Hepatitis aguda de evolución fatal
Hepatitis aguda de evolución fatal
Hepatitis aguda de evolución fatal

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Clínicos leoneses<br />
PONFERRADA 2011<br />
Begoña Álvarez Cuenllas.<br />
R1 Aparato Digestivo.<br />
Complejo Asistencial Universitario <strong>de</strong> León.
Caso clínico II:<br />
E.A.:<br />
Ictericia progresiva <strong>de</strong> 7 días <strong>de</strong> <strong>evolución</strong>, con coluria y<br />
prurito. No dolor abdominal ni fiebre. No sd general.<br />
Niega ingesta <strong>de</strong> nuevos fármacos y productos <strong>de</strong><br />
herboristería. No ha realizado viajes recientes.<br />
Exploración:<br />
• COC, TA 160/80. Tª 36.5ºC. Ictericia mucocutánea<br />
marcada. Estigmas cutáneos <strong>de</strong> hepatopatía crónica. No<br />
signos <strong>de</strong> encefalopatía.<br />
• ACP sin hallazgos.<br />
• Abdomen: ligeramente globuloso, no doloroso, no masas<br />
ni megalias. No signos <strong>de</strong> irritación peritoneal. No ascitis.<br />
• No e<strong>de</strong>mas en MID (amputación MII).
Pruebas complementarias:<br />
Día ingreso<br />
Leucocitos 11300<br />
Hb 14.2<br />
Plaquetas 154.000<br />
Protrombina 48%<br />
Glucosa 248<br />
Creatinina 0.26<br />
GOT 3088<br />
GPT 1891<br />
F alcalina 480<br />
GGT 597<br />
Br total (BrD) 27 (18)<br />
COAGULOPATÍA<br />
CITOLISIS<br />
ICTERICIA
Pruebas complementarias (II):<br />
Eco<br />
abdominal<br />
RM<br />
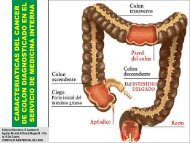
Hepatomegalia, contorno polilobulado sin LOES.<br />
Vesícula con cálculos y pared engrosada.<br />
Colédoco normal con vía intrahepática prominente.<br />
Porta <strong>de</strong> 12 mm y bazo <strong>de</strong> 13 cms.<br />
Líquido libre perihepático y en ambas gotieras paracólicas.<br />
Hepatomegalia sin LOES<br />
Eje esplenoportal permeable.<br />
Recanalización <strong>de</strong> vena umbilical, múltiples colaterales en<br />
todo el hemiabdomen superior.<br />
Vía biliar normal.<br />
Ascitis <strong>de</strong> escasa cuantía.<br />
q Se <strong>de</strong>scarta una ictericia obstructiva.<br />
q Se confirman signos <strong>de</strong> hepatopatía crónica.
Pruebas complementarias (III):<br />
Serologías<br />
Autoinmunidad<br />
Otras pruebas<br />
<strong>de</strong> laboratorio<br />
• VHA: IgM negativa. NEGATIVOS<br />
• VHB: HBs Ag (-) Anti HBs (-), antiHBc (-), DNA VHB (-).<br />
• VHC: negativo.<br />
• Anti VHS: IgG positivo, IgM negativo.<br />
• Anti VEB: IgM negativo.<br />
• Anti VHZ: IgM negativo.<br />
• Anti CMV: IgG e IgM negativos.<br />
• ANA, ANCAs, AMA, anti-LKM, anti LC-1, anti SLA:<br />
negativos.<br />
• Anti músculo liso: (+) 1/640.<br />
• α1-AT 250.<br />
• Ceruloplasmina: 78 mg/dl. Cu orina: 25.9 mcg/24 h.<br />
• Hipergammaglobulinemia policlonal.<br />
• Fe 73. Transferrina 211. Ferritina 760.<br />
• Sistemático y sedimento <strong>de</strong> orina: normal.<br />
• Rx tórax: sin alteraciones groseras.
Acute on Chronic Liver Failure:<br />
• Daño hepático agudo<br />
manifestado por ictericia<br />
y coagulopatía.<br />
• Complicado por ascitis<br />
o encefalopatía antes <strong>de</strong><br />
4 semanas.<br />
• En un paciente con<br />
hepatopatía crónica<br />
(conocida o no).<br />
ETIOLOGÍA:<br />
Agentes infecciosos:<br />
- P.B.E.<br />
- Virus hepatotropos y otros.<br />
- Reactivación <strong>de</strong> hepatitis B o C.<br />
- Otros agentes infecciosos no virales.<br />
Etiología no infecciosa:<br />
- Alcohol.<br />
- Fármacos, hierbas.<br />
- <strong>Hepatitis</strong> autoinmune o Enf. Wilson.<br />
- HDA por varices.<br />
- Cirugía.<br />
Desconocida. Sarin APASL, 2009
¿Qué actitud tomarías?<br />
¿Biopsia hepática?.<br />
¿Tratamiento empírico?.<br />
¿Con qué?.
