ICCBH 22 Congress Review
Welcome to the ICCBH 2022 congress review. The 10th International Conference on Children’s Bone Health took place in Dublin from 2–5 July 2022 with attendees from around the globe, both in person and online.
Welcome to the ICCBH 2022 congress review.
The 10th International Conference on Children’s Bone Health took place in Dublin from 2–5 July 2022 with attendees from around the globe, both in person and online.

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
ACHONDROPLASIA.EXPERT<br />
CONGRESS REVIEWS<br />
<strong>ICCBH</strong> 20<strong>22</strong><br />
Welcome to the <strong>ICCBH</strong> 20<strong>22</strong> congress review.<br />
The 10th International Conference on Children’s Bone Health<br />
took place in Dublin from 2–5 July 20<strong>22</strong>. The meeting brought<br />
together scientists, clinicians, and allied health professionals<br />
from a variety of disciplines to gain a better understanding of<br />
the growing skeleton in health and disease, with leading experts<br />
delivering new insights into both molecular mechanisms and a<br />
range of clinical aspects, from bone physiopathology to treatment.<br />
As always, it is encouraging to see groups sharing posters<br />
and oral communications on the natural history and treatment<br />
of achondroplasia, which hopefully will translate into greater<br />
awareness and understanding of the condition.<br />
Tawfeg Ben-Omran, Senior Consultant and Division Chief<br />
Genetics and Genomic Medicine, Sidra Medicine, Qatar<br />
NATURAL HISTORY<br />
Associations between<br />
height, HRQoL and<br />
functional independence<br />
READ MORE ON PAGE 3<br />
EMERGING THERAPIES<br />
IN ACHONDROPLASIA<br />
New clinical data<br />
for vosoritide and<br />
TransCon CNP<br />
TURN TO PAGE 7<br />
MORE<br />
INSIDE<br />
Bone development PAGE 2<br />
Optimising care for bone diseases PAGE 11<br />
Considering fracture risk PAGE 12<br />
Expanding knowledge in skeletal dysplasia PAGE 14<br />
Novel therapies in skeletal dysplasia PAGE 15<br />
Meet the expert PAGE 17<br />
SUPPORTING INDEPENDENCE<br />
IN ACHONDROPLASIA<br />
A look at how to support<br />
independence in<br />
school-age children, with a<br />
particular focus on toileting<br />
FIND OUT MORE ON PAGE 9<br />
Oral communication abstracts, posters, and presentation can be found in full here<br />
This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are<br />
asked to report any suspected adverse reactions. Treatments mentioned in this document may not be approved for use in your country. Please consult<br />
local licensing authorities for further information.<br />
Some links in this document are “external links” to websites over which BioMarin has no control and for which BioMarin assumes no responsibility.<br />
When visitors choose to follow a link to any external website, they are subject to the cookie, privacy and legal policies of the external website.<br />
Compliance with applicable data protection and accessibility requirements of external websites linked to from this website falls outside the control<br />
of BioMarin and is the explicit responsibility of the external website.<br />
Achondroplasia.expert is organised and funded by BioMarin. The latest API be found on the Achondroplasia.expert website, under the Prescribing<br />
Information tab. Or click here.<br />
© 20<strong>22</strong> BioMarin International Ltd.<br />
All Rights Reserved. EU-VOX-00685 November 20<strong>22</strong><br />
1
Achondroplasia.expert <strong>Congress</strong> <strong>Review</strong>s: <strong>ICCBH</strong> 20<strong>22</strong><br />
BONE DEVELOPMENT<br />
Skeletal development and growth were covered in a selection of posters.<br />
Here we summarise a study measuring skeletal robustness, and the<br />
use of biomarkers to measure small increments of growth in children<br />
with achondroplasia.<br />
included correlation of biomarkers<br />
with the annualised growth rate, AGV,<br />
and within-participant CXM variability.<br />
No significant association was found between<br />
CXM concentrations and the annualized<br />
change from baseline in height Z-score;<br />
however, there were significant associations<br />
between CXM concentrations and both<br />
AGV for height and change from baseline<br />
for sitting height. High within-participant<br />
CXM variability was observed, comprising<br />
approximately 57% of the total variability.<br />
Significant associations were also detected<br />
between CTX1 concentrations and the change<br />
from baseline for sitting height, and between<br />
PRO-C2 and the AGV for height. [P131]<br />
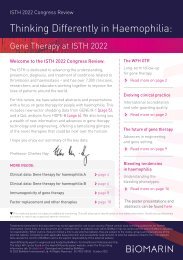
Yingling et al. identified variation in skeletal<br />
robustness as an important determinant of<br />
bone strength in youth and young adults in<br />
the Iowa Bone Development Study. Robusticity<br />
reflects the relationship between periosteal<br />
expansion relative to longitudinal growth,<br />
and is a marker of bone strength. This may<br />
be detrimental during training and with<br />
ageing, but few studies have investigated the<br />
impact of bone strength and functionality on<br />
robustness during puberty and at maturity.<br />
This study used pQCT measures of bone<br />
strength of the tibial diaphysis for males and<br />
females at age 11 and 25 from the Iowa Bone<br />
Development Study. The results showed less<br />
robust bones were weaker, and more robust<br />
Change in quadrant from young to maturity<br />
Percentage %<br />
100<br />
80<br />
60<br />
40<br />
20<br />
0<br />
Same<br />
Lower<br />
Male<br />
Improvement<br />
