muscle soreness. Journal of the American Academy of<br />
Orthopaedic Surgeons 2002;10(1):67–73.<br />
Moher 1998<br />
Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et<br />
al.Does quality of reports of randomised trials affect estimates of<br />
intervention efficacy reported in meta-analyses?. Lancet 1995;352<br />
(9128):609–13.<br />
Proske 2001<br />
Proske U, Morgan DL. Muscle damage from eccentric exercise:<br />
mechanism, mechanical signs, adaptation and clinical applications.<br />
Journal of Physiology 2001;537(2):333–45.<br />
Reisman 2005<br />
Reisman S, Walsh LD, Proske U. Warm-up stretches reduce<br />
sensations of stiffness and soreness after eccentric exercise. Medicine<br />
and Science in Sports and Exercise 2005;37(6):929–36.<br />
RevMan 2003<br />
The Nordic Cochrane Centre, The Cochrane Collaboration.<br />
Review Manager (RevMan). 4.2 for Windows. Copenhagen: The<br />
Nordic Cochrane Centre, The Cochrane Collaboration, 2003.<br />
Schulz 1995<br />
Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence<br />
of bias. Dimensions of methodological quality associated with<br />
estimates of treatment effects in controlled trials. JAMA 1995;273<br />
(5):408–12.<br />
Shrier 2004<br />
Shrier I. Does stretching improve performance?A systematic and<br />
critical review of the literature. Clinical Journal of Sport Medicine<br />
2004;14(5):267–73.<br />
Thacker 2004<br />
Thacker SB, Gilchrist J, Stroup DF, Kimsey CD. The impact of<br />
stretching on sports injury risk: a systematic review of the literature.<br />
Medicine and Science in Sports and Exercise 2004;36(3):371–8.<br />
10
Weerakkody 2001<br />
Weerakkody NS, Whitehead NP, Canny BJ, Gregory JE, Proske U.<br />
Large-fibre mechanoreceptors contribute to muscle soreness after<br />
eccentric exercise. Journal of Pain 2001;2(4):209–19.<br />
Weldon 2003<br />
Weldon SM, Hill RH. The efficacy of stretching for prevention of<br />
exercise-related injury: a systematic review of the literature. Manual<br />
Therapy 2003;8(3):141–50.<br />
Wessel 1994<br />
Wessel J, Wan A. Effect of stretching on the intensity of delayedonset<br />
muscle soreness. Clinical Journal of Sport Medicine 1994;4(2):<br />
82–7.<br />
Yeung 2003<br />
Yeung EW, Yeung SS. Interventions for preventing lower limb softtissue<br />
injuries in runners. Cochrane Database of Systematic Reviews<br />
2003, Issue 4. [DOI: 10.1002/14651858.CD001256]<br />
References to other published versions of this review<br />
Herbert 2002<br />
Herbert RD, Gabriel M. Effects of pre- and post-exercise stretching<br />
on muscle soreness, risk of injury and athletic performance: a<br />
systematic review. BMJ 2002;325(7362):468–72.<br />
∗ Indicates the major publication for the study<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
11
C H A R A C T E R I S T I C S O F S T U D I E S<br />
Characteristics of included studies [ordered by study ID]<br />
Buroker 1989<br />
Methods Randomised (between subjects) design<br />
Participants 23 participants (16 men and 7 women) aged 18-33 years with no known contraindications to exercise.<br />
None was highly physically trained and none were extremely active in the six weeks preceding the study.<br />
Interventions Control group (N = 8): no stretching.<br />
One stretch group 1 (N = 7): stretched left knee extensors after exercise.<br />
A second stretch group (N = 8): stretched left knee extensors and right plantarflexors after exercise.<br />
Stretches (10 30-second static stretches, each separated by 10 seconds rest, to noticeable tension or slight<br />
discomfort)were performed at 2-hour intervals for the first 24 hours and 4-hour intervals for the following<br />
48 hours except that participants were allowed to sleep for 8 hours each night.<br />
Outcomes The following measures were taken on days 1, 2 and 3:<br />
1. Soreness on a 0-6 scale (0 = no pain, light pain only on palpation, 4 = moderate pain, stiffness and/or<br />
weakness, especially on movement, 6 = severe pain limiting range of movement)<br />
2. Force required to invoke tenderness (sum of measures at 9 sites)<br />
3. Force required to invoke tenderness (highest value from 9 or 10 sites)<br />
Notes Data from the two stretch groups were pooled.<br />
Stretched after exercise.<br />
Soreness induced with 20 minutes of step-down exercise.<br />
