Simply Healthcare Plans, Inc
Simply Healthcare Plans, Inc
Simply Healthcare Plans, Inc

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong><br />
<strong>Simply</strong> Care (HMO SNP) H5471-008/<strong>Simply</strong> Comfort (HMO SNP) H5471-009<br />
Miami-Dade County<br />
2012 Formulary<br />
(List of Covered Drugs)<br />
PLEASE READ: THIS DOCUMENT CONTAINS INFORMATION ABOUT THE DRUGS WE<br />
COVER IN THIS PLAN<br />
Note to existing members: This formulary has changed since last year. Please review this document to<br />
make sure that it still contains the drugs you take.<br />
This document includes <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. partial formulary as of January 1, 2012. For a<br />
complete, updated formulary, please visit our Web site at www.mysimplymedicare.com or call 1-877-577-<br />
0115, Sunday, Monday, Tuesday, Wednesday, Thursday, Friday, Saturday, 8:00 a.m.-8:00p.m. Eastern.<br />
TTY/TDD users should call 711 Telecommunications Relay Services.<br />
Beneficiaries must use network pharmacies to access their prescription drug benefit. Benefits, formulary,<br />
pharmacy network, premium and/or copayments/coinsurance may change on January 1, 2013.<br />
“A Coordinated Care plan with a Medicare Advantage contract”<br />
To get this material in other formats or ask for language translation services, call <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>.<br />
Member Services at 1-877-577-0115 (TTY/TDD users only: 711 Telecommunications Relay Services), if you<br />
need plan information in another format.<br />
This information is available for free in other languages. Please contact our Member Service’s department at 1-<br />
877-577-0115 or 711 for TTY, for additional information.<br />
Esta información esta disponible de gratis en otros idiomas. Por favor llame a nuestro departamento de<br />
Servicios al Afiliados al 1-877-577-0115. Si usted usa un dispositivo TTY, por favor llame al 711.<br />
Formulary ID: 12487 Ver 5/ Formulary ID: 12488 Ver 5<br />
H5471_2012AForm_Retail CMS File & Use 08/29/2011<br />
i
What is the <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>.’s Formulary<br />
A formulary is a list of covered drugs selected by <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. in consultation with a team of<br />
health care providers, which represents the prescription therapies believed to be a necessary part of a quality<br />
treatment program. <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. will generally cover the drugs listed in our formulary as long<br />
as the drug is medically necessary, the prescription is filled at a <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. network<br />
pharmacy, and other plan rules are followed. For more information on how to fill your prescriptions, please<br />
review your Evidence of Coverage.<br />
This document is a partial formulary and includes only some of the drugs covered by <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>,<br />
<strong>Inc</strong>. For a complete listing of all prescription drugs covered by <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. , please visit our<br />
Web site at www.mysimplymedicare.com or call 1-877-577-0115, Sunday, Monday, Tuesday, Wednesday,<br />
Thursday, Friday, Saturday, 8:00 am – 8:00 pm Eastern. TTY/TDD users should call 711 Telecommunications<br />
Relay Services.<br />
Can the Formulary change<br />
Generally, if you are taking a drug on our 2012 formulary that was covered at the beginning of the year,<br />
we will not discontinue or reduce coverage of the drug during the 2012 coverage year except when a new,<br />
less expensive generic drug becomes available or when new adverse information about the safety or<br />
effectiveness of a drug is released. Other types of formulary changes, such as removing a drug from our<br />
formulary, will not affect members who are currently taking the drug. It will remain available at the same<br />
cost-sharing for those members taking it for the remainder of the coverage year. We feel it is important<br />
that you have continued access for the remainder of the coverage year to the formulary drugs that were<br />
available when you chose our plan, except for cases in which you can save additional money or we can<br />
ensure your safety.<br />
If we remove drugs from our formulary, or add prior authorization, quantity limits and/or step therapy<br />
restrictions on a drug or move a drug to a higher cost-sharing tier, we must notify affected members of the<br />
change at least 60 days before the change becomes effective, or at the time the member requests a refill of<br />
the drug, at which time the member will receive a 60-day supply of the drug. If the Food and Drug<br />
Administration deems a drug on our formulary to be unsafe or the drug’s manufacturer removes the drug<br />
from the market, we will immediately remove the drug from our formulary and provide notice to members<br />
who take the drug. The enclosed formulary is current as of January 1, 2012. To get updated information<br />
about the drugs covered by <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>., please visit our Web site at<br />
www.mysimplymedicare.com or call Member Services at 1-877-577-0115, Sunday, Monday, Tuesday,<br />
Wednesday, Thursday, Friday, Saturday, 8:00 am – 8:00 pm Eastern. TTY/TDD users should call 711<br />
Telecommunications Relay Services. In the event of a mid-year non-maintenance formulary change such<br />
as changing a preferred or non-preferred formulary drug, adding an additional requirement or limit to a<br />
drug, remove a dosage form, or exchanging therapeutic alternatives by adding or deleting a drug or<br />
changing a tier as a result of a therapeutic alternative, we will notify you by providing you with a written<br />
notice of the non-maintenance formulary change.<br />
How do I use the Formulary<br />
There are two ways to find your drug within the formulary:<br />
ii
Medical Condition<br />
The formulary begins on page 1. The drugs in this formulary are grouped into categories depending on the<br />
type of medical conditions that they are used to treat. For example, drugs used to treat a heart condition are<br />
listed under the category, “Cardiovascular Agents”. If you know what your drug is used for, look for the<br />
category name in the list that begins on page 1. Then look under the category name for your drug.<br />
Alphabetical Listing<br />
If you are not sure what category to look under, you should look for your drug in the Index that begins on<br />
page 46. The Index provides an alphabetical list of all of the drugs included in this document. Both brand<br />
name drugs and generic drugs are listed in the Index. Look in the Index and find your drug. Next to your<br />
drug, you will see the page number where you can find coverage information. Turn to the page listed in the<br />
Index and find the name of your drug in the first column of the list.<br />
What are generic drugs<br />
<strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. covers both brand name drugs and generic drugs. A generic drug is approved<br />
by the FDA as having the same active ingredient as the brand name drug. Generally, generic drugs cost less<br />
than brand name drugs.<br />
Are there any restrictions on my coverage<br />
Some covered drugs may have additional requirements or limits on coverage. These requirements and limits<br />
may include:<br />
<br />
Prior Authorization: <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. requires you or your physician to get prior<br />
authorization for certain drugs. This means that you will need to get approval from <strong>Simply</strong> <strong>Healthcare</strong><br />
<strong>Plans</strong>, <strong>Inc</strong>. before you fill your prescriptions. If you don’t get approval, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>.<br />
may not cover the drug.<br />
<br />
Quantity Limits: For certain drugs, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. limits the amount of the drug that<br />
<strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. limits will cover. For example, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. provides 30<br />
tablets per prescription for LIPITOR 10 MG TABLETS. This may be in addition to a standard one<br />
month or three month supply.<br />
<br />
Step Therapy: In some cases, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. requires you to first try certain drugs to<br />
treat your medical condition before we will cover another drug for that condition. For example, if Drug<br />
A and Drug B both treat your medical condition, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. may not cover Drug B<br />
unless you try Drug A first. If Drug A does not work for you, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. will then<br />
cover Drug B.<br />
You can find out if your drug has any additional requirements or limits by looking in the formulary that begins<br />
on page 1. You can also get more information about the restrictions applied to specific covered drugs by<br />
visiting our Web site at www.mysimplymedicare.com.<br />
iii
You can ask <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. to make an exception to these restrictions or limits. See the section,<br />
“How do I request an exception to the <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. formulary” on page iv for information<br />
about how to request an exception.<br />
What if my drug is not on the Formulary<br />
If your drug is not included in this list of covered drugs, you should first contact Member Services and ask if<br />
your drug is covered. This document includes only a partial list of covered drugs, so <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>,<br />
<strong>Inc</strong>. may cover your drug. You can contact Member Services at 1-877-577-0115, Sunday, Monday, Tuesday,<br />
Wednesday, Thursday, Friday, Saturday, 8:00 am – 8:00 pm Eastern. TTY/TDD users should call 711<br />
Telecommunications Relay Services.<br />
If you learn that <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. does not cover your drug, you have two options:<br />
<br />
You can ask Member Services for a list of similar drugs that are covered by <strong>Simply</strong> Complete (HMO<br />
SNP). When you receive the list, show it to your doctor and ask him or her to prescribe a similar drug<br />
that is covered by <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>.<br />
<br />
You can ask <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. to make an exception and cover your drug. See below for<br />
information about how to request an exception.<br />
How do I request an exception to the <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. Formulary<br />
You can ask <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. to make an exception to our coverage rules. There are several types<br />
of exceptions that you can ask us to make.<br />
<br />
You can ask us to cover your drug even if it is not on our formulary.<br />
<br />
You can ask us to waive coverage restrictions or limits on your drug. For example, for certain drugs,<br />
<strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. limits the amount of the drug that we will cover. If your drug has a<br />
quantity limit, you can ask us to waive the limit and cover more.<br />
<br />
You can ask us to provide a higher level of coverage for your drug. If your drug is contained in our nonpreferred<br />
brand tier, you can ask us to cover it at the cost-sharing amount that applies to drugs in the<br />
preferred brand tier instead. This would lower the amount you must pay for your drug. Please note, if<br />
we grant your request to cover a drug that is not on our formulary, you may not ask us to provide a<br />
higher level of coverage for the drug. “Also, you may not ask us to provide a higher level of coverage<br />
for drugs that are in the Tier 5, Specialty tier.”<br />
Generally, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. will only approve your request for an exception if the alternative drugs<br />
included on the plan’s formulary, the lower-tiered drug or additional utilization restrictions would not be as<br />
effective in treating your condition and/or would cause you to have adverse medical effects.<br />
You should contact us to ask us for an initial coverage decision for a formulary, tiering or utilization restriction<br />
exception. When you are requesting a formulary, tiering or utilization restriction exception you should<br />
iv
submit a statement from your prescriber’s or physician supporting your request. Generally, we must<br />
make our decision within 72 hours of getting your prescribing physician’s supporting statement. You can<br />
request an expedited (fast) exception if you or your doctor believe that your health could be seriously harmed by<br />
waiting up to 72 hours for a decision. If your request to expedite is granted, we must give you a decision no<br />
later than 24 hours after we get your prescriber’s or prescribing physician’s supporting statement.<br />
What do I do before I can talk to my doctor about changing my drugs or requesting an<br />
exception<br />
As a new or continuing member in our plan you may be taking drugs that are not on our formulary. Or, you may<br />
be taking a drug that is on our formulary but your ability to get it is limited. For example, you may need a prior<br />
authorization from us before you can fill your prescription. You should talk to your doctor to decide if you<br />
should switch to an appropriate drug that we cover or request a formulary exception so that we will cover the<br />
drug you take. While you talk to your doctor to determine the right course of action for you, we may cover your<br />
drug in certain cases during the first 90 days you are a member of our plan.<br />
For each of your drugs that is not on our formulary or if your ability to get your drugs is limited, we will cover a<br />
temporary 30-day supply (unless you have a prescription written for fewer days) when you go to a network<br />
pharmacy. After your first 30-day supply, we will not pay for these drugs, even if you have been a member of<br />
the plan less than 90 days.<br />
If you are a resident of a long-term care facility, we will allow you to refill your prescription until we have<br />
provided you with 93-day transition supply, consistent with dispensing increment, (unless you have a<br />
prescription written for fewer days). We will cover more than one refill of these drugs for the first 90 days you<br />
are a member of our plan. If you need a drug that is not on our formulary or if your ability to get your drugs is<br />
limited, but you are past the first 90 days of membership in our plan, we will cover a 31-day emergency supply<br />
of that drug (unless you have a prescription for fewer days) while you pursue a formulary exception.<br />
For current members who are changing from one treatment setting to another, for example entering a<br />
longterm care facility from a hospital or being discharged from a hospital to home, the member and provider<br />
will need to utilize our exception and appeals process should the drugs not be on our formulary. Members<br />
entering or being discharged from a long-term care facility will be allowed a one-time emergency supply of a<br />
31-day supply for medications which the member has not already received a transition supply. In addition,<br />
the dispensing pharmacist will need to call the Pharmacy Help Desk to receive appropriate directions to<br />
dispense a prescription required due to a level of care change.<br />
For more information<br />
For more detailed information about your <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. prescription drug coverage, please<br />
review your Evidence of Coverage and other plan materials.<br />
If you have questions about <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>., please call Member Services at 1-877-577-0115,<br />
Sunday, Monday, Tuesday, Wednesday, Thursday, Friday, Saturday, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommunications Relay Services. Or visit www.mysimplymedicare.com.<br />
If you have general questions about Medicare prescription drug coverage, please call Medicare at 1-800-<br />
MEDICARE (1-800-633-4227) 24 hours a day/7 days a week. TTY/TDD users should call 1-877-486-2048.<br />
Or, visit www.medicare.gov.<br />
v
<strong>Simply</strong>’s (HMO SNP) Formulary<br />
The abridged formulary below provides coverage information about some of the drugs covered by <strong>Simply</strong><br />
<strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. If you have trouble finding your drug in the list, turn to the Index that begins on page 46.<br />
Remember: This is only a partial list of drugs covered by <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. If your prescription is<br />
not in this partial formulary, please visit our Web site at www.mysimplymedicare.com or call Member Services<br />
at 1-877-577-0115, Sunday, Monday, Tuesday, Wednesday, Thursday, Friday, Saturday, 8:00 am – 8:00 pm<br />
Eastern. TTY/TDD users should call 711 Telecommunications Relay Services, for additional help.<br />
The first column of the chart lists the drug name. Brand name drugs are capitalized (e.g., LIPITOR 10 mg) and<br />
generic drugs are listed in lower-case italics (e.g., pravastatin sodium 10 mg).<br />
The information in the Requirements/Limits column tells you if <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. has any special<br />
requirements for coverage of your drug.<br />
ST<br />
PA<br />
BD<br />
QL<br />
SP<br />
E<br />
GC<br />
Step Therapy<br />
Prior Authorization<br />
BvD Prior Authorization, may be covered under Medicare Part B or Part D depending upon the<br />
circumstances. Information may need to be submitted describing the use setting of the drug to make the<br />
determination.<br />
Quantity Limit per 30 day supply<br />
This prescription may be available only at certain pharmacies. For more information consult your<br />
Pharmacy Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm<br />
Eastern. TTY/TDD users should call 711 Telecommunication Relay Services<br />
This prescription drug is not normally covered in a Medicare Prescription Drug Plan. The amount you<br />
pay when you fill a prescription for this drug does not count towards your total drug costs (that is, the<br />
amount you pay does not help you qualify for catastrophic coverage). In addition, if you are receiving<br />
extra help to pay for your prescriptions, you will not get any extra help to pay for this drug.<br />
We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
vi
Plan H5471-008 <strong>Simply</strong> Care (HMO SNP)<br />
Below is a chart showing your co-payment/co-insurance by drug tier.<br />
Formulary Drug Tier<br />
Copayment/Co-insurance at Retail<br />
Pharmacies<br />
Copayment/Co-insurance for 90<br />
day supply at retail pharmacies<br />
Tier 1 $0 $0<br />
Tier 2 $0 $0<br />
Tier 3 $10 $30<br />
Tier 4 $25 Limited to 30 day supply<br />
Tier 5 33% Limited to 30 day supply<br />
Plan H5471-009 <strong>Simply</strong> Comfort (HMO SNP)<br />
Below is a chart showing your co-payment/co-insurance by drug tier.<br />
Formulary Drug Tier<br />
Copayment/Co-insurance at Retail<br />
Pharmacies<br />
Copayment/Co-insurance for 90<br />
day supply at retail pharmacies<br />
Tier 1 $0 $0<br />
Tier 2 $0 $0<br />
Tier 3 $10 $30<br />
Tier 4 $25 Limited to 30 day supply<br />
Tier 5 33% Limited to 30 day supply<br />
vii
<strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong><br />
<strong>Simply</strong> Care (HMO SNP) H5471-008/ <strong>Simply</strong> Comfort (HMO SNP)<br />
H5471-009<br />
Condado de Miami-Dade<br />
Formulario de 2012<br />
(Lista de medicamentos cubiertos)<br />
LEA POR FAVOR: ESTE DOCUMENTO CONTIENE INFORMACIÓN SOBRE LOS<br />
MEDICAMENTOS QUE CUBRE ESTE PLAN<br />
Nota a los afiliados existentes: Este formulario ha cambiado desde el año pasado. Revise este documento<br />
para asegurarse de que sigue incluyendo los medicamentos que toma.<br />
Este documento contiene el formulario parcial de <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. actualizado al 1 de enero<br />
de 2012. Si desea el formulario completo y actualizado, visite nuestro sitio web en<br />
www.mysimplymedicare.com o llame al 1-877-577-0115. Se atiende domingos, lunes, martes, miércoles,<br />
jueves, viernes y sábados de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben<br />
marcar 711, el Centro de Enlace de Telecomunicaciones.<br />
Los beneficiarios deben usar las farmacias de la red para tener acceso a su beneficio de medicamentos recetados.<br />
El 1 de enero de 2013 podría haber cambios en los beneficios, el formulario, la red de farmacias, las primas, los<br />
copagos o el coaseguro.<br />
Una Organización Medicare Advantage con contrato con Medicare.<br />
Si desea este material o información del plan en otro formato, o si desea servicios de traducción de idiomas,<br />
comuníquese con el Departamento de Servicios para Afiliados de <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. llamando al 1-<br />
877-577-0115 (los usuarios con TTY/TDD deben marcar 711, el Centro de Enlace de Telecomunicaciones).<br />
Id. del Formulario: 12487, Ver. 5 / Id. del Formulario: 12488, Ver.5<br />
