Diagnostic Ultrasound - Abdomen and Pelvis
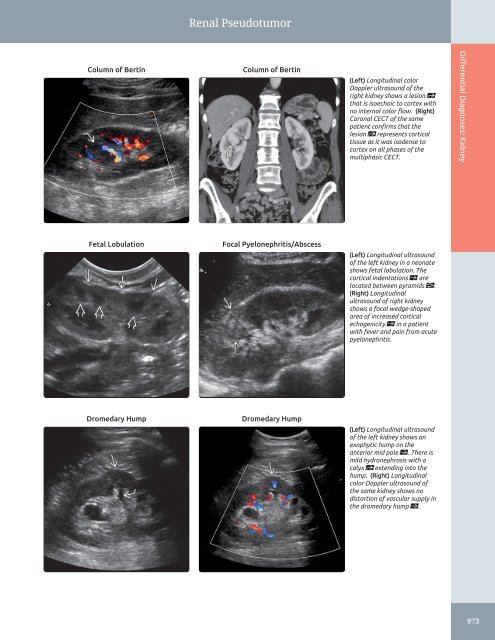
Renal Pseudotumor Column of Bertin Column of Bertin (Left) Longitudinal color Doppler ultrasound of the right kidney shows a lesion st that is isoechoic to cortex with no internal color flow. (Right) Coronal CECT of the same patient confirms that the lesion st represents cortical tissue as it was isodense to cortex on all phases of the multiphasic CECT. Differential Diagnoses: Kidney Fetal Lobulation Focal Pyelonephritis/Abscess (Left) Longitudinal ultrasound of the left kidney in a neonate shows fetal lobulation. The cortical indentations ſt are located between pyramids . (Right) Longitudinal ultrasound of right kidney shows a focal wedge-shaped area of increased cortical echogenicity ſt in a patient with fever and pain from acute pyelonephritis. Dromedary Hump Dromedary Hump (Left) Longitudinal ultrasound of the left kidney shows an exophytic hump on the anterior mid pole ſt. There is mild hydronephrosis with a calyx st extending into the hump. (Right) Longitudinal color Doppler ultrasound of the same kidney shows no distortion of vascular supply in the dromedary hump ſt. 973
Dilated Renal Pelvis 974 Differential Diagnoses: Kidney DIFFERENTIAL DIAGNOSIS Common • Obstructed Renal Pelvis • Reflux Into Dilated Renal Pelvis • Extrarenal Pelvis • Physiologic Distention of Renal Pelvis • Parapelvic Cyst • Prominent Renal Vessel • Urothelial Carcinoma Less Common • Pyonephrosis • Hemonephrosis • Renal Sinus Hemorrhage • Pararenal Fluid Collections • Peripelvic Cyst • Intrarenal Abscess • Calyceal Diverticulum • Acute Renal Vein Thrombosis Rare but Important • Pyelogenic Cyst • Multilocular Cystic Nephroma • Lucent Sinus Lipomatosis • Renal Lymphoma • Retroperitoneal Lymphoma • Renal Artery Aneurysm • Arteriovenous Malformation (AVM) • Intrarenal Varices • Renal Lymphangiomatosis ESSENTIAL INFORMATION Key Differential Diagnosis Issues • Important to differentiate between obstruction and nonobstruction ○ Follow ureter to level of obstruction to determine cause • Ultrasound is first-line modality for detection but other modalities such as CT, MR, VCUG, and retrograde pyelography may be required for definitive diagnosis • Nuclear scintigraphy differentiates obstruction from nonobstructive dilatation Helpful Clues for Common Diagnoses • Obstructed Renal Pelvis ○ Isolated dilatation of renal pelvis is uncommon ○ Dilatation elsewhere in GU tract determined by level of obstruction – For example, ureteropelvic junction obstruction manifests with pelvic dilatation and (to lesser degree) calyceal dilatation – Ureterovesical junction obstruction presents with hydroureter as well as pelvicalyceal dilatation ○ Determine if unilateral or bilateral ○ Level of obstruction