Risk of bias<br />
Item Authors’ judgement Description<br />
Allocation concealment? Unclear B - Unclear<br />
Dawson 2005<br />
Methods Randomised (within subjects, cross-over)design<br />
Participants 17 semi-professional Australian rules football players.<br />
Interventions Stretch condition: 15 minutes of supervised gentle stretching of the legs and back. This involved “2-3<br />
repeats of 30 s held stretches across several muscle groups and joints”.<br />
Control condition: no recovery procedures.<br />
Outcomes The following measures were taken at 15 and 48 hours:<br />
1. Soreness (“how do you feel today?”) measured on a 1-7 scale anchored at “very, very good” and “very,<br />
very sore”.<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
12
Dawson 2005 (Continued)<br />
Notes Part of a larger study in which each subject was exposed on 12 occasions, each separated by one week, to<br />
one of four interventions (control, stretch, pool walking, hot-cold regimen).<br />
Initial condition was allocated randomly and subsequent conditions by alternation. Stretch was before<br />
exercise.<br />
Soreness was induced by playing football.<br />
All participants underwent a “pool recovery program” on the two days following exercise.<br />
Risk of bias<br />
Item Authors’ judgement Description<br />
Allocation concealment? Unclear B - Unclear<br />
Gulick 1996<br />
Methods Randomised (between subjects) design<br />
Participants ~22 untrained participants randomly drawn from a larger sample of 35 men and 38 women aged 21 to<br />
40 years.<br />
Interventions Stretch group (N ~ 11): static stretches of the wrist extensor muscles to “end range” for 10 minutes soon<br />
after exercise.<br />
Control group (N ~ 11): two placebo tablets after exercise and one further placebo tablet 24 hours later.<br />
Outcomes The following measures were taken 24, 48 and 72 hours after exercise:<br />
1. On a 10 cm visual analogue scale anchored at “no soreness at all” and “soreness as bad as it could be”<br />
2. Force required to invoke tenderness (sum of measures at 9 sites).<br />
Notes Part of a larger study in which subjects were randomised to seven interventions (control, stretch, antiinflammatory<br />
drug, intense exercise, ice massage, herbal ointment).<br />
Stretch was after exercise.<br />
Soreness was induced by 15 sets of 15 isokinetic eccentric wrist extensor contractions.<br />
Risk of bias<br />
Item Authors’ judgement Description<br />
Allocation concealment? Unclear B - Unclear<br />
High 1989<br />
Methods Randomised (between subjects) design<br />
Participants 30 untrained participants (stretch group, 7 men and 7 women, mean age 19.4 years; control group, 8<br />
men and 8 women, mean age 20.4 years)<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
13
High 1989 (Continued)<br />
Interventions Stretch group: stretched the quadriceps muscles (5 stretches, twice each on each leg for 50 seconds) of<br />
both legs prior to exercise. Control group: did not stretch.<br />
Outcomes The following measures were taken at 24 hour intervals for 5 days:<br />
1. Soreness on a 0-6 scale (0 = “absence of soreness”, 6 = “most severe pain possible from soreness”.<br />
Notes Part of a larger study in which subjects were randomised to four interventions (control, stretch, warm-up,<br />
warm-up and stretch).<br />
Stretch was before exercise.<br />
Soreness was induced by 80 up to minutes of step-down exercise.<br />
Risk of bias<br />
Item Authors’ judgement Description<br />
Allocation concealment? Unclear B - Unclear<br />
Johansson 1999<br />
Methods Randomised (between legs) design<br />
Participants 10 health female physiotherapy students (24 (SD 3) years, 62 (SD 3) kg, 169 (SD 5) cm), not taking antiinflammatory<br />
medication, with no lower limb musculoskeletal symptoms, had not participated in weight<br />
training for more than 3 hours per week, and were not experiencing DOMS at the time of testing.<br />
Interventions Stretch leg: four 20-second “hamstring hurdle” stretches, with 20 second rests between stretches. Stretch<br />
intensity was sufficient to induce a strong feeling of stretch but not pain.<br />
Control leg: the hamstring muscles on the other side of the body were not stretched.<br />
Outcomes The following measures were taken 24, 48 and 96 hours after exercise:<br />
