Vitiligo: More than a skin disease Sophie Heason - University of ...
Vitiligo: More than a skin disease Sophie Heason - University of ...
Vitiligo: More than a skin disease Sophie Heason - University of ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Vitiligo</strong>: <strong>More</strong> <strong>than</strong> a <strong>skin</strong> <strong>disease</strong><br />
<strong>Sophie</strong> <strong>Heason</strong> and Gerry Kent<br />
<strong>University</strong> <strong>of</strong> Sheffield, UK<br />
“I feel that without vitiligo I would be a different person, my personality is trapped<br />
behind a wall <strong>of</strong> being very self-conscious about myself. My only wish is to be cured -<br />
to be normal”<br />
“I can now say that it [vitiligo] doesn't affect my life at all, because I won't let my vitiligo<br />
make me unhappy and neither will my family and friends let it.”<br />
<strong>Vitiligo</strong> is a disfiguring disorder in which there is a progressive depigmentation <strong>of</strong><br />
<strong>skin</strong>. <strong>Vitiligo</strong> affects between one and four percent <strong>of</strong> the population, regardless <strong>of</strong><br />
race or sex. Patches, also known as lesions, <strong>of</strong> white <strong>skin</strong> and hair develop<br />
unpredictably. While there is a genetic component to vitiligo, race, sex and age do<br />
not affect the incidence <strong>of</strong> the <strong>disease</strong>. The cause is yet unknown and there is no<br />
commonly used treatment. Although there are no health complications with the<br />
<strong>disease</strong>, vitiligo can have a pr<strong>of</strong>ound psychological effect on sufferers. Kent and<br />
Al'Abadie (1996) found a high levels <strong>of</strong> distress in people with vitiligo compared to<br />
the general population. In the study described below, 44 percent <strong>of</strong> the sample<br />
reported an incident <strong>of</strong> stigma as a result <strong>of</strong> their vitiligo. However, as the above<br />
1
quotes illustrate, reaction to the disorder varies and not everyone with vitiligo has<br />
psychological or social difficulties.<br />
The aim <strong>of</strong> this report is to develop an understanding <strong>of</strong> the factors that<br />
contribute to distress in people with vitiligo. After discussing theoretical issues, the<br />
results <strong>of</strong> a quantitative study will be described and discussed. The aim <strong>of</strong> the study<br />
is to test the predictions that theory follow from theoretical perspectives in this area.<br />
To understand response to vitiligo we need to look at theories from both<br />
sociology and psychology. Erving G<strong>of</strong>fman (1963) produced important work on<br />
stigma that informs us about the interaction between a ‘marked’ person and their<br />
‘markers’. Psychological research on appearance, depression and anxiety about<br />
others’ evaluation <strong>of</strong> ourselves informs us about how people respond to their own<br />
disfigurement and the potential <strong>of</strong> stigmatisation.<br />
Sociological and psychological perspectives<br />
G<strong>of</strong>fman (1963) began his study <strong>of</strong> stigma by looking back at the original meaning<br />
<strong>of</strong> the word. Stigma is a Greek word used to describe a physical mark that would<br />
be placed on a person to signify them as deviant, such as the branding <strong>of</strong> slaves.<br />
Today, stigma refers to the social marks that are defined as undesirable and<br />
deviant. These marks range from physical disability, to perceived weaknesses such<br />
as mental illness, and tribal stigma - connected to race or religion. Intrinsic in the<br />
discussion <strong>of</strong> stigma is the issue <strong>of</strong> deviance. Deviance is a social process, not a<br />
static state. Therefore a person is only deviant when labelled as such. Harper<br />
(1999) showed this by highlighting the affect that culture has on decisions about<br />
acceptance <strong>of</strong> individuals. In Nepal, Antigua and Yucatan, an obese child was seen<br />
as affluent and a desirable playmate, while in the US obesity was seen as deviant<br />
and a reason for rejection.<br />
Albrecht et al (1983) found a distinct difference in response to people with<br />
physical disabilities and those with social deviance such as ex-convicts and the<br />
mentally ill. Visibility <strong>of</strong> the mark was also found to be an important factor. After<br />
comparing attitudes to people with different types <strong>of</strong> mark, Weiner, Perry and<br />
2
Magnussen (1988) discovered that physically based stigmas are perceived as<br />
