WEISS-April PV-SA Review - VetLearn.com
WEISS-April PV-SA Review - VetLearn.com
WEISS-April PV-SA Review - VetLearn.com

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
CE<br />
364 Vol. 23, No. 4 <strong>April</strong> 2001<br />
Article #5 (1.5 contact hours)<br />
Refereed Peer <strong>Review</strong><br />
KEY FACTS<br />
■ Signs of inflammatory liver<br />
disease in cats can mimic those<br />
of other liver conditions.<br />
■ Establishing a definitive diagnosis<br />
is important because approaches<br />
to treatment vary.<br />
■ Prolonged survival can be<br />
expected in cats that survive for<br />
at least 3 months following<br />
diagnosis of inflammatory liver<br />
disease.<br />
Email <strong>com</strong>ments/questions to<br />
<strong>com</strong>pendium@medimedia.<strong>com</strong><br />
Inflammatory Liver<br />
Diseases in Cats<br />
University of Minnesota<br />
Douglas J. Weiss, DVM, PhD<br />
Josanne Gagne, DVM<br />
Pamela J. Armstrong, DVM, MS, MBA<br />
ABSTRACT: Inflammatory liver diseases <strong>com</strong>prise the second most <strong>com</strong>mon cause of liver<br />
disease in cats. The two major forms of inflammatory liver disease described in North America<br />
are cholangiohepatitis (acute and chronic forms) and lymphocytic portal hepatitis. Signalment,<br />
clinical signs, clinical laboratory data, and ultrasonography can be used to establish a presumptive<br />
diagnosis of inflammatory liver disease; however, hepatic biopsy is needed for<br />
definitive diagnosis. Differences in treatment strategies for cholangiohepatitis and lymphocytic<br />
portal hepatitis warrant establishing a definitive diagnosis. Prognosis for long-term survival is<br />
good for cats that survive the first 2 to 3 months after diagnosis of either of these diseases.<br />
In North America, major causes of feline liver disease include the following 1 :<br />
■ Hepatic lipidosis—50% of cases<br />
■ Inflammatory liver disease—25%<br />
■ Malignant lymphoma—5%<br />
■ Carcinoma—4%<br />
Terminology used to describe inflammatory liver diseases of cats can be confusing.<br />
1–3 These terms include suppurative or acute cholangiohepatitis, chronic<br />
cholangiohepatitis, chronic progressive nonsuppurative cholangiohepatitis, pericholangiohepatitis,<br />
chronic lymphocytic cholangitis, progressive lymphocytic<br />
cholangitis, sclerosing cholangitis, lymphocytic-plasmacytic cholangitis/cholangiohepatitis,<br />
lymphocytic cholangitis/cholangiohepatitis, lymphocytic portal hepatitis,<br />
and biliary cirrhosis. 1–4 Some authors have preferred to use the general term<br />
cholangiohepatitis <strong>com</strong>plex or cholangiohepatitis/cholangitis <strong>com</strong>plex. 2,5 Recent retrospective<br />
studies have clarified the classification of these diseases into acute cholangiohepatitis,<br />
chronic cholangiohepatitis, and lymphocytic portal hepatitis. 1,4<br />
TYPES OF INFLAMMATORY LIVER DISEASE<br />
Although there is no universally accepted classification of inflammatory liver<br />
disease in cats, a classification scheme based on histopathologic features is gaining<br />
support. 1,3 Two major types of inflammatory liver disease have been described<br />
based on distinct histopathologic features: cholangiohepatitis (acute and<br />
chronic forms) and lymphocytic portal hepatitis. 1 Another syndrome that may
Compendium <strong>April</strong> 2001 Small Animal/Exotics 365<br />
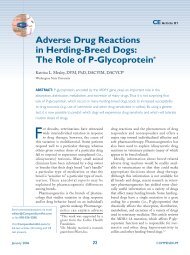
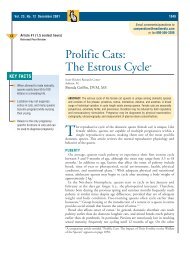
Figure 1—Histopathologic section of liver from a cat with<br />
acute cholangiohepatitis showing a greatly enlarged portal<br />
area (left side) and a portion of a hepatic lobule (right side).<br />
The portal area is characterized by infiltration of large numbers<br />
of neutrophils, inflammatory exudate within bile ducts<br />
(arrows), and fibrosis (H&E stain).<br />
be distinct from cholangiohepatitis and lymphocytic<br />
portal hepatitis, called progressive lymphocytic cholangitis/cholangiohepatitis,<br />
has been described. 6,7 Liver fluke<br />
infestation can also cause inflammatory liver disease. 8<br />
Acute Cholangiohepatitis<br />
Acute cholangiohepatitis is characterized by infiltration<br />
of large numbers of neutrophils into portal areas of<br />
the liver and into bile ducts (Figure 1). 1 Disruption of<br />
the periportal limiting plate results in necrosis of hepatocytes<br />
adjacent to portal areas and infiltration of neutrophils<br />
into hepatic lobules. Acute cholangiohepatitis<br />
may begin as an ascending bacterial infection within<br />
the biliary tract; however, bacteria have been isolated<br />
from the liver or gallbladder in only a few cases. 2,9 Failure<br />
to isolate organisms may be due in part to previous<br />
antibiotic therapy and failure to culture for anaerobic<br />
organisms. Organisms that have been isolated include<br />
Bacteroides, Escherichia coli, Clostridium, and αhemolytic<br />