1. Hamstring muscle soreness on a 100 mm visual analogue scale (0 = “no soreness”, 100 = “worst possible<br />
soreness”).<br />
2. Tenderness measured with an algometer at 5 locations.<br />
Notes Stretch was before exercise.<br />
Soreness was induced with 10 sets of 10 isokinetic knee flexor contractions.<br />
Risk of bias<br />
Item Authors’ judgement Description<br />
Allocation concealment? Unclear B - Unclear<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
14
Maxwell 1988<br />
Methods Randomised (between subjects) design<br />
Participants ~14 female first-year college students randomly drawn from a larger sample of 20 participants aged 18-<br />
25 years (mean 19.4) and with varying histories of physical activity<br />
Interventions Stretch group (N ~ 6): participants lay in prone with the hips in a neutral position. A static stretch was<br />
applied to the quadriceps to the point of discomfort and held for 15 seconds.<br />
Control group (N ~ 6): participants did not stretch.<br />
Outcomes The following measures were taken 24, 48 and 72 hours after exercise:<br />
1. Pain experienced in the quadriceps muscle whilst descending a flight of stairs rated on a 10 cm visual<br />
analogue scale anchored at 0 (“no pain”) and 10 (“severe pain”).<br />
Notes Stretch was after exercise.<br />
Soreness was induced with 15 minutes of step-down exercise.<br />
Risk of bias<br />
Item Authors’ judgement Description<br />
Allocation concealment? Unclear B - Unclear<br />
McGlynn 1979<br />
Methods Randomised (between subjects) design<br />
Participants 24 men aged 18-26 years who had not engaged in any systematic activity with their non-dominant arms<br />
in the past 30 days<br />
Interventions Stretch group (N ~ 12): participants “hyperextended” the “forearm” for two minutes before releasing the<br />
stretch for one minute. This sequence was repeated four times each at 6, 25, 30, 49 and 54 hours after<br />
exercise.<br />
Control group (N ~12): participants did not stretch.<br />
Outcomes The following measures were taken 24, 48 and 72 hours after exercise:<br />
1. Pain rated on a 30-point scale, where 0-10 was “mild” pain, 11-20 was “moderate” pain, and 21-30<br />
was “severe” pain.<br />
Notes Part of a larger study in which subjects were randomised to three interventions (control, stretch, biofeedback).<br />
Strech was after exercise.<br />
Soreness was induced with eccentric elbow flexor exercises perfomed to failure.<br />
Risk of bias<br />
Item Authors’ judgement Description<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
15
McGlynn 1979 (Continued)<br />
Allocation concealment? Unclear B - Unclear<br />
Terry 1985<br />
Methods Randomised (between legs) design<br />
Participants 30 healthy participants, 15 men and 15 women, aged between 18 and 35 years. The modal level of exercise<br />
was three times per week.<br />
Interventions Stretch (hold-relax)leg: participants lay prone with a wedge under the thigh and the knee was actively<br />
flexed as far as possible. Then the participant performed an isometric contraction against manual resistance<br />
for 4-6 seconds. This was followed by two seconds of relaxation and then an 8 second passive stretch. This<br />
was repeated 5 times.<br />
Control leg: the other leg was not stretched.<br />
Outcomes The following measures were taken on days 2 and 3:<br />
1. “Pain” (or, variably, “pain, soreness or stiffness” or “soreness”)experienced that day during functional<br />
movements rated on a scale of 0 (“no pain”) to 7 (“unbearably painful”).<br />
Notes Stretching was after exercise.<br />
Soreness was induced with 20 minutes of step-up and step-down exercise.<br />
Risk of bias<br />
Item Authors’ judgement Description<br />
Allocation concealment? Unclear B - Unclear<br />
Wessel 1994a<br />
Methods Randomised (between legs) design<br />
Participants 10 sedentary adults (5 women and 5 men) with no history of back or lower limb injury or disease, mean<br />
age 24.2 (SD 5.37), mean height 175.5 cm (SD 7.6) and mean mass 66.3 kg (8.9)<br />
Interventions Stretch leg: ten 60-second stretches of the hamstring muscles prior to exercise.<br />
Control leg: not stretched.<br />
Outcomes The following measures were taken at 12 hour intervals to 72 hours after exercise:<br />
1. Pain on a 10 cm visual analogue scale while walking on an “even” surface.<br />