H5471_2012AForm_RetailBIL CMS File & Use 08/29/2011<br />
1
¿Qué es el Formulario de <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>.<br />
El formulario es una lista de medicamentos seleccionados cubiertos por <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. en<br />
colaboración con un equipo de proveedores de atención médica, que representa las terapias farmacológicas<br />
consideradas como parte necesaria de un programa de tratamiento de calidad. Por lo general, <strong>Simply</strong> <strong>Healthcare</strong><br />
<strong>Plans</strong>, <strong>Inc</strong>. cubrirá los medicamentos incluidos en nuestro formulario siempre y cuando se necesiten por razones<br />
médicas, el medicamento sea surtido en una farmacia de la red de <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>., y se hayan<br />
seguido otras reglas de cobertura. Si desea más información sobre cómo hacer para que le surtan sus<br />
medicamentos recetados, consulte su Evidencia de Cobertura.<br />
Este documento es un formulario parcial y solo incluye algunos de los medicamentos cubiertos por <strong>Simply</strong><br />
<strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. Si desea la lista completa de todos los medicamentos recetados cubiertos por <strong>Simply</strong><br />
<strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>., visite nuestro sitio web en www.mysimplymedicare.com o llame al 1-877-577-0115. Se<br />
atiende domingos, lunes, martes, miércoles, jueves, viernes y sábados de 8:00 a.m. a 8:00 p.m., hora del Este.<br />
Los usuarios con TTY/TDD deben marcar 711, el Centro de Enlace de Telecomunicaciones.<br />
¿Es posible que cambie el formulario<br />
Por lo general, si está tomando un medicamento de nuestro formulario de 2012 que estaba cubierto al<br />
principio del año, no lo descontinuaremos ni reduciremos su cobertura durante el año de cobertura 2012,<br />
excepto cuando un medicamento genérico nuevo y menos costoso se ponga a disposición, o cuando se<br />
publique nueva información adversa sobre la seguridad o efectividad de un medicamento. Otros tipos de<br />
cambios en el formulario, como el retiro de un medicamento de nuestro formulario, no afectará a los<br />
afiliados que están tomando actualmente el medicamento. Seguirá estando disponible con la misma<br />
participación de costos para aquellos afiliados que lo están tomando durante el resto del año de cobertura.<br />
Creemos que es importante que usted tenga acceso continuo durante el resto del año de la cobertura a los<br />
medicamentos del formulario que estaban disponibles cuando eligió nuestro plan, excepto en los casos en<br />
los que pueda ahorrar dinero o podamos garantizar su seguridad.<br />
Si retiramos medicamentos de nuestro formulario o añadimos autorizaciones previas, límites en las<br />
cantidades o restricciones en la terapia por fases en un medicamento, o trasladamos un medicamento a un<br />
nivel con distribución de costos más alta, debemos notificar a los afiliados afectados sobre el cambio<br />
cuando menos con 60 días de anticipación a que entre en vigencia. Alternativamente, daremos notificación<br />
cuando el afiliado solicite la repetición de la receta del medicamento, momento en el cual el afiliado<br />
recibirá un surtido de 60 días del medicamento en cuestión. Si la Administración de Alimentos y<br />
Medicamentos considera que un medicamento en nuestro formulario no es seguro, o el fabricante del<br />
medicamento lo retira del mercado, nosotros eliminaremos inmediatamente dicho medicamento de nuestro<br />
formulario y daremos aviso a los afiliados que lo usan. El formulario adjunto está actualizado al 1 de enero<br />
de 2012. Si desea información actualizada de los medicamentos cubiertos por <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>,<br />
<strong>Inc</strong>., visite nuestro sitio web en www.mysimplymedicare.com o comuníquese con el Departamento de<br />
Servicios para Afiliados llamando al 1-877-577-0115. Se atiende domingos, lunes, martes, miércoles,<br />
jueves, viernes y sábados de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben<br />
marcar 711, el Centro de Enlace de Telecomunicaciones. En caso de que se haga un cambio en el<br />
formulario de un medicamento que no sea de mantenimiento a mitad de año, como el cambio de un<br />
medicamento preferido o no preferido del formulario, añadir un requisito adicional o poner un límite a un<br />
medicamento, retirar una forma de dosis, o intercambiar alternativas terapéuticas agregando o eliminando<br />
un medicamento o cambiando un nivel como resultado de una alternativa terapéutica, se lo notificaremos<br />
mediante aviso por escrito del cambio en el formulario del medicamento que no es de mantenimiento.<br />
2
¿Cómo uso el formulario<br />
Hay dos maneras de encontrar su medicamento en el formulario.<br />
Afección<br />
El formulario comienza en la página 1. Los medicamentos en este formulario se agrupan en categorías en<br />
función del tipo de afecciones que tratan habitualmente. Por ejemplo, los medicamentos para tratar<br />
afecciones cardiacas se incluyen en la categoría “Agentes Cardiovasculares”. Si sabe para qué sirve su<br />
medicamento, busque el nombre de la categoría en la lista que comienza en la página 1. A continuación<br />
busque su medicamento en dicha categoría.<br />
Lista en orden alfabético<br />
Si no sabe a qué categoría corresponde su medicamento, deberá buscarlo en el Índice que comienza en la<br />
página 46.. El Índice ofrece una lista alfabética de todos los medicamentos incluidos en este documento. El<br />
Índice incluye tanto los medicamentos de marca como los genéricos. Busque en el Índice para encontrar su<br />
medicamento. Junto al medicamento, verá el número de la página que contiene la información sobre la<br />
cobertura. Vaya a la página indicada en el Índice y encuentre el nombre de su medicamento en la primera<br />
columna de la lista.<br />
¿Qué son los medicamentos genéricos<br />
<strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. cubre medicamentos genéricos y de marca. Un medicamento genérico recibirá<br />
la aprobación de la FDA si tiene el mismo ingrediente activo que el medicamento de marca. Por lo general,<br />
los medicamentos genéricos cuestan menos que los de marca.<br />
¿Hay restricciones en mi cobertura<br />
Algunos medicamentos cubiertos pueden tener requisitos adicionales o limitaciones en la cobertura. Estos<br />
requisitos y límites pueden incluir:<br />
<br />
Autorización Previa. <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. requiere que usted o su médico obtengan<br />
autorización previa para ciertos medicamentos. Esto significa que necesitará obtener aprobación de<br />
<strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. antes de que pueda surtir sus recetas. Si no obtiene la aprobación, es<br />
posible que <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. no cubra el medicamento.<br />
<br />
Límites en la Cantidad. Para ciertos medicamentos, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. limita la cantidad<br />
del medicamento que <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. va a cubrir. Por ejemplo, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>,<br />
<strong>Inc</strong>. proporciona 30 tabletas por receta del medicamento LIPITOR EN TABLETAS DE 10 MG. Esto<br />
puede ser adicional al suministro estándar de un mes o tres meses.<br />
<br />
Terapia por Fases. En algunos casos, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. requiere que usted pruebe primero<br />
ciertos medicamentos para tratar su condición médica antes de que demos cobertura a otro medicamento<br />
para dicha afección. Por ejemplo, si tanto el Medicamento A como el Medicamento B tratan su<br />
condición médica, es posible que <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. no cubra el Medicamento B a menos<br />
3
que usted pruebe primero el Medicamento A. Si el Medicamento A no funciona en su caso, <strong>Simply</strong><br />
<strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. cubrirá el Medicamento B.<br />
Usted puede consultar el formulario que comienza en la página 1 para determinar si su medicamento tiene<br />
requisitos o límites adicionales. También puede obtener más información sobre las restricciones que se aplican a<br />
medicamentos cubiertos específicos si visita nuestro sitio web en www.mysimplymedicare.com.<br />
Puede solicitar a <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. que haga una excepción a estas restricciones o límites. Consulte<br />
la sección “¿Cómo solicito una excepción en el formulario de <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>.” en la página 4<br />
para obtener información sobre cómo solicitar una excepción.<br />
¿Qué sucede si su medicamento no está en el formulario<br />
Si su medicamento no está incluido en esta lista de medicamentos cubiertos, debe comunicarse primero con el<br />
Departamento de Servicios para Afiliados para preguntar si está cubierto. Como este documento solo incluye<br />
una lista parcial de los medicamentos cubiertos, es posible que <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. cubra su<br />
medicamento. Puede comunicarse con el Departamento de Servicios para Afiliados llamando al 1-877-577-<br />
0115. Se atiende domingos, lunes, martes, miércoles, jueves, viernes y sábados de 8:00 a.m. a 8:00 p.m., hora<br />
del Este. Los usuarios con TTY/TDD deben marcar 711, el Centro de Enlace de Telecomunicaciones.<br />
Si se entera de que <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. no cubre su medicamento, usted tiene dos opciones:<br />
<br />
Puede solicitar al Departamento de Servicios para Afiliados que le dé una lista de medicamentos<br />
similares que estén cubiertos por <strong>Simply</strong> Care (HMO SNP). Cuando reciba la lista, muéstrela a su<br />
médico y pídale que le recete un medicamento similar que esté cubierto por <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>,<br />
<strong>Inc</strong>.<br />
<br />
Puede solicitar a <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. que haga una excepción a estas restricciones o límites.<br />
Consulte la sección que sigue para obtener información sobre cómo solicitar una excepción.<br />
¿Cómo solicito una excepción en el formulario de <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>.<br />
Puede solicitar a <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. que haga una excepción a nuestras reglas de cobertura. Hay<br />
varios tipos de excepciones que puede pedir.<br />
<br />
Puede solicitarnos que cubramos su medicamento aunque no esté incluido en nuestro formulario.<br />
<br />
Puede solicitarnos que cancelemos las restricciones o limitaciones en la cobertura para su medicamento.<br />
Por ejemplo, en algunos medicamentos, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. limita la cantidad que tendrá<br />
cobertura. Si su medicamento tiene un límite en la cantidad, puede solicitarnos que cancelemos dicha<br />
limitación y cubramos una mayor cantidad.<br />
<br />
Puede pedirnos que proporcionemos un nivel de cobertura más alto para su medicamento. Si su<br />
medicamento está incluido en nuestro nivel de medicamentos de marca no preferidos, puede solicitarnos<br />
que en su lugar lo cubramos en el nivel de participación de costos que se aplica a los medicamentos que<br />
4
están en el nivel de medicamentos de marca preferidos. Esto reduciría la cantidad que debe pagar por el<br />
medicamento. Tenga presente que si concedemos la solicitud de cubrir un medicamento que no se<br />
incluye en nuestro formulario, usted no puede pedirnos que demos un nivel de cobertura más alto para<br />
dicho medicamento. “Asimismo, no puede pedirnos que demos un nivel de cobertura más alto a los<br />
medicamentos que están en el Nivel 5, que corresponde a los medicamentos especiales.”<br />
Por lo general, <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. solo aprobará su solicitud para una excepción si los medicamentos<br />
alternativos incluidos en el formulario del plan, o el medicamento de nivel más bajo o las restricciones de uso<br />
adicional no son tan eficaces para tratar su afección o pueden ocasionar efectos médicos adversos.<br />
Debe comunicarse con nosotros para solicitar una decisión de cobertura inicial para una excepción en el<br />
formulario, el nivel o la limitación en el uso. Cuando solicite una excepción en el formulario, el nivel o la<br />
limitación en el uso, debe presentar una declaración de su médico, o de quien le receta, que respalde su<br />
solicitud. Por lo general, debemos tomar una decisión en un plazo de 72 horas a partir del momento en el que<br />
hayamos recibido la declaración de respaldo de su médico tratante. Usted puede solicitar una excepción<br />
acelerada (rápida) si su médico considera que una espera de 72 horas para una decisión puede perjudicar<br />
gravemente su salud. Si se concede acelerar su solicitud, debemos otorgarle una decisión antes de 24 horas a<br />
partir del momento en que recibamos la declaración de respaldo de su médico tratante o de quien le receta.<br />
¿Qué debo hacer antes de hablar con mi médico sobre el cambio de mis medicamentos o la<br />
solicitud de una excepción<br />
Si usted es afiliado nuevo o continúa en nuestro plan, podría estar tomando medicamentos que no están en<br />
nuestro formulario. O podría estar tomando un medicamento que está en nuestro formulario pero su capacidad<br />
para adquirirlo es limitada. Por ejemplo, podría necesitar una autorización previa de nuestra parte para poder<br />
surtir su receta. Debe hablar con su médico para decidir si debe cambiar a un medicamento apropiado que<br />
nosotros cubramos o solicitar una excepción en el formulario para que podamos cubrir el medicamento que está<br />
tomando. Mientras habla con su médico para determinar el mejor modo de actuar para usted, podríamos cubrir<br />
su medicamento en ciertos casos durante los primeros 90 días de su afiliación a nuestro plan.<br />
Para cada uno de sus medicamentos que no esté en nuestro formulario, o si su capacidad para adquirir sus<br />
medicamentos es limitada, daremos cobertura a un suministro temporal de 30 días (a menos que tenga una<br />
receta para un número menor de días) cuando vaya a una farmacia de la red. Después de su primer suministro<br />
de 30 días, nosotros no pagaremos estos medicamentos, incluso si usted ha estado afiliado al plan menos de 90<br />
días.<br />
Si reside en un establecimiento de atención médica prolongada, le permitiremos que surta su receta hasta que<br />
hayamos proporcionado un suministro de transición de 93 días, consistente con el incremento en el suministro,<br />
(a menos que su receta indique un número menor de días). Daremos cobertura a más de un surtido de estos<br />
medicamentos durante los primeros 90 días de su afiliación a nuestro plan. Si necesita un medicamento que no<br />
está en nuestro formulario, o si su capacidad para adquirir sus medicamentos es limitada, pero han pasado los<br />
primeros 90 días de su afiliación a nuestro plan, daremos cobertura a un suministro de emergencia de 31 días de<br />
dicho medicamento (a menos que su receta indique un número menor de días) mientras busca una excepción en<br />
el formulario.<br />
Para los afiliados actuales que están cambiando de un lugar de tratamiento a otro, por ejemplo, si después de<br />
estar en un hospital ingresan a un establecimiento de atención médica prolongada, o que regresan a su hogar<br />
después de ser dados de alta de un hospital, el afiliado y el proveedor deberán utilizar nuestro proceso de<br />
excepciones y apelaciones en caso de que los medicamentos no estén en nuestro formulario. Los afiliados que<br />
ingresan a un establecimiento de atención médica prolongada, o que salen de él, tendrán permitido un<br />
5
suministro único de emergencia de 31 días de los medicamentos para los cuales no hayan recibido aún un<br />
suministro de transición. Adicionalmente, el farmacéutico que surte la receta deberá comunicarse con el Centro de<br />
Ayuda para Farmacias con el fin de recibir instrucciones apropiadas para surtir una receta requerida debido a un<br />
cambio en el nivel de la atención.<br />
Si desea más información<br />
Si desea información detallada sobre su cobertura de medicamentos recetados de <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>.,<br />
consulte su Evidencia de Cobertura y demás documentos del plan.<br />
Si tiene preguntas sobre <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>., comuníquese con el Departamento de Servicios para<br />
Afiliados llamando al 1-877-577-0115. Se atiende domingos, lunes, martes, miércoles, jueves, viernes y<br />
sábados de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar 711, el Centro de<br />
Enlace de Telecomunicaciones. O visite www.mysimplymedicare.com.<br />
Si tiene alguna pregunta general sobre la cobertura de medicamentos recetados de Medicare, comuníquese con<br />
Medicare llamando al 1-800-MEDICARE (1-800-633-4227). Se atiende las 24 horas del día, los 7 días de la<br />
semana. Las personas con impedimentos auditivos pueden llamar al 1-877-486-2048 o visitar la página<br />
www.medicare.gov.<br />
Formulario de <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>.<br />
El formulario abreviado que se ofrece a continuación proporciona información de cobertura de algunos de los<br />
medicamentos cubiertos por <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. Si tiene problemas para encontrar su medicamento<br />
en la lista, diríjase al Índice que comienza en la página 46. Recuerde: Ésta es solo una lista parcial de los<br />
medicamentos recetados cubiertos por <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. Si su medicamento recetado no está en<br />
este formulario parcial, visite nuestro sitio web en www.mysimplymedicare.com o comuníquese con el<br />
Departamento de Servicios para Afiliados llamando al 1-877-577-0115. Se atiende domingos, lunes, martes,<br />
miércoles, jueves, viernes y sábados de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben<br />
marcar 711, el Centro de Enlace de Telecomunicaciones, para recibir más ayuda.<br />
En la primera columna del diagrama se incluye el nombre del medicamento. Los medicamentos de marca están<br />
con letras mayúsculas (por ejemplo, LIPITOR 10 mg), y los medicamentos genéricos se incluyen con letras<br />
minúsculas en itálica (por ejemplo, pravastatin sodium 10 mg).<br />
La información en la columna de requisitos y límites indica si <strong>Simply</strong> <strong>Healthcare</strong> <strong>Plans</strong>, <strong>Inc</strong>. tiene algún<br />
requisito especial para dar cobertura a su medicamento.<br />
ST<br />
PA<br />
BD<br />
QL<br />
SP<br />
6<br />
Terapia por fases.<br />
Autorización previa.<br />
Autorización Previa BvD, podría tener cobertura con la Parte B o la Parte D de Medicare dependiendo<br />
de las circunstancias. Puede ser necesario enviar información sobre el uso del medicamento y la<br />
situación específica para tomar una determinación.<br />
Límite en la Cantidad por suministro de 30 días.<br />
Este medicamento recetado solo podría estar disponible en algunas farmacias. Si desea más<br />
información, consulte su Directorio de Farmacias o comuníquese con el Departamento de Servicios
E<br />
GC<br />
para Afiliados llamando al 1-877-577-0115. Se atiende los siete días de la semana de 8:00 a.m. a 8:00<br />
p.m., hora del Este. Los usuarios con TTY/TDD deben marcar 711, el Centro de Enlace de<br />
Telecomunicaciones.<br />
Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de<br />
Medicare. La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en<br />
cuenta en su costo total de medicamentos (es decir, la cantidad que paga no le ayuda a reunir los<br />
requisitos para la cobertura por catástrofe). Además, si está recibiendo ayuda adicional para pagar sus<br />
medicamentos, no obtendrá ningún otro tipo de ayuda adicional para pagar este medicamento.<br />
Proporcionamos cobertura adicional de este medicamento recetado durante la brecha en la cobertura.<br />
Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
7
<strong>Simply</strong> Care (HMO SNP) A continuación se ofrece una tabla con el copago o coaseguro por<br />
nivel de medicamento.<br />
Nivel del medicamento en el<br />
formulario<br />
Copago o coaseguro en farmacias<br />
minoristas<br />
Copago o coaseguro para<br />
pedido por correo y suministro<br />
de 90 días en farmacias<br />
minoristas<br />
Nivel 1 $0 $0<br />
Nivel 2 $0 $0<br />
Nivel 3 $10 $30<br />
Nivel 4 $25 Limitado a un suministro de 30<br />
días<br />
Nivel 5 33% Limitado a un suministro de 30<br />
días<br />
<strong>Simply</strong> Comfort (HMO SNP) A continuación se ofrece una tabla con el copago o coaseguro<br />
por nivel de medicamento.<br />
Nivel del medicamento en el<br />
formulario<br />
Copago o coaseguro en farmacias<br />
minoristas<br />
Copago o coaseguro para<br />
pedido por correo y suministro<br />
de 90 días en farmacias<br />
minoristas<br />
Nivel 1 $0 $0<br />
Nivel 2 $0 $0<br />
Nivel 3 $10 $30<br />
Nivel 4 $25 Limitado a un suministro de 30<br />
días<br />
Nivel 5 33% Limitado a un suministro de 30<br />
días<br />
8
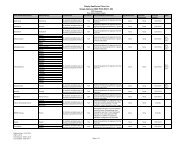
Drug Name Tier Notes<br />
ANALGESICS<br />
Nonsteroidal Anti-inflammatory Drugs<br />