Green–Same<br />
Red–Same<br />
bones were stronger. Furthermore, it was<br />
shown that changes in robusticity and bone<br />
strength can occur from puberty to maturity,<br />
although the majority of individuals did<br />
not move quadrants – instead tending<br />
to stay weaker or stronger for their size.<br />
The authors concluded that one factor<br />
affecting these changes may be lifestyle<br />
choices, such as exercise. [P3]<br />
Ljungberg et al. assessed different circulating<br />
biomarkers related to bone growth, including<br />
collagen fragments as surrogate markers<br />
for growth in 23 children. The biomarkers<br />
analysed were CXM, N- terminal proCNP,<br />
CTX1, P1NP, and PRO-C2. Endpoints<br />
Percentage %<br />
80<br />
60<br />
40<br />
20<br />
0<br />
Same<br />
Lower<br />
Female<br />
Improvement<br />
Green–Same<br />
Red–Same<br />
Yingling et al. [P3]<br />
ACHONDROPLASIA NATURAL HISTORY<br />
With new treatments becoming available for achondroplasia, work continues<br />
to understand the natural history – providing knowledge of complications,<br />
manifestations, and the physical and mental burden across the lifespan.<br />
Irving et al. shared baseline characteristics<br />
from ACHieve – a multicentre, longitudinal,<br />
observational study in children with<br />
achondroplasia from birth to age 8, at<br />
enrolment, from North America, Europe,<br />
and Oceania. The aim is to collect information<br />
on complication onset and progression,<br />
detailed anthropometry including longitudinal<br />
height velocity, and changes in body<br />
proportionality. As of December 2021,<br />
154 children have been enrolled. The mean<br />
age at enrolment was 4 years, with 26%<br />
under 2 years. Anthropometrics are reported<br />
by subgroups of age at enrolment, and the<br />
mean height SDS in the various age groups<br />
at baseline confirms progressive shortness<br />
relative to peers without achondroplasia.<br />
Likewise, the upper-to-lower body segment<br />
ratios suggest that body proportions remain<br />
disproportionate with age in children with<br />
achondroplasia. ACHieve provides important<br />
observational data which will serve as an<br />
important reference for future intervention<br />
trials targeting the underlying pathology,<br />
and will continue to collect data on the<br />
timing, frequency, and characteristics<br />
of growth patterns, body proportionality,<br />
and complications in children with<br />
achondroplasia. [P147]<br />
Irving et al. also reported associations<br />
between height and HRQoL and functional<br />
independence in an exploratory analysis in<br />
121 children with achondroplasia enrolled in<br />
the vosoritide Phase 3 trial. Height Z-scores<br />
were assessed every 3 months, and HRQoL<br />
assessed every 6 months using the PedsQL,<br />
QoLISSY, and WeeFIM questionnaires. For<br />
all instruments, mean scores were generally<br />
lower in subjects with greater height deficit<br />
(at least –6 SDS) compared to taller subjects<br />
with height Z-score greater than −4 SDS.<br />
Clear linear relationships between height<br />
Z-scores and several domain scores were<br />
observed, most notably in the PedsQL<br />
Physical domain, the height-specific<br />
QoLISSY Physical domain, and the WeeFIM<br />
Self-care and Mobility domains. These data<br />
2 3
Achondroplasia.expert <strong>Congress</strong> <strong>Review</strong>s: <strong>ICCBH</strong> 20<strong>22</strong><br />
WeeFIM and height Z-score<br />
Mean (+/- SE) Score<br />
60<br />
55<br />
50<br />
45<br />
40<br />
35<br />
30<br />
0<br />
N:<br />
Self-care<br />
102 190 82<br />
187 102 82<br />
confirm that height deficit in achondroplasia<br />
impacts HRQoL and function, and suggest<br />
that therapies with the potential to reduce<br />
height deficit may also improve HRQoL and<br />
functional independence. [P140]<br />
Noori et al. conducted a systematic review<br />
on the clinical burden of achondroplasia and<br />
management of achondroplasia-associated<br />
complications. The aim was to identify studies<br />
published in English between 2011–2021<br />
Mobility<br />
Cognitive<br />
WeeFIM Caregiver-reported<br />
187 190<br />
102 187 190 82<br />
≤ -6 > -6 to ≤ -5 > -5 to ≤ -4 > -4<br />
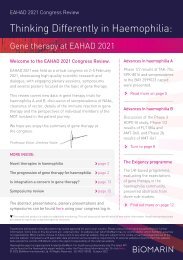
Clinical trials of compounds under investigation for achondroplasia<br />
Irving et al. [P140]<br />
reporting symptoms or complications<br />
associated with achondroplasia, as well<br />
as management options.<br />
Of 4,337 records identified, 79 were selected.<br />
Among children who underwent imaging<br />
studies, cervicomedullary compression or<br />
stenosis of the craniocervical junction was<br />
prevalent in 24–94%. Hydrocephalus was<br />
present in 3–41% of cases and thoracolumbar<br />
spinal stenosis in <strong>22</strong>–42%. High rates of<br />
Investigational therapies Mechanism of action Trial status Study Number<br />
Vosoritide*<br />
TransCon CNP<br />
Recifercept<br />
lnfigratinib<br />
*Approved by FDA and EMA in 2021<br />
Analog of C-type<br />
Natriuretic Peptide<br />
Long-acting prodrug of<br />
C-type Natriuretic Peptide<br />
Soluble recombinant human fibroblast<br />
growth factor receptor 3 decoy<br />
Fibroblast growth factor receptor<br />
1–3 typrosine kinase inhibitor<br />
Phase 2 and phase 3 trials<br />
completed; extension<br />
studies ongoing<br />
Phase 2 trials ongoing<br />
Phase 2 trials ongoing<br />
Phase 2 trial and its<br />
extension study trial<br />
NCT03989947;<br />
NCT03424018<br />
NCT04085523;<br />
NCT05246033<br />
NCT0463815;<br />