Notes Randomisation was by toss of a coin.<br />
Stretching was before exercise.<br />
Soreness was induced by 3 sets of 20 isokinetic eccentric knee flexor contractions.<br />
Risk of bias<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
16
Wessel 1994a (Continued)<br />
Item Authors’ judgement Description<br />
Allocation concealment? Unclear B - Unclear<br />
Wessel 1994b<br />
Methods Randomised (between legs) design<br />
Participants 10 sedentary adults (2 women and 8 men) with no history of back or lower limb injury or disease, mean<br />
age 25.2 (SD 3.36), mean height 171.2 cm (SD 7.29) and mean mass 61.3 kg (7.12)<br />
Interventions Stretch leg: ten 60-second stretches of the hamstring muscles after exercise.<br />
Control leg: not stretched.<br />
Outcomes The following measures were taken at 12 hour intervals to 72 hours after exercise:<br />
1. Pain on a 10 cm visual analogue scale while walking on an “even” surface.<br />
Notes Randomisation was by toss of a coin.<br />
Stretching was after exercise.<br />
Soreness was induced by 3 sets of 20 isokinetic eccentric knee flexor contractions.<br />
Risk of bias<br />
Item Authors’ judgement Description<br />
Allocation concealment? Unclear B - Unclear<br />
DOMS: delayed onset muscle soreness<br />
s: second<br />
SD: standard deviation<br />
~: approximately<br />
The numbers of participants given in the Participants and Interventions columns are the number of participants who received the<br />
stretch or control intervention. Thus, in studies with three or more arms the number of participants given is less than the total number<br />
of participants in the study. In Gulick 1996, 73 participants were randomised to 7 groups but the size of each group is not given, so<br />
sample sizes are given as “~11”. In Maxwell 1988, 20 participants were randomised to 3 groups but the size of each group is not given,<br />
so sample sizes are given as “~6”. In McGlynn 1979, 36 participants were randomised to 3 groups but the size of each group is not<br />
given, so sample sizes are given as “~12”.<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
17
Characteristics of excluded studies [ordered by study ID]<br />
Abraham 1977 Stretching occurred 24 hours after exercise; not clear if conditions (stretch/flex) were randomised.<br />
Bale 1991 No stretch condition.<br />
de Vries 1966 Not randomised (compared before and after stretch).<br />
Jayaraman 2004 Stretching did not begin until 36 hours after exercise.<br />
Lightfoot 1997 Plantarflexors were sore, but quadriceps and hamstring muscles were stretched (fails criterion of “stretching<br />
technique designed to prevent or treat delayed-onset muscle soreness”).<br />
Lund 1998 Not randomised (used historical controls).<br />
Prentice 1982 Stretch combined with heat or cold; interventions 24 hours after exercise; did not measure soreness.<br />
Rahnama 2005 Stretching combined with jogging and walking and submaximal concentric contractions.<br />
Reilly 2002 Not clearly randomised; stretch combined with jogging and “shake-down”.<br />
Rodenburg 1994 Intervention was a combination of warm-up, stretch and massage.<br />
Smith 1993 Compares effects of static and ballistic stretching.<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
18
D A T A A N D A N A L Y S E S<br />
Comparison 1. Pre-exercise stretching<br />
Outcome or subgroup title<br />
1 Soreness on day 0.5 (assessed 6-<br />
17 hours post-exercise)<br />
2 Soreness on day 1 (assessed 18-<br />
29 hours post-exercise)<br />
3 Soreness on day 1.5 (assessed 30-<br />
41 hours post-exercise)<br />
4 Soreness on day 2 (assessed 42-<br />
53 hours post-exercise)<br />
5 Soreness on day 2.5 (assessed 54-<br />
65 hours post-exercise)<br />
6 Soreness on day 3 (assessed 66-<br />
77 hours post-exercise)<br />
No. of<br />
studies<br />
Comparison 2. Post-exercise stretching<br />
Outcome or subgroup title<br />
1 Soreness on day 0.5 (assessed 6-<br />
17 hours post-exercise)<br />
2 Soreness on day 1 (assessed 18-<br />
29 hours post-exercise)<br />
3 Soreness on day 1.5 (assessed 30-<br />
41 hours post-exercise)<br />
4 Soreness on day 2 (assessed 42-<br />
53 hours post-exercise)<br />
5 Soreness on day 2.5 (assessed 54-<br />
65 hours post-exercise)<br />
6 Soreness on day 3 (assessed 66-<br />
