Le resurfaçage total de la hanche : le retour du ... - desc orthopedie
Le resurfaçage total de la hanche : le retour du ... - desc orthopedie
Le resurfaçage total de la hanche : le retour du ... - desc orthopedie
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
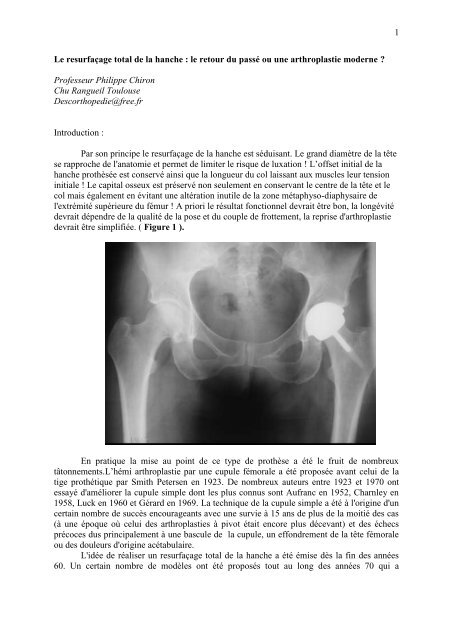
1<strong>Le</strong> <strong>resurfaçage</strong> <strong>total</strong> <strong>de</strong> <strong>la</strong> <strong>hanche</strong> : <strong>le</strong> <strong>retour</strong> <strong>du</strong> passé ou une arthrop<strong>la</strong>stie mo<strong>de</strong>rne ?Professeur Philippe ChironChu Rangueil ToulouseDesc<strong>orthopedie</strong>@free.frIntro<strong>du</strong>ction :Par son principe <strong>le</strong> <strong>resurfaçage</strong> <strong>de</strong> <strong>la</strong> <strong>hanche</strong> est sé<strong>du</strong>isant. <strong>Le</strong> grand diamètre <strong>de</strong> <strong>la</strong> têtese rapproche <strong>de</strong> l'anatomie et permet <strong>de</strong> limiter <strong>le</strong> risque <strong>de</strong> luxation ! L’offset initial <strong>de</strong> <strong>la</strong><strong>hanche</strong> prothèsée est conservé ainsi que <strong>la</strong> longueur <strong>du</strong> col <strong>la</strong>issant aux musc<strong>le</strong>s <strong>le</strong>ur tensioninitia<strong>le</strong> ! <strong>Le</strong> capital osseux est préservé non seu<strong>le</strong>ment en conservant <strong>le</strong> centre <strong>de</strong> <strong>la</strong> tête et <strong>le</strong>col mais éga<strong>le</strong>ment en évitant une altération inuti<strong>le</strong> <strong>de</strong> <strong>la</strong> zone métaphyso-diaphysaire <strong>de</strong>l'extrémité supérieure <strong>du</strong> fémur ! A priori <strong>le</strong> résultat fonctionnel <strong>de</strong>vrait être bon, <strong>la</strong> longévité<strong>de</strong>vrait dépendre <strong>de</strong> <strong>la</strong> qualité <strong>de</strong> <strong>la</strong> pose et <strong>du</strong> coup<strong>le</strong> <strong>de</strong> frottement, <strong>la</strong> reprise d'arthrop<strong>la</strong>stie<strong>de</strong>vrait être simplifiée. ( Figure 1 ).En pratique <strong>la</strong> mise au point <strong>de</strong> ce type <strong>de</strong> prothèse a été <strong>le</strong> fruit <strong>de</strong> nombreuxtâtonnements.L’hémi arthrop<strong>la</strong>stie par une cupu<strong>le</strong> fémora<strong>le</strong> a été proposée avant celui <strong>de</strong> <strong>la</strong>tige prothétique par Smith Petersen en 1923. De nombreux auteurs entre 1923 et 1970 ontessayé d'améliorer <strong>la</strong> cupu<strong>le</strong> simp<strong>le</strong> dont <strong>le</strong>s plus connus sont Aufranc en 1952, Charn<strong>le</strong>y en1958, Luck en 1960 et Gérard en 1969. La technique <strong>de</strong> <strong>la</strong> cupu<strong>le</strong> simp<strong>le</strong> a été à l'origine d'uncertain nombre <strong>de</strong> succès encourageants avec une survie à 15 ans <strong>de</strong> plus <strong>de</strong> <strong>la</strong> moitié <strong>de</strong>s cas(à une époque où celui <strong>de</strong>s arthrop<strong>la</strong>sties à pivot était encore plus décevant) et <strong>de</strong>s échecsprécoces <strong>du</strong>s principa<strong>le</strong>ment à une