Streptococcus. 2 Congenital or acquired abnormalities<br />
of the biliary system, including anatomic abnormalities<br />
of the gallbladder or <strong>com</strong>mon bile duct and<br />
gallstones (i.e., choleliths), may predispose cats to<br />
cholangiohepatitis. Choleliths appear to be an infrequent<br />
cause of inflammatory liver disease. 2 Conversely,<br />
inspissation of bile, which may cause partial or <strong>com</strong>plete<br />
obstruction of the <strong>com</strong>mon bile duct, gallbladder,<br />
or intrahepatic bile ducts, appears to frequently ac<strong>com</strong>pany<br />
cholangiohepatitis and may require surgical intervention.<br />
Chronic Cholangiohepatitis<br />
Chronic cholangiohepatitis is theorized to be a later<br />
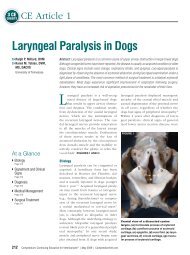
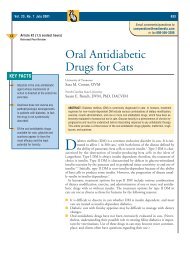
Figure 2—Histopathologic section of liver from a cat with<br />
chronic cholangiohepatitis. Note extensive fibrosis and scattered<br />
inflammatory cells in an enlarged portal area (A), a<br />
small island of hepatocytes (large arrows), and extensive bile<br />
duct proliferation (small arrows; H&E stain).<br />
stage of acute cholangiohepatitis. 1,10 It is characterized<br />
by a mixed inflammatory infiltrate in portal areas and<br />
bile ducts consisting of neutrophils, lymphocytes, and<br />
plasma cells (Figure 2). 1 Unlike acute cholangiohepatitis,<br />
bile duct hypertrophy and portal fibrosis are prominent<br />
features of the disease. Other conditions that may<br />
be confused with chronic cholangiohepatitis include feline<br />
infectious peritonitis virus, Toxoplasma infections,<br />
and liver fluke infestation. In liver fluke infestation,<br />
eosinophil numbers are usually increased in portal areas,<br />
whereas eosinophils are rare or absent in other<br />
types of chronic cholangiohepatitis.<br />
Diseases frequently associated with cholangiohepatitis<br />
include inflammatory bowel disease and pancreatitis.<br />
Of cats with cholangiohepatitis, 83% had concurrent<br />
inflammatory infiltrates in the duodenum and/or jejunum<br />
and 50% had pancreatic lesions. 9 How these<br />
disorders relate to one another is unclear. Some authors<br />
theorize that inflammatory bowel disease causes reflux<br />
of bacteria or other constituents of duodenal contents<br />
into the <strong>com</strong>mon bile duct with resultant pancreatitis<br />
and cholangiohepatitis. 1–5<br />
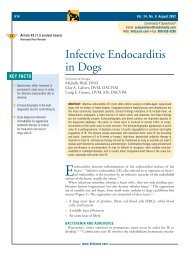
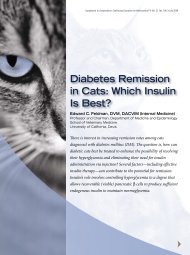
Lymphocytic Portal Hepatitis<br />
Lymphocytic portal hepatitis appears to be distinct<br />
from acute and chronic cholangiohepatitis. It is characterized<br />
by infiltration of lymphocytes and plasma cells<br />
but not neutrophils into portal areas but not into bile<br />
ducts (Figure 3). Variable degrees of bile duct hypertrophy<br />
and fibrosis are present. 1,10<br />
Lymphocytic portal hepatitis is a <strong>com</strong>mon finding in<br />
older cats. In a retrospective study of cat livers obtained<br />
at necropsy, 82% of cats over 10 years of age had
366 Small Animal/Exotics Compendium <strong>April</strong> 2001<br />
Figure 3—Histopathologic section from a cat with lymphocytic<br />
portal hepatitis. Note the enlarged portal area containing<br />
large numbers of lymphocytes, mild fibrosis, and bile<br />
duct proliferation (H&E stain).<br />
histopathologic changes consistent with lymphocytic<br />
portal hepatitis, whereas only 10% of cats younger than<br />
10 years of age showed these histopathologic changes. 11<br />
Few of these cats had a clinical diagnosis of liver disease.<br />
However, not all cats with lymphocytic infiltrates in<br />
portal areas are asymptomatic. In a review of 175 liver<br />
biopsies from cats with clinical evidence of liver disease,<br />
15% had a diagnosis of lymphocytic portal hepatitis. 1<br />
Because of the presence of lymphocytes and plasma<br />
cells in portal areas and the lack of concurrent diseases,<br />
several authors have speculated that lymphocytic portal<br />
hepatitis is an immune-mediated disease. 1,3 However,<br />
data on the role of immune mechanisms in the initiation<br />
and/or perpetuation of lymphocytic portal hepatitis<br />
have not been reported.<br />
Liver Flukes<br />
Several species of liver flukes have been reported in<br />
cats in the United States. 8 The incidence of infestation<br />
varies by geographic region. The condition occurs frequently<br />
in Florida, for example, whereas only one case<br />
was identified over 10 years at the University of Minnesota<br />
Veterinary Teaching Hospital. 1 Histopathologic<br />
features of liver fluke infestation include distended and<br />
fibrotic bile ducts and epithelial proliferation of bile<br />
duct walls. 8 A mixed inflammatory infiltrate, consisting<br />
of macrophages, lymphocytes, plasma cells, eosinophils,<br />