77 hours post-exercise)<br />
No. of<br />
participants Statistical method Effect size<br />
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected<br />
3 70 Mean Difference (IV, Fixed, 95% CI) -0.52 [-11.30,<br />
10.26]<br />
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected<br />
2 40 Mean Difference (IV, Fixed, 95% CI) 0.72 [-11.20, 12.64]<br />
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected<br />
2 40 Mean Difference (IV, Fixed, 95% CI) -2.50 [-15.82,<br />
10.82]<br />
No. of<br />
studies<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
No. of<br />
participants Statistical method Effect size<br />
2 51 Mean Difference (IV, Fixed, 95% CI) -0.47 [-6.05, 5.12]<br />
4 127 Mean Difference (IV, Fixed, 95% CI) -1.04 [-6.88, 4.79]<br />
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected<br />
5 158 Mean Difference (IV, Fixed, 95% CI) 1.12 [-4.63, 6.87]<br />
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected<br />
3 67 Mean Difference (IV, Fixed, 95% CI) -0.03 [-7.49, 7.43]<br />
19
Comparison 3. Either pre- or post-exercise stretching<br />
Outcome or subgroup title<br />
1 Soreness on day 0.5 (assessed 6-<br />
17 hours post-exercise)<br />
2 Soreness on day 1 (assessed 18-<br />
29 hours post-exercise)<br />
3 Soreness on day 1.5 (assessed 30-<br />
41 hours post-exercise)<br />
4 Soreness on day 2 (assessed 42-<br />
53 hours post-exercise)<br />
5 Soreness on day 2.5 (assessed 54-<br />
65 hours post-exercise)<br />
6 Soreness on day 3 (assessed 66-<br />
77 hours post-exercise)<br />
No. of<br />
studies<br />
No. of<br />
participants Statistical method Effect size<br />
3 71 Mean Difference (IV, Fixed, 95% CI) -0.97 [-6.24, 4.29]<br />
7 197 Mean Difference (IV, Fixed, 95% CI) -0.93 [-6.05, 4.20]<br />
2 40 Mean Difference (IV, Fixed, 95% CI) 1.0 [-14.37, 16.37]<br />
7 198 Mean Difference (IV, Fixed, 95% CI) 1.04 [-4.14, 6.22]<br />
2 40 Mean Difference (IV, Fixed, 95% CI) -0.75 [-13.25,<br />
11.76]<br />
5 107 Mean Difference (IV, Fixed, 95% CI) -0.28 [-6.79, 6.22]<br />
Analysis 1.1. Comparison 1 Pre-exercise stretching, Outcome 1 Soreness on day 0.5 (assessed 6-17 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 1 Pre-exercise stretching<br />
Outcome: 1 Soreness on day 0.5 (assessed 6-17 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Wessel 1994a 10 4 (5) 10 9 (25) -5.00 [ -20.80, 10.80 ]<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
20
Analysis 1.2. Comparison 1 Pre-exercise stretching, Outcome 2 Soreness on day 1 (assessed 18-29 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 1 Pre-exercise stretching<br />
Outcome: 2 Soreness on day 1 (assessed 18-29 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
High 1989 14 63.2 (37.5) 16 66.9 (37.5) 16.1 % -3.70 [ -30.60, 23.20 ]<br />
Johansson 1999 10 52.2 (15.5) 10 51 (15.8) 61.7 % 1.20 [ -12.52, 14.92 ]<br />
Wessel 1994a 10 14 (24) 10 17 (28) 22.2 % -3.00 [ -25.86, 19.86 ]<br />
Total (95% CI) 34 36 100.0 % -0.52 [ -11.30, 10.26 ]<br />
Heterogeneity: Chi 2 = 0.16, df = 2 (P = 0.92); I 2 =0.0%<br />
Test for overall effect: Z = 0.09 (P = 0.92)<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
Analysis 1.3. Comparison 1 Pre-exercise stretching, Outcome 3 Soreness on day 1.5 (assessed 30-41 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 1 Pre-exercise stretching<br />
Outcome: 3 Soreness on day 1.5 (assessed 30-41 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Wessel 1994a 10 27 (30) 10 26 (28) 1.00 [ -24.43, 26.43 ]<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
21
Analysis 1.4. Comparison 1 Pre-exercise stretching, Outcome 4 Soreness on day 2 (assessed 42-53 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 1 Pre-exercise stretching<br />
Outcome: 4 Soreness on day 2 (assessed 42-53 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Johansson 1999 10 70.5 (16.6) 10 69.4 (17.1) 65.1 % 1.10 [ -13.67, 15.87 ]<br />
Wessel 1994a 10 32 (24) 10 32 (22) 34.9 % 0.0 [ -20.18, 20.18 ]<br />
Total (95% CI) 20 20 100.0 % 0.72 [ -11.20, 12.64 ]<br />
Heterogeneity: Chi 2 = 0.01, df = 1 (P = 0.93); I 2 =0.0%<br />
Test for overall effect: Z = 0.12 (P = 0.91)<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
Analysis 1.5. Comparison 1 Pre-exercise stretching, Outcome 5 Soreness on day 2.5 (assessed 54-65 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 1 Pre-exercise stretching<br />
