- Page 2 and 3:
Ingrid Kreissig (Ed.) Primary Retin
- Page 4 and 5:
Professor Dr. med. Ingrid Kreissig
- Page 6 and 7:
Contents 1 The History of Retinal D
- Page 8 and 9:
List of Contributors Gary W. Abrams
- Page 10 and 11:
List of Contributors XI Hermann D.
- Page 12 and 13:
2 Helmholz in 1850 made an accurate
- Page 14 and 15:
4 (vitreous, gelatin) into the ante
- Page 16 and 17:
6 with scleral resection that set t
- Page 18 and 19:
8 ditis [72-74].Temperatures up to
- Page 20 and 21:
10 1 The History of Retinal Detachm
- Page 22 and 23:
12 1 The History of Retinal Detachm
- Page 24 and 25:
14 1 The History of Retinal Detachm
- Page 26 and 27:
16 ion [147]. Perfluorocarbon liqui
- Page 28 and 29:
18 1 The History of Retinal Detachm
- Page 30 and 31:
20 1 The History of Retinal Detachm
- Page 32 and 33:
22 1 The History of Retinal Detachm
- Page 34 and 35:
24 1 The History of Retinal Detachm
- Page 36 and 37:
26 2 Prophylaxis in Fellow Eye of P
- Page 38 and 39:
28 2 Prophylaxis in Fellow Eye of P
- Page 40 and 41:
30 2 Prophylaxis in Fellow Eye of P
- Page 42 and 43:
32 found that eyes with pre-existin
- Page 44 and 45:
34 2 Prophylaxis in Fellow Eye of P
- Page 46 and 47:
36 3 Encircling Operation with Drai
- Page 48 and 49:
38 3 Encircling Operation with Drai
- Page 50 and 51:
40 3 Encircling Operation with Drai
- Page 52 and 53:
42 3 Encircling Operation with Drai
- Page 54 and 55:
44 3 Encircling Operation with Drai
- Page 56 and 57:
46 3 Encircling Operation with Drai
- Page 58 and 59:
48 3 Encircling Operation with Drai
- Page 60 and 61:
50 3 Encircling Operation with Drai
- Page 62 and 63:
52 3 Encircling Operation with Drai
- Page 64 and 65:
Chapter 4 Pneumatic Retinopexy for
- Page 66 and 67:
Technique 57 Case Selection Proper
- Page 68 and 69:
Technique 59 Table 4.1. Gas charact
- Page 70 and 71:
Technique 61 solution; however,thes
- Page 72 and 73:
Technique 63 gas reflux. Following
- Page 74 and 75:
Complications: Prevention and Manag
- Page 76 and 77:
New Possibilities 67 ing on type an
- Page 78 and 79:
Results 69 Table 4.7 (continued) Au
- Page 80 and 81:
Discussion 71 surgical failures. Fa
- Page 82 and 83:
Discussion 73 Disadvantages of PR A
- Page 84 and 85:
References 75 situations, then to p
- Page 86 and 87:
References 77 24. Tornambe PE, Hilt
- Page 88 and 89:
References 79 51. Pournaras CJ, Don
- Page 90 and 91:
Chapter 5 Vitrectomy for the Primar
- Page 92 and 93:
Indications 83 Table 5.1. Indicatio
- Page 94 and 95:
Indications 85 Fig. 5.2. The vitreo
- Page 96 and 97:
Surgical Technique 87 vitrectomy an
- Page 98 and 99:
Outcomes 89 will be visible under a
- Page 100 and 101:
Outcomes 91 almost no persistent su
- Page 102 and 103:
References 93 7. Heimann H, Bornfel
- Page 104 and 105:
96 6 Minimal Segmental Buckling Wit
- Page 106 and 107:
98 6 Minimal Segmental Buckling Wit
- Page 108 and 109:
100 the operating table with the re
- Page 110 and 111:
102 6 Minimal Segmental Buckling Wi
- Page 112 and 113:
104 6 Minimal Segmental Buckling Wi
- Page 114 and 115:
106 a b 6 Minimal Segmental Bucklin
- Page 116 and 117:
108 a b 6 Minimal Segmental Bucklin
- Page 118 and 119:
110 6 Minimal Segmental Buckling Wi
- Page 120 and 121:
112 6 Minimal Segmental Buckling Wi
- Page 122 and 123:
114 a 6 Minimal Segmental Buckling
- Page 124 and 125:
116 a b 6 Minimal Segmental Bucklin
- Page 126 and 127:
118 6 Minimal Segmental Buckling Wi
- Page 128 and 129:
120 6 Minimal Segmental Buckling Wi
- Page 130 and 131:
122 c d 6 Minimal Segmental Bucklin
- Page 132 and 133:
124 c Fig. 6.14c 6 Minimal Segmenta
- Page 134 and 135:
Table 6.1. Preoperative characteris
- Page 136 and 137:
Table 6.3. Final attachment after m
- Page 138 and 139:
130 Choroidals In 4 of the 1,462 de
- Page 140 and 141:
Table 6.4. Visual acuity at 2 years
- Page 142 and 143:
134 6 Minimal Segmental Buckling Wi
- Page 144 and 145:
136 6 Minimal Segmental Buckling Wi
- Page 146 and 147:
138 6 Minimal Segmental Buckling Wi
- Page 148 and 149: 140 Probably, the future question n
- Page 150 and 151: 142 6 Minimal Segmental Buckling Wi
- Page 152 and 153: 144 6 Minimal Segmental Buckling Wi
- Page 154 and 155: 146 7 Pharmacological Approaches to
- Page 156 and 157: 148 7 Pharmacological Approaches to
- Page 158 and 159: 150 7 Pharmacological Approaches to
- Page 160 and 161: 152 heparin was published in eyes u
- Page 162 and 163: 154 search for compounds with hepar
- Page 164 and 165: 156 7 Pharmacological Approaches to
- Page 166 and 167: 158 7 Pharmacological Approaches to
- Page 168 and 169: Chapter 8 Systematic Review of Effi
- Page 170 and 171: Materials and Methods 163 Table 8.2
- Page 172 and 173: Discussion 165 30% 25% 20% 15% 10%
- Page 174 and 175: Discussion 167 Fig. 8.2. The small
- Page 176 and 177: Conclusion 169 vitrectomy and searc
- Page 178 and 179: References 171 8. Brazitikos PD, D
- Page 180 and 181: References 173 34. Gunduz K, Gunalp
- Page 182 and 183: References 175 63. Schepens CL (195
- Page 184 and 185: 178 9 Repair of Primary Retinal Det
- Page 186 and 187: 180 a b Fig. 9.3a,b. Legend see pag
- Page 188 and 189: 182 9 Repair of Primary Retinal Det
- Page 190 and 191: 184 9 Repair of Primary Retinal Det
- Page 192 and 193: 186 a b 9 Repair of Primary Retinal
- Page 194 and 195: 188 might eliminate traction on the
- Page 196 and 197: 190 9 Repair of Primary Retinal Det
- Page 200 and 201: Retinal Detachment Repair: Outlook
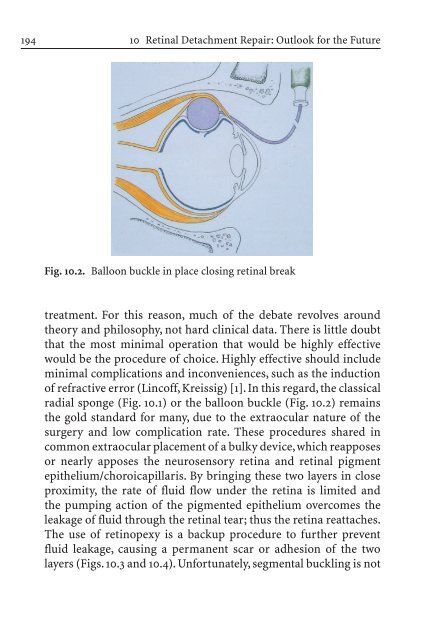
- Page 202 and 203: Retinal Detachment Repair: Outlook
- Page 204 and 205: Retinal Detachment Repair: Outlook
- Page 206 and 207: Retinal Detachment Repair: Outlook
- Page 208 and 209: Retinal Detachment Repair: Outlook
- Page 210 and 211: Retinal Detachment Repair: Outlook
- Page 212 and 213: References 207 It is impossible to
- Page 214 and 215: 210 C Campbell 7 case selection 57,
- Page 216 and 217: 212 M Machemer 13 macular - complic
- Page 218 and 219: 214 retinal - detachment - - bilate