NCT05116046<br />
NCT04265651;<br />
NCT05145010<br />
Nooti et al. [P121]<br />
sleep disordered breathing were reported,<br />
including OSA in up to 80%. Ear infections<br />
were a recurrent complication, with hearing<br />
impairment evident in up to 75%. Between<br />
19–63% underwent cervicomedullary<br />
decompression, with neurologic improvement<br />
in 50–100% of cases. Management of spinal<br />
stenosis through decompressive surgery was<br />
more commonly performed in adolescents<br />
and adults, and was associated with a high<br />
rate of intraoperative complications. Upper<br />
airway surgery usually improved respiratory<br />
indices, but few adolescents and adults<br />
had complete resolution of symptoms.<br />
According to one multinational crosssectional<br />
study, orthopaedic procedures<br />
were among the most common surgeries<br />
in people with achondroplasia, reported in<br />
46%. The authors concluded that individuals<br />
with achondroplasia require ongoing<br />
medical surveillance and management<br />
of complications that diminish functional<br />
capacity, reduce quality of life, and can be<br />
potentially life-threatening. [P121]<br />
The same group presented a second poster<br />
detailing a second set of findings from<br />
their systematic literature review, focusing<br />
on interventional and real-world studies<br />
reporting efficacy or effectiveness, safety, or<br />
quality of life outcomes for limb-lengthening<br />
or pharmacologic treatment for patients<br />
with achondroplasia. Smith et al. selected<br />
4 interventional – 3 for vosoritide, and<br />
1 examining the safety of meclizine. Phase 3<br />
data show vosoritide significantly improves<br />
mean AGV and height Z-scores compared<br />
to placebo, but with no significant changes<br />
in upper-to-lower body segment ratio or<br />
mean standing height. An additional 29 realworld<br />
studies examined limb-lengthening<br />
and/or growth hormone treatment. Limblengthening<br />
procedures effectively increased<br />
limb length, with a mean gain of 7.1–10.2,<br />
5.6–9.5, and 6–14.7 cm, for the femur, tibia,<br />
and humerus, respectively. The procedures<br />
also improved body proportionality, quality<br />
of life, and daily functionality, but were<br />
associated with a high complication rate<br />
and required long recovery periods. Growth<br />
hormone demonstrated inconsistent efficacy<br />
in recent studies. These findings suggest that<br />
patients with achondroplasia have limited<br />
treatment options that increase height<br />
and improve body proportionality, thereby<br />
augmenting quality of life. [P120]<br />
Watt et al. presented 2-year results of a<br />
study offering annual hearing screening<br />
in children with achondroplasia. A new<br />
screening programme in Glasgow aims<br />
to detect new otological problems, and to<br />
estimate the prevalence of hearing loss, OSA,<br />
and frequency of interventions in children<br />
with achondroplasia in Scotland. To date,<br />
9 children have participated; the mean age<br />
was 10.6 years. First and second screening<br />
appointments had a pick-up rate of new<br />
problems of 0 and 11.1%, respectively.<br />
Overall, 67% of the children were previously<br />
known to the ENT or audiology departments.<br />
Due to challenges of small sample size and<br />
the impact of the COVID-19 pandemic, the<br />
scope was expanded to a cross-sectional<br />
review in a larger group of 26 children; here<br />
the prevalence of hearing loss was 46.2%<br />
with median age at detection of 3 years.<br />
The prevalence of OSA was 34.6%, and 38.5%<br />
and 34.6% of had undergone insertion of<br />
grommets or tonsillectomy, respectively.<br />
The authors concluded that the screening<br />
programme did not detect new hearing<br />
4 5
Achondroplasia.expert <strong>Congress</strong> <strong>Review</strong>s: <strong>ICCBH</strong> 20<strong>22</strong><br />
problems in children with achondroplasia<br />
in its initial years but did confirm a high<br />
prevalence of hearing loss and OSA compared<br />
to the general paediatric population without<br />
achondroplasia, however more data is<br />
required for robust recommendations.<br />
[P126]<br />
Rhoda et al. shared the results of an<br />
observational study of foetal foramen<br />
magnum and foramen magnum stenosis<br />
development in achondroplasia, looking for<br />
early evidence of complications in utero.<br />
Advances in novel therapies broaden the<br />
scope for patents with achondroplasia, and<br />
is theorised that earlier administration will<br />
optimise outcomes. Foetal development<br />
of the foramen magnum, thoracolumbar<br />
spine, and hippocampus in achondroplasia<br />
is not well understood. This study used MRI<br />
to visualise these structures in 6 foetuses<br />
with achondroplasia, and by generating 3D<br />
reconstructed images to derive a measurable<br />
dataset. A method was devised to orientate<br />
images into standard sagittal, coronal, and<br />
transverse planes, which helped to account<br />
for foetal movement. Results suggested<br />
the measurement system devised had an<br />
average inter-observer variability of 7.2%.<br />
Pre- and post-natal foramen magnum stenosis score<br />
After birth, all babies had post-natal MRI<br />
scans to detect foramen magnum stenosis;<br />
this was confirmed in 4 children, 3 of<br />
whom had been flagged by the radiologist<br />
on the pre-natal scans, and who went on<br />
to require decompression surgery. This<br />
dataset demonstrates that complications<br />