Outcome: 5 Soreness on day 2.5 (assessed 54-65 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Wessel 1994a 10 27 (19) 10 29 (27) -2.00 [ -22.46, 18.46 ]<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
22
Analysis 1.6. Comparison 1 Pre-exercise stretching, Outcome 6 Soreness on day 3 (assessed 66-77 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 1 Pre-exercise stretching<br />
Outcome: 6 Soreness on day 3 (assessed 66-77 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Johansson 1999 10 39.4 (23.8) 10 38.2 (24.1) 40.3 % 1.20 [ -19.79, 22.19 ]<br />
Wessel 1994a 10 13 (17) 10 18 (22) 59.7 % -5.00 [ -22.23, 12.23 ]<br />
Total (95% CI) 20 20 100.0 % -2.50 [ -15.82, 10.82 ]<br />
Heterogeneity: Chi 2 = 0.20, df = 1 (P = 0.65); I 2 =0.0%<br />
Test for overall effect: Z = 0.37 (P = 0.71)<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
Analysis 2.1. Comparison 2 Post-exercise stretching, Outcome 1 Soreness on day 0.5 (assessed 6-17 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 2 Post-exercise stretching<br />
Outcome: 1 Soreness on day 0.5 (assessed 6-17 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Dawson 2005 14 60 (17) 17 57 (10) 30.6 % 3.00 [ -7.09, 13.09 ]<br />
Wessel 1994b 10 4 (6) 10 6 (9) 69.4 % -2.00 [ -8.70, 4.70 ]<br />
Total (95% CI) 24 27 100.0 % -0.47 [ -6.05, 5.12 ]<br />
Heterogeneity: Chi 2 = 0.65, df = 1 (P = 0.42); I 2 =0.0%<br />
Test for overall effect: Z = 0.16 (P = 0.87)<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
23
Analysis 2.2. Comparison 2 Post-exercise stretching, Outcome 2 Soreness on day 1 (assessed 18-29 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 2 Post-exercise stretching<br />
Outcome: 2 Soreness on day 1 (assessed 18-29 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Buroker 1989 15 61.7 (15.1) 8 64 (5.9) 45.3 % -2.30 [ -10.97, 6.37 ]<br />
McGlynn 1979 12 29.4 (20) 12 27.5 (19.5) 13.6 % 1.90 [ -13.90, 17.70 ]<br />
Terry 1985 30 23.6 (23.6) 30 24.7 (23.6) 23.8 % -1.10 [ -13.04, 10.84 ]<br />
Wessel 1994b 10 13 (16) 10 13 (16) 17.3 % 0.0 [ -14.02, 14.02 ]<br />
Total (95% CI) 67 60 100.0 % -1.04 [ -6.88, 4.79 ]<br />
Heterogeneity: Chi 2 = 0.24, df = 3 (P = 0.97); I 2 =0.0%<br />
Test for overall effect: Z = 0.35 (P = 0.73)<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
Analysis 2.3. Comparison 2 Post-exercise stretching, Outcome 3 Soreness on day 1.5 (assessed 30-41 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 2 Post-exercise stretching<br />
Outcome: 3 Soreness on day 1.5 (assessed 30-41 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Wessel 1994b 10 22 (22) 10 21 (22) 1.00 [ -18.28, 20.28 ]<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
24
Analysis 2.4. Comparison 2 Post-exercise stretching, Outcome 4 Soreness on day 2 (assessed 42-53 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 2 Post-exercise stretching<br />
Outcome: 4 Soreness on day 2 (assessed 42-53 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Buroker 1989 15 65.2 (23.1) 8 68.5 (13.7) 14.6 % -3.30 [ -18.36, 11.76 ]<br />
Dawson 2005 14 52 (15) 17 48 (10) 39.2 % 4.00 [ -5.18, 13.18 ]<br />
McGlynn 1979 12 29.4 (20) 12 27.2 (20.4) 12.7 % 2.20 [ -13.96, 18.36 ]<br />
Terry 1985 30 23.3 (24) 30 24.4 (24) 22.4 % -1.10 [ -13.25, 11.05 ]<br />
Wessel 1994b 10 26 (22) 10 26 (17) 11.1 % 0.0 [ -17.23, 17.23 ]<br />
Total (95% CI) 81 77 100.0 % 1.12 [ -4.63, 6.87 ]<br />
Heterogeneity: Chi 2 = 0.87, df = 4 (P = 0.93); I 2 =0.0%<br />
Test for overall effect: Z = 0.38 (P = 0.70)<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
Analysis 2.5. Comparison 2 Post-exercise stretching, Outcome 5 Soreness on day 2.5 (assessed 54-65 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 2 Post-exercise stretching<br />
Outcome: 5 Soreness on day 2.5 (assessed 54-65 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Wessel 1994b 10 24 (19) 10 24 (17) 0.0 [ -15.80, 15.80 ]<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
25
Analysis 2.6. Comparison 2 Post-exercise stretching, Outcome 6 Soreness on day 3 (assessed 66-77 hours<br />
post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 2 Post-exercise stretching<br />
Outcome: 6 Soreness on day 3 (assessed 66-77 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Buroker 1989 15 51.8 (20.2) 8 50.3 (26.5) 12.6 % 1.50 [ -19.52, 22.52 ]<br />