onset-uncontrollable and linked with reactions <strong>of</strong> pity and plans to help, whereas<br />
stigmas based on mental and behavioural problems are perceived as onset-<br />
controllable and reacted to with anger, little liking, and no plans to help. They also<br />
found that perceptions <strong>of</strong> onset controllability are open to change given appropriate<br />
information. In their experiment, information was given emphasising that the onset<br />
<strong>of</strong> mental illness is not controllable. After this, respondents' judgement and affect<br />
towards a person with mental illness in a vignette became more positive. Weiner<br />
later extended this line <strong>of</strong> research with Schwarzer (1991) a<strong>skin</strong>g if there are factors<br />
other <strong>than</strong> onset controllability that influence reactions to a marked individual. Onset<br />
causality was shown to be related to pity, anger and support again. Descriptions <strong>of</strong><br />
people who actively cope with their problem received more pity and less anger <strong>than</strong><br />
those who did not cope well. They were also attributed with a higher chance for<br />
improvement and more likely to receive important social support.<br />
What does this mean to someone with vitiligo? While vitiligo is a physical<br />
disorder, the patches can be mistaken for dirty marks, a social deviance. With its<br />
cause not widely known the individual may be blamed for their lesions. A common<br />
response is to conceal lesions, which avoids the possibility <strong>of</strong> stigmatisation, but<br />
can cause anxiety and preoccupation with the concealment (Smart and Wegne,<br />
1999; Schmidd-Ott et al, 1999). Disclosure is a way <strong>of</strong> changing the stigma<br />
process, but is ‘effort-full’ and demands excellent social skills. Even if the person<br />
does disclose the cause <strong>of</strong> the disorder and its onset is perceived as<br />
uncontrollable, does someone with vitiligo really want to be treated with pity and a<br />
desire to help?<br />
Jacoby (1994) divided stigma into enacted and felt types. An actual incident<br />
<strong>of</strong> discrimination or marking was termed enacted stigma while felt stigma is the<br />
expectation <strong>of</strong> being marked. Thirty-two percent <strong>of</strong> respondents in a sample <strong>of</strong><br />
people with epilepsy said that they felt that their <strong>disease</strong> affected their opportunities<br />
in work, while only two percent reported enacted incidents <strong>of</strong> stigma related to<br />
work. Scambler and Hopkins (1986) found that enacted stigma is far less common<br />
3
<strong>than</strong> felt stigma, arguing that felt stigma is no less disabling <strong>than</strong> enacted stigma as<br />
it leads to rejection anxiety and avoidance.<br />
Stigma and appearance<br />
Immediate recognition <strong>of</strong> an individual's difference from the norm is through their<br />
appearance. Not only can appearances indicate an underlying difference but it can<br />
be seen as a source <strong>of</strong> deviance in itself. For example, a person seated in a<br />
wheelchair can be marked <strong>of</strong>f as being different due to a physical disability, but the<br />
use <strong>of</strong> the wheelchair can itself be stigmatising. Research in social cognition<br />
indicates that we need categorical representations to function efficiently in a social<br />
world (Macrae & Bodenhausen, 2000). Such categorisation begins at an early age<br />
and influences intended behaviour towards visibly different people (Harper, 1999),<br />
thus initiating the stigma process.<br />
Such categorisation is not only affected by disfigurement, level <strong>of</strong><br />
attractiveness also affects others’ perceptions <strong>of</strong> a person. There is a social<br />
understanding that beautiful people are good. Dion, Berschied and Walster (1972)<br />
first discussed this common finding in an important paper. They found that attractive<br />
people are judged to be more socially desirable <strong>than</strong> unattractive persons, to be<br />
perceived as having more total happiness in their lives and more success in their<br />
social and pr<strong>of</strong>essional lives. Interestingly attractive people were not judged to be<br />
better parents <strong>than</strong> unattractive people are. This may indicate an insight that<br />
attractive people may be better received socially and reap the benefits from this,<br />
but are no different in more internal attributes such as parenting style.<br />