of achondroplasia initiate in the foetus, and<br />
will form a foundation upon which to study<br />
the early natural history. Further work using<br />
motion-corrected MRI to gather normative<br />
data in unaffected controls is needed, but<br />
expanding on this knowledge will provide<br />
tangible measures for the consideration of<br />
early interventional therapy, perhaps even<br />
in the pre-natal setting. [P2]<br />
Brett et al. also presented a poster on<br />
foramen magnum stenosis in infants with<br />
achondroplasia, investigating the natural<br />
history of cervicomedullary cord compression<br />
without signal change. The AFMS was<br />
developed to classify the severity of stenosis<br />
and inform appropriate neurosurgical<br />
management, and has been shown to<br />
have good observer reliability. At baseline,<br />
approximately half of infants demonstrate<br />
AFMS3/4. All children with AFMS4 are<br />
referred for neurosurgery, whilst well<br />
Pt ID Prenatal FMS score Post-natal FMS score Post-natal FMS score Surgical Intervention<br />
001 36 +6 AFMS0 4m AFMS1 17m AFMS1 N<br />
002 32 +4 AFMS0 4m AFMS2 10m AFMS2 N<br />
003 35 +2 AFMS1 5m 7m AFMS4 Y<br />
004 34 +5 AFMS1 2m AFMS4 Y<br />
005 34 +1 AFMS1 2m AFMS1 8m AFMS4 Y<br />
006 34 +1 AFMS0<br />
Rhoda et al. [P2]<br />
children with AFMS3 undergo repeat MRI<br />
after 12 months. As the natural history of<br />
children with AFMS3 is currently unclear,<br />
the objective of this study was to review<br />
follow-up MRI assessments of 16 infants<br />
initially classified as AFMS3 at two centres in<br />
the UK to define the evolution of this degree of<br />
stenosis. Follow-up MRI showed improvement<br />
in 37.5% to either AFMS1 or AFMS2; there<br />
was no change in 25%, and 37.5% progressed<br />
to AFMS4. Given that more than one-third of<br />
infant’s progress and require neurosurgical<br />
referral, the authors recommend a refinement<br />
of the screening approach to perform followup<br />
MRI at 6 and 12 months, which will help<br />
improve management in this at-risk cohort,<br />
and inform family counselling. [P128]<br />
EMERGING TREATMENT OPTIONS IN<br />
ACHONDROPLASIA<br />
Posters and Late Meeting presentations at the meeting shared data for both<br />
vosoritide and TransCNP in children and adolescents with achondroplasia,<br />
including early real-world experience from France and Germany.<br />
Irving et al. reported on growth velocity<br />
and pubertal milestones with vosoritide for<br />
achondroplasia, using data from the BMN<br />
111-202 and BMN 111-301 studies, and their<br />
ongoing extensions (111-205 and 111-302).<br />
Subjects continuing into the extensions<br />
had a median treatment exposure of 6.0<br />
and 2.4 years, respectively. Standing<br />
heights at each 6-month visit were used<br />
to assess growth and calculate AGV. Overall,<br />
82 subjects had data to assess onset of<br />
Tanner stage 2–5, and 149 to assess AGV for<br />
Tanner stage 1 or onset of Tanner stage 2–5.<br />
AFMS at follow-up MRI in infants classified<br />
as AFMS3 at baseline (n=16)<br />
AFMS1/2 AFMS3 AFMS4<br />
Brett et al. [P128]<br />
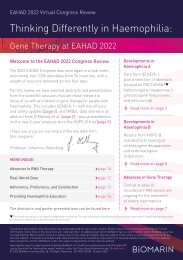
As expected, peak growth velocity occurred<br />
at Tanner 2 for females and Tanner 4 for<br />
males. The peak growth velocity on vosoritide<br />
was 5.81 and 6.36 cm/year for females and<br />
males, respectively – compared to 6.65 and<br />
7.66 cm/year in the general US population.<br />
In conclusion, vosoritide preserved the<br />
overall growth duration and the timing of<br />
pubertal milestones while increasing growth<br />
velocity. More data are required to determine<br />
whether the timing of pubertal development<br />
in children with achondroplasia treated with<br />
vosoritide follows that of average stature<br />
6 7
Achondroplasia.expert <strong>Congress</strong> <strong>Review</strong>s: <strong>ICCBH</strong> 20<strong>22</strong><br />
children, as well as to understand how the<br />
timing compares to that of untreated children<br />
with achondroplasia. Monitoring of these<br />
subjects will continue until they reach their<br />
final adult height in order to help better<br />
understand the potential impact of pubertal<br />
milestones in achondroplasia. [P139]<br />
Cormier-Daire et al. shared the early<br />
experience with vosoritide therapy in<br />
clinical practice, with data from over<br />
100 participants in France and Germany<br />
treated with vosoritide in the first 3–4 months<br />
of treatment availability. Children were<br />
aged 2–15 years, and received treatment<br />
for 0.5–4.0 months. Common practices<br />
essential for successful therapy initiation<br />
included establishing families and children’s<br />
readiness for treatment, customised<br />
information and training, readily available<br />
support from healthcare professionals,<br />
regular follow-up, a well-connected<br />
multidisciplinary team, and seamless<br />
logistics and storage arrangements for<br />
pharmacies and families. Additional<br />
support from nurses or other healthcare<br />
personnel at patients’ homes in the early<br />
days of home treatment was also useful.<br />
Appropriate infrastructure was required for<br />
prescription and treatment, as well as for<br />
completing baseline assessments such as<br />
anthropometrics, vital signs, radiographs,<br />
bone-markers, blood tests, and Tannerstaging.<br />
Common side effects for this group<br />
of patients in real-world practice included<br />
local reactions at the injection site, and<br />
transient hypotension. Common concerns<br />
