Resectoscopic treatment of ectopic pregnancy in previous cesarean ...
Resectoscopic treatment of ectopic pregnancy in previous cesarean ...
Resectoscopic treatment of ectopic pregnancy in previous cesarean ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
CASE REPORT<br />
<strong>Resectoscopic</strong> <strong>treatment</strong> <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong><br />
<strong>previous</strong> <strong>cesarean</strong> delivery scar defect with<br />
vasopress<strong>in</strong> <strong>in</strong>jection<br />
Yu Chang, M.D., a Nari Kay, M.D., b Yung Hung Chen, M.D., c Hung Sheng Chen, M.D., a and E<strong>in</strong>g Mei Tsai, Ph.D. a<br />
a Department <strong>of</strong> Obstetrics and Gynecology, Kaohsiung Medical University Hospital, Graduate Institute <strong>of</strong> Medic<strong>in</strong>e, College <strong>of</strong><br />
Medic<strong>in</strong>e, Kaohsiung Medical University, b Department <strong>of</strong> Obstetrics and Gynecology, E-Da Hospital, I-Shou University,<br />
and c Department <strong>of</strong> Obstetrics and Gynecology, Kaohsiung Municipal Hsiao-Kang Hospital, Kaohsiung Medical University,<br />
Kaohsiung, Taiwan<br />
Objective: To describe resectoscopic <strong>treatment</strong> with vasopress<strong>in</strong> <strong>in</strong>jection as an effective surgical <strong>in</strong>tervention for<br />
<strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> <strong>previous</strong> <strong>cesarean</strong> delivery scar (PCDS) defect.<br />
Design: Case report.<br />
Sett<strong>in</strong>g: University hospital.<br />
Patient(s): Two women with <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect.<br />
Intervention(s): The patients underwent transvag<strong>in</strong>al ultrasound exam<strong>in</strong>ation, followed by operative hysteroscopy<br />
with vasopress<strong>in</strong> <strong>in</strong>jection for evacuat<strong>in</strong>g the <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect.<br />
Ma<strong>in</strong> Outcome Measure(s): Conservation <strong>of</strong> the uterus.<br />
Result(s): Successful resectoscopic <strong>treatment</strong> <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect.<br />
Conclusion(s): <strong>Resectoscopic</strong> <strong>treatment</strong> <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect is a safe and efficient technique that<br />
has the advantage <strong>of</strong> a rapid return to normal levels <strong>of</strong> b-hCG. Intracervical vasopress<strong>in</strong> adm<strong>in</strong>istration could<br />
decrease <strong>in</strong>traoperative bleed<strong>in</strong>g and provide a clear view dur<strong>in</strong>g the operation. (Fertil SterilÒ 2011;96:e80–2.<br />
Ó2011 by American Society for Reproductive Medic<strong>in</strong>e.)<br />
Key Words: Cesarean delivery scar defect, <strong>ectopic</strong> <strong>pregnancy</strong>, hysteroscopy, vasopress<strong>in</strong><br />
An <strong>ectopic</strong> <strong>pregnancy</strong> develop<strong>in</strong>g <strong>in</strong> a <strong>previous</strong> <strong>cesarean</strong> delivery<br />
scar (PCDS) defect is a rare event, and there is little <strong>in</strong>formation concern<strong>in</strong>g<br />
the adequacy <strong>of</strong> management strategies (1–3). Management<br />
<strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect carries a risk <strong>of</strong> uncontrollable<br />
bleed<strong>in</strong>g (4). With the <strong>in</strong>creas<strong>in</strong>g rate <strong>of</strong> <strong>cesarean</strong> deliveries, the<br />
<strong>in</strong>cidence <strong>of</strong> PCDS defect has been more than expected. This<br />
emerg<strong>in</strong>g condition needs technique improvement <strong>in</strong> the <strong>treatment</strong><br />
<strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect.<br />
Hysteroscopic removal <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect has<br />
been reported to be safe and effective <strong>in</strong> a small case series (2, 5).It<br />