Subsequent research has found that attractive people are perceived as<br />
more sociable, dominant, having better mental health, and having better social skills<br />
(Fiengold, 1992) However attractive people are not attributed with particularly<br />
greater character. The beauty and goodness stereotype is intrinsic in society, and<br />
is illustrated well in the powerful and extreme world <strong>of</strong> Hollywood in which<br />
disfigurement and ugliness are related to badness, and films highly biased in this<br />
4
stereotype encourage short-term favouritism to attractive people (Smith, McIntosh &<br />
Bazzini, 1999).<br />
These stereotypes have significant implications. Kerr et al (1985) used a<br />
mock trial to assess the effect <strong>of</strong> victim attractiveness and disfigurement on jurors’<br />
conviction <strong>of</strong> a defendant in a car theft and resulting accident. Defendants were<br />
significantly less likely to be convicted when the victim was unattractive or<br />
disfigured. Stevenage and McKay (1999) asked pr<strong>of</strong>essional recruitment personnel<br />
to assess personal qualities, job skills, and approval for a job based on a CV and<br />
photograph. Applicants with a facial disfigurement were perceived to be less able<br />
for the job and have fewer personal qualities and job skills. This is interesting in<br />
comparison to perceptions <strong>of</strong> people in a wheelchair who were not at a<br />
disadvantage. Perhaps this is due to the recruitment personnel being aware <strong>of</strong><br />
equal opportunities for wheelchair users, yet not having thought about their own<br />
assumptions <strong>of</strong> a person who is disfigured. To summarise the findings <strong>of</strong> influence<br />
<strong>of</strong> appearance on others’ assumption, a disfigured person is less likely to be<br />
perceived as successful and more likely to be perceived as ‘bad’. Also<br />
disfigurement increases possibility <strong>of</strong> conviction in a court and decreases<br />
opportunities in the job market.<br />
Effects <strong>of</strong> stigma on well-being<br />
The values that western society has placed on appearance and image is shown to<br />
have an effect on those who are different. Jones et al (1984) argue that labelling a<br />
person as deviant and unacceptable may influence their self-concept, behaviour,<br />
cognition and psychological health. In a study <strong>of</strong> young people with crani<strong>of</strong>acial<br />
anomalies, dissatisfaction with facial appearance was related to low global self<br />
worth, and low self perceptions <strong>of</strong> social acceptance (Pope & Ward, 1997). Altabe<br />
& Thompson (1996) described how an individual’s ideas and assumptions about<br />
their body are stored in a cognitive framework called the self-schema. The schema<br />
is proposed to affect information processing and behaviour, and consequently<br />
affect. Beuf (1990) suggests that a person with a visible stigma may internalise<br />
5
others' attitudes towards them and develop feelings <strong>of</strong> worthlessness. Bernstein<br />
(1990) discussed how disfigurement affects development in view <strong>of</strong> Erikson's<br />
developmental stages, with disappointment and lower levels <strong>of</strong> interaction in<br />
infancy, assumptions based on the beauty myth during childhood, and dealing with<br />
loss and a spoiled identity when developing a sense <strong>of</strong> self during adolescence.<br />
Bernstein takes evidence from studies performed on perception <strong>of</strong> strangers and<br />
generalises findings to all relationships that a disfigured person may have. Leary<br />
and Kowalski (1995) propose that self presentation is at the heart <strong>of</strong> social anxiety.<br />
A person who has strong intentions about presenting themselves in a certain way<br />
may become anxious about their ability to self present adequately, they will find<br />
obstructions to this presentation very stressful.<br />
Mark Leary has led a great deal <strong>of</strong> work in relation to social exclusion theory.<br />
He argues that humans have a fundamental motivation to be included in social<br />
groups and are gregarious by nature (Leary & Kowalski, 1995). He and his<br />
confederates argue that our ancestors who worked well in a group and who could<br />
monitor how well accepted they were, were at an evolutionary advantage over the<br />
isolated individual. Therefore, the need to belong has evolved as an inherited drive.<br />
Leary takes the argument further and states that a large proportion <strong>of</strong> social<br />