ARTHROTEC 4<br />
CELEBREX 100, 200 MG 3 QL 60 ST<br />
CELEBREX 50, 400 MG 3 QL 62/31 ST<br />
diclofenac potassium 2<br />
diclofenac sodium 2<br />
diflunisal 2<br />
etodolac 2<br />
FELDENE 4<br />
fenoprofen calcium 2<br />
FLECTOR 4<br />
flurbiprofen 2<br />
ibuprofen 1 GC<br />
INDOCIN 4<br />
indomethacin 1 GC<br />
ketoprofen 1 GC<br />
ketoprofen er 2<br />
ketorolac tromethamine inj 1 GC<br />
ketorolac tromethamine tab 1 QL 20/5 GC<br />
meclofenamate sodium 2<br />
meloxicam susp 1 QL 300 GC<br />
meloxicam tab 1 QL 30 GC<br />
MOBIC 4 PA<br />
nabumetone 2<br />
NALFON 4<br />
NAPRELAN 4<br />
NAPROSYN 4<br />
naproxen 1 GC<br />
oxaprozin 2<br />
oxycodone hcl/ibuprofen 2<br />
piroxicam 1 GC<br />
sulindac 2<br />
tolmetin sodium 2<br />
Opioid Analgesics<br />
apap/cod 300-15 mg tab 2 QL 403/31<br />
apap/cod 300-30 mg tab 2 QL 372/31<br />
apap/cod 300-60 mg tab 2 QL 180<br />
apap/cod sol 2<br />
ascomp/codeine 2<br />
astramorph 1 GC<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
1
Drug Name Tier Notes<br />
butalbital/apap/caff 1 E GC<br />
co-gesic 2 QL 240<br />
duramorph 1 GC<br />
EMBEDA 3 QL 90<br />
endocet 2 QL 372<br />
endocet 10-650 mg 2 QL 186<br />
endocet 7.5-500 mg 2 QL 248<br />
fentanyl lozenge 5 PA<br />
fentanyl lozenge 0.2 mg 2 PA<br />
fentanyl transdermal patch 2 QL 10<br />
FENTORA 5 PA<br />
FIORICET/CODEINE 4 PA<br />
FIORINAL/CODEINE 3<br />
hydroco/apap 10-325 mg 1 QL 186/31 GC<br />
hydroco/apap 10-500 mg 1 QL 248/31 GC<br />
hydroco/apap 10-650 mg 1 QL 186/31 GC<br />
hydroco/apap 10-660 mg 1 QL 186/31 GC<br />
hydroco/apap 2.5-500 mg 1 QL 248/31 GC<br />
hydroco/apap 5-325 mg 1 QL 372/31 GC<br />
hydroco/apap 5-500 mg 1 QL 248/31 GC<br />
hydroco/apap 7.5-325 mg 1 QL 372/31 GC<br />
hydroco/apap 7.5-500 mg 1 QL 248/31 GC<br />
hydroco/apap 7.5-650 mg 1 QL 186/31 GC<br />
hydroco/apap 7.5-750 mg 1 QL 155/31 GC<br />
hydroco/apap sol 1 GC<br />
hydroco/ibuprofen 2 QL 155/31<br />
hydromorphone hcl 1 GC<br />
infumorph 4<br />
KADIAN CR 10, 50, 80 MG 3 QL 90<br />
KADIAN CR 100, 200 MG 3 QL 180<br />
KADIAN CR 20, 30, 60 MG 3 QL 120<br />
levorphanol 1 GC<br />
LORCET 4 PA<br />
LORTAB 4 PA<br />
MAGNACET 4<br />
margesic-h 2<br />
MAXIDONE 4<br />
methadone hcl 2<br />
methadose 2<br />
morphine sulfate 2<br />
morphine sulfate inj 1 GC<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
2
Drug Name Tier Notes<br />
MS CONTIN 4 PA<br />
nalbuphine hcl 1 GC<br />
NORCO 4 PA<br />
NUCYNTA 4<br />
ONSOLIS 4 PA<br />
OPANA 4<br />
OPANA ER 30 MG 3 QL 90<br />
OPANA ER 5, 10, 20, 40 MG 3 QL 120<br />
ORAMORPH 4<br />
orphenadrine/asa/caff 2<br />
oxycodone hcl 2<br />
OXYCODONE HCL SOL 4<br />
oxycodone/apap 2 QL 372/31<br />
oxycodone/apap 7.5-500mg 2 QL 248/31<br />
OXYCONTIN CR 4 PA QL 120<br />
OXYCONTIN CR 80 MG 4 PA QL 180<br />
oxymorphone 2<br />
PANLOR SS 4<br />
pentazocine/apap 2 QL 180<br />
PERCOCET 4 PA<br />
PERCODAN 4 PA<br />
repan 1 E GC<br />
roxicet 5-325 mg tab 2 QL 372/31<br />
roxicet 5-500 mg tab 2 QL 248/31<br />
roxicet sol 2<br />
ROXICODONE 15, 30 MG TAB 4<br />
roxicodone 5mg tab 2 PA<br />
RYZOLT 4 ST<br />
stagesic 2<br />
tramadol hcl 1 QL 240 GC<br />
tramadol hcl er 2 QL 240 ST<br />
tramadol hcl/apap 2 QL 240<br />
ANESTHETICS<br />
Local Anesthetics<br />
lidocaine 1 GC<br />
lidocaine/prilocaine 2<br />
LIDODERM 4 PA QL 90/30<br />
ANTIBACTERIALS<br />
Aminoglycosides<br />
ak-tob 1 GC<br />
gentak 2<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
3
Drug Name Tier Notes<br />
gentamicin 1 GC<br />
gentamicin/nacl 100 mg 1 GC<br />
gentamicin/nacl 60, 80 mg 2<br />
gentasol 1 GC<br />
kanamycin sulfate 1 GC<br />
neomycin sulfate 2<br />
paromomycin 2<br />
tobramycin inj 2<br />
tobramycin sulfate 1 GC<br />
tobrasol 1 GC<br />
Antibacterials, Other<br />
acetic acid 2<br />
baciim 2<br />
bacitracin 1 GC<br />
CHANTIX 0.5 MG 4 QL 11<br />
clindamycin hcl 2<br />
clindamycin phosphate 2<br />
colistimethate sodium 2 BD<br />
FLAGYL 4<br />
HIPREX 4<br />
LINCOCIN 4<br />
MACROBID 4<br />
MACRODANTIN 4<br />
methenamine hippurate 2<br />
METROCREAM 4<br />
METROGEL 4<br />
METROLOTION 4<br />
metronidazole cap, tab 1 GC<br />
metronidazole crm 2<br />
mupirocin 2<br />
nitrofurantoin 2<br />
nitrofurantoin macrocrystal 2<br />
nitrofurantoin monohydrate 2<br />
NORITATE 4<br />
trimethoprim 1 GC<br />
VANCOCIN HCL CAP 5<br />
VANCOCIN HCL INJ 3 BD<br />
vancomycin hcl 2 BD<br />
vandazole 2<br />
ZYVOX 5<br />
Beta-lactam, Cephalosporins<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
4
Drug Name Tier Notes<br />
cefaclor 2<br />
cefazolin sodium 1 GC<br />
cefdinir 2<br />
cefepime 1 GC<br />
cefoxitin sodium 1 GC<br />
cefpodoxime 2<br />
ceftriaxone sodium 1 GC<br />
cefuroxime axetil 1 GC<br />
cefuroxime sodium 1 GC<br />
cephalexin 1 GC<br />
FORTAZ 2<br />
KEFLEX 4<br />
ROCEPHIN 4<br />
SPECTRACEF 4<br />
SUPRAX 4<br />
ZINACEF 4<br />
Beta-lactam, Other<br />
AZACTAM IN DEXTROSE 3<br />
INVANZ 2<br />
MERREM 3<br />
PRIMAXIN 2<br />
Beta-lactam, Penicillins<br />
amoxicillin 200mg chw tab 3<br />
amoxicillin cap, susp, tab 1 GC<br />
amoxicillin/clavulanate p 2<br />
ampicillin 1 GC<br />
ampicillin/sulbactam 10-5 gm 2 BD<br />
dicloxacillin sodium 2<br />
MOXATAG 4<br />
nafcillin 1, 10 gm 1 GC<br />
nafcillin 20 mg/ml 2<br />
OXACILLIN INJ 1 GC<br />
OXACILLIN DEX INJ 2<br />
penicillin g potassium 1 GC<br />
penicillin g sodium 1 GC<br />
penicillin v potassium 1 GC<br />
PFIZERPEN 1 GC<br />
piperacillin sodium 1 GC<br />
Macrolides<br />
azithromycin 2<br />
erythrocin stearate 2<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
5
Drug Name Tier Notes<br />
erythromycin 1 GC<br />
erythromycin ethylsuccinate 2<br />
erythromycin/sulfisoxazole 1 GC<br />
KETEK 4<br />
PCE 4<br />
romycin 1 GC<br />
Quinolones<br />
ciprofloxacin 1 GC<br />
IQUIX 4<br />
LEVAQUIN INJ, TAB 4<br />
LEVAQUIN SOL, PREMIX 3<br />
NOROXIN 4<br />
OCUFLOX 4<br />
ofloxacin 2<br />
PROQUIN 4<br />
Sulfonamides<br />
KLARON 4<br />
SILVADENE 4<br />
silver sulfadiazine 1 GC<br />
ssd 1 GC<br />
sulfadiazine 2<br />
sulfamethoxazole/trimetho 1 GC<br />
thermazene 1 GC<br />
Tetracyclines<br />
doxycycline 10 mg/ml inj 1 GC BD<br />
doxycycline hyclate 1 GC<br />
doxycycline monohydrate 1 GC<br />
MINOCIN 4 PA<br />
minocycline 2<br />
MONODOX 4<br />
ORACEA 4 PA<br />
PERIOSTAT 4<br />
SOLODYN 105 MG 3<br />
SOLODYN 45, 90, 135 MG 4 PA<br />
SOLODYN 65, 115 MG 3 PA<br />
tetracycline hcl 1 GC<br />
ANTICONVULSANTS<br />
Anticonvulsants, Other<br />
KEPPRA 4<br />
KEPPRA XR 500 MG 4 PA<br />
levetiracetam 2<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
6
Drug Name Tier Notes<br />
phenobarbital 1 E GC<br />
primidone 2<br />
Calcium Channel Modifying Agents<br />
CELONTIN 4<br />
ethosuximide 2<br />
LYRICA 4 QL 90<br />
zonisamide 2<br />
Gamma-aminobutyric Acid (GABA) Augmenting Agents<br />
divalproex sodium 2<br />
gabapentin 2<br />
GABITRIL 12 MG 4 QL 120<br />
GABITRIL 2, 16 MG 4 QL 60<br />
GABITRIL 4 MG 4<br />
MYSOLINE 4 PA<br />
NEURONTIN 4 PA<br />
NEURONTIN SOL 4<br />
SABRIL 500 MG TAB 5 PA QL 186/31<br />
SABRIL SOL 5 PA<br />
valproate sodium 1 GC<br />
valproic acid 2<br />
Glutamate Reducing Agents<br />
FELBATOL 4<br />
LAMICTAL 4<br />
LAMICTAL KIT 3<br />
lamotrigine 2<br />
lamotrigine 150, 200 mg 2 QL 90<br />
topiramate cap 2<br />
Sodium Channel Agents<br />
BANZEL 200 MG TAB 4 PA QL 480<br />
BANZEL 400 MG TAB 4 PA QL 240<br />
carbamazepine 1 GC<br />
CARBATROL 100, 200 MG 4 QL 30<br />
CARBATROL 300 MG 4 QL 160<br />
DILANTIN INFATABS 4<br />
fosphenytoin sodium 1 GC<br />
oxcarbazepine 2<br />
PEGANONE 4<br />
PHENYTEK 3<br />
phenytoin 1 GC<br />
phenytoin er 200mg cap 2<br />
phenytoin susp 2<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
7
Drug Name Tier Notes<br />
TEGRETOL 4<br />
VIMPAT INJ, ORAL SOL 4 QL 1200<br />
VIMPAT TAB 4 QL 60<br />
Sodium Channel Inhibitors<br />
BANZEL SUSP 4<br />
ANTIDEMENTIA AGENTS<br />
Cholinesterase Inhibitors<br />
ARICEPT 4<br />
donepezil 2<br />
EXELON 3 QL 31/31<br />
galantamine 12 mg tab 2 QL 62/31<br />
galantamine 4 mg tab 2<br />
galantamine 8 mg tab 2 QL 30<br />
galantamine er cap 2 QL 31/31<br />
RAZADYNE 4 PA QL 180<br />
Glutamate Pathway Modifiers<br />
NAMENDA SOL 3 QL 360<br />
NAMENDA TAB 3 QL 60<br />
ANTIDEPRESSANTS<br />
Antidepressants, Other<br />
ABILIFY DISCMELT 4 PA<br />
ABILIFY INJ 4 PA QL 120<br />
ABILIFY SOL 4 PA<br />
ABILIFY TAB 4 PA QL 30<br />
APLENZIN 4 QL 30 ST<br />
budeprion 2<br />
bupropion 2<br />
bupropion sr 100 mg tab 2<br />
bupropion sr 150 mg tab 2 QL 62/31<br />
bupropion sr 200 mg tab 2 QL 60<br />
maprotiline hcl 2<br />
mirtazapine 2<br />
nefazodone hcl 1 GC<br />
OLEPTRO 4<br />
paroxetine er 12.5 mg tab 2 QL 180<br />
SEROQUEL XR 3 QL 60<br />
SYMBYAX 4 QL 30<br />
trazodone hcl 1 GC<br />
Monoamine Oxidase Inhibitors<br />
EMSAM 4 QL 31/31<br />
MARPLAN 4<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
8
Drug Name Tier Notes<br />
PARNATE 4<br />
phenelzine 2<br />
tranylcypromine sulfate 2<br />
Serotonin/Norepinephrine Reuptake Inhibitors<br />
citalopram 10 mg tab 1 QL 60 GC<br />
citalopram 20 mg tab 1 QL 90 GC<br />
citalopram 40 mg tab 1 QL 30 GC<br />
citalopram sol 1 GC<br />
CYMBALTA 20, 30 MG 3 QL 62/31<br />
CYMBALTA 60 MG 3 QL 31/31<br />
fluoxetine 10 mg cap 2 QL 240<br />
fluoxetine 20 mg cap 2 QL 120<br />
fluoxetine 40 mg cap 2 QL 60<br />
fluoxetine sol, tab 2<br />
fluvoxamine maleate 2 QL 90<br />
LEXAPRO SOL 3 QL 600<br />
LEXAPRO TAB 3 QL 30<br />
LUVOX 4<br />
paroxetine er 25 mg tab 2 QL 90<br />
paroxetine er 37.5 mg tab 2<br />
PAXIL 4<br />
PRISTIQ 4 QL 30<br />
PROZAC 4 PA<br />
PROZAC WEEKLY 4<br />
SARAFEM 4<br />
selfemra 4<br />
venlafaxine 2<br />
venlafaxine er 150 mg tab 2 QL 60<br />
venlafaxine er 225 mg tab 2 QL 30<br />
venlafaxine er 37.5,75 mg tab 2 QL 90<br />
VIIBRYD 4<br />
Tricyclics<br />
amitriptyline hcl 1 GC<br />
amoxapine 2<br />
chlordiazepoxide/amitript 2<br />
clomipramine hcl 2<br />
desipramine hcl 2<br />
doxepin hcl 1 GC<br />
imipramine hcl 1 GC<br />
imipramine pamoate 2<br />
NORPRAMIN 4<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
9
Drug Name Tier Notes<br />
nortriptyline hcl 1 GC<br />
PAMELOR 4 PA<br />
perphenazine/amitriptylin 2<br />
protriptyline hcl 2<br />
SURMONTIL 4<br />
ANTIDOTES, DETERRENTS, AND TOXICOLOGICAL AGENTS<br />
Antidotes<br />
EXJADE 125 MG TAB 4 PA<br />
EXJADE 250, 500 MG TAB 5 PA<br />
fomepizole 1 GC<br />
Deterrents<br />
ANTABUSE 4<br />
CHANTIX 1 MG 4 QL 180<br />
CHANTIX PAK 4 QL 53<br />
NICOTROL 4<br />
Toxicological Agents<br />
buprenorphine 2<br />
naloxone hcl 1 GC<br />
naltrexone hcl 2<br />
pentazocine/naloxone hcl 2<br />
SUBOXONE 4<br />
ANTIEMETICS<br />
Antiemetics<br />
CELLCEPT INJ 4 BD<br />
chlorpromazine 10, 25mg tab 2 BD<br />
chlorpromazine inj, tab 2<br />
diphenhydramine hcl 1 GC<br />
dronabinol 10 mg 2 QL 60 BD<br />
dronabinol 2.5, 5 mg 2 BD<br />
EMEND 125 MG 4 QL 2/31<br />
EMEND 40 MG 4 QL 1/31<br />
EMEND 80 MG 4 QL 2/21<br />
EMEND PAK 4 QL 6/31<br />
granisetron 0.1mg/ml inj, tab 1 QL 60 GC BD<br />
granisetron 1mg/ml inj 1 GC BD<br />
GRANISOL 2 BD<br />
hydroxyzine hcl 2<br />
hydroxyzine pamoate 1 GC<br />
MARINOL 4 PA<br />
meclizine hcl 2<br />
metoclopramide hcl 1 GC<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
10
Drug Name Tier Notes<br />
METOZOLV 4 ST<br />
ondansetron inj 2 QL 160 BD<br />
ondansetron 24 mg tab 2 QL 30 BD<br />
ondansetron 4 mg tab 2 BD<br />
ondansetron 8 mg tab 2 QL 60 BD<br />
ondansetron odt 2 QL 60 BD<br />
ondansetron sol 1 GC BD<br />
perphenazine 2<br />
phenadoz 2<br />
PHENERGAN 4<br />
prochlorperazine 1 GC<br />
prochlorperazine edisylate 1 GC<br />
prochlorperazine maleate 1 GC BD<br />
promethazine hcl 2<br />
promethegan 2<br />
SANCUSO 4 QL 2/21 BD<br />
ANTIFUNGALS<br />
Antifungals<br />
amphotericin b 2 BD<br />
ANCOBON 4<br />
ciclopirox 2<br />
clotrimazole 2<br />
econazole nitrate 2<br />
fluconazole 1 GC<br />
fluconazole 2 mg/ml inj 1 GC BD<br />
GRIFULVIN V 4<br />
GRIS-PEG 4<br />
griseofulvin microsize 2<br />
GYNAZOLE-1 4<br />
itraconazole 2<br />
ketoconazole 2<br />
LAMISIL 4<br />
LOPROX GEL 4 PA<br />
LOPROX SHAMPOO 4<br />
miconazole 2<br />
MYCAMINE 5<br />
NAFTIN 3<br />
NATACYN 4<br />
NIZORAL 4<br />
NOXAFIL 5 PA<br />
nyamyc 2<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
11
Drug Name Tier Notes<br />
nystatin 1 GC<br />
nystatin powder, tab 2<br />
nystop 2<br />
ORAVIG 3<br />
OXISTAT 4<br />
pedi-dri 2<br />
PENLAC NAIL LACQUER 4<br />
SPORANOX 4 PA<br />
terbinafine 2 PA<br />
terconazole 2<br />
zazole 2<br />
ZOLINZA 5 PA QL 120<br />
ANTIGOUT AGENTS<br />
Antigout Agents<br />
allopurinol 1 GC<br />
COLCRYS 3<br />
probenecid 2<br />
ULORIC 3 PA QL 30<br />
ANTIINFLAMMATORIES<br />
Glucocorticoids<br />
dexamethasone 1 GC<br />
dexamethasone sod phos 1 GC<br />
methylprednisolone 1 GC<br />
methylprednisolone ac 2<br />
MILLIPRED 4<br />
ORAPRED 4<br />
PEDIAPRED 4<br />
prednisolone sod phosp 1 GC<br />
prednisone 1 GC<br />
SOLU-CORTEF 4<br />
SOLU-MEDROL 4<br />
ANTIMIGRAINE AGENTS<br />
Abortive Agents<br />
dihydroergotamine mesylate 1 GC<br />
FROVA 4<br />
IMITREX 4 PA<br />
MAXALT 4<br />
migergot 2<br />
MIGRANAL 4<br />
RELPAX 4 QL 9<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
12
Drug Name Tier Notes<br />
sumatriptan succ inj 2 QL 10<br />
sumatriptan succ tab 2 QL 18<br />
Prophylactic Agents<br />
timolol maleate 1 GC<br />
topiramate 50 mg tab 2 QL 240<br />
topiramate tab 2 QL 60<br />
ANTIMYASTHENIC AGENTS<br />
Parasympathomimetics<br />
MESTINON 4<br />
MESTINON 60 MG TAB 4 PA<br />
MYTELASE 4<br />
pyridostigmine bromide 2<br />
ANTIMYCOBACTERIALS<br />
Antimycobacterials, Other<br />
dapsone 2<br />
MYCOBUTIN 4<br />
Antituberculars<br />
CAPASTAT SULFATE 4<br />
ethambutol hcl 2<br />
isonarif 2<br />
isoniazid 1 GC<br />
MYAMBUTOL 4<br />
PASER 3<br />
PRIFTIN 4<br />
pyrazinamide 2<br />
rifampin 2<br />
TRECATOR 4<br />
ANTINEOPLASTICS<br />
Alkylating Agents<br />
BUSULFEX 4 BD<br />
CEENU 4<br />
cyclophosphamide 2 BD<br />
HEXALEN 5<br />
LEUKERAN 3<br />
MATULANE 5<br />
melphalan 1 GC BD<br />
SEROMYCIN 4<br />
Antiangiogenic Agents<br />
REVLIMID 5 PA QL 30 SP<br />
THALOMID 5 PA QL 30<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
13
Drug Name Tier Notes<br />
THALOMID 200 MG 5 PA QL 60<br />
Antiestrogens/Modifiers<br />
EMCYT 4<br />
FARESTON 4 QL 30<br />
tamoxifen citrate 2<br />
Antimetabolites<br />
HYDREA 4<br />
hydroxyurea 2<br />
TABLOID 3<br />
Antineoplastics, Other<br />
ALIMTA 5 BD<br />
amifostine 5 BD<br />
AVASTIN 5 PA<br />
bleomycin sulfate 1 GC BD<br />
DOCETAXEL 5<br />
ELITEK 5<br />
GEMZAR 5 BD<br />
HALAVEN 5<br />
HERCEPTIN 5<br />
IDAMYCIN 5 BD<br />
idarubicin hcl 5 BD<br />
IFEX 4 BD<br />
IFOSFAMIDE 50 MG/ML 1 GC BD<br />
IFOSFAMIDE/MESNA 1 GM 2<br />
IFOSFAMIDE/MESNA 3 GM 3 BD<br />
irinotecan hcl inj 1 GC<br />
IXEMPRA 5<br />
leucovorin inj 1 GC BD<br />
leucovorin tab 2<br />
LEUSTATIN 2 BD<br />
mesna inj 2 BD<br />
MESNEX INJ 5 BD<br />
MESNEX TAB 4<br />
mitoxantrone hcl 2 BD<br />
MUSTARGEN 4 BD<br />
NIPENT 5 BD<br />
NOVANTRONE 5 BD<br />
ONTAK 5<br />
oxaliplatin inj 1 GC BD<br />
paclitaxel 1 GC BD<br />
pentostatin inj 2 BD<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
14
Drug Name Tier Notes<br />
PHOTOFRIN 5<br />
PREZISTA 4<br />
PROLEUKIN 5<br />
TAXOTERE 80 MG/2ML INJ 5<br />
TAXOTERE 80 MG/4ML INJ 4<br />
TRISENOX 4 BD<br />
VELCADE 5 PA<br />
VIDAZA 5 PA<br />
Aromatase Inhibitors, 3rd Generation<br />
anastrozole 5<br />
ARIMIDEX 3 QL 30<br />
exemestane 2<br />
letrozole 2<br />
Enzyme Inhibitors<br />
etoposide 1 GC BD<br />
HYCAMTIN 5 BD<br />
Molecular Target Inhibitors<br />
AFINITOR 2.5 MG 3<br />
AFINITOR 5 MG, 10 MG 5 PA QL 30<br />
GLEEVEC 100 MG 5 PA QL 120<br />
GLEEVEC 400 MG 5 PA QL 60<br />
IRESSA 5 QL 30<br />
ISTODAX 4 PA<br />
NEXAVAR 5 PA QL 120 SP<br />
SPRYCEL 100 MG 5 PA QL 30<br />
SPRYCEL 20, 50, 70 MG 5 PA QL 60<br />
SPRYCEL 80, 140 MG 5 PA<br />
SUTENT 5 PA QL 30<br />
TARCEVA 5 PA QL 30<br />
TASIGNA 5 PA QL 120<br />
TYKERB 5 PA QL 150<br />
VANDETANIB 5<br />
VOTRIENT 5 PA QL 120<br />
Monoclonal Antibodies<br />
ARZERRA 5 QL 400 BD<br />
CAMPATH 5<br />
RITUXAN 5 PA<br />
Retinoids<br />
PANRETIN 5<br />
TARGRETIN 5 PA<br />
TRETINOIN 3 PA<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
15
Drug Name Tier Notes<br />
ANTIPARASITICS<br />
Anthelmintics<br />
ALBENZA 3<br />
mebendazole 2<br />
STROMECTOL 4<br />
Antiprotozoals<br />
chloroquine phosphate 2<br />
DARAPRIM 4<br />
hydroxychloroquine sulfate 2<br />
LACRISERT 4<br />
MALARONE 4<br />
mefloquine hcl 2<br />
MEPRON 5<br />
NEBUPENT 4 QL 6/28 BD<br />
PENTAM 4 BD<br />
PLAQUENIL 4<br />
Pediculicides/ Scabicides<br />
acticin 1 GC<br />
EURAX 4<br />
lindane 2<br />
malathion 2<br />
OVIDE 4<br />
permethrin 2<br />
ANTIPARKINSON AGENTS<br />
Antiparkinson Agents<br />
amantadine 2<br />
APOKYN 5 QL 90 SP<br />
AZILECT 3 QL 30<br />
benztropine mesylate 1 GC<br />
bromocriptine mesylate 2<br />
carbidopa/levodopa 2<br />
COMTAN 3 QL 240<br />
MIRAPEX 4<br />
MIRAPEX ER 4 PA<br />
PARCOPA 4<br />
PARLODEL 4 PA<br />
pramipexole 2<br />
ropinirole hcl 2<br />
selegiline hcl 2<br />
SINEMET 4<br />
SINEMET CR 4 PA<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
16
Drug Name Tier Notes<br />
STALEVO 3<br />
trihexyphenidyl hcl 1 GC<br />
ANTIPSYCHOTICS<br />
Atypicals<br />
clozapine 2<br />
FANAPT 4 PA QL 62/31<br />
FAZACLO 4 ST<br />
GEODON 3 QL 60<br />
INVEGA 6 MG TAB 4 QL 60 ST<br />
INVEGA INJ 4<br />
INVEGA TAB 4 QL 30 ST<br />
LATUDA 4<br />
RISPERDAL 4<br />
RISPERDAL CONSTA 4 QL 2/28<br />
risperidone 2 QL 68/34<br />
risperidone sol 2 QL 522/34<br />
SEROQUEL 3 QL 90<br />
SEROQUEL 300, 400 MG 3 QL 60<br />
ZYPREXA 3 QL 30<br />
ZYPREXA ZYDIS 3 QL 30<br />
Conventional<br />
fluphenazine 2<br />
fluphenazine decanoate 2<br />
HALDOL 4<br />
haloperidol decanoate 2<br />
haloperidol lactate 1 GC<br />
haloperidol oral conc 1 GC<br />
haloperidol tab 2<br />
loxapine succinate 2<br />
LOXITANE 2<br />
NAVANE 4<br />
ORAP 4<br />
thioridazine hcl 1 GC<br />
thiothixene 2<br />
trifluoperazine hcl 2<br />
ANTISPASTICITY AGENTS<br />
Antispasticity Agents<br />
baclofen 1 GC<br />
tizanidine hcl 2<br />
ANTIVIRALS<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
17
Drug Name Tier Notes<br />
Anti-cytomegalovirus (CMV) Agents<br />
foscarnet sodium 2 BD<br />
ganciclovir 2<br />
VALCYTE SOL 4 QL 968<br />
VALCYTE TAB 5 QL 102<br />
ZIRGAN 4 QL 5<br />
Anti-HIV Agents, Non-nucleoside Reverse Transcriptase Inhibitors<br />
ATRIPLA 5<br />
EDURANT 4<br />
INTELENCE 5 QL 120<br />
RESCRIPTOR 4<br />
SUSTIVA 3<br />
VIRAMUNE 4<br />
Anti-HIV Agents, Nucleoside and Nucleotide Reverse Transcriptase Inhibitors<br />
COMBIVIR TAB 5<br />
didanosine 2<br />
EMTRIVA 4<br />
EPIVIR 4<br />
EPZICOM TAB 5<br />
RETROVIR IV INFUSION 4<br />
stavudine 2<br />
TRIZIVIR 5<br />
TRUVADA 5<br />
VIDEX 4<br />
VIREAD 4<br />
ZIAGEN 3<br />
zidovudine 2<br />
Anti-HIV Agents, Other<br />
FUZEON 5 QL 60<br />
ISENTRESS 5 QL 60<br />
SELZENTRY 150 MG 5 QL 60<br />
SELZENTRY 300 MG 5 QL 120<br />
Anti-HIV Agents, Protease Inhibitors<br />
APTIVUS 5<br />
CRIXIVAN 3<br />
INVIRASE CAP 4<br />
INVIRASE TAB 5<br />
KALETRA 4<br />
LEXIVA 3<br />
NORVIR 4<br />
PREZISTA 4<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
18
Drug Name Tier Notes<br />
REYATAZ 3<br />
VIRACEPT 4<br />
VIRACEPT 625 MG TAB 5<br />
Anti-influenza Agents<br />
rimantadine hcl 2<br />
TAMIFLU 30 MG 4 QL 84/180<br />
TAMIFLU 45 MG 4 QL 42/180<br />
TAMIFLU 75 MG 4 QL 28<br />
Antihepatitis Agents<br />
BARACLUDE SOL 4 QL 600<br />
BARACLUDE TAB 5 QL 30<br />
EPIVIR HBV 4<br />
HEPSERA 4<br />
INFERGEN 5 PA<br />
PEGASYS 5 PA QL 4<br />
PEGINTRON 5 PA<br />
ribapak 400, 600 mg 5 PA QL 56/28<br />
RIBAPAK PAK 5 PA QL 56<br />
ribasphere 200 mg cap, tab 4 PA QL 180<br />
ribasphere 400, 600mg tab 5 PA QL 60<br />
ribavirin 2 PA<br />
TYZEKA 4 QL 30<br />
Antiherpetic Agents<br />
acyclovir 1 GC<br />
famciclovir 2<br />
trifluridine 2<br />
valacyclovir 1 gm tab 2 QL 30<br />
valacyclovir 500 mg tab 2 QL 60<br />
ANXIOLYTICS<br />
Antidepressants<br />
paroxetine 10 tab 1 QL 30 GC<br />
paroxetine susp 1 GC<br />
paroxetine tab 1 QL 60 GC<br />
PAXIL 4<br />
PEXEVA 4 QL 60<br />
PEXEVA 10 MG 4 QL 30<br />
sertraline hcl 1 QL 60 GC<br />
Anxiolytics, Other<br />
alprazolam 1 E GC<br />
buspirone 1 GC<br />
chlordiazepoxide hcl 1 E GC<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
19
Drug Name Tier Notes<br />
cloraepate dipotassium 1 E GC<br />
clozazepam 1 E GC<br />
diazepam 1 E GC<br />
lorazepam 1 E GC<br />
meprobamate 2<br />
oxazepam 1 E GC<br />
Serotonin/Norepinephrine Reuptake Inhibitors<br />
sertraline hcl conc 2<br />
BIPOLAR AGENTS<br />
Bipolar Agents<br />
lithium carbonate 1 GC<br />
LITHIUM CITRATE 3<br />
SAPHRIS 4 QL 60 ST<br />
BLOOD GLUCOSE REGULATORS<br />
Antidiabetic Agents<br />
acarbose 2<br />
ACTOPLUS MET 3 QL 93/31 ST<br />
ACTOS 3 QL 31/31<br />
ACTOS 15 MG 3 QL 93/31<br />
ALCOHOL SWABS 3<br />
AVANDAMET 4 QL 62/31 ST<br />
AVANDAMET 2/500 MG 4 QL 124/31 ST<br />
AVANDARYL 4 QL 30 ST<br />
AVANDARYL 4/2 MG 4 QL 31/31 ST<br />
AVANDIA 2 MG 4 QL 124/31 ST<br />
AVANDIA 4 MG 4 QL 62/31 ST<br />
AVANDIA 8 MG 4 QL 31/31 ST<br />
BYETTA 10 MCG 4 QL 1.2 ST<br />
BYETTA 5 MCG 4 QL 2.4 ST<br />
DUETACT 3 QL 30 ST<br />
FORTAMET 4 ST<br />
GAUZE PADS 3<br />
glimepiride 1 GC<br />
glipizide 1 GC<br />
