Colloid Osmotic Pressure in Health and Disease* - VetLearn.com
Colloid Osmotic Pressure in Health and Disease* - VetLearn.com
Colloid Osmotic Pressure in Health and Disease* - VetLearn.com

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
CE<br />
896 V<br />
Vol. 23, No. 10 October 2001<br />
Article #4 (1.5 contact hours)<br />
Refereed Peer Review<br />
KEY FACTS<br />
■ COP is the ma<strong>in</strong> force reta<strong>in</strong><strong>in</strong>g<br />
fluid with<strong>in</strong> the vasculature <strong>and</strong><br />
can be altered <strong>in</strong> different<br />
disease states.<br />
■ Album<strong>in</strong> is the ma<strong>in</strong><br />
determ<strong>in</strong>ant of COP.<br />
■ Use of formulas to calculate<br />
COP us<strong>in</strong>g total prote<strong>in</strong> values<br />
is not as accurate as actual<br />
COP measurement, especially<br />
<strong>in</strong> critically ill animals.<br />
<strong>Colloid</strong> <strong>Osmotic</strong><br />
<strong>Pressure</strong> <strong>in</strong> <strong>Health</strong><br />
<strong>and</strong> <strong>Disease*</strong><br />
Tufts University<br />
Daniel L. Chan, DVM<br />
Elizabeth A. Rozanski, DVM<br />
Lisa M. Freeman, DVM, PhD<br />
John E. Rush, DVM, MS<br />
Email <strong>com</strong>ments/questions to<br />
<strong>com</strong>pendium@medimedia.<strong>com</strong><br />
or fax 800-556-3288<br />
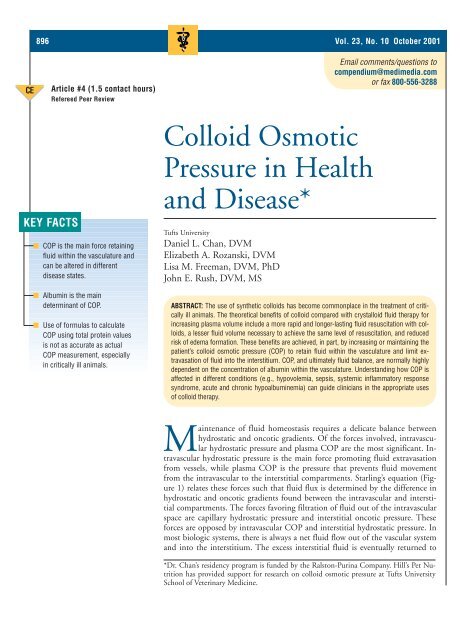
ABSTRACT: The use of synthetic colloids has be<strong>com</strong>e <strong>com</strong>monplace <strong>in</strong> the treatment of critically<br />
ill animals. The theoretical benefits of colloid <strong>com</strong>pared with crystalloid fluid therapy for<br />
<strong>in</strong>creas<strong>in</strong>g plasma volume <strong>in</strong>clude a more rapid <strong>and</strong> longer-last<strong>in</strong>g fluid resuscitation with colloids,<br />
a lesser fluid volume necessary to achieve the same level of resuscitation, <strong>and</strong> reduced<br />
risk of edema formation. These benefits are achieved, <strong>in</strong> part, by <strong>in</strong>creas<strong>in</strong>g or ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g the<br />
patient’s colloid osmotic pressure (COP) to reta<strong>in</strong> fluid with<strong>in</strong> the vasculature <strong>and</strong> limit extravasation<br />
of fluid <strong>in</strong>to the <strong>in</strong>terstitium. COP, <strong>and</strong> ultimately fluid balance, are normally highly<br />
dependent on the concentration of album<strong>in</strong> with<strong>in</strong> the vasculature. Underst<strong>and</strong><strong>in</strong>g how COP is<br />
affected <strong>in</strong> different conditions (e.g., hypovolemia, sepsis, systemic <strong>in</strong>flammatory response<br />
syndrome, acute <strong>and</strong> chronic hypoalbum<strong>in</strong>emia) can guide cl<strong>in</strong>icians <strong>in</strong> the appropriate uses<br />
of colloid therapy.<br />
Ma<strong>in</strong>tenance of fluid homeostasis requires a delicate balance between<br />
hydrostatic <strong>and</strong> oncotic gradients. Of the forces <strong>in</strong>volved, <strong>in</strong>travascular<br />
hydrostatic pressure <strong>and</strong> plasma COP are the most significant. Intravascular<br />
hydrostatic pressure is the ma<strong>in</strong> force promot<strong>in</strong>g fluid extravasation<br />
from vessels, while plasma COP is the pressure that prevents fluid movement<br />
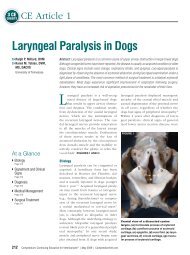
from the <strong>in</strong>travascular to the <strong>in</strong>terstitial <strong>com</strong>partments. Starl<strong>in</strong>g’s equation (Figure<br />
1) relates these forces such that fluid flux is determ<strong>in</strong>ed by the difference <strong>in</strong><br />
hydrostatic <strong>and</strong> oncotic gradients found between the <strong>in</strong>travascular <strong>and</strong> <strong>in</strong>terstitial<br />
<strong>com</strong>partments. The forces favor<strong>in</strong>g filtration of fluid out of the <strong>in</strong>travascular<br />
space are capillary hydrostatic pressure <strong>and</strong> <strong>in</strong>terstitial oncotic pressure. These<br />
forces are opposed by <strong>in</strong>travascular COP <strong>and</strong> <strong>in</strong>terstitial hydrostatic pressure. In<br />
most biologic systems, there is always a net fluid flow out of the vascular system<br />
<strong>and</strong> <strong>in</strong>to the <strong>in</strong>terstitium. The excess <strong>in</strong>terstitial fluid is eventually returned to<br />
*Dr. Chan’s residency program is funded by the Ralston-Pur<strong>in</strong>a Company. Hill’s Pet Nutrition<br />
has provided support for research on colloid osmotic pressure at Tufts University<br />
School of Veter<strong>in</strong>ary Medic<strong>in</strong>e.