behaviour is directed at improving inclusion in groups (Leary, 1990). Leary argues<br />
that social isolation leads to loneliness, negative affect, ill health, changes in<br />
processing <strong>of</strong> social information, anxiety, and even criminality (Baumeister and<br />
Leary, 1995)<br />
The discussion has been on how stigma is a social process. The perception<br />
and behaviour <strong>of</strong> both the marked person and the marker influence the effect <strong>of</strong><br />
stigma. In the context <strong>of</strong> a world in which there is a reaction against disfigured<br />
people a situation in which a person with vitiligo has to manage the constant<br />
possibility <strong>of</strong> exclusion by others is created. They also have to deal with their own<br />
thoughts, feelings and behaviour in response to their stigma. The aim <strong>of</strong> the study<br />
reported below was to explore the relationships between experience <strong>of</strong> stigma on<br />
the one hand, and report <strong>of</strong> how intrusive the stigmatising disorder is on the other.<br />
6
Method<br />
Participants<br />
A postal questionnaire was sent to 680 members <strong>of</strong> The <strong>Vitiligo</strong> Society, a national<br />
charity. They had been contacted through the society magazine and returned a<br />
consent slip agreeing to participate. The questionnaires were sent in the early<br />
summer as previous research has shown that at this time people with vitiligo are<br />
preparing for revealing summer clothes and the darker <strong>skin</strong> around the patches that<br />
make the lesions more noticeable. Therefore issues related to vitiligo were in the<br />
forefront <strong>of</strong> the participants minds.<br />
Measures<br />
In addition to demographic information (sex, age, ethnic origin, and marital status)<br />
the following measures were used.<br />
• <strong>Vitiligo</strong> Severity Scale<br />
A scale devised by the authors based on the Psoriasis Severity Scale cited by<br />
Papadapoulos & Bor (1999) measured location and extent <strong>of</strong> body coverage <strong>of</strong><br />
vitiligo.<br />
• The Hospital Anxiety and Depression Scale (Zigmond & Snaith, 1983)<br />
• Illness Intrusiveness Scale (Devins, 1999)<br />
Illness intrusiveness is the main dependent variable in this study. The illness<br />
intrusiveness scale measures the degree to which a particular disorder or <strong>disease</strong><br />
affect different aspects <strong>of</strong> life, such as social involvement, recreation and<br />
occupation. According to Devins (1999), illness intrusiveness is the effect <strong>of</strong> illness<br />
related experiences on the person's ability to engage in rewarding and valued<br />
activities. It is a mediating factor between illness and treatment on the one hand,<br />
and distress on the other. The majority <strong>of</strong> research using this concept has been with<br />
7
patients with health threatening illnesses that require extensive treatment, such as<br />
renal failure and lupus. Devins et al (1994) found relationships between illness<br />
intrusiveness and perceived stigma and, in another study, levels <strong>of</strong> personal control<br />
(1989). Perceived stigma and lack <strong>of</strong> control over progression <strong>of</strong> vitiligo may be<br />
important factors in the effect <strong>of</strong> vitiligo on psychological health.<br />
• The Appearance Schemas Inventory (Cash & Labarge, 1996)<br />
The Appearance Schemas Inventory (ASI) assesses appearance related cognitive<br />
assumptions such as those discussed by Altabe & Thompson (1996). Individuals<br />
scoring highly on the ASI will focus a great deal on their appearance, and its effect<br />
on interpersonal situations, will invest emotionally in their appearance and will have<br />
internalised social stereotypes <strong>of</strong> appearance (Cash & Labarge. 1996). This<br />
schema may influence processing <strong>of</strong> information related to others' reactions to<br />
one's appearance, relating to the concept <strong>of</strong> perceived stigma.<br />
• Fear <strong>of</strong> Negative Evaluation - short version (Watson & Friend, 1969;)<br />
Watson and Friend (1969) constructed two scales to measure levels <strong>of</strong> social<br />
anxiety. The fear <strong>of</strong> negative evaluation scale measures expectation <strong>of</strong> negative<br />
evaluation and subsequent anxiety. The version used was shorter and items with<br />
reverse meaning had been excluded (Kent, 2001).<br />
• Qualitative Question re stigmatisation and coping<br />