bascu<strong>le</strong> <strong>de</strong> <strong>la</strong> cupu<strong>le</strong>, un effondrement <strong>de</strong> <strong>la</strong> tête fémora<strong>le</strong>ou <strong>de</strong>s dou<strong>le</strong>urs d'origine acétabu<strong>la</strong>ire.L'idée <strong>de</strong> réaliser un <strong>resurfaçage</strong> <strong>total</strong> <strong>de</strong> <strong>la</strong> <strong>hanche</strong> a été émise dès <strong>la</strong> fin <strong>de</strong>s années60. Un certain nombre <strong>de</strong> modè<strong>le</strong>s ont été proposés tout au long <strong>de</strong>s années 70 qui a
2l'exception <strong>de</strong> ceux <strong>de</strong> Mül<strong>le</strong>r et <strong>de</strong> Gérard (métal/métal) étaient <strong>de</strong>s prothèses à coup<strong>le</strong> <strong>de</strong>frottement métal/polyéthylène : P<strong>la</strong>trinieri, Freeman (11) ( Figure 2 )., Aubriot, Wagner (27), Salzer en Europe et Amstutz (3)aux USA. La qualité <strong>de</strong>srésultats fonctionnels à court terme et <strong>le</strong> dynamisme <strong>de</strong>s concepteurs ont provoqué unvéritab<strong>le</strong> engouement pour cette technique (19); cependant un certain nombre d'insuffisancesliées directement à <strong>la</strong> conception <strong>du</strong> matériel ont été à l'origine d’un grand nombre <strong>de</strong><strong>de</strong>scel<strong>le</strong>ments précoces qui ont con<strong>du</strong>it <strong>le</strong>s concepteurs eux-mêmes a l’abandonner ; <strong>la</strong>condamnation <strong>du</strong> <strong>resurfaçage</strong> <strong>total</strong> <strong>de</strong> <strong>la</strong> <strong>hanche</strong> a été signée en France à l'occasion <strong>de</strong> <strong>la</strong>SOFCOT 1985. Mac minn en 1991 (18)et Amstutz en 1995(1), ont proposé une prothèse avecun coup<strong>le</strong> <strong>de</strong> frottement métal/métal, une cupu<strong>le</strong> acétabu<strong>la</strong>ire non cimentée en press fit avecun effet <strong>de</strong> surface sablé et une cupu<strong>le</strong> fémora<strong>le</strong> cimentée. Des séries <strong>de</strong> suivi clinique avec unmatériel et une technique i<strong>de</strong>ntique ont montré <strong>de</strong>s résultats favorab<strong>le</strong>s avec un taux <strong>de</strong><strong>de</strong>scel<strong>le</strong>ments et <strong>de</strong> complications superposab<strong>le</strong> à celui <strong>de</strong>s arthrop<strong>la</strong>sties à pivot.Actuel<strong>le</strong>ment <strong>le</strong> <strong>resurfaçage</strong> <strong>de</strong> <strong>la</strong> <strong>hanche</strong> est utilisé <strong>la</strong>rgement en Ang<strong>le</strong>terre auCanada et en Belgique, régulièrement en Suisse en Al<strong>le</strong>magne en Espagne aux USA, très peuen France. Ce <strong>retour</strong> <strong>du</strong> <strong>resurfaçage</strong> est-il justifié ? Un certain nombre d'arguments vont dansce sens :1 <strong>Le</strong> matériel a évolué :11 <strong>Le</strong> coup<strong>le</strong> <strong>de</strong> frottement.<strong>Le</strong>s prothèses <strong>de</strong> <strong>resurfaçage</strong> actuel<strong>le</strong>ment posées ont toutes un coup<strong>le</strong> <strong>de</strong> frottement <strong>du</strong>r/<strong>du</strong>r,métal/métal ( Figure 3 ).