Compendium October 2001 Small Animal/Exotics 897<br />
Figure 1—Starl<strong>in</strong>g’s Equation relates fluid flux (J v) as the difference<br />
between hydrostatic (P c – P i ) <strong>and</strong> oncotic (π c – π i ) gradients,<br />
where P c is the <strong>in</strong>travascular hydrostatic pressure, P i is the<br />
<strong>in</strong>terstitial hydrostatic pressure, π c is the <strong>in</strong>travascular oncotic<br />
pressure, <strong>and</strong> π i is the <strong>in</strong>terstitial oncotic pressure. K is the filtration<br />
coefficient represent<strong>in</strong>g the conductance or relative ease<br />
of fluids to cross the membrane, <strong>and</strong> σ is the reflection coefficient,<br />
which represents the permeability of the membrane or<br />
pore size. The arrows <strong>in</strong>dicate the direction of each force.<br />
the <strong>in</strong>travascular fluid spaces via the lymphatic system.<br />
Two additional factors responsible for modulat<strong>in</strong>g<br />
the impact of Starl<strong>in</strong>g’s forces on fluid flux are the reflection<br />
coefficient <strong>and</strong> the filtration coefficient:<br />
• The reflection coefficient (σ) represents the permeability<br />
of the membrane to macromolecules. Mechanisms<br />
affect<strong>in</strong>g macromolecular permeability <strong>in</strong>clude<br />
differences <strong>in</strong> size <strong>and</strong> charge of the molecules<br />
<strong>and</strong> route of transport. Macromolecules cross the<br />
microvascular membrane through large pores on the<br />
venous side of the capillary, <strong>and</strong> their transport is<br />
also <strong>in</strong>fluenced by the charge of endothelial cells <strong>and</strong><br />
the <strong>com</strong>position of glycocalyx close to the endothelial<br />
membrane.<br />
• The filtration coefficient (Κ) represents conductance<br />
or the ease with which water <strong>and</strong> small molecules<br />
cross the membrane. In contrast to macromolecules,<br />
water <strong>and</strong> small molecules filter through both the<br />
small <strong>and</strong> large pores along the entire length of the<br />
capillary membrane. 1<br />
The <strong>in</strong>terplay of Starl<strong>in</strong>g’s forces is dynamic <strong>and</strong><br />
varies considerably among organ systems. For example,<br />
the permeability of capillary membranes to album<strong>in</strong> is<br />
quite high <strong>in</strong> the lungs. As a result, an effective oncotic<br />
gradient cannot be ma<strong>in</strong>ta<strong>in</strong>ed <strong>and</strong> therefore COP is<br />
less important <strong>in</strong> controll<strong>in</strong>g fluid extravasation <strong>in</strong> this<br />
system. To <strong>com</strong>pensate, lymphatic dra<strong>in</strong>age is enhanced,<br />
prevent<strong>in</strong>g accumulation of filtered fluid. This<br />
π c<br />
π i<br />
J v = K [(P c – P i) – σ (π c – π i)]<br />
expla<strong>in</strong>s why pulmonary edema is more <strong>com</strong>mon <strong>in</strong> situations<br />
of high hydrostatic pressures, such as fluid overload<br />
<strong>and</strong> congestive heart failure (CHF), but relatively<br />
un<strong>com</strong>mon <strong>in</strong> hypoprote<strong>in</strong>emia. In contrast, the capillary<br />
permeability to album<strong>in</strong> is low <strong>in</strong> the subcutaneous<br />
<strong>in</strong>terstitium, which helps to account for the greater tendency<br />
to develop peripheral edema <strong>in</strong> hypo-oncotic<br />
states. This edema formation may be countered <strong>in</strong> cl<strong>in</strong>ical<br />
practice with support wraps, which <strong>in</strong>crease the <strong>in</strong>terstitial<br />
hydrostatic pressure.<br />
GENERATION AND MAINTENANCE<br />
OF COLLOID OSMOTIC PRESSURE<br />
Album<strong>in</strong> is the pr<strong>in</strong>cipal contributor to COP, account<strong>in</strong>g<br />
for approximately 80% of plasma COP. 2 Other<br />
prote<strong>in</strong>s (e.g., immunoglobul<strong>in</strong>s, fibr<strong>in</strong>ogen) also<br />
contribute to COP. These plasma prote<strong>in</strong>s are marg<strong>in</strong>ally<br />
permeable through the capillary membranes <strong>and</strong><br />
are therefore concentrated with<strong>in</strong> the vasculature. Because<br />
of the poor permeability of these osmotically active<br />
prote<strong>in</strong>s (i.e., album<strong>in</strong>, immunoglobul<strong>in</strong>s, fibr<strong>in</strong>ogen),<br />
a concentration gradient is created across the<br />
membrane, generat<strong>in</strong>g most of the COP.<br />
Another property that is a significant contributor to<br />
COP is the Gibbs-Donnan effect. Most prote<strong>in</strong>s, <strong>in</strong>clud<strong>in</strong>g<br />
album<strong>in</strong>, are negatively charged molecules surrounded<br />
by noncovalently bound cations such as sodium.<br />
These sodium ions act <strong>in</strong>dependently from their<br />
own concentration gradients <strong>and</strong> further <strong>in</strong>crease the<br />
water-reta<strong>in</strong><strong>in</strong>g effect of COP with<strong>in</strong> the vasculature.<br />
This effect is additive <strong>and</strong> <strong>in</strong>creases disproportionately<br />
with <strong>in</strong>creas<strong>in</strong>g album<strong>in</strong> concentration. Acidemia,<br />
which is <strong>com</strong>mon <strong>in</strong> critically ill patients, decreases the<br />
relative negative charge of album<strong>in</strong>, limit<strong>in</strong>g the Gibbs-<br />
Donnan effect <strong>and</strong> reduc<strong>in</strong>g the effective COP.<br />
Generation <strong>and</strong> ma<strong>in</strong>tenance of the COP (<strong>and</strong> album<strong>in</strong><br />
<strong>in</strong> particular) are important <strong>in</strong> healthy animals.<br />
The relationship between album<strong>in</strong> synthesis <strong>and</strong> COP<br />
is <strong>in</strong><strong>com</strong>pletely understood. Album<strong>in</strong> synthesis takes<br />
place exclusively <strong>in</strong> hepatocytes. In situations of adequate<br />
nutritional status <strong>and</strong> ample supply of am<strong>in</strong>o<br />
acids, album<strong>in</strong> synthesis is thought to be regulated by<br />
hepatic plasma COP. 3 However, other factors <strong>in</strong>dependent<br />
of COP may also be <strong>in</strong>volved <strong>in</strong> album<strong>in</strong> synthesis.<br />
4 For example, album<strong>in</strong> is known as a negative<br />
acute-phase reactant, which means that its synthesis is<br />
suppressed <strong>in</strong> response to <strong>in</strong>flammation. Controversy<br />
exists as to whether the adm<strong>in</strong>istration of natural or artificial<br />
colloids could, <strong>in</strong> fact, suppress album<strong>in</strong> synthesis.<br />
3–5 A recent <strong>in</strong> vitro study demonstrated significant<br />
decreases <strong>in</strong> album<strong>in</strong> synthesis by isolated hepatocytes<br />
when the cultures were <strong>in</strong>cubated with solutions of album<strong>in</strong><br />