glipizide/metformin hcl 2<br />
GLUCOPHAGE 4<br />
GLUCOTROL 4<br />
GLUCOVANCE 4<br />
GLUMETZA 4<br />
glyburide 1 GC<br />
glyburide micronized 1 GC<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
20
Drug Name Tier Notes<br />
glyburide/metformin hcl 1 GC<br />
GLYNASE 4<br />
GLYSET 4<br />
INSULIN PEN NEEDLES 3<br />
INSULIN SYRG/NEEDLES 3<br />
JANUMET 3 QL 60<br />
JANUVIA 3 QL 31/31<br />
METAGLIP 4<br />
metformin hcl 1 GC<br />
metformin hcl er 500 mg 1 QL 120 GC<br />
metformin hcl er 750 mg 1 QL 90 GC<br />
nateglinide 2<br />
ONGLYZA 4 QL 30 ST<br />
PRANDIN 4<br />
PRECOSE 4<br />
STARLIX 4<br />
SYMLIN 120 INJ 1000 MCG 4 PA QL 35<br />
SYMLIN 600 MCG INJ 4 PA QL 22<br />
SYMLINPEN 60 INJ 1000 MCG 4 PA QL 12<br />
WELCHOL 3<br />
Glycemic Agents<br />
GLUCAGEN HYPOKIT 4<br />
GLUCAGON EMERGENCY KIT 3<br />
PROGLYCEM 4<br />
Insulins<br />
APIDRA 4<br />
APIDRA SOLOSTAR 4<br />
HUMALOG 3 QL 30<br />
HUMALOG MIX 3<br />
HUMALOG PEN 3<br />
HUMULIN 70/30 3<br />
HUMULIN N 3<br />
HUMULIN R 3<br />
LANTUS 3<br />
LANTUS SOLOSTAR 3<br />
LEVEMIR 3<br />
NOVOLIN 70/30 3<br />
NOVOLIN N 3<br />
NOVOLIN R 3<br />
NOVOLOG 3<br />
NOVOLOG MIX 70/30 3<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
21
Drug Name Tier Notes<br />
BLOOD PRODUCTS/MODIFIERS/ VOLUME EXPANDERS<br />
Anticoagulants<br />
ARIXTRA 2.5 MG/0.5ML 3 QL 15.5/31<br />
ARIXTRA 5 MG/0.4ML 3 QL 12.4/31<br />
ARIXTRA 5.0 MG/0.4ML 3 QL 24.8/31<br />
ARIXTRA 7.5 MG/0.6ML 3 QL 18.6/31<br />
enoxaparin 2<br />
FRAGMIN 10000 U 2<br />
FRAGMIN 12500, 15000, 18000 U 5<br />
FRAGMIN 2500 U/0.2ML, 25000 U 3 QL 2/5D<br />
FRAGMIN 7500 U/0.3ML 3 QL 3.8/5D<br />
heparin sodium 1 GC BD<br />
heparin sodium/d5w 1 GC<br />
heparin sodium/nacl 1 GC<br />
INNOHEP 2<br />
jantoven 1 GC<br />
LOVENOX 100 MG/ML 4 QL 20/10<br />
LOVENOX 120 MG/0.8ML 4 QL 16/10<br />
LOVENOX 150 MG/ML 4 QL 20/10<br />
LOVENOX 30 MG/0.3ML 4 QL 6/10<br />
LOVENOX 300 MG/3ML 4 QL 3/1<br />
LOVENOX 40 MG/0.4ML 4 QL 8/10<br />
LOVENOX 60 MG/0.6ML 4 QL 12/10<br />
LOVENOX 80 MG/0.8ML 4 QL 16/10<br />
PRADAXA 4<br />
warfarin sodium 1 GC<br />
Blood Formation Modifiers<br />
NEUMEGA 5 QL 21/21<br />
Blood Formation Products<br />
anagrelide 2<br />
LEUKINE 250 MCG 5 PA<br />
LEUKINE 500 MCG 1 PA GC<br />
MOZOBIL 4 PA<br />
NEULASTA 5 PA<br />
NEUPOGEN 5 PA QL 16<br />
NEUPOGEN 480 MCG/1.6ML 5 PA QL 32<br />
PROCRIT 10000/ML 4 PA QL 12/28<br />
PROCRIT 2000/ML 4 PA QL 23<br />
PROCRIT 20000/ML 5 PA QL 12/28<br />
PROCRIT 3000/ML 4 PA QL 16<br />
PROCRIT 4000/ML 4 PA QL 12<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
22
Drug Name Tier Notes<br />
PROCRIT 40000/ML 5 PA QL 6/28<br />
PROMACTA 5<br />
Coagulants<br />
CYKLOKAPRON 3<br />
Platelet Aggregation Agents<br />
AGGRENOX 3<br />
cilostazol 2<br />
dipyridamole 2<br />
EFFIENT 4 QL 30<br />
PERSANTINE 4<br />
PLAVIX 3<br />
PLETAL 4<br />
ticlopidine hcl 2<br />
CARDIOVASCULAR AGENTS<br />
ACE Inhibitors<br />
benazepril hcl/hztc 1 GC<br />
captopril/hctz 1 GC<br />
enalapril maleate/hctz 1 GC<br />
fosinopril sodium/hctz 2<br />
lisinopril/hctz 1 GC<br />
LOTENSIN HCT 4<br />
moexipril/hctz 2<br />
quinapril/hctz 2<br />
Alpha-adrenergic Agonists<br />
clonidine hcl 1 GC<br />
guanabenz 2<br />
methyldopa 2<br />
methyldopa/hctz 2<br />
methyldopate hcl 1 GC<br />
midodrine hcl 2<br />
Alpha-adrenergic Blocking Agents<br />
doxazosin mesylate 1 GC<br />
MINIPRESS 4<br />
prazosin hcl 1 GC<br />
terazosin hcl 1 GC<br />
Antiarrhythmics<br />
amiodarone hcl 2<br />
disopyramide phosphate 2<br />
flecainide acetate 2<br />
mexiletine hcl 2<br />
MULTAQ 3 QL 60<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
23
Drug Name Tier Notes<br />
NORPACE 4<br />
pacerone 2<br />
procainamide hcl 1 GC<br />
propafenone hcl 2<br />
quinidine gluconate cr 2<br />
quinidine sulfate 2<br />
RYTHMOL CAP 3<br />
RYTHMOL TAB 4<br />
sorine 1 GC<br />
sotalol hcl 1 GC<br />
TIKOSYN 4 QL 60<br />
Beta-adrenergic Blocking Agents<br />
acebutolol hcl 1 GC<br />
atenolol 1 GC<br />
atenolol/chlorthalidone 1 GC<br />
betaxolol hcl 2<br />
bisoprolol fumarate 2<br />
bisoprolol fumarate/hctz 2<br />
BYSTOLIC 10 MG 3 QL 120<br />
BYSTOLIC 2.5, 5 MG 3 QL 30<br />
BYSTOLIC 20MG 3 QL 60<br />
carvedilol 1 GC<br />
INDERAL 4<br />
INNOPRAN 4<br />
KERLONE 4<br />
labetalol hcl 2<br />
LEVATOL 1 GC<br />
LOPRESSOR 4<br />
metoprolol succinate er 1 QL 60 GC<br />
metoprolol tartrate 1 GC<br />
metoprolol/hctz 2<br />
nadolol 1 GC<br />
nadolol/bend 2<br />
pindolol 1 GC<br />
propranolol 20 mg/5ml sol 1 GC<br />
propranolol 40 mg/5ml sol 2<br />
propranolol er 2<br />
propranolol inj, tab 1 GC<br />
propranolol/hctz 1 GC<br />
Calcium Channel Blocking Agents<br />
afeditab cr 2 QL 30<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
24
Drug Name Tier Notes<br />
amlodipine besylate 1 GC<br />
amlodipine besylate/benaz 2 QL 30<br />
cartia xt 2 QL 30<br />
dilt-xr 2 QL 60<br />
diltiazem cd 2 QL 30<br />
diltiazem er 360, 420 mg cap 2 QL 30<br />
diltiazem er cap 2<br />
diltiazem inj, tab 2<br />
felodipine er 2 QL 30<br />
ISOPTIN 4<br />
isradipine 2<br />
LOTREL 3<br />
nicardipine hcl 1 GC<br />
nifediac cc 2 QL 30<br />
nifedical xl 2 QL 30<br />
nifedipine 2<br />
nifedipine er 2 QL 30<br />
nimodipine 2<br />
nisoldipine 2 QL 30<br />
NORVASC 4 PA<br />
PROCARDIA 4<br />
PROCARDIA XL 4 PA<br />
taztia xt 2 QL 30<br />
verapamil hcl 1 GC<br />
Cardiovascular Agents, Other<br />
digoxin 1 GC<br />
LANOXIN 4<br />
pentoxifylline er 1 GC<br />
RANEXA 3 QL 60 ST<br />
Diuretics<br />
acetazolamide 2<br />
amiloride hcl 2<br />
amiloride/hctz 1 GC<br />
bumetanide 1 GC<br />
chlorothiazide 1 GC<br />
chlorthalidone 1 GC<br />
DYRENIUM 4<br />
EDECRIN SODIUM 4<br />
eplerenone 2<br />
furosemide 1 GC<br />
hctz 1 GC<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
25
Drug Name Tier Notes<br />
indapamide 1 GC<br />
INSPRA 4<br />
LASIX 20, 40 MG 4<br />
LASIX 80 MG 2<br />
MAXZIDE 4<br />
methazolamide 2<br />
methyclothiazide 1 GC<br />
metolazone 2<br />
MICROZIDE 4<br />
spironolactone 1 GC<br />
torsemide 2<br />
triamterene/hctz 1 GC<br />
Dyslipidemics<br />
CRESTOR 3 QL 31/31<br />
fenofibrate 2 QL 30<br />
gemfibrozil 2 QL 60<br />
LESCOL 2<br />
LIPITOR 3 QL 30<br />
LIPOFEN 4 PA<br />
LIVALO 4 QL 30 ST<br />
LOFIBRA 2 PA QL 30<br />
LOPID 4<br />
lovastatin 2 QL 60<br />
LOVAZA 3 QL 120<br />
MEVACOR 4 QL 60<br />
niacor 1 GC<br />
NIASPAN 3<br />
PRAVACHOL 4 PA QL 30<br />
pravastatin sodium 2 QL 30<br />
prevalite 2<br />
SIMCOR 1000/40 MG 4<br />
SIMCOR 500/20, 750/20 MG 4 QL 30<br />
simvastatin 1 QL 30 GC<br />
TRICOR 3 QL 30<br />
ZETIA 3 QL 30 ST<br />
Renin-Angiotensin-Aldosterone System Inhibitors<br />
benazepril hcl 1 GC<br />
BENICAR 4 QL 30<br />
BENICAR HCT 4 QL 30<br />
captopril 1 GC<br />
DIOVAN 3 QL 62/31<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
26
Drug Name Tier Notes<br />
DIOVAN 320 MG 3 QL 31/31<br />
DIOVAN HCT 3 QL 62/31<br />
DIOVAN HCT 320-12.5, 320-25MG 3 QL 31/31<br />
enalapril maleate 1 GC<br />
fosinopril sodium 2<br />
HYZAAR 4<br />
lisinopril 1 GC<br />
losartan 1 QL 30 GC<br />
losartan/hctz 1 QL 30 GC<br />
LOTENSIN 4<br />
MAVIK 4<br />
MICARDIS 4 QL 30<br />
MICARDIS HCT 4 QL 30<br />
moexipril hcl 2<br />
perindopril erbumine 2<br />
quinapril hcl 2<br />
ramipril 2<br />
TEKTURNA 3 QL 30<br />
TEKTURNA HCT 3 QL 30<br />
trandolapril 2<br />
Vasodilators<br />
hydralazine hcl 2<br />
isochron 2<br />
ISORDIL 4<br />
isosorbide dinitrate 1 GC<br />
isosorbide mononitrate 2<br />
minitran 2 QL 30<br />
minoxidil 2<br />
MONOKET 4<br />
NITRO-BID 4<br />
NITRO-DUR 4<br />
nitroglycerin 1 GC<br />
NITROLINGUAL PUMPSPRAY 4<br />
NITROSTAT 4<br />
CENTRAL NERVOUS SYSTEM AGENTS<br />
Amphetamines, ADHD<br />
amphetamine salts combo 2<br />
dextroamphetamine sulfate 2<br />
methamphetamine hcl 2<br />
Non-Amphetamines, ADHD<br />
FOCALIN 4<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
27
Drug Name Tier Notes<br />
METADATE CAP 3<br />
METADATE TAB 2<br />
methylin 2<br />
methylphenidate hcl 2<br />
RITALIN CAP 4<br />
RITALIN TAB 4 PA<br />
STRATTERA 10, 18, 25 MG 4 QL 60<br />
STRATTERA 40, 60, 80, 100 MG 4 QL 30<br />
Non-Amphetamines, Other<br />
AMPYRA 5 PA QL 60<br />
AVONEX KIT 30 MCG 5 PA QL 4/28<br />
AVONEX PREFL KIT 30 MCG 5 PA QL 2/28<br />
BETASERON 5 PA QL 15<br />
COPAXONE 5 QL 30 BD<br />
GILENYA 5<br />
INTUNIV 4<br />
REBIF 5 PA QL 12<br />
RILUTEK 3<br />
SAVELLA 3 QL 30<br />
SAVELLA 4-WEEK TITRATION 3 QL 60<br />
XENAZINE 12.5 MG 5 PA QL 240<br />
XENAZINE 25 MG 5 PA QL 120<br />
DENTAL AND ORAL AGENTS<br />
Dental and Oral Agents<br />
chlorhexadine gluconate 1 GC<br />
KEPIVANCE 5<br />
periogard 1 GC<br />
pilocarpine hcl 2<br />
triamcinolone in orabase 1 GC<br />
DERMATOLOGICAL AGENTS<br />
Dermatological Agents<br />
8-MOP 5<br />
ala-cort 1 GC<br />
alclometasone dipropionate 2<br />
ALDARA 4 QL 24<br />
amcinonide 2<br />
betamethasone dipropionate 1 GC<br />
betamethasone valerate 1 GC<br />
calcipotriene 2 QL 60<br />
claravis 2<br />
clobetasol propionate 2<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
28
Drug Name Tier Notes<br />
clotrimazole/beta crm 1 GC<br />
clotrimazole/beta lot 2<br />
CONDYLOX 4<br />
desonide 2<br />
desoximetasone 2<br />
diflorasone diacetate 2<br />
DOVONEX 4 QL 120<br />
erythromycin/benzoyl pero 2<br />
FINACEA 4<br />
fluocinolone acetonide 1 GC<br />
fluocinonide 1 GC<br />
fluocinonide emollient ba 1 GC<br />
fluorouracil 2<br />
fluticasone propionate 2<br />
halobetasol propionate 2<br />
HALOG 4<br />
hydrocortisone 1 GC<br />
hydrocortisone butyrate 2<br />
hydrocortisone valerate 2<br />
imiquimod 2 QL 24<br />
KENALOG 4<br />
LAC-HYDRIN 4<br />
laclotion 2<br />
LOCOID 4<br />
lokara 2<br />
LOTRISONE 4<br />
LUXIQ 4<br />
mometasone furoate 2<br />
nystatin/triamcinolone 1 GC<br />
OLUX 4<br />
OXSORALEN 4<br />
OXSORALEN ULTRA 5<br />
PANDEL 4<br />
podofilox 2<br />
prednicarbate 2<br />
PROTOPIC 4<br />
REGRANEX 5<br />
SANTYL 4<br />
selenium sulfide 1 GC<br />
SOLARAZE 3<br />
SORIATANE 5<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
29
Drug Name Tier Notes<br />
sotret 2<br />
TAZORAC 3<br />
triamcinolone acetonide 1 GC<br />
triderm 1 GC<br />
u-cort 2<br />
VOLTAREN 4<br />
ENZYME REPLACEMENT/ MODIFIERS<br />
Enzyme Replacement/ Modifiers<br />
ADAGEN 5 SP<br />
ALDURAZYME 5 SP<br />
BUPHENYL 5<br />
CEREDASE 5<br />
CEREZYME 5 SP BD<br />
FABRAZYME 5 SP BD<br />
KUVAN 5 PA<br />
MYOZYME 5<br />
NAGLAZYME 5<br />
ORFADIN 5 SP<br />
PANCREAZE 4<br />
ZAVESCA 5 QL 90<br />
ZENPEP 3<br />
GASTROINTESTINAL AGENTS<br />
Antispasmodics, Gastrointestinal<br />
atropine sulfate 1 GC<br />
dicyclomine hcl 1 GC<br />
glycopyrrolate 2<br />
methscopolamine 2<br />
PAMINE 4<br />
ROBINUL 4<br />
Gastrointestinal Agents, Other<br />
diphenoxylate/atropine 1 GC<br />
ELMIRON 4<br />
entocort ec 4<br />
gaviltye-g 1 GC<br />
gavilyte-c 1 GC<br />
gavilyte-n 1 GC<br />
GOLYTELY 3<br />
HELIDAC THERAPY 4<br />
KRISTALOSE 4<br />
lactulose 1 GC<br />
LOMOTIL 4<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
30
Drug Name Tier Notes<br />
loperamide hcl 1 GC<br />
MOTOFEN 4<br />
MOVIPREP 3<br />
NULYTELY 3<br />
polyethylene glycol 2<br />
PREVPAC 4<br />
PYLERA 4<br />
RELISTOR 4<br />
XIFAXAN 4<br />
Histamine2 (H2) Blocking Agents<br />
famotidine 1 GC<br />
nizatidine 150 mg 1 GC<br />
nizatidine 300 mg 2<br />
PEPCID 4<br />
ranitidine 1 GC<br />
ranitidine 150 mg cap 2<br />
ranitidine syr 2<br />
Irritable Bowel Syndrome Agents<br />
AMITIZA 3<br />
LOTRONEX 3 QL 60<br />
Protectants<br />
CARAFATE 4<br />
misoprostol 2<br />
sucralfate 2<br />
Proton Pump Inhibitors<br />
DEXILANT 4 QL 180/365<br />
lansoprazole 2<br />
NEXIUM 3<br />
NEXIUM INJ 4<br />
omeprazole 2<br />
pantoprazole sodium 2 QL 30<br />
PRILOSEC 4 PA<br />
PROTONIX 4<br />
GENITOURINARY AGENTS<br />
Antispasmodics, Urinary<br />
DETROL 3 QL 60<br />
DETROL LA 3 QL 30<br />
flavoxate 2<br />
GELNIQUE 4<br />
oxybutynin chloride 1 GC<br />
oxybutynin chloride er 2<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
31
Drug Name Tier Notes<br />
OXYTROL 4<br />
SANCTURA 4<br />
VESICARE 3 QL 30<br />
Benign Prostatic Hypertrophy Agents<br />
AVODART 3 QL 30<br />
finasteride 2 QL 30<br />
FLOMAX 4 QL 60<br />
JALYN 4<br />
PROSCAR 4 PA<br />
tamsulosin 2 QL 60<br />
Genitourinary Agents, Other<br />
CIALIS 1 QL 6 E GC<br />
CUPRIMINE 4<br />
METHERGINE 3<br />
VIAGRA 1 QL 6 E GC<br />
Phosphate Binders<br />
calcium acetate 2<br />
FOSRENOL 4 ST<br />
PHOSLO 3<br />
RENVELA 3 QL 270<br />
HORMONAL AGENTS, STIMULANT/REPLACEMENT/ MODIFYING (THYROID)<br />
Hormonal Agents, Stimulant/Replacement/Modifying (Thyroid)<br />
levothroid 1 GC<br />
levothyroxine sodium 1 GC<br />
levoxyl 1 GC<br />
liothyronine sodium inj 1 GC<br />
liothyronine sodium tab 2<br />
SYNTHROID 3<br />
unithroid 1 GC<br />
HORMONAL AGENTS, STIMULANT/REPLACEMENT/MODIFYING (ADRENAL)<br />
Glucocorticoids/Mineralocorticoids<br />
fludrocortisone 1 GC<br />
hydrocortisone 1 GC<br />
HORMONAL AGENTS, STIMULANT/REPLACEMENT/MODIFYING (PITUITARY)<br />
Hormonal Agents, Stimulant/Replacement/Modifying (Pituitary)<br />
chorionic gonadotropin 2<br />
desmopressin acetate 2<br />
HUMATROPE 12 MG 5 PA QL 2<br />
HUMATROPE 6, 24 MG 5 PA QL 1<br />
HUMATROPE COMBO PACK 5 PA QL 6<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
32
Drug Name Tier Notes<br />
INCRELEX 5 SP<br />
NORDITROPIN 4<br />
novarel 4<br />
NUTROPIN 5 PA QL 6<br />
NUTROPIN AQ 5 PA QL 12<br />
OMNITROPE 4<br />
OMNITROPE 5.8 MG 4 PA<br />
PREGNYL 4<br />
SAIZEN 5 MG 5 PA<br />
SAIZEN 8.8 MG 4<br />
SEROSTIM 5 PA<br />
HORMONAL AGENTS, STIMULANT/REPLACEMENT/MODIFYING (SEX<br />
HORMONES/MODIFIERS)<br />
Anabolic Steroids<br />
ANADROL-50 5<br />
OXANDRIN 4 PA<br />
oxandrolone 10mg tab 5 QL 60<br />
oxandrolone 2.5mg tab 2 QL 120<br />
Androgens<br />
ANDRODERM 4 PA QL 30<br />
ANDROXY 4<br />
danazol 2<br />
METHITEST 4<br />
testosterone cypionate 2<br />
testosterone enanthate 2<br />
Estrogens<br />
ESTRACE 4<br />
estradiol 0.0375, 0.06 mg dis 2<br />
estradiol dis 2 QL 4<br />
estradiol tab 1 GC<br />
FEMRING 4<br />
FEMTRACE 4<br />
MENEST 4<br />
MENOSTAR 4<br />
PREMARIN 3<br />
Progestins<br />
AYGESTIN 2<br />
jolivette 2<br />
medroxyprogesterone ac inj 1 QL 50 GC<br />
medroxyprogesterone ac tab 1 GC<br />
MEGACE 4<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
33
Drug Name Tier Notes<br />
megestrol acetate 2<br />
NOR-QD 4<br />
NORA-BE 2<br />
norethindrone acetate 2<br />
ORTHO MICRONOR 4<br />
PROMETRIUM 4<br />
PROVERA 4<br />
Selective Estrogen Receptor Modifying Agents<br />
EVISTA 3 QL 30<br />
HORMONAL AGENTS, SUPPRESSANT (ADRENAL)<br />
Hormonal Agents, Suppressant (Adrenal)<br />
LYSODREN 3<br />
HORMONAL AGENTS, SUPPRESSANT (PARATHYROID)<br />
Hormonal Agents, Suppressant (Parathyroid)<br />
SENSIPAR 30 MG 3 QL 60<br />
SENSIPAR 60 MG 5 QL 60<br />
SENSIPAR 90 MG 5 QL 124/31<br />
HORMONAL AGENTS, SUPPRESSANT (PITUITARY)<br />
Hormonal Agents, Suppressant (Pituitary)<br />
FIRMAGON 4 PA<br />
leuprolide acetate 2 PA<br />
LUPRON DEPOT 4 PA<br />
LUPRON DEPOT-PED 5 PA<br />
octreotide acetate 1 PA GC<br />
SANDOSTATIN 5 PA<br />
SANDOSTATIN 0.05 MG/ML 4 PA<br />
SOMATULINE 120 MG/.5ML 5 PA<br />
SOMATULINE 60 MG/0.2ML 4 PA<br />
SOMAVERT 5 PA QL 30 SP<br />
SYNAREL 5<br />
HORMONAL AGENTS, SUPPRESSANT (SEX HORMONES/MODIFIERS)<br />
Antiandrogens<br />
bicalutamide 2 QL 30<br />
FASLODEX 2<br />
flutamide 2<br />
NILANDRON 4 QL 60<br />
ZYTIGA 5<br />
HORMONAL AGENTS, SUPPRESSANT (THYROID)<br />
Antithyroid Agents<br />
methimazole 2<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
34
Drug Name Tier Notes<br />
propylthiouracil 2<br />
IMMUNOLOGICAL AGENTS<br />
Immune Suppressants<br />
ATGAM 3 BD<br />
azathioprine 2 BD<br />
CELLCEPT SUSP 5 BD<br />
cyclosporine 2 BD<br />
ENBREL 25 MG 5 PA<br />
ENBREL 25 MG/0.5ML 5 PA QL 8<br />
ENBREL 50 MG/ML 4 PA QL 7.84/28<br />
gengraf 2 BD<br />
HUMIRA 20 MG/0.4ML 5 PA QL 2/28<br />
HUMIRA 40 MG/0.8ML 5 PA QL 6/28<br />
HUMIRA PEN-CROHNS 5 PA<br />
IMURAN 4 PA<br />
mercaptopurine 2<br />
methotrexate 1 GC<br />
methotrexate 50 mg/ml inj 2<br />
mycophenolate mofetil 2 BD<br />
MYFORTIC 3 BD<br />
NEORAL 4 BD<br />
ORENCIA 5 PA<br />
ORTHOCLONE OKT3 5 BD<br />
PROGRAF 4 BD<br />
PURINETHOL 4<br />
RAPAMUNE 0.5 MG TAB 4<br />
RAPAMUNE 1, 2 MG TAB 4 BD<br />
RAPAMUNE SOL 4 BD<br />
REMICADE 5 QL 7<br />
SANDIMMUNE CAP, SOL 4 BD<br />
SANDIMMUNE INJ 4<br />
SIMPONI 5 PA<br />
SIMULECT 5 BD<br />
tacrolimus 2 BD<br />
TORISEL 5 BD<br />
ZORTRESS 4 BD<br />
Immunizing Agents, Passive<br />
GAMASTAN S/D 4 BD<br />
GAMMAGARD LIQUID 5 BD<br />
GAMUNEX 4 PA<br />
PRIVIGEN 4 PA<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
35
Drug Name Tier Notes<br />
THYMOGLOBULIN 5 BD<br />
VIVAGLOBIN 5 BD<br />
Immunomodulators<br />
ACTIMMUNE 5 PA SP<br />
ARCALYST 5 PA<br />
INTRON A 10 MU INJ 5<br />
INTRON A 18 MU INJ 4<br />
INTRON A PEN 4<br />
KINERET 5 PA QL 20.77/31<br />
leflunomide 2 QL 30<br />
Vaccines<br />
ACTHIB 4<br />
ADACEL 4<br />
BOOSTRIX 4<br />
CERVARIX 4<br />
COMVAX 4<br />
DAPTACEL 4<br />
DECAVAC 4<br />
DIPHTHERIA/TETANUS TOXOID 2<br />
ENGERIX-B VACC 4<br />
GARDASIL 4<br />
HAVRIX 4<br />
IMOVAX RABIES (H.D.C.V.) 3<br />
INFANRIX 4<br />
IPOL INACTIVATED IPV 4<br />
IXIARO 4<br />
JE-VAX 4<br />
M-M-R II 4<br />
MENACTRA 4<br />
MENOMUNE-A/C/Y/W-135 4<br />
MENVEO INJ 4<br />
PEDVAX HIB 4<br />
PROQUAD 4<br />
RABAVERT 3<br />
RECOMBIVAX HB 4<br />
ROTATEQ 4<br />
TETANUS TOXOID ADSORBED 4<br />
TETANUS/DIPHTHERIA TOXOID 4<br />
TRIPEDIA 4<br />
TWINRIX 4<br />
TYPHIM VI 4<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
36
Drug Name Tier Notes<br />
VAQTA 4<br />
VARIVAX 3<br />
YF-VAX 4<br />
ZOSTAVAX 4 QL 1<br />
INFLAMMATORY BOWEL DISEASE AGENTS<br />
Glucocorticoids<br />
dexamethasone 2<br />
procto-pak 1 GC<br />
proctocream-hc 1 GC<br />
proctosol hc 1 GC<br />
proctozone-hc 1 GC<br />
Salicylates<br />
APRISO 3 QL 120<br />
ASACOL DR 400 MG 4 QL 180<br />
ASACOL HD 800 MG 4 QL 150<br />
balsalazide disodium 2<br />
LIALDA 3<br />
mesalamine 2<br />
PENTASA 4<br />
ROWASA 4<br />
Sulfonamides<br />
sulfasalazine 2<br />
sulfazine ec 2<br />
METABOLIC BONE DISEASE AGENTS<br />
Metabolic Bone Disease Agents<br />
alendronate 35, 70 mg 2 QL 4/28<br />
alendronate 5, 10, 40 mg 2 QL 30<br />
calcitonin-salmon 2 QL 3.8/31 BD<br />
calcitriol 2 BD<br />
FORTEO 4<br />
fortical 3 BD<br />
FOSAMAX 4 PA<br />
FOSAMAX PLUS D 70-2800 MG 4 QL 4 ST<br />
FOSAMAX PLUS D 70-5600 MG 4 QL 4/28 ST<br />
HECTOROL 3 BD<br />
MIACALCIN 4 BD<br />
pamidronate disodium 1 GC<br />
PROLIA 4<br />
ROCALTROL 4 BD<br />
SKELID 4<br />
XGEVA 5<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
37
Drug Name Tier Notes<br />
ZEMPLAR 3 BD<br />
ZOMETA 5 BD<br />
MISCELLANEOUS THERAPEUTIC AGENTS<br />
Miscellaneous Therapeutic Agents<br />
FEMHRT 4<br />
jinteli 2<br />
junel 2<br />
kariva 2<br />
kelnor 2<br />
leena 3<br />
lessina 4<br />
levora 1 GC<br />
LO/OVRAL 4<br />
LOESTRIN 4<br />
LOSEASONIQUE 4<br />
low-ogestrel 2<br />
lutera 28 day 2<br />
LYBREL 4<br />
microgestin 2<br />
MODICON 4<br />
mononessa 2<br />
neomycin/polymyxin b sulf 1 GC<br />
NORDETTE 4<br />
NORINYL 4<br />
nortrel 2<br />
NUVARING 4<br />
ocella 2<br />
ogestrel 2<br />
ORTHO EVRA 4<br />
ORTHO TRI-CYCLEN LO 4<br />
ORTHO-CEPT 4<br />
ORTHO-CYCLEN 4<br />
ORTHO-NOVUM 4<br />
OVCON 4<br />
PREFEST 4<br />
PREMPHASE 3<br />
PREMPRO 3<br />
previfem 2<br />
solia 2<br />
sprintec 2<br />
sronyx 2<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
38
Drug Name Tier Notes<br />
NUTRIENTS/ MINERALS/ ELECTROLYTES<br />
Vitamins<br />
PRENATABS OBN 3<br />
OPHTHALMIC AGENTS<br />
Ophthalmic Agents, Other<br />
ak-con 1 GC<br />
bacitracin/neomycin/polym 1 GC<br />
bacitracin/polymyxin b 1 GC<br />
MAXITROL 4<br />
MYDRIACYL 1 GC<br />
neomycin/polymyxin/dexame 1 GC<br />
neomycin/polymyxin/gramic 2<br />
neomycin/polymyxin/hc 2<br />
NEOSPORIN SOL 2<br />
parcaine 1 GC<br />
POLY PRED 4<br />
poly-dex 1 GC<br />
PRED-G 4<br />
RESTASIS 3<br />
sulfacetamide sodium/pred 1 GC<br />
tobramycin/dexamethasone 2<br />
trimethoprim sulfate/poly 2<br />
tropicamide 1 GC<br />
Ophthalmic Anti-allergy Agents<br />
azelastine ophth sol 2<br />
cromolyn sodium 2<br />
OPTIVAR 4<br />
PATADAY 3<br />
PATANOL 4<br />
Ophthalmic Anti-inflammatories<br />
dexamethasone sod phos 1 GC<br />
FLAREX 4<br />
fluorometholone 1 GC<br />
flurbiprofen sodium 1 GC<br />
FML 4<br />
ketorolac 1 GC<br />
LOTEMAX 4<br />
MAXIDEX 4<br />
NEVANAC 4<br />
OCUFEN 4<br />
OMNIPRED 4<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
39
Drug Name Tier Notes<br />
ORAPRED 4<br />
PRED FORTE 4<br />
PRED MILD 4<br />
prednisolone acetate 1 GC<br />
prednisolone sod phosp op 1 GC<br />
Ophthalmic Antiglaucoma Agents<br />
ALPHAGAN P 3<br />
apraclonidine 2<br />
AZOPT 3<br />
betaxolol hcl 2<br />
brimonidine tartrate 2<br />
carteolol hcl 1 GC<br />
COMBIGAN 3<br />
dorzolamide hcl 2<br />
dorzolamide hcl/timolol malea 2 QL 10<br />
IOPIDINE 4<br />
ISTALOL 4<br />
LEVOBUNOLOL HCL 3<br />
levobunolol hcl 0.5% op sol 1 GC<br />
metipranolol 2<br />
OPTIPRANOLOL 4<br />
PHOSPHOLINE IODIDE 4<br />
PILOPINE HS 4<br />
PROPINE 4<br />
timolol 2<br />
timolol maleate op 2<br />
Ophthalmic Prostaglandin and Prostamide Analogs<br />
latanoprost 2<br />
LUMIGAN 2<br />
TRAVATAN Z 3 QL 5<br />
OTIC AGENTS<br />
Otic Agents<br />
acetasol hc 2<br />
cortomycin 1 GC<br />
DERMOTIC 4<br />
