Headspace-Master-2016

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Head Space:<br />
a handbook on brain injury<br />
Claire Freeman<br />
BDes (Hons), PGDip Mktg, PGDip Rehab<br />
Bernadette Cassidy<br />
BA (Hons), PGCRM, PhD
Brain Injury New Zealand wholeheartedly supports the<br />
project undertaken by Claire Freeman and Bernadette<br />
Cassidy to produce the publication “Head Space” A<br />
handbook on brain injury.<br />
New Zealand Spinal Trust is to be commended for encouraging and supporting<br />
them to produce such a publication which will serve all those in New Zealand who<br />
experience a brain injury, their family, whanau and friends. Ninety [90] people a day<br />
are affected by brain injury in some form and many are the result of concussion. That<br />
represents between 24 000 and 33 000 people in a year.<br />
The most challenging aspect is that so often it is a hidden injury, depending on the<br />
severity, and the difficulties experienced by individuals and those around them are<br />
not necessarily obvious to the public in general.<br />
This publication will be incredibly useful as a guide to anyone seeking answers and<br />
gives comprehensive explanations and suggestions that will satisfy the majority<br />
of concerns. It is such a good pointer for people to take the next step in getting<br />
professional help if they haven’t already done so.<br />
Brain Injury New Zealand sees this book as an ideal item to be given to everyone<br />
affected, at the assessment stage or on discharge from hospital.<br />
Congratulations for pursuing such a worthwhile initiative.<br />
Graham Menary<br />
Chief Executive<br />
Brain Injury New Zealand<br />
Disclaimer: This publication has been produced with the support of the Brain Injury Unit, Burwood Hospital and<br />
the Brain Injury Association NZ. It is intended as a guide only and should not be used to replace the medical<br />
opinions of your health professionals. Medical knowledge is constantly evolving and preferred rehabilitation<br />
techniques may differ from region to region. Readers are strongly advised to confirm that information in this<br />
publication conforms to current standards of practice endorsed by your health professionals.<br />
Published by:<br />
The New Zealand Spinal Trust<br />
Burwood Hospital, Private Bag 4708, Christchurch, New Zealand<br />
All rights reserved. No part of this publication may be copied, reproduced, stored or transmitted by any mechanical,<br />
photographic or electronic processes or techniques, for public or private use, without the express written permission of the<br />
publisher.<br />
© New Zealand Spinal Trust, 2009<br />
To learn more about the New Zealand Spinal Trust go to:<br />
www.nzspinaltrust.org.nz<br />
This edition printed January 2010.<br />
ISBN 978-0-473-15091-4
Foreword<br />
by Sir Tim Wallis<br />
Where, before this book was published, could a family get this very<br />
important information?<br />
This book will be a great help both to the people who sustain a brain injury<br />
and to their families and carers. All the different aspects of injury and<br />
recovery are described very clearly and helpfully. My wife says she wishes<br />
such a book had been available when I had my accident in 1996.<br />
A brilliant book.<br />
Well done and thank you, Bernadette and Claire.<br />
Sir Tim Wallis<br />
Acknowledgements<br />
The authors wish to acknowledge the support and encouragement of<br />
the Brain Injury Association Canterbury, especially Sue Wilson for her<br />
enthusiasm and interest in the handbook.<br />
We wish to acknowledge and thank Christine Fry, Charge Nurse Manager<br />
and the staff of the Burwood Brain Injury Rehabilitation Unit for their<br />
contributions and support, Wendy Fulton for help with distributing the draft<br />
for comments and Julian Verkaaik for his original concept of the handbook.<br />
Thanks to John Maasch for his help with the stroke section. Grateful thanks<br />
to Barbara Freeman, Jock Vennell and Cecile Tait for their editorial skills.<br />
Finally, very special thanks to the members of the Christchurch and<br />
Ashburton Brain Injury Association Canterbury ‘Chat Room’ groups,<br />
especially Shane Thrower, Mike St. John, Archie Andrews, Graeme Sudlow,<br />
Brendan, Noel, Cate, Paul & Carmen Lee, Merv and Elizabeth, Noel, Douglas,<br />
Sue Brown, and to all those with a brain injury who gave so generously of<br />
their time in the development of this handbook.<br />
4
Guide to the Handbook<br />
Foreword &<br />
Your Brain<br />
Physical<br />
Thinking<br />
(Cognitive)<br />
Emotional<br />
Life after<br />
brain injury<br />
Personal<br />
Journeys<br />
A brief overview of a brain injury and what<br />
to expect following your brain injury<br />
Physical effects you may experience after<br />
your brain injury<br />
Problems with thinking and communication<br />
you may experience as a result of your<br />
brain injury<br />
Changes in mood and behaviour you may<br />
experience after a brain injury<br />
Getting back into your community and<br />
adjusting to life after a brain injury<br />
A collection of personal journeys from<br />
people who have had a brain injury<br />
Resources<br />
Author’s note, books, videos,<br />
DVD’s, websites on brain<br />
injury and glossary<br />
GUIDE TO CHAPTER CONTENTS<br />
Headaches<br />
Page 23<br />
This is a visual guide<br />
to each chapter’s<br />
contents.<br />
In each of the chapter contents,<br />
there will be a picture to show<br />
you which part of your brain<br />
has been affected.<br />
Guide to page number<br />
and chapter contents.<br />
5<br />
5
Chapter Contents<br />
4 .............. Foreword<br />
5 ............... Guide to the Handbook<br />
6 ............... Contents<br />
9 ............. Chapter 1 - Your Brain<br />
10 .............. Effects of a Brain Injury<br />
11 .............. Coma and Glasgow Coma Scale<br />
12 ............... Post Traumatic Amnesia (PTA)<br />
13 .............. Types of Brain Injury<br />
16 .............. Stroke<br />
19 .............. Left and Right Brain<br />
20 .............. How the Brain Works<br />
21 .............. Frontal Lobe Damage<br />
22 .............. Temporal Lobe Damage<br />
23 .............. Parietal Lobe Damage<br />
24 .............. Occipital Lobe Damage<br />
25 .............. Cerebellum Damage<br />
26 .............. Brain Stem Damage<br />
28 ............. Chapter 2 - Physical<br />
29 .............. Fatigue and Tiredness<br />
32 .............. Headaches<br />
34 .............. Seizures<br />
36 .............. Movement, Balance, Co-ordination and Dyspraxia<br />
38 .............. The Five Senses: Touch, Smell, Taste, Vision and Hearing<br />
40 .............. Swallowing / Dysphagia<br />
41 .............. Bladder and Bowel Issues (Continence)<br />
44 ............ Chapter 3 - Thinking (cognitive)<br />
45 .............. Vision and Perception Issues<br />
47 .............. Communication Issues / Aphasia<br />
49 .............. Planning, Organizing and Problem-Solving<br />
51 .............. Attention and Concentration Issues<br />
54 .............. Memory Issues<br />
6
Chapter Contents<br />
58 ............ Chapter 4 - Emotional issues<br />
59 .............. Anger, Frustration, Depression and Anxiety<br />
62 .............. Sexual Issues<br />
65 .............. Behaviour and Self-Centredness<br />
67 .............. Lack of Motivation<br />
69 .............. Emotional Extremes<br />
72 ............ Chapter 5 - Life after brain injury<br />
73 .............. Brain Injury in New Zealand - Statistics<br />
74 .............. The Rehabilitation Team<br />
77 .............. Family / Relationships<br />
84 .............. Getting Back to Work<br />
88 .............. Driving After a Brain Injury<br />
92 .............. Nutrition / Alcohol<br />
95 .............. Exercise / Brain Gym<br />
98 .............. Socialising / Recreation<br />
102<br />
Chapter 6 - Personal Journeys<br />
103 .............. Mike<br />
105 .............. Cate<br />
107 .............. Graeme<br />
108 .............. Elizabeth and Merv<br />
109 .............. Paul<br />
111 .............. Cecile<br />
115 Chapter 7 - Author’s Note,<br />
Resources, Glossary<br />
116 ............. Author’s note from Claire and Bernadette<br />
117 ............. Resources<br />
121 ............. Glossary<br />
7
Your Brain<br />
Your Brain
Introduction<br />
Brain injury occurs when the brain’s tissue is damaged<br />
or is not working properly. Anything that can damage<br />
brain tissue can cause a brain injury. Brain injuries<br />
can be the result of a blow to the head, such as from<br />
a fall, sports injury, car accident, an assault, cycling or<br />
from any other outside influence.<br />
There are other ways in which the brain may suffer<br />
an injury without a blow to the head. For example,<br />
the brain can lose its blood supply or a blood vessel can break so that<br />
bleeding into the brain tissue occurs. This is usually referred to as a ‘stroke’.<br />
A stroke is one of the most frequent causes of brain injury in older people.<br />
Other causes of injury to the brain can be a drug overdose, a tumour, an<br />
infection, a lack of oxygen or chemical poisoning.<br />
Sometimes the term ‘head injury’ is used instead of brain injury. This can be<br />
misleading as a head injury can include other injuries to the head, such as jaw<br />
or skull fractures, which may not involve the brain.<br />
This handbook is concerned with injuries to the brain and will refer to these<br />
as ‘brain injuries’.<br />
Clinical identification of a brain injury includes<br />
one or more of the following:<br />
• Confusion or disorientation<br />
• Loss of consciousness<br />
• Post-traumatic amnesia<br />
9
Effects of a Brain Injury<br />
The effects of a brain injury are wide ranging<br />
and may result in the following:<br />
Physical disabilities<br />
Sensory disabilities (for example, sight, smell)<br />
Personality changes<br />
Thinking (cognitive) disabilities (for example, difficulty thinking clearly,<br />
planning and following through, memory problems)<br />
Difficulty expressing or understanding language<br />
Many people who have a brain injury continue to have ongoing<br />
problems which may include some of the following:<br />
Aggression<br />
Depression<br />
Anxiety<br />
Impulsiveness<br />
Mood swings<br />
Poor concentration<br />
Difficulty with problem-solving<br />
Passivity<br />
Socially inappropriate behaviour<br />
Changes in thinking processes<br />
Loss of memory<br />
10
Coma and<br />
Glasgow Coma Scale<br />
Eyes<br />
Verbal<br />
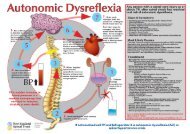
Glasgow Coma Scale<br />
Brain injuries are usually classified<br />
according to severity. They can be mild,<br />
moderate, or severe. When a brain injury<br />
occurs, two assessments are used to<br />
measure the severity: the Glasgow Coma<br />
Scale (GCS) and the duration of Post-<br />
Traumatic Amnesia (PTA).<br />
Post-Traumatic Amnesia refers to the<br />
time between injury and the recovery of<br />
full memory for day-to-day events. The<br />
Glasgow Coma Scale is the most widely<br />
used scoring system for measuring the<br />
level of consciousness following traumatic<br />
brain injury. GCS has three parts: an<br />
assessment of eye opening, best motor<br />
response and best verbal response.<br />
1 2 3 4 5 6<br />
Does not<br />
Opens eyes in<br />
Opens eyes in Opens eyes<br />
open eyes<br />
response to painful<br />
N/A<br />
N/A<br />
response to voice spontaneously<br />
stimuli<br />
Makes no<br />
sounds<br />
Incomprehensible<br />
sounds<br />
Utters inappropriate<br />
words<br />
Confused,<br />
disoriented<br />
Oriented, converses<br />
normally<br />
N/A<br />
Motor<br />
Makes no<br />
movements<br />
Reaction to<br />
painful stimuli<br />
Abnormal flexion to<br />
painful stimuli<br />
Flexion / Withdrawal<br />
to painful stimuli<br />
Localizes painful<br />
stimuli<br />
Obeys<br />
commands<br />
A scoring system is used, with the lowest score being 3 and the<br />
highest 15. For example, a score of 8 or less would be regarded as<br />
a severe brain injury resulting in a coma state; a score of 9 to 12<br />
would indicate a moderate brain injury; and a score of 13 to 15<br />
would indicate a mild brain injury.<br />
3 4 5 6 7 8 9 10 11 12 13 14 15<br />
severe injury moderate injury mild injury<br />
11
Post-Traumatic Amnesia (PTA)<br />
If you are in a coma as a result of a brain injury,<br />
afterwards you may have Post-Traumatic Amnesia<br />
(PTA). Even mild concussion can cause a short period<br />
of Post Traumatic Amnesia.<br />
Someone emerging from a coma does not just wake<br />
up, they go through a gradual process of regaining<br />
consciousness. This stage of recovery may last for hours, days or<br />
weeks.<br />
This may be a very confusing time for you. You may not have any idea<br />
of time, talking may be difficult and you may be very tired. Behavioural<br />
changes can also affect you. For example, some people become passive,<br />
or aggressive, abusive and agitated after being in a coma during the PTA<br />
stage. Some people liken PTA to being in a dream-like state.<br />
Some medical professionals believe that the duration of PTA is the best<br />
indicator of the severity of a brain injury.<br />
You will have little awareness of any behavioural and cognitive<br />
impairments and usually will remember nothing of what happened<br />
during PTA, even though you were fully awake. The good news is that<br />
PTA does not last forever.<br />
Symptoms of Post-Traumatic Amnesia:<br />
No idea of time.<br />
Talking may be difficult.<br />
You may be tired.<br />
Your behaviour may change. You may become<br />
aggressive, abusive or agitated.<br />
12
Types of Brain Injury<br />
Many terms are used to describe the different types of brain injuries,<br />
the severity of brain injuries and the causes of brain injuries.<br />
Below are some of the more common terms used.<br />
Concussion:<br />
This is the most common and least serious type of<br />
traumatic brain injury. It is usually as a result of a direct<br />
blow to the head, or when the brain is shaken. It is not<br />
usually associated with penetrating injuries to the head.<br />
Concussion can also be due to a fall or sports injury<br />
(for example, playing rugby).<br />
Acquired brain injury:<br />
This term is used to describe any damage to the brain not present at birth<br />
(for example, from a car accident or a blow to the head).<br />
Traumatic brain injury:<br />
This term is used when an outside force traumatically injures the brain.<br />
Anoxic brain injury occurs when the brain does not receive<br />
oxygen for several minutes or longer. Cells in the brain<br />
need oxygen to survive and function.<br />
Hypoxic brain injury results when the brain does not<br />
receive enough oxygen. An hypoxic injury is not as severe<br />
as an anoxic injury, but brain cells can still die from a lack<br />
of oxygen.<br />
13
Types of Brain Injury<br />
Mild brain injury<br />
A mild brain injury is when there is trauma to the head.<br />
At least one of the following symptoms needs to be<br />
present for a mild brain injury:<br />
• A period of loss of consciousness (no more<br />
than 30 minutes)<br />
• Loss of memory<br />
• Feeling dazed, disorientated or confused<br />
• Initial Glasgow Coma Scale score of 13-15<br />
• Post-Traumatic Amnesia not longer than 24<br />
hours<br />
Moderate brain injury<br />
A moderate brain injury is more severe than a mild<br />
brain injury. Symptoms include:<br />
• Glasgow Coma Scale score of 9 - 13<br />
• Confusion lasts from days to weeks<br />
• Physical, thinking and/or behavioural issues<br />
can last for months. In some cases they may be<br />
permanent<br />
Severe brain injury<br />
• Glasgow Coma Scale score of 8 or less<br />
• This person is generally in a prolonged<br />
unconscious state<br />
• Substantial physical, behavioural and/or thinking<br />
issues as a result of the injury<br />
14
Types of Brain Injury<br />
Open head injury (penetration)<br />
When an object enters the brain, such as a sharp object.<br />
Coup/contrecoup injury<br />
A coup injury occurs at the site of impact. A contrecoup<br />
injury is when there is damage to a part or region of<br />
the brain that is opposite to where the blow is received,<br />
often causing rupture of the affected parts.<br />
Contusion<br />
A contusion is bruising (bleeding) on the brain caused by<br />
small blood vessels leaking into brain tissue. A contusion<br />
occurs as a result of trauma to the brain and in many<br />
cases is more serious than a concussion.<br />
Haematoma<br />
A haematoma is a collection of blood as a result of internal<br />
bleeding from trauma or an aneurysm. An aneurysm is<br />
a widening and possible rupture of an artery, vein or the<br />
heart itself.<br />
Diffuse axonal injury<br />
A diffuse axonal injury can be caused by violent shaking<br />
of the head. The movement of the brain inside the skull<br />
causes extensive tearing of nerve tissue which can cause<br />
brain chemicals to be released, causing additional injury.<br />
15
Stroke<br />
When the brain's blood supply is cut off, a stroke can occur.<br />
Blood carries nutrients and oxygen to the brain. Without a supply of<br />
blood to the brain, cells may be damaged or destroyed.<br />
A stroke causes damage to the brain, which affects how the body works<br />
and functions. It can also affect your mental processes, such as how you<br />
think, your emotions and the way you communicate.<br />
The effects from a stroke can be felt immediately.<br />
Infarction<br />
When brain tissue dies due to a stroke, this damage is called cerebral<br />
infarction. An infarct is an area of dead tissue.<br />
Two main types of stroke<br />
Blockage.<br />
The most common stroke is caused by a<br />
clot that blocks an artery. This is called an<br />
ischaemic stroke.<br />
Bleed.<br />
The second type of stroke is caused by a<br />
bleed, such as when a blood vessel bursts.<br />
This causes a haemorrhagic stroke.<br />
Possible outcomes from a stroke<br />
