Resectoscopic treatment of ectopic pregnancy in previous cesarean ...
Resectoscopic treatment of ectopic pregnancy in previous cesarean ...
Resectoscopic treatment of ectopic pregnancy in previous cesarean ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
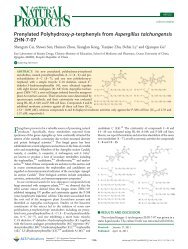
FIGURE 1<br />
Longitud<strong>in</strong>al view <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect (case 1).<br />
The gestational sac is located <strong>in</strong> the PCDS defect and separated<br />
from the cervical canal and endometrial cavity. PCDS ¼ <strong>previous</strong><br />
<strong>cesarean</strong> delivery scar.<br />
Chang. Resectoscopy for <strong>cesarean</strong> scar <strong>pregnancy</strong>. Fertil Steril 2011.<br />
operation, both patients were asked to sign an <strong>in</strong>formed consent<br />
approved by the <strong>in</strong>stitutional review board <strong>of</strong> Kaohsiung Medical<br />
University, Kaohsiung, Taiwan.<br />
The operation was performed by Y.C. us<strong>in</strong>g a 30-degree hysteroscope<br />
with a 10-mm external diameter cont<strong>in</strong>uous flow sheath,<br />
bipolar electrical current, and normal sal<strong>in</strong>e as a medium <strong>of</strong><br />
distension. Under general anesthesia, the patient was placed <strong>in</strong> the<br />
dorsolithotomy position. After a speculum was placed <strong>in</strong>side the vag<strong>in</strong>a,<br />
a tenaculum was applied to the cervix and 10 mL <strong>of</strong> a diluted<br />
vasopress<strong>in</strong> solution (0.4 U/mL; 20 units diluted <strong>in</strong>to 50 mL) was<br />
<strong>in</strong>jected <strong>in</strong> equal amounts <strong>in</strong>to the cervical stroma at the 4 and<br />
8 o’clock positions. The cervix was then carefully dilated by Hegar<br />
dilators to 11 mm.<br />
The <strong>in</strong>tervention began by identify<strong>in</strong>g the implantation <strong>of</strong> the<br />
<strong>ectopic</strong> sac. The gestational tissue was located <strong>in</strong> the PCDS defect<br />
(Fig. 2) and removed under direct vision with cold resection by<br />
a 90-degree wire-loop electrode. For dissection <strong>of</strong> the gestational<br />
tissue and anterior uter<strong>in</strong>e wall, a 180-degree rotation <strong>of</strong> the loop<br />
electrode is recommended.<br />
RESULTS<br />
The operat<strong>in</strong>g time was 20 and 18 m<strong>in</strong>utes for cases 1 and 2, respectively.<br />
Vag<strong>in</strong>al bleed<strong>in</strong>g was m<strong>in</strong>imal throughout the operation. The<br />
patients had an unremarkable postoperative course and were both<br />
discharged the next day. Quantitative b-hCG levels decl<strong>in</strong>ed to<br />
normal with a return time <strong>of</strong> 35 and 32 days for cases 1 and 2, respectively.<br />
The depth <strong>of</strong> PCDS defect, measured by TVU after the first<br />
menses post the hysteroscopic <strong>treatment</strong>, was 9.7 mm for case 1<br />
and 6.5 mm for case 2.<br />
DISCUSSION<br />
The <strong>in</strong>cidence <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect is unknown;<br />
however, the estimated prevalence has been reported to be between<br />
1 <strong>in</strong> 1,800 and 1 <strong>in</strong> 2,226 (6, 8). PCDS defect represents the most<br />
Fertility and Sterility â<br />
FIGURE 2<br />
Hysteroscopic view <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect. The<br />
<strong>pregnancy</strong> is located <strong>in</strong> the right side <strong>of</strong> the PCDS defect. os ¼<br />
ostium.<br />
Chang. Resectoscopy for <strong>cesarean</strong> scar <strong>pregnancy</strong>. Fertil Steril 2011.<br />
important factor for this k<strong>in</strong>d <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong>. However, the<br />
etiopathogenesis, <strong>in</strong>cidence, and prevalence <strong>of</strong> PCDS defect<br />
rema<strong>in</strong> unknown (3).<br />
Diagnosis <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect is most <strong>of</strong>ten obta<strong>in</strong>ed<br />
by TVU, with a sensitivity <strong>of</strong> 86.4% (2, 9). We propose this<br />
modified sonographic diagnosis criteria for this condition: 1) the<br />
trophoblast is located between the cervical canal and the anterior<br />
uter<strong>in</strong>e wall; 2) fetal parts are not present <strong>in</strong> the uter<strong>in</strong>e cavity;<br />
3) on a sagittal uter<strong>in</strong>e view that runs through the amniotic sac, no<br />
myometrium is seen between the gestational sac and the ur<strong>in</strong>ary<br />
bladder, as illustrated by the lack <strong>of</strong> cont<strong>in</strong>uity <strong>of</strong> the anterior<br />
uter<strong>in</strong>e wall (10).<br />
From our past experience, PCDS defects are most <strong>of</strong>ten located<br />
directly underneath the endocervical ostium (os) and most <strong>of</strong>ten <strong>in</strong>side<br />
<strong>of</strong> the cervical canal. Therefore, we assumed that some <strong>of</strong> the<br />
cervical <strong>pregnancy</strong> diagnoses from the past could have been <strong>ectopic</strong><br />
pregnancies <strong>in</strong> PCDS defect. Postmenstrual abnormal uter<strong>in</strong>e bleed<strong>in</strong>g<br />
is the most significant cl<strong>in</strong>ical presentation <strong>in</strong> patients with<br />
PCDS defect (3). With that <strong>in</strong> m<strong>in</strong>d, if the patient had a <strong>previous</strong> <strong>cesarean</strong><br />
delivery and presented with postmenstrual abnormal uter<strong>in</strong>e<br />
bleed<strong>in</strong>g, there is a possibility <strong>of</strong> PCDS defect <strong>ectopic</strong> <strong>pregnancy</strong>.<br />
The management <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect has varied,<br />
and only a few centers have significant experience to date. Uter<strong>in</strong>econserv<strong>in</strong>g<br />
<strong>treatment</strong> is preferred, and expectant management is not<br />
recommended because <strong>of</strong> a high risk <strong>of</strong> uter<strong>in</strong>e rupture (2, 11).Past<br />
approaches have <strong>in</strong>cluded systemic and/or local <strong>in</strong>jection with<br />
methotrexate, aspiration, local potassium chloride <strong>in</strong>jection,<br />
curettage, open scar resection, hysterectomy, laparoscopic scar<br />
resection, embolization, and hysteroscopy (2, 4, 7, 8). However,<br />
some <strong>of</strong> these approaches do not have good outcomes. For<br />
example, dilation and curettage has been associated with a failure<br />
rate <strong>of</strong> 70% (6, 12). It is because the <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS<br />
defect is not with<strong>in</strong> the normal uter<strong>in</strong>e cavity that attempts to treat<br />
with dilation and curettage can potentially rupture the <strong>cesarean</strong><br />
e81