DIAGNÓSTICO: Marcados signos <strong>de</strong> esteatohepatitis <strong>aguda</strong><br />
compatible con origen alcohólico y signos <strong>de</strong> proliferación<br />
ductular (asociado a obstrucción biliar, sepsis o fármacos).<br />
Biopsia hepática<br />
• Infiltrado lobulillar agudo a expensas <strong>de</strong> neutrófilos.<br />
• Presencia <strong>de</strong> hialina <strong>de</strong> Mallory.<br />
• Imágenes <strong>de</strong> esteatosis macro y microgranular.<br />
• Se observan algunos trombos biliares intracanaliculares.<br />
• Infiltrado inflamatorio agudo con neutrófilos y eosinófilos<br />
en los espacios porta con marcada proliferación ductular.<br />
• Presencia <strong>de</strong> <strong>de</strong>stacados signos <strong>de</strong> fibrosis pericelular y<br />
perivenular.
Evolución:<br />
Ingreso Día 2 Día 5 Día 7<br />
D í a<br />
12<br />
D í a<br />
16<br />
D í a<br />
22<br />
D í a<br />
25<br />
Día 27<br />
Leucos 11300 11100 12.600 11100 16500 21800 23300 21100 23600<br />
Hb 14.2 13.8 13.9 14.2 14.9 15 14.3 13.7 11.2<br />
Plaquetas 154000 169000 213000 192000 263000 232000 167000 127000 107000<br />
Protrombina 48% 55% 71% 73% 63% 68% 69% 50% 28%<br />
Glucosa 248 198 190 169 279 343 93 196 237<br />
Creatinina 0.26 0.28 0.86 1.1 1.39 1.43 2.32 5,1 8.65<br />
GOT 3088 889 113 73 53 34 43 33<br />
GPT 1891 1055 386 199 76 43 30 28<br />
F alcalina 480 486 472 462 426 432<br />
GGT 597 390 312 284 251 185 182<br />
Br T (BrD) 27 (18)<br />
Dia 1 Día 7 Día 14 Día 21 Día 28<br />
Child B8 C10 C10 C11 C13<br />
MELD 26 26 29 33 47<br />
Maddrey 74 77 77 94 163<br />
Lille 0.99 0.99 0.99 0.99 0.99<br />
3 1<br />
(20.6)<br />
3 9<br />
(34)<br />
I C T E R I C I A<br />
4 4<br />
(37)<br />
5 4<br />
(43)<br />
5 8<br />
(45)<br />
Encefalopatía<br />
hepática<br />
5 4<br />
(43)<br />
5 6<br />
(46)<br />
E<br />
X<br />
I<br />
T<br />
U<br />
S<br />
Sd. Hepato-Renal
HEPATITIS E:
DIAGNÓSTICO:<br />
PERÍODO DE INCUBACIÓN<br />
Fase prodrómica<br />
Pavio N. Current Opinion in Infectious Diseases 2010, 23: 521-27
Particularida<strong>de</strong>s:<br />
• En países occidnts la<br />
seroprevalencia es <strong>de</strong><br />
3-16%. En España<br />
(Cataluña) es <strong>de</strong>l 7.3%.<br />
Zoonosis a partir <strong>de</strong>l<br />
cerdo ¿?<br />
• Infecciones subclínicas.<br />
Fogeda M et al J Med Virol 2009; 81<br />
• Las embarazadas <strong>de</strong>sarrollan más<br />
frecuentemente fallo hepático<br />
fulminante.<br />
• La hepatitis E se asocia con:<br />
q Prematuriedad.<br />
q Bajo peso al nacer.<br />
q Mortalidad perinatal.<br />
Pal R. J. Gastroenterol. Hepatol. 2005; 20: 1094-101<br />
Kar P. Am. J. Gastroenterol 2008; 103: 2495-501<br />
q Receptores <strong>de</strong> Tx <strong>de</strong> órgano<br />
sólido:<br />
q VHE crónica.<br />
q Recuentos más bajos <strong>de</strong><br />
linfocitos.<br />
Legrand-Abravanel F et al. J. Infect Dis 2010; 202<br />
q VIH<br />
Dalton H.R. et al. N Engl J Med 2009; 361<br />
q LNH en tto con Rituximab<br />
Ollier L et al. Ann Intern Med 2009; 150<br />
q Enf hepática previa y<br />
malnutridos.<br />
Kumar N. et al J. Hepatol 2007; 46<br />
• Hasta un 21% <strong>de</strong> los casos<br />
diagnosticados <strong>de</strong> hepatitis<br />
medicamentosa eran <strong>de</strong>bidos<br />
a una infección <strong>aguda</strong> por el<br />
VHE.<br />
Dalton HR, et al Aliment Pharmacol Ther 2007<br />
Actualmente hay dos vacunas<br />
en estudios <strong>de</strong> fase III que<br />
han <strong>de</strong>mostrado utilidad<br />
frente al genotipo asiático,<br />
pero ninguna <strong>de</strong> ellas está<br />
comercializada.
Casos <strong>de</strong> <strong>Hepatitis</strong> <strong>aguda</strong> por VHE en León:<br />
El caso <strong>de</strong><br />
hoy<br />
Sexo Varón Varón Mujer Varón Mujer<br />
Edad 86 48 55 56 85<br />
Antec.<br />
Pers.<br />
GOT<br />
GPT<br />
S.I. Hepatopatía<br />
cr. (OH)<br />
733<br />
1948<br />
3088<br />
1971<br />
Hipotiroidismo<br />
artritis<br />
psoriásica<br />
2726<br />
2982<br />
S.I. HTA, DMII, DL.<br />
Histerectomía<br />
1058<br />
2397<br />
1104<br />
1258<br />
Bil T 14 58 32 4 11,5<br />
Evolución Favorable Éxitus Favorable Favorable Favorable
GRACIAS!!!