McGlynn 1979 12 11.4 (9.9) 12 11.4 (13) 65.1 % 0.0 [ -9.25, 9.25 ]<br />
Wessel 1994b 10 17 (17) 10 18 (19) 22.3 % -1.00 [ -16.80, 14.80 ]<br />
Total (95% CI) 37 30 100.0 % -0.03 [ -7.49, 7.43 ]<br />
Heterogeneity: Chi 2 = 0.03, df = 2 (P = 0.98); I 2 =0.0%<br />
Test for overall effect: Z = 0.01 (P = 0.99)<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
Analysis 3.1. Comparison 3 Either pre- or post-exercise stretching, Outcome 1 Soreness on day 0.5<br />
(assessed 6-17 hours post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 3 Either pre- or post-exercise stretching<br />
Outcome: 1 Soreness on day 0.5 (assessed 6-17 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Wessel 1994a 10 4 (5) 10 9 (25) 11.1 % -5.00 [ -20.80, 10.80 ]<br />
Dawson 2005 14 60 (17) 17 57 (10) 27.2 % 3.00 [ -7.09, 13.09 ]<br />
Wessel 1994b 10 4 (6) 10 6 (9) 61.7 % -2.00 [ -8.70, 4.70 ]<br />
Total (95% CI) 34 37 100.0 % -0.97 [ -6.24, 4.29 ]<br />
Heterogeneity: Chi 2 = 0.93, df = 2 (P = 0.63); I 2 =0.0%<br />
Test for overall effect: Z = 0.36 (P = 0.72)<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
26
Analysis 3.2. Comparison 3 Either pre- or post-exercise stretching, Outcome 2 Soreness on day 1 (assessed<br />
18-29 hours post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 3 Either pre- or post-exercise stretching<br />
Outcome: 2 Soreness on day 1 (assessed 18-29 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Buroker 1989 15 61.7 (15.1) 8 64 (5.9) 35.0 % -2.30 [ -10.97, 6.37 ]<br />
High 1989 14 63.2 (37.5) 16 66.9 (37.5) 3.6 % -3.70 [ -30.60, 23.20 ]<br />
Johansson 1999 10 52.2 (15.5) 10 51 (15.8) 14.0 % 1.20 [ -12.52, 14.92 ]<br />
McGlynn 1979 12 29.4 (20) 12 27.5 (19.5) 10.5 % 1.90 [ -13.90, 17.70 ]<br />
Terry 1985 30 23.6 (23.6) 30 24.7 (23.6) 18.4 % -1.10 [ -13.04, 10.84 ]<br />
Wessel 1994a 10 14 (24) 10 17 (28) 5.0 % -3.00 [ -25.86, 19.86 ]<br />
Wessel 1994b 10 13 (16) 10 13 (16) 13.4 % 0.0 [ -14.02, 14.02 ]<br />
Total (95% CI) 101 96 100.0 % -0.93 [ -6.05, 4.20 ]<br />
Heterogeneity: Chi 2 = 0.40, df = 6 (P = 1.00); I 2 =0.0%<br />
Test for overall effect: Z = 0.35 (P = 0.72)<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
Analysis 3.3. Comparison 3 Either pre- or post-exercise stretching, Outcome 3 Soreness on day 1.5<br />
(assessed 30-41 hours post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 3 Either pre- or post-exercise stretching<br />
Outcome: 3 Soreness on day 1.5 (assessed 30-41 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Wessel 1994a 10 27 (30) 10 26 (28) 36.5 % 1.00 [ -24.43, 26.43 ]<br />
Wessel 1994b 10 22 (22) 10 21 (22) 63.5 % 1.00 [ -18.28, 20.28 ]<br />
Total (95% CI) 20 20 100.0 % 1.00 [ -14.37, 16.37 ]<br />
Heterogeneity: Chi 2 = 0.0, df = 1 (P = 1.00); I 2 =0.0%<br />
Test for overall effect: Z = 0.13 (P = 0.90)<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
27
Analysis 3.4. Comparison 3 Either pre- or post-exercise stretching, Outcome 4 Soreness on day 2 (assessed<br />
42-53 hours post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 3 Either pre- or post-exercise stretching<br />
Outcome: 4 Soreness on day 2 (assessed 42-53 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Buroker 1989 15 65.2 (23.1) 8 68.5 (13.7) 11.8 % -3.30 [ -18.36, 11.76 ]<br />
Johansson 1999 10 70.5 (16.6) 10 69.4 (17.1) 12.3 % 1.10 [ -13.67, 15.87 ]<br />
Dawson 2005 14 52 (15) 17 48 (10) 31.8 % 4.00 [ -5.18, 13.18 ]<br />
McGlynn 1979 12 29.4 (20) 12 27.2 (20.4) 10.3 % 2.20 [ -13.96, 18.36 ]<br />
Terry 1985 30 23.3 (24) 30 24.4 (24) 18.2 % -1.10 [ -13.25, 11.05 ]<br />
Wessel 1994a 10 32 (24) 10 32 (22) 6.6 % 0.0 [ -20.18, 20.18 ]<br />
Wessel 1994b 10 26 (22) 10 26 (17) 9.0 % 0.0 [ -17.23, 17.23 ]<br />
Total (95% CI) 101 97 100.0 % 1.04 [ -4.14, 6.22 ]<br />
Heterogeneity: Chi 2 = 0.88, df = 6 (P = 0.99); I 2 =0.0%<br />
Test for overall effect: Z = 0.39 (P = 0.69)<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
28
Analysis 3.5. Comparison 3 Either pre- or post-exercise stretching, Outcome 5 Soreness on day 2.5<br />
(assessed 54-65 hours post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 3 Either pre- or post-exercise stretching<br />
Outcome: 5 Soreness on day 2.5 (assessed 54-65 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Wessel 1994a 10 27 (19) 10 29 (27) 37.4 % -2.00 [ -22.46, 18.46 ]<br />