<strong>and</strong> hetastarch. 5
898 Small Animal/Exotics Compendium October 2001<br />
A low plasma COP has been associated with <strong>in</strong>creased<br />
mortality <strong>in</strong> critically ill humans. 6 Critically ill<br />
veter<strong>in</strong>ary patients have also been recognized as hav<strong>in</strong>g<br />
abnormally low COP, but actual correlation to out<strong>com</strong>e<br />
has not been established. 7 Perhaps more important<br />
than the actual plasma COP is the ratio between<br />
plasma <strong>and</strong> <strong>in</strong>terstitial COP. Conditions result<strong>in</strong>g <strong>in</strong><br />
acute hypoalbum<strong>in</strong>emia dramatically decrease <strong>in</strong>travascular<br />
COP relative to <strong>in</strong>terstitial COP <strong>and</strong> can result <strong>in</strong><br />
hypovolemia, decreased tissue oxygenation, <strong>and</strong> systemic<br />
edema formation. 2,8 For example, <strong>in</strong> a case <strong>in</strong><br />
which there is significant acute blood loss followed by<br />
massive crystalloid <strong>in</strong>fusion, the decrease <strong>in</strong> <strong>in</strong>travascular<br />
COP promotes edema formation. Although peripheral<br />
edema may not have serious consequences <strong>in</strong> most<br />
patients, <strong>in</strong>test<strong>in</strong>al edema could be life-threaten<strong>in</strong>g <strong>in</strong><br />
cases of <strong>in</strong>test<strong>in</strong>al surgery due to an <strong>in</strong>creased risk for<br />
anastomotic dehiscence. 9 In cases of chronic hypoalbum<strong>in</strong>emia,<br />
as seen with prote<strong>in</strong>-los<strong>in</strong>g enteropathy <strong>and</strong><br />
prote<strong>in</strong>-los<strong>in</strong>g nephropathy, COP is decreased <strong>in</strong> both<br />
the <strong>in</strong>terstitium <strong>and</strong> the <strong>in</strong>travascular space, <strong>and</strong> therefore<br />
the ratio between these two <strong>com</strong>partments is preserved<br />
<strong>and</strong> fluid balance is ma<strong>in</strong>ta<strong>in</strong>ed. These patients<br />
would have a low COP but no signs of edema unless<br />
crystalloids were adm<strong>in</strong>istered. In the absence of peripheral<br />
edema, colloid therapy would offer little benefit<br />
<strong>in</strong> these chronic cases.<br />
OTHER MEASURES OF FLUID BALANCE<br />
As discussed, COP counterbalances hydrostatic pressure.<br />
Hydrostatic pressure is dependent on arterial<br />
blood pressure, precapillary <strong>and</strong> postcapillary resistance,<br />
<strong>and</strong> venous pressure. 10 Cl<strong>in</strong>ically, it is difficult to<br />
measure hydrostatic pressure, although pulmonary capillary<br />
wedge pressure (PCWP; measured via a Swan-<br />
Ganz catheter) <strong>and</strong> central venous pressure (CVP)<br />
might be useful as cl<strong>in</strong>ical correlates of hydrostatic pressure.<br />
A PCWP–COP gradient has also been shown to<br />
accurately predict the presence of pulmonary edema <strong>in</strong><br />
critically ill humans, 11 although no such relationships<br />
have been demonstrated <strong>in</strong> veter<strong>in</strong>ary medic<strong>in</strong>e <strong>and</strong><br />
PCWP is not rout<strong>in</strong>ely measured. In addition to hydrostatic<br />
<strong>and</strong> oncotic forces, <strong>in</strong>creased vascular permeability<br />
has a major impact on fluid balance.<br />
MEASUREMENT OF<br />
COLLOID OSMOTIC PRESSURE<br />
<strong>Colloid</strong> osmotic pressure may be predicted or directly<br />
measured. Because the concentration of plasma prote<strong>in</strong>s<br />
<strong>in</strong> part determ<strong>in</strong>es COP, predictive equations of<br />
COP based on total prote<strong>in</strong> concentrations have been<br />
proposed. 12 Although these equations provide values<br />
that correlate well with COP <strong>in</strong> healthy humans, they<br />
are unreliable <strong>in</strong> critically ill patients. 13,14 This is due <strong>in</strong><br />
part to changes <strong>in</strong> blood pH, particularly acidemia,<br />
which <strong>in</strong>fluence the Gibbs-Donnan effect. Attempts to<br />
apply these equations to dogs <strong>and</strong> cats have not produced<br />
reliable results. 15 Although new formulas have<br />
improved the ability to use total prote<strong>in</strong> to predict<br />
COP, direct measurements rema<strong>in</strong> the method of<br />
choice for determ<strong>in</strong><strong>in</strong>g COP <strong>in</strong> cl<strong>in</strong>ical patients. 14–16 A<br />
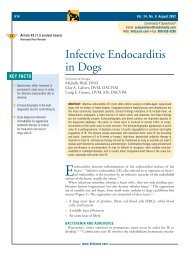
<strong>com</strong>mercial colloid osmometer can be used to directly<br />
measure COP <strong>in</strong> the cl<strong>in</strong>ical sett<strong>in</strong>g, provid<strong>in</strong>g rapid<br />
<strong>and</strong> reliable results (e.g., Wescor ® 4420, Logan, UT;<br />
Figure 2).<br />
Some authors have cautioned that certa<strong>in</strong> conditions<br />
can alter the read<strong>in</strong>g of the COP by a colloid osmometer.<br />
Such artifacts as severely hemolyzed samples can reportedly<br />
falsely elevate COP read<strong>in</strong>gs through the addition<br />
of free hemoglob<strong>in</strong>, while the use of liquid<br />
anticoagulants <strong>in</strong> sample collection can cause a dilutional<br />
effect <strong>and</strong> falsely lower the COP measurement. 17<br />
Normally, immunoglobul<strong>in</strong>s are only m<strong>in</strong>or contributors<br />
to COP. In cases of severe hypergammaglobul<strong>in</strong>emia<br />
(e.g., multiple myeloma, fel<strong>in</strong>e <strong>in</strong>fectious peritonitis),<br />
however, COP can be dramatically elevated. 15 The<br />
consequences of an abnormally elevated COP are unclear,<br />
although high COP could <strong>in</strong>hibit album<strong>in</strong> synthesis<br />
<strong>and</strong> result <strong>in</strong> hypoalbum<strong>in</strong>emia. 4,5 Pathologic<br />
changes associated with hypergammaglobul<strong>in</strong>emia are<br />
usually attributed to <strong>in</strong>creases <strong>in</strong> blood viscosity <strong>and</strong><br />
the deposition of immunoglobul<strong>in</strong> <strong>com</strong>plexes but apparently<br />
not to the altered COP.<br />
Figure 2—Schematic representation of a colloid osmometer.<br />
A sample (serum, plasma, or hepar<strong>in</strong>ized whole blood) from<br />
a patient is <strong>in</strong>jected <strong>in</strong>to Chamber A <strong>and</strong> allowed to equilibrate<br />
with the reference Chamber B (conta<strong>in</strong><strong>in</strong>g 0.9%<br />
sal<strong>in</strong>e). Chambers A <strong>and</strong> B are separated by a selectively permeable<br />
synthetic membrane. The COP of the sample causes<br />
water <strong>and</strong> small solute molecules to move from Chamber B<br />
to Chamber A with a fall <strong>in</strong> pressure <strong>in</strong> the lower chamber.<br />
This negative pressure is measured by the transducer <strong>and</strong><br />
equals the COP of the sample <strong>in</strong> Chamber A.