3<strong>Le</strong>s progrès <strong>de</strong> <strong>la</strong> tribologie et <strong>la</strong> précision <strong>de</strong>s machines-outils mo<strong>de</strong>rnes permettentaujourd'hui <strong>de</strong> réaliser <strong>de</strong>s arthrop<strong>la</strong>sties avec <strong>de</strong>s têtes <strong>de</strong> grand diamètre dont <strong>le</strong> taux d'usureest très faib<strong>le</strong> et <strong>la</strong> tail<strong>le</strong> <strong>de</strong>s débris re<strong>la</strong>rgués inférieure à un micron ce qui permet <strong>le</strong>urtransport par <strong>le</strong>s macrophages (10). <strong>Le</strong>s cupu<strong>le</strong>s fémora<strong>le</strong>s <strong>de</strong> <strong>resurfaçage</strong> et <strong>le</strong>s têtes <strong>de</strong> granddiamètre adaptab<strong>le</strong>s sur <strong>de</strong>s tiges fémora<strong>le</strong>s sont articu<strong>la</strong>b<strong>le</strong>s avec <strong>de</strong>s pièces acétabu<strong>la</strong>iresi<strong>de</strong>ntiques.L'évaluation <strong>de</strong> ce coup<strong>le</strong> <strong>de</strong> frottement peut ainsi se faire sur <strong>de</strong> gran<strong>de</strong>s séries <strong>de</strong>prothèses <strong>total</strong>es <strong>de</strong> <strong>hanche</strong> à pivot ou <strong>de</strong> <strong>resurfaçage</strong>. En cas <strong>de</strong> complications précoces auniveau <strong>de</strong> <strong>la</strong> cupu<strong>le</strong> <strong>resurfaçage</strong> il est possib<strong>le</strong> <strong>de</strong> ne réaliser qu'une reprise unipo<strong>la</strong>ire ; <strong>le</strong> tauxd'usure très faib<strong>le</strong> <strong>de</strong> ces coup<strong>le</strong>s métal métal avec même une notion <strong>de</strong> rodage, permetd'espérer qu'une reprise tardive pourrait aussi n’être qu’unipo<strong>la</strong>ire.12 L’imp<strong>la</strong>nt acétabu<strong>la</strong>ire: il s'agit d'une pièce unique dont <strong>le</strong>s parois ont dans <strong>la</strong>plupart <strong>de</strong>s modè<strong>le</strong>s 3 mm d'épaisseur. Ce sont tous <strong>le</strong>s cas <strong>de</strong>s pièces non cimentées enMétasul* dont <strong>la</strong> face en contact avec l'os est recouverte d'une projection <strong>de</strong> titane dont <strong>la</strong>granu<strong>la</strong>tion et l'épaisseur sont variab<strong>le</strong>s.13 L’imp<strong>la</strong>nt fémoral: <strong>le</strong>s cupu<strong>le</strong>s fémora<strong>le</strong>s actuel<strong>le</strong>s ne recouvrent que <strong>la</strong> surfacecarti<strong>la</strong>gineuse sans empiéter sur <strong>le</strong> col afin <strong>de</strong> limiter sa dévascu<strong>la</strong>risation et d'éviter <strong>de</strong>sconflits fémoro-acétabu<strong>la</strong>ires antérieur ou postérieur néfastes. El<strong>le</strong>s sont proposées en <strong>de</strong>nombreuses tail<strong>le</strong>s tous <strong>le</strong>s un ou <strong>de</strong>ux millimètres afin <strong>de</strong> se rapprocher <strong>le</strong> plus possib<strong>le</strong> <strong>de</strong> <strong>la</strong>tail<strong>le</strong> initia<strong>le</strong> <strong>de</strong> <strong>la</strong> tête. El<strong>le</strong>s sont munies d'une tige <strong>de</strong> petite tail<strong>le</strong> dont l'efficacité sur <strong>la</strong>répartition <strong>de</strong>s contraintes au niveau <strong>du</strong> col reste très discutée. Il semb<strong>le</strong> cependant que cettetige facilite <strong>la</strong> pose <strong>de</strong> <strong>la</strong> cupu<strong>le</strong> et permette d'évaluer <strong>la</strong> bonne direction postopératoire <strong>de</strong> <strong>la</strong>prothèse ainsi qu’une éventuel<strong>le</strong> micro mobilité. Toutes <strong>le</strong>s cupu<strong>le</strong>s sont actuel<strong>le</strong>mentcimentées ce qui permet d'obtenir d'emblée une parfaite stabilité et <strong>de</strong> compenser l’irrégu<strong>la</strong>rité<strong>de</strong> surface <strong>de</strong> certaine tête fémora<strong>le</strong> notamment dans <strong>le</strong> cadre <strong>de</strong>s nécroses.2 La technique opératoire peut être simplifiée.21 L’orientation <strong>de</strong> <strong>la</strong> cupu<strong>le</strong>:
4Il s'agit d'un <strong>de</strong>s temps diffici<strong>le</strong>s <strong>de</strong> <strong>la</strong> technique opératoire. En effet une mauvaise orientation<strong>de</strong> <strong>la</strong> cupu<strong>le</strong> entraîne <strong>de</strong>s contraintes anorma<strong>le</strong>s sur <strong>le</strong> col sources <strong>de</strong> rupture et <strong>de</strong>s conflits <strong>du</strong>col avec <strong>le</strong>s parois acétabu<strong>la</strong>ires au prothètique. Ces conflits sont à l'origine d'un remaniementavec encoche <strong>du</strong> col en regard <strong>de</strong> <strong>la</strong> zone <strong>de</strong> conflit. <strong>Le</strong>s particu<strong>le</strong>s libérées sont cependant <strong>de</strong>sparticu<strong>le</strong>s osseuses organiques qui ne sont pas à l’origine d’une métallose. Une certaineadaptation <strong>du</strong> col au conflit reste possib<strong>le</strong>(7).Il faut que <strong>la</strong> cupu<strong>le</strong> soit située dans <strong>le</strong> p<strong>la</strong>nsagittal <strong>de</strong> préférence au centre <strong>du</strong> col et dans <strong>le</strong> p<strong>la</strong>n frontal en position neutre ou en valgus,en évitant <strong>le</strong> varus qui est source <strong>de</strong> contraintes trop importantes (6).Pour bien orienter <strong>la</strong> cupu<strong>le</strong> <strong>de</strong> nombreux systèmes <strong>de</strong> visée plus ou moins comp<strong>le</strong>xes sontproposés. <strong>Le</strong>s systèmes endoarticu<strong>la</strong>ires <strong>de</strong> conceptions variab<strong>le</strong>s nécessitent tous une bonnesvision <strong>de</strong> <strong>la</strong> tête et une exposition <strong>la</strong>rge <strong>du</strong> col source <strong>de</strong> dévascu<strong>la</strong>risation(15)( Figure 4 ).La navigation <strong>de</strong> <strong>la</strong> <strong>hanche</strong> est plus fiab<strong>le</strong> ; <strong>la</strong> prise <strong>de</strong>s différents points necessite cependanttoujours une exposition <strong>la</strong>rge <strong>du</strong> col(22)( Figure 5)..
5Nous proposons une technique simp<strong>le</strong> qui consiste à positionner avant <strong>la</strong> réalisation <strong>de</strong> <strong>la</strong>voie d'abord une broche <strong>du</strong> trochanter vers <strong>la</strong> tête sous contrô<strong>le</strong> d’un amplificateur <strong>de</strong>bril<strong>la</strong>nce(8)( Figure 6 et 7)..
6Il est ainsi possib<strong>le</strong> <strong>de</strong> choisir au cas par cas <strong>la</strong> bonne position <strong>la</strong> cupu<strong>le</strong> avec une courbed'apprentissage très rapi<strong>de</strong>. La technique guidée par broche permet d'utiliser plus faci<strong>le</strong>ment<strong>de</strong>s voies d'abord minima<strong>le</strong>s invasives.22 La voie d'abord :La conservation <strong>de</strong> <strong>la</strong> tête et <strong>du</strong> col qui gènent l’expsition <strong>de</strong> l’acétabulum, ainsi quel'exposition <strong>du</strong> col pour positionner <strong>la</strong> cupu<strong>le</strong> con<strong>du</strong>isent à réaliser <strong>la</strong> plupart <strong>du</strong> temps <strong>de</strong>svoies d'abord é<strong>la</strong>rgies qu'el<strong>le</strong>s soient postérieure, antérieure avec trochantérotomie ou selonHardinge(17). <strong>Le</strong>s éco<strong>le</strong>s françaises proposent <strong>de</strong>s voies minima<strong>le</strong>s invasives antérieures(Piriou / Ju<strong>de</strong>t) ou antéro <strong>la</strong>téra<strong>le</strong> (Chiron(8))( Figure 8 )..