Much like a traumatic brain injury, every stroke is different. For some<br />
people the symptoms may be quite mild and only last a short time as<br />
there may not have been any permanent damage. Other strokes can<br />
cause more severe and permanent damage.<br />
Recovery from a stroke can take months, this is when most progress<br />
will take place. For some people, their recovery can continue for<br />
several years.<br />
16
Stroke<br />
Transient Ischaemic Attack (TIA)<br />
Transient Ischaemic Attack is often called a mini stroke. It happens<br />
when the blood supply to your brain is interrupted very briefly, causing<br />
symptoms similar to a stroke, Generally these symptoms disappear<br />
after a short amount of time, usually no longer than an hour, but they<br />
can last up to 24 hours. TIA can be an important warning sign for a<br />
more serious stroke and preventative measures should be taken as<br />
soon as possible.<br />
Symptoms of TIA are:<br />
Difficulty speaking<br />
Vision problems, such as<br />
loss of sight in one eye or<br />
blurred vision<br />
Secondary Stroke Prevention<br />
These preventative measures may decrease the risk of another stroke<br />
happening. Secondary strokes can be more damaging to the brain, so<br />
prevention is the best way to avoid this from happening.<br />
Control your blood<br />
pressure, make sure it is<br />
not too high<br />
Mild temporary paralysis on<br />
one side of the body, such as<br />
the face, arm or leg<br />
Exercise regularly<br />
Stop smoking<br />
Control and monitor<br />
your diabetes<br />
Decrease your<br />
cholesterol level<br />
Maintain a healthy weight<br />
and eat healthily<br />
Avoid excessive alcohol<br />
Avoid excessive stress<br />
Have regular check ups with<br />
your general practitioner<br />
Take medications as<br />
prescribed by your doctor<br />
which can help reduce the<br />
chances of secondary stroke<br />
17
Stroke<br />
Signs and symptoms<br />
that someone has had a stroke:<br />
Slurred speech<br />
Headache<br />
Problems with vision<br />
Confusion<br />
Numbness or weakness down<br />
one side of the body<br />
Ongoing problems associated<br />
with having a stroke:<br />
Balance problems<br />
Memory issues<br />
Difficulty with swallowing<br />
Weakness or paralysis<br />
Fatigue<br />
Speech and language problems<br />
Problems with bladder and<br />
bowels<br />
Emotional mood swings<br />
Sensation, too sensitive, or<br />
lack of sensation<br />
Visual problems<br />
Pain<br />
Cognitive issues, such<br />
as thinking, learning,<br />
concentrating, remembering<br />
18
Left and Right Brain<br />
The brain is divided into two parts or ‘hemispheres’. The left<br />
side of the brain controls the right side of the body and the<br />
right side of the brain controls the left side of the body.<br />
The right side of the brain takes visual information and<br />
interprets it creatively. The left is the logical and analytical<br />
side. It takes the information collected by the right side and<br />
analyses and applies language to it.<br />
People with right side injuries often deny having an injury as<br />
the brain does not realise that something is wrong. If you<br />
have an injury to the left side, you may know something is<br />
not right. You may find it difficult to solve complex problems<br />
and consequently you may feel depressed because of this.<br />
Left Side of Brain<br />
The left side of the brain controls:<br />
Right Side of Brain<br />
The right side of the brain controls:<br />
Movement of right side of body<br />
Problem-solving<br />
Expression (words)<br />
Mathematical calculation<br />
Seeing in black and white<br />
Speech and language<br />
Reading and writing<br />
Organisation skills<br />
Movement of left side of body<br />
Holistic thought<br />
Intuition and emotional expression<br />
Creativity and thinking<br />
Visual memory, drawing, and music skills<br />
Spatial visualisation<br />
Seeing in colour<br />
Using pictures, not words<br />
1 + 1<br />
19
How the Brain Works<br />
There are 100 billion nerve cells in your brain. On each nerve cell are<br />
two branches:<br />
Dendrites, which receive incoming messages from other cells<br />
in the form of an electrical impulse.<br />
Axons, which carry outgoing signals to other cells.<br />
Interconnected, they provide super-fast communication, allowing the<br />
brain to send messages from one side to the other, which lets you<br />
move and make decisions. This is done by a chemical that is shot from<br />
the axon across a gap (synapse) where it triggers another cell to send<br />
a message.<br />
An injury to your brain can destroy or damage these nerve cells, which<br />
means that some messages will not get through or may get scrambled<br />
along the way.<br />
20
Frontal Lobe Damage<br />
COMMON EFFECTS OF FRONTAL LOBE DAMAGE<br />
Loss of spontaneity<br />
Personality changes<br />
Sexually uninhibited<br />
Inflexible thinking<br />
Repetition of words, gestures or acts<br />
Mood - *Aggressive and explosive anger<br />
Initiative and planning -<br />
*Difficulty sequencing<br />
*Reduced problem-solving skills<br />
Motor function -<br />
*Paralysis and loss of simple movement<br />
Memory - *Selective attention and reduced concentration<br />
Language - *Decrease of verbal expression ability<br />
21
Temporal Lobe Damage<br />
COMMON EFFECTS OF TEMPORAL LOBE DAMAGE<br />
Language - *Difficulty recognising words<br />
*Loss of inhibition while talking<br />
Memory - *Difficulty recognising faces<br />
*Difficulty identifying, locating and categorizing objects<br />
*Short-term memory loss<br />
Mood - *Increased aggressive behaviour<br />
*Increase or decrease in sexual desire<br />
Selective attention -<br />
*Decreased recall of verbal and/or visual content<br />
22
Parietal Lobe Damage<br />
COMMON EFFECTS OF PARIETAL LOBE DAMAGE<br />
Limb / facial movements are affected<br />
Loss of spatial awareness<br />
Changes in feeling / touch<br />
Problems with naming objects<br />
Right/left confusion<br />
Writing and maths difficulties<br />
Difficulty with multi-tasking<br />
Voluntary movement -<br />
*Problems with eye-hand co-ordination<br />
*Lack of awareness of body parts<br />
Visual attention -<br />
*Reading and drawing problems<br />
*Inability to focus visual attention<br />
23
Occipital Lobe Damage<br />
COMMON EFFECTS OF OCCIPITAL LOBE DAMAGE<br />
Vision -<br />
*Difficulty identifying colours and recognising drawn objects<br />
*Blind spots<br />
*Hallucinations<br />
*Visual distortions<br />
*Not seeing some words<br />
*Difficulty reading and writing<br />
*Difficulty recognising the movement of an object<br />
*Difficulty visually locating objects<br />
24
Cerebellum Damage<br />
COMMON EFFECTS OF CEREBELLUM DAMAGE<br />
Difficulty with balance<br />
Equilibrium -<br />
*Tremors<br />
*Dizziness<br />
Muscle tone -<br />
*Inability to grasp objects<br />
*Slurred speech<br />
Movement -<br />
*Problems with fine movement and co-ordination<br />
*Problems with mobility<br />
*Difficulty with rapid movements<br />
25
Brain-Stem Damage<br />
COMMON EFFECTS OF BRAIN-STEM DAMAGE.<br />
Problems with the physical act of talking<br />
Difficulty swallowing food and liquid<br />
Decreased breathing capacity<br />
Sleeping difficulties<br />
Problems with balance and movement<br />
Problems with blood pressure and sweating<br />
Digestion and temperature problems<br />
26
Physical<br />
Physical
Chapter Contents<br />
Fatigue and Tiredness<br />
Page 29<br />
Headaches<br />
Page 32<br />
Seizures<br />
Page 34<br />
Movement, Balance,<br />
Co-ordination and Dyspraxia<br />
Page 36<br />
The Five Senses: Touch, Smell,<br />
Taste, Vision and Hearing<br />
Page 38<br />
Swallowing / Dysphagia<br />
Page 40<br />
Bladder and Bowel Issues<br />
(Continence)<br />
Page 41<br />
28
Fatigue and Tiredness<br />
Why am I tired?<br />
After an injury, your brain uses a lot of the body’s energy to heal<br />
and consequently it needs a lot of sleep to help it recover.<br />
Fatigue is extremely common after a brain injury. The sleep your body<br />
craves may be fragmented and can have little effect on the tiredness you<br />
feel. You may find activities tire you quickly, even ones like reading which<br />
are not that physical but require a lot of mental work.<br />
Fatigue may be caused by damage to the part of the brain that is responsible<br />
for wakefulness, consciousness and sleep rhythm. After a brain injury, it<br />
may take longer to recouperate and ‘recharge’ than before your injury.<br />
Ways of coping<br />
Recognise the early signs of fatigue and take it easy,<br />
stop and rest. Do not keep pushing yourself.<br />
Say no to the excessive demands of others. Be open<br />
about your problems with others but don’t go on about<br />
the issues. Beware of sounding like a ‘broken record.’<br />
Plan periods of rest and take naps. Make naps a regular<br />
part of your day and try to have them at the same time<br />
every day.<br />
29
Ways of coping<br />
Do your most demanding activity in the morning when<br />
you have the most mental energy.<br />
Eating a light meal can sometimes help, and drinking<br />
plenty of water.<br />
8pm<br />
Try to establish a set time to go to bed each night and<br />
get up at the same time each day.<br />
walk<br />
nap<br />
read<br />
Vary your daily activities to avoid monotony.<br />
Do I have the<br />
energy?<br />
Pace yourself, do not rush. Learn to stop and think<br />
before you proceed to do an activity. Ask yourself, “Do<br />
I have enough energy to finish? Do I need to break it<br />
down or do it differently?”<br />
Try to avoid doing too much and getting over-tired. A<br />
really busy day can set you back for several days.<br />
When you get tired, expect that tasks will take you<br />
longer to complete.<br />
30
Ways of coping<br />
Avoid high-stimulation locations, such as shopping<br />
malls on busy days.<br />
Sit down to do tasks that you usually do standing.<br />
Allow time for taking mini-rests within that task time.<br />
Flickering fluorescent lights, television and computer<br />
monitors can cause tiredness in some people.<br />
=<br />
Limit your intake of fluids during the evening to avoid<br />
having your sleep disturbed by a full bladder.<br />
limit drinking after 6pm<br />
If necessary, don’t go alone, and ask for assistance.<br />
If possible, avoid shopping during the school holidays.<br />
Carefully plan activities to avoid doing too much and<br />
be aware of too much stimuli.<br />
Cate’s experience<br />
When someone is taking you somewhere, hand over some of the responsibility<br />
for getting there and back. It will save your energy for useful tasks and help you<br />
to be less stressed.<br />
31
Headaches<br />
Headaches are the most common physical complaint people experience<br />
after trauma to the head or neck. A headache can be the result of a<br />
number of different factors, such as pressure from your neck or the base<br />
of your head. You may also get a stabbing headache that may last a few<br />
seconds. Headaches can also be caused by a lack of water (dehydration)<br />
or stress.<br />
Keep a diary of your headaches. Every time you have a headache, recall<br />
the date, time of day, foods recently eaten, your emotions, level of activity,<br />
and anything else you feel is relevant. A diary can help you to modify<br />
your environment and eliminate potential causes of headaches.<br />
Talk to your doctor about possible solutions or ways of coping with<br />
headaches.<br />
Foods that may trigger headaches:<br />
Chocolate<br />
Alcohol (especially red wine)<br />
Avocados<br />
Bananas<br />
Some types of beans<br />
Cheese<br />
Peanut butter<br />
Peas<br />
Pizza<br />
Sour cream<br />
Chicken liver<br />
Coffee<br />
Cured meats (such as bacon, ham)<br />
Fermented, pickled, or marinated foods<br />
Monosodium glutamate (MSG)<br />
Nuts<br />
Onions<br />
Vinegar (except white)<br />
Yeast-raised breads and cakes<br />
Yogurt<br />
Wheat<br />
Sugar<br />
Dairy products<br />
Nutrition is important - eliminate from your diet any foods<br />
that may trigger headaches. If you are not sure which foods<br />
these may be, use the list above as a guide.<br />
32
Ways of coping<br />
Try not to do too much, especially immediately after<br />
your injury. It may be best to aim to do only 2-3 tasks<br />
a day.<br />
Drink water regularly throughout the day and drink<br />
more if you are exercising. It can also help to take<br />
bottled water with you when you go out.<br />
Take time out, either to go for a walk or sit outside in<br />
the fresh air and sunshine - try to relax.<br />
Physiotherapy to loosen up muscles in the base of the<br />
neck, or swimming gently in warm water can also help.<br />
Aquajogging or aquacise can help too.<br />
Use relaxation techniques, breathing or meditation<br />
exercises.<br />
Cate’s experience<br />
The back of my head still aches all the time. The brain ache feels like my brain is<br />
very inflamed and crashing around to get out of my skull - like a game of squash<br />
going on in there. The skull ache is either all over, in one section, or a fine line<br />
along the left side, or is in the middle of my forehead.<br />
I try walking in the fresh air, drink water, rest or get involved in some activity<br />
that helps take the focus off the ache. Medication is usually my last resort for<br />
really bad headaches.<br />
33
Seizures<br />
What are Seizures?<br />
A seizure is a sudden, temporary, unusual discharge of electrical impulses<br />
in one specific area of the brain that may quickly spread, causing<br />
uncontrolled stimulation of nerves and muscles.<br />
Why seizures can occur after a brain injury<br />
Anything that disturbs the normal pattern or activity of the brain can<br />
lead to seizures, which may also be the result of trauma to the brain.<br />
It is not clear what causes seizures but some neurologists think that<br />
trauma excites the nerves within the brain, causing them to go out of<br />
rhythm. A seizure is the body’s effort to correct this irregularity.<br />
Seizures can generally be classified as either “simple” (no change in the<br />
level of consciousness) or “complex”. Seizures may also be classified as<br />
generalized (whole body affected) or focal (only one part or side of the<br />
body is affected).<br />
Most seizures last from 30 seconds to 2 minutes and do not cause lasting<br />
harm. However, it is a medical emergency if seizures last longer than 5<br />
minutes or if a person has many seizures and does not wake up between<br />
them. Seizures can have many causes, including medication, high fever,<br />
brain injury and certain diseases. People who have recurring seizures due<br />
to a brain disorder have epilepsy. Some types of epilepsy are hereditary.<br />
What is Epilepsy?<br />
One in fifty people have epilepsy at some point in their lives and epilepsy<br />
usually affects 1% to 2% of the population. The people affected have<br />
recurring and spontaneous seizures.<br />
Epilepsy can be caused by a severe head injury, stroke, birth trauma, brain<br />
tumour, toxins, brain infection, brain disease, genetic conditions or drug<br />
abuse. In many cases, the cause is unknown.<br />
34
Ways of coping<br />
Take all prescribed medications as directed by your<br />
doctor. If you are having problems with a particular<br />
medication, tell your doctor.<br />
Make sure you eat well and have plenty of sleep and<br />
rest. Avoid stimulants such as coffee, tea, energy drinks,<br />
soft drinks, chocolate and nicotine (smoking) as they<br />
may trigger seizures.<br />
Taking regular exercise is beneficial for overall health,<br />
(for example, swimming, using the gym, yoga, walking)<br />
but avoid strenuous activity that may trigger a seizure.<br />
Always consult your doctor for advice before you<br />
start on an exercise programme.<br />
If you drive, it is important to talk to your doctor<br />
about whether it is advisable to do so. You may need<br />
to wait or be assessed before driving again. Check<br />
with your insurer also.<br />
Avoid any activities or sports that could be dangerous<br />
to yourself and others until your medication dosage<br />
has been regulated.<br />
Avoid unnecessary stress and lack of sleep as these<br />
two conditions can trigger seizures.<br />
My<br />
Seizures...<br />
Let others know about your seizures as this will help<br />
to make them more comfortable, as well as providing<br />
you with valuable help and support.<br />
35
What is wrong?<br />
Movement, Balance,<br />
Co-ordination<br />
and Dyspraxia<br />
The movement and balance parts of the brain may have been damaged<br />
which may mean you either cannot move certain parts of your body or<br />
they will not do what you want them to do. In effect, it may be hard to<br />
co-ordinate parts of your body.<br />
With DYSPRAXIA, the messages from the brain to the parts of the<br />
body you want to move are getting scrambled. A person with dyspraxia<br />
may look as if they are uncoordinated, or when given a command, can not<br />
perform that command immediately.<br />
Ways of coping<br />
A physiotherapist can help improve your movement<br />
or adapt the way you perform a movement to make it<br />
easier.<br />
2<br />
1<br />
3<br />
4<br />
Break down tasks into a series of activities.<br />
Rest between activities.<br />
Repeat each specific activity with physical, verbal or<br />
visual cues, such as an instruction board.<br />
When you get better at each activity sequence, then<br />
the verbal, visual or physical cues can be gradually<br />
withdrawn.<br />
36
Ways of coping<br />
Let people know that you have problems with<br />
movement and/or co-ordination as they may think<br />
you are being lazy, clumsy or are drunk. Practise ways<br />
of saying this that you are comfortable with. Role play<br />
if necessary.<br />
Try different techniques such as the Feldenkrais<br />
method - a series of movements designed to retrain<br />
the body’s movement patterns for pain control and<br />