Compendium October 2001 Small Animal/Exotics 899<br />
Several studies have established normal values of<br />
COP <strong>in</strong> veter<strong>in</strong>ary patients us<strong>in</strong>g colloid osmometry.<br />
Normal can<strong>in</strong>e plasma COP values range from 14 to<br />
27 mm Hg, whereas normal fel<strong>in</strong>e plasma COP values<br />
can range from 21 to 34 mm Hg. 2,15,16 The reported<br />
mean COP <strong>in</strong> whole blood was 19.9 ± 2.1 mm Hg <strong>in</strong><br />
dogs <strong>and</strong> 24.7 ± 3.7 mm Hg <strong>in</strong> cats. 18 However, just as<br />
with any laboratory test, a reference range should be established<br />
for the particular colloid osmometer <strong>and</strong> protocol<br />
used.<br />
FLUID BALANCE IN DISEASES<br />
The normal dynamics of various fluid <strong>com</strong>partments<br />
are altered dur<strong>in</strong>g different disease states. Changes may<br />
<strong>in</strong>clude the follow<strong>in</strong>g:<br />
• Increased vascular permeability<br />
• Acute or chronic decreases <strong>in</strong> album<strong>in</strong> (<strong>and</strong> COP)<br />
• Increased <strong>in</strong>travascular hydrostatic pressure<br />
Increased vascular permeability is one of the more challeng<strong>in</strong>g<br />
conditions encountered <strong>in</strong> critically ill patients<br />
<strong>and</strong> one <strong>in</strong> which the use of synthetic colloids is perhaps<br />
most controversial. Diseases associated with <strong>in</strong>creased<br />
vascular permeability <strong>in</strong>clude the systemic <strong>in</strong>flammatory<br />
response syndrome (SIRS), acute<br />
respiratory distress syndrome (ARDS), pneumonia,<br />
sepsis, vasculitis, reperfusion <strong>in</strong>jury, pancreatitis, <strong>and</strong><br />
anaphylaxis. 10,17,19,20 Additionally, envenomation (e.g.,<br />
bees, wasps, rattlesnakes), trauma, burns, smoke <strong>in</strong>halation,<br />
<strong>and</strong> multiple blood transfusions are also associated<br />
with <strong>in</strong>creased vascular permeability. 19 Inflammatory<br />
cytok<strong>in</strong>es can <strong>in</strong>duce changes <strong>in</strong> endothelial cells that<br />
<strong>in</strong>crease microvascular permeability <strong>and</strong> lead to capillary<br />
leakage. 21 For example, dur<strong>in</strong>g reperfusion of hypoxic<br />
tissue, the endothelial junctions <strong>in</strong> capillary<br />
membranes separate, <strong>in</strong>creas<strong>in</strong>g the number <strong>and</strong> size of<br />
the pores <strong>in</strong> the capillary membranes. 22 In sepsis, it is<br />
thought that endothelial damage occurs as a result, <strong>in</strong><br />
part, of the action of activated, degranulat<strong>in</strong>g neutrophils.<br />
23 Subsequently, the <strong>in</strong>creased capillary permeability<br />
is responsible for album<strong>in</strong> leakage <strong>and</strong> a decrease<br />
<strong>in</strong> plasma COP. With a decrease <strong>in</strong> plasma COP, fluid<br />
filtration from the <strong>in</strong>travascular <strong>com</strong>partment is enhanced<br />
<strong>and</strong> leads to edema formation <strong>and</strong> fluid loss<br />
<strong>in</strong>to third spaces. The subsequent loss of plasma volume<br />
contributes to the cardiovascular dysfunction <strong>and</strong><br />
tissue hypoperfusion <strong>in</strong> sepsis.<br />
In patients with ARDS, <strong>in</strong>flammatory cytok<strong>in</strong>es are<br />
released <strong>in</strong> response to septic <strong>and</strong> <strong>in</strong>flammatory stimuli<br />
<strong>and</strong> cause deranged capillary permeability. These<br />
patients usually receive aggressive fluid therapy, result-<br />
<strong>in</strong>g <strong>in</strong> elevated pulmonary hydrostatic pressure. The<br />
<strong>com</strong>b<strong>in</strong>ation of these effects favors filtration of fluid<br />
<strong>in</strong>to the pulmonary <strong>in</strong>terstitium <strong>and</strong> may impair pulmonary<br />
gas exchange. 19 With the <strong>in</strong>creased permeability,<br />
the oncotic gradient between the pulmonary vasculature<br />
<strong>and</strong> <strong>in</strong>terstitium is dim<strong>in</strong>ished, caus<strong>in</strong>g COP<br />
to be<strong>com</strong>e less significant <strong>in</strong> affect<strong>in</strong>g fluid flux. This<br />
<strong>in</strong>crease <strong>in</strong> permeability also presents a problem for<br />
patients receiv<strong>in</strong>g synthetic colloids. Although there<br />
are some data to suggest that medium-sized macromolecules<br />
could attenuate some of the <strong>in</strong>creased permeability,<br />
most artificial colloids are heterogeneous<br />
solutions conta<strong>in</strong><strong>in</strong>g various-sized macromolecules.<br />
For example, hetastarch conta<strong>in</strong>s molecules rang<strong>in</strong>g<br />
from 20 to 2500 kD (6% hetastarch <strong>in</strong> 0.9% sodium<br />
chloride, Abbott Laboratories, North Chicago, IL).<br />
The smaller particles may easily pass through capillary<br />
membranes <strong>and</strong> extravasate <strong>in</strong>to the pulmonary <strong>in</strong>terstitium.<br />
This could potentially lead to worsen<strong>in</strong>g of<br />
pulmonary edema. 24<br />
When hypoalbum<strong>in</strong>emia results from nephrotic syndrome,<br />
the exact mechanism of fluid retention <strong>and</strong> edema<br />
formation rema<strong>in</strong>s controversial. A pervasive theory<br />
states that renal sodium <strong>and</strong> water retention occur as a<br />
response to low <strong>in</strong>travascular volume caused by the<br />
transudation of fluid from the plasma to the <strong>in</strong>terstitial<br />
<strong>com</strong>partment due to a low plasma COP. 25 However,<br />
some studies have cast doubt on this theory, <strong>and</strong> edema<br />
formation <strong>in</strong> nephrotic patients is now thought to occur<br />
as a result of primary renal mechanisms of sodium<br />
<strong>and</strong> water retention, <strong>in</strong>dependent of COP. 26 Therefore,<br />
the use of colloids to raise the COP <strong>in</strong> this patient population<br />
may not be warranted. Similarly, <strong>in</strong>creases <strong>in</strong><br />
pulmonary hydrostatic pressure are often seen <strong>in</strong> CHF.<br />
<strong>Colloid</strong> fluid therapy is usually avoided <strong>in</strong> animals with<br />
CHF due to concerns about <strong>in</strong>travascular volume overload<br />
<strong>and</strong> subsequent worsen<strong>in</strong>g of pulmonary edema or<br />
pleural effusion.<br />
COLLOID FLUID THERAPY<br />
Treatment of critically ill animals typically entails correction<br />
of dehydration <strong>and</strong> hypoperfusion via the adm<strong>in</strong>istration<br />
of <strong>in</strong>travenous fluids to <strong>com</strong>pensate for fluid<br />
losses <strong>and</strong> to ma<strong>in</strong>ta<strong>in</strong> cardiovascular homeostasis.<br />
Intravenous fluids are categorized as either a crystalloid<br />