neomycin/polymyxin/hc 2<br />
RESPIRATORY TRACT AGENTS<br />
Anti-inflammatories, Inhaled Corticosteroids<br />
ASMANEX 4<br />
FLONASE 4<br />
FLOVENT 3 QL 60<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
40
Drug Name Tier Notes<br />
FLOVENT HFA 110, 220 MCG 3 QL 12<br />
FLOVENT HFA 44 MCG 3 QL 10.6<br />
flunisolide 2 QL 25/25<br />
fluticasone propionate 2 QL 32<br />
NASACORT 4<br />
NASONEX 3<br />
OMNARIS 4<br />
PULMICORT 4<br />
PULMICORT INH SUSP 4 BD<br />
QVAR 40 MCG AER 3 QL 14.6<br />
QVAR 80 MCG AER 3 QL 21.9<br />
RHINOCORT AQUA 4 QL 18<br />
Antihistamines<br />
ASTELIN 4 QL 60/31<br />
ASTEPRO 3 QL 60/31<br />
azelastine nasal spr 2 QL 30/25<br />
cetirizine hcl 2 QL 300<br />
clemastine fumarate 2<br />
fexofenadine 180 mg 2 QL 30<br />
fexofenadine 30, 60 mg 2 QL 60<br />
palgic liq 2<br />
palgic tab 4<br />
PATANASE 4<br />
SEMPREX-D 4<br />
Antileukotrienes<br />
ACCOLATE 3 QL 60<br />
SINGULAIR 4 QL 30 ST<br />
SINGULAIR CHW 5MG 4 QL 60 ST<br />
zafirlukast 2<br />
ZYFLO CR 4 QL 120<br />
Bronchodilators, Anticholinergic<br />
ATROVENT HFA 4 QL 25.8/31<br />
ipratropium bromide inh sol 2 BD<br />
ipratropium bromide nasal spr 2 QL 30<br />
SPIRIVA HANDIHALER 3 QL 60<br />
Bronchodilators, Phosphodiesterase Inhibitors (Xanthines)<br />
aminophylline 1 GC<br />
LUFYLLIN 4<br />
theochron 1 GC<br />
theophylline er 2<br />
theophylline er 400, 600 mg 1 GC<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
41
Drug Name Tier Notes<br />
Bronchodilators, Sympathomimetic<br />
ADVAIR DISKUS 3 QL 60<br />
ADVAIR HFA 3 QL 12<br />
albuterol sulfate er 2<br />
albuterol sulfate neb 1 GC BD<br />
albuterol sulfate syrup, tab 1 GC<br />
albuterol sulfate/ipratro 1 GC BD<br />
COMBIVENT 3 QL 29.4/31<br />
FORADIL 4<br />
levalbuterol inh sol 2 BD<br />
MAXAIR 4<br />
metaproterenol sulfate 2<br />
PERFOROMIST 4 BD<br />
PROAIR HFA 3 QL 17<br />
PROVENTIL HFA 4 QL 13.4<br />
SEREVENT DISKUS 3 QL 60<br />
SYMBICORT 3 QL 10.2<br />
terbutaline sulfate 2<br />
VENTOLIN HFA 3 QL 36<br />
Mast Cell Stabilizers<br />
cromolyn sodium 2 BD<br />
GASTROCROM 4<br />
Pulmonary Antihypertensives<br />
LETAIRIS 5 PA QL 31/31<br />
REVATIO INJ 3 PA QL 1125<br />
REVATIO TAB 5 PA QL 90<br />
TRACLEER 5 PA QL 60 SP<br />
VENTAVIS 5 BD<br />
Respiratory Tract Agents, Other<br />
benzonatate 1 E GC<br />
hydroco/homatropine 1 E GC<br />
hydromet 1 E GC<br />
PROLASTIN 5 SP<br />
promethazine vc/codeine 1 E GC<br />
promethazine/codeine 1 E GC<br />
PULMOZYME 5 BD<br />
TOBI 2 BD<br />
TYZINE 3<br />
TYZINE PED NASAL DRO 4<br />
XOLAIR 5 PA QL 7/28 SP<br />
SEDATIVES/HYPNOTICS<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
42
Drug Name Tier Notes<br />
Sedatives/Hypnotics<br />
estazolam 1 E GC<br />
flurazepam 1 E GC<br />
LUNESTA 4<br />
NUVIGIL 4 PA<br />
PROVIGIL 100 MG 4 PA QL 60<br />
PROVIGIL 200 MG 4 PA QL 30<br />
ROZEREM 4 ST<br />
SONATA 4 PA<br />
temazepam 1 E GC<br />
triazolam 1 E GC<br />
XYREM 5 SP<br />
zaleplon 10 mg 2 QL 60<br />
zaleplon 5 mg 2 QL 30<br />
zolpidem tartrate 1 QL 30 GC<br />
SKELETAL MUSCLE RELAXANTS<br />
Skeletal Muscle Relaxants<br />
cyclobenzaprine hcl 1 GC<br />
FEXMID 4 PA<br />
FLEXERIL 4<br />
metaxalone 2 ST<br />
methocarbamol 1 GC<br />
NORFLEX 4<br />
orphenadrine citrate 2<br />
PARAFON FORTE DSC 4<br />
ROBAXIN 4<br />
SKELAXIN 4<br />
SOMA 4 PA<br />
THERAPEUTIC NUTRIENTS/ MINERALS/ ELECTROLYTES<br />
Electrolyte/Mineral Modifiers<br />
KAYEXALATE 4<br />
kionex 2<br />
SAMSCA 5 PA QL 60<br />
sodium polystyrene sulfon 2<br />
Electrolyte/Mineral Replacement<br />
AMINOSYN 4 BD<br />
AMINOSYN II 4 BD<br />
AMINOSYN II M 3.5%/DEXTRO<br />
4 BD<br />
AMINOSYN II/DEXTROSE 4 BD<br />
AMINOSYN IIM INJ 3.5%/D5W 4<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
43
Drug Name Tier Notes<br />
AMINOSYN M 4 BD<br />
AMINOSYN-HBC 4 BD<br />
aminosyn-hf 2 BD<br />
AMINOSYN-PF 4 BD<br />
aminosyn/electrolyte 2 BD<br />
CLINIMIX/DEXTROSE 4 BD<br />
clinisol sf 15% 4 BD<br />
dextrose 1 GC<br />
dextrose/nacl inj 1 GC BD<br />
folic acid 1 E GC<br />
freamine iii 2 BD<br />
FREAMINE III 3% 4 BD<br />
hepatamine 2 BD<br />
INTRALIPID 4<br />
intralipid 20% inj 2<br />
IONOSOL-MB 4<br />
IONOSOL-T 4<br />
isolyte-h/dextrose 5% 2<br />
isolyte-m/dextrose 5% 2<br />
ISOLYTE-P/DEXTROSE 5% 4<br />
ISOLYTE-S 4<br />
ISOLYTE-S/DEXTROSE 5% 4<br />
K-TAB 4<br />
kcl/d5w 1 GC<br />
kcl/d5w/lr inj 1 GC BD<br />
kcl/d5w/nacl 1 GC<br />
kcl/nacl 0.3-0.9 inj 2<br />
kcl/nacl inj 1 GC<br />
klor-con 1 GC<br />
lactated ringer's irr 1 GC<br />
lactated ringer's viaflex 1 GC<br />
levocarnitine 2 BD<br />
liposyn 4<br />
magnesium sulfate 1 GC<br />
NEPHRAMINE 4 BD<br />
normosol-m in d5w 2<br />
NORMOSOL-R 4<br />
normosol-r in d5w 2<br />
OSMOPREP 3<br />
physiolyte 1 GC<br />
physiosol irrigation 1 GC<br />
SP-This prescription may be available only at certain pharmacies. For more information consult your Pharmacy<br />
Directory or call Member Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD<br />
users should call 711 Telecommu-nication Relay Services; E-This prescription drug is not normally covered in a<br />
Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count<br />
towards your to-tal drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In<br />
addi-tion, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this<br />
drug.; GC-We provide additional coverage of this prescription drug in the coverage gap. Please refer to our<br />
Evidence of Coverage for more information about this coverage.<br />
44
Drug Name Tier Notes<br />
PLASMA-LYTE 56 4<br />
PLASMA-LYTE A 4<br />
PLASMA-LYTE-148 4<br />
PLASMA-LYTE-148/D5W 4<br />
PLASMA-LYTE-56/D5W 4<br />
plasma-lyte-r 2<br />
potassium chloride 1 GC<br />
potassium citrate er 2<br />
premasol 1 GC BD<br />
PROCALAMINE 4 BD<br />
PROSOL 4 BD<br />
ringer's injection 1 GC<br />
ringer's irrigation 1 GC<br />
sodium bicarbonate 1 GC<br />
sodium chloride 0.9% irr 1 GC<br />
sodium chloride 0.45%,0.9%,3% 1 GC BD<br />
sodium chloride 2.5 meq/ml 2 BD<br />
sodium chloride 5% 1 GC<br />
SODIUM FLUORIDE 1<br />
sodium lactate 1 GC<br />
TRAVASOL 4 BD<br />
vitamin d 1 E GC<br />
SP-Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información, consulte su<br />
Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115.<br />
Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios con TTY/TDD deben marcar<br />
711; E-Este medicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare.<br />
La cantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total de<br />
medicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástrofe).<br />
Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayuda<br />
adicional para pagar este medicamento.; GC-Proporcionamos cobertura adicional de este medicamento recetado durante<br />
la brecha en la cobertura. Consulte nuestra Evidencia de Cobertura para obtener más información sobre esta cobertura.<br />
45
8<br />
8-mop .................................... 28<br />
A<br />
abilify discmelt ........................ 8<br />
abilify inj ................................. 8<br />
abilify sol ................................ 8<br />
abilify tab ................................ 8<br />
acarbose ................................. 20<br />
accolate ................................. 41<br />
acebutolol hcl ........................ 24<br />
acetasol hc ............................. 40<br />
acetazolamide ........................ 25<br />
acetic acid ................................ 4<br />
acthib ..................................... 36<br />
acticin .................................... 16<br />
actimmune ............................. 36<br />
actoplus met .......................... 20<br />
actos ...................................... 20<br />
actos 15 mg ........................... 20<br />
acyclovir ................................ 19<br />
adacel .................................... 36<br />
adagen ................................... 30<br />
advair diskus ......................... 42<br />
advair hfa .............................. 42<br />
afeditab cr .............................. 24<br />
afinitor 2.5 mg ....................... 15<br />
afinitor 5 mg, 10 mg.............. 15<br />
aggrenox ................................ 23<br />
ak-con .................................... 39<br />
ak-tob ...................................... 3<br />
ala-cort .................................. 28<br />
albenza .................................. 16<br />
albuterol sulfate er ................. 42<br />
albuterol sulfate neb .............. 42<br />
albuterol sulfate syrup, tab .... 42<br />
albuterol sulfate/ipratro ......... 42<br />
alclometasone dipropionate .. 28<br />
alcohol swabs ........................ 20<br />
aldara ..................................... 28<br />
aldurazyme ............................ 30<br />
alendronate 35, 70 mg ........... 37<br />
alendronate 5, 10, 40 mg ....... 37<br />
alimta..................................... 14<br />
allopurinol ............................. 12<br />
alphagan p ............................. 40<br />
alprazolam ............................. 19<br />
amantadine ............................ 16<br />
amcinonide ............................ 28<br />
amifostine .............................. 14<br />
amiloride hcl ......................... 25<br />
amiloride/hctz ....................... 25<br />
aminophylline ....................... 41<br />
aminosyn ............................... 43<br />
aminosyn ii ............................ 43<br />
aminosyn ii m 3.5%/dextro ... 43<br />
aminosyn ii/dextrose ............. 43<br />
aminosyn iim inj 3.5%/d5w .. 43<br />
aminosyn m ........................... 44<br />
aminosyn/electrolyte ............. 44<br />
aminosyn-hbc ........................ 44<br />
aminosyn-hf .......................... 44<br />
aminosyn-pf .......................... 44<br />
amiodarone hcl ...................... 23<br />
amitiza ................................... 31<br />
amitriptyline hcl ...................... 9<br />
amlodipine besylate .............. 25<br />
amlodipine besylate/benaz .... 25<br />
amoxapine ............................... 9<br />
amoxicillin 200mg chw tab ..... 5<br />
amoxicillin cap, susp, tab ........ 5<br />
amoxicillin/clavulanate p ........ 5<br />
amphetamine salts combo ..... 27<br />
amphotericin b ...................... 11<br />
ampicillin ................................ 5<br />
ampicillin/sulbactam 10-5 gm . 5<br />
ampyra................................... 28<br />
anadrol-50 ............................. 33<br />
anagrelide .............................. 22<br />
anastrozole ............................ 15<br />
ancobon ................................. 11<br />
androderm ............................. 33<br />
androxy ................................. 33<br />
antabuse................................. 10<br />
apap/cod 300-15 mg tab .......... 1<br />
apap/cod 300-30 mg tab .......... 1<br />
apap/cod 300-60 mg tab .......... 1<br />
apap/cod sol ............................ 1<br />
apidra..................................... 21<br />
apidra solostar ....................... 21<br />
aplenzin ................................... 8<br />
apokyn ................................... 16<br />
apraclonidine ......................... 40<br />
apriso ..................................... 37<br />
aptivus ................................... 18<br />
arcalyst .................................. 36<br />
aricept ...................................... 8<br />
arimidex ................................ 15<br />
arixtra 2.5 mg/0.5ml .............. 22<br />
arixtra 5 mg/0.4ml ................. 22<br />
arixtra 5.0 mg/0.4ml .............. 22<br />
arixtra 7.5 mg/0.6ml .............. 22<br />
arthrotec .................................. 1<br />
arzerra ................................... 15<br />
asacol dr 400 mg ................... 37<br />
asacol hd 800 mg .................. 37<br />
ascomp/codeine ....................... 1<br />
asmanex................................. 40<br />
astelin .................................... 41<br />
astepro ................................... 41<br />
astramorph............................... 1<br />
atenolol .................................. 24<br />
atenolol/chlorthalidone ......... 24<br />
atgam ..................................... 35<br />
atripla .................................... 18<br />
atropine sulfate ...................... 30<br />
atrovent hfa ........................... 41<br />
avandamet ............................. 20<br />
avandamet 2/500 mg ............. 20<br />
avandaryl ............................... 20<br />
avandaryl 4/2 mg................... 20<br />
avandia 2 mg ......................... 20<br />
avandia 4 mg ......................... 20<br />
avandia 8 mg ......................... 20<br />
avastin ................................... 14<br />
avodart................................... 32<br />
avonex kit 30 mcg ................. 28<br />
avonex prefl kit 30 mcg ........ 28<br />
aygestin ................................. 33<br />
azactam in dextrose ................. 5<br />
azathioprine ........................... 35<br />
azelastine nasal spr ................ 41<br />
azelastine ophth sol ............... 39<br />
azilect .................................... 16<br />
azithromycin ........................... 5<br />
azopt ...................................... 40<br />
B<br />
baciim ...................................... 4<br />
bacitracin ................................. 4<br />
bacitracin/neomycin/polym... 39<br />
bacitracin/polymyxin b ......... 39<br />
baclofen ................................. 17<br />
balsalazide disodium ............. 37<br />
banzel 200 mg tab ................... 7<br />
banzel 400 mg tab ................... 7<br />
banzel susp .............................. 8<br />
baraclude sol ......................... 19<br />
baraclude tab ......................... 19<br />
46
enazepril hcl ........................ 26<br />
benazepril hcl/hztc ................ 23<br />
benicar ................................... 26<br />
benicar hct ............................. 26<br />
benzonatate ........................... 42<br />
benztropine mesylate ............ 16<br />
betamethasone dipropionate .. 28<br />
betamethasone valerate ......... 28<br />
betaseron ............................... 28<br />
betaxolol hcl .................... 24, 40<br />
bicalutamide .......................... 34<br />
bisoprolol fumarate ............... 24<br />
bisoprolol fumarate/hctz ....... 24<br />
bleomycin sulfate .................. 14<br />
boostrix ................................. 36<br />
brimonidine tartrate ............... 40<br />
bromocriptine mesylate ......... 16<br />
budeprion ................................ 8<br />
bumetanide ............................ 25<br />
buphenyl ................................ 30<br />
buprenorphine ....................... 10<br />
bupropion ................................ 8<br />
bupropion sr 100 mg tab ......... 8<br />
bupropion sr 150 mg tab ......... 8<br />
bupropion sr 200 mg tab ......... 8<br />
buspirone ............................... 19<br />
busulfex ................................. 13<br />
butalbital/apap/caff ................. 2<br />
byetta 10 mcg ........................ 20<br />
byetta 5 mcg .......................... 20<br />
bystolic 10 mg ....................... 24<br />
bystolic 2.5, 5 mg .................. 24<br />
bystolic 20mg ........................ 24<br />
C<br />
calcipotriene .......................... 28<br />
calcitonin-salmon .................. 37<br />
calcitriol ................................ 37<br />
calcium acetate ...................... 32<br />
campath ................................. 15<br />
capastat sulfate ...................... 13<br />
captopril ................................ 26<br />
captopril/hctz......................... 23<br />
carafate .................................. 31<br />
carbamazepine ......................... 7<br />
carbatrol 100, 200 mg ............. 7<br />
carbatrol 300 mg ..................... 7<br />
carbidopa/levodopa ............... 16<br />
carteolol hcl ........................... 40<br />
cartia xt.................................. 25<br />
carvedilol............................... 24<br />
ceenu ..................................... 13<br />
cefaclor .................................... 5<br />
cefazolin sodium ..................... 5<br />
cefdinir .................................... 5<br />
cefepime .................................. 5<br />
cefoxitin sodium...................... 5<br />
cefpodoxime ............................ 5<br />
ceftriaxone sodium .................. 5<br />
cefuroxime axetil .................... 5<br />
cefuroxime sodium.................. 5<br />
celebrex 100, 200 mg .............. 1<br />
celebrex 50, 400 mg ................ 1<br />
cellcept inj ............................. 10<br />
cellcept susp .......................... 35<br />
celontin .................................... 7<br />
cephalexin ............................... 5<br />
ceredase ................................. 30<br />
cerezyme ............................... 30<br />
cervarix ................................. 36<br />
cetirizine hcl .......................... 41<br />
chantix 0.5 mg ......................... 4<br />
chantix 1 mg .......................... 10<br />
chantix pak ............................ 10<br />
chlordiazepoxide hcl ............. 19<br />
chlordiazepoxide/amitript ....... 9<br />
chlorhexadine gluconate ....... 28<br />
chloroquine phosphate .......... 16<br />
chlorothiazide ........................ 25<br />
chlorpromazine 10, 25mg tab 10<br />
chlorpromazine inj, tab ......... 10<br />
chlorthalidone ....................... 25<br />
chorionic gonadotropin ......... 32<br />
cialis ...................................... 32<br />
ciclopirox .............................. 11<br />
cilostazol ............................... 23<br />
ciprofloxacin ........................... 6<br />
citalopram 10 mg tab .............. 9<br />
citalopram 20 mg tab .............. 9<br />
citalopram 40 mg tab .............. 9<br />
citalopram sol .......................... 9<br />
claravis .................................. 28<br />
clemastine fumarate .............. 41<br />
clindamycin hcl ....................... 4<br />
clindamycin phosphate............ 4<br />
clinimix/dextrose................... 44<br />
clinisol sf 15%....................... 44<br />
clobetasol propionate ............ 28<br />
clomipramine hcl .................... 9<br />
clonidine hcl .......................... 23<br />
cloraepate dipotassium .......... 20<br />
clotrimazole ........................... 11<br />
clotrimazole/beta crm ............ 29<br />
clotrimazole/beta lot .............. 29<br />
clozapine ............................... 17<br />
clozazepam ............................ 20<br />
co-gesic ................................... 2<br />
colcrys ................................... 12<br />
colistimethate sodium ............. 4<br />
combigan ............................... 40<br />
combivent .............................. 42<br />
combivir tab .......................... 18<br />
comtan ................................... 16<br />
comvax .................................. 36<br />
condylox ................................ 29<br />
copaxone ............................... 28<br />
cortomycin ............................ 40<br />
crestor .................................... 26<br />
crixivan ................................. 18<br />
cromolyn sodium ............ 39, 42<br />
cuprimine .............................. 32<br />
cyclobenzaprine hcl .............. 43<br />
cyclophosphamide................. 13<br />
cyclosporine .......................... 35<br />
cyklokapron........................... 23<br />
cymbalta 20, 30 mg ................. 9<br />
cymbalta 60 mg ....................... 9<br />
D<br />
danazol .................................. 33<br />
dapsone ................................. 13<br />
daptacel ................................. 36<br />
daraprim ................................ 16<br />
decavac .................................. 36<br />
dermotic ................................ 40<br />
desipramine hcl ....................... 9<br />
desmopressin acetate ............. 32<br />
desonide ................................ 29<br />
desoximetasone ..................... 29<br />
detrol ..................................... 31<br />
detrol la ................................. 31<br />
dexamethasone ................ 12, 37<br />
dexamethasone sod phos . 12, 39<br />
dexilant .................................. 31<br />
dextroamphetamine sulfate ... 27<br />
dextrose ................................. 44<br />
dextrose/nacl inj .................... 44<br />
diazepam ............................... 20<br />
diclofenac potassium ............... 1<br />
diclofenac sodium ................... 1<br />
dicloxacillin sodium ................ 5<br />
dicyclomine hcl ..................... 30<br />
47
didanosine ............................. 18<br />
diflorasone diacetate ............. 29<br />
diflunisal ................................. 1<br />
digoxin .................................. 25<br />
dihydroergotamine mesylate . 12<br />
dilantin infatabs ....................... 7<br />
diltiazem cd ........................... 25<br />
diltiazem er 360, 420 mg cap 25<br />
diltiazem er cap ..................... 25<br />
diltiazem inj, tab .................... 25<br />
dilt-xr..................................... 25<br />