more efficient motor function. Tai Chi and dance<br />
therapy can also be helpful.<br />
Tricia’s experience<br />
I find walking on soft ground (dirt tracks or sand) very beneficial, rather than<br />
walking on solid footpaths. I also have difficulty walking on uneven surfaces<br />
such as stony riverbanks.<br />
I do find that riding a bike is very good for my lower back pain as it seems to<br />
put me in alignment.<br />
Shane’s experience<br />
I have paralysis on my right side so my balance is not very good. If I find an<br />
area of my body that’s not working very well, I keep working on it. When I first<br />
started walking, I practised a little bit every day, setting small but achievable<br />
goals. Gradually I made the ground a little bit uneven and progressed onto that<br />
as my confidence with walking grew.<br />
When I am tired, my balance is worse. You need to be fresh and rested.<br />
37
The Five Senses:<br />
Touch, Smell, Taste,<br />
Vision and Hearing<br />
What is wrong?<br />
You may not be able to see, hear, smell, taste or feel things as you did<br />
before your injury, and fatigue commonly affects your senses too.<br />
Hypersensitivity is when your skin is extra-sensitive and even light<br />
touching may be uncomfortable.<br />
Why can’t I feel things or why<br />
do they feel different?<br />
You might not have actual damage to the sense organs such as the skin,<br />
eyes, ears or tongue. With a brain injury, the damage has happened in<br />
a part of the cerebrum called the sensory cortex, which receives the<br />
sensations you feel.<br />
Ways of coping<br />
For vision problems, tinted lenses may help if your eyes<br />
are sensitive to the light. The use of an eye patch can<br />
help double or triple vision. Ask your OT to refer you<br />
to a recommended Optometrist if you have any vision<br />
concerns.<br />
To help with touch sensation, rub different textures<br />
over your skin.<br />
Be extra careful with appliances, hot objects or fumes.<br />
38
Ways of coping<br />
Use a timer when cooking and make sure you have a<br />
smoke alarm in the kitchen.<br />
If you are cooking, try not to get distracted - it might<br />
pay to keep the phone off the hook or not answer<br />
it. You may want to use simpler methods of cooking<br />
such as a microwave oven.<br />
To help with taste, try spicy foods or foods with<br />
different textures. This will make eating food an<br />
exciting experience.<br />
When rested and alert, you may notice flavours and<br />
taste more of them.<br />
Shane’s experience<br />
My taste and smell is affected. On my first bite, I can taste it, but when I take the<br />
second bite, I can’t, although when I’m fresh and rested, I can taste food better.<br />
Cooking can become an issue as I need to write down the ingredients I put into<br />
the recipe as taste testing doesn’t work. I don’t go on how I think it tastes, as if<br />
I did, it would be too spicy or salty. If I think the food tastes nice, then it will be<br />
too hot for my partner. And although my sense of smell is affected, there are<br />
the benefits of not having smell in some areas!<br />
I use noise-cancelling headphones to block out extra noises such as computers<br />
and buzzing sounds. People just think I’m listening to music so I don’t look silly,<br />
but it cuts out all the background noise, which is great.<br />
39
Swallowing<br />
(Dysphagia)<br />
Dysphagia is a chewing and swallowing disorder which can occur after a<br />
traumatic brain injury which affects the co-ordination of the swallowing<br />
muscles.<br />
If you have dysphagia, you may have difficulty swallowing, or you may<br />
be experiencing pain while swallowing. Some people have difficulty<br />
swallowing liquids, foods or their saliva. If you cannot swallow normally,<br />
you are at risk of not eating the right foods in order to stay healthy or to<br />
maintain your normal weight. Other risks are foods or liquids entering<br />
the windpipe and becoming stuck, which you may be unable to clear by<br />
coughing or clearing your throat.<br />
Ways of coping<br />
It may be easier for you to eat pureed food, soft food<br />
and thickened liquids to get enough calories. Also avoid<br />
dry foods and breads as these may get stuck in your<br />
throat. Also avoid spicy foods as these can produce<br />
acid reflux.<br />
Try eating several small meals instead of three large<br />
meals a day.<br />
Sitting upright when eating helps food go down easier.<br />
Talk to your rehabilitation team members such as the<br />
dietician and speech language therapist about ways to<br />
manage your swallowing difficulties.<br />
40
Bladder and Bowel<br />
Issues (Continence)<br />
Following an acute brain injury, you may have continence accidents.<br />
Continence means voluntary control over going to the toilet, incontinence<br />
means you are unable to control when you go to the toilet. Continence is<br />
both a cognitive and physical skill – in that the person recognises the signs<br />
that they need to visit the toilet and then acts on the signs. After a brain<br />
injury, these basic skills may need to be relearned or extra time may need<br />
to be allowed. Other factors that can affect continence are medication,<br />
physical disability, communication difficulties and embarrassment.<br />
In cases where incontinence is prolonged, people are usually catheterized,<br />
which involves placing a tube in the bladder. Once the catheter is<br />
removed the person will be retrained until he/she relearns the messages<br />
and signs to use the toilet. Doctors and nurses will help you to establish<br />
a routine.<br />
Ways of coping<br />
When you go out, be aware of nearby toilets in case<br />
you need to go. Make a practice of going to the toilet<br />
before you leave home.<br />
Carry spare clothes and soap with you in case of an<br />
accident.<br />
Wear special incontinence pads if you think you might<br />
have an accident. Have spares handy.<br />
41
Ways of coping<br />
Ask your doctor about medication that can help with<br />
incontinence.<br />
Shane’s experience<br />
Early on, I used to write in my diary if I had been to the toilet because I would<br />
forget if I’d gone or not, and think I’d need to go even if I’d just been. A lot of<br />
the time, your body doesn’t know, so I’d think, ‘Do I need to go to the toilet?’,<br />
and if it’s written down, it’s easy to know if you might need to go again. This is<br />
especially important in the initial stage after your accident.<br />
Melinda’s experience<br />
I didn’t have a problem until my stress levels increased. My clinical psychologist<br />
told me that changes in bowel function, such as having diarrhoea or constipation,<br />
can occur from increased stress levels.<br />
Another thing was that I had constipation because of the pills I had to take. A<br />
doctor said to me I can either take more medication to alleviate the constipation<br />
or have kiwifruit juice everyday. It was the best advice I was given. Now when I<br />
take my pills, I have my kiwifruit juice - it is part of my medication routine.<br />
42
Cognitive<br />
Thinking<br />
(Cognitive)
Chapter Contents<br />
Vision and Perception Issues<br />
Page 45<br />
Communication Issues / Aphasia<br />
Page 47<br />
Planning, Organising and<br />
Problem-Solving<br />
Page 49<br />
Attention and Concentration Issues<br />
Page 51<br />
Memory Issues<br />
Page 54<br />
44
Vision and Perception<br />
Issues<br />
You may be confused by similar sounding words or not understand what<br />
people are saying. You may have difficulty with vision and you may have<br />
a lack of awareness of one side of your body.<br />
Why is my brain slower at understanding and<br />
acting upon information?<br />
Your brain may have been shaken and the millions of pathways that<br />
carry information may be damaged, which means they no longer run as<br />
smoothly and quickly as they did before your brain injury.<br />
Ways of coping<br />
Create your environment. If you need peace and quiet,<br />
go where that is available.<br />
If you can only handle short periods of conversation,<br />
let other people know this.<br />
Take a dictaphone to record conversations if you think<br />
the conversation will be longer than what you will be<br />
able to cope with.<br />
45
Ways of coping<br />
If possible, ask for written as well as verbal formats so<br />
that you can check and double-check your work.<br />
Use maps where possible. Mark where you need to go<br />
and where you have come from.<br />
Cate’s experience<br />
If you can’t bear looking at maps, I find it helpful to ask someone to take me there<br />
first and check out steps and stairs etc. The second time I go alone prior to the<br />
appointment and the third time I make the journey, I can function when I’m there<br />
(at the destination).<br />
46
Communication<br />
Issues / Aphasia<br />
What is wrong?<br />
Expressing yourself or understanding what you hear or read may be<br />
affected by your brain injury. Speech may be unclear or it may be hard<br />
to find the words you want. Poor memory or attention may affect your<br />
ability to talk or recall information. It may also be more difficult to follow<br />
the social rules of conversation than before your brain injury.<br />
Aphasia is when you have problems with speech and comprehension<br />
of words. Depending upon the damage to the brain, it may mean you<br />
can speak, but not write, or you may be able to sing, but not speak.<br />
Another common form of aphasia is when you say one word when you<br />
meant to say another, such as ‘Pass me the fridge..’ when you meant to<br />
say, ‘Pass me the butter...’.<br />
Why?<br />
As a result of your injury, there may have been damage to a cranial nerve<br />
in the brain which affects the way you speak or swallow food.<br />
Ways of coping<br />
Look at people’s facial expressions to see what they<br />
are saying.<br />
Try to have important information written down in an<br />
easily accessible place that you will remember.<br />
A speech language therapist can help you with<br />
communication difficulties, such as expressing yourself<br />
clearly.<br />
47
Ways of coping<br />
Pause and take a breath before speaking.<br />
Take your time.<br />
Be aware of repeating yourself or how often you say a<br />
phrase (for example, ‘have I told you about?).<br />
or<br />
Talking is a lot harder when you are tired. Try to rest<br />
if you are having difficulty talking.<br />
Melinda’s experience<br />
In the beginning, I lacked the ability to communicate socially and nicely, so I’d just<br />
come out and say what I thought. There was no social build-up, so no social niceties<br />
such as ‘Hi, how are you?’. I’d just state what I wanted or needed. This came<br />
across as rude to other people but I wasn’t aware of being rude. Your brain is in<br />
survival mode, so you say the minimal amount. All the ‘fluff’ that goes on around<br />
conversations is not there; you have to relearn that again.<br />
Shane’s experience<br />
I really try not to think that I know what the person is about to say. I prefer to<br />
see people in person as I find their body language helps with what they are<br />
communicating to me – it’s easier to interpret what they might be saying if you<br />
can see their facial expressions.<br />
I also try to let people talk. I’m a big talker so I need to let people have a chance<br />
to talk and I try to make sure I hear all sides to the story before making up my<br />
mind.<br />
48
Planning, Organising<br />
and Problem-Solving<br />
If you have damaged the front part of your brain – the frontal lobe - you<br />
may have problems with planning activities, getting things in the right<br />
sequence and evaluating possible errors. Because of this, you may find it<br />
difficult handling multiple activities.<br />
Ways of coping<br />
Your Occupational Therapist can assist in planning and<br />
organising your time to achieve your daily tasks.<br />
Do one thing at a time.<br />
Plan what you are going to do, then write a list and tick<br />
off as you go. Have lists for different activities that you<br />
do on a regular basis. Laminate your list and put it in an<br />
obvious place to remind you.<br />
Do not rush, take your time.<br />
49
Ways of coping<br />
1. Turn on jug<br />
2. Get cup<br />
3. Put in tea bag<br />
4. Pour water<br />
5. Pour milk<br />
6. Drink and<br />
enjoy!<br />
Write down each step or activity.<br />
Break tasks into small steps.<br />
Keep stimuli or noise down to a minimum.<br />
Paper diaries are great for people who prefer not<br />
to use electronic diaries such as a cell phone<br />
or computers.<br />
Do not be too proud to ask for help, and if help is<br />
offered, accept if needed.<br />
Cate’s experience<br />
If I have a plan and someone else makes a change, I am likely to have an<br />
accident, or other symptoms kick in until I can process the changes that I<br />
haven’t made. I cannot carry out someone else’s plan until I have had the<br />
chance to process it.<br />
Melinda’s experience<br />
Before my accident, I loved projects and completing tasks and goals. After<br />
the injury, I lost my ability to multitask. I remember saying to the health<br />
professionals, ‘I’ve become a bit like a man, I’ve lost my ability to multitask’. We<br />
all had a laugh.<br />
50
Attention and<br />
Concentration<br />
Issues<br />
Attention is a process which lets you focus on information coming in<br />
from your surroundings. Concentration requires your attention for a<br />
set period of time. You may not realise that your ability to concentrate<br />
is any different to what it was prior to your injury. You may be more<br />
easily distracted or have trouble keeping track of what is being said or<br />
done. People may mistake your inability to maintain attention as a lack of<br />
motivation or intelligence.<br />
Attention can be divided into five levels:<br />
• Focused attention<br />
This is the kind of attention used when we are actively attending to<br />
something. It is our ability to attend to one thing to the exclusion of<br />
everything else. For example, when you are studying or driving.<br />
• Sustained attention<br />
The ability to concentrate on one task for a certain period of time<br />
without switching off. Many people with a brain injury find they lose<br />
concentration quite quickly.<br />
• Selective attention<br />
This is when you have the ability to avoid all distractions and focus on<br />
one thing. For example, after a brain injury you may not be able to read<br />
a letter when there is a radio playing in the background.<br />
• Alternating attention<br />
The ability to shift the focus of attention and to alter it<br />
between tasks.<br />
• Divided attention<br />
This is the ability to respond to multiple tasks at the same time, or to<br />
give two or more responses simultaneously. For example, you might be<br />
watching television while eating your breakfast. After a brain injury, some<br />
people find that they are unable to concentrate on more than one thing<br />
at a time.<br />
(Referenced from www.headwayireland.ie/)<br />
51
Ways of coping<br />
Keep to regular sleep times and before periods of<br />
attention and concentration, remove yourself from<br />
stimulus to a quiet place.<br />
Be aware of times when you may be more alert, such<br />
as in the mornings.<br />
When setting out tasks, consider what steps are<br />
involved in order to complete the task.<br />
If possible, try to eliminate background noises such<br />
as radios and people talking. Try using earplugs or<br />
noise-cancelling headphones.<br />
Silently tell yourself ‘Pay attention!’.<br />
Ask people to repeat themselves or speak slower if<br />
they are speaking too fast or you do not understand<br />
them.<br />
Have regular breaks.<br />
52
Ways of coping<br />
John<br />
John<br />
John<br />
If someone tells you their name, a way to remember<br />
it is to repeat it back to them. It may also help to<br />
paraphrase what has just been said to you to let the<br />
person know you understood what they have said.<br />
Answerphones are useful as you can keep listening to<br />
them for clarification.<br />
Write down or record distracting internal thoughts<br />
to get them out of your head until you have<br />
time to think them through.<br />
Cate’s experience<br />
I frequently forget mid-sentence what I’m talking about so I usually ask the other<br />
person what was I talking about. I also might say ‘cupboard’ instead of ‘fridge’ or<br />
‘chapter’ instead of ‘page’.<br />
53
Memory Issues<br />
What is memory?<br />
Your brain has suffered damage and as a result you may have difficulty<br />
remembering things in any of the three categories below. Things that<br />
may make your memory worse are a lack of sleep, stress and fatigue. It<br />
is important to remember that the memory is like a muscle - the more<br />
you use it, the stronger it gets.<br />
There are three types of memory:<br />
Immediate/sensory memory<br />
Short-term memory<br />
Long-term memory<br />
held for a few seconds<br />
held for a bit longer<br />
consists of memories of personal<br />
experience, learned behaviour<br />
and knowledge and information<br />
Loss of memory is also called amnesia.<br />
Types of amnesia include:<br />
Anterograde amnesia<br />
Retrograde amnesia<br />
Global amnesia<br />
memory loss that occurs following<br />
the event that caused the brain injury<br />
memory loss that occurs prior to the<br />
accident or event that caused the brain<br />
injury.<br />
a total loss of memory<br />
Ways of coping<br />
Use a diary, notebook or dictaphone everyday.<br />
54
Ways of coping<br />
Wall calendar planners or computer calendars are<br />
very useful.<br />
Label things such as household items, rooms or<br />
anything you have difficulty remembering.<br />
Write ‘to do’ lists for each day.<br />
Have a place for everything in your home, such as a<br />
filing system for bills and letters.<br />
Make sure you keep it in an easily accessible place.<br />