Four open ended questions concerning a situation in which someone had said or<br />
done something negative as a result <strong>of</strong> the respondent’s vitiligo and how the<br />
respondent had coped with this was also included.<br />
Results<br />
Population<br />
Six hundred and ten valid questionnaires were returned. Seventy five percent <strong>of</strong> the<br />
respondents were women, and 90% were white. The mean age was 48 years, with<br />
8
a range <strong>of</strong> 16-91. Ninety-seven percent <strong>of</strong> the respondents had lesions on their face<br />
or hands. Four percent <strong>of</strong> the respondents were significantly depressed and 22%<br />
were significantly anxious (scoring over 11 on the relevant scales <strong>of</strong> the Hospital<br />
Anxiety and Depression Scale).<br />
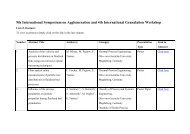
Correlation<br />
Table 1 shows the relationships between the items in the questionnaire. It is clear<br />
that as people get older the vitiligo becomes less intrusive and anxiety and fear <strong>of</strong><br />
negative evaluation decreases. There is a cluster <strong>of</strong> relationships between fear <strong>of</strong><br />
negative evaluation, anxiety, depression, importance <strong>of</strong> appearance, and illness<br />
intrusiveness.<br />
People who have reported a stigmatising event show higher levels <strong>of</strong><br />
importance <strong>of</strong> appearance and illness intrusiveness. Those with greater coverage<br />
<strong>of</strong> lesions and older people reported more experience <strong>of</strong> stigma.<br />
Regression analysis<br />
Regression analysis indicates how much each variable contributes to level <strong>of</strong> illness<br />
intrusiveness. Forty nine percent <strong>of</strong> the variance in illness intrusiveness was<br />
explained. Table 2 indicates the variables entered into the analysis. Age,<br />
importance <strong>of</strong> appearance, depression and report <strong>of</strong> enacted stigma each made<br />
significant contributions to illness intrusiveness.<br />
9
age<br />
ethnicity<br />
visibility<br />
Table 1: Correlation matrix for questionnaire measures<br />
area covered by lesions<br />
fear <strong>of</strong> negative<br />
evaluation (fne)<br />
age ethnic vis area FNE anx dep IA ii marital stigma<br />
-0.28<br />
anxiety -0.14 0.56<br />
depression 0.38 0.65<br />
importance <strong>of</strong><br />
appearance (IA)<br />
0.56 0.49 0.42<br />
illness intrusiveness (ii) -0.27 0.46 0.50 0.54 0.54<br />
marital status 0.14<br />
reported stigmatising<br />
event<br />
0.12 0.16 -0.24<br />
(Indicated r values have a p >.001 )<br />
Table 2: Results <strong>of</strong> single regression <strong>of</strong> variables explaining illness intrusiveness<br />
Variable Beta p value<br />
age -0.202
Discussion<br />
depression 0.333
found that older people are less affected by appearance impairment. Porter & Beuf<br />
(1988) found that age has a direct effect on well-being in a sample <strong>of</strong> people with<br />
vitiligo. They found that importance <strong>of</strong> appearance, self esteem, perceived<br />
discrimination and support are not mediating variables, which is surprising<br />
considering that the same authors found that age is related to perceived stigma<br />
(1991) and Ginsberg and Link (1989) found that people who are older at onset <strong>of</strong><br />
<strong>skin</strong> <strong>disease</strong> have lower sensitivity to other's opinions, anticipated rejection and<br />
feelings <strong>of</strong> guilt and shame. This could be linked to the significant correlation found<br />
between age, fear <strong>of</strong> negative evaluation and social anxiety. Kent (2000) also found<br />
age at onset significant. Further investigation needs to be done in this study to<br />
determine if any mediating variables exist in this sample.<br />
Report <strong>of</strong> enacted stigma.<br />
The finding that those who reported enacted stigma were more affected supports<br />
previous research by their disfigurement. There is the issue <strong>of</strong> recall and<br />
interpretation <strong>of</strong> events, in that people may have been stigmatised and not have<br />
been able to recall the event, or seen it as <strong>of</strong>fensive. Those who interpret particular<br />
events as enacted stigma or have high felt stigma (not measured in this study) may<br />
have a high fear <strong>of</strong> negative evaluation. Interesting opportunities for further study.<br />
Race<br />
These findings indicate that ethnic origin is not related to illness intrusiveness,<br />
supporting previous research. Porter & Beuf (1991) compared the effect <strong>of</strong> race on<br />