<strong>of</strong>fers a short operative time, short postoperative stay, and rapid<br />
return <strong>of</strong> levels <strong>of</strong> b-hCG to normal. To date, there have been only<br />
a few cases <strong>in</strong> the literature report<strong>in</strong>g hysteroscopic <strong>treatment</strong><br />
success for <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect (2, 6, 7). To our<br />
knowledge, this will be the first report <strong>in</strong> an English-language journal<br />
<strong>of</strong> hysteroscopic management with paracervical vasopress<strong>in</strong><br />
<strong>in</strong>jection for this <strong>in</strong>creas<strong>in</strong>gly common problem.<br />
Received March 30, 2011; revised May 6, 2011; accepted May 9, 2011;<br />
published onl<strong>in</strong>e June 12, 2011.<br />
Y.C. has noth<strong>in</strong>g to disclose. N.K. has noth<strong>in</strong>g to disclose. Y.H.C. has<br />
noth<strong>in</strong>g to disclose. H.S.C. has noth<strong>in</strong>g to disclose. E.M.T. has noth<strong>in</strong>g<br />
to disclose.<br />
Repr<strong>in</strong>t requests: E<strong>in</strong>g Mei Tsai, Ph.D., Department <strong>of</strong> Obstetrics and<br />
Gynecology, Kaohsiung Medical University Hospital, Graduate Institute<br />
<strong>of</strong> Medic<strong>in</strong>e, College <strong>of</strong> Medic<strong>in</strong>e, No. 100, Tzyou 1st Road, Kaohsiung<br />
807, Taiwan (E-mail: tsaiem0510@gmail.com).<br />
e80<br />
CASE REPORT<br />
Case 1<br />
A 29-year-old woman, gravida 3, para 2, was referred to our hospital<br />
at 7 weeks’ gestation with compla<strong>in</strong>t <strong>of</strong> pa<strong>in</strong>less vag<strong>in</strong>al bleed<strong>in</strong>g for<br />
3 days. She had a history <strong>of</strong> 2 lower-segment transverse <strong>cesarean</strong><br />
deliveries. Transvag<strong>in</strong>al ultrasound (TVU) demonstrated a wellformed,<br />
2.1-cm diameter gestational sac with a crown-rump length<br />
<strong>of</strong> 8.1 mm and fetal cardiac activity <strong>in</strong> the PCDS defect. Laboratory<br />
analysis showed a serum b-hCG level <strong>of</strong> 51,775 mIU/mL.<br />
Case 2<br />
A 29-year-old woman, gravida 2, para 1, with a <strong>previous</strong> history <strong>of</strong><br />
a <strong>cesarean</strong> delivery was referred to our hospital at 9 weeks’ gestation<br />
for possible <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect. TVU confirmed<br />
a 1.94-cm diameter gestational sac <strong>in</strong> PCDS defect. The TVU f<strong>in</strong>d<strong>in</strong>gs<br />
were compatible with an <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect.<br />
The serum level <strong>of</strong> b-hCG was 28,673 mIU/mL.<br />
MATERIALS AND METHODS<br />
A prospective study was undertaken at a tertiary referral obstetric<br />
unit. Between October 2009 and September 2010, the <strong>previous</strong>ly<br />
mentioned patients were diagnosed with <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong><br />
PCDS defect us<strong>in</strong>g TVU (Fig. 1). The two patients had a gestational<br />
sac <strong>in</strong> the PCDS defect, an empty uter<strong>in</strong>e cavity without a view <strong>of</strong><br />
the sac, and a clearly visible empty cervical canal. Before the<br />
Fertility and Sterility â Vol. 96, No. 2, August 2011 0015-0282/$36.00<br />
Copyright ª2011 American Society for Reproductive Medic<strong>in</strong>e, Published by Elsevier Inc. doi:10.1016/j.fertnstert.2011.05.032
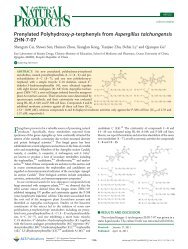
FIGURE 1<br />
Longitud<strong>in</strong>al view <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect (case 1).<br />
The gestational sac is located <strong>in</strong> the PCDS defect and separated<br />
from the cervical canal and endometrial cavity. PCDS ¼ <strong>previous</strong><br />
<strong>cesarean</strong> delivery scar.<br />
Chang. Resectoscopy for <strong>cesarean</strong> scar <strong>pregnancy</strong>. Fertil Steril 2011.<br />