Keep a pack of post-it notes with you to remind you<br />
of tasks.<br />
Use a watch with an alarm to help you remember<br />
things such as when your dinner is cooked. It may also<br />
be helpful to use an oven-timer.<br />
Repeat things to help you remember them, such as<br />
people’s names. Try not to take it personally or think<br />
badly of yourself if you forget.<br />
55
Ways of coping<br />
Create an association with a name by relating it to<br />
something else - maybe a picture.<br />
Put things back in the same place after use.<br />
Shane’s experience<br />
I have a little diary or notepad and find they are better than pieces of paper<br />
everywhere. I use my reminder on my cellphone a lot too. My memory has<br />
been affected like a lot of people with brain injuries. My short-term memory is<br />
OK, but my mid-term memory is bad, so I have problems remembering, anything<br />
around five hours ago, but my long-term memory is OK. I also try to associate<br />
words with people’s names, like if they are tall and their name is Tanya, I think,<br />
‘tall Tanya like a tree’. Plus I’ll repeat people’s names back to them to help me<br />
remember their name.<br />
Melinda’s experience<br />
My memory is coming back as it’s getting better all the time. I found the worst<br />
thing affected was my short-term memory with my medium and long-term<br />
memory not so much. When I get fatigued, I turn into what I call ‘brain-injured<br />
Melinda’ . I know it is just me, but I really don’t like ‘brain injured Melinda’. She<br />
has no tolerance for others and no short-term memory.<br />
In the beginning, I had trouble recalling things. A major problem I was having was<br />
that I’d have breakfast and wash my dishes, then I’d have breakfast again and do<br />
this sometimes up to six times. I put on two-and-a-half stone, until I realised what<br />
was going on. Now I wash all my dishes from the day before, have breakfast, and<br />
leave the dishes to let me know I’ve eaten already.<br />
My brain injury likes routine. Routine means the brain can conserve energy. Now<br />
I have lots of ways to save energy.<br />
56
Emotional<br />
Emotional
Chapter Contents<br />
Anger, Frustration,<br />
Depression and Anxiety<br />
Page 59<br />
Sexual Issues<br />
Page 62<br />
Behaviour, including Self-Centredness<br />
Page 65<br />
Lack of Motivation<br />
Page 67<br />
Emotional Extremes<br />
Page 69<br />
58
Why do I feel like this?<br />
Anger, Frustration,<br />
Depression and<br />
Anxiety<br />
After a brain injury, you may experience feelings of anger and irritability.<br />
This is because there is often direct damage to the parts of the brain that<br />
are involved in controlling behaviour. You may feel as if you are on an<br />
emotional roller-coaster and little things may upset you.<br />
The middle section of the brain is quite primitive, much like an animal’s<br />
brain. This is the automatic response area of the brain which means that<br />
you do something without consciously thinking about it. The front part of<br />
the brain is the bit that rationalises before you ‘act upon your emotions’.<br />
It may be this part that is damaged, making it hard for you to control the<br />
way you act and feel.<br />
Ways of coping<br />
When you feel very angry and want to hit out at<br />
something or someone, try to redirect your thoughts<br />
away from who or what is making you angry.<br />
Some people find that deep breathing and relaxation<br />
techniques such as yoga can be helpful. These can be<br />
particularly helpful before you sleep.<br />
Sorry<br />
If you have upset someone as a result of your actions<br />
or words, make them aware that it may be as a<br />
consequence of your injury. It might be helpful to also<br />
apologise to them.<br />
59
Ways of coping<br />
If possible, begin a light, daily exercise programme.<br />
Try not to be too hard on yourself. Lowering your<br />
expectations of yourself and/or others will lower<br />
anxiety.<br />
1 2 3 4 5<br />
6 7 8 9 10<br />
Count to ten. It’s simple and a good distraction.<br />
If you feel you are ‘losing it’, remove yourself from the<br />
situation and calm down before returning.<br />
Express yourself assertively. Talk it out, rather than<br />
bottling it up and allowing resentment to build.<br />
Find someone who is prepared to listen.<br />
Identify the triggers - recognise the situations that<br />
wind you up, then either avoid them or work out a<br />
better way of coping.<br />
Take time out for at least 15 minutes if you feel you<br />
are about to lose control. The more time out you<br />
have, the more you learn to control your feelings and<br />
outbursts.<br />
60
Ways of coping<br />
Talk through how you feel with somebody who is a<br />
good listener.<br />
Get involved in a brain injury support group, as talking<br />
to others in a similar situation helps.<br />
Ask yourself ‘What can I do?’, not ‘What can’t I do?’<br />
Try not to focus too much on yourself and be more<br />
aware of how others are feeling.<br />
Melinda’s experience<br />
After my accident, people such as bus drivers and supermarket staff often<br />
thought I was angry at them as I’d raise my voice, but I was just frustrated<br />
at myself, at my inability to communicate with them effectively. However, I<br />
found ways to avoid that, such as sitting down to rest for 5 minutes before<br />
catching a bus. I also go to the supermarket at less busy times, such as early<br />
in the morning or late at night.<br />
Shane’s experience<br />
I was placed on depression tablets after my accident. I hate medication<br />
and I like to do things as naturally as possible, so I tried to get off them as<br />
soon as possible. Doctors told me I’d never play sport or work again, so I got<br />
depressed and for good reason! I remember I went for a walk into a part of<br />
the hospital where there were people worse off than myself and I actually<br />
felt lucky. I try to concentrate on the positive aspects of what I can do and I<br />
do the things I enjoy, such as gardening. I really love the feeling of dirt on my<br />
hands, it’s very relaxing.<br />
61
Sexual Issues<br />
Sexual difficulties can occur after a traumatic brain injury which will<br />
depend on the severity of the injury. Some people may feel embarrassed<br />
or uncomfortable talking with hospital staff about their concerns. So<br />
information about sexual difficulties and problems is very important.<br />
Why is sexuality affected by a brain injury?<br />
In the centre of the brain there is a structure known as the hypothalamus,<br />
which plays an important role in regulating sex drive by controlling the<br />
release of sex hormones. Following an injury, this part of the brain can be<br />
damaged and result in sexual appetite and behaviour being affected.<br />
After a brain injury some people may find that they are<br />
experiencing changes to their sexuality which may consist of<br />
the following:<br />
• A lower sex drive: some people comment that they have a lower<br />
sex drive after a traumatic brain injury. While others comment<br />
that there has been no change or that their sex drive has<br />
increased.<br />
• Disinterest in sex or not having sex as often as before the injury:<br />
This can be due to sexual problems, relationship break-ups,<br />
problems in forming new relationships, depression or stress, and<br />
physical disability.<br />
• Problems with erections: some men experience erectile<br />
problems or impotence for a short time after a traumatic brain<br />
injury.<br />
• Problems with orgasms: some men may have problems with<br />
having orgasms. This does not appear to be a significant problem<br />
for women after a brain injury.<br />
Certain medications can lessen your sex drive, you will need to talk to<br />
your GP about whether the medication you are taking may be a cause.<br />
Other factors are fatigue, stress, depression and anxiety. Depression,<br />
anxiety and stress are common after a brain injury and can affect a<br />
person’s sexuality by lowering their sexual response and desire.<br />
62
If the brain injury occurred in a car accident, the person may have<br />
sustained other injuries, e.g. spinal cord damage, injuries to the pelvis and<br />
hip bones or nerve damage. Any of these injuries will have an affect on a<br />
person’s sexual functioning.<br />
Other factors that can affect your sexuality after a brain injury is<br />
something called ‘sexual disinhibition’ this is where the person with a<br />
traumatic brain injury does or say something that is inappropriate or that<br />
may cause offence.<br />
People often ask the question, when is it ok to resume a sexual relationship<br />
after a brain injury. Like any other activity, sex can make your heart beat<br />
faster, if you have been having regular exercise then this should be ok.<br />
Fatigue is probably the biggest problem as you may tire easily after sex.<br />
Communicate with your partner, let them know how you feel and share<br />
any worries that you may have. If you feel that you are not ready physically<br />
and emotionally then wait until you feel that you are ready.<br />
It’s important to discuss any concerns that you have with your doctor<br />
counsellor or family member. If you are a member of a Brain Injury<br />
Support Group, the support worker will be a valuable source of help.<br />
Ways of coping with DECREASED sexual interest<br />
Try some relaxation techniques such as meditation,<br />
yoga or tai chi.<br />
Communicate openly with your partner. Maybe ask<br />
them for physical contact of a non-sexual nature.<br />
Sometimes counselling or other therapies can help.<br />
Making an effort with your appearance can help to<br />
boost confidence and self-esteem.<br />
63
Ways of coping with INCREASED sexual interest<br />
Accept and acknowledge any inappropriate behaviour<br />
you may be displaying to others.<br />
Communicate and be open with your partner about<br />
your increased sexual desire.<br />
If someone you like does not share the same feelings<br />
you have, do not worry too much as this can happen<br />
to anyone.<br />
For further information, ask a counsellor or<br />
psychologist to recommend books or other sources<br />
of information that may be helpful.<br />
Melinda’s experience<br />
There was a man and a lady living in an old persons’ home. They had liked each<br />
other for a long time. One day, the man finally plucked up his courage and said,<br />
‘Mabel, would you like to go upstairs and make love?’.<br />
Mabel replied, ‘Oh Arthur, I can only manage one or the other!’<br />
- and I thought “That is so brain injury - only one task at a time!”<br />
64
Behaviour, including<br />
Self-Centredness<br />
Why am I acting like this?<br />
Because of your injury, you may behave in a way that others around<br />
you feel is childish or inappropriate. Perhaps you have been resentful<br />
of people telling you what and what not to do. Appropriate behaviour<br />
will need to be relearned. Be aware of what others say to you, because<br />
although you may think what you are doing is fine, it may not seem<br />
appropriate to those around you.<br />
Ways of coping<br />
Consult a therapist if you have concerns that people<br />
are ignoring you. They may be able to help with advice<br />
on how to engage with others.<br />
If others tell you that you are acting inappropriately,<br />
listen to them. Ask your friends to be open and<br />
honest.<br />
Practice stopping and thinking things through before<br />
acting them out.<br />
Keep a diary and record details of your thoughts and<br />
feelings - this will help you to become better at sensing<br />
when you are about to do something inappropriate.<br />
65
Shane’s experience<br />
Behaviour and self-centredness – that’s a big one with people with a brain<br />
injury. People are quite self-centred, so I always tried to think of other people.<br />
I try to take time out before I act and not tell people about my injury as you<br />
don’t need to tell everyone everything. Try not to get angry when people say ‘I<br />
forget all the time’, because often people do forget things. I find it helpful to<br />
think that I’m not the only one with a problem.<br />
Cate’s experience<br />
Yeah, I think I got self-centred after my injury. I regret it afterwards and wish I<br />
had listened to others more.<br />
When you are with others, try to gauge when it’s OK to talk about yourself, and<br />
just enjoy being with others. You can recover later without others knowing, and<br />
you’ll still be able to enjoy their company at other times too.<br />
I’ve also found that it’s good to be aware of what other people may be feeling<br />
or coping with. Their load may be as difficult, yet different from yours.<br />
66
Lack of Motivation<br />
Lack of motivation is a direct result of frontal lobe damage. You may<br />
be unable to plan activities or ‘think about the future’. Thinking about<br />
goals can often be overwhelming. It may seem easier to sit back and do<br />
nothing.<br />
As time passes, a lack of motivation can lead to friends not contacting<br />
you, a lack of pleasure and a kind of ‘depression’ or numbness of the<br />
mind. A lack of motivation can lead to isolation.<br />
Ways of coping<br />
Break down activities into small steps - this will make<br />
them seem less overwhelming.<br />
Focus on each step, one at a time.<br />
Get involved with a brain injury support group. This<br />
will lead to support from other members with similar<br />
issues.<br />
Structure your day and get into a regular routine. This<br />
will encourage you not to rely on your own motivation<br />
to do things.<br />
67
Ways of coping<br />
Recognise that your lack of motivation is not a sign of<br />
depression and help make family and friends aware of<br />
this.<br />
Set short-term and long-term goals.<br />
Write down your goals and put them in an obvious<br />
place.<br />
10 min<br />
of<br />
Tell people about these goals. This will ensure that they<br />
keep asking you about how they are coming along and<br />
provide accountability.<br />
Donald’s experience<br />
I might not be as quick doing jobs or other things now, but I do get them<br />
done. I don’t pull out halfway through, or what I’m doing will never get done.<br />
It’s about just getting things done.<br />
Shane’s experience<br />
I set myself goals, even if they are small ones like setting a time to get up.<br />
I plan ahead and then I’m motivated to get up, even if it’s to do some cleaning<br />
or helping the neighbours. I try to ask busy people to do things for me as they<br />
are usually well organised so tend to get things done!<br />
I also tell people my goals, and then there’s a high chance they will ask you<br />
about them down the track which motivates you to carry out the goals.<br />
68
Emotional Extremes<br />
Why do I feel like this?<br />
Emotional extremes are generally due to damage to your frontal lobe, or to the<br />
parts of the brain that produce certain mood neurotransmitters, such as serotonin.<br />
You may also suffer from frequent mood swings.<br />
Due to your injury, your emotions may be affected. They may be either really intense,<br />
or may seem to have disappeared. Some people say it feels like you are a robot.<br />
At the other extreme, you may want to laugh or cry at the smallest of things.<br />
Ways of coping<br />
If you feel flat, keep a diary monitoring your emotions<br />
and try to link your thoughts to feelings. This will help<br />
link up the pathways between thought and emotion.<br />
If you are highly sensitive to emotions, change the topic<br />
of conversation or distract yourself with an activity.<br />
As a way of distraction, try to do the opposite of what<br />
you are doing physically (e.g. change from sitting to<br />
standing).<br />
Explain your situation to others and make a joke of it<br />
if you can.<br />
69
Ways of coping<br />
Be open about the situation. People should understand<br />
that your actions are due to your brain injury.<br />
Do not be afraid to get professional help.<br />
Shane’s experience<br />
Since my accident, I get very emotional – I love watching “chick flicks” with<br />
my wife now. I actually find with action ones, there’s too much happening, too<br />
much of a story line, whereas chick flicks are just about love and it’s quite slow<br />
paced – my wife thinks it’s great! I do cry though, and I’m not embarrassed as<br />
it’s actually a beautiful emotion.<br />
Melinda’s experience<br />
Before my brain injury, I only ever cried if something, or someone died. Now I<br />
have found myself bursting into tears, for example when I went into a car repair<br />
place, they did a small repair and didn’t charge me and I burst into tears with<br />
gratitude, and that’s so not me. It’s like I can’t control these little outbursts. Also<br />
I freak out if my routine is changed unexpectedly, especially if I’m fatigued.<br />
70
Life after<br />
brain injury<br />
Life
Chapter Contents<br />
Brain Injury in New Zealand - Statistics<br />
Page 73<br />
The Rehabilitation Team<br />
Page 74<br />
Family / Relationships<br />
Page 77<br />
Getting Back to Work<br />
Page 84<br />
Driving After a Brain Injury<br />
Page 88<br />
Nutrition / Alcohol<br />
Page 92<br />
Exercise / Brain Gym<br />
Page 96<br />
Socialising / Recreation<br />
Page 98<br />
72
Brain Injury in<br />
New Zealand – Statistics<br />
10,000 to 17,000 people per year<br />
acquire brain injuries in NZ.<br />
50% of severe brain injuries<br />
are due to car accidents.<br />
According to the Brain Injury Association,<br />
brain injury can be caused by the following:<br />
• In 2006, the New Zealand Guidelines Group<br />
and ACC, estimated that approximately<br />
10,000 to 17,000 people needed hospital<br />
care for a brain injury.<br />
•<br />
• 8% to 10% of those admitted to hospital<br />
with a brain injury will be in the moderateto-severe<br />
category.<br />
•<br />
• 50% of those admitted to hospital with a<br />
severe brain injury will be due to motor<br />
