antibioticos macrolidos - Farmacologia Virtual
antibioticos macrolidos - Farmacologia Virtual
antibioticos macrolidos - Farmacologia Virtual

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
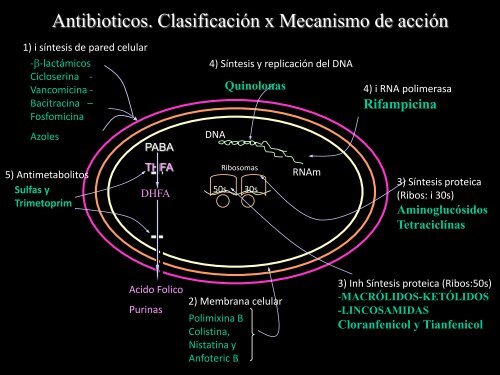
Antibioticos. Clasificación x Mecanismo de acción<br />
1) i síntesis de pared celular<br />
--lactámicos<br />
Cicloserina -<br />
Vancomicina -<br />
Bacitracina –<br />
Fosfomicina<br />
Azoles<br />
5) Antimetabolitos<br />
Sulfas y<br />
Trimetoprim<br />
PABA<br />
THFA<br />
DHFA<br />
Acido Folico<br />
Purinas<br />
4) Síntesis y replicación del DNA<br />
DNA<br />
Quinolonas<br />
Ribosomas<br />
50s 30s<br />
2) Membrana celular<br />
Polimixina B<br />
Colistina,<br />
Nistatina y<br />
Anfoteric B<br />
RNAm<br />
4) i RNA polimerasa<br />
Rifampicina<br />
3) Síntesis proteica<br />
(Ribos: i 30s)<br />
Aminoglucósidos<br />
Tetraciclínas<br />
3) Inh Síntesis proteica (Ribos:50s)<br />
-MACRÓLIDOS-KETÓLIDOS<br />
-LINCOSAMIDAS<br />
Cloranfenicol y Tianfenicol
ANTIBIOTICOS MACROLIDOS<br />
• Bacteriostaticos --- bactericidas.<br />
• Eritromicina 1952.<br />
• Alternativa en pctes alergicos a penicilina.<br />
• Usos: infecciones respiratorias, de piel y tejidos<br />
blandos. ITS (Chlamydia y chancroide), pero…no<br />
activ N. gonorrhoeae, H. influenza. Px en Ruptura<br />
prematura de membranas (250 mg c/6h x7d o<br />
hasta parto).<br />
• Pero…Absorcion G-I erratica, vida ½ corta,<br />
niveles sanguineos bajos e inestabilidad en medio<br />
acido=penicilinas.
2<br />
G<br />
E<br />
N<br />
E<br />
R<br />
A<br />
C<br />
I<br />
O<br />
N<br />
E<br />
S<br />
1º G.<br />
2º G.<br />
Eritromicina S. erytreus<br />
Oleandomicina S. antibioticus<br />
Carbamicina<br />
Espiramicina S. ambofaciens<br />
Josamicina<br />
Miocamicina<br />
Azitromicina<br />
Diritromicina<br />
Claritromicina<br />
Rokytamicina<br />
Roxitromicina<br />
Naturales<br />
BACTERIOSTÁTICOS<br />
↑ dosis + bacterias en<br />
crecimiento<br />
BACTERICIDAS<br />
Semisinteticos<br />
BACTERICIDAS<br />
Efecto postantibióico prolongado
MACROLIDOS<br />
KETOLIDO$<br />
Telitromicina (Ketex) y Cetromicina<br />
Derivados semisinteticos de eritromicina<br />
• Gran actividad contra Neumococo-R a penic<br />
y resto <strong>macrolidos</strong>.<br />
• EPA: 10 h contra Neumococo.<br />
• Usos: Neumococo de comunidad,<br />
amigdalitis, bronquitis y otitis media. 400<br />
mg, bid.