diovan .................................... 26<br />
diovan 320 mg....................... 27<br />
diovan hct .............................. 27<br />
diovan hct 320-12.5, 320-25mg<br />
........................................... 27<br />
diphenhydramine hcl ............. 10<br />
diphenoxylate/atropine .......... 30<br />
diphtheria/tetanus toxoid ....... 36<br />
dipyridamole ......................... 23<br />
disopyramide phosphate........ 23<br />
divalproex sodium ................... 7<br />
docetaxel ............................... 14<br />
donepezil ................................. 8<br />
dorzolamide hcl ..................... 40<br />
dorzolamide hcl/timolol malea<br />
........................................... 40<br />
dovonex ................................. 29<br />
doxazosin mesylate ............... 23<br />
doxepin hcl .............................. 9<br />
doxycycline 10 mg/ml inj ....... 6<br />
doxycycline hyclate ................ 6<br />
doxycycline monohydrate ....... 6<br />
dronabinol 10 mg .................. 10<br />
dronabinol 2.5, 5 mg ............. 10<br />
duetact ................................... 20<br />
duramorph ............................... 2<br />
dyrenium ............................... 25<br />
E<br />
econazole nitrate ................... 11<br />
edecrin sodium ...................... 25<br />
edurant................................... 18<br />
effient .................................... 23<br />
elitek ...................................... 14<br />
elmiron .................................. 30<br />
embeda .................................... 2<br />
emcyt ..................................... 14<br />
emend 125 mg ....................... 10<br />
emend 40 mg ......................... 10<br />
emend 80 mg ......................... 10<br />
emend pak ............................. 10<br />
emsam ..................................... 8<br />
emtriva .................................. 18<br />
enalapril maleate ................... 27<br />
enalapril maleate/hctz ........... 23<br />
enbrel 25 mg ......................... 35<br />
enbrel 25 mg/0.5ml ............... 35<br />
enbrel 50 mg/ml .................... 35<br />
endocet .................................... 2<br />
endocet 10-650 mg .................. 2<br />
endocet 7.5-500 mg ................. 2<br />
engerix-b vacc ....................... 36<br />
enoxaparin ............................. 22<br />
entocort ec ............................. 30<br />
epivir ..................................... 18<br />
epivir hbv .............................. 19<br />
eplerenone ............................. 25<br />
epzicom tab ........................... 18<br />
erythrocin stearate ................... 5<br />
erythromycin ........................... 6<br />
erythromycin ethylsuccinate ... 6<br />
erythromycin/benzoyl pero ... 29<br />
erythromycin/sulfisoxazole ..... 6<br />
estazolam............................... 43<br />
estrace ................................... 33<br />
estradiol 0.0375, 0.06 mg dis 33<br />
estradiol dis ........................... 33<br />
estradiol tab ........................... 33<br />
ethambutol hcl ....................... 13<br />
ethosuximide ........................... 7<br />
etodolac ................................... 1<br />
etoposide ............................... 15<br />
eurax ...................................... 16<br />
evista ..................................... 34<br />
exelon ...................................... 8<br />
exemestane ............................ 15<br />
exjade 125 mg tab ................. 10<br />
exjade 250, 500 mg tab ......... 10<br />
F<br />
fabrazyme .............................. 30<br />
famciclovir ............................ 19<br />
famotidine ............................. 31<br />
fanapt..................................... 17<br />
fareston .................................. 14<br />
faslodex ................................. 34<br />
fazaclo ................................... 17<br />
felbatol .................................... 7<br />
feldene ..................................... 1<br />
felodipine er .......................... 25<br />
femhrt .................................... 38<br />
femring .................................. 33<br />
femtrace ................................. 33<br />
fenofibrate ............................. 26<br />
fenoprofen calcium ................. 1<br />
fentanyl lozenge ...................... 2<br />
fentanyl lozenge 0.2 mg .......... 2<br />
fentanyl transdermal patch ...... 2<br />
fentora ..................................... 2<br />
fexmid ................................... 43<br />
fexofenadine 180 mg ............. 41<br />
fexofenadine 30, 60 mg ......... 41<br />
finacea ................................... 29<br />
finasteride .............................. 32<br />
fioricet/codeine ....................... 2<br />
fiorinal/codeine ....................... 2<br />
firmagon ................................ 34<br />
flagyl ....................................... 4<br />
flarex ..................................... 39<br />
flavoxate ................................ 31<br />
flecainide acetate ................... 23<br />
flector ...................................... 1<br />
flexeril ................................... 43<br />
flomax ................................... 32<br />
flonase ................................... 40<br />
flovent ................................... 40<br />
flovent hfa 110, 220 mcg ...... 41<br />
flovent hfa 44 mcg ................ 41<br />
fluconazole ............................ 11<br />
fluconazole 2 mg/ml inj ........ 11<br />
fludrocortisone ...................... 32<br />
flunisolide ............................. 41<br />
fluocinolone acetonide .......... 29<br />
fluocinonide .......................... 29<br />
fluocinonide emollient ba ..... 29<br />
fluorometholone .................... 39<br />
fluorouracil ............................ 29<br />
fluoxetine 10 mg cap ............... 9<br />
fluoxetine 20 mg cap ............... 9<br />
fluoxetine 40 mg cap ............... 9<br />
fluoxetine sol, tab .................... 9<br />
fluphenazine .......................... 17<br />
fluphenazine decanoate ......... 17<br />
flurazepam ............................. 43<br />
flurbiprofen ............................. 1<br />
flurbiprofen sodium .............. 39<br />
flutamide ............................... 34<br />
fluticasone propionate ..... 29, 41<br />
fluvoxamine maleate ............... 9<br />
fml ......................................... 39<br />
focalin ................................... 27<br />
48
folic acid................................ 44<br />
fomepizole............................. 10<br />
foradil .................................... 42<br />
fortamet ................................. 20<br />
fortaz ....................................... 5<br />
forteo ..................................... 37<br />
fortical ................................... 37<br />
fosamax ................................. 37<br />
fosamax plus d 70-2800 mg .. 37<br />
fosamax plus d 70-5600 mg .. 37<br />
foscarnet sodium ................... 18<br />
fosinopril sodium .................. 27<br />
fosinopril sodium/hctz .......... 23<br />
fosphenytoin sodium ............... 7<br />
fosrenol ................................. 32<br />
fragmin 10000 u .................... 22<br />
fragmin 12500, 15000, 18000 u<br />
........................................... 22<br />
fragmin 2500 u/0.2ml, 25000 u<br />
........................................... 22<br />
fragmin 7500 u/0.3ml............ 22<br />
freamine iii ............................ 44<br />
freamine iii 3% ...................... 44<br />
frova ...................................... 12<br />
furosemide............................. 25<br />
fuzeon .................................... 18<br />
G<br />
gabapentin ............................... 7<br />
gabitril 12 mg .......................... 7<br />
gabitril 2, 16 mg ...................... 7<br />
gabitril 4 mg ............................ 7<br />
galantamine 12 mg tab ............ 8<br />
galantamine 4 mg tab .............. 8<br />
galantamine 8 mg tab .............. 8<br />
galantamine er cap .................. 8<br />
gamastan s/d .......................... 35<br />
gammagard liquid ................. 35<br />
gamunex ................................ 35<br />
ganciclovir............................. 18<br />
gardasil .................................. 36<br />
gastrocrom............................. 42<br />
gauze pads ............................. 20<br />
gaviltye-g .............................. 30<br />
gavilyte-c............................... 30<br />
gavilyte-n .............................. 30<br />
gelnique ................................. 31<br />
gemfibrozil ............................ 26<br />
gemzar ................................... 14<br />
gengraf .................................. 35<br />
gentak ...................................... 3<br />
gentamicin ............................... 4<br />
gentamicin/nacl 100 mg .......... 4<br />
gentamicin/nacl 60, 80 mg ...... 4<br />
gentasol ................................... 4<br />
geodon ................................... 17<br />
gilenya ................................... 28<br />
gleevec 100 mg ..................... 15<br />
gleevec 400 mg ..................... 15<br />
glimepiride ............................ 20<br />
glipizide................................. 20<br />
glipizide/metformin hcl ......... 20<br />
glucagen hypokit ................... 21<br />
glucagon emergency kit ........ 21<br />
glucophage ............................ 20<br />
glucotrol ................................ 20<br />
glucovance ............................ 20<br />
glumetza ................................ 20<br />
glyburide ............................... 20<br />
glyburide micronized ............ 20<br />
glyburide/metformin hcl ....... 21<br />
glycopyrrolate ....................... 30<br />
glynase .................................. 21<br />
glyset ..................................... 21<br />
golytely ................................. 30<br />
granisetron 0.1mg/ml inj, tab 10<br />
granisetron 1mg/ml inj .......... 10<br />
granisol .................................. 10<br />
grifulvin v.............................. 11<br />
griseofulvin microsize ........... 11<br />
gris-peg ................................. 11<br />
guanabenz ............................. 23<br />
gynazole-1 ............................. 11<br />
H<br />
halaven .................................. 14<br />
haldol..................................... 17<br />
halobetasol propionate .......... 29<br />
halog ...................................... 29<br />
haloperidol decanoate ........... 17<br />
haloperidol lactate ................. 17<br />
haloperidol oral conc ............. 17<br />
haloperidol tab ...................... 17<br />
havrix .................................... 36<br />
hctz ........................................ 25<br />
hectorol ................................. 37<br />
helidac therapy ...................... 30<br />
heparin sodium ...................... 22<br />
heparin sodium/d5w .............. 22<br />
heparin sodium/nacl .............. 22<br />
hepatamine ............................ 44<br />
hepsera .................................. 19<br />
herceptin ................................ 14<br />
hexalen .................................. 13<br />
hiprex ...................................... 4<br />
humalog................................. 21<br />
humalog mix ......................... 21<br />
humalog pen .......................... 21<br />
humatrope 12 mg .................. 32<br />
humatrope 6, 24 mg .............. 32<br />
humatrope combo pack ......... 32<br />
humira 20 mg/0.4ml .............. 35<br />
humira 40 mg/0.8ml .............. 35<br />
humira pen-crohns ................ 35<br />
humulin 70/30 ....................... 21<br />
humulin n .............................. 21<br />
humulin r ............................... 21<br />
hycamtin ................................ 15<br />
hydralazine hcl ...................... 27<br />
hydrea .................................... 14<br />
hydroco/apap 10-325 mg ........ 2<br />
hydroco/apap 10-500 mg ........ 2<br />
hydroco/apap 10-650 mg ........ 2<br />
hydroco/apap 10-660 mg ........ 2<br />
hydroco/apap 2.5-500 mg ....... 2<br />
hydroco/apap 5-325 mg .......... 2<br />
hydroco/apap 5-500 mg .......... 2<br />
hydroco/apap 7.5-325 mg ....... 2<br />
hydroco/apap 7.5-500 mg ....... 2<br />
hydroco/apap 7.5-650 mg ....... 2<br />
hydroco/apap 7.5-750 mg ....... 2<br />
hydroco/apap sol ..................... 2<br />
hydroco/homatropine ............ 42<br />
hydroco/ibuprofen ................... 2<br />
hydrocortisone................. 29, 32<br />
hydrocortisone butyrate ........ 29<br />
hydrocortisone valerate ......... 29<br />
hydromet ............................... 42<br />
hydromorphone hcl ................. 2<br />
hydroxychloroquine sulfate .. 16<br />
hydroxyurea .......................... 14<br />
hydroxyzine hcl ..................... 10<br />
hydroxyzine pamoate ............ 10<br />
hyzaar .................................... 27<br />
I<br />
ibuprofen ................................. 1<br />
idamycin ................................ 14<br />
idarubicin hcl ........................ 14<br />
ifex ........................................ 14<br />
ifosfamide 50 mg/ml ............. 14<br />
ifosfamide/mesna 1 gm ......... 14<br />
ifosfamide/mesna 3 gm ......... 14<br />
49
imipramine hcl ........................ 9<br />
imipramine pamoate ................ 9<br />
imiquimod ............................. 29<br />
imitrex ................................... 12<br />
imovax rabies (h.d.c.v.)......... 36<br />
imuran ................................... 35<br />
increlex .................................. 33<br />
indapamide ............................ 26<br />
inderal ................................... 24<br />
indocin..................................... 1<br />
indomethacin ........................... 1<br />
infanrix .................................. 36<br />
infergen ................................. 19<br />
infumorph ................................ 2<br />
innohep .................................. 22<br />
innopran ................................ 24<br />
inspra ..................................... 26<br />
insulin pen needles ................ 21<br />
insulin syrg/needles ............... 21<br />
intelence ................................ 18<br />
intralipid ................................ 44<br />
intralipid 20% inj .................. 44<br />
intron a 10 mu inj .................. 36<br />
intron a 18 mu inj .................. 36<br />
intron a pen ........................... 36<br />
intuniv ................................... 28<br />
invanz ...................................... 5<br />
invega 6 mg tab ..................... 17<br />
invega inj ............................... 17<br />
invega tab .............................. 17<br />
invirase cap ........................... 18<br />
invirase tab ............................ 18<br />
ionosol-mb ............................ 44<br />
ionosol-t ................................ 44<br />
iopidine ................................. 40<br />
ipol inactivated ipv ................ 36<br />
ipratropium bromide inh sol .. 41<br />
ipratropium bromide nasal spr<br />
........................................... 41<br />
iquix ........................................ 6<br />
iressa ..................................... 15<br />
irinotecan hcl inj ................... 14<br />
isentress ................................. 18<br />
isochron ................................. 27<br />
isolyte-h/dextrose 5% ............ 44<br />
isolyte-m/dextrose 5% .......... 44<br />
isolyte-p/dextrose 5% ............ 44<br />
isolyte-s ................................. 44<br />
isolyte-s/dextrose 5% ............ 44<br />
isonarif .................................. 13<br />
isoniazid ................................ 13<br />
isoptin .................................... 25<br />
isordil .................................... 27<br />
isosorbide dinitrate ................ 27<br />
isosorbide mononitrate .......... 27<br />
isradipine ............................... 25<br />
istalol ..................................... 40<br />
istodax ................................... 15<br />
itraconazole ........................... 11<br />
ixempra ................................. 14<br />
ixiaro ..................................... 36<br />
J<br />
jalyn....................................... 32<br />
jantoven ................................. 22<br />
janumet .................................. 21<br />
januvia ................................... 21<br />
je-vax..................................... 36<br />
jinteli ..................................... 38<br />
jolivette ................................. 33<br />
junel....................................... 38<br />
K<br />
kadian cr 10, 50, 80 mg ........... 2<br />
kadian cr 100, 200 mg ............. 2<br />
kadian cr 20, 30, 60 mg ........... 2<br />
kaletra .................................... 18<br />
kanamycin sulfate ................... 4<br />
kariva..................................... 38<br />
kayexalate ............................. 43<br />
kcl/d5w .................................. 44<br />
kcl/d5w/lr inj ......................... 44<br />
kcl/d5w/nacl .......................... 44<br />
kcl/nacl 0.3-0.9 inj ................ 44<br />
kcl/nacl inj ............................. 44<br />
keflex....................................... 5<br />
kelnor .................................... 38<br />
kenalog .................................. 29<br />
kepivance .............................. 28<br />
keppra ...................................... 6<br />
keppra xr 500 mg .................... 6<br />
kerlone................................... 24<br />
ketek ........................................ 6<br />
ketoconazole ......................... 11<br />
ketoprofen ............................... 1<br />
ketoprofen er ........................... 1<br />
ketorolac ................................ 39<br />
ketorolac tromethamine inj ..... 1<br />
ketorolac tromethamine tab ..... 1<br />
kineret ................................... 36<br />
kionex .................................... 43<br />
klaron ...................................... 6<br />
klor-con ................................. 44<br />
kristalose ............................... 30<br />
k-tab ...................................... 44<br />
kuvan ..................................... 30<br />
L<br />
labetalol hcl ........................... 24<br />
lac-hydrin .............................. 29<br />
laclotion................................. 29<br />
lacrisert .................................. 16<br />
lactated ringer's irr ................ 44<br />
lactated ringer's viaflex ......... 44<br />
lactulose ................................ 30<br />
lamictal .................................... 7<br />
lamictal kit .............................. 7<br />
lamisil .................................... 11<br />
lamotrigine .............................. 7<br />
lamotrigine 150, 200 mg ......... 7<br />
lanoxin................................... 25<br />
lansoprazole .......................... 31<br />
lantus ..................................... 21<br />
lantus solostar ........................ 21<br />
lasix 20, 40 mg ...................... 26<br />
lasix 80 mg ............................ 26<br />
latanoprost ............................. 40<br />
latuda ..................................... 17<br />
leena ...................................... 38<br />
leflunomide ........................... 36<br />
lescol ..................................... 26<br />
lessina .................................... 38<br />
letairis .................................... 42<br />
letrozole................................. 15<br />
leucovorin inj ........................ 14<br />
leucovorin tab........................ 14<br />
leukeran ................................. 13<br />
leukine 250 mcg .................... 22<br />
leukine 500 mcg .................... 22<br />
leuprolide acetate .................. 34<br />
leustatin ................................. 14<br />
levalbuterol inh sol ................ 42<br />
levaquin inj, tab ....................... 6<br />
levaquin sol, premix ................ 6<br />
levatol .................................... 24<br />
levemir .................................. 21<br />
levetiracetam ........................... 6<br />
levobunolol hcl ...................... 40<br />
levobunolol hcl 0.5% op sol . 40<br />
levocarnitine .......................... 44<br />
levora..................................... 38<br />
levorphanol ............................. 2<br />
levothroid .............................. 32<br />
50
levothyroxine sodium............ 32<br />
levoxyl................................... 32<br />
lexapro sol ............................... 9<br />
lexapro tab ............................... 9<br />
lexiva ..................................... 18<br />
lialda ...................................... 37<br />
lidocaine .................................. 3<br />
lidocaine/prilocaine ................. 3<br />
lidoderm .................................. 3<br />
lincocin .................................... 4<br />
lindane ................................... 16<br />
liothyronine sodium inj ......... 32<br />