vehicle accidents.<br />
traffic accidents<br />
injury at birth<br />
sporting accidents<br />
tumours<br />
accidents at home<br />
drug and alcohol abuse<br />
industrial accidents<br />
near drowning<br />
strokes<br />
other factors<br />
Some groups in the community are more likely to have a brain injury than others:<br />
Young adults aged 15 - 19, especially males.<br />
Children in the age group 0-4 years as a result of falls from<br />
playground equipment, windows and stairs, and physical abuse.<br />
The elderly aged 60 or over, mainly from falls in the home.<br />
73
The Rehabilitation Team<br />
These are some of the people who may be involved in your recovery.<br />
They are here to help you become as independent as possible.<br />
Doctor<br />
The doctor is the team member responsible for your<br />
rehabilitation programme and for taking care of the medical<br />
aspects of your treatment. The doctor keeps you, your family<br />
and referring doctor informed about your progress.<br />
Key/Primary Nurse<br />
Nurses work with the rehabilitation team to solve problems<br />
and manage medical issues. Key / primary nurses are experts<br />
in bladder, bowel, nutrition, pain, skin integrity, breathing, selfcare,<br />
co-ordination of medical regimens and related issues.<br />
They provide ongoing patient and family education and help<br />
you set goals for maximum independence.<br />
Occupational Therapist<br />
An occupational therapist (OT) is skilled in helping you<br />
learn, or relearn, the day-to-day activities needed to achieve<br />
maximum independence and quality of life. OTs offer treatment<br />
programmes to help you with bathing, dressing, preparing a<br />
meal, house cleaning, arts and crafts activities or gardening.<br />
They make recommendations and offer training in the use of<br />
adaptive equipment to help with issues related to your injury.<br />
OTs also help with any changes you might need to your home<br />
or workplace.<br />
Physiotherapist<br />
A physiotherapist’s aim is to help you increase your physical<br />
strength as well as improve your co-ordination, reduce<br />
spasticity, maintain muscles in paralysed limbs, protect skin<br />
from pressure sores and help you gain greater control over<br />
bladder and bowel function. They can also teach you to use any<br />
assistive devices you may need, such as a wheelchair.<br />
74
Speech and Language Therapist<br />
A speech and language therapist (SLT) helps with problems you<br />
may have with your speech, language, and communication skills.<br />
You may need help in making your speech easier to understand<br />
or in being able to say what you want in speech or writing.<br />
You may be having a hard time understanding what people are<br />
saying to you or you may have some difficulty reading. The SLT<br />
will work with you to improve your skills and will also help<br />
you learn ways to deal with these changes. You may also<br />
have problems with swallowing as a result of damage to the<br />
brain stem. A speech and language therapist can help in this<br />
area too.<br />
Dieticians<br />
Dieticians are specially-trained experts in food and nutrition<br />
and aim to promote good health through good nutrition. They<br />
will advise you about your nutritional requirements which are<br />
important in promoting recovery and healthy living.<br />
Clinical Psychologist<br />
Clinical psychologists are involved in dealing with the emotional<br />
and behavioural problems that occur after a brain injury.<br />
Neuropsychologist<br />
Neuropsychologists are clinical psychologists who specialise<br />
in brain injury and behaviour. They will carry out assessments<br />
to identify problems you may have with thinking, memory and<br />
perception. A Neuropsychologist can help you to understand<br />
the changes in your thinking, memory or behaviour that<br />
are due to your illness or injury. You may be given tests to<br />
assess a range of thinking and memory skills. The results of<br />
these tests can help to create the right treatment for you.<br />
The Neuropsychologist can also assist you and your family to<br />
understand how changes in thinking and behaviour may affect<br />
living in the community.<br />
75
Social Worker<br />
The social worker will help you to maintain and strengthen<br />
links with family, friends and the wider community and assist<br />
with access to community resources and entitlements.<br />
Social workers are responsible for arranging social security<br />
benefits, and ACC benefits and also arrange appropriate<br />
living accommodation once you are ready to return to your<br />
community.<br />
Other therapists you may find in the rehabilitation<br />
unit include:<br />
• Recreation therapists/officers who can help you discover the wide<br />
range of recreation options available in their community.<br />
•<br />
•<br />
• Vocational rehabilitation specialists who can help you assess your job<br />
skills with a view to returning to work. A vocational rehabilitation<br />
specialist will arrange additional training and educational opportunities<br />
to help you achieve your vocational goals. They also work with other<br />
agencies to obtain equipment, training and placement.<br />
76
Family / Relationships<br />
Your brain injury will have a big impact on your family, especially if you are<br />
experiencing emotional or behavioural problems because of your injury.<br />
Families that cope better with a brain injured member, seem to have a<br />
more flexible attitude and embrace change, seeing it as a challenge rather<br />
than a problem. It helps if there is open communication between all the<br />
parties involved, from the person who has had the injury to the family<br />
and the professionals involved in the rehabilitation process. The family will<br />
also need to have a positive attitude, treating the person with warmth and<br />
respect and not seeing him/her as a burden.<br />
Family members will generally go through a series of emotions after you<br />
have had your injury. These are:<br />
Shock and panic.<br />
Seeing you injured can create feelings of anguish, confusion,<br />
hopelessness and frustration at having no control over<br />
the likely outcome.<br />
Relief, elation and denial - there is<br />
disbelief at what has happened.<br />
Once the life-threatening phase has passed, there<br />
is often a sense of relief. Your family will be full of<br />
expectancy, optimism and hope for a full recovery.<br />
They may want to deny or ignore changes in you.<br />
Denial of the consequences of your injury may be<br />
strengthened by a number of factors. Medical predictions about your<br />
recovery may be different to what has actually happened in terms of your<br />
recovery. Doctors may have said you would remain comatose or never<br />
walk or talk again and yet, in reality, you may have made a better recovery<br />
than predicted. This may cause you to lose faith in the medical profession<br />
and what they tell you. In reality, it is extremely difficult to predict your<br />
outcome, especially over time. An awareness of the reality of your injury<br />
usually comes after you leave hospital and are back home.<br />
77
Hope - things are hard but<br />
they will get better.<br />
Due to the uncertainty surrounding the exact outcomes<br />
of your brain injury, family members will often focus<br />
on a physical disability that may show relatively rapid<br />
improvement, rather than cognitive and behavioural<br />
changes, that tend to take longer to show an improvement.<br />
They may assume that with faith, determination and hard work, problems<br />
will be overcome. Alternatively, there may be an expectation that medical<br />
science will find a cure for your injury.<br />
Realisation, anger, depression<br />
and mourning - the family<br />
member may not get better<br />
The reality of how your injury has affected your life will<br />
become apparent once you leave hospital and go home.<br />
You may start to feel angry at either yourself, your<br />
family, medical staff or anyone involved in your accident.<br />
There may be feelings of guilt or regret over what could<br />
have been done to prevent the injury. There may be disruptions in the<br />
relationships you had with different family members, such as your partner,<br />
your children or your parents. They may find that they also need to help<br />
you with your recovery.<br />
Acceptance and recognition -<br />
it’s time to get on with life, even<br />
though things may be different.<br />
Although this stage of your recovery may take a long<br />
time to arrive, it will happen. That’s not to say you will<br />
not revisit past stages, but a form of acceptance should be possible for you<br />
and your family.<br />
78
Ways of coping for YOU<br />
Avoid triggers that may make you angry,<br />
such as a specific person or place.<br />
Breathe,<br />
count to 10<br />
If you feel that you are getting angry, try to calm<br />
down by taking a few deep breaths, count to<br />
ten and talk to the person about the issue or<br />
problem.<br />
Sometimes your family may be right and their ideas<br />
may be good ones - be open to their suggestions.<br />
You may need to prove your abilities to your family<br />
members a few times (for example, driving a car).<br />
Other responsibilities and privileges will return<br />
once you have shown them your capabilities.<br />
Be patient.<br />
Communicate respectfully with family and friends.<br />
This may be hard if the part of your brain that<br />
controls anger is damaged. You may need help<br />
with retraining in communication skills.<br />
Support Group<br />
Encourage family members to join a brain injury<br />
support group with you.<br />
If your relationships with family members and<br />
friends are strained, seek outside counselling.<br />
79
Ways of coping for YOU<br />
Generate fresh friendships and networks.<br />
Ways of Coping for<br />
FAMILY AND FRIENDS<br />
Acknowledge that in the early medical stages,<br />
the situation is out of your hands. Trying to take<br />
control will only lead to frustration and panic.<br />
Express how you are feeling and make sure you<br />
do not bottle your feelings up.<br />
Learn relaxation techniques. It is important you<br />
take time out in order to be there emotionally<br />
and physically for the affected family member.<br />
Delegate responsibilities as people will often want<br />
to help but do not know how.<br />
Take one day at a time - this makes it easier to see<br />
the small signs of progress.<br />
Ask the health professionals to share information.<br />
The more informed you are about the condition<br />
of your family member, the better equipped you<br />
will be to deal with the situation.<br />
80
Ways of coping for FAMILY AND FRIENDS<br />
You will need to work through a series of emotions<br />
as you go through each stage. If possible, talk to a<br />
counsellor.<br />
It’s normal to feel down<br />
Acknowledge that acceptance of the situation may<br />
not come for a while. It is normal to feel upset,<br />
angry or depressed. Crying helps and is normal.<br />
I can not change what happened<br />
Accept that you are not responsible and that taking<br />
the blame will not alter what has happened.<br />
Talk to your family member the way you used to.<br />
but understand that they will be different.<br />
Future<br />
Accept that the past is behind you and the future<br />
is what is important.<br />
Past<br />
Make the most of what your family or friends can<br />
do. Do not concentrate on what they cannot do.<br />
Look after yourself first and foremost. You are no<br />
good to anyone if you are tired and grumpy.<br />
81
Ways of coping for FAMILY AND FRIENDS<br />
Put off until tomorrow what is not absolutely<br />
necessary.<br />
What do<br />
you think?<br />
Let the person with the brain injury make as many<br />
decisions as they can cope with and ask their<br />
opinion even if that is not totally necessary.<br />
Do not give up your job unless it is absolutely<br />
necessary.<br />
Both carer and cared-for need time on their own.<br />
This is extremely important and may need to be<br />
strictly scheduled.<br />
help?<br />
Discuss role changes with other family members<br />
and ask for help if necessary.<br />
You may need to take responsibility for<br />
implementing changes in roles, and in other areas<br />
such as time out. Be aware that the person who<br />
has had the injury may still see themselves as they<br />
were before the injury.<br />
View change as a challenge and an opportunity<br />
rather than a problem.<br />
change<br />
82
Ways of coping for FAMILY AND FRIENDS<br />
Recognise that in order for your family member to<br />
make progress, they will need to take risks such as<br />
travelling alone. These risks will need to be taken if<br />
real progress is to be made.<br />
Allow the person to make a few mistakes, but not<br />
too many so that they lose confidence and dignity.<br />
Make some tasks easily achievable to build up their<br />
confidence.<br />
Try to create a stable, consistent environment,<br />
especially in the beginning stages when confusion<br />
may be commonplace.<br />
Always keep the injured family member informed<br />
about what is going on.<br />
Carmen’s experience<br />
Sometimes it’s useful when you and the family member who has a brain injury are<br />
talking to other people to have some kind of cue, such as tugging on your ear, to<br />
let the person with the brain injury know they are talking too loud, too fast or too<br />
much.<br />
83
Getting Back to Work<br />
Returning to work is possible for some people who have had a brain<br />
injury. After you have recovered and been assessed by a vocational<br />
support specialist, work options will be discussed with you.<br />
This may require you and the vocational specialist visiting your former<br />
work place or new work placement and discussing with the employer<br />
your options with regard to work, hours and support needed.<br />
Ask yourself ‘What can I do?’ and ‘What am I going to have difficulty with?’<br />
Studies have shown that it is not the severity of injury that will affect<br />
your return to work, but whether you have a realistic insight into your<br />
condition accompanied by self-acceptance.<br />
Returning too early to work can be both a positive and negative experience<br />
for you. Positive elements are that it will give you a realistic insight into<br />
your own capabilities, and negatively, you may find it emotionally and<br />
physically difficult during the initial period, especially with the effect on<br />
your fatigue levels.<br />
The best thing you can do is to start small and work up from there.<br />
1 Acute care - rest and gain strength.<br />
2 Initial rehabilitation - work on getting better, physically, mentally<br />
and emotionally.<br />
3 At home, establish a routine and increase your participation<br />
around the home.<br />
4 Work out what you can do and what kind of job you would like<br />
to do.<br />
5 Work on stress and anxiety management levels and apply those<br />
to your work place.<br />
6 Analyse your work environment - what is involved and sort<br />
out how to make things easy on yourself - talk to a<br />
vocational consultant.<br />
7 Start your job part-time and if you feel able, increase your hours gradually.<br />
84
Supported Employment<br />
You may find supported employment is an option that<br />
could work for you. Supported employment includes<br />
job placement, training and advocacy, ongoing assessment<br />
and continuous monitoring. It may also involve educating<br />
employers and colleagues about your needs. Usually,<br />
supported employment works best if you have had a severe<br />
brain injury. It may continue indefinitely or diminish over<br />
time, depending on your needs.<br />
Ways of coping<br />
Ask for a support person to attend interviews<br />
that you may have with ACC or WINZ, such as<br />
a member of your rehabilitation team. Your local<br />
Brain Injury Association may have a support person<br />
who could help.<br />
Employment help<br />
Ask to be referred to a vocational support<br />
service.<br />
Start with small steps and work up from there (for<br />
example, from part-time work to full-time).<br />
Part time<br />
Full time<br />
Make sure the job you get is right for you and that<br />
you will not become over-stimulated.<br />
Assess your capabilities for the job you want.<br />
What can I do?<br />
85
Ways of coping<br />
Lifeline<br />
Try volunteer work as this can be a good stepping<br />
stone to paid work.<br />
Limit multi-tasking in your job as taking on too<br />
much will increase your fatigue levels.<br />
Aim to work at your own pace. Limiting tasks that<br />
have deadlines should help lower overall stress<br />
levels.<br />
Limit new learning in the beginning. Try to utilise<br />
old familiar skills and knowledge.<br />
An interesting job will be a lot more stimulating<br />
than something dull and boring. An interesting job<br />
will lower frustration levels.<br />
Your employer will need to be educated about<br />
your capabilities. Make sure they are fully aware<br />
of your limitations as well as your capabilities.<br />
Information may need to come from a member of<br />
your rehabilitation team.<br />
Use coping mechanisms such as lists, wall planners,<br />
diaries, dictaphones and any tools that will help to<br />
compensate for shortcomings you may have as a<br />
result of your injury.<br />
86
Ways of coping<br />
Arrange for monitoring and feedback from your<br />
employer on how you are progressing.<br />
I’m ready for work<br />
Return to work when you feel you are ready to<br />
do so.<br />
Cate’s experience<br />
I was expected to suddenly go back full-time, as well as go to other appointments.<br />
That was a regressive step and I just couldn’t manage.<br />
Shane’s experience<br />
In 2008, I did a course five years after my brain injury. This was one week<br />
full-time, then five alternate Saturdays, then another week full-time. I managed it<br />
