Dental Asia March/April 2019
For more than two decades, Dental Asia is the premium journal in linking dental innovators and manufacturers to its rightful audience. We devote ourselves in showcasing the latest dental technology and share evidence-based clinical philosophies to serve as an educational platform to dental professionals. Our combined portfolio of print and digital media also allows us to reach a wider market and secure our position as the leading dental media in the Asia Pacific region while facilitating global interactions among our readers.
For more than two decades, Dental Asia is the premium journal in linking dental innovators
and manufacturers to its rightful audience. We devote ourselves in showcasing the latest dental technology and share evidence-based clinical philosophies to serve as an educational platform to dental professionals. Our combined portfolio of print and digital media also allows us to reach a wider market and secure our position as the leading dental media in the Asia Pacific region while facilitating global interactions among our readers.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
User Report<br />
initial drilling channel must be inferior to<br />
that of the first osteotome used. Thus,<br />
the addition of bone substitute is only<br />
required to further increase the volume of<br />
sinus floor obtained. If the residual bone<br />
height is between 4 and 6 mm, it may be<br />
necessary to first place a bone substitute<br />
in the drilling channel before inserting the<br />
first osteotome, which will, in this case,<br />
have a convex end.<br />
Before implantation, an X-ray is taken to<br />
view the arch obtained. Bone substitutes,<br />
like xenografts and β-TCP, seem to be as<br />
effective as autogenic bone to increase<br />
an atrophic maxillary ridge with the sinus<br />
floor elevation technique. 9-11<br />
Advantages and disadvantages<br />
A transcrestal sinus floor elevation<br />
osteotomy is an approach most dental<br />
practitioners use because of its benefits<br />
namely:<br />
• it is considered a low invasive<br />
surgery with minimal postoperative<br />
follow-ups 13<br />
• it does not require end drilling, thus<br />
better bone/implant interface with<br />
lower risk of heating<br />
• only a very small enlargement of the<br />
alveolar crest is made with an improved<br />
peri-implant bone density 14-15<br />
• simultaneous implant placement is<br />
possible<br />
• reduced treatment time, as implant<br />
integration occurs at the same time<br />
as bone filling consolidation (3 to 6<br />
months, according to residual bone<br />
height)<br />
• lower in cost because it is a single<br />
surgery with a smaller amount of<br />
biomaterial used, as the implant<br />
contributes to increase the volume of<br />
the sinus floor.<br />
Despite all of its advantages, a transcrestal<br />
sinus floor elevation osteotomy is not<br />
without its drawbacks as it is a blind<br />
technique – sinus membrane is not<br />
visible 12 , patient feels discomfort due<br />
to the shocks caused by the osteotome<br />
hammering technique and it is not suitable<br />
for treatment of extensive defects.<br />
Conclusion<br />
The essential factor to enable<br />
simultaneous implant placements seems<br />
to be the residual bone height of the<br />
sinus floor before filling. The minimal<br />
value stated varies between 4 and 6 mm,<br />
according to studies. 1-16 However, more<br />
than this value, primary stability is one<br />
of the key conditions of success, hence<br />
the importance:<br />
• of the site preparation technique with<br />
an atraumatic condensing osteotomy<br />
• of the ability to compact the filling<br />
material<br />
• of the design of the implant itself.<br />
Although this is a blind technique<br />
that carries the risk of perforating<br />
the Schneiderian membrane, in very<br />
specific cases, transcrestal sinus floor<br />
elevation osteotomy represents the most<br />
cost-effective solution for the patient.<br />
This article will focus on two clinical<br />
cases which illustrate a new transcrestal<br />
sinus floor elevation technique with<br />
Osteo Safe ® , the automatic impactor<br />
developed by Anthogyr (Fig. 1).<br />
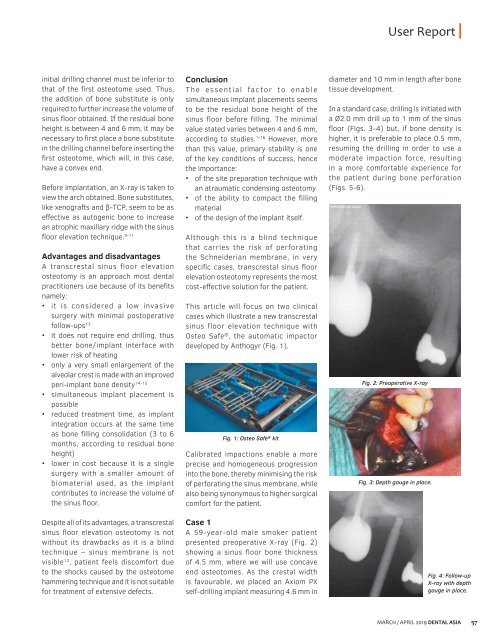
Fig. 1: Osteo Safe ® kit<br />
Calibrated impactions enable a more<br />
precise and homogeneous progression<br />
into the bone, thereby minimising the risk<br />
of perforating the sinus membrane, while<br />
also being synonymous to higher surgical<br />
comfort for the patient.<br />
Case 1<br />
A 59-year-old male smoker patient<br />
presented preoperative X-ray (Fig. 2)<br />
showing a sinus floor bone thickness<br />
of 4.5 mm, where we will use concave<br />
end osteotomes. As the crestal width<br />
is favourable, we placed an Axiom PX<br />
self-drilling implant measuring 4.6 mm in<br />
diameter and 10 mm in length after bone<br />
tissue development.<br />
In a standard case, drilling is initiated with<br />
a Ø2.0 mm drill up to 1 mm of the sinus<br />
floor (Figs. 3-4) but, if bone density is<br />
higher, it is preferable to place 0.5 mm,<br />
resuming the drilling in order to use a<br />
moderate impaction force, resulting<br />
in a more comfortable experience for<br />
the patient during bone perforation<br />
(Figs. 5-6).<br />
Fig. 2: Preoperative X-ray<br />
Fig. 3: Depth gauge in place.<br />
Fig. 4: Follow-up<br />
X-ray with depth<br />
gauge in place.<br />
MARCH / APRIL <strong>2019</strong> DENTAL ASIA 57