liothyronine sodium tab ........ 32<br />
lipitor ..................................... 26<br />
lipofen ................................... 26<br />
liposyn ................................... 44<br />
lisinopril ................................ 27<br />
lisinopril/hctz ........................ 23<br />
lithium carbonate .................. 20<br />
lithium citrate ........................ 20<br />
livalo ..................................... 26<br />
lo/ovral .................................. 38<br />
locoid..................................... 29<br />
loestrin................................... 38<br />
lofibra .................................... 26<br />
lokara..................................... 29<br />
lomotil ................................... 30<br />
loperamide hcl ....................... 31<br />
lopid ...................................... 26<br />
lopressor ................................ 24<br />
loprox gel .............................. 11<br />
loprox shampoo ..................... 11<br />
lorazepam .............................. 20<br />
lorcet ....................................... 2<br />
lortab ....................................... 2<br />
losartan .................................. 27<br />
losartan/hctz .......................... 27<br />
loseasonique .......................... 38<br />
lotemax .................................. 39<br />
lotensin .................................. 27<br />
lotensin hct ............................ 23<br />
lotrel ...................................... 25<br />
lotrisone................................. 29<br />
lotronex ................................. 31<br />
lovastatin ............................... 26<br />
lovaza .................................... 26<br />
lovenox 100 mg/ml ............... 22<br />
lovenox 120 mg/0.8ml .......... 22<br />
lovenox 150 mg/ml ............... 22<br />
lovenox 30 mg/0.3ml ............ 22<br />
lovenox 300 mg/3ml ............. 22<br />
lovenox 40 mg/0.4ml ............ 22<br />
lovenox 60 mg/0.6ml ............ 22<br />
lovenox 80 mg/0.8ml ............ 22<br />
low-ogestrel........................... 38<br />
loxapine succinate ................. 17<br />
loxitane .................................. 17<br />
lufyllin ................................... 41<br />
lumigan ................................. 40<br />
lunesta ................................... 43<br />
lupron depot .......................... 34<br />
lupron depot-ped ................... 34<br />
lutera 28 day .......................... 38<br />
luvox ....................................... 9<br />
luxiq ...................................... 29<br />
lybrel ..................................... 38<br />
lyrica ....................................... 7<br />
lysodren ................................. 34<br />
M<br />
macrobid ................................. 4<br />
macrodantin............................. 4<br />
magnacet ................................. 2<br />
magnesium sulfate ................ 44<br />
malarone ................................ 16<br />
malathion............................... 16<br />
maprotiline hcl ........................ 8<br />
margesic-h ............................... 2<br />
marinol .................................. 10<br />
marplan ................................... 8<br />
matulane ................................ 13<br />
mavik..................................... 27<br />
maxair ................................... 42<br />
maxalt .................................... 12<br />
maxidex ................................. 39<br />
maxidone ................................. 2<br />
maxitrol ................................. 39<br />
maxzide ................................. 26<br />
mebendazole ......................... 16<br />
meclizine hcl ......................... 10<br />
meclofenamate sodium ........... 1<br />
medroxyprogesterone ac inj .. 33<br />
medroxyprogesterone ac tab . 33<br />
mefloquine hcl ...................... 16<br />
megace .................................. 33<br />
megestrol acetate ................... 34<br />
meloxicam susp ....................... 1<br />
meloxicam tab ......................... 1<br />
melphalan .............................. 13<br />
menactra ................................ 36<br />
menest ................................... 33<br />
menomune-a/c/y/w-135 ........ 36<br />
menostar ................................ 33<br />
menveo inj ............................. 36<br />
meprobamate ......................... 20<br />
mepron .................................. 16<br />
mercaptopurine ..................... 35<br />
merrem .................................... 5<br />
mesalamine ........................... 37<br />
mesna inj ............................... 14<br />
mesnex inj ............................. 14<br />
mesnex tab ............................ 14<br />
mestinon ................................ 13<br />
mestinon 60 mg tab ............... 13<br />
metadate cap .......................... 28<br />
metadate tab .......................... 28<br />
metaglip................................. 21<br />
metaproterenol sulfate ........... 42<br />
metaxalone ............................ 43<br />
metformin hcl ........................ 21<br />
metformin hcl er 500 mg ....... 21<br />
metformin hcl er 750 mg ....... 21<br />
methadone hcl ......................... 2<br />
methadose ............................... 2<br />
methamphetamine hcl ........... 27<br />
methazolamide ...................... 26<br />
methenamine hippurate ........... 4<br />
methergine............................. 32<br />
methimazole .......................... 34<br />
methitest ................................ 33<br />
methocarbamol ...................... 43<br />
methotrexate .......................... 35<br />
methotrexate 50 mg/ml inj .... 35<br />
methscopolamine .................. 30<br />
methyclothiazide ................... 26<br />
methyldopa ............................ 23<br />
methyldopa/hctz .................... 23<br />
methyldopate hcl ................... 23<br />
methylin ................................ 28<br />
methylphenidate hcl .............. 28<br />
methylprednisolone ............... 12<br />
methylprednisolone ac .......... 12<br />
metipranolol .......................... 40<br />
metoclopramide hcl ............... 10<br />
metolazone ............................ 26<br />
metoprolol succinate er ......... 24<br />
metoprolol tartrate ................. 24<br />
metoprolol/hctz ..................... 24<br />
metozolv ................................ 11<br />
metrocream ............................. 4<br />
metrogel .................................. 4<br />
51
metrolotion .............................. 4<br />
metronidazole cap, tab ............ 4<br />
metronidazole crm .................. 4<br />
mevacor ................................. 26<br />
mexiletine hcl ........................ 23<br />
miacalcin ............................... 37<br />
micardis ................................. 27<br />
micardis hct ........................... 27<br />
miconazole ............................ 11<br />
microgestin ............................ 38<br />
microzide............................... 26<br />
midodrine hcl ........................ 23<br />
migergot ................................ 12<br />
migranal ................................ 12<br />
millipred ................................ 12<br />
minipress ............................... 23<br />
minitran ................................. 27<br />
minocin ................................... 6<br />
minocycline ............................. 6<br />
minoxidil ............................... 27<br />
mirapex ................................. 16<br />
mirapex er ............................. 16<br />
mirtazapine .............................. 8<br />
misoprostol ............................ 31<br />
mitoxantrone hcl ................... 14<br />
m-m-r ii ................................. 36<br />
mobic....................................... 1<br />
modicon................................. 38<br />
moexipril hcl ......................... 27<br />
moexipril/hctz ....................... 23<br />
mometasone furoate .............. 29<br />
monodox ................................. 6<br />
monoket................................. 27<br />
mononessa ............................. 38<br />
morphine sulfate ...................... 2<br />
morphine sulfate inj ................ 2<br />
motofen ................................. 31<br />
moviprep ............................... 31<br />
moxatag ................................... 5<br />
mozobil ................................. 22<br />
ms contin ................................. 3<br />
multaq ................................... 23<br />
mupirocin ................................ 4<br />
mustargen .............................. 14<br />
myambutol ............................ 13<br />
mycamine .............................. 11<br />
mycobutin ............................. 13<br />
mycophenolate mofetil.......... 35<br />
mydriacyl .............................. 39<br />
myfortic ................................. 35<br />
myozyme ............................... 30<br />
mysoline .................................. 7<br />
mytelase ................................ 13<br />
N<br />
nabumetone ............................. 1<br />
nadolol................................... 24<br />
nadolol/bend .......................... 24<br />
nafcillin 1, 10 gm .................... 5<br />
nafcillin 20 mg/ml ................... 5<br />
naftin ..................................... 11<br />
naglazyme ............................. 30<br />
nalbuphine hcl ......................... 3<br />
nalfon ...................................... 1<br />
naloxone hcl .......................... 10<br />
naltrexone hcl ........................ 10<br />
namenda sol ............................ 8<br />
namenda tab ............................ 8<br />
naprelan ................................... 1<br />
naprosyn .................................. 1<br />
naproxen .................................. 1<br />
nasacort ................................. 41<br />
nasonex ................................. 41<br />
natacyn .................................. 11<br />
nateglinide ............................. 21<br />
navane ................................... 17<br />
nebupent ................................ 16<br />
nefazodone hcl ........................ 8<br />
neomycin sulfate ..................... 4<br />
neomycin/polymyxin b sulf .. 38<br />
neomycin/polymyxin/dexame 39<br />
neomycin/polymyxin/gramic 39<br />
neomycin/polymyxin/hc . 39, 40<br />
neoral..................................... 35<br />
neosporin sol ......................... 39<br />
nephramine ............................ 44<br />
neulasta ................................. 22<br />
neumega ................................ 22<br />
neupogen ............................... 22<br />
neupogen 480 mcg/1.6ml ...... 22<br />
neurontin ................................. 7<br />
neurontin sol............................ 7<br />
nevanac ................................. 39<br />
nexavar .................................. 15<br />
nexium................................... 31<br />
nexium inj ............................. 31<br />
niacor..................................... 26<br />
niaspan .................................. 26<br />
nicardipine hcl ....................... 25<br />
nicotrol .................................. 10<br />
nifediac cc ............................. 25<br />
nifedical xl ............................ 25<br />
nifedipine .............................. 25<br />
nifedipine er .......................... 25<br />
nilandron ............................... 34<br />
nimodipine ............................ 25<br />
nipent..................................... 14<br />
nisoldipine ............................. 25<br />
nitro-bid................................. 27<br />
nitro-dur ................................ 27<br />
nitrofurantoin .......................... 4<br />
nitrofurantoin macrocrystal ..... 4<br />
nitrofurantoin monohydrate .... 4<br />
nitroglycerin .......................... 27<br />
nitrolingual pumpspray ......... 27<br />
nitrostat ................................. 27<br />
nizatidine 150 mg .................. 31<br />
nizatidine 300 mg .................. 31<br />
nizoral ................................... 11<br />
nora-be .................................. 34<br />
norco ....................................... 3<br />
nordette ................................. 38<br />
norditropin............................. 33<br />
norethindrone acetate ............ 34<br />
norflex ................................... 43<br />
norinyl ................................... 38<br />
noritate .................................... 4<br />
normosol-m in d5w ............... 44<br />
normosol-r ............................. 44<br />
normosol-r in d5w ................. 44<br />
noroxin .................................... 6<br />
norpace .................................. 24<br />
norpramin ................................ 9<br />
nor-qd .................................... 34<br />
nortrel .................................... 38<br />
nortriptyline hcl ..................... 10<br />
norvasc .................................. 25<br />
norvir ..................................... 18<br />
novantrone............................. 14<br />
novarel................................... 33<br />
novolin 70/30 ........................ 21<br />
novolin n ............................... 21<br />
novolin r ................................ 21<br />
novolog ................................. 21<br />
novolog mix 70/30 ................ 21<br />
noxafil ................................... 11<br />
nucynta .................................... 3<br />
nulytely ................................. 31<br />
nutropin ................................. 33<br />
nutropin aq ............................ 33<br />
nuvaring ................................ 38<br />
52
nuvigil ................................... 43<br />
nyamyc .................................. 11<br />
nystatin .................................. 12<br />
nystatin powder, tab .............. 12<br />
nystatin/triamcinolone ........... 29<br />
nystop .................................... 12<br />
O<br />
ocella ..................................... 38<br />
octreotide acetate .................. 34<br />
ocufen .................................... 39<br />
ocuflox .................................... 6<br />
ofloxacin ................................. 6<br />
ogestrel .................................. 38<br />
oleptro ..................................... 8<br />
olux ....................................... 29<br />
omeprazole ............................ 31<br />
omnaris .................................. 41<br />
omnipred ............................... 39<br />
omnitrope .............................. 33<br />
omnitrope 5.8 mg .................. 33<br />
ondansetron inj ..................... 11<br />
ondansetron 24 mg tab .......... 11<br />
ondansetron 4 mg tab ............ 11<br />
ondansetron 8 mg tab ............ 11<br />
ondansetron odt ..................... 11<br />
ondansetron sol ..................... 11<br />
onglyza .................................. 21<br />
onsolis ..................................... 3<br />
ontak ...................................... 14<br />
opana ....................................... 3<br />
opana er 30 mg ........................ 3<br />
opana er 5, 10, 20, 40 mg ........ 3<br />
optipranolol ........................... 40<br />
optivar ................................... 39<br />
oracea ...................................... 6<br />
oramorph ................................. 3<br />
orap ....................................... 17<br />
orapred ............................ 12, 40<br />
oravig .................................... 12<br />
orencia ................................... 35<br />
orfadin ................................... 30<br />
orphenadrine citrate .............. 43<br />
orphenadrine/asa/caff .............. 3<br />
ortho evra .............................. 38<br />
ortho micronor ...................... 34<br />
ortho tri-cyclen lo .................. 38<br />
ortho-cept .............................. 38<br />
orthoclone okt3 ..................... 35<br />
ortho-cyclen .......................... 38<br />
ortho-novum .......................... 38<br />
osmoprep ............................... 44<br />
ovcon ..................................... 38<br />
ovide ...................................... 16<br />
oxacillin inj ............................ 5<br />
oxacillin dex inj....................... 5<br />
oxaliplatin inj ........................ 14<br />
oxandrin ................................ 33<br />
oxandrolone 10mg tab........... 33<br />
oxandrolone 2.5mg tab.......... 33<br />
oxaprozin................................. 1<br />
oxazepam .............................. 20<br />
oxcarbazepine ......................... 7<br />
oxistat .................................... 12<br />
oxsoralen ............................... 29<br />
oxsoralen ultra ....................... 29<br />
oxybutynin chloride .............. 31<br />
oxybutynin chloride er .......... 31<br />
oxycodone hcl ......................... 3<br />
oxycodone hcl sol ................... 3<br />
oxycodone hcl/ibuprofen ........ 1<br />
oxycodone/apap ...................... 3<br />
oxycodone/apap 7.5-500mg .... 3<br />
oxycontin cr ............................ 3<br />
oxycontin cr 80 mg ................. 3<br />
oxymorphone .......................... 3<br />
oxytrol ................................... 32<br />
P<br />
pacerone ................................ 24<br />
paclitaxel ............................... 14<br />
palgic liq................................ 41<br />
palgic tab ............................... 41<br />
pamelor ................................. 10<br />
pamidronate disodium ........... 37<br />
pamine ................................... 30<br />
pancreaze ............................... 30<br />
pandel .................................... 29<br />
panlor ss .................................. 3<br />
panretin ................................. 15<br />
pantoprazole sodium ............. 31<br />
parafon forte dsc ................... 43<br />
parcaine ................................. 39<br />
parcopa .................................. 16<br />
parlodel ................................. 16<br />
parnate ..................................... 9<br />
paromomycin .......................... 4<br />
paroxetine 10 tab ................... 19<br />
paroxetine er 12.5 mg tab ........ 8<br />
paroxetine er 25 mg tab ........... 9<br />
paroxetine er 37.5 mg tab ........ 9<br />
paroxetine susp...................... 19<br />
paroxetine tab ........................ 19<br />
paser ...................................... 13<br />
pataday .................................. 39<br />
patanase ................................. 41<br />
patanol ................................... 39<br />
paxil................................... 9, 19<br />
pce ........................................... 6<br />
pediapred ............................... 12<br />
pedi-dri .................................. 12<br />
pedvax hib ............................. 36<br />
peganone ................................. 7<br />
pegasys .................................. 19<br />
pegintron ............................... 19<br />
penicillin g potassium ............. 5<br />
penicillin g sodium .................. 5<br />
penicillin v potassium ............. 5<br />
penlac nail lacquer ................ 12<br />
pentam ................................... 16<br />
pentasa................................... 37<br />
pentazocine/apap ..................... 3<br />
pentazocine/naloxone hcl ...... 10<br />
pentostatin inj ........................ 14<br />
pentoxifylline er .................... 25<br />
pepcid .................................... 31<br />
percocet ................................... 3<br />
percodan .................................. 3<br />
perforomist ............................ 42<br />
perindopril erbumine ............. 27<br />
periogard ............................... 28<br />
periostat ................................... 6<br />
permethrin ............................. 16<br />
perphenazine ......................... 11<br />
perphenazine/amitriptylin ..... 10<br />
persantine .............................. 23<br />
pexeva ................................... 19<br />
pexeva 10 mg ........................ 19<br />
pfizerpen ................................. 5<br />
phenadoz ............................... 11<br />
phenelzine ............................... 9<br />
phenergan .............................. 11<br />
phenobarbital ........................... 7<br />
phenytek .................................. 7<br />
phenytoin................................. 7<br />
phenytoin er 200mg cap .......... 7<br />
phenytoin susp ........................ 7<br />
phoslo .................................... 32<br />
phospholine iodide ................ 40<br />
photofrin ................................ 15<br />
physiolyte .............................. 44<br />
physiosol irrigation ............... 44<br />
53
pilocarpine hcl ....................... 28<br />
pilopine hs ............................. 40<br />
pindolol ................................. 24<br />
piperacillin sodium.................. 5<br />