8<strong>Le</strong>s différentes publications rapportent un taux variab<strong>le</strong> <strong>de</strong> fractures al<strong>la</strong>nt <strong>de</strong> 0,25% à 3 % .El<strong>le</strong>s sont souvent précoces (dans 50 à 75 % <strong>de</strong>s cas avant un an) (5).El<strong>le</strong>s sont trois fois plus fréquentes chez <strong>le</strong>s femmes et quatre fois plus fréquentes chez<strong>le</strong>s obèses (14).El<strong>le</strong>s sont aussi directement liées à l'état local <strong>de</strong> l'os : nécroses éten<strong>du</strong>es <strong>de</strong> plus <strong>de</strong> 50%, arthroses polykystiques, synovites inf<strong>la</strong>mmatoires.Enfin <strong>le</strong> geste opératoire lui-même peut être source <strong>de</strong> fracture, cupu<strong>le</strong> fémora<strong>le</strong> envarus ou réalisation d'une encoche à <strong>la</strong> partie supérieure <strong>du</strong> col <strong>du</strong>e au passage <strong>de</strong> <strong>la</strong> fraisecylindrique si <strong>la</strong> prothèse est positionnée trop en valgus (13).43 Défaut architectural <strong>de</strong> <strong>la</strong> <strong>hanche</strong> :La pièce acétabu<strong>la</strong>ire non déformab<strong>le</strong> doit être mise en press fit. Une insuffisance <strong>de</strong>couverture acétabu<strong>la</strong>ire trop importante peut être une contreindication (4)( Figure 11 )..
. De même au niveau <strong>du</strong> fémur un troub<strong>le</strong> directionnel <strong>du</strong> col vers l’avant ou vers l'arrière nepourra pas être corrigé par un <strong>resurfaçage</strong> . De même un col <strong>de</strong> court liés à <strong>de</strong>s lésionsimportantes <strong>de</strong> <strong>la</strong> tête ou à une ostéochondrite ne pourra pas être corrigé par un <strong>resurfaçage</strong>dnt <strong>la</strong> corecction maximumest <strong>de</strong> l’ordre <strong>de</strong> 5 mm.( Figure 12 )9
1044 En synthèse, <strong>le</strong> terrain idéal est un homme encore jeune avec une bonne qualitéosseuse dynamique qui a une arthrose <strong>le</strong> plus souvent <strong>du</strong>e à une épiphysiolyse ( Figure 13 et14 )ou une nécrose d'un volume inférieur à 50 % . La contre-indication absolue est unefemme <strong>de</strong> plus <strong>de</strong> 60 ans obèse.6 Ou est <strong>le</strong> problème ?Si un certain nombre d'arguments sont en faveur <strong>du</strong> <strong>resurfaçage</strong> <strong>de</strong> <strong>la</strong> <strong>hanche</strong>, ilpersiste un certain nombre <strong>de</strong> freins à <strong>la</strong> réalisation <strong>de</strong> cette technique :
11* <strong>Le</strong> coup<strong>le</strong> <strong>de</strong> frottement est un coup<strong>le</strong> métal/métal ; toutes <strong>le</strong>s publications montrent qu'i<strong>le</strong>xiste un re<strong>la</strong>rgage <strong>de</strong> particu<strong>le</strong>s <strong>de</strong> métal notamment <strong>de</strong> cobalt et <strong>de</strong> chrome ; <strong>le</strong> cobalt esturiné, <strong>le</strong> chrome peut être stocké au niveau <strong>du</strong> foie(25, 26). <strong>Le</strong> risque cancérigène <strong>de</strong> cesparticu<strong>le</strong>s n'a jamais été démontré ; en pratique <strong>le</strong>s prothèses a coup<strong>le</strong> métal polyéthylèneutilisées <strong>la</strong>rgement <strong>de</strong>puis plus <strong>de</strong> 40 ans libèrent aussi <strong>de</strong>s particu<strong>le</strong>s <strong>de</strong> chrome et <strong>de</strong> cobaltnotamment <strong>le</strong>s arthrop<strong>la</strong>sties <strong>de</strong> genou (12); <strong>le</strong>s plombages <strong>de</strong>ntaires sont sources d'une <strong>de</strong>plus gran<strong>de</strong> libération <strong>de</strong> particu<strong>le</strong>s <strong>de</strong> matériaux <strong>du</strong> même type que <strong>le</strong>s prothèses articu<strong>la</strong>iresnotamment lorsque