from families and patients focused on<br />
AGV over 6-month intervals by Tanner stage in children treated with vosoritide in studies 202/205 and 301/302<br />
6-month interval<br />
Annualised Growth Velocity (cm/yr)<br />
15<br />
14<br />
13<br />
12<br />
11<br />
10<br />
9<br />
8<br />
7<br />
6<br />
5<br />
4<br />
3<br />
2<br />
1<br />
0<br />
-1<br />
I<br />
Female<br />
II III IV V<br />
Tanner Stage<br />
n 49 57 25 21 23 15 18 9 3 6<br />
Whiskers indicate 2.5th and 97.5th percentiles. Of note, the peak growth velocity in the general US population<br />
is 6.65 and 7.66 cm/year for females and males, respectively.<br />
Male<br />
Irving et al. [P139]<br />
pain and the daily burden of injections, as<br />
well as the duration of treatment needed,<br />
long-term effects and safety, and potential<br />
natural history changes after treatment.<br />
This early experience is essential for practice<br />
evaluation, and will help to develop standards<br />
and guidelines for patient care. [P138]<br />
TransCon CNP is an investigational prodrug<br />
of CNP in development for children with<br />
achondroplasia. McDonnell et al. reported<br />
baseline characteristics for the Phase 2<br />
ACcomplisH trial, which is evaluating<br />
the safety and efficacy of once-weekly<br />
TransCon CNP in 57 prepubertal children<br />
with achondroplasia. The primary efficacy<br />
endpoint evaluates AHV at 52 weeks, with<br />
baseline AHV calculated based on either<br />
medical history or a visit in the ACHieve<br />
natural history study – taken around<br />
12 months prior to randomisation. The<br />
mean age at enrolment was 5.9 years, and<br />
90% had been diagnosed prior to 6 months<br />
of age. At ACcomplisH baseline, 54.4%<br />
had sleep apnoea, 42.1% ear infections,<br />
17.5% foramen magnum stenosis, 15.8%<br />
kyphosis, and 15.8% reported nervous system<br />
disorders – very similar to those reported<br />
for the natural history in the published<br />
literature. The baseline characteristics as<br />
evaluated by different age groups show<br />
expected differences in baseline variables<br />
with expected variability in pre-treatment<br />
AHV across age-groups. The high percentage<br />
of early diagnoses indicates potential<br />
opportunity for early intervention. [P148]<br />
SUPPORTING INDEPENDENCE IN<br />
ACHONDROPLASIA<br />
Achondroplasia can affect an individual’s performance across a number of<br />
activities of daily living, including independence in toileting. This can have a<br />
knock-on effect on quality of life and self-esteem. Several posters presented<br />
at the meeting looked at how to support independence for children and young<br />
people with achondroplasia.<br />
Massey et al. used PEDI-CAT to explore the<br />
impact of achondroplasia on development<br />
in areas including responsibility, social and<br />
cognitive function, mobility, and daily activities.<br />
PEDI-CAT assessments were conducted<br />
with 25 parents through face-to-face and<br />
virtual consultations at one specialist clinic<br />
in the UK. Participant t-scores revealed<br />
–1 SDS below the normative mean population<br />
in the daily activities domain for young<br />
children (3–7 years), and –1.5 in those aged<br />
7–14 years. The mobility domain showed<br />
–2 SDS in younger children, and –3 SDS in the<br />
older group. Participants were within 0.5 SDS<br />
for the social, cognitive, and responsibility<br />
domains. Overall, the results showed a<br />
greater impact on functional performance<br />
relative to typical development for older versus<br />
8 9
Achondroplasia.expert <strong>Congress</strong> <strong>Review</strong>s: <strong>ICCBH</strong> 20<strong>22</strong><br />
younger children. These results highlight<br />
strengths of children and young people<br />
with achondroplasia, as well as confirming<br />
difficulties in mobility and daily activities.<br />
In clinical practice, this may mean that<br />
therapists see a decrease in functional ability<br />
in the areas of daily activities and mobility,<br />
but not necessarily in social, cognitive, and<br />
responsibility domains. The authors note that<br />
the disproportion and elbow contractures<br />
associated with achondroplasia contribute<br />
to the functional impact, and recommend<br />
occupational therapy interventions that use<br />
a strengths-based approach such as goaldirected<br />
training to help maximise a child’s<br />
performance across domains. Assessment of<br />
Impact of achondroplasia on key domains<br />
28%<br />
Daily Activities t-scores<br />
20%<br />
16%<br />
36%<br />
the domains captured through the PEDI-CAT<br />
will also have utility as a metric of response to<br />
treatment with new and investigational drugs.<br />
[P169]<br />
A poster from Johnson et al. considered<br />
whether children aged 7–12 years old with<br />
achondroplasia have appropriate adaptations<br />
required to support independence in toileting,<br />
using data from a single retrospective<br />
study in 24 children. Toileting is a complex<br />
multistep task and there may be many<br />
reasons for limitations in this area, such as<br />
short stature, and loss of full extension at the<br />
elbow and rhizomelia. The findings showed<br />
that 58% had environmental adaptations<br />
28%<br />
Mobility t-scores<br />
12%<br />
>250 below >150
Achondroplasia.expert <strong>Congress</strong> <strong>Review</strong>s: <strong>ICCBH</strong> 20<strong>22</strong><br />
advice/support and all found this to be helpful.<br />
Patients and families suggested offering the<br />
following services in the order of preference:<br />