solution or a colloid solution based on their <strong>com</strong>position.<br />
A crystalloid is an aqueous solution with small particles<br />
that are normally osmotically active <strong>in</strong> body fluids<br />
<strong>and</strong> that can easily pass through the capillary membrane.<br />
Examples <strong>in</strong>clude 0.9% sal<strong>in</strong>e, lactated R<strong>in</strong>ger’s<br />
solution, <strong>and</strong> hypertonic sal<strong>in</strong>e. A colloid is an aqueous<br />
solution conta<strong>in</strong><strong>in</strong>g both small <strong>and</strong> large particles (larger<br />
than 30 kD), with the larger molecules be<strong>in</strong>g too large
900 Small Animal/Exotics Compendium October 2001<br />
to filter through capillary membranes. <strong>Colloid</strong>s can be<br />
either natural (e.g., whole blood, plasma, album<strong>in</strong> solutions)<br />
or synthetic (e.g., dextrans, hydroxyethyl starches,<br />
hemoglob<strong>in</strong>-glutamers [Oxyglob<strong>in</strong> ® , Biopure Corporation,<br />
Cambridge, MA]). <strong>Colloid</strong> therapy <strong>and</strong> products<br />
have been recently reviewed. 27 Parenteral nutrition <strong>com</strong>ponents<br />
such as am<strong>in</strong>o acid solutions, lipid emulsions,<br />
<strong>and</strong> dextrose solutions behave similarly to crystalloids<br />
<strong>and</strong> have COP measurements less than 1 mm Hg. 28<br />
<strong>Colloid</strong> therapy is employed based on the pr<strong>in</strong>ciple<br />
that the patient’s COP can be <strong>in</strong>fluenced by the adm<strong>in</strong>istration<br />
of either natural or synthetic colloids. Properties<br />
of the different colloids may help predict their <strong>in</strong><br />
vivo effects. For example, the <strong>in</strong>herent COP of synthetic<br />
colloids ranges from 29 to 65 mm Hg, <strong>and</strong> therefore the<br />
degree of COP change will depend on the type <strong>and</strong> volume<br />
of colloid used. 18,28–30 Other factors, such as the<br />
half-life of each particular colloid <strong>and</strong> the duration of<br />
effect, are thought to also <strong>in</strong>fluence the effect on COP.<br />
The expected <strong>in</strong>crease <strong>in</strong> COP associated with particular<br />
dosages <strong>and</strong> types of colloids has not been established.<br />
While there are many benefits to colloid therapy<br />
(e.g., more rapid <strong>and</strong> longer-last<strong>in</strong>g resuscitation), there<br />
are potential side effects associated with synthetic colloid<br />
adm<strong>in</strong>istration. 20 These rare side effects can be<br />
dose-dependent, such as fluid overload <strong>and</strong> changes <strong>in</strong><br />
coagulation parameters, or the more unpredictable anaphylactic/anaphylactoid<br />
reactions <strong>and</strong> acute renal failure.<br />
2,16,18 To m<strong>in</strong>imize the occurrence of some of these<br />
effects, general re<strong>com</strong>mendations have been made, <strong>in</strong>clud<strong>in</strong>g<br />
dose re<strong>com</strong>mendations for various colloids<br />
(e.g., 20 ml/kg/day for hetastarch) <strong>and</strong> monitor<strong>in</strong>g<br />
COP dur<strong>in</strong>g colloid therapy. Some authors have advocated<br />
us<strong>in</strong>g the COP to guide colloid adm<strong>in</strong>istration<br />
(e.g., adm<strong>in</strong>ister<strong>in</strong>g colloids until the patient’s COP is<br />
at least 15 mm Hg). 31 However, this therapeutic goal<br />
may not be optimal <strong>in</strong> all situations. In our experience,<br />
st<strong>and</strong>ard colloid therapy (20 to 40 ml/kg/day of hetastarch)<br />
results <strong>in</strong> only modest changes <strong>in</strong> COP of 4 to<br />
5 mm Hg posttreatment <strong>in</strong> most animals. Adm<strong>in</strong>istration<br />
of synthetic colloids does not appear to <strong>in</strong>crease<br />
COP <strong>in</strong> a predictable manner, although a general dosedependent<br />
effect is seen. The benefit of COP monitor<strong>in</strong>g<br />
dur<strong>in</strong>g colloid therapy may be clearer when observ<strong>in</strong>g<br />
trends rather than attempt<strong>in</strong>g to achieve a certa<strong>in</strong><br />
COP level. As with any laboratory test, the actual value<br />
is mean<strong>in</strong>gless when taken out of context with respect<br />
to the cl<strong>in</strong>ical assessment of the patient.<br />
Increased transcapillary leakage of fluid <strong>and</strong> prote<strong>in</strong>s<br />
is often seen <strong>in</strong> critically ill patients. 1 Cont<strong>in</strong>ued use of<br />
crystalloids for fluid therapy <strong>in</strong> these patients could result<br />
<strong>in</strong> significant fluid losses from the <strong>in</strong>travascular<br />
space. Reduc<strong>in</strong>g vascular permeability may be of value<br />
to counteract the resultant tissue edema <strong>and</strong> hypovolemia.<br />
In some studies, the use of dextrans <strong>and</strong> hetastarch<br />
was shown to attenuate macromolecular leakage<br />
by presumably occlud<strong>in</strong>g some of the endothelial<br />
“gaps” associated with some conditions (e.g., ischemia,<br />
sepsis). 23,32,33 However, there are concerns over the use<br />
of heterogeneous colloid solutions <strong>in</strong> states of <strong>in</strong>creased<br />
permeability because the smaller colloid particles will<br />
extravasate <strong>in</strong>to the <strong>in</strong>terstitium <strong>and</strong> potentially promote<br />
edema. 34 Furthermore, the clearance of these<br />
small, osmotically active particles from the pulmonary<br />
<strong>in</strong>terstitium is particularly slow, <strong>and</strong> so colloids should<br />
be used with judicious care <strong>in</strong> cases of <strong>in</strong>creased pulmonary<br />
vascular permeability. 35<br />
COLLOID OSMOTIC PRESSURE<br />
MEASUREMENTS IN CLINICAL CASES<br />
The three cases <strong>in</strong> Box 1 illustrate how measurement<br />
of COP could impact cl<strong>in</strong>ical decisions <strong>in</strong> both the diagnosis<br />
<strong>and</strong> treatment of veter<strong>in</strong>ary patients. In Case 1,<br />
the acute decrease <strong>in</strong> COP associated with blood loss,<br />
coupled with <strong>in</strong>creased hydrostatic pressure from aggressive<br />
fluid adm<strong>in</strong>istration <strong>and</strong> possible <strong>in</strong>creased vascular<br />
permeability from massive blood transfusions,<br />
favored edema formation. Restoration of the <strong>in</strong>travascular/<strong>in</strong>terstitial<br />
COP gradient with synthetic colloids<br />
may have facilitated edema clearance.<br />
In Case 2, a similarly low COP was measured, yet no<br />
edema was noted. This was due to the chronicity of<br />
prote<strong>in</strong> loss that allowed equilibration of prote<strong>in</strong> distribution<br />
between the <strong>in</strong>travascular <strong>and</strong> <strong>in</strong>terstitial <strong>com</strong>partments,<br />