MACROLIDOS<br />
Espectro Actividad Anti-microbiana<br />
1ra Generacion =bacteriostaticos<br />
pero dosis …bactericidas. Activos xa Gram+.<br />
Sust naturalesActinomycetos.<br />
Pseudomonas y Enterobacterias son resistentes a Macrólidos de 1ra<br />
2da generacion =bactericidas.<br />
Activos Gram+ y algunos Gram- (Azitro y<br />
Claritro). Semisinteticas.<br />
Pseudomonas aun son resistentes a Macrólidos de 2da
Espectro de actividad<br />
Neumococo<br />
Estreptococo Cl. tetani. Cl. perfringes.<br />
Mycoplasma Listeria Estafilococo ?
H. influenzae<br />
2da generación (Elección)<br />
Coryn. difteriae<br />
Legionella<br />
Morax. catarralis<br />
Chlamydia Neisseria g. ?<br />
Mycoplasma<br />
pneumoniae<br />
Campylobacter<br />
diarrea<br />
En ñ con diarrea del viajero la Azitromicina es de eleccion
MACROLIDOS<br />
Tienen EPA (Claritro 3v > Eritro)
MEC ACCION: Unen reversible a sitio P de subunidad 50s ribosomal (33<br />
proteinas diferentes y 2 moleculas de ARN).<br />
• bloquea transpeptidacion y translocacion y detiene la elongacion de cadena<br />
peptidica.<br />
Antagonismo competitivo!!!
MACROLIDOS<br />
RESISTENCIA<br />
1. Mutacion cromosomica en R ribosomal,<br />
x plasmidos, cruzada. Gram+, Gram-,<br />
Legionella y otros.<br />
2. Impermeabilidad pared bacteriana<br />
(Enterobacteriaceas y S.<br />
epidermidis).<br />
3. Enzimas (esterasas y fosforilasas) q’<br />
hidrolisan a <strong>macrolidos</strong>.<br />
Enterobacteriaceas. Cruzada.<br />
(Ags: 3 enzimas q`acetilan, adenilan y<br />
fosforilan) (cloranfenicol: acetiltransferasa).
MACROLIDOS<br />
FARMACOCINETICA<br />
• Eritromicina-base se destruye en medio acido<br />
(Tab cubierta enterica, sales de Eritro: estolato, etilsuccinato, estearato).<br />
• 2da G.: +resistentes a medio acido. biodisp.<br />
• Absorcion retardada por alimentos.<br />
• Adm i.v. lactobionato (10 mcg/ml)
PLASMA<br />
Alfa-glicoproteina (40-90%)<br />
Lactobionato IV +++<br />
Macrólidos de 2º G ++<br />
Eritromicina +<br />
Distribuye en tejidos y fluidos Concentra Tejido pleural y<br />
sinovial<br />
Eritro desmetilada en higado<br />
(inactiva) orina 5% v.o. y<br />
15% de parenteral.<br />
Claritro (metab activo y vida<br />
½ 6h). Azitro 40h<br />
residuos<br />
plasma—union proteinas, (alfa-glicoproteina, 40-90%) tejidos y fluidos<br />
corporales +prostata, liquido sinovial y pleural, humores. Placenta<br />
10% y leche materna. SNC incipiente (No Ags, No Tetra, Si Clor).
Eritro—filtracion<br />
glomerular y reabsorbe<br />
parcialmente en zona<br />
tubular,<br />
Eliminación<br />
bilis 30% y enterohepatica.<br />
Claritromicina es=eritro<br />
Azitro 10% orina y resto x heces.
MACROLIDOS<br />
FARMACOPATOLOGIA<br />
• Seguros y eficaces y > 2da generacion.<br />
• +++G-intestinal: n-v, ardor epigastrico, diarrea,<br />
regurgitaciones acidas.<br />
• I.M. dolorosa. I.v. tromboflebitis.
Racciones alergicas (raras) exantema,<br />
fiebre, eosinofilia, urticaria.<br />
Superinfecciones por Cándida o Cl. difficile<br />
Cándida<br />
Cl. difficile
MACROLIDOS<br />
FARMACOPATOLOGIA<br />
• Eritro: colestasis intraH, inicia en 2-3 sem:<br />
dolores colicos, n-v, fiebre e ictericia, x<br />
hipersensibilidad.<br />
• En ñ no Htoxicidad pero, estenosis<br />
hipertrofica de piloro.<br />
• Eritro dosis i.v. = ototoxicidad (reversible)
Elección en:<br />
– Legionella pneumofilica<br />
– Campylobacter jejuni<br />
– Bordetella pertussis<br />
Usos Clínicos<br />
– Corynebacterium diphtheriae<br />
– Micoplasma pneumoniae<br />
– Chlamydia trachomatis<br />
Alternativas en alergia a<br />
penicilina: infecciones Estrepto y<br />
Estafilo.<br />
-Px fiebre reumatica<br />
-Tx de trepanomatosis.