with significant difficulty all the way, but I got to the end by pushing myself.<br />
Don’t rush into things. Take it in small chunks. Take your time and make sure<br />
you’re healed and ready to go back to work as you may find you hit big obstacles,<br />
which may lead to depression. I found that part-time work in the beginning was<br />
important, and I also think it is important that you find a job you enjoy, because<br />
working makes you feel good.<br />
I have a meeting every six weeks with my supervisor and we go over how I’m doing.<br />
I find that because I’ve had this injury, I often think, ‘Am I doing a good enough job?’<br />
and seeing my supervisor helps clarify that. I’d hate to think my workmates are<br />
doing extra work for me, so seeing the supervisor is reassuring.<br />
87
Driving after a<br />
Brain Injury<br />
You may be keen to return to driving and regain your independence after<br />
you have had a brain injury. However, driving is an activity that requires the<br />
co-ordination of both mental and physical skills. Even if you are confident<br />
that your driving skills have remained intact after an injury, it’s still important<br />
to take the necessary steps to ensure safe driving.<br />
Land Transport New Zealand (LTNZ)<br />
and Medical Advice<br />
Following a traumatic brain injury, it is difficult to provide a simple answer<br />
as to how soon after your brain injury you can start driving again.The<br />
recommendation will depend on the individual’s circumstances, the degree<br />
of injury, and subsequent recovery. Generally the LTNZ is guided by the<br />
advice of the medical personnel concerned.<br />
How will a brain injury affect my driving?<br />
Brain injury will affect people in different ways. The LTNZ lists on their<br />
website some of the consequences of a brain injury that could affect<br />
someone’s driving. These include:<br />
Altered vision<br />
• Not seeing signs or traffic hazards on one side of the car.<br />
• Misjudging distance and speed.<br />
Altered thinking patterns<br />
• Slowed thinking, making it difficult to make decisions at busy<br />
intersections.<br />
• Trouble coping with too much sensory information at once.<br />
• Loss of concentration resulting in a decrease in driving<br />
abilities.<br />
• Short-term memory loss affecting driving.<br />
88
Epilepsy<br />
• Brain injuries severe enough to have caused<br />
• unconsciousness or loss of memory may result in epilepsy.<br />
(This does not include seizures immediately after the injury,<br />
which are considered part of the injury process).<br />
Physical challenges<br />
• Reaction time may be slowed.<br />
• Co-ordinating hand and feet movements may be difficult.<br />
• Ability to steer may be reduced due to muscle weakness.<br />
• There may be problems using foot pedals.<br />
When can I start driving again?<br />
Whether a person can return to driving will depend on the type of licence<br />
(and any endorsements) they hold, and the nature and extent of the brain<br />
injury. Higher criteria apply where commercial classes and endorsements<br />
are concerned.<br />
For serious brain injuries, Land Transport New Zealand usually requires a<br />
neurologist’s report and an occupational therapist’s assessment before a<br />
person will be allowed to start driving again.<br />
If you have an ACC case manager, check whether funding is available for<br />
driving assessments and/or specialist medical assessments (if required).<br />
Medical assessment<br />
If you would like to start driving again, you need to consult your<br />
GP who can determine if you are fit enough to drive. The doctor<br />
may recommend (or require) an additional assessment from an<br />
occupational therapist.<br />
An occupational therapist will:<br />
• Give advice on licence issues following an injury or crash<br />
• Look at how any physical or cognitive changes might affect<br />
your driving abilities<br />
• Ensure that you are likely to satisfy driving standards<br />
• Determine if lessons are required to improve your confidence<br />
or to help you become a better driver<br />
• Help a learner-driver develop the skills needed for driving.<br />
What does the driving assessment involve?<br />
The driving assessment is divided into two sections:<br />
• An off-road assessment<br />
• An on-road practical driving assessment 89
Each section takes about 90 minutes to complete and you can have a<br />
family member, friend or support person with you. Usually an appointment<br />
for the on-road assessment will be arranged at the end of the off-road<br />
assessment. You can request that both assessments take place in the one<br />
appointment if you prefer.<br />
Off-road assessment<br />
The off-road assessment starts with an interview, where you will have the<br />
opportunity to discuss any issues or concerns that you may have with,<br />
about your driving. You will also be asked to provide the following<br />
information:<br />
• The type of car you drive<br />
• Where you drive (what areas/ locations you drive to)<br />
• Your current licence status<br />
• Any difficulties you may have when driving<br />
The occupational therapist will also check your vision, your physical<br />
abilities (your movements, strength and co-ordination). They will also<br />
look at other factors which may be affecting your driving such as muscle<br />
strength, endurance, pain and fatigue.<br />
On-road assessment<br />
The on-road assessment records your ability to drive in real-life situations.<br />
It is normally undertaken in a dual-controlled car provided by the driving<br />
service. Both manual and automatic vehicles are available. On the drive, you<br />
will be accompanied by an occupational therapist and a driving instructor.<br />
The instructor will sit beside you to give you directions about where to<br />
drive.<br />
Ways of coping<br />
Don’t rush - remember that if you are not ready to<br />
drive, you will be putting yourself or others lives in<br />
danger.<br />
90
Ways of coping<br />
Guidelines<br />
Check the Land Transport New Zealand guidelines.<br />
These highlight the process involved in getting back<br />
on the road, and give reasons why brain injury might<br />
compromise your driving.<br />
Listen to your family members if they have concerns<br />
about you returning to driving.<br />
Ask the rehabilitation team when you would need<br />
to arrange a driving assessment and how to obtain a<br />
referral.<br />
Melinda’s experience<br />
• I drive at less than 100km/hour in the country now, because my reflexes<br />
are slower. I feel I have a better chance of stopping in time for a child or<br />
animal.<br />
• To remove time pressure, I aim to arrive everywhere five minutes early. This<br />
means I can cope with unexpected delays such as roadworks.<br />
• If I begin to feel fatigued while driving, my right eye goes out-of-focus. This is<br />
my body’s signal to stop and rest, so I always carry a sleeping bag and pillow<br />
in the car. I may even need a one-hour nap.<br />
• Extra distractions hamper my concentration, so I don’t play music in the car<br />
or chat to passengers while driving (I let them know when they get in the<br />
car).<br />
• Driving in the rain or in the dark used to be difficult. It took time to build up<br />
my driving tolerance, concentration levels and multi-tasking ability.<br />
• I pre-visualise my driving route so I’m in the correct lane well before I need<br />
to be. This means I can also choose to avoid big roundabouts as the amount<br />
of visual information can be over-whelming.<br />
91
Nutrition / Alcohol<br />
After a brain injury, you may notice some changes to your eating patterns<br />
and how you feel about food. Some people find that problems with their<br />
memory can affect how much food they eat. For example, they may forget<br />
that they had eaten breakfast. Brain injury may affect your capacity to feel<br />
full or hungry, which may cause you to eat too much or too little. Some<br />
people notice that their sense of taste or smell has changed. This may<br />
be the case in the earlier phase of your recovery and should improve<br />
gradually. A change in your sense of taste or smell can also be due to the<br />
side-effects of medication.<br />
Breakfast<br />
The human brain needs good quality fuel, so eating<br />
a well-balanced diet that is low in cholesterol<br />
and saturated animal fat is important. The saying<br />
‘what is good for the body is good for the brain’<br />
is very true. Most healthy eating and nutrition<br />
books stress the importance of eating a healthy<br />
breakfast to start the day.<br />
The brain needs vitamins and minerals particularly<br />
the antioxidant vitamins E and C which protect<br />
the brain. People who have experienced a brain<br />
injury often describe the food available in hospital<br />
as bland. Some have even enlisted family and<br />
friends to supplement their hospital diet with<br />
nutritious meals.<br />
Eat Omega-3<br />
foods, like<br />
salmon, sardines,<br />
mussels and<br />
walnuts.<br />
When you have a brain injury, you will need to<br />
give your brain every bit of extra help, including<br />
nutritional help, so it can recover to the best<br />
of its abilities. Omega-3 foods (such as oily fish<br />
like salmon and sardines), flax seeds and walnuts,<br />
should be included in your diet. A diet high in<br />
Omega-3 avoids excess sugar and starch and is<br />
high in anti-oxidants which will maximize the<br />
function of the brain cells and promote the<br />
healing and recovery of damaged cells.<br />
92
If you have problems with swallowing, a speech<br />
and language therapist can help with this. If you<br />
have a food allergy, get advice from a dietician.<br />
Physical activity and exercise will help you to<br />
maintain a healthy body weight. Exercise is also<br />
good for general well-being. However, be aware<br />
that when it comes to exercise or any physical<br />
activity, you may be restricted due to poor balance,<br />
fatigue, poor vision or other complications as a<br />
result of your brain injury.<br />
Alcohol<br />
People recovering from a brain injury are advised<br />
to avoid alcohol. This is particularly important in<br />
the early recovery phase. Alcohol can affect the<br />
brain’s ability to function and can also affect the<br />
brain in other ways. For example, alcohol can:<br />
Increase the possibility of becoming depressed.<br />
Increase the possibility of a seizure.<br />
Limit your recovery.<br />
Interfere with your ability to think and learn new things.<br />
Cause impulsive behaviour.<br />
Cause problems with balance, walking and talking.<br />
93
Nutritional tips<br />
Limit your intake of fried food and processed foods.<br />
Choose low-fat dairy products and lean meats.<br />
Eat foods rich in antioxidants (for example, fruit,<br />
vegetables, seeds and fish) and good amounts of<br />
cereal, grainy bread and other grains.<br />
Avoid foods containing hydrogenated fats, such as<br />
some margarines and cooking oils, as they are a<br />
major source of chronic disease.<br />
Glucose is important as it provides the fuel needed<br />
to keep the cells alive and functioning. If you<br />
notice that your concentration declines in the late<br />
morning or afternoon, eating a snack containing<br />
glucose such as fruit can help.<br />
Reduce the amount of salt you consume as this<br />
can help to control high blood pressure and fluid<br />
retention.<br />
Some people find caffeine, which is found in coffee,<br />
tea, chocolate, and in some energy drinks such as<br />
coke, difficult to tolerate after a brain injury. Drink<br />
no more than four cups of coffee per day and avoid<br />
it altogether after your initial injury.<br />
Try setting up an eating diary or chart and record<br />
what you eat each day. This can help you to<br />
remember the foods you have been eating and<br />
identify the times when you have felt full or hungry,<br />
and other changes affecting your body and mind.<br />
94
Exercise / Brain Gym<br />
Establishing an exercise routine can be very beneficial. We all know that<br />
exercise is good for us. Some research studies show that regular exercise<br />
can help improve memory.<br />
Whatever form of exercise you choose, it does not have to be exhausting.<br />
Mild aerobic exercise, such as walking for 20 minutes at least three times<br />
a week, stimulates blood flow and the delivery of essential oxygen to the<br />
brain.<br />
Another advantage of physical exercise is that it encourages sleep, which will<br />
help to give your brain the rest it needs to concentrate and remember.<br />
NOTE: Always check with your doctor before beginning a new exercise<br />
program.<br />
Types of exercise you may like to try:<br />
Walking three times a week.<br />
Light yoga.<br />
Tai Chi – recommended for balance and posture.<br />
Light gym routines.<br />
Light jogging.<br />
Cycling.<br />
Swimming.<br />
During the development of this book a number of focus groups were held<br />
with people with brain injuries about what they found helpful during their<br />
recovery. Some of the above activities were mentioned as being beneficial.<br />
Brain gym was also mentioned for helping with physical co-ordination,<br />
memory and reading etc.<br />
95
Brain Gym<br />
Basically, brain gym is a programme of 26 repetitive movements which claims to integrate<br />
body and mind to bring about improvements in concentration, memory, reading, writing,<br />
organizing, listening and physical coordination. Brain gym was developed in the 1970s<br />
by Paul and Gail Dennison and called Brain Gym or Educational Kinesiology (Edu-K)<br />
“learning through movement.” The programme has been widely used in British State<br />
schools and in parts of the United States and Canada.<br />
The Dennisons claim that any learning challenges can be overcome by finding the<br />
right movements, the use of which will create new pathways in the brain. They claim<br />
that the repetition of the 26 Brain Gym movements “activates the brain for optimal<br />
storage and retrieval of information.”<br />
Below and on the next page are a few<br />
exercises you might like to try<br />
Stretch out<br />
your toes<br />
with your feet<br />
crossed. This<br />
lessens tension<br />
in your hips<br />
and pelvic area<br />
and improves<br />
posture.<br />
Cross your<br />
left ankle over<br />
your right one.<br />
Intertwine<br />
your fingers<br />
and bring them<br />
to the chest.<br />
Move your legs<br />
in the opposite<br />
direction to<br />
your arms then<br />
vice versa.<br />
Massage your ears from top<br />
to bottom with both hands.<br />
96
Massage the<br />
area where<br />
the skull is<br />
attached to<br />
the neck and<br />
at the same<br />
time massage<br />
your navel area.<br />
Rest one hand<br />
on your upper<br />
lip while the<br />
other hand<br />
lies on your<br />
back-bone.<br />
One hand<br />
massages<br />
the area to<br />
the side, just<br />
above the<br />
chest, while<br />
the other<br />
hand rests<br />
on the navel.<br />
Pull your head<br />
outwards with<br />
your thumb.<br />
Sketch two<br />
images with<br />
both hands at<br />
the same time.<br />
Rest one hand<br />
on the lower<br />
lip and one<br />
hand on the<br />
pubic bone.<br />
Draw<br />
horizontal<br />
eights with<br />
each hand<br />
in the air.<br />
Stretch one<br />
arm up and<br />
grasp in the<br />
middle with<br />
the other arm.<br />
97
Socialising / Recreation<br />
You may feel anxious about returning to a social life or taking up leisure<br />
activities after a brain injury. However, it is important to join in these<br />
activities where possible and where practical.<br />
To begin with, there may be certain situations or environments which<br />
you may find stressful, tiring and uncomfortable. It is important to know<br />
your limits, what works and what does not. Noisy environments, like pubs<br />
and clubs, may create too much stimuli and confuse a person with a brain<br />
injury.<br />
In her book ‘Just a Bang on the Head’, Rosie Belton describes how, after<br />
her head injury, she found conversation at parties very difficult, especially<br />
if there was music in the background. She also describes how patterned<br />
carpets in hotels or other buildings would create problems for her<br />
visually.<br />
No two people with a brain injury have the same experience. It is very<br />
individual, so you have to decide what will work best for you and try to<br />
gradually acclimatise yourself to particular situations.<br />
Ways of coping<br />
Small steps are important when socialising again. You<br />
may encounter new surroundings and new people and<br />
this new stimuli will make you feel tired.<br />
If you decide to see a movie, make sure it is not too<br />
stimulating as this may make you fatigued.<br />
98
Ways of coping<br />
Parties are also environments that may make you<br />
tired - communicate this to key people before you<br />
reach ‘crisis point’.<br />
Picking up a sport (if you are able) is a great way to<br />
improve your physical fitness and stamina.<br />
If you have difficulty walking, try handcyling. Various<br />
sports organisations for the disabled such as<br />
Parafed, hire out bikes.<br />
Take your time and return to activities gradually.<br />
You’re talking<br />
too fast....<br />
Establish cues with your family and friends. For<br />
example, a tug on the ear can let you know if you<br />
are talking too fast.<br />
What were the activities that you enjoyed doing<br />
before your injury? Listening to music, visiting the<br />
library or being a member of a book club? Get<br />
friends and family to help you establish some of<br />
those activities again.<br />
Resource Book<br />
Start a ‘resource book’ with information about<br />
your personal interests, days and times of activities,<br />
contact people, accessibility etc. This ‘resource<br />
book’ can help with cognitive problems (for<br />
example, memory loss).<br />
99
Shane’s experience<br />