Wessel 1994b 10 24 (19) 10 24 (17) 62.6 % 0.0 [ -15.80, 15.80 ]<br />
Total (95% CI) 20 20 100.0 % -0.75 [ -13.25, 11.76 ]<br />
Heterogeneity: Chi 2 = 0.02, df = 1 (P = 0.88); I 2 =0.0%<br />
Test for overall effect: Z = 0.12 (P = 0.91)<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
Analysis 3.6. Comparison 3 Either pre- or post-exercise stretching, Outcome 6 Soreness on day 3 (assessed<br />
66-77 hours post-exercise).<br />
Review: Stretching to prevent or reduce muscle soreness after exercise<br />
Comparison: 3 Either pre- or post-exercise stretching<br />
Outcome: 6 Soreness on day 3 (assessed 66-77 hours post-exercise)<br />
Study or subgroup Stretch Control Mean Difference Weight Mean Difference<br />
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI<br />
Buroker 1989 15 51.8 (20.2) 8 50.3 (26.5) 9.6 % 1.50 [ -19.52, 22.52 ]<br />
Johansson 1999 10 39.4 (23.8) 10 38.2 (24.1) 9.6 % 1.20 [ -19.79, 22.19 ]<br />
McGlynn 1979 12 11.4 (9.9) 12 11.4 (13) 49.6 % 0.0 [ -9.25, 9.25 ]<br />
Wessel 1994a 10 13 (17) 10 18 (22) 14.3 % -5.00 [ -22.23, 12.23 ]<br />
Wessel 1994b 10 18 (19) 10 17 (17) 17.0 % 1.00 [ -14.80, 16.80 ]<br />
Total (95% CI) 57 50 100.0 % -0.28 [ -6.79, 6.22 ]<br />
Heterogeneity: Chi 2 = 0.36, df = 4 (P = 0.99); I 2 =0.0%<br />
Test for overall effect: Z = 0.09 (P = 0.93)<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
-100 -50 0 50 100<br />
Favours stretch Favours control<br />
29
A P P E N D I C E S<br />
Appendix 1. Search strategy for The Cochrane Library<br />
#1. stretch*<br />
#2. flexib*<br />
#3. PLIABILITY single term (MeSH)<br />
#4. (range near motion)<br />
#5. (((((warmup or warm-up) or (warm next down)) or cooldown) or cool-down) or (cool next down))<br />
#6. ((((#1 or #2) or #3) or #4) or #5)<br />
#7. (sore* near musc*)<br />
#8. doms<br />
#9. MUSCLE CONTRACTION explode all trees (MeSH)<br />
#10. MUSCLE SKELETAL single term (MeSH)<br />
#11. (#9 or #10)<br />
#12. PAIN single term (MeSH)<br />
#13. (#11 and #12)<br />
#14. (#7 or #8 or #13)<br />
#15. (#6 and #14)<br />
Appendix 2. Search strategy for MEDLINE (OVID WEB)<br />
1. stretch$.tw.<br />
2. flexib$.tw.<br />
3. Pliability/<br />
4. (range adj3 motion).tw.<br />
5. Range of Motion, Articular/<br />
6. (warmup or warm-up or warm up or cooldown or cool-down or cool down).tw.<br />
7. or/1-6<br />
8. (sore$ adj3 musc$).tw.<br />
9. DOMS.tw.<br />
10. exp Muscle Contraction/<br />
11. Muscle, Skeletal/<br />
12. or/10-11<br />
13. Pain/<br />
14. and/12-13<br />
15. or/8-9,14<br />
16. and/7,15<br />
Appendix 3. Search strategy for PEDro<br />
The first search combined the following terms with “OR”:<br />
[in the Title/abstract field] stretch*, sore*, DOMS<br />
The second search combined the following terms with “AND”:<br />
[in the Therapy field] stretching, mobilisation, manipulation, massage<br />
[in the Subdiscipline field] sports<br />
[in the Problem field] pain<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
30
W H A T ’ S N E W<br />
Last assessed as up-to-date: 15 August 2006.<br />
4 July 2008 Amended Converted to new review format.<br />
H I S T O R Y<br />
Protocol first published: Issue 1, 2004<br />
Review first published: Issue 4, 2007<br />
C O N T R I B U T I O N S O F A U T H O R S<br />
The protocol for the current review was written by Rob Herbert. Data collection, data extraction, quality assessment, data analysis<br />
and interpretation were carried out by Marcos de Noronha and Rob Herbert. Rob Herbert wrote the review. Marcos de Noronha<br />
commented on drafts and approved the final version. Rob Herbert is guarantor for the review.<br />
D E C L A R A T I O N S O F I N T E R E S T<br />
None known.<br />
S O U R C E S O F S U P P O R T<br />
Internal sources<br />
• University of Sydney, Australia.<br />
External sources<br />
• No sources of support supplied<br />
I N D E X T E R M S<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
31
Medical Subject Headings (MeSH)<br />
∗ Exercise; Muscle Stretching Exercises; Muscular Diseases [ ∗ prevention & control]; Pain [ ∗ prevention & control]; Randomized Con-<br />
trolled Trials as Topic<br />
MeSH check words<br />
Humans<br />
Stretching to prevent or reduce muscle soreness after exercise (Review)<br />
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.<br />
32