reaction to stigma in people with vitiligo. They found that race is not related directly<br />
to degree <strong>of</strong> disturbance, but may be mediated by perceived stigmatisation (with<br />
higher scores in black people) importance <strong>of</strong> appearance (with higher scores in<br />
women and white people) and self-esteem in which there was no variation by group<br />
in the sample. Porter & Beuf (1988) found that race has no direct significant effect<br />
on psychological disturbance, only operating indirectly through importance <strong>of</strong><br />
appearance and perceived discrimination. This relates to Kent’s work (1999) that<br />
12
found that race was related to perceived stigma. Further analysis <strong>of</strong> this data will<br />
discern the role <strong>of</strong> ethnicity as a mediating variable.<br />
Appearance and concealability<br />
The finding that visibility and extent <strong>of</strong> vitiligo lesions are not related to illness<br />
intrusiveness contributes to a body <strong>of</strong> research with mixed findings. Some research<br />
with people with different <strong>skin</strong> <strong>disease</strong>s suggests that visibility and appearance <strong>of</strong><br />
the <strong>disease</strong> are important. Jowett and Ryan (1985) found that a fifth <strong>of</strong> eczema<br />
sufferers said that the physical appearance <strong>of</strong> the <strong>disease</strong> was the worst aspect <strong>of</strong><br />
the condition. In the same study the majority <strong>of</strong> acne sufferers said that the worst<br />
aspect <strong>of</strong> the <strong>disease</strong> was the appearance and their subsequent lack <strong>of</strong> self-<br />
confidence. Porter & Beuf (1988) reported that people with lower severity vitiligo<br />
were less likely to be disturbed by the <strong>disease</strong>. They found that those with higher<br />
severity are more likely to perceive discrimination, and therefore to have increased<br />
psychological disturbance. Porter & Beuf (1991) found that visibility is not directly<br />
related to disturbance, but indirectly by its effect on perceived stigmatisation. The<br />
role <strong>of</strong> visibility and extent <strong>of</strong> vitiligo lesions in illness intrusiveness is not clear.<br />
Conclusion<br />
The sample used in this study does have its limitations. The problem <strong>of</strong><br />
representing the general population is clear in the imbalance between numbers <strong>of</strong><br />
men and women, and the lack <strong>of</strong> representation <strong>of</strong> non white people is difficult to<br />
resolve. Further limitations are in the recruitment <strong>of</strong> respondents in that they are all<br />
members <strong>of</strong> the <strong>Vitiligo</strong> Society. Time between sending and return <strong>of</strong> the<br />
questionnaire did not significantly affect scores on any <strong>of</strong> the variables.<br />
It is clear from this study that a person with vitiligo must cope with more <strong>than</strong><br />
their <strong>skin</strong> <strong>disease</strong>. A high proportion <strong>of</strong> the sample reported the experience <strong>of</strong><br />
enacted stigma along with heightened anxiety. The influence <strong>of</strong> social<br />
categorisation and societal assumptions about appearance is tw<strong>of</strong>old in this<br />
situation. The first influence is on the fact that markers view disfigurement as a<br />
13
stigma. The second, and internal, influence is that it there seems to be a<br />
relationship between the degree to which a person with vitiligo has internalised<br />
these stereotypes (importance <strong>of</strong> appearance) and the intrusiveness <strong>of</strong> their illness<br />
into everyday activities. This reinforces the process model <strong>of</strong> stigma that G<strong>of</strong>fman<br />
originally proposed.<br />
There are two explanations for the finding that illness intrusiveness<br />
decreases with age, and the negative correlation between age, fear <strong>of</strong> negative<br />
evaluation and anxiety. Either the person changes their perceptions <strong>of</strong> the world<br />
and their mark with time, or a longer life has allowed more time to develop a useful<br />
repertoire <strong>of</strong> coping behaviours. The former explanation would be supported by a<br />
negative correlation between age and importance <strong>of</strong> appearance, but this was not<br />
been found in this study. The latter explanation is supported by research in coping<br />