thus preserv<strong>in</strong>g the normal gradient. This illustrates<br />
that edema cannot be predicted solely by the<br />
COP.<br />
In Case 3, the presence of generalized edema with a<br />
normal COP supports either an <strong>in</strong>crease <strong>in</strong> vascular<br />
permeability or the <strong>in</strong>ability to clear <strong>in</strong>terstitial fluid, as<br />
may be seen with lymphatic obstruction associated with<br />
neoplasia as the cause for edema. Lymphatic obstruction<br />
was unlikely <strong>in</strong> this case because of the distribution<br />
of edema, leav<strong>in</strong>g vasculitis as the ma<strong>in</strong> diagnostic<br />
differential. The normal COP also helped determ<strong>in</strong>e<br />
that colloid therapy was not <strong>in</strong>dicated <strong>in</strong> this case.<br />
Knowledge of the COP can help <strong>in</strong> classify<strong>in</strong>g <strong>and</strong> diagnos<strong>in</strong>g<br />
diseases associated with edema as well as determ<strong>in</strong><strong>in</strong>g<br />
the appropriate situations <strong>in</strong> which synthetic<br />
colloids might be used. <strong>Colloid</strong> osmotic pressure is an<br />
important concept <strong>in</strong> underst<strong>and</strong><strong>in</strong>g the pathophysiology<br />
of edema, fluid resuscitation, <strong>and</strong> colloid therapy.<br />
FUTURE RESEARCH<br />
As the <strong>in</strong>tricacies of COP <strong>in</strong> both health <strong>and</strong> disease<br />
are further elucidated, an <strong>in</strong>dividual patient’s COP
902 Small Animal/Exotics Compendium October 2001<br />
Box 1. Cl<strong>in</strong>ical Cases<br />
Case 1<br />
A 10-year-old, <strong>in</strong>tact male, 26-kg weimaraner was presented<br />
for acute weakness <strong>and</strong> hematemesis. Initial packed cell volume<br />
(PCV) was 32%, serum total solids (TS) were 4.2 g/dl, <strong>and</strong><br />
<strong>in</strong>itial COP was 16.4 mm Hg (reference range, 17 to 23 mm<br />
Hg). The dog was tachycardic <strong>and</strong> weak <strong>and</strong> had pale mucous<br />
membranes <strong>and</strong> poor pulse quality. Hypovolemic shock was<br />
aggressively treated over 3 hours with 5 L (200 ml/kg) of lactated<br />
R<strong>in</strong>ger’s solution, but severe hematemesis cont<strong>in</strong>ued <strong>and</strong> PCV,<br />
TS, <strong>and</strong> COP cont<strong>in</strong>ued to drop precipitously (PCV, 13%; TS,<br />
2.1 g/dl; COP, 10.3 mm Hg) with no improvement <strong>in</strong><br />
hemodynamic signs. Dur<strong>in</strong>g resuscitation, multiple blood<br />
transfusions (7 units of packed erythrocytes) were adm<strong>in</strong>istered.<br />
The dog became extremely edematous, especially on its limbs<br />
<strong>and</strong> face. At surgery, a large gastric ulcer was identified <strong>and</strong><br />
attributed to NSAID therapy for arthritis. The peripheral edema<br />
began to resolve only after several days of supportive care,<br />
<strong>in</strong>clud<strong>in</strong>g colloid therapy with hetastarch <strong>and</strong> fresh-frozen<br />
plasma. Follow<strong>in</strong>g colloid therapy, COP had <strong>in</strong>creased to 14.6<br />
mm Hg, while TS were 4.3 g/dl.<br />
could potentially be used as a prognostic <strong>in</strong>dicator. Although<br />
some studies have related low COP to an <strong>in</strong>creased<br />
risk of develop<strong>in</strong>g pulmonary edema <strong>in</strong> humans,<br />
no such studies have been conducted <strong>in</strong> veter<strong>in</strong>ary medic<strong>in</strong>e.<br />
6 Measurement of COP can also be used as a guide<br />
for colloid therapy. However, an optimal level of COP<br />
achieved with colloid therapy <strong>in</strong> various cl<strong>in</strong>ical sett<strong>in</strong>gs<br />
has yet to be determ<strong>in</strong>ed. Because COP is so dependent<br />
on plasma album<strong>in</strong> concentrations, the impact of nutri-<br />
Peripheral edema due to low COP.<br />
Case 2<br />
A 5-year-old, neutered, 24-kg Labrador retriever was presented for an 8-week history of small-bowel diarrhea <strong>and</strong><br />
weight loss. The st<strong>and</strong>ard gastro<strong>in</strong>test<strong>in</strong>al workup <strong>in</strong>cluded a <strong>com</strong>plete blood cell count (CBC), biochemical profile,<br />
multiple fecal exam<strong>in</strong>ations, abdom<strong>in</strong>al imag<strong>in</strong>g studies, <strong>and</strong> endoscopy with biopsies. Based on cl<strong>in</strong>ical f<strong>in</strong>d<strong>in</strong>gs <strong>and</strong><br />
histologic characteristics, the dog was diagnosed with severe lymphocytic-plasmacytic <strong>in</strong>flammatory bowel disease.<br />
Despite a low serum album<strong>in</strong> of 1.4 g/dl (reference range, 3.0 to 4.2 g/dl) <strong>and</strong> a low COP of 10.6 mm Hg, no edema<br />
was detected.<br />
Case 3<br />
A 7-year-old, spayed, 31-kg Doberman p<strong>in</strong>cher was presented for lethargy, <strong>in</strong>appetence, <strong>and</strong> edema extend<strong>in</strong>g<br />
from the face to all four limbs. A diagnostic workup was performed, <strong>and</strong> no abnormalities were noted on the CBC,<br />
ur<strong>in</strong>alysis, thoracic radiography, or abdom<strong>in</strong>al ultrasound. On a biochemical profile, the album<strong>in</strong> concentration was 3.0<br />
g/dl (reference range, 3.0 to 4.2 g/dl) but was otherwise unremarkable. Systolic blood pressure (130 mm Hg), CVP (3<br />
cm H 2O), <strong>and</strong> COP (21.8 mm Hg) were with<strong>in</strong> normal limits. Given the normal COP, the edema could not be<br />
expla<strong>in</strong>ed by low oncotic pressure. Titers for ehrlichiosis, leptospirosis, <strong>and</strong> ant<strong>in</strong>uclear antigen were negative. Sk<strong>in</strong><br />
biopsies demonstrated neutrophilic <strong>in</strong>filtration of vascular walls, consistent with vasculitis. S<strong>in</strong>ce no <strong>in</strong>cit<strong>in</strong>g cause was<br />
identified, prednisone (20 mg q12h PO) was <strong>in</strong>itiated. After 2 weeks of therapy, the edema <strong>com</strong>pletely resolved <strong>and</strong> the<br />
dog showed no other signs of illness. Prednisone was gradually discont<strong>in</strong>ued.<br />
tional support, either parenteral or enteral, on overall album<strong>in</strong><br />
synthesis needs to be evaluated. Development of<br />
newer synthetic colloids with decreased side effects <strong>and</strong><br />
<strong>in</strong>creased <strong>in</strong>travascular persistence holds much promise<br />
for the treatment of critically ill patients. As our underst<strong>and</strong><strong>in</strong>g<br />
of COP <strong>in</strong> health <strong>and</strong> disease cont<strong>in</strong>ues to develop,<br />
direct measurements of COP <strong>in</strong> cl<strong>in</strong>ical patients<br />
could be<strong>com</strong>e an <strong>in</strong>dispensable tool <strong>in</strong> the monitor<strong>in</strong>g<br />
<strong>and</strong> treatment of critically ill animals.