and neutrophils, is frequently present in portal areas.<br />
The presence of eosinophils is suggestive of liver fluke<br />
infestation because eosinophils are rarely seen in other<br />
types of inflammatory liver disease. 1<br />
DIAGNOSIS<br />
Clinical Signs<br />
Clinical signs associated with inflammatory liver diseases<br />
are variable, nonspecific, and frequently similar to<br />
those associated with hepatic lipidosis (Table 1). 10 Partial<br />
or <strong>com</strong>plete anorexia is the most <strong>com</strong>mon (and<br />
sometimes the only) clinical sign. Other less frequently<br />
observed clinical signs include weight loss, depression,<br />
vomiting, diarrhea, and fever. Cats with acute cholangiohepatitis<br />
tend to be younger (median age, 3.3 years)<br />
than cats with chronic cholangiohepatitis (median age,<br />
9 years), lymphocytic portal hepatitis (median age, 8.2<br />
years), or hepatic lipidosis (median age, 6.2 years). 10<br />
Male cats are more frequently affected with acute<br />
cholangiohepatitis than are female cats. 10 Cats with<br />
acute cholangiohepatitis are more acutely and severely<br />
ill than cats with most other types of liver disease. 10<br />
Prominent clinical signs in acute cholangiohepatitis include<br />
fever, depression, and dehydration.<br />
Jaundice and altered liver size are frequently the only<br />
findings that direct attention to liver disease (Table<br />
1). 3,10 Jaundice is most easily observed in the sclera but<br />
TABLE 1<br />
Signalment and Clinical Signs Associated with Inflammatory Liver Diseases and Hepatic Lipidosis in Cats<br />
Acute Chronic Lymphocytic Hepatic<br />
Observation Cholangiohepatitis Cholangiohepatitis Portal Hepatitis Lipidosis<br />
Age Young Middle age Middle age Middle age<br />
Gender bias Males Males None None<br />
Onset of signs Days Weeks Weeks Days to weeks<br />
Severity of illness Severe Mild to moderate Mild Mild to severe<br />
Anorexia Frequent Frequent Frequent All cases<br />
Weight loss Frequent Frequent Frequent All cases<br />
Fever Frequent Infrequent Rare Rare<br />
Jaundice Frequent Frequent Frequent Frequent<br />
Hepatomegaly Frequent Frequent Frequent Frequent<br />
Ascites Rare Rare Rare Rare
Compendium <strong>April</strong> 2001 Small Animal/Exotics 367<br />
TABLE 2<br />
Clinical Laboratory Alterations in Inflammatory Liver Diseases, Hepatic Lipidosis, and Hepatic Lymphoma<br />
Acute Chronic Lymphocytic Hepatic Hepatic<br />
Parameter Cholangiohepatitis Cholangiohepatitis Portal Hepatitis Lipidosis Lymphoma<br />
Neutrophilia Frequent Infrequent Rare Rare Frequent<br />
Left shift Frequent Infrequent Rare Rare Infrequent<br />
Serum bilirubin Mild increase Moderate increase Mild increase Marked increase Mild increase<br />
Alanine Moderate increase Moderate increase Mild to moderate Marked increase Moderate to<br />
aminotransferase increase marked increase<br />
Serum alkaline Frequently normal Mild to moderate Normal to mild Moderate to Moderate to<br />
phosphatase increase increase marked increase marked increase<br />
Fasting bile acids Increased Increased Increased Increased Increased<br />
may also be observed in the soft palate or under the<br />
tongue. Ecchymotic hemorrhages and/or prolonged<br />
bleeding from venipuncture sites may occur. When liver<br />
size is evaluated radiographically, approximately half<br />
of cats with acute or chronic cholangiohepatitis, lymphocytic<br />
portal hepatitis, or hepatic lipidosis have hepatomegaly<br />
and the remaining cats have normal-sized<br />
livers. 10 Therefore, hepatomegaly is a frequent finding<br />
in feline inflammatory liver diseases but cannot be used<br />
to differentiate the various causes.<br />
Laboratory Evaluation<br />
Hematologic and biochemical testing are essential to<br />
establish a diagnosis of liver disease (Table 2). Fasting<br />
bile acid determination is the test that is most consistently<br />
abnormal in all types of inflammatory liver disease. 10<br />
Laboratory changes typically seen with acute cholangiohepatitis<br />
include mild neutrophilia and left shift,<br />
normal or slightly increased serum bilirubin and serum<br />
alkaline phosphatase (<strong>SA</strong>P) levels, and substantially increased<br />
alanine aminotransferase (ALT) level. 10 This<br />
profile tends to differentiate acute cholangiohepatitis<br />
from chronic cholangiohepatitis, hepatic lipidosis, and<br />
hepatic neoplasia.<br />
Laboratory changes typical of chronic cholangiohepatitis<br />
include substantial increases in serum bilirubin,<br />
<strong>SA</strong>P, and ALT levels. 10 Other associated changes may<br />
include mild nonregenerative anemia, hyperglobulinemia,<br />
lymphocytosis, and hyperglycemia. 3,10<br />
Laboratory alterations associated with lymphocytic<br />
portal hepatitis include normal to variably increased<br />
serum bilirubin, ALT, and <strong>SA</strong>P levels. When all inflammatory<br />