hydrotherapy, family days, information<br />
sessions, a transition clinic, equipment advice,<br />
information leaflets, and wheelchair advice.<br />
In conclusion, multiple opinions from patients<br />
and their families were positive, suggesting<br />
the metabolic bone service is meeting current<br />
needs. This feedback will be used to plan how<br />
to develop the service further. [P152]<br />
The European Registries for Rare Bone and<br />
Mineral Conditions (EuRR-Bone), launched<br />
in April 2020, started with prospective<br />
data collection on the occurrence of rare<br />
bone and mineral diseases by using an<br />
electronic registry. To date, 40 centres from<br />
18 countries have reported over 800 cases,<br />
including 260 patients with bone and mineral<br />
conditions. The Core Registry – the second<br />
platform within EuRR-Bone – will gather a<br />
little more information, and is collecting a<br />
common dataset to support the goals of the<br />
European Reference Network for Rare Bone<br />
Diseases. In addition, four disease-specific<br />
modules on achondroplasia, osteogenesis<br />
imperfecta, rare hypophosphataemic<br />
disorders and fibrous dysplasia have been<br />
developed by expert working groups. The<br />
modules make it possible to introduce more<br />
detailed data, such as phenotype, genotype,<br />
biochemistry, and clinical science – as well<br />
as the opportunity to log follow-up data.<br />
Ertl et al. outlined how patients can access<br />
the platform, view their data and complete<br />
patient-reported outcomes. The ability to<br />
collect longitudinal patient- and clinicianreported<br />
outcomes gives the platform the<br />
functionality to study meaningful longterm<br />
clinical outcomes in a wide range of<br />
conditions across all ages. In addition, there<br />
is a committee which will analyse data for<br />
research purposes. [P158]<br />
CONSIDERING FRACTURE RISK<br />
Childhood cancer survivors are at risk of developing skeletal late effects,<br />
and fracture is also a risk in children across a variety of skeletal disorders<br />
treated with classic steroids, such as osteoporosis, Duchenne muscular<br />
dystrophy, or rheumatic diseases.<br />
Nicola Crabtree looked at promises and<br />
pitfalls in interpretation of paediatric<br />
vertebral fracture assessment. The<br />
identification of vertebral fractures in<br />
children is a critical component of the<br />
assessment of bone health, and may be<br />
common in children with osteoporosis due<br />
to both their underlying condition or its<br />
treatment, particularly with glucocorticoids.<br />
Vertebral fracture assessment is performed<br />
more often than plain lateral radio graphs.<br />
Several studies have demonstrated this to<br />
be at least as reliable as radiographs for<br />
identifying moderate and severe vertebral<br />
fractures. However, both techniques were<br />
equally poor when identifying mild vertebral<br />
fractures. Unfortunately, the lack of<br />
agreement when identifying mild vertebral<br />
fractures was also challenged when using<br />
semi- or fully automated techniques,<br />
where reader opinion is eliminated. The<br />
main difficulty lies in reliably distinguishing<br />
normal physiological or developmental<br />
morphological variability from fracture,<br />
which is further complicated by the lack of<br />
normative vertebral morphological data.<br />
However, despite these challenges, the<br />
most recent paediatric position statement<br />
from the International Society of Clinical<br />
Densitometry (2019) has endorsed the use<br />
of vertebral fracture assessment providing<br />
the reader has experience of paediatric<br />
vertebral fractures – and with the caveat that<br />
further imaging is required in cases where<br />
vertebral visualisation is limited, where a<br />
single Genant Grade 1 fracture is identified<br />
that would change management, or where<br />
the radiographic findings are not typical for<br />
an osteoporotic vertebral fracture. In such<br />
cases, either plain lateral radiography or<br />
whole-spine MRI is recommended. [IS10]<br />
Stefan Jackowski’s oral focused on the<br />
prevalence and severity of vertebral fracture<br />
in children with various disorders treated<br />
with classic or dissociative steroids. This<br />
descriptive study of children enrolled in the<br />
STOPP and VPB15 (vamorolone) research<br />
programs showed average daily steroid<br />
doses from highest to lowest (mg/kg/day in<br />
prednisone equivalents) of 0.47, 0.44, 0.37,<br />
and 0.30 for Duchenne muscular dystrophy,<br />
nephrotic syndrome, rheumatic disorders,<br />
and leukaemia, respectively. The proportion<br />
of children with at least one vertebral fracture<br />
was 13.6%, 10.3%, 8.3%, and 1.8% for<br />
leukaemia, Duchenne muscular dystrophy,<br />
rheumatic disorders, and nephrotic<br />
syndrome, respectively. Despite the longest<br />
average duration of vamorolone, and highest<br />
average daily dose, boys with Duchenne<br />
muscular dystrophy had the lowest average<br />
Spine Deformity Index – a measure of overall<br />
spine burden. Children with leukaemia had<br />
the lowest classic glucocorticoid exposure,<br />
yet the most severe osteoporotic phenotype –<br />
highlighting disease-specific factors beyond<br />
steroid exposure likely influenced<br />
the vertebral fracture burden. [OC17]<br />
Demi de Winter looked at risk and<br />
determinants of reduced bone mineral<br />
density and fractures in a Dutch cohort<br />
of 2,003 childhood cancer survivors (the<br />