Compendium October 2001 Small Animal/Exotics 903<br />
REFERENCES<br />
1. Holbeck S, Bentzer P, Wikstr<strong>and</strong> C, Gr<strong>and</strong>e PO: Dextran, gelat<strong>in</strong>,<br />
<strong>and</strong> hydroxyethyl starch do not affect permeability for album<strong>in</strong><br />
<strong>in</strong> cat skeletal muscle. Crit Care Med 29(1):123–128, 2001.<br />
2. Smiley LE, Garvey MS: The use of hetastarch as adjunct therapy<br />
<strong>in</strong> 26 dogs with hypoalbum<strong>in</strong>emia: A phase two cl<strong>in</strong>ical trial. J<br />
Vet Intern Med 8(3):195–202, 1994.<br />
3. Pietrangelo A, P<strong>and</strong>uro A, Chowdhury JR, Shafritz DA: Album<strong>in</strong><br />
gene expression is down-regulated by album<strong>in</strong> or macromolecule<br />
<strong>in</strong>fusion <strong>in</strong> the rat. J Cl<strong>in</strong> Invest 89:1755–1760, 1992.<br />
4. Schmid M, Sch<strong>in</strong>dler R, Weig<strong>and</strong> K: Is album<strong>in</strong> synthesis regulated<br />
by the colloid osmotic pressure? Effect of album<strong>in</strong> <strong>and</strong><br />
dextran on album<strong>in</strong> <strong>and</strong> total prote<strong>in</strong> synthesis <strong>in</strong> isolated rat<br />
hepatocytes. Kl<strong>in</strong> Wochenschr 64:23–28, 1986.<br />
5. Vlahos AL, Matthew H, Yu P, et al: Effects of physiologic album<strong>in</strong> <strong>and</strong><br />
hespan levels on hepatocytes <strong>in</strong> vitro. J Trauma 48(6): 1075–1080, 2000.<br />
6. Rackow EC, Fe<strong>in</strong> IA, Leppo J: <strong>Colloid</strong> osmotic pressure as a<br />
prognostic <strong>in</strong>dicator of pulmonary edema <strong>and</strong> mortality <strong>in</strong> the<br />
critically ill. Chest 72:709–713, 1977.<br />
7. K<strong>in</strong>g LG, Culp AM, Clay ME: Measurement of colloid osmotic<br />
pressure <strong>in</strong> a small animal <strong>in</strong>tensive care unit [Abstract]. Proc 4th Int Vet Emerg Crit Care Symp:701, 1994.<br />
8. Rackow EC, Weil MH, MacNeil AR, et al: Effects of crystalloid<br />
<strong>and</strong> colloid fluids on extravascular lung water <strong>in</strong> hypoprote<strong>in</strong>emic<br />
dogs. J Appl Physiol 62(6):2421–2425, 1987.<br />
9. Prien T, Backhaus N, Pelster F, et al: Effect of <strong>in</strong>traoperative fluid<br />
adm<strong>in</strong>istration <strong>and</strong> colloid osmotic pressure on the formation<br />
of <strong>in</strong>test<strong>in</strong>al edema dur<strong>in</strong>g gastro<strong>in</strong>test<strong>in</strong>al surgery. J Cl<strong>in</strong> Anesth<br />
2:317–323, 1990.<br />
10. Guyton AC: The body fluid <strong>com</strong>partments: Extracellular <strong>and</strong><br />
<strong>in</strong>tracellular fluids; <strong>in</strong>terstitial fluid <strong>and</strong> edema, <strong>in</strong> Guyton AC,<br />
Hall JE (eds): Textbook of Medical Physiology, ed 9. Philadelphia,<br />
WB Saunders Co, 1996, pp 297–313.<br />
11. Rackow EC, Fe<strong>in</strong> IA, Siegel J: The relationship of the colloid osmotic-pulmonary<br />
artery wedge pressure gradient to pulmonary<br />
edema <strong>and</strong> mortality <strong>in</strong> critically ill patients. Chest 82:433–437,<br />
1982.<br />
12. L<strong>and</strong>is EM, Pappenheimer JR: Exchange of substances through<br />
capillary walls, <strong>in</strong> Halm<strong>in</strong>ton WF, Dow P (eds): H<strong>and</strong>book of<br />
Physiology. Wash<strong>in</strong>gton, DC, American Physiological Society,<br />
1963, pp 961–1034.<br />
13. Geranton F, Chantrel F, Bouiller M, et al: Prediction of colloid<br />
osmotic pressure <strong>in</strong> renal patients. Cl<strong>in</strong> Nephrol 53(4): 269–275,<br />
2000.<br />
14. Barclay SA, Bennett D: The direct measurement of plasma colloid<br />
osmotic pressure is superior to colloid osmotic pressure derived<br />
from album<strong>in</strong> or total prote<strong>in</strong>. Intensive Care Med<br />
13(2):114–118, 1987.<br />
15. Thomas LA, Brown SA: Relationship between colloid osmotic<br />
pressure <strong>and</strong> plasma prote<strong>in</strong> concentration <strong>in</strong> cattle, horses,<br />
dogs, <strong>and</strong> cats. Am J Vet Res 53:2241–2243, 1992.<br />
16. Brown SA, Dusza K, Boehmer J: Comparison of measured <strong>and</strong><br />
calculated values for colloid osmotic pressure <strong>in</strong> hospitalized animals.<br />
Am J Vet Res 55(7):910–914, 1994.<br />
17. Rudloff E, Kirby R: <strong>Colloid</strong> osmometry. Cl<strong>in</strong> Tech Small Anim<br />
Pract 15(3):119–125, 2000.<br />
18. Culp AM, Clay ME, Baylor IA, K<strong>in</strong>g LG: <strong>Colloid</strong> osmotic pressure<br />
<strong>and</strong> total solids measurements <strong>in</strong> normal dogs <strong>and</strong> cats [abstract].<br />
Proc 4th Int Vet Emerg Crit Care Symp:705, 1994.<br />
19. Haupt MT, Kaufman BS, Carlson RW: Fluid resuscitation <strong>in</strong><br />
patients with <strong>in</strong>creased vascular permeability. Crit Care Cl<strong>in</strong><br />
8(2):341–353, 1992.<br />
20. Kongstad L, Moller AD, Gr<strong>and</strong>e PO: Reflection coefficient for<br />
album<strong>in</strong> <strong>and</strong> capillary fluid permeability <strong>in</strong> cat calf muscle after<br />
traumatic <strong>in</strong>jury. Acta Physiol Sc<strong>and</strong> 165(4):369– 377, 1999.<br />
21. Marx G, Vangerow B, Burczyk C, et al: Evaluation of non<strong>in</strong>vasive<br />
determ<strong>in</strong>ants for capillary leakage syndrome <strong>in</strong> septic shock<br />
patients. Intensive Care Med 26:1252–1258, 2000.<br />
22. Wissel<strong>in</strong>k W, Patetsios P, Panetta TF, et al: Medium molecular<br />
weight pentastarch reduces reperfusion <strong>in</strong>jury by decreas<strong>in</strong>g capillary<br />
leak <strong>in</strong> an animal model of sp<strong>in</strong>al cord ischemia. J Vasc<br />
Surg 27(1):109–116, 1998.<br />
23. Webb AR, Moss RF, Tighe D, et al: A narrow range, medium<br />
molecular weight pentastarch reduces structural organ damage<br />
<strong>in</strong> a hyperdynamic porc<strong>in</strong>e model of sepsis. Intensive Care Med<br />
18:348–355, 1992.<br />
24. Holcroft JW, Trunkey DD, Carpenter MA: Extravasation of album<strong>in</strong><br />
<strong>in</strong> tissues of normal <strong>and</strong> septic baboons <strong>and</strong> sheep. J Surg<br />
Res 26:341–347, 1979.<br />
25. Fadnes HO, Pape JF, Sundsfjord JA: A study on oedema mechanism<br />
<strong>in</strong> nephrotic syndrome. Sc<strong>and</strong> J Cl<strong>in</strong> Lab Invest 46:533–<br />
538, 1986.<br />
26. Ichikawa I, Rennke HG, Houer JR, et al: Role of <strong>in</strong>trarenal<br />
mechanisms <strong>in</strong> the impaired salt excretion of experimental<br />
nephrotic syndrome. J Cl<strong>in</strong> Invest 71:91–103, 1979.<br />
27. Kirby R, Rudloff E: The critical need for colloids: Ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g fluid<br />
balance. Compend Cont<strong>in</strong> Educ Pract Vet 19(6):705–718, 1997.<br />
28. Chan DL, Freeman LM, Rozanski EA, Rush JE: <strong>Colloid</strong> osmotic<br />
pressure of parenteral nutrition <strong>com</strong>ponents <strong>and</strong> other fluids<br />
<strong>com</strong>monly used <strong>in</strong> critically ill animals. JVECC, <strong>in</strong> press, 2001.<br />
29. Bumpus SE, Hask<strong>in</strong>s SC, Kass PH: Effect of synthetic colloids<br />
on refractometric read<strong>in</strong>gs of totals solids. J Vet Emerg Crit Care<br />
8(1):21–26, 1998.<br />
30. Tonnessen T, Tollofsrud S, Kongsgaard E, et al: <strong>Colloid</strong> osmotic<br />
pressure of plasma replacement fluids. Acta Anaesthiol Sc<strong>and</strong><br />
37:424–426, 1993.<br />
31. K<strong>in</strong>g LG: <strong>Colloid</strong> osmometry, <strong>in</strong> Bonagura (ed): Kirk’s Current<br />
Vet Therapy XIII. Philadelphia, WB Saunders Co, 2000, pp<br />
116–118.<br />
32. Zikria BA, K<strong>in</strong>g TC, Stanford J, Freeman HP: A biophysical approach<br />
to capillary permeability. Surgery 105(5):625–631, 1989.<br />
33. Oz MC, FitzPatrick MF, Zikria BA, et al: Attenuation of microvascular<br />
permeability dysfunction <strong>in</strong> postischemic striated<br />
muscle by hydroxyethyl starch. Microvasc Res 50(1):71–79,<br />
1995.<br />
34. McGrath AM, Conhaim RL, Myers GA, Harms BA: Pulmonary<br />
vascular filtration of starch-based macromolecules: Effects on<br />
lung fluid balance. J Surg Res 65(2):128–134, 1996.<br />
35. Matthay MA, Berthraume Y, Staub NC: Long-term clearance of<br />
liquid <strong>and</strong> prote<strong>in</strong> from the lungs of unanesthetized sheep. J<br />
Appl Physiol 59:928–934, 1985.