liver diseases are <strong>com</strong>pared with hepatic lipidosis,<br />
patients with hepatic lipidosis tend to have higher<br />
total bilirubin concentrations and higher ALT and <strong>SA</strong>P<br />
levels. 10 The hallmarks of hepatic lipidosis include jaundice<br />
and tenfold or greater increases in ALT and <strong>SA</strong>P<br />
levels without a corresponding increase in γ-glutamyl<br />
transferase (GGT). 12 In other forms of liver disease in<br />
cats, increases in GGT tend to parallel increases in <strong>SA</strong>P.<br />
When the clinical chemistry profile reveals evidence<br />
of liver disease, hyperthyroidism should be ruled out.<br />
Hyperthyroid cats frequently have changes in ALT and<br />
<strong>SA</strong>P levels that may be indistinguishable from those associated<br />
with inflammatory liver diseases. 13 The increased<br />
enzyme concentrations normalize with treatment<br />
of hyperthyroidism. Pathologic changes in the<br />
liver associated with hyperthyroidism have not been<br />
well characterized.<br />
Liver Imaging<br />
Abdominal ultrasonography is often helpful in evaluating<br />
extrahepatic disorders associated with cholangiohepatitis.<br />
14,15 Most cats with acute or chronic cholangiohepatitis<br />
or lymphocytic portal hepatitis have<br />
variable or no detectable alterations in the echogenicity<br />
of the hepatic parenchyma. Conversely, most cats with<br />
hepatic lipidosis have hyperechoic hepatic parenchyma.<br />
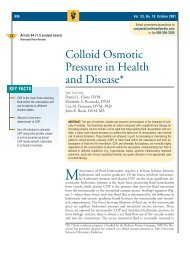
Bile duct abnormalities may be observed in cholangiohepatitis.<br />
These abnormalities include gallbladder<br />
and/or <strong>com</strong>mon bile duct distention, cholelithiasis,<br />
cholecystitis, and bile sludging (Figure 4). 2 The normal<br />
gallbladder is anechoic and appears round in the transverse<br />
scan and pear-shaped in the longitudinal scan. 14 It<br />
is important to remember that gallbladder filling occurs<br />
normally with fasting; therefore, caution must be exercised<br />
when interpreting gallbladder enlargement in an<br />
anorectic or fasting cat. 14 The <strong>com</strong>mon bile duct can<br />
usually be seen as an anechoic, tortuous, tubular structure<br />
2 to 4 mm in diameter with an echogenic wall. 14<br />
Distention of the gallbladder and <strong>com</strong>mon bile duct<br />
(i.e., greater than 5 mm in diameter) occurs as a result<br />
of cholecystitis or biliary obstruction. 14 The gallbladder<br />
wall may be<strong>com</strong>e thickened as a result of inflammation
368 Small Animal/Exotics Compendium <strong>April</strong> 2001<br />
Figure 4—Sonogram of a cat with <strong>com</strong>plete bile duct obstruction.<br />
Note the enlarged <strong>com</strong>mon bile duct (large arrow) and<br />
dilated intrahepatic bile ducts (small arrows). Bile sludge<br />
within the <strong>com</strong>mon bile duct is echogenic.<br />
or edema. The thickened gallbladder wall has a layered<br />
or double-walled appearance. Bile sludge within the<br />
gallbladder or <strong>com</strong>mon bile duct appears echogenic. 14<br />
Liver Cytology/Histopathology<br />
Evaluation of pathologic changes in the liver is essential<br />
in differentiating inflammatory liver diseases from<br />
hepatic lipidosis and neoplasia. 16–20 Percutaneous fineneedle<br />
aspiration; percutaneous tissue biopsy; and keyhole,<br />
laparoscopic, and intraoperative wedge biopsy<br />
procedures have been described. 16,17 Fine-needle aspirates<br />
can usually be performed without anesthesia.<br />
When a 22-gauge needle is used for collection of aspiration<br />
specimens, the risk of hemorrhage is minimal;<br />
however, the risk is greater if large tissue biopsy needles<br />
are used. Therefore, coagulation testing is re<strong>com</strong>mended<br />
before a tissue biopsy specimen is collected. Collection<br />
of bile from the gallbladder for cytologic evaluation<br />
and bacterial culture has the potential to result in<br />
rupture with resultant bile peritonitis. Therefore, aspiration<br />
of the gallbladder should be attempted only with<br />
ultrasonographic guidance or exploratory laparotomy.<br />
The diagnostic utility of liver cytology is controversial.<br />
Several reports indicate that cytologic evaluation is<br />
highly efficient in identifying hepatic lipidosis and hepatic<br />
lymphoma; however, inflammatory liver diseases are<br />
more difficult to identify cytologically. 17–19 Results of another<br />
retrospective study, however, indicate poor correlation<br />
between liver cytology and histopathology. 20 Hepatic<br />
lipidosis is cytologically characterized by clusters of<br />
hepatocytes in which the cytoplasm is distended with<br />
lipid-filled droplets (Figure 5). Malignant lymphoma<br />
cells readily exfoliate and can be diagnosed by cytologic<br />
Figure 5—Cytologic specimen from a cat with hepatic lipidosis.<br />