que <strong>le</strong>s plombs sont situés en vis-à-vis ou lorsqu'il existe une couronnemétallique ; <strong>la</strong> re<strong>la</strong>tion <strong>de</strong> cause à effet entre l'existence d'une prothèse articu<strong>la</strong>ire et unetumeur primitive n'a jamais été démontrée. <strong>Le</strong> risque tératogène est lui aussi théorique. Ilconvient cependant par pru<strong>de</strong>nce <strong>de</strong> discuter avec <strong>la</strong> ma<strong>la</strong><strong>de</strong> <strong>de</strong> son désir <strong>de</strong> grossesse et <strong>de</strong>l'informer <strong>de</strong> l'état <strong>de</strong>s connaissances actuel<strong>le</strong>s. Cette information <strong>de</strong>vrait être faite nonseu<strong>le</strong>ment lorsqu'il est mis en p<strong>la</strong>ce un coup<strong>le</strong> métal/métal mais éga<strong>le</strong>ment lorsqu'il est mis enp<strong>la</strong>ce une prothèse dont l'une <strong>de</strong>s pièces <strong>de</strong> frottement est métallique.* La courbe d'apprentissage : <strong>la</strong> réalisation d'un <strong>resurfaçage</strong> <strong>de</strong> <strong>la</strong> <strong>hanche</strong> est une nouvel<strong>le</strong>technique. La présence <strong>de</strong> <strong>la</strong> tête <strong>du</strong> col gêne pour réaliser l'arthrop<strong>la</strong>stie acétabu<strong>la</strong>ire dans <strong>de</strong>bonnes conditions ; <strong>le</strong> bon positionnement <strong>de</strong> <strong>la</strong> cupu<strong>le</strong> <strong>de</strong>man<strong>de</strong> l'apprentissage <strong>de</strong> geste et <strong>de</strong>concepts nouveaux. Il est souvent diffici<strong>le</strong> pour un chirurgien qui maîtrise bien sa technique<strong>de</strong> prothèses <strong>total</strong>es standards d'admettre <strong>de</strong> faire courir à ses ma<strong>la</strong><strong>de</strong>s <strong>de</strong>s risquessupplémentaires <strong>le</strong> temps <strong>de</strong> <strong>la</strong> courbe d'apprentissage. C'est pourquoi nous p<strong>la</strong>idons pour <strong>la</strong>technique guidée par broche qui simplifie gran<strong>de</strong>ment <strong>la</strong> courbe d'apprentissage.(9)* <strong>Le</strong> bon choix <strong>de</strong> l'imp<strong>la</strong>nt dépend essentiel<strong>le</strong>ment <strong>de</strong> <strong>la</strong> tige qui pourra être mise en p<strong>la</strong>celors <strong>de</strong> <strong>la</strong> reprise . En effet il est absolument interdit <strong>de</strong> changer <strong>de</strong> fabricant lors <strong>de</strong> <strong>la</strong> reprisearthrop<strong>la</strong>stie. <strong>le</strong> type <strong>de</strong> Metasul* étant différent en fonction <strong>de</strong>s sociétés <strong>de</strong> même que <strong>la</strong>congruence entre <strong>le</strong>s pièces.* L’absence <strong>de</strong> recul : <strong>Le</strong> recul <strong>de</strong>vient conséquent avec <strong>de</strong>s séries bien suivies (2, 23, 24). Lacourbe <strong>de</strong> survie <strong>de</strong> ce type d’imp<strong>la</strong>nt oscil<strong>le</strong> entre 99% et 94% à six ans en fonction <strong>de</strong>sauteurs.Conclusion<strong>Le</strong> <strong>resurfaçage</strong> <strong>total</strong> <strong>de</strong> <strong>la</strong> <strong>hanche</strong> est un principe ancien que <strong>le</strong>s progrès <strong>de</strong> l'ingénierie et <strong>de</strong> <strong>la</strong>tribologie font entrer dans l'arsenal thérapeutique <strong>de</strong>s lésions articu<strong>la</strong>ires évoluées. <strong>Le</strong><strong>resurfaçage</strong> <strong>de</strong> l'épau<strong>le</strong> donne parallè<strong>le</strong>ment <strong>de</strong>s résultats satisfaisants. Réaliser un <strong>resurfaçage</strong>nécessite une sé<strong>le</strong>ction rigoureuse <strong>de</strong>s ma<strong>la</strong><strong>de</strong>s en évitant <strong>le</strong>s personnes