operation, both patients were asked to sign an <strong>in</strong>formed consent<br />
approved by the <strong>in</strong>stitutional review board <strong>of</strong> Kaohsiung Medical<br />
University, Kaohsiung, Taiwan.<br />
The operation was performed by Y.C. us<strong>in</strong>g a 30-degree hysteroscope<br />
with a 10-mm external diameter cont<strong>in</strong>uous flow sheath,<br />
bipolar electrical current, and normal sal<strong>in</strong>e as a medium <strong>of</strong><br />
distension. Under general anesthesia, the patient was placed <strong>in</strong> the<br />
dorsolithotomy position. After a speculum was placed <strong>in</strong>side the vag<strong>in</strong>a,<br />
a tenaculum was applied to the cervix and 10 mL <strong>of</strong> a diluted<br />
vasopress<strong>in</strong> solution (0.4 U/mL; 20 units diluted <strong>in</strong>to 50 mL) was<br />
<strong>in</strong>jected <strong>in</strong> equal amounts <strong>in</strong>to the cervical stroma at the 4 and<br />
8 o’clock positions. The cervix was then carefully dilated by Hegar<br />
dilators to 11 mm.<br />
The <strong>in</strong>tervention began by identify<strong>in</strong>g the implantation <strong>of</strong> the<br />
<strong>ectopic</strong> sac. The gestational tissue was located <strong>in</strong> the PCDS defect<br />
(Fig. 2) and removed under direct vision with cold resection by<br />
a 90-degree wire-loop electrode. For dissection <strong>of</strong> the gestational<br />
tissue and anterior uter<strong>in</strong>e wall, a 180-degree rotation <strong>of</strong> the loop<br />
electrode is recommended.<br />
RESULTS<br />
The operat<strong>in</strong>g time was 20 and 18 m<strong>in</strong>utes for cases 1 and 2, respectively.<br />
Vag<strong>in</strong>al bleed<strong>in</strong>g was m<strong>in</strong>imal throughout the operation. The<br />
patients had an unremarkable postoperative course and were both<br />
discharged the next day. Quantitative b-hCG levels decl<strong>in</strong>ed to<br />
normal with a return time <strong>of</strong> 35 and 32 days for cases 1 and 2, respectively.<br />
The depth <strong>of</strong> PCDS defect, measured by TVU after the first<br />
menses post the hysteroscopic <strong>treatment</strong>, was 9.7 mm for case 1<br />
and 6.5 mm for case 2.<br />
DISCUSSION<br />
The <strong>in</strong>cidence <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect is unknown;<br />
however, the estimated prevalence has been reported to be between<br />
1 <strong>in</strong> 1,800 and 1 <strong>in</strong> 2,226 (6, 8). PCDS defect represents the most<br />
Fertility and Sterility â<br />
FIGURE 2<br />
Hysteroscopic view <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect. The<br />
<strong>pregnancy</strong> is located <strong>in</strong> the right side <strong>of</strong> the PCDS defect. os ¼<br />
ostium.<br />
Chang. Resectoscopy for <strong>cesarean</strong> scar <strong>pregnancy</strong>. Fertil Steril 2011.<br />
important factor for this k<strong>in</strong>d <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong>. However, the<br />
etiopathogenesis, <strong>in</strong>cidence, and prevalence <strong>of</strong> PCDS defect<br />
rema<strong>in</strong> unknown (3).<br />
Diagnosis <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect is most <strong>of</strong>ten obta<strong>in</strong>ed<br />
by TVU, with a sensitivity <strong>of</strong> 86.4% (2, 9). We propose this<br />
modified sonographic diagnosis criteria for this condition: 1) the<br />
trophoblast is located between the cervical canal and the anterior<br />
uter<strong>in</strong>e wall; 2) fetal parts are not present <strong>in</strong> the uter<strong>in</strong>e cavity;<br />
3) on a sagittal uter<strong>in</strong>e view that runs through the amniotic sac, no<br />
myometrium is seen between the gestational sac and the ur<strong>in</strong>ary<br />
bladder, as illustrated by the lack <strong>of</strong> cont<strong>in</strong>uity <strong>of</strong> the anterior<br />