Note a cluster of hepatocytes in which the cytoplasm is<br />
distended with clear lipid droplets (Wright’s stain).<br />
Figure 6—Cytologic specimen from a cat with malignant<br />
lymphoma. Note many large lymphoblasts and normal-appearing<br />
hepatocytes (Wright’s stain).<br />
evaluation (Figure 6). Cytologic diagnosis of inflammatory<br />
liver diseases is hampered by blood contamination,<br />
which introduces variable numbers of blood leukocytes<br />
into the samples. Therefore, the cytologist is left to determine<br />
whether leukocytes are of blood origin or represent<br />
inflammatory lesions within the liver (Figure 7).<br />
Cytologic techniques in which samples are collected<br />
without aspirating minimize blood contamination and<br />
improve the chances that inflammatory lesions can be<br />
identified. 17 Use of a 22-gauge needle connected to a<br />
12-ml syringe via an 84-cm flexible extension set (i.e.,<br />
used for intravenous infusion lines) has been re<strong>com</strong>mended.<br />
17 The needle is inserted into the liver and<br />
moved back and forth 8 to 10 times without aspiration.<br />
Ultrasound-guided aspiration and biopsy techniques<br />
more consistently produce diagnostic specimens than<br />
do blind techniques. 21 Ultrasound-guided fine-needle<br />
aspiration can be used to sample bile as well as hepatic
370 Small Animal/Exotics Compendium <strong>April</strong> 2001<br />
Figure 7—Cytologic specimen from a cat with acute cholangiohepatitis.<br />
Note clusters of normal-appearing hepatocytes<br />
and large numbers of neutrophils (Wright’s stain).<br />
parenchyma. Such samples can be examined cytologically<br />
to look for inflammatory cells and bacteria and<br />
can be cultured to confirm bacterial infections.<br />
TREATMENT<br />
Cholangiohepatitis<br />
The major specific therapy for acute and chronic<br />
cholangiohepatitis is antibiotics. 2,4 Surgical intervention<br />
has been re<strong>com</strong>mended if discrete choleliths or <strong>com</strong>plete<br />
biliary obstruction is identified. When <strong>com</strong>plete<br />
extrahepatic bile duct obstruction is identified, surgical<br />
de<strong>com</strong>pression and biliary-to-intestinal diversion (i.e.,<br />
cholecystoduodenostomy or cholecystojejunostomy) are<br />
re<strong>com</strong>mended. 2 However, surgery is not indicated for<br />
bile duct enlargement or obstruction due to fluke infestation.<br />
Bacterial culture and sensitivity testing of liver<br />
tissue, bile, choleliths, or gallbladder specimens should<br />
be used to select appropriate antimicrobial agents whenever<br />
possible. Antibiotics chosen for treatment of<br />
cholangiohepatitis should be excreted in the bile in active<br />
form and should be active against aerobic and<br />
anaerobic intestinal coliforms. Tetracycline, ampicillin,<br />
amoxicillin, erythromycin, chloramphenicol, and<br />
metronidazole are excreted in the bile in active form;<br />
however, several of these agents have significant adverse<br />
side effects. 5 Erythromycin is not effective against gramnegative<br />
bacteria, tetracycline is hepatotoxic, and chloramphenicol<br />
may cause anorexia. As a result, ampicillin<br />
or amoxicillin <strong>com</strong>bined with clavulanic acid is frequently<br />
used. All are broad-spectrum antibiotics, effective<br />
against both gram-negative and gram-positive organisms,<br />
and are well tolerated by cats. These drugs may<br />
be <strong>com</strong>bined with metronidazole to extend the spectrum<br />
to anaerobes and more coliforms. Treatment with<br />
antibiotics for 2 months or longer is re<strong>com</strong>mended.<br />
When cats with chronic cholangiohepatitis fail to respond<br />
to antibiotic therapy alone within 2 to 3 weeks,<br />
prednisolone is usually added as an empiric treatment. 5<br />
The antiinflammatory and immunosuppressive properties<br />
of prednisolone may be beneficial in limiting hepatocellular<br />
injury. Additionally, prednisolone may enhance<br />
appetite. An immunosuppressive dose of prednisolone<br />
(2.2 to 4 mg/kg q24h) should be used initially. The<br />
dosage is slowly tapered to an alternate-day regimen (1 to<br />
2 mg/kg q48h) for long-term maintenance. A schedule<br />
<strong>com</strong>monly used is to start therapy at 2 mg/kg bid for 2<br />
weeks, then progressively reduce the dosage as follows: 2<br />
mg/kg sid for 2 weeks; 1 mg/kg sid for 2 weeks; and 1<br />
mg/kg q48h for 4 weeks. Biochemical values should be<br />
monitored prior to each reduction in dosage, and the<br />
dosage should be reduced only if substantial improvement<br />
in clinical signs and substantial reductions in ALT<br />
and <strong>SA</strong>P levels are observed. Doses as low as 0.5 mg/kg<br />
q48h may be sufficient for long-term maintenance.<br />
Long-term corticosteroid treatment is well tolerated by<br />
most cats, and side effects are usually minimal.