I keep socialising to a limit, just because of fatigue. I choose where I go because<br />
a lot of places have too much stimuli and are too noisy. I still like to go out,<br />
but if we do go out to a bar, I make sure it’s not too loud, but I don’t make an<br />
issue of saying to people ‘Turn the music down’. If I don’t like it, I need to go<br />
somewhere else. I need to accept that there will be others who do like loud<br />
music and I shouldn’t get my way just because I have a brain injury. You have<br />
more control in your own home, but not out at a restaurant or bar.<br />
Mike’s experience<br />
Be aware that following a brain injury, your friends are likely to change. Many<br />
who were not true friends in the first place may find the changes in you too<br />
difficult to cope with and may want to distance themselves from the situation.<br />
It’s not your fault and those who are true friends will stick by you.<br />
It is normal for a person with brain injury to undergo many different physical<br />
and emotional changes and be in a completely different “head space” than<br />
they were before the head injury. That former head space is what the friends<br />
you lose were relating to, but the new person you are may hold less appeal to<br />
them and they move on. It’s a simple fact that life changes result in changes in<br />
associates and friends. That’s life!<br />
At the end of the day it doesn’t matter that you no longer see certain friends<br />
because you will always make new friends who can relate to whatever head<br />
space you are in and these are the friends worth having!<br />
From my own experience I can say that many of the friends and associates I<br />
regularly “hung around” with, went their own way and didn’t keep in touch. In<br />
those early times, that did cause me a little concern but after my accident in<br />
the end it did not matter because I have since found a few really good, close<br />
friends with whom I love spending time.<br />
100
Personal<br />
Journeys<br />
Journeys
Personal Journeys<br />
Mike<br />
Page 103<br />
Cate<br />
Page 105<br />
Graeme<br />
Page 107<br />
Elizabeth and Merv<br />
Page 108<br />
Paul<br />
Page 109<br />
Cecile<br />
Page 111<br />
102
Mike<br />
As a young adult living in Christchurch, I used to be one of the pit crew for<br />
a guy named Rob who raced a six-cylinder Super Saloon car at Woodford<br />
Glen each Saturday evening. Also living at the same place as myself was<br />
my best mate, Tony, who worked with Rob. Along with a group of a few<br />
others we were your typical bunch of young friends. We used to hit the<br />
town and do many things together - drinking, weight-training, carousing<br />
and partying etc, including working on the race car at Rob’s place and<br />
pit-crewing on the weekends.<br />
One week, Tony informed me that Rob wanted to travel with the car and<br />
the pit crew down to Dunedin for some special racing with international<br />
guests and that each of us would get the opportunity to drive the car.<br />
I was keen to go, despite the fact that I had previously agreed with my<br />
brother, Peter, to take part in gate marshalling and security at an upcoming<br />
Split Enz concert. Peter and I had been part of a similar arrangement for<br />
another concert a few weeks previously and had had a great time. Peter<br />
and I had also done a fair bit of weight training together with some very<br />
encouraging results. Tony and I had also been weight training together<br />
for most of the previous year and were both very fit and muscular at the<br />
time.<br />
A few days before Tony and I were to leave on that trip, Peter telephoned<br />
me to talk about the concert. I could hear the dismay in my brother’s<br />
voice when I told him that I was going down to Dunedin instead. I also<br />
felt a painful knot in my stomach right at the moment I told him that I<br />
was going down south rather than going with him to the concert. That<br />
unfamiliar pain was my intuition that my decision was terribly wrong and<br />
the consequences would be devastating.<br />
Eight of us went in two vehicles. The first a V8 ute towing the race car<br />
on a trailer, with Rob and his girlfriend and another mate driving, and the<br />
other a Holden HQ sedan with two in the back and three across the<br />
front. Tony was driving, another guy named Greg was between us in the<br />
middle and I was on the passenger side with the seat belt-on.<br />
On February 3rd, 1984, we began the journey south, calling into my<br />
mother’s house in Geraldine to give her the good news about my fitting<br />
and turning career taking a definite turn for the better.<br />
103
We travelled on from Geraldine to Winchester where we stayed the night<br />
at someone’s farm, then got under way again the morning of February<br />
4. Around 3.15pm, I had been snoozing but awoke just as we rounded<br />
a long left-hand bend into the township of Wakouiti. For some reason,<br />
Tony had at that moment pulled onto the other side of the road and was<br />
accelerating in a passing manoeuvre. In the split second that I’d opened<br />
my eyes, an unseen car popped over a rise in the road before us, and<br />
that’s where my memory ends until I came around in hospital weeks later.<br />
Apparently we’d had a high-speed head-on collision with that oncoming<br />
car. The front-left side of my forehead had struck the left metal roof pillar<br />
and left me in a coma for 22 days.<br />
As well as severe head injuries, I had a smashed left femur, a broken bone<br />
and destroyed ligaments in my right foot, a wrenched spine and neck.<br />
The type of head injuries I suffered are classed as ‘coup, contra coup’,<br />
where after impacting the inside-front of my skull, my brain had bounced<br />
backward and against the rear of my skull, damaging the sector of my<br />
brain associated with vision thus causing ongoing problems.<br />
All in all I was in pretty good shape considering the high-speed crash had<br />
killed two of the four people in the other car. Out of both cars, the only<br />
person without serious injuries was a rear passenger in our car named<br />
Gary. The other rear passenger, his girlfriend Fiona, also suffered a broken<br />
left femur. Greg in the front with no seat-belt had hit the dashboard pretty<br />
hard and had some internal injures, but the windshield had exploded out<br />
on impact so he suffered no head trauma. He was out of hospital in a<br />
couple of weeks. Tony’s head had hit the top of the steering wheel and he<br />
suffered a minor head injury.<br />
Since that day Tony is the only one out of that group I have remained<br />
in touch with. That accident caused major changes to everyone’s life in<br />
different ways, including that of my family. I have often wondered to myself<br />
what would have happened if I had not made the decision to travel to<br />
Dunedin but stayed in Christchurch with my brother. Obviously what’s<br />
done is done and can never be changed, but these days, with so much<br />
free time on my hands, I just can’t help wondering.<br />
104
Cate<br />
I hit my head at work on 20 September 2002. It happened like this: I was<br />
asked after lunch to clean the laundry. I knew it was a big job and I was<br />
tired so said it was too much for a Friday afternoon. I was then asked<br />
to make a start on it and continue the job next week. I was tidying and<br />
cleaning in the laundry for a while, then went to the area under the<br />
stairs. I got down on the floor before realising I hadn’t brought a cloth to<br />
wipe the floor in the corner. I immediatly put my hands on the floor and<br />
sprang upwards forgetting that I was under the stairs. The impact to the<br />
back of my head was so huge I could never forget it. I actually thought all<br />
my teeth were gone! I then tried to stand up away from the stairwell, but<br />
fell over on my left side, breaking my glasses frame and going unconscious<br />
for about forty-five minutes.<br />
I remember the first aid staff member, asking me what day of the week<br />
it was and other questions and I laughed because it seemed I was in<br />
a ridiculous situation, being aware of only part of what was going on,<br />
and (asking) what day of the week it was seemed irrelevant to my<br />
predicament.<br />
At that stage (after the accident) it felt like I was struggling through an<br />
impossible fog, partially floating with no idea where my feet would land,<br />
seeing things moving that were not, and experiencing a great collection<br />
of unmanageable and very frightening symptoms. In those early weeks, it<br />
would take half a day to get out of bed, get showered and get breakfast.<br />
Because I was not capable of getting myself safely to and from work, my<br />
older sister came to stay with me for a couple of weeks, walking me to<br />
the bus stop each morning. Actually she didn’t stay a week, because I<br />
needed so much dark and quiet time that I couldn’t bear to have anyone<br />
in the house. I walked strangely - sort of spastic (only partially affected by<br />
gravity it seemed) falling to one side or the other, falling into gutters, and<br />
against power poles and fences. After a while, I began vomiting onto the<br />
grass on the way to the bus in the mornings and that was a sign to me<br />
that it was stupid to try and carry on. My doctor gave me a certificate,<br />
and I went on the sickness benefit and eventually the invalids benefit.<br />
105
One of the things I was told (after my injury) was not to give up on things<br />
I did prior to my injury. I tried to cycle a few blocks occasionally, though<br />
I was no longer prepared to bike through town as I had been doing. On<br />
one occasion (January 2004) I had planned to walk with a friend to her<br />
place, taking the bike, but someone in the neighbourhood offered her a<br />
ride, so I had to bike to her place instead. I have great difficulty coping<br />
with a change of plan, especially if it comes from someone else. As I rode<br />
along, having not been able to process the information around the change<br />
of plan, I hit the back of a parked car, bashing my head several times on<br />
the back window and falling down off the boot to the road, getting very<br />
bruised on the tow-bar as I fell. I am no longer safe on the bike as there<br />
seems to be a delay between the brain wanting to use the brakes and my<br />
hands actually carrying out the task.<br />
It was after this second accident that I began dropping and over-filling<br />
everything. I seemed to have no idea where my head was in relation to<br />
fixed objects like the letterbox, the fence, the gate or shelves.<br />
It’s been six years now, since the first accident. It took me five years to<br />
accept that I am the way I am, and that I have to plan and live my life<br />
around the symptoms as safely as I can. I no longer spend a huge amount<br />
of energy attempting to hide the symptoms in shame at being disabled in<br />
the way that I am. Early on, I made myself a motto, - ‘get up, get out, and<br />
get on with it’. Each part of it is a challenge, but it has helped me to have<br />
a sense of purpose each day, and I’ve learnt quite a lot.<br />
106
Graeme<br />
I was involved in a car accident in 1993 which resulted in serious brain<br />
injury. My life changed in a flash and I had to learn how to walk, talk and<br />
breathe correctly again.<br />
The doctors said they had done all they could, so I put my thinking cap<br />
on and thought ‘natural medicine’, as there is so much we don`t know<br />
about the brain. I got involved in massage therapy and they (natural health<br />
specialists) tried different herbs and oils on me. It was amazing, the herbs,<br />
especially basil, seemed to stimulate the brain.<br />
I also found that after massage therapy I would walk a lot better. That was<br />
a big help because early on I had a lot of trouble walking and had terrible<br />
balance. Massage made all the difference. What was really good was that<br />
once I was mobile again, I was able to go walking.<br />
Key point: I found the fitter I got, the better my brain worked and I<br />
became more aware of my surroundings. But the best thing I did for my<br />
brain injury was Whole Brain Learning, nickname “brain gym”. That`s<br />
where they teach you how to use both sides of the brain, but also how<br />
to believe in yourself, and that there is no such word as ‘can`t’.<br />
Through visualization you can achieve anything and I became very positive<br />
about myself. I now believe nothing is impossible and I can do anything if I<br />
believe in myself. I told myself to do what I could and enjoy life. I believe<br />
in living life to the full and to be prepared to try new things.<br />
Today I can partially run and have a part-time paid job, which a few years<br />
ago I thought was impossible. So my advice is NEVER, NEVER GIVE UP!<br />
107
Elizabeth and Merv<br />
Elizabeth had an epileptic seizure and a resulting brain scan found that<br />
she had a brain tumour, which had to be removed. Further tests revealed<br />
21 nerve endings had not knitted together and her short term memory<br />
is now terrible.<br />
“For about two years I had bad, bad headaches and no-one wanted to<br />
know me,” she said.<br />
“My GP said he couldn’t help me anymore so he sent me to a psychiatrist,<br />
which I found degrading.”<br />
A person with a brain injury can often be mistaken as having a mental<br />
illness, or that they are drunk. People being pulled over by police while<br />
driving because others had reported they were slurring their speech<br />
prior to driving their vehicle was not unheard of. Consequently, people<br />
with a brain injury now carry a card which includes a list of the signs of<br />
brain injury.<br />
Anger can be another consequence. For Merv, (Elizabeth’s husband) the<br />
best policy when his wife gets angry is to walk away. Learning to accept<br />
that they could not do things they used to be able to do with a click of<br />
their fingers was one of the hardest things to deal with.<br />
Elizabeth and Merv first met 50 years ago but only got married seven<br />
years ago, after Elizabeth had her brain injury. For Merv, Elizabeth was<br />
just Elizabeth, and while her memories were often lacking, one thing was<br />
for sure, as a team, they have a very capable brain.<br />
108
Paul<br />
Fourteen years ago I was hit as a pedestrian by a car. I was not expected<br />
to survive. I was in post traumatic amnesia (PTA) for ten months. To this<br />
day, I still don’t remember the event and I have been told I never will. I<br />
could walk with assistance after ten weeks, but it required eight months<br />
of intensive hospital therapy before I could go home.<br />
I had to do what most brain injured people have to do; relearn how to<br />
walk, talk, write, read, dress, run and learn. After my accident all of my<br />
medical knowledge was lost, so in a matter of seconds, I lost seven years<br />
of work and study. I also lost a lot of my old memories which meant I had<br />
difficulty remembering family and friends.<br />
In short, almost all of my old friends have basically drifted away and some<br />
have not been able to accept me as I am now, they remember the old me,<br />
and only want that person. I have, however, made a few new friends.<br />
It took a very long time to retrieve a lot of the things I knew pre-injury.<br />
I get confused about some of my thoughts and whether I am retrieving<br />
old memories from before my injury, or whether they are new memories<br />
I have gained from recent discussions.<br />
I was told post injury I would not be able to learn new things. However<br />
I went to Whole Brain Learning and learnt to juggle before it was two<br />
years post injury. This showed me that if you try hard, you can learn new<br />
things. This led me to do bursary accounting and a few other subjects. All<br />
of it was new to me and although I passed, I had to work much harder<br />
than what I had been used to.<br />
I found loneliness to be a big problem as I often feel quite isolated which<br />
makes it important to be involved in either courses or activity groups.<br />
I do remember that in the early stages of my recovery, no one, including<br />
myself, knew if today was going to be a leap-forward day, a fall-back day,<br />
or a no-change day. During my recovery, I have found that sometimes I<br />
will have fall-back days.<br />
109
Because my injury was over fourteen years ago, I can honestly say that<br />
I have never stopped improving. As long as you continue to believe in<br />
yourself and try new things all the time, you will notice improvements.<br />
Now I am one of the assistant coachs for the Special Olympics Basketball<br />
Team. I also play the piano at Woodchester Hospital Resthome and I have<br />
enrolled to do a University paper next year which will be a good test of<br />
my learning ability.<br />
110
Cecile<br />
I was nearly there, driving home with my carefully contemplated purchase<br />
of potted flowers for Mothers’ Day. I remember everything up until the<br />
split second before I reached that intersection, then nothing…. for three<br />
weeks.<br />
I don’t remember the vehicle travelling at speed at me through the<br />
compulsory stop sign and fourteen of my ribs breaking. I don’t remember<br />
the ambulances and the police at the scene. I neither remember the jawsof–life<br />
the firemen used to prise open the roof of my car, nor the bodyboard<br />
I was attached to when I was pulled up and out.<br />
It’s all a mystery to me - the two operations the ambulance staff<br />
performed on me so I could breathe air not blood, before their trip<br />
back to Christchurch Public Hospital…I’ve never slept for two weeks<br />
before!<br />
My months in Burwood Hospital, where I was transferred after Public,<br />
are a bit of a blur but I was well looked after. After a while, I had my own<br />
room and it felt like a second home. A multitude of family and friends<br />
came to see me.<br />