DCCSS-LATER 2 study). BMD was measured<br />
at the lumbar spine, total body, and total<br />
hip, and fracture incidence compared with<br />
Swedish normative data. The SIR of any<br />
first fracture was 3.53 and 5.35 for male<br />
and female survivors, respectively. Vertebral<br />
fractures were prevalent in 13.3% of evaluable<br />
survivors. In the models for low or very<br />
low BMD, male sex, underweight, shorter<br />
follow-up time, total body irradiation, cranial<br />
irradiation, carboplatin dose ≥2,000 mg/m 2 ,<br />
cyclophosphamide equivalent dose<br />
≥8,000 g/m 2 , hypogonadism, growth<br />
hormone deficiency, hyperthyroidism,<br />
low physical activity, vitamin D or B12<br />
deficiency, and folic acid deficiency were<br />
statistically significant. Male sex, obesity,<br />
previous or current smoking, and very<br />
low lumbar spine BMD were significantly<br />
associated with fractures. The authors<br />
conclude that childhood cancer survivors are<br />
at increased risk of any fracture, but identify<br />
several modifiable risk factors for reduced<br />
BMD and vertebral fractures. [OC18]<br />
12 13
Achondroplasia.expert <strong>Congress</strong> <strong>Review</strong>s: <strong>ICCBH</strong> 20<strong>22</strong><br />
EXPANDING KNOWLEDGE IN<br />
SKELETAL DYSPLASIA<br />
Groups from around the world shared new information on genetic mutations<br />
contributing to the development of various skeletal dysplasias. Some of these<br />
may provide targets for future novel therapies.<br />
Juliana Marulanda presented insights into the<br />
dysregulation of the osteocyte transcriptome<br />
in a mouse model of Duchenne muscular<br />
dystrophy by the assessment of dysregulation<br />
of bone gene expression by comparing the<br />
transcriptome of the tibia diaphysis in growing<br />
mdx and wild-type mice. RNA sequencing<br />
revealed 13,231 actively expressed genes<br />
across both genotypes. Of these, 438 genes<br />
were differentially expressed in mdx mice<br />
(77 upregulated, 361 downregulated). Of<br />
the downregulated genes, 259 were part<br />
of the osteocyte transcriptome signature,<br />
and were predominantly expressed by<br />
mature osteocytes. In an overrepresentation<br />
analysis of the differentially expressed<br />
genes that were not part of the osteocyte<br />
transcriptome signature (77 upregulated,<br />
102 downregulated), 56 of the upregulated<br />
genes were found to play a role in immune<br />
function and haematopoiesis, whereas<br />
extracellular matrix organisation genes<br />
were highly enriched among downregulated<br />
genes. Dmd was not actively expressed in<br />
the tibia of either wild-type or mdx mice,<br />
suggesting dysregulation of the cortical bone<br />
transcriptome in mdx mice is unlikely to be<br />
directly caused by the Dmd defect. [OC<strong>22</strong>]<br />
Dominyka Batkovskyte presented the case<br />
of a patient with a syndromic short stature,<br />
skeletal abnormalities and developmental<br />
delay and a homozygous missense variant in<br />
TOMM7 (c.73T>C, p.W25R). The boy was born<br />
to healthy non-consanguineous parents, but<br />
presented with failure to thrive, severe short<br />
stature, and muscular hypotonia. Skeletal<br />
survey revealed mild platyspondyly with<br />
ovoid vertebral bodies, slender long tubular<br />
bones with relatively large epiphyses, coxa<br />
valga, slender metacarpals and proximal<br />
phalanges, and relatively large neurocranium.<br />
The patient died before the age of 3. Previous<br />
evidence from functional studies suggests<br />
the TOMM7 variant is hypomorphic and leads<br />
to abnormal growth and severe lipoatrophy.<br />
In this study, variant-specific and knock-out<br />
mouse models were used to validate the<br />
functional consequences. Tomm7 R/R mice had<br />
normal early growth but developed rapidly<br />
progressing emaciation at 9–10 weeks of age<br />
and died, whereas Tomm7 del/del mice showed<br />
severe growth failure in early postnatal<br />
stages. In addition, mutant mice showed<br />
slight shortening of vertebral bodies and<br />
the tibial growth plate, with reduced cellular<br />
density and proliferation. Tomm7 mutant mice<br />
also showed severe lipoatrophy and unique<br />
alteration in mitochondrial function. This<br />
study identifies TOMM7 as a new candidate<br />
gene for human disease with syndromic short<br />
stature and developmental delay. [LM3]<br />
NOVEL THERAPIES IN SKELETAL DYSPLASIA<br />
New therapies are in development for many different skeletal dysplasias.<br />
This round-up gives a selection across several conditions, including<br />
hypochondroplasia, hypophosphatasia, and other genetic bone disorders.<br />
As part of the Allied Health Professionals Orals<br />
Session, Raja Padidela presented an interim<br />
analysis from a UK cohort of 20 children with<br />
hypophosphatasia treated with asfotase alfa.<br />
Visits occurred at enrolment, 3 and 6 months,<br />
and every 6 months thereafter. Height Z-score<br />
at first assessment was −2.67, and changed<br />
by −0.09, while weight Z-score was −2.15 and<br />
changed by 0.11. BAMF scores for lower and<br />
upper extremities were 6 and 7.5, respectively,<br />
and were significantly improved. Parent- and<br />
child-reported PedsQoL scores were 52.50<br />
and 64.13, respectively, and changed by 4.35<br />
and 14.67. Starting Bleck scores were relatively<br />
high and remained stable throughout followup.<br />
Serious adverse events were infrequent<br />
(n=5, 10 events), with only one event (injectionsite<br />
atrophy) related to asfotase alfa.<br />