Compendium <strong>April</strong> 2001 Small Animal/Exotics 371<br />
Methotrexate in <strong>com</strong>bination with prednisolone has<br />
been re<strong>com</strong>mended for cats that fail to respond to<br />
prednisolone therapy. 2 A suggested dose is 0.4 mg per<br />
cat divided into three doses and given over 24 hours.<br />
The dose is repeated every 7 to 10 days. Because<br />
methotrexate has moderate myelosuppressive potential,<br />
total leukocyte count should be monitored and treatment<br />
should be discontinued if total leukocyte count<br />
drops below 3000/µl. 22<br />
Ursodeoxycholic acid is re<strong>com</strong>mended for cats with<br />
all types of inflammatory liver disease. It has antiinflammatory,<br />
immunomodulatory, and antifibrotic properties<br />
as well as the ability to increase fluidity of biliary secretions.<br />
Ursodeoxycholic acid has been safely administered<br />
to cats at a dose of 10 to 15 mg/kg PO q24h. 3 However,<br />
ursodeoxycholic acid should not be given to cats with<br />
<strong>com</strong>plete bile duct obstruction. Efficacy has not been<br />
established for any type of feline liver disease, but clinical<br />
trials in human patients with hepatitis support improved<br />
quality of life. 2 Adverse effects in cats are un<strong>com</strong>mon<br />
and usually limited to mild diarrhea.<br />
Cats with acute cholangiohepatitis require aggressive<br />
supportive care. These cats are frequently acutely ill<br />
and have fluid and electrolyte derangements that should<br />
be corrected. Treatment with injectable vitamin K 1 (5<br />
mg SC q24–48h) can be given if bleeding diatheses develop.<br />
2,5 Hepatic encephalopathy appears to be un<strong>com</strong>mon<br />
in cats with acquired liver disease and is manifest<br />
most frequently by excessive salivation. Hepatic encephalopathy<br />
can be managed by giving lactulose (0.5<br />
to 1.0 ml/kg PO q8h) with or without enteric antibiotics<br />
(neomycin [20 mg/kg PO q8–12h]). 5,23 Anorexia<br />
must be managed promptly to prevent further deterioration<br />
in clinical condition and possible development of<br />
concurrent hepatic lipidosis. Assisted oral feeding<br />
should be tried for up to 12 hours after which a nasoesophageal<br />
tube should be placed. Ensuring adequate<br />
intake of a high-energy, high-protein diet is a high priority<br />
throughout treatment. Protein is an important nutrient<br />
for liver repair and regeneration and should not<br />
be restricted unless hepatic encephalopathy occurs.<br />
The response of cats with cholangiohepatitis to therapy<br />
should be monitored though use of serial <strong>com</strong>plete<br />
blood counts and chemistry profiles. Persistent increases<br />
in ALT activity and serum total bilirubin concentration<br />
and/or increasing <strong>SA</strong>P activity suggest that treatment<br />
has been inadequate.<br />
Lymphocytic Portal Hepatitis<br />
The approach to treatment of lymphocytic portal<br />
hepatitis is based on the hypothesis that the liver injury<br />
is immune mediated. Immunosuppressive doses of corticosteroids<br />
are used as described above for chronic<br />
cholangiohepatitis. Anecdotal reports indicate prolonged<br />
improvement in clinical signs with prednisolone<br />
treatment. Others, however, report poor control of disease<br />
progression with corticosteroid treatment. 2 Azathioprine<br />
(0.3 mg/kg PO q48–72h) has been tried, but<br />
side effects, including inappetence and leukopenia, limit<br />
its use. Low-dose weekly methotrexate therapy has<br />
been used in a few affected cats. 2<br />
Response to treatment for lymphocytic portal hepatitis<br />
is difficult to assess because the disease progresses<br />
very slowly. A persistent increase in ALT and/or increasing<br />
total serum bilirubin concentration during<br />
corticosteroid treatment indicates that the disease is inadequately<br />
controlled.<br />
PROGNOSIS<br />
Limited studies of the response of cats with cholangiohepatitis<br />
to antibiotic treatment suggest that survival<br />
of cats with acute and chronic forms of the disease is<br />
similar. Approximately half of the cats die or are euthanized<br />
within 90 days after diagnosis. The other half<br />
have prolonged survival. 10 Better understanding of the<br />