I remember the doctors’ rounds, the week before my discharge. “Good<br />
morning, Doctors!”, I gleefully exclaimed in the corridor. On arrival at<br />
my bed, one of the doctors informed me, “We’ve decided to prescribe<br />
something to calm you down, you’re too happy.”<br />
Well. I thought quickly and then in a flash of insight: the doctors were<br />
spending the majority of their day with people who were ill, in pain,<br />
traumatized. A cheerful, optimistic patient was not what they were<br />
expecting. I apologized and explained I was feeling well that day. They<br />
decided not to drug me.<br />
In the dining room at Burwood, I recall attempting to talk to another<br />
patient. I can’t forget him, because he burst into tears with every question<br />
I asked. Adapting to change can be difficult. I know that I focused on what<br />
I still had, not on what I’d lost. I’m still building on that.<br />
111
I’ve always loved a challenge. This may be what saved me, when my<br />
subconscious took over all of my brain’s functioning. Does survival depend<br />
on the strength of the will to live?<br />
What a wonderful learning opportunity this has been. I’ve learned how<br />
to pace myself, how to survive on an Invalid’s Benefit, and how to come<br />
to terms with the thought that I may never work again.<br />
I never knew that traumatic brain injury existed before it became a major<br />
part of my life. There’s a long list of how it affects a person. It causes<br />
fatigue, loss of balance, loss of co-ordination, short-term memory loss…<br />
….I can’t quite recall the rest of the list.<br />
I can no longer do the things I love as often as I’d like, but now I value them<br />
more. Recently, I’ve found it gratifying that I come across as a “normal”<br />
person to strangers.<br />
For a long time, I felt vulnerable - a new experience for me. I was also<br />
frustrated by my inability to express myself effectively, my lack of energy,<br />
my forgetting and fumbling. I have now engineered a masterful ‘mind<br />
library’ of compensatory techniques, strategies and options I can access,<br />
when required.<br />
I have no regrets. Before this happened, I used to assess my life every<br />
six months. I would ask myself - ‘ What would I really want to do if I<br />
discovered I only had six months to live?’ Then I’d go out and do it.<br />
The lengthening list of what we as humans take for granted, continues to<br />
dumbfound me. I took my senses for granted. Now they’re shimmering<br />
shadows, hinting, and I miss them.<br />
I did make one mistake while driving that day - I assumed the vehicle<br />
would stop at a ‘stop’ sign. I won’t be making that mistake again.<br />
This wasn’t my first near-death experience and I don’t wish to make a<br />
habit of it. I joke that I arrived at the pearly gates and exclaimed “Take<br />
me back. I’ve got things to do”. Now, I don’t know whether I’ll get them<br />
done or not. I do know though, that I’ll keep on trying. I’ve learned that<br />
my personality thrives on achieving goals. I have returned to feeling<br />
productive as a human being.<br />
When one person has a serious accident, it’s as if a pebble is projected<br />
into a pond. There is a ripple effect, as other lives are affected. Friends<br />
have just begun confiding in me the dramatic impact my event has had<br />
on their lives.<br />
112
In retrospect, I feel lucky that I had already packed so much into my<br />
life. I’ve travelled, I’ve loved, and I’ve lived. I’ve hitchhiked alone across<br />
the Sahara Desert - memories enough for a lifetime and I still have a<br />
life. ‘Growing old’ will be a familiar gust of warm desert air. I’ve decided<br />
to remain a bachelorette. My hands are full with just one person to<br />
nurture.<br />
I almost feel as if everything in my life was preparing me for what has<br />
happened. I am handling it. I adapt easily, I embrace change as a learning<br />
opportunity and I love meeting people. It has taken an event of this<br />
magnitude to get me to slow down. I’m fine, but when it happened I only<br />
hope that I was wearing a nice pair of knickers….<br />
‘Brain injury is about living with two faces’<br />
Cecile Tait<br />
113
Resources<br />
Resources
Chapter Contents<br />
Author’s note from Claire and Bernadette<br />
Page 116<br />
Resources<br />
Page 117<br />
Glossary<br />
Page 121<br />
115
Author’s note - Claire Freeman<br />
Author and Illustrator<br />
Compiling and illustrating this book has been a journey for me. I have<br />
met some inspiring and incredible individuals who, despite their brain<br />
injuries, have gone on to lead phenomenal lives. Many who were given<br />
bleak outcomes by health professionals, have gone on to run world class<br />
races, enrolled for university courses, provide support for others with an<br />
injury, and just live their lives with grace and integrity.<br />
As someone who had a spinal injury at age 17 as a result of a motor<br />
vehicle accident, I know first-hand how important information is for those<br />
with the injury and their family and friends. Having an injury, whether it<br />
be a spinal injury or brain injury, can be such a confusing and terrifying<br />
time for everyone. What makes it worse is not knowing or understanding<br />
the injury. My hope for this book is that it helps the person with an injury<br />
understand their condition and provides support for that person.<br />
Lastly, I want to say thank you to everyone who has been a part of this<br />
process. The information contained within it has come from the consumers<br />
themselves, which I feel gives the book its consumer-based authenticity.<br />
Author’s note - Bernadette Cassidy<br />
Author and Editor<br />
According to the Brain Injury Association of New Zealand, everyday 90<br />
people sustain a brain injury, which is staggering. If you are recovering<br />
from a brain injury or you have a loved one with a brain injury<br />
- you/they will need access to a wide range of information and resources.<br />
This handbook is the first step in providing that information in a format<br />
that is easy to understand. Having the appropriate information about a<br />
brain injury and the impact it has on a person can help remove the fear<br />
and stress associated with it.<br />
It has been a privilege to have been involved in the development of<br />
this handbook and to have had the opportunity to work closely with<br />
the Canterbury Brain Injury Association and its members who gave so<br />
generously of their time.<br />
116
Resources<br />
Book<br />
Video<br />
Website<br />
CD / DVD<br />
Books<br />
Resources – all the following are held in the Allan Bean Centre Library, Christchurch. Contact<br />
the Library on 03 383 9484 or email abclibrary@burwood.org.nz for further details. These<br />
resources can be borrowed anywhere in New Zealand. Many will also be available at your<br />
local library.<br />
Brain injury workbook: exercises for cognitive rehabilitation<br />
(2003). Powell, Trevor. Speechmark Publishing Ltd.<br />
Brainlash: maximize your recovery from mild brain injury 2nd edition<br />
(1999) Denton, Gail.L. Demos Publishing.<br />
Conversation and brain damage<br />
(2003). Goodwin, Charles. Oxford University Press.<br />
Coping with mild traumatic brain injury<br />
(1998). Stoler, Diane Roberts. Avery Publishing Group.<br />
Cracked: recovering after traumatic brain injury<br />
(2003). Calderwood, Lynsey. Jessica Kingsley Publishers.<br />
The Everest within: life with brain injury<br />
(2000). Brain Injury Association of New Zealand. Clarity Publishing.<br />
Gray matters: brain injury, the inside perspective<br />
(2006).Lerner, Heidi. AuthorHouse.<br />
Head injury: a practical guide<br />
(2004). Powell, Trevor. Speechmark Publishing.<br />
Head injury and the family: a life living perspective<br />
(1994). Dell Orto, Arthur E. PMD Publishing Group<br />
I had brain surgery, what’s your excuse? : an illustrated memoir<br />
(2004). Becker, Suzy. Workman Pub.<br />
117
Resources<br />
Just a bang on the head: living with a brain injury<br />
(2005). Belton, Rosie. Craig Potton Publishers.<br />
Interrupted lives: rehabilitation and learning following brain injury<br />
(2005). Rees, Roger R. IP Communications.<br />
Ketchup on the baseboard: rebuilding life after brain injury<br />
(2004). Rocchio, Carolyn. Lash & Associates Pub./Training Inc.<br />
Life after Brain Injury: who am I? 2nd ed<br />
(1996). Boskey, Dana S (ed). HDI Publishers.<br />
Life after head injury: the experiences of twenty<br />
young people and their families<br />
(1995) Hubert, Jane. Avebury Publishers,<br />
Life after stroke: a guide for people with a stroke and their families<br />
(1998). Stroke Foundation of NZ.<br />
Listening in the silence, seeing in the dark:<br />
reconstructing life after brain injury<br />
(2002). Johansen. Ruthann Knechel. University of California Press.<br />
Living with brain injury: a guide for families and caregivers<br />
(1998) Acorn, S (ed.) University of Toronto Press.<br />
My stroke of insight: a brain scientist’s personal journey<br />
(2008) Bolte-Taylor, Jill. Hodder & Stoughton<br />
Normal again: redefining life with brain injury<br />
(2001). Swiercinsky, Dennis P. Writer’s Showcase.<br />
Over my head: a doctor’s own story of head<br />
injury from the inside looking out.<br />
(1998). Osborn, Claudia L. Andrews McMeel Pub.<br />
Sexual difficulties after traumatic brain injury and ways to deal with it<br />
(2003). Aloni, Ronit. Charles C. Thomas.<br />
Stranger in the mirror: a true story of stroke survival<br />
and transformation: written with insight, compassion and<br />
humor for brain injury survivors and their families<br />
(2006). Little, M. E. Author House.<br />
118
Stroke-free for life : the complete guide to<br />
stroke prevention and treatment<br />
(2002). Weibers, David O. Cliff Street Books.<br />
Stroke Rehabilitation: guidelines for exercise<br />
and training to optimize motor skill<br />
(2003). Carr, Janet H. Butterworth-Heineman.<br />
The Omega-3 connection: the groundbreaking omega-3<br />
antidepression diet and brain program<br />
(2001). Stoll, A. L. Simon & Schuster.<br />
Traumatic brain injury: rehabilitation for everyday adaptive living<br />
(2002). Ponsford, J., Sloan, S and Snow, P. Psychology Press.<br />
Traumatic brain injury rehabilitation : children and adolescents 2nd ed<br />
(1998). Ylvisaker, Mark. Butterworth-Heinemann.<br />
Working after brain injury: what can I do?<br />
(1996). DeBoskey, Dana S. (ed). HDI Publishers.<br />
You and me: an education program about sex and<br />
sexuality after a traumatic brain injury<br />
(1999). Simpson, Grahame. Brain Injury Rehabilitation Unit<br />
Videos<br />
Head on: a film about life after head injury<br />
(2000) Producer: William Fairbank. Willstone Productions<br />
Stroke in midlife<br />
(1998) Brain Foundation Australia. Tribal Productions.<br />
A stroke survivor’s guide to independence: wheelchair<br />
transfers for families and caregivers<br />
(2001) Producers: Jane Champion and Jan Davies. International Clinical<br />
Educators<br />
119
Websites<br />
Brain Injury Association New Zealand<br />
www.brain-injury.nz.org<br />
The Brain Injury Association New Zealand provides information,<br />
advocacy and support to people with brain injury and their families.<br />
Centre for Neuro Skills – Traumatic brain<br />
injury resources and information.<br />
www.neuroskills.com<br />
Traumatic brain injury: a survival guide (2000). Johnson, Glen.<br />
www.tbiguide.com/<br />
Head Injury Association of New Zealand<br />
www.head-injury.org.nz<br />
The Head Injury Society of New Zealand was formed in 1987 to raise<br />
head injury issues at a national level, to increase understanding and<br />
recognition and to help address the needs of those who have suffered<br />
head injury and their families.<br />
DVDs and CD-ROMs<br />
Best intentions: how to remember things you need to do<br />
(1998). Practical Memory Institute.<br />
Brain anatomy and function CD-ROM<br />
(2005). Traumatic Brain Injury Educational Series. Centre for Neuro<br />
Skills. USA<br />
120
Glossary<br />
Amnesia: Loss of memory.<br />
Anoxic: A severe deficiency of oxygen in tissues or organs.<br />
Anterograde amnesia: Memory loss that occurs before brain<br />
damage.<br />
Anxiety: A feeling of distress, apprehension and unease that may be<br />
caused by fear, danger, mental disorders or psychological imbalance.<br />
Aphasia: The loss of a previously-held ability to speak or understand<br />
spoken or written language, due to disease or injury of the brain.<br />
Axons: Nerve fibres that can rapidly conduct impulses away from the<br />
neuron cell body.<br />
Brain Stem: The section of the brain that joins with the spinal cord,<br />
responsible for the control of reflexes and such essential internal<br />
mechanisms as respiration and heartbeat.<br />
Cerebellum: A large section of the brain, serving to coordinate voluntary<br />
movements, posture, and balance in humans, being in back of and below<br />
the cerebrum and consisting of two lateral lobes and a central lobe.<br />
Cerebral cortex: The outer layer of gray matter of the cerebral<br />
hemispheres, largely responsible for higher brain functions, including<br />
sensation, voluntary muscle movement, thought, reasoning, and memory.<br />
Cerebral hemispheres: A cerebral hemisphere is defined as one<br />
of the two regions of the brain that are on the left or right side of the<br />
brain.<br />
Cognitive abilities: The mental process of perception, memory,<br />
judgment, and reasoning.<br />
Coma: A state of deep, often prolonged unconsciousness, usually the<br />
result of injury, disease, or poison, in which an individual is incapable of<br />
sensing or responding to external stimuli and internal needs.<br />
Concussion: Injury to the brain due to a blow, fall, or sudden impact<br />
with another object or surface.<br />
Continence: The ability to voluntarily control urinary and faecal<br />
waste.<br />
121
Contrecoup: An injury to a part of the brain opposite the site of<br />
the primary injury.<br />
Contusion: An injury that doesn’t break the skin but results in some<br />
damage to underneath tissue.<br />
Dendrites: Any of several parts branching from the body of a neuron<br />
that receive and transmit nerve impulses.<br />
Dysphagia: Difficulty in swallowing.<br />
Dyspraxia: Impairment of the ability to perform co-ordinated<br />
movements.<br />
Epilepsy: A neurological disorder characterized by a sudden recurring<br />
attack of motor, sensory, or psychic malfunction with or without loss of<br />
consciousness or convulsive seizure.<br />
Fatigue: Physical or mental weariness resulting from exertion.<br />
Frontal lobe: The part of the brain lying directly behind the forehead.<br />
Glasgow Coma Scale: A scale that is used to assess the severity of a<br />
brain injury, that consists of values from 3 to 15. The scale is obtained by<br />
measuring the ratings of how the person with a brain injury responds to<br />
certain standard stimuli by opening the eyes, giving a verbal response, and<br />
giving a motor response, and that for a low score (as 3 to 5) indicates a<br />
poor chance of recovery and for a high score (as 8 to 15) indicates a good<br />
chance of recovery.<br />
Global amnesia: A total loss of memory.<br />
Haematoma: A localized swelling filled with blood resulting from a<br />
break in a blood vessel.<br />
Haemorrhagic stroke: A blood vessel bursts within the brain causing<br />
bleeding (haemorrhage) into the brain.<br />
Hypoxia: Diminished availability of oxygen to body tissues.<br />
Ischaemic stroke: Most common stroke caused by a clot that blocks<br />
an artery that carries blood to the brain.<br />
Infarction: An area of dead tissue. A cerebral infarction is the ischemic<br />
kind of stroke due to a disturbance in the blood vessels supplying blood<br />
to the brain.<br />
Neuron: A nerve cell.<br />
122
Neurotransmitters: Chemicals made in the nervous system that act<br />
as messengers, helping or interfering with the function of nerve cells in the<br />
nervous system.<br />
Occipital Lobe: The back section of the brain having the shape of a<br />
three-sided pyramid and containing the visual centre of the brain.<br />
Paralysis: Loss of the ability of muscles to activate.<br />
Parietal Lobe: The upper middle lobe of the brain located above the<br />
temporal lobe. Complex sensory information from the body is processed in<br />
the parietal lobe, which also controls the ability to understand language.<br />
Passivity: The trait of remaining inactive that may be due to a lack of<br />
initiative.<br />
Rehabilitation: An active process whereby the person with a health<br />
concern works to optimise their physical, mental and social abilities.<br />
Retrograde amnesia: Memory loss that occurs after brain damage.<br />
Seizure: A sudden unusual discharge of electrical impulses in a specific<br />
area of the brain that causes uncontrolled stimulation of nerves and<br />
muscles.<br />
Sensory cortex: The region of the cerebral cortex concerned with<br />
receiving and interpreting sensory information from various parts of the<br />
body.<br />
Serotonin: A neurotransmitter that is involved in sleep, depression,<br />
memory, and other neurological processes.<br />
Stroke: A blockage or hemorrhage of a blood vessel leading to the brain,<br />
causing inadequate oxygen supply. Depending on the extent and location<br />
of the abnormality, can cause symptoms as weakness, paralysis of parts of<br />
the body, speech difficulties, and, if severe, loss of consciousness or death.<br />
Temporal Lobe: The lobe of each cerebral hemisphere lying to the<br />
side and rear of the frontal lobe. The temporal lobe controls hearing and<br />
some aspects of language, perception, emotion, and memory.<br />
123
Empowering New Zealanders<br />
with a spinal cord impairment<br />
to live independent,<br />
productive and<br />
confident lives – right now!<br />
Head Space: a handbook on brain injury – published by the New Zealand Spinal Trust.