âgées, <strong>le</strong>s obèses et <strong>le</strong>ssujets dont <strong>le</strong>s os ont une résistance mécanique globa<strong>le</strong> ou loca<strong>le</strong> insuffisante. Il convient <strong>de</strong>choisir une technique <strong>de</strong> visée pour <strong>le</strong> positionnement <strong>de</strong> <strong>la</strong> cupu<strong>le</strong> acétabu<strong>la</strong>ire simp<strong>le</strong> etfiab<strong>le</strong>. La courbe d'apprentissage doit commencer par <strong>de</strong>s cours centrés sur <strong>la</strong> techniqueopératoire comme celui que nous avons proposé <strong>le</strong> 14 décembre 2007 à Toulouse, suivi <strong>de</strong>visite chez <strong>de</strong>s chirurgiens qui pratiquent régulièrement cette technique, puis <strong>de</strong> <strong>la</strong> réalisationd'arthrop<strong>la</strong>sties <strong>total</strong>es <strong>de</strong> <strong>hanche</strong> à pivot à grosse tête par <strong>la</strong> voie d'abord choisie pour <strong>le</strong><strong>resurfaçage</strong> afin <strong>de</strong> se familiariser avec <strong>le</strong> positionnement <strong>de</strong> <strong>la</strong> pièce acétabu<strong>la</strong>ire, enfin par <strong>la</strong>réalisation d'un <strong>resurfaçage</strong> chez un homme mince et dynamique avec un bon capital osseux.Bibliographie :
1. Amstutz H, Beau<strong>le</strong> P, Dorey F, and coll e. Metal-on-metal hybrid surfacearthrop<strong>la</strong>sty: two to six-year follow-up study. J Bone Joint Surg 86-A: 28-39, 2004.2. Amstutz HC. Present state of metal-on-metal hybrid hip resurfacing. J Surg OrthopAdv 17: 12-16, 2008.3. Amstutz HC. The THARIES hip resurfacing technique. Orthop Clin North Am 13:813-832, 1982.4. Amstutz HC, Antonia<strong>de</strong>s JT, and <strong>Le</strong> Duff MJ. Results of metal-on-metal hybrid hipresurfacing for Crowe type-I and II <strong>de</strong>velopmental dysp<strong>la</strong>sia. J Bone Joint Surg Am 89: 339-346, 2007.5. Amstutz HC, Campbell PA, and <strong>Le</strong> Duff MJ. Fracture of the neck of the femur aftersurface arthrop<strong>la</strong>sty of the hip. J Bone Joint Surg Am 86-A: 1874-1877, 2004.6. Beau<strong>le</strong> PE, and Amstutz HC. Orientation of the femoral component in surfacearthrop<strong>la</strong>sty of the hip. J Bone Joint Surg Am 87: 1162, 2005.7. Beau<strong>le</strong> PE, Campbell PA, Hoke R, and Dorey F. Notching of the femoral neck<strong>du</strong>ring resurfacing arthrop<strong>la</strong>sty of the hip: a vascu<strong>la</strong>r study. J Bone Joint Surg Br 88: 35-39,2006.8. chiron p. Use of a gui<strong>de</strong> wire in hip resurfacing arthrop<strong>la</strong>sty. Osteologie 14: 65-68, 2005.9. Chiron p, and Laffosse JM. Prothèses <strong>total</strong>es <strong>de</strong> Hanche: <strong>le</strong>s choix. . Paris: 2005, p.257-262.10. Dumb<strong>le</strong>ton JH, and Man<strong>le</strong>y MT. Metal-on-Metal <strong>total</strong> hip rep<strong>la</strong>cement: what doesthe literature say? J Arthrop<strong>la</strong>sty 20: 174-188, 2005.11. Freeman MA. Total surface rep<strong>la</strong>cement hip arthrop<strong>la</strong>sty. Clin Orthop Re<strong>la</strong>t Res 2-4,1978.12. Howie DW, McGee MA, Costi K, and Graves SE. Metal-on-metal resurfacingversus <strong>total</strong> hip rep<strong>la</strong>cement-the value of a randomized clinical trial. Orthop Clin North Am36: 195-201, ix, 2005.13. Lavigne M, Parvizi J, Beck M, Siebenrock KA, Ganz R, and <strong>Le</strong>unig M. Anteriorfemoroacetabu<strong>la</strong>r impingement: part I. Techniques of joint preserving surgery. Clin OrthopRe<strong>la</strong>t Res 61-66, 2004.14. <strong>Le</strong> Duff MJ, Amstutz HC, and Dorey FJ. Metal-on-metal hip resurfacing for obesepatients. J Bone Joint Surg Am 89: 2705-2711, 2007.15. <strong>Le</strong>unig M, and Ganz R. Vascu<strong>la</strong>rity of the femoral head after Birmingham hipresurfacing. A technetium Tc 99m bone