behaviour and is certainly promising. Future research that may clarify the issues<br />
raised in this study would examine importance <strong>of</strong> appearance with more depth;<br />
perhaps a qualitative methodology would be more suited. Also research in the<br />
coping process and applying the coping research to ageing would be useful.<br />
The relationship between depressed mood and illness intrusiveness opens<br />
up more issues. The influence <strong>of</strong> depression on cognition may be related to<br />
interpretation <strong>of</strong> events <strong>of</strong> stigma. Also the cluster <strong>of</strong> correlations between anxiety,<br />
fear <strong>of</strong> negative evaluation, importance <strong>of</strong> appearance and depression leave<br />
questions about moderating and mediating variables. These can be explored<br />
through further analysis.<br />
The fact that experience <strong>of</strong> stigma affects illness intrusiveness is to be<br />
expected. This is a huge social problem. The tackling <strong>of</strong> the values in society that<br />
lead to stigmatisation <strong>of</strong> people who look different is well beyond the scope <strong>of</strong> this<br />
paper. Some research has been done on the education <strong>of</strong> young people before a<br />
disfigured child joined their class. The findings were promising. Perhaps a more<br />
realistic way to reduce intrusiveness in people with vitiligo is to support them in<br />
exploring and using effective coping strategies.<br />
14
References<br />
Albrecht, G., Walker, V., & Levy, J. (1982) Social Distance from the Stigmatised: A test<br />
<strong>of</strong> two theories. Social Science and Medicine, 16: 1319-1327<br />
Altabe, M. & Thompson, J.K. (1996) Body Image: A Cognitive Self-Schema Construct<br />
Cognitive Therapy and Research, 20 (2): 171-193<br />
Baumeister, R.F. & Leary, M. (1995) The Need to Belong: Desire for Personal<br />
Attachment as a Fundamental Human Motivation Psychological Bulletin, 117 (3): 97-529.<br />
Beuf, A.H. (1990) Perspectives: Stigmatisation, Objectification and the Self Beauty and<br />
the Beast; Appearance Impaired Children in America. Uni <strong>of</strong> Penn Press, Phil.<br />
Cash, T. F. & Labarge, A. S. (1996) Development <strong>of</strong> the Appearance Schemas<br />
Inventory: A New Cognitive Body Image Assessment, Cognitive Therapy and Research,<br />
20 (1): 37-50<br />
Devins, G. M. (1989) Enhancing personal control and minimising illness intrusiveness.<br />
(Eds N. G.Kutner, D. D. Cardenas & J. D. Bower). Maximising rehabilitation in chronic<br />
renal <strong>disease</strong>, PME Publishing Co.<br />
Devins, G. M., Henderikus J. S. & Koopmans, J. P. (1994) Psychosocial impact <strong>of</strong><br />
laryngectomy mediated by perceived stigma and illness intrusiveness. Canadian Journal<br />
<strong>of</strong> Psychiatry, 39: 608-616<br />
Devins, G. M. & Edworthy, S. M. In press Illness intrusiveness explains race-related<br />
quality <strong>of</strong> life differences among women with systemic lupus erythematosus.<br />
Dion, K., Berschied, E. & Walster, E. (1972) What is Beautiful is Good Journal <strong>of</strong><br />
Personality and Social Psychology, 24 (3): 285-290<br />
Fiengold, A. (1992) Good Looking People are not What We Think. Psychological Bulletin,<br />
111 (2): 304-341<br />
Ginsburg I.H. & Link, B.G. (1989) Feelings <strong>of</strong> Stigmatisation in Patients with Psoriasis<br />
Journal <strong>of</strong> the American Academy <strong>of</strong> dermatology, 20: 53-63<br />
15
G<strong>of</strong>fman, E. (1963) Stigma: Notes on the Management <strong>of</strong> Spoiled Identity, Englewood<br />
Cliffs, NJ: Prentice Hall<br />
Harper, D.C. (1999) Social Psychology <strong>of</strong> Difference: Stigma, Spread and Stereotypes <strong>of</strong><br />
Childhood Rehabilitation Psychology, 44 (2): 131-144<br />
Jacoby, A. (1994) Felt versus Enacted stigma: A Concept Revisited. Social Science and<br />
Medicine, 38 (2): 269-274<br />
Jones, E. E., Farina, A., Hastorf, A., Marcus, H., Miller, D. & Scott, R. (1984) Social<br />
Stigma: The Psychology <strong>of</strong> Marked Relationships. NY: WH Freeman<br />
Jowett, S. & Ryan, T. (1985) Skin <strong>disease</strong> and handicap: an analysis <strong>of</strong> the impact <strong>of</strong><br />
<strong>skin</strong> conditions. Social Science and Medicine 20 (4): 425-429<br />
Kent, G. (1999) Correlates <strong>of</strong> Perceived Stigma in <strong>Vitiligo</strong> Psychology and Health, 14:<br />
241-251<br />
Kent, G. (2000) Understanding the Experiences <strong>of</strong> People with Disfigurements; an<br />