Traveler's diarrhea: updates for pediatricians<br />
Pediatr Ann. 2008 Dec;37(12):814-20.<br />
Ang JY, Mathur A.<br />
Children who travel are at risk of developing the same illnesses that affect<br />
adult travelers. Treatment, etiology and actual risk of TD in children<br />
are not well defined. Prevention and self-treatment of TD should be<br />
discussed in great detail during pre-travel counseling. This includes<br />
information and instructions on various preventive measures as well as<br />
when to use medications and the potential adverse effects associated<br />
with these medications.<br />
A TD that is mild can be managed effectively by appropriate use of oral<br />
rehydration solutions. Families should be advised to carry ORS<br />
packets and start treatment in children as soon as the diarrhea begins.<br />
Self treatment with antibiotics such as azithromycin may be considered<br />
in children if diarrhea is moderate to severe.<br />
Caregivers should contact local health authorities if there is no<br />
improvement especially after self treatment with antibiotics.
Claritromicina en
MACROLIDOS<br />
PRECAUCIONES<br />
• No infecciones graves (Sepsis, osteomielitis).<br />
• Contraindicado estolato de Eritro en Enf H.<br />
• No asociar alcaloides cornezuelo de centeno<br />
ergotismo con necrosis de extremidades.
ORIGINAL ARTICLE<br />
Azithromycin and the Risk of Cardiovascular Death<br />
Wayne A. Ray, Ph.D., Katherine T. Murray, M.D., Kathi Hall, B.S., Patrick G. Arbogast,<br />
Ph.D., and C. Michael Stein, M.B., Ch.B.<br />
N Engl J Med 2012; 366:1881-1890May 17, 2012<br />
• DISCUSSION<br />
• We found that a 5-day course of azithromycin was associated with a<br />
small absolute increase in the risk of cardiovascular death, which was<br />
most pronounced for patients in the highest decile of the baseline risk<br />
of cardiovascular disease. There was no increased risk of death from<br />
noncardiovascular causes among patients who took azithromycin, but<br />
there was an increase in the risk of death from any cause. The risk of<br />
cardiovascular death was significantly greater with azithromycin than<br />
with either amoxicillin or ciprofloxacin but did not differ significantly<br />
from the risk with levofloxacin.
LINCOSAMIDAS<br />
Quimicamente diferentes a los <strong>macrolidos</strong> pero semejantes x: mec<br />
accion, espectro antibacteriano y farmacocinetica.
LINCOSAMIDAS<br />
ESPECTRO ANTIBACTERIANO<br />
• Sensibles, =Eritro: Gram+.<br />
• No sensibles, Gram- aerobios (C. difficile,<br />
Neisseria, Enterobacter y H. influenza).<br />
• Resistentes Enterococos.<br />
+++Anaerobios:<br />
Bacteroides, Fusobacterium, Actinomyces, C.<br />
perfringis, Peptoestreptococos y<br />
Campylobacter.
MEC ACCION<br />
Bacteriostaticas. Unen sitio A de 50s ribosomal=i sintesis<br />
proteica. = cloranf y <strong>macrolidos</strong>.<br />
Antagonismo competitivo!!!
Mecanismos de resistencia<br />
-x plasmidos = <strong>macrolidos</strong>, R cruzada.<br />
-5% Estafilococos y 0-10% de B. fragilis son R a clindamicina.
LINCOSAMIDAS<br />
FARMACOCINETICA<br />
CLINDA.<br />
• Oral 75% pasa a sangre y es independiente<br />
de alimentos. Palmitato (v.o, 1h 2.8mcg/ml)<br />
y fosfato (i.v. 5mcg/ml).<br />
LINCO, 75% en ayunas y 25% con alimentos.<br />
• Atraviesan la placenta<br />
• No llegan LCR
LINCOSAMIDAS<br />
FCOPATOLOGIA<br />
• Clinda y Linco, 10% diarrea y >colitis<br />
pseudomembranosa (diarrea mucosanguinolenta,<br />
dolor abdominal, n-v) C.<br />
difficile (toxina).<br />
• i.m.=dolor e i.v.=tromboflebitis.<br />
Rapida=colapso cardio-vascular (K).<br />
• Clinda, no Htoxica, pero transaminasas.