piroxicam ................................ 1<br />
plaquenil ................................ 16<br />
plasma-lyte 56 ....................... 45<br />
plasma-lyte a ......................... 45<br />
plasma-lyte-148..................... 45<br />
plasma-lyte-148/d5w............. 45<br />
plasma-lyte-56/d5w............... 45<br />
plasma-lyte-r ......................... 45<br />
plavix..................................... 23<br />
pletal ...................................... 23<br />
podofilox ............................... 29<br />
poly pred ............................... 39<br />
poly-dex ................................ 39<br />
polyethylene glycol ............... 31<br />
potassium chloride ................ 45<br />
potassium citrate er ............... 45<br />
pradaxa .................................. 22<br />
pramipexole........................... 16<br />
prandin .................................. 21<br />
pravachol ............................... 26<br />
pravastatin sodium ................ 26<br />
prazosin hcl ........................... 23<br />
precose .................................. 21<br />
pred forte ............................... 40<br />
pred mild ............................... 40<br />
pred-g .................................... 39<br />
prednicarbate ......................... 29<br />
prednisolone acetate .............. 40<br />
prednisolone sod phosp ......... 12<br />
prednisolone sod phosp op .... 40<br />
prednisone ............................. 12<br />
prefest .................................... 38<br />
pregnyl .................................. 33<br />
premarin ................................ 33<br />
premasol ................................ 45<br />
premphase ............................. 38<br />
prempro ................................. 38<br />
prenatabs obn ........................ 39<br />
prevalite................................. 26<br />
previfem ................................ 38<br />
prevpac .................................. 31<br />
prezista ............................ 15, 18<br />
priftin..................................... 13<br />
prilosec .................................. 31<br />
primaxin .................................. 5<br />
primidone ................................ 7<br />
pristiq ...................................... 9<br />
privigen ................................. 35<br />
proair hfa ............................... 42<br />
probenecid ............................. 12<br />
procainamide hcl ................... 24<br />
procalamine ........................... 45<br />
procardia ............................... 25<br />
procardia xl ........................... 25<br />
prochlorperazine ................... 11<br />
prochlorperazine edisylate .... 11<br />
prochlorperazine maleate ...... 11<br />
procrit 10000/ml.................... 22<br />
procrit 2000/ml...................... 22<br />
procrit 20000/ml.................... 22<br />
procrit 3000/ml...................... 22<br />
procrit 4000/ml...................... 22<br />
procrit 40000/ml.................... 23<br />
proctocream-hc ..................... 37<br />
procto-pak ............................. 37<br />
proctosol hc ........................... 37<br />
proctozone-hc ........................ 37<br />
proglycem ............................. 21<br />
prograf ................................... 35<br />
prolastin................................. 42<br />
proleukin ............................... 15<br />
prolia ..................................... 37<br />
promacta ................................ 23<br />
promethazine hcl ................... 11<br />
promethazine vc/codeine ...... 42<br />
promethazine/codeine ........... 42<br />
promethegan .......................... 11<br />
prometrium ............................ 34<br />
propafenone hcl ..................... 24<br />
propine .................................. 40<br />
propranolol 20 mg/5ml sol .... 24<br />
propranolol 40 mg/5ml sol .... 24<br />
propranolol er ........................ 24<br />
propranolol inj, tab ................ 24<br />
propranolol/hctz .................... 24<br />
propylthiouracil ..................... 35<br />
proquad ................................. 36<br />
proquin .................................... 6<br />
proscar ................................... 32<br />
prosol..................................... 45<br />
protonix ................................. 31<br />
protopic ................................. 29<br />
protriptyline hcl ..................... 10<br />
proventil hfa .......................... 42<br />
provera .................................. 34<br />
provigil 100 mg ..................... 43<br />
provigil 200 mg ..................... 43<br />
prozac ...................................... 9<br />
prozac weekly ......................... 9<br />
pulmicort ............................... 41<br />
pulmicort inh susp ................. 41<br />
pulmozyme ............................ 42<br />
purinethol .............................. 35<br />
pylera..................................... 31<br />
pyrazinamide ......................... 13<br />
pyridostigmine bromide ........ 13<br />
Q<br />
quinapril hcl .......................... 27<br />
quinapril/hctz ........................ 23<br />
quinidine gluconate cr ........... 24<br />
quinidine sulfate .................... 24<br />
qvar 40 mcg aer ..................... 41<br />
qvar 80 mcg aer ..................... 41<br />
R<br />
rabavert ................................. 36<br />
ramipril .................................. 27<br />
ranexa .................................... 25<br />
ranitidine ............................... 31<br />
ranitidine 150 mg cap ............ 31<br />
ranitidine syr ......................... 31<br />
rapamune 0.5 mg tab ............. 35<br />
rapamune 1, 2 mg tab ............ 35<br />
rapamune sol ......................... 35<br />
razadyne .................................. 8<br />
rebif ....................................... 28<br />
recombivax hb ....................... 36<br />
regranex ................................. 29<br />
relistor ................................... 31<br />
relpax..................................... 12<br />
remicade ................................ 35<br />
renvela ................................... 32<br />
repan ........................................ 3<br />
rescriptor ............................... 18<br />
restasis ................................... 39<br />
retrovir iv infusion ................ 18<br />
revatio inj .............................. 42<br />
revatio tab.............................. 42<br />
revlimid ................................. 13<br />
reyataz ................................... 19<br />
rhinocort aqua ....................... 41<br />
ribapak 400, 600 mg ............. 19<br />
ribapak pak ............................ 19<br />
ribasphere 200 mg cap, tab ... 19<br />
ribasphere 400, 600mg tab .... 19<br />
ribavirin ................................. 19<br />
rifampin ................................. 13<br />
54
ilutek .................................... 28<br />
rimantadine hcl ...................... 19<br />
ringer's injection .................... 45<br />
ringer's irrigation ................... 45<br />
risperdal................................. 17<br />
risperdal consta ..................... 17<br />
risperidone............................. 17<br />
risperidone sol ....................... 17<br />
ritalin cap .............................. 28<br />
ritalin tab ............................... 28<br />
rituxan ................................... 15<br />
robaxin .................................. 43<br />
robinul ................................... 30<br />
rocaltrol ................................. 37<br />
rocephin................................... 5<br />
romycin ................................... 6<br />
ropinirole hcl ......................... 16<br />
rotateq ................................... 36<br />
rowasa ................................... 37<br />
roxicet 5-325 mg tab ............... 3<br />
roxicet 5-500 mg tab ............... 3<br />
roxicet sol ................................ 3<br />
roxicodone 15, 30 mg tab........ 3<br />
roxicodone 5mg tab................. 3<br />
rozerem ................................. 43<br />
rythmol cap ........................... 24<br />
rythmol tab ............................ 24<br />
ryzolt ....................................... 3<br />
S<br />
sabril 500 mg tab ..................... 7<br />
sabril sol .................................. 7<br />
saizen 5 mg ........................... 33<br />
saizen 8.8 mg ........................ 33<br />
samsca ................................... 43<br />
sanctura ................................. 32<br />
sancuso .................................. 11<br />
sandimmune cap, sol ............. 35<br />
sandimmune inj ..................... 35<br />
sandostatin............................. 34<br />
sandostatin 0.05 mg/ml ......... 34<br />
santyl ..................................... 29<br />
saphris ................................... 20<br />
sarafem .................................... 9<br />
savella ................................... 28<br />
savella 4-week titration ......... 28<br />
selegiline hcl ......................... 16<br />
selenium sulfide .................... 29<br />
selfemra ................................... 9<br />
selzentry 150 mg ................... 18<br />
selzentry 300 mg ................... 18<br />
semprex-d .............................. 41<br />
sensipar 30 mg ...................... 34<br />
sensipar 60 mg ...................... 34<br />
sensipar 90 mg ...................... 34<br />
serevent diskus ...................... 42<br />
seromycin .............................. 13<br />
seroquel ................................. 17<br />
seroquel 300, 400 mg ............ 17<br />
seroquel xr ............................... 8<br />
serostim ................................. 33<br />
sertraline hcl .......................... 19<br />
sertraline hcl conc ................. 20<br />
silvadene ................................. 6<br />
silver sulfadiazine ................... 6<br />
simcor 1000/40 mg ............... 26<br />
simcor 500/20, 750/20 mg .... 26<br />
simponi .................................. 35<br />
simulect ................................. 35<br />
simvastatin ............................ 26<br />
sinemet .................................. 16<br />
sinemet cr .............................. 16<br />
singulair................................. 41<br />
singulair chw 5mg ................. 41<br />
skelaxin ................................. 43<br />
skelid ..................................... 37<br />
sodium bicarbonate ............... 45<br />
sodium chloride 0.9% irr...... 45<br />
sodium chloride<br />
0.45%,0.9%,3%................. 45<br />
sodium chloride 2.5 meq/ml . 45<br />
sodium chloride 5% .............. 45<br />
sodium fluoride ..................... 45<br />
sodium lactate ....................... 45<br />
sodium polystyrene sulfon .... 43<br />
solaraze ................................. 29<br />
solia ....................................... 38<br />
solodyn 105 mg ....................... 6<br />
solodyn 45, 90, 135 mg ........... 6<br />
solodyn 65, 115 mg ................. 6<br />
solu-cortef ............................. 12<br />
solu-medrol ........................... 12<br />
soma ...................................... 43<br />
somatuline 120 mg/.5ml........ 34<br />
somatuline 60 mg/0.2ml........ 34<br />
somavert ................................ 34<br />
sonata .................................... 43<br />
soriatane ................................ 29<br />
sorine ..................................... 24<br />
sotalol hcl .............................. 24<br />
sotret ...................................... 30<br />
spectracef ................................ 5<br />
spiriva handihaler .................. 41<br />
spironolactone ....................... 26<br />
sporanox ................................ 12<br />
sprintec .................................. 38<br />
sprycel 100 mg ...................... 15<br />
sprycel 20, 50, 70 mg ............ 15<br />
sprycel 80, 140 mg ................ 15<br />
sronyx .................................... 38<br />
ssd ........................................... 6<br />
stagesic .................................... 3<br />
stalevo ................................... 17<br />
starlix..................................... 21<br />
stavudine ............................... 18<br />
strattera 10, 18, 25 mg........... 28<br />
strattera 40, 60, 80, 100 mg... 28<br />
stromectol .............................. 16<br />
suboxone ............................... 10<br />
sucralfate ............................... 31<br />
sulfacetamide sodium/pred ... 39<br />
sulfadiazine ............................. 6<br />
sulfamethoxazole/trimetho ...... 6<br />
sulfasalazine .......................... 37<br />
sulfazine ec ............................ 37<br />
sulindac ................................... 1<br />
sumatriptan succ inj .............. 13<br />
sumatriptan succ tab .............. 13<br />
suprax ...................................... 5<br />
surmontil ............................... 10<br />
sustiva ................................... 18<br />
sutent ..................................... 15<br />
symbicort............................... 42<br />
symbyax .................................. 8<br />
symlin 120 inj 1000 mcg....... 21<br />
symlin 600 mcg inj ................ 21<br />
symlinpen 60 inj 1000 mcg ... 21<br />
synarel ................................... 34<br />
synthroid ............................... 32<br />
T<br />
tabloid ................................... 14<br />
tacrolimus .............................. 35<br />
tamiflu 30 mg ........................ 19<br />
tamiflu 45 mg ........................ 19<br />
tamiflu 75 mg ........................ 19<br />
tamoxifen citrate ................... 14<br />
tamsulosin ............................. 32<br />
tarceva ................................... 15<br />
targretin ................................. 15<br />
tasigna ................................... 15<br />
taxotere 80 mg/2ml inj .......... 15<br />
55
taxotere 80 mg/4ml inj .......... 15<br />
tazorac ................................... 30<br />
taztia xt .................................. 25<br />
tegretol .................................... 8<br />
tekturna ................................. 27<br />
tekturna hct............................ 27<br />
temazepam ............................ 43<br />
terazosin hcl .......................... 23<br />
terbinafine ............................. 12<br />
terbutaline sulfate .................. 42<br />
terconazole ............................ 12<br />
testosterone cypionate ........... 33<br />
testosterone enanthate ........... 33<br />
tetanus toxoid adsorbed......... 36<br />
tetanus/diphtheria toxoid ....... 36<br />
tetracycline hcl ........................ 6<br />
thalomid ................................ 13<br />
thalomid 200 mg ................... 14<br />
theochron............................... 41<br />
theophylline er ...................... 41<br />
theophylline er 400, 600 mg . 41<br />
thermazene .............................. 6<br />
thioridazine hcl ...................... 17<br />
thiothixene............................. 17<br />
thymoglobulin ....................... 36<br />
ticlopidine hcl ........................ 23<br />
tikosyn ................................... 24<br />
timolol ................................... 40<br />
timolol maleate ...................... 13<br />
timolol maleate op ................. 40<br />
tizanidine hcl ......................... 17<br />
tobi ........................................ 42<br />
tobramycin inj ......................... 4<br />
tobramycin sulfate ................... 4<br />
tobramycin/dexamethasone ... 39<br />
tobrasol .................................... 4<br />
tolmetin sodium ...................... 1<br />
topiramate 50 mg tab ............ 13<br />
topiramate cap ......................... 7<br />
topiramate tab........................ 13<br />
torisel..................................... 35<br />
torsemide ............................... 26<br />
tracleer ................................... 42<br />
tramadol hcl ............................ 3<br />
tramadol hcl er ........................ 3<br />
tramadol hcl/apap .................... 3<br />
trandolapril ............................ 27<br />
tranylcypromine sulfate .......... 9<br />
travasol .................................. 45<br />
travatan z ............................... 40<br />
trazodone hcl ........................... 8<br />
trecator .................................. 13<br />
tretinoin ................................. 15<br />
triamcinolone acetonide ........ 30<br />
triamcinolone in orabase ....... 28<br />
triamterene/hctz ..................... 26<br />
triazolam ............................... 43<br />
tricor ...................................... 26<br />
triderm ................................... 30<br />
trifluoperazine hcl ................. 17<br />
trifluridine ............................. 19<br />
trihexyphenidyl hcl ............... 17<br />
trimethoprim ........................... 4<br />
trimethoprim sulfate/poly...... 39<br />
tripedia .................................. 36<br />
trisenox .................................. 15<br />
trizivir .................................... 18<br />
tropicamide ........................... 39<br />
truvada................................... 18<br />
twinrix ................................... 36<br />
tykerb .................................... 15<br />
typhim vi ............................... 36<br />
tyzeka .................................... 19<br />
tyzine ..................................... 42<br />
tyzine ped nasal dro .............. 42<br />
U<br />
u-cort ..................................... 30<br />
uloric ..................................... 12<br />
unithroid ................................ 32<br />
V<br />
valacyclovir 1 gm tab ............ 19<br />
valacyclovir 500 mg tab ........ 19<br />
valcyte sol ............................. 18<br />
valcyte tab ............................. 18<br />
valproate sodium ..................... 7<br />
valproic acid ............................ 7<br />
vancocin hcl cap ...................... 4<br />
vancocin hcl inj ....................... 4<br />
vancomycin hcl ....................... 4<br />
vandazole ................................ 4<br />
vandetanib ............................. 15<br />
vaqta ...................................... 37<br />
varivax................................... 37<br />
velcade .................................. 15<br />
venlafaxine .............................. 9<br />
venlafaxine er 150 mg tab ...... 9<br />
venlafaxine er 225 mg tab ...... 9<br />
venlafaxine er 37.5,75 mg tab . 9<br />
ventavis ................................. 42<br />
ventolin hfa ........................... 42<br />
verapamil hcl ......................... 25<br />
vesicare ................................. 32<br />
viagra..................................... 32<br />
vidaza .................................... 15<br />
videx ...................................... 18<br />
viibryd ..................................... 9<br />
vimpat inj, oral sol .................. 8<br />
vimpat tab................................ 8<br />
viracept .................................. 19<br />
viracept 625 mg tab ............... 19<br />
viramune ............................... 18<br />
viread..................................... 18<br />
vitamin d ............................... 45<br />
vivaglobin ............................. 36<br />
voltaren ................................. 30<br />
votrient .................................. 15<br />
W<br />
warfarin sodium .................... 22<br />
welchol .................................. 21<br />
X<br />
xenazine 12.5 mg .................. 28<br />
xenazine 25 mg ..................... 28<br />
xgeva ..................................... 37<br />
xifaxan................................... 31<br />
xolair ..................................... 42<br />
xyrem .................................... 43<br />
Y<br />
yf-vax .................................... 37<br />
Z<br />
zafirlukast .............................. 41<br />
zaleplon 10 mg ...................... 43<br />
zaleplon 5 mg ........................ 43<br />
zavesca .................................. 30<br />
zazole .................................... 12<br />
zemplar .................................. 38<br />
zenpep ................................... 30<br />
zetia ....................................... 26<br />
ziagen .................................... 18<br />
zidovudine ............................. 18<br />
zinacef ..................................... 5<br />
zirgan..................................... 18<br />
zolinza ................................... 12<br />
zolpidem tartrate ................... 43<br />
zometa ................................... 38<br />
zonisamide .............................. 7<br />
zortress .................................. 35<br />
zostavax................................. 37<br />
zyflo cr .................................. 41<br />
zyprexa .................................. 17<br />
zyprexa zydis ........................ 17<br />
56
zytiga ..................................... 34 zyvox ....................................... 4<br />
57