Integration <strong>of</strong> Four Models <strong>of</strong> Social and Psychological Functioning Psychology, Health<br />
and Medicine, 5 (2): 117-129<br />
Kent, G and Al'Abadie, M. (1996) Psychological affects <strong>of</strong> vitiligo: A critical incident<br />
analysis. Journal <strong>of</strong> the Academy <strong>of</strong> Dermatology, 35 (6): 895-898<br />
Kerr, R., Bull, R., MacNoun, R. & Rathborn, H. (1985) Effects <strong>of</strong> Victim Attractiveness,<br />
Care and Disfigurement on the Judgements <strong>of</strong> American and British Mock Jurors Journal<br />
<strong>of</strong> Social Psychology, 24: 47-58<br />
Leary, M. (1990) Responses to Social Exclusion: Social Anxiety, Jealousy, Loneliness,<br />
Depression and Self Esteem Journal <strong>of</strong> Social and clinical Psychology, 9 (2): 221-229<br />
Leary, M. & Kowalski, R M. (1995) Social Anxiety. Guildford Press. New York<br />
Macrae, N. and Bodenhausen, G.V. (2000) Social Cognition: Thinking Categorically about<br />
Others Annual Review <strong>of</strong> Psychology, 51: 93-120<br />
Papadopoulos, L. & Bor, R. (1999) Psychological Approaches to Dermatology.<br />
Leicester, BPS Books.<br />
16
Pope, A.W. & Ward, J (1997) Self Perceived Facial Appearance and Psychosocial<br />
Adjustment in Preadolescents with Cran<strong>of</strong>acial Anomalies<br />
Porter, J. & Beuf, A.H. (1988) Response <strong>of</strong> Older People to Impaired Appearance: The<br />
Effect <strong>of</strong> Age on Disturbance by <strong>Vitiligo</strong> Journal <strong>of</strong> Ageing studies, 2 (2): 167-181<br />
Porter, J. & Beauf, A.H. (1991) Racial Variation in Reaction to Physical Stigma: A Study<br />
<strong>of</strong> Degree <strong>of</strong> Disturbance by <strong>Vitiligo</strong> Among Black and White Patients Journal <strong>of</strong> Health<br />
and Social Behaviour, 32: 192-204<br />
Porter, J., Beauf, A., Lerner, A. & Norlund, J. (1987) Response to cosmetic<br />
disfigurement: Patients with vitiligo. Cutis, 39: 493-494<br />
Scambler, G. & Hopkins, A. (1986) Being epileptic: Coming to terms with Stigma<br />
Sociology <strong>of</strong> Health and Illness, 8: 26-43<br />
Schmidd-Ott, G., Kuensebeck, H.W. Jaeger,B., Werfel, T., Frahm, K., Ruitman, J.,<br />
Kapp, A. & Lamprecht, F. (1999) Validity Study for the Stigmatisation Experience in<br />
Atopic Dermatitis and Psoriatic Patients Acta Dermatologica Venereologica, 79: 443-447<br />
Schwarzer, R. & Weiner, B. (1991) Stigma Controllability and Coping as Predictors <strong>of</strong><br />
Emotions and Social Support. Journal for Social and Personal Relationships, 8: 133-140<br />
Smart, L. & Wegner, D.M. (1999) Covering Up What Can't Be Seen: Concealable<br />
Stigma and Mental Control Journal <strong>of</strong> Personality and Social Psychology, 77 (3): 474-<br />
486<br />
Smith, S.M., McIntosh, W.D. & Bazzini, D.G. (1999) Are the Beautiful Good in<br />
Hollywood? An Investigation <strong>of</strong> the Beauty and Goodness Stereotype on Film Basic and<br />
Applied Psychology, 21 (1): 69-80<br />
Stevenage, S.V. & McKay, Y. (1999) Model Applicants: The Effect <strong>of</strong> Facial Appearance<br />
on Recruitment Decisions British Journal <strong>of</strong> Psychology, 90: 221-234<br />
Watson, D. & Friend, R. (1969) Measurement <strong>of</strong> socio-evaluative anxiety. Journal <strong>of</strong><br />
Consulting and Clinical Psychology, 33 (4): 448-457.<br />
Weiner, B., Perry, R. and Magnussen, J. (1988) An Attributional Analysis <strong>of</strong> Reactions to<br />
Stigmas Journal <strong>of</strong> Personality and Social Psychology, 55 (5): 738-748<br />
17
Zigmond, A.S. and Snaith, R.P. (1983) The Hospital and Anxiety and Depression Scale.<br />
Acta Psychiatra Scandinavica 67: 361-370<br />
<strong>Sophie</strong> <strong>Heason</strong> is a Ph.D. research student in the Psychology Department at The<br />
<strong>University</strong> <strong>of</strong> Sheffield. <strong>Sophie</strong>’s main field <strong>of</strong> research is health psychology; with<br />
interests in disfigurement, body image, coping processes, social anxiety and depression,<br />
and stigma. Her previous research includes social networks in people with learning<br />
disabilities and applied work with people with learning disabilities and challenging<br />
behaviour.<br />
Gerry Kent is a senior lecturer in Clinical Psychology at the <strong>University</strong> <strong>of</strong> Sheffield. He<br />
has a range <strong>of</strong> interests within health psychology, but they centre around the effects <strong>of</strong><br />
illness on social and psychological well-being.<br />
Email address: s.heason@sheffield.ac.uk<br />
18