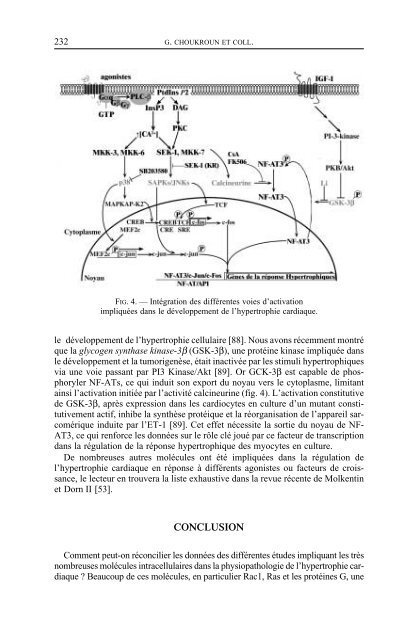
232 G. CHOUKROUN ET COLL.FIG. 4. — Intégration <strong>de</strong>s différentes voies d’activationimpliquées dans le développement <strong>de</strong> l’hypertrophie cardiaque.le développement <strong>de</strong> l’hypertrophie cellulaire [88]. Nous avons récemment montréque la glycogen synthase kinase-3β (GSK-3β), une protéine kinase impliquée dansle développement et la tumorigenèse, était inactivée par les stimuli hypertrophiquesvia une voie passant par PI3 Kinase/Akt [89]. Or GCK-3β est capable <strong>de</strong> phosphorylerNF-ATs, ce qui induit son export du noyau vers le cytoplasme, limitantainsi l’activation initiée par l’activité calcineurine (fig. 4). L’activation constitutive<strong>de</strong> GSK-3β, après expression dans les cardiocytes en culture d’un mutant constitutivementactif, inhibe la synthèse protéique et la réorganisation <strong>de</strong> l’appareil sarcomériqueinduite par l’ET-1 [89]. Cet effet nécessite la sortie du noyau <strong>de</strong> NF-AT3, ce qui renforce les données sur le rôle clé joué par ce facteur <strong>de</strong> transcriptiondans la régulation <strong>de</strong> la réponse hypertrophique <strong>de</strong>s myocytes en culture.De nombreuses autres molécules ont été impliquées dans la régulation <strong>de</strong>l’hypertrophie cardiaque en réponse à différents agonistes ou facteurs <strong>de</strong> croissance,le lecteur en trouvera la liste exhaustive dans la revue récente <strong>de</strong> Molkentinet Dorn II [53].CONCLUSIONComment peut-on réconcilier les données <strong>de</strong>s différentes étu<strong>de</strong>s impliquant les trèsnombreuses molécules intracellulaires dans la physiopathologie <strong>de</strong> l’hypertrophie cardiaque? Beaucoup <strong>de</strong> ces molécules, en particulier Rac1, Ras et les protéines G, une
MÉCANISMES MOLÉCULAIRES DE L’HYPERTROPHIE VENTRICULAIRE GAUCHE 233fois activées par fixation d’un agoniste sur son récepteur, relaient le signal en activantcertaines isoformes <strong>de</strong> PKC et les MAP kinases, en particulier SAPK. D’autre partl’élévation du calcium intracellulaire secondaire à la synthèse d’InsP3 active les MAPkinases et la calcineurine. Toutes ces voies concourent à l’activation <strong>de</strong> facteurs <strong>de</strong>transcription, en particulier MEF2c, AP1 (hétérodimère composé <strong>de</strong> c-Jun et <strong>de</strong>c-Fos) et NF-AT, dont l’action au niveau <strong>de</strong>s régions régulatrices <strong>de</strong>s gènes ciblesest responsable <strong>de</strong> l’induction <strong>de</strong>s gènes <strong>de</strong> la réponse hypertrophique (fig. 4).De grands progrès ont été effectués ces dix <strong>de</strong>rnières années dans la compréhensionet le démembrement <strong>de</strong>s voies <strong>de</strong> signalisation intracellulaire impliquéesdans la physiopathologie <strong>de</strong> l’hypertrophie cardiaque. La responsabilité <strong>de</strong> cesnombreuses voies <strong>de</strong> signalisation dans le contrôle <strong>de</strong> la réponse hypertrophiquedémontre la gran<strong>de</strong> complexité <strong>de</strong> ce phénomène. Ces voies <strong>de</strong> transmission pourraient<strong>de</strong>venir <strong>de</strong>s cibles nouvelles dans le développement <strong>de</strong> stratégies thérapeutiquesvisant la prise en charge <strong>de</strong> l’hypertrophie <strong>ventriculaire</strong> <strong>gauche</strong> et dans laprévention <strong>de</strong> son évolution vers l’insuffisance cardiaque congestive.BIBLIOGRAPHIE1. COHN JN. Structural basis for heart failure. Ventricular remo<strong>de</strong>ling and its pharmacological inhibition.Circulation, 1995, 91, 2504-2507.2. KATZ AM. The heart in congestive failure. Cardioscience, 1990, 1, 3-6.3. LENFANT C. Report of the task force on research in heart failure. Circulation, 1994, 90, 1118-1123.4. FOLEY RN, PARFREY PS, SARNAK MJ. Clinical epi<strong>de</strong>miology of cardiovascular disease in chronicrenal disease. Am J Kidney Dis, 1998, 32, S112-S119.5. GOODWIN JF. The frontiers of cardiomyopathy. Br Heart J, 1982, 48, 1-18.6. KATZ A. Scientific insights from clinical studies of converting-enzyme inhibitors in the failingheart. Trends Cardiovasc Med, 1995, 5, 37-47.7. BENJAMIN EJ, LEVY D. Why is left ventricular hypertrophy so predictive of morbidity and mortality? Am J Med Sci, 1999, 317, 168-175.8. FROHLICH ED, APSTEIN C, CHOBANIAN AV et al. The heart in hypertension. N Engl J Med, 1992,327, 998-1008.9. RIALS SJ, WU Y, XU X et al. Regression of left ventricular hypertrophy with captopril restoresnormal ventricular action potential duration, dispersion of refractoriness, and vulnerability to inducibleventricular fibrillation. Circulation, 1997, 96, 1330-1336.10. DEVEREUX RB, SIMONE G, GANAU A et al. Left ventricular hypertrophy and hypertension. Clin ExpHypertens, 1993, 15, 1025-1032.11. FOLEY RN, PARFREY PS, HARNETT JD et al. Clinical and echocardiographic disease in patientsstarting end-stage renal disease therapy. Kidney Int, 1995, 47, 186-192.12. WEBER KT, JALIL JE, JANICKI JS et al. Myocardial collagen remo<strong>de</strong>ling in pressure overload hypertrophy.A case for interstitial heart disease. Am J Hypertens, 1989, 931-940.13. SPIRITO P, SEIDMAN C, MCKENNA W et al. The management of hypertrophic cardiomyopathy. NEngl J Med, 1997, 36, 775-785.14. OLIVETTI G, QUAINI F, LAGRASTA C et al. Myocyte cellular hypertrophy and hyperplasia contributeto ventricular wall remo<strong>de</strong>ling in anemia-induced cardiac hypertrophy in rats. Am J Pathol, 1992,141, 227-239.15. WASHBURN RA, SAVAGE DD, DEARWATER SR et al. Echocardiographic left ventricular mass andphysical activity : quantification of the relation in spinal cord injured and apparently healthy activemen. Am J Cardiol, 1986, 58, 1248-1253.16. BONNE G, CARRIER L, RICHARD P et al. Génétique <strong>de</strong>s cardiomyopathies hypertrophiques. Mé<strong>de</strong>cine/Sciences, 1998, 14, 1054-1066.