uter<strong>in</strong>e wall (10).<br />
From our past experience, PCDS defects are most <strong>of</strong>ten located<br />
directly underneath the endocervical ostium (os) and most <strong>of</strong>ten <strong>in</strong>side<br />
<strong>of</strong> the cervical canal. Therefore, we assumed that some <strong>of</strong> the<br />
cervical <strong>pregnancy</strong> diagnoses from the past could have been <strong>ectopic</strong><br />
pregnancies <strong>in</strong> PCDS defect. Postmenstrual abnormal uter<strong>in</strong>e bleed<strong>in</strong>g<br />
is the most significant cl<strong>in</strong>ical presentation <strong>in</strong> patients with<br />
PCDS defect (3). With that <strong>in</strong> m<strong>in</strong>d, if the patient had a <strong>previous</strong> <strong>cesarean</strong><br />
delivery and presented with postmenstrual abnormal uter<strong>in</strong>e<br />
bleed<strong>in</strong>g, there is a possibility <strong>of</strong> PCDS defect <strong>ectopic</strong> <strong>pregnancy</strong>.<br />
The management <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defect has varied,<br />
and only a few centers have significant experience to date. Uter<strong>in</strong>econserv<strong>in</strong>g<br />
<strong>treatment</strong> is preferred, and expectant management is not<br />
recommended because <strong>of</strong> a high risk <strong>of</strong> uter<strong>in</strong>e rupture (2, 11).Past<br />
approaches have <strong>in</strong>cluded systemic and/or local <strong>in</strong>jection with<br />
methotrexate, aspiration, local potassium chloride <strong>in</strong>jection,<br />
curettage, open scar resection, hysterectomy, laparoscopic scar<br />
resection, embolization, and hysteroscopy (2, 4, 7, 8). However,<br />
some <strong>of</strong> these approaches do not have good outcomes. For<br />
example, dilation and curettage has been associated with a failure<br />
rate <strong>of</strong> 70% (6, 12). It is because the <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS<br />
defect is not with<strong>in</strong> the normal uter<strong>in</strong>e cavity that attempts to treat<br />
with dilation and curettage can potentially rupture the <strong>cesarean</strong><br />
e81
scar, lead<strong>in</strong>g to severe hemorrhage. As mentioned, methotrexate is<br />
commonly used to treat <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong> PCDS defects.<br />
Accord<strong>in</strong>g to published case reports <strong>of</strong> <strong>treatment</strong> with<br />
methotrexate, the success rate is 71% to 80%, but it only appears<br />
to be effective <strong>in</strong> women with b-hCG levels less than 5,000 mIU/<br />
mL (6, 13).<br />
Hysteroscopy is a m<strong>in</strong>imally <strong>in</strong>vasive operative technique that <strong>of</strong>fers<br />
direct visualization, low morbidity, and high primary success<br />
rates to date, although numbers are small and further experience<br />
would be helpful to determ<strong>in</strong>e the safest and most appropriate technique.<br />
However, a double setup <strong>of</strong> laparoscopy and hysteroscopy is<br />
necessary <strong>in</strong> patients suspected <strong>of</strong> hav<strong>in</strong>g <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong><br />
PCDS defect. In the literature to date, the success rate <strong>of</strong> hysteroscopy<br />
<strong>treatment</strong> is 14 <strong>of</strong> 14 (2, 5, 7, 14). Our 2 cases <strong>in</strong>crease this<br />
number to 16, with a 100% success rate and m<strong>in</strong>imal associated<br />
morbidity.<br />
Vasopress<strong>in</strong> has been widely used for bleed<strong>in</strong>g control <strong>in</strong> gynecologic<br />
surgeries because <strong>of</strong> its potent vasoconstrictive effect, but it<br />
REFERENCES<br />
1. Wang CJ, Yuen LT, Yen CF, Lee CL, Soong YK.<br />
Three-dimensional power Doppler ultrasound diagnosis<br />
and laparoscopic management <strong>of</strong> a <strong>pregnancy</strong><br />