pathogenesis of these diseases and initiation of standard<br />
treatment protocols <strong>com</strong>bined, when needed, with surgical<br />
correction of bile duct obstruction should increase<br />
the number of cats that survive long-term.<br />
Lymphocytic portal hepatitis appears to be a very<br />
slowly progressive condition. Mean survival for cats<br />
with this condition was reported to be 36.9 months. 10<br />
In three cats with an initial diagnosis of mild lymphocytic<br />
portal hepatitis with minimal fibrosis and no bile<br />
duct proliferation, necropsies were performed 4 to 7<br />
years after initial diagnosis. Liver sections at necropsy<br />
showed marked progression in the severity of lesions,<br />
which were characterized by marked lymphocytic infiltrates,<br />
severe fibrosis, and severe bile duct hyperplasia.<br />
Therefore, the prognosis for cats with lymphocytic portal<br />
hepatitis appears to be primarily dependent on the<br />
severity of lesions at the time of diagnosis.<br />
REFERENCES<br />
1. Gagne J, Weiss DJ, Armstrong PJ: Histopathologic evaluation<br />
of feline inflammatory liver diseases. Vet Pathol<br />
33:521–526, 1996.<br />
2. Center <strong>SA</strong>, Rowland PH: The cholangitis/cholangiohepatitis<br />
<strong>com</strong>plex in the cat. Proc 12th Annu Vet Med Forum. Orlando,<br />
FL, American College of Veterinary Internal Medicine,<br />
1994, pp 771–776.<br />
3. Johnson S: Chronic hepatic disorders, in Ettinger S (ed):<br />
Textbook of Veterinary Internal Medicine, ed 4. Philadelphia,<br />
WB Saunders Co, 2000, pp 1308–1310.<br />
4. Jones BR: Feline liver disease. Aust Vet Pract 19:28–36, 1989.<br />
5. Zawie DA, Garvey MS: Feline hepatic disease. Vet Clin<br />
North Am Small Anim 2:1201–1230, 1984.<br />
6. Lucke VM, Davis JD: Progressive lymphocytic cholangitis in
372 Small Animal/Exotics Compendium <strong>April</strong> 2001<br />
the cat. J Small Anim Pract 25:249–260, 1984.<br />
7. Day MJ: Immunohistochemical characterization of the lesions<br />
of feline progressive lymphocytic cholangitis/cholangiohepatitis.<br />
J Comp Pathol 119:135–147, 1998.<br />
8. Bielsa LM, Greiner EC: Liver flukes (Pltynosomum concinnum)<br />
in cats. JAAHA 21:269–274, 1985.<br />
9. Weiss DJ, Gagne JM, Armstrong PJ: Relationship between<br />
inflammatory hepatic disease and inflammatory bowel disease,<br />
pancreatitis, and nephritis. JAVMA 209:1114–1116,<br />
1996.<br />
10. Gagne JM, Armstrong PJ, Weiss DJ, et al: Clinical features<br />
of inflammatory liver disease in cats: 41 cases (1983–1993).<br />
JAVMA 214:513–516, 1999.<br />
11. Weiss DJ, Gagne JM, Armstrong PJ: Characterization of<br />
portal lymphocytic infiltrates in feline liver. Vet Clin Pathol<br />
24:91–95, 1995.<br />
12. Biourge VB: Sequential findings in cats with hepatic lipidosis.<br />
Fel Pract 21:25–28, 1993.<br />
13. Peterson ME, Turrel JM: Feline hyperthyroidism, in Kirk<br />
RW (ed): Current Veterinary Therapy IX. Philadelphia, WB<br />
Saunders Co, 1986, pp 1026–1033.<br />
14. Leveille R, Biller DS, Shiroma JT: Sonographic evaluation of<br />
the <strong>com</strong>mon bile duct in cats. J Vet Intern Med 10:296–299,<br />
1996.<br />
15. Penninck D, Berry C: Liver imaging in the cat. Semin Vet<br />
Med Surg 12:10–21, 1997.<br />
16. Kristensen AT, Weiss DJ, Klausner JS, Hardy R: Evaluation<br />
of hepatic cytology as a diagnostic tool in canine and feline<br />
hepatic disease. Compend Contin Educ Pract Vet 12:797–<br />
809, 1990.<br />
17. Menard M, Papageorges M: Fine-needle biopsies: How to<br />
increase diagnostic yield. Compend Contin Educ Pract Vet 19:<br />
738–740, 1997.<br />
18. Stockhaus C, Teske E: Clinical usefulness of liver cytology in<br />
the dog and cat. Kleintierpraxis 42:687, 1997.<br />
19. Roth L: Comparison of liver cytology interpretation and<br />
biopsy diagnosis. Vet Pathol 36:487, 1999.<br />
20. Fondacaro JV, Guilpin VO, Powers BE, Twedt DC: Diagnostic<br />
correlation of liver aspiration cytology with histopathology<br />
in dogs and cats with liver disease. Proc 17th Am<br />
Vet Intern Med Forum. Chicago, IL, 1999, p 719.<br />
21. de Rycke LMJH, van Bree HJJ, Simoens PJM: Ultrasoundguided<br />
tissue-core biopsy of liver, spleen, and kidney in normal<br />
dogs. Vet Rad Ultrasound 40:294–299, 1999.<br />
22. Couto CG: Toxicity of anticancer chemotherapy. Proc 10th<br />