904 Small Animal/Exotics Compendium October 2001<br />
ARTICLE<br />
CE<br />
#4 CE TEST<br />
The article you have read qualifies for 1.5 contact<br />
hours of Cont<strong>in</strong>u<strong>in</strong>g Education Credit from<br />
the Auburn University College of Veter<strong>in</strong>ary Med-<br />
ic<strong>in</strong>e. Choose the best answer to each of the follow-<br />
<strong>in</strong>g questions; then mark your answers on the<br />
postage-paid envelope <strong>in</strong>serted <strong>in</strong> Compendium.<br />
1. Intravascular COP<br />
a. is generated by <strong>in</strong>terstitial album<strong>in</strong> <strong>and</strong> other prote<strong>in</strong>s.<br />
b. preserves fluid with<strong>in</strong> the vasculature <strong>and</strong> opposes<br />
extravasation of fluid <strong>in</strong>to the <strong>in</strong>terstitium.<br />
c. is a negligible Starl<strong>in</strong>g force <strong>in</strong> biologic systems.<br />
d. is preserved despite losses of album<strong>in</strong> encountered<br />
<strong>in</strong> many different diseases.<br />
2. Starl<strong>in</strong>g’s equation<br />
a. can be accurately calculated us<strong>in</strong>g CVP <strong>and</strong> plasma.<br />
b. relates fluid shifts <strong>in</strong> terms of reflection <strong>and</strong> filtration<br />
coefficients.<br />
c. relates fluid flux as a difference <strong>in</strong> hydrostatic <strong>and</strong><br />
oncotic gradients found between the <strong>in</strong>travascular<br />
<strong>and</strong> <strong>in</strong>terstitial <strong>com</strong>partments.<br />
d. is the relationship of forces regulat<strong>in</strong>g fluid homeostasis<br />
<strong>and</strong> is constant among all organ systems.<br />
3. Album<strong>in</strong><br />
a. is the ma<strong>in</strong> contributor to COP.<br />
b. synthesis is solely regulated by hepatic COP.<br />
c. is <strong>com</strong>pletely impermeable through capillary membranes.<br />
d. is an acute-phase prote<strong>in</strong>, <strong>and</strong> its synthesis is <strong>in</strong>creased<br />
<strong>in</strong> response to <strong>in</strong>flammation.<br />
4. One rationale for adm<strong>in</strong>ister<strong>in</strong>g synthetic colloids is to<br />
<strong>in</strong>crease<br />
a. endogenous album<strong>in</strong> synthesis.<br />
b. lymphatic dra<strong>in</strong>age.<br />
c. plasma COP.<br />
d. total prote<strong>in</strong>.<br />
5. The Gibbs-Donnan effect<br />
a. refers to <strong>in</strong>creased membrane permeability due to<br />
<strong>in</strong>flammation.<br />
b. contributes to COP by attract<strong>in</strong>g immunoglobul<strong>in</strong>s<br />
<strong>and</strong> other osmotically active prote<strong>in</strong>s to album<strong>in</strong>.<br />
c. <strong>in</strong>creases COP by attract<strong>in</strong>g sodium ions to album<strong>in</strong><br />
aga<strong>in</strong>st their concentration gradient.<br />
d. is the difference between the oncotic <strong>and</strong> hydrostatic<br />
gradients.<br />
6. Increased vascular permeability<br />
a. is counteracted by <strong>in</strong>creased prote<strong>in</strong> synthesis.<br />
b. can be easily reduced by adm<strong>in</strong>ister<strong>in</strong>g synthetic<br />
colloids.<br />
c. is usually transient <strong>and</strong> not significant <strong>in</strong> cl<strong>in</strong>ical<br />
cases.<br />
d. has been associated with conditions such as sepsis,<br />
SIRS, ARDS, vasculitis, <strong>and</strong> burns.<br />
7. Measurement of COP<br />
a. is <strong>in</strong>accurate <strong>in</strong> acidemic patients; therefore, predictive<br />
formulas of COP based on total solids should<br />
be used.<br />
b. can be used to guide colloid therapy <strong>and</strong> help evaluate<br />
causes of edema.<br />
c. can be falsely reduced <strong>in</strong> hemolyzed samples.<br />
d. is useful <strong>in</strong> calculat<strong>in</strong>g the exact dose of colloid<br />
therapy.<br />
8. Plasma COP values above the reference range<br />
a. have significant implications for colloid therapy.<br />
b. can be seen with severe hypergammaglobul<strong>in</strong>emia<br />
associated with fel<strong>in</strong>e <strong>in</strong>fectious peritonitis or multiple<br />
myeloma.<br />
c. can be used as a therapeutic endpo<strong>in</strong>t of colloid<br />
therapy.<br />
d. predispose patients to pulmonary edema.<br />
9. Animals with chronic hypoprote<strong>in</strong>emia<br />
a. are best treated with natural rather than with synthetic<br />
colloids.<br />
b. should be treated with synthetic colloids until COP<br />
is restored to normal.<br />
c. do not require treatment because COP is ma<strong>in</strong>ta<strong>in</strong>ed<br />
at normal levels by other molecules.<br />
d. may not require treatment if cl<strong>in</strong>ical signs (e.g.,<br />
edema) are absent.<br />
10. Desirable characteristics of newly developed synthetic<br />
colloids <strong>in</strong>clude<br />
a. <strong>in</strong>creased antigenic stimulation <strong>and</strong> uniform particle<br />
size.<br />
b. a shorter half-life than current synthetic colloids.<br />
c. decreased side effects <strong>and</strong> <strong>in</strong>creased <strong>in</strong>travascular<br />
persistence.<br />
d. decreased <strong>in</strong>travascular persistence <strong>and</strong> the ability<br />
to <strong>in</strong>crease vascular permeability.