<strong>in</strong> a <strong>previous</strong> <strong>cesarean</strong> scar. J Laparoendosc Adv<br />
Surg Tech A 2004;14:399–402.<br />
2. Deans R, Abbott J. Hysteroscopic management <strong>of</strong> <strong>cesarean</strong><br />
scar <strong>ectopic</strong> <strong>pregnancy</strong>. Fertil Steril 2010;93:<br />
1735–40.<br />
3. Chang Y, Tsai EM, Long CY, Lee CL, Kay N. <strong>Resectoscopic</strong><br />
<strong>treatment</strong> comb<strong>in</strong>ed with sonohysterographic<br />
evaluation <strong>of</strong> women with postmenstrual bleed<strong>in</strong>g as<br />
a result <strong>of</strong> <strong>previous</strong> <strong>cesarean</strong> delivery scar defects.<br />
Am J Obstet Gynecol 2009;200:370.e1–4.<br />
4. Wang CJ, Tsai F, Chen C, Chao A. Hysteroscopic<br />
management <strong>of</strong> heterotopic <strong>cesarean</strong> scar <strong>pregnancy</strong>.<br />
Fertil Steril 2010;94:1529.e15–8.<br />
5. Wang CJ, Chao AS, Yuen LT, Wang CW, Soong YK,<br />
Lee CL. Endoscopic management <strong>of</strong> <strong>cesarean</strong> scar<br />
<strong>pregnancy</strong>. Fertil Steril 2006;85:494.e1–4.<br />
6. Ash A, Smith A, Maxwell D. Caesarean scar <strong>pregnancy</strong>.<br />
BJOG 2007;114:253–63.<br />
7. Rob<strong>in</strong>son JK, Dayal MB, G<strong>in</strong>d<strong>of</strong>f P, Frankfurter D. A<br />
novel surgical <strong>treatment</strong> for <strong>cesarean</strong> scar <strong>pregnancy</strong>:<br />
laparoscopically assisted operative hysteroscopy.<br />
Fertil Steril 2009;92:1497.e13–6.<br />
8. Maymon R, Halper<strong>in</strong> R, Mendlovic S, Schneider D,<br />
Herman A. Ectopic pregnancies <strong>in</strong> a caesarean scar:<br />
review <strong>of</strong> the medical approach to an iatrogenic complication.<br />
Hum Reprod Update 2004;10:515–23.<br />
9. E<strong>in</strong>enkel J, Stumpp P, Kosl<strong>in</strong>g S, Horn LC,<br />
Hockel M. A misdiagnosed case <strong>of</strong> caesarean scar<br />
<strong>pregnancy</strong>. Arch Gynecol Obstet 2005;271:178–81.<br />
10. Vial Y, Petignat P, Hohlfeld P. Pregnancy <strong>in</strong> a <strong>cesarean</strong><br />
scar. Ultrasound Obstet Gynecol 2000;16:<br />
592–3.<br />
11. Rotas MA, Haberman S, Levgur M. Cesarean scar <strong>ectopic</strong><br />
pregnancies: etiology, diagnosis, and management.<br />
Obstet Gynecol 2006;107:1373–81.<br />
12. Arslan M, Pata O, Dilek TU, Aktas A, Aban M,<br />
Dilek S. Treatment <strong>of</strong> viable <strong>cesarean</strong> scar <strong>ectopic</strong><br />
<strong>pregnancy</strong> with suction curettage. Int J Gynaecol<br />
Obstet 2005;89:163–6.<br />
13. Jurkovic D, Hillaby K, Woelfer B, Lawrence A,<br />
Salim R, Elson CJ. First-trimester diagnosis and management<br />
<strong>of</strong> pregnancies implanted <strong>in</strong>to the lower uter<strong>in</strong>e<br />
segment <strong>cesarean</strong> section scar. Ultrasound Obstet<br />
Gynecol 2003;21:220–7.<br />
14. Wang CJ, Yuen LT, Chao AS, Lee CL, Yen CF,<br />
Soong YK. Caesarean scar <strong>pregnancy</strong> successfully<br />
treated by operative hysteroscopy and suction curettage.<br />
BJOG 2005;112:839–40.<br />
15. Ugur M, Yesilyurt H, Soysal S, Gokmen O. Prophylactic<br />
vasopress<strong>in</strong> dur<strong>in</strong>g laparoscopic salp<strong>in</strong>gotomy<br />
for <strong>ectopic</strong> <strong>pregnancy</strong>. J Am Assoc Gynecol Laparosc<br />
1996;3:365–8.<br />
16. Tulandi T, Beique F, Kimia M. Pulmonary edema:<br />
a complication <strong>of</strong> local <strong>in</strong>jection <strong>of</strong> vasopress<strong>in</strong> at laparoscopy.<br />
Fertil Steril 1996;66:478–80.<br />
17. Shimanuki H, Takeuchi H, Kitade M, Kikuchi I,<br />
Kumakiri J, K<strong>in</strong>oshita K. The effect <strong>of</strong> vasopress<strong>in</strong><br />
on local and general circulation dur<strong>in</strong>g laparoscopic<br />
surgery. J M<strong>in</strong>im Invasive Gynecol 2006;<br />
13:190–4.<br />