Kal Kan Symp:37–46, 1986.<br />
23. Center <strong>SA</strong>: Diseases of the liver. Strombeck’s Small Animal<br />
Gastroenterology, ed 3. Philadelphia, WB Saunders Co, 1996,<br />
pp 860–873.<br />
About the Authors<br />
Drs. Weiss and Gagne are affiliated with the Department<br />
of Veterinary Pathobiology, and Dr. Armstrong with the<br />
Department of Small Animal Clinical Sciences, University<br />
of Minnesota, St. Paul. Dr. Weiss is a Diplomate of the<br />
American College of Veterinary Pathologists. Dr. Armstrong<br />
is a Diplomate of the American College of Veterinary<br />
Internal Medicine.<br />
ARTICLE<br />
CE<br />
#5 CE TEST<br />
The article you have read qualifies for 1.5 contact<br />
hours of Continuing Education Credit from<br />
the Auburn University College of Veterinary<br />
Medicine. Choose the one best answer to each of the<br />
following questions; then mark your answers on<br />
the test form inserted in Compendium.<br />
1. Dilation of the gallbladder and/or <strong>com</strong>mon bile duct<br />
is most frequently seen in which of the following feline<br />
liver diseases?<br />
a. cholangiohepatitis c. lymphocytic portal hepatitis<br />
b. hepatic lipidosis d. toxic hepatopathy<br />
2. Histopathologic lesions consisting of infiltration of<br />
large numbers of neutrophils into portal areas and bile<br />
duct best describes which of the following types of feline<br />
liver disease?<br />
a. acute cholangiohepatitis<br />
b. hepatic lipidosis<br />
c. lymphocytic portal hepatitis<br />
d. hepatic cysts<br />
3. A serum chemistry profile characterized by marked increases<br />
in <strong>SA</strong>P, ALT, and bilirubin levels and normal<br />
or slight increases in GGT is most consistent with<br />
which of the following feline liver diseases?<br />
a. acute cholangiohepatitis<br />
b. hepatic lipidosis<br />
c. lymphocytic portal hepatitis<br />
d. hepatic cysts<br />
4. A cat presented with a history of acute onset of severe<br />
lethargy, dehydration, fever, and anorexia of 3 days’<br />
duration is most consistent with which of the following<br />
types of feline liver disease?<br />
a. acute cholangiohepatitis<br />
b. hepatic lipidosis<br />
c. lymphocytic portal hepatitis<br />
d. hepatic cysts<br />
5. Finding clusters of hepatocytes in which the cytoplasm<br />
contains large, clear vacuoles in a cytologic specimen<br />
of feline liver is most consistent with which of the following<br />
types of liver disease?<br />
a. acute cholangiohepatitis<br />
b. hepatic lipidosis<br />
c. lymphocytic portal hepatitis<br />
d. hepatic lymphoma<br />
6. Which of the following is the most definitive test(s)<br />
for differentiating cholangiohepatitis from lymphocytic<br />
portal hepatitis and hepatic lipidosis?<br />
a. <strong>SA</strong>P and ALT c. ultrasonography<br />
b. fasting bile acids d. liver biopsy<br />
7. Which of the following is the most appropriate antibiotic<br />
to use in treating acute or chronic cholangiohepatitis?
Compendium <strong>April</strong> 2001 Small Animal/Exotics 373<br />
a. tetracycline c. sulfadiazine<br />
b. penicillin d. ampicillin<br />
8. Which of the following treatment protocols is most<br />
appropriate for a cat with chronic cholangiohepatitis<br />
and <strong>com</strong>plete bile duct obstruction?<br />
a. Treat with ampicillin for 3 to 4 months and then<br />
reevaluate to see whether bile duct obstruction has<br />
resolved.<br />
b. Surgically correct bile duct obstruction before initiating<br />
medical treatment.<br />
c. Treat with ursodeoxycholic acid to dissolve inspissated<br />
bile in the <strong>com</strong>mon bile duct.<br />
d. Treat with a <strong>com</strong>bination of antibiotics and ursodeoxycholic<br />
acid and reevaluate bile duct obstruction<br />
in 3 to 4 months.<br />
9. The presence of large immature lymphoid cells in portal<br />
areas is consistent with which of the following diseases?<br />
a. chronic cholangiohepatitis<br />
b. hepatic lipidosis<br />
c. lymphocytic portal hepatitis<br />
d. malignant lymphoma<br />
10. Mild neutrophilia and left shift are most frequently associated<br />
with which of the following feline liver diseases?<br />
a. acute cholangiohepatitis<br />
b. hepatic lipidosis<br />
c. lymphocytic portal hepatitis<br />
d. chronic cholangiohepatitis