Farmacopatología<br />
Colitis pseudomembranosa Agrava miastenia gravis<br />
bloqueo neuromuscular de<br />
Aminoglucosidos e i placa<br />
neuromotriz (no juntas)
LINCOSAMIDAS<br />
FARMACOPATOLOGIA<br />
Reacciones alergicas (raras)<br />
erupciones cutaneas, fiebre, urticaria. Eritema<br />
multiforme, anafilaxia, Sd Stevens Johnson.
USOS CLINICOS<br />
• Tx germenes<br />
ANAEROBIOS.<br />
• +Ags en abscesos, e<br />
infecciones abdominales<br />
severas, peritonitis, EPI.<br />
• Alternativa (penicilina) en<br />
osteomielitis x Estaf aureus.<br />
• Gardnerella vaginalis<br />
(vaginosis bact)
LINCOSAMIDAS<br />
USOS CLINICOS<br />
• Px quirurgica abdominal<br />
• Px infecciones estreptococicas<br />
• clinda+pirimetamina=encefalitis<br />
x T.gondii (SIDA)<br />
• clinda+quinina = Malaria-R /
TELITROMICINA Y CETROMICINA<br />
Derivados<br />
sintéticos<br />
Neumococo resistente a<br />
Penicilina y Macrólidos
Usos Clínicos de Telitromicina y Cetromicina<br />
Amigdalitis<br />
Bronquitis<br />
Neumonía
• Nature Reviews Drug Discovery 9, 260 (April 2010) |<br />
• Trial watch: Phase III success for novel Clostridium difficile<br />
antibiotic<br />
• Abstract<br />
• The results of the second of two Phase III trials evaluating the<br />
macrocyclic antibiotic fidaxomicin (OPT-80, PAR-101), developed by<br />
Optimer Pharmaceuticals, confirm that it is as efficacious as<br />
vancomycin for treating patients with Clostridium difficile infection<br />
(CDI). It is also associated with a lower incidence of recurrence of<br />
CDI.
C difficile organism (National Institutes<br />
of Health)<br />
February 4, 2011 — Compared with vancomycin, fidaxomicin (Optimer Pharmaceuticals, Inc)<br />
produces noninferior rates of clinical cure in adults with Clostridium difficile infection. In addition, for<br />
some strains, fidaxomicin is associated with a significantly lower rate of recurrence, according to the<br />
findings of a randomized trial.<br />
Thomas J. Louie, MD, with the University of Calgary, in Calgary, Alberta, Canada, reported the study<br />
findings of the randomized phase 3 trial in the February 3 issue of theNew England Journal of<br />
Medicine.<br />
According to the researchers, fidaxomicin is a macrocyclic antibiotic that is more active in vitro<br />
than vancomycin in clinical isolates of C difficile, including the NAP1/BI/027 strain.<br />
"This activity, in combination with minimal systemic absorption, high fecal concentrations, and limited<br />
activity in vitro and in vivo against components of the normal gut flora, makes fidaxomicin a<br />
promising candidate that may provide highly active but more selective therapy for C.<br />
difficile infection," the study authors write.<br />
The current study included 629 adults with acute symptoms of C difficile infection, with a positive<br />
result on a stool toxin test. Patients were randomly assigned to receive fidaxomicin at a dose of 200<br />
mg twice daily or vancomycin at a dose of 125 mg 4 times daily. Both medicines were taken orally<br />
for 10 days.<br />
Of the patients, 548 (87.1%) could be evaluated for the per-protocol analysis. The rates of clinical<br />
cure with fidaxomicin were noninferior to those observed with vancomycin in both the modified<br />
intent-to-treat analysis (88.2% vs 85.8% with fidaxomicin vs vancomycin, respectively) and the perprotocol<br />
analysis (92.1% and 89.8%, respectively).
•