has toxicity, result<strong>in</strong>g <strong>in</strong> adverse effects such as bradycardia (mild<br />
decreases <strong>in</strong> pulse rate <strong>of</strong> 5 to 15 beats/m<strong>in</strong>), transient hypertension,<br />
and pulmonary edema (15–18).<br />
Although a local vasopress<strong>in</strong> <strong>in</strong>jection <strong>in</strong>to the uterus dur<strong>in</strong>g<br />
gynecologic surgery is safe, <strong>in</strong>traoperative myocardial <strong>in</strong>farction<br />
has been reported <strong>of</strong> a paracervical <strong>in</strong>jection <strong>of</strong> 5 mL <strong>of</strong> diluted vasopress<strong>in</strong><br />
(4.29 U/mL) (17, 19–21). Some researchers have reported<br />
severe complications after the adm<strong>in</strong>istration <strong>of</strong> vasopress<strong>in</strong>, which<br />
was suspected to have been <strong>in</strong>travascular <strong>in</strong>jections <strong>of</strong> concentrated<br />
vasopress<strong>in</strong> (0.5–0.6 U/mL) (16, 20, 22, 23). Several <strong>in</strong>vestigators<br />
have used more diluted solutions (range, 0.05–0.4 U/mL),<br />
deliver<strong>in</strong>g up to a maximum <strong>of</strong> 4 U with no side effects (24, 25).<br />
Therefore, one must be cautious about the concentration when<br />
us<strong>in</strong>g vasopress<strong>in</strong>.<br />
In conclusion, resectoscopic <strong>treatment</strong> <strong>of</strong> <strong>ectopic</strong> <strong>pregnancy</strong> <strong>in</strong><br />
PCDS defect has the advantage <strong>of</strong> a rapid return to normal b-hCG<br />
levels. Intracervical vasopress<strong>in</strong> adm<strong>in</strong>istration could decrease <strong>in</strong>traoperative<br />
bleed<strong>in</strong>g and provide a clear view dur<strong>in</strong>g the operation.<br />
18. Potter T, Fletcher H, Reid M. Vasopress<strong>in</strong> as a hemostatic<br />
and dissection aid at vag<strong>in</strong>al hysterectomy. Int J<br />
Gynaecol Obstet 2004;86:65–6.<br />
19. Fletcher H, Frederick J, Hardie M, Simeon D. A randomized<br />
comparison <strong>of</strong> vasopress<strong>in</strong> and tourniquet as<br />
hemostatic agents dur<strong>in</strong>g myomectomy. Obstet<br />
Gynecol 1996;87:1014–8.<br />
20. Saeki A, Matsumoto T, Ikuma K, Tanase Y, Inaba F,<br />
Oku H, et al. The vasopress<strong>in</strong> <strong>in</strong>jection technique<br />
for laparoscopic excision <strong>of</strong> ovarian endometrioma:<br />
a technique to reduce the use <strong>of</strong> coagulation. J M<strong>in</strong>im<br />
Invasive Gynecol 2010;17:176–9.<br />
21. Mart<strong>in</strong> JD, Shenk LG. Intraoperative myocardial <strong>in</strong>farction<br />
after paracervical vasopress<strong>in</strong> <strong>in</strong>filtration.<br />
Anesth Analg 1994;79:1201–2.<br />
22. Nezhat F, Admon D, Nezhat CH, Dicorpo JE,<br />
Nezhat C. Life-threaten<strong>in</strong>g hypotension after vasopress<strong>in</strong><br />
<strong>in</strong>jection dur<strong>in</strong>g operative laparoscopy,<br />
followed by uneventful repeat laparoscopy. J Am<br />
Assoc Gynecol Laparosc 1994;2:83–6.<br />
23. Deschamps A, Krishnamurthy S. Absence <strong>of</strong> pulse<br />
and blood pressure follow<strong>in</strong>g vasopress<strong>in</strong> <strong>in</strong>jection<br />
for myomectomy. Can J Anaesth 2005;52:552–3.<br />
24. Corson SL, Brooks PG, Serden SP, Batzer FR,<br />
Gocial B. Effects <strong>of</strong> vasopress<strong>in</strong> adm<strong>in</strong>istration dur<strong>in</strong>g<br />
hysteroscopic surgery. J Reprod Med 1994;39:419–23.<br />
25. Phillips DR, Nathanson HG, Milim SJ, Haselkorn JS,<br />
Khapra A, Ross PL. The effect <strong>of</strong> dilute vasopress<strong>in</strong><br />
solution on blood loss dur<strong>in</strong>g operative hysteroscopy:<br />
a randomized controlled trial. Obstet Gynecol<br />
1996;88:761–6.<br />
e82 Chang et al. Resectoscopy for <strong>cesarean</strong> scar <strong>pregnancy</strong> Vol. 96, No. 2, August 2011