The authors concluded that asfotase alfa<br />
helps children with hypophosphatasia<br />
maintain stable outcomes. [P129]<br />
Carl Dambkowski shared an oral<br />
communication on low-dose infigratinib –<br />
an oral selective fibroblast growth factor<br />
receptor TKI – which has demonstrated<br />
activity in a preclinical model of<br />
hypochondroplasia. FGFR3 mutations<br />
play a crucial role in achondroplasia,<br />
but also in thanatophoric dysplasia<br />
and hypochondroplasia – a condition<br />
characterised by disproportionate short<br />
stature and a growth deficit affecting both<br />
endochondral and intramembranous<br />
ossification. There are currently no approved<br />
therapies for hypochondroplasia, but the<br />
group tested the hypothesis that infigratinib<br />
could improve the hypochondroplasia<br />
phenotype and improve ossification in<br />
a preclinical mouse model. Fgfr3 N534K/+<br />
mice treated with 1 mg/kg infigratinib<br />
every 3 days did not show obvious and<br />
significant modification of the dwarf<br />
phenotype. In contrast, Fgfr3 N534K/+ mice<br />
treated with 1 mg/kg infigratinib daily for<br />
21 days showed a statistically significant<br />
increase in appendicular and axial skeletal<br />
measures. Long bone length was statistically<br />
significantly increased in Fgfr3 N534K/+ mice vs<br />
Fgfr3 +/+ mice, and treatment also modified<br />
skull shape and mandible length, with<br />
an increase in foramen magnum length<br />
(+3.72%). Infigratinib also modified cartilage<br />
growth plate organisation, in particular the<br />
hypertrophic chondrocyte area. These results<br />
provide a rationale for targeting FGFR3 with a<br />
specific TKI for the treatment of children with<br />
hypochondroplasia. [OC1]<br />
Alison Boyce presented results from a<br />
Phase 2, open-label trial in 9 subjects<br />
who were administered with denosumab<br />
for fibrous dysplasia. Denosumab was<br />
administered for 6-months at 120 mg/dose<br />
monthly, with loading doses on Weeks 2 and 3.<br />
14 15
Achondroplasia.expert <strong>Congress</strong> <strong>Review</strong>s: <strong>ICCBH</strong> 20<strong>22</strong><br />
Treatment was followed by a 14-month<br />
observation period with intensive monitoring.<br />
Bone formation marker procollagen-1<br />
propeptide decreased by 92% from baseline,<br />
and resorption marker C-telopeptide by<br />
81%. Scans showed decreased measures of<br />
lesion activity, and lesion biopsies confirmed<br />
decreased cellularity in both fibrous and<br />
osseous tissue, and decreased osteocyte<br />
lacunae size. Five serious adverse events<br />
occurred in two subjects, all unrelated to<br />
treatment. Six subjects had treatmentrelated<br />
adverse events, but all were mineral<br />
abnormalities of mild-to-moderate severity.<br />
Post-denosumab discontinuation data was<br />
available in five subjects: two experienced<br />
bone turnover rebound above pre-treatment<br />
levels after 3 and 8 months. In one<br />
subject with panostotic disease, rebound<br />
resulted in severe hypercalcemia requiring<br />
hospitalisation. The authors conclude that<br />
denosumab has the potential to provide<br />
clinical benefit by reducing lesion activity<br />
in adults with fibrous dysplasia, although<br />
post-discontinuation rebound may<br />
be associated with life-threatening<br />
hypercalcemia, particularly in individuals<br />
with severe disease. [OC2]<br />
Leanne Ward shared skeletal health data<br />
for boys with Duchenne muscular dystrophy<br />
treated with vamorolone, a first-in-class<br />
dissociative steroid. In total 48 treatmentnaïve<br />
ambulatory boys 4–7 years of age<br />
initiated vamorolone at one of four doses<br />
for 6 months, followed by permitted dose<br />
escalations/de-escalations for 2 years.<br />
Serum bone turnover marker Z-scores were<br />
assessed from baseline to 6 and 30 months<br />
(adjusted for age and height percentile at<br />
each visit). Significant increases in serum<br />
osteocalcin and CTX z-scores were observed<br />
from baseline to 6 and 30 months; P1NP<br />
Z-scores were similar from baseline to<br />
6 and 30 months. The average bone<br />
age to chronological age difference was<br />
–1.1 years (P
LIST OF ABBREVIATIONS<br />
AFMS – Achondroplasia Foramen<br />
Magnum Score<br />
AGV – annualised growth velocity<br />
AHV – annualised height velocity<br />
BAMF – Brief Assessment of Motor Function<br />
BMD – bone mineral density<br />
CTX1 – C-terminal telopeptide of<br />
type 1 collagen<br />
CXM – collagen X fragment<br />
DXA – dual-energy x-ray absorptiometry<br />
ENT – ear, nose, and throat<br />
hr-pQCT – High-resolution peripheral<br />
quantitative computed tomography<br />
HRQoL – Health-related quality of life<br />
iPSC – induced pluripotent stem cells<br />
MRI – magnetic resonance imaging<br />
N-terminal proCNP – C-type natriuretic<br />
peptide propeptide<br />
OSA – obstructive sleep apnoea<br />
P1NP – N-terminal propeptide of<br />
type 1 collagen<br />
PEDI-CAT – Pediatric Evaluation of Disability<br />
Inventory – Computer Adaptive Test<br />
pQCT – Peripheral Quantitative Computed<br />
Tomography<br />
PedsQoL – Pediatric Quality of Life Inventory<br />
PRO-C2 – N-terminal propeptide of<br />
type 2 collagen<br />
QoLISSY – Quality of Life in Short<br />
Stature Youth<br />
SDS – standard deviation score<br />
Siglec15 – sialic acid-binding<br />
immunoglobulin-like lectin 15<br />
SIR – standardised incidence ratio<br />
TKI – tyrosine kinase inhibitor<br />
WeeFIM – Functional Independence<br />
Measures in Children