scan/sing<strong>le</strong> photon emission computed tomographystudy. J Arthrop<strong>la</strong>sty 22: 784-785; author reply 785-786, 2007.16. Marker DR, Sey<strong>le</strong>r TM, Jinnah RH, De<strong>la</strong>nois RE, Ulrich SD, and Mont MA.Femoral neck fractures after metal-on-metal <strong>total</strong> hip resurfacing: a prospective cohort study.J Arthrop<strong>la</strong>sty 22: 66-71, 2007.17. McBry<strong>de</strong> CW, Revell MP, Thomas AM, Treacy RB, and Pynsent PB. Theinfluence of surgical approach on outcome in birmingham hip resurfacing. Clin Orthop Re<strong>la</strong>tRes 466: 920-926, 2008.18. McMinn D, Treacy R, Lin K, and Pynsent P. Metal on metal surface rep<strong>la</strong>cement ofthe hip. Experience of the McMinn prothesis. Clin Orthop Re<strong>la</strong>t Res S89-98, 1996.19. Murray WR, and Van Meter JW. Surface rep<strong>la</strong>cement hip arthrop<strong>la</strong>sty: results ofthe first seventy-four consecutive cases at the University of California, San Francisco. Hip156-166, 1982.20. Naal FD, Maffiu<strong>le</strong>tti NA, Munzinger U, and Hersche O. Sports after hipresurfacing arthrop<strong>la</strong>sty. Am J Sports Med 35: 705-711, 2007.12
1321. Pol<strong>la</strong>rd TC, Baker RP, Eastaugh-Waring SJ, and Bannister GC. Treatment of theyoung active patient with osteoarthritis of the hip. A five- to seven-year comparison of hybrid<strong>total</strong> hip arthrop<strong>la</strong>sty and metal-on-metal resurfacing. J Bone Joint Surg Br 88: 592-600,2006.22. Schnurr C, Michael JW, Eysel P, and Konig DP. Image<strong>le</strong>ss navigation of hipresurfacing arthrop<strong>la</strong>sty increases the imp<strong>la</strong>nt accuracy. Int Orthop 2007.23. Steffen RT, Pandit HP, Pa<strong>la</strong>n J, Beard DJ, Gund<strong>le</strong> R, McLardy-Smith P, MurrayDW, and Gill HS. The five-year results of the Birmingham Hip Resurfacing arthrop<strong>la</strong>sty: ANINDEPENDENT SERIES. J Bone Joint Surg Br 90: 436-441, 2008.24. Treacy RB, McBry<strong>de</strong> CW, and Pynsent PB. Birmingham hip resurfacingarthrop<strong>la</strong>sty. A minimum follow-up of five years. J Bone Joint Surg Br 87: 167-170, 2005.25. Vendittoli PA, Ganapathi M, and Lavigne M. Blood and urine metal ion <strong>le</strong>vels inyoung and active patients after Birmingham hip resurfacing arthrop<strong>la</strong>sty. J Bone Joint Surg Br89: 989; author reply 989-990, 2007.26. Vendittoli PA, Mottard S, Roy AG, Dupont C, and Lavigne M. Chromium andcobalt ion re<strong>le</strong>ase following the Durom high carbon content, forged metal-on-metal surfacerep<strong>la</strong>cement of the hip. J Bone Joint Surg Br 89: 441-448, 2007.27. Wagner H. Surface rep<strong>la</strong>cement arthrop<strong>la</strong>sty of the hip. Clin Orthop Re<strong>la</strong>t Res 102-130, 1978.Légen<strong>de</strong>sFigure 1 : Resurfaçage <strong>total</strong> <strong>de</strong> <strong>la</strong> <strong>hanche</strong>.Figure 2 : <strong>Le</strong> <strong>resurfaçage</strong> <strong>de</strong> Freeman métal/polyéthylène.Figure 3 : Resurfaçage mo<strong>de</strong>rne métal/métal cupu<strong>le</strong> ciment, acétabulum press fit.Figure 4 : Systèmes <strong>de</strong> visée endoarticu<strong>la</strong>ires.Figure 5 : Visée par navigation.Figure 6 : Visée guidée par amplificateur .Figure 7 : La cupu<strong>le</strong> est située au centre <strong>du</strong> colFigure 8 : Voie minima<strong>le</strong> invasive antéro<strong>la</strong>téra<strong>le</strong>.Figure 9 : Resurfaçage <strong>total</strong>/Tige et grosse tête.Figure 10 : Fracture <strong>du</strong> col sur : os fragi<strong>le</strong> ( dialysé = contre indication )Figure 11 : Contre indication : acétabulum non rétentif.Figure 12 : Contre indication : col court, très réroversé.Figure 13 : 35 Ans, arthrose sur épiphysiolyse.Figure 14 : Resurfaçage avec correction <strong>de</strong> <strong>la</strong> malposition <strong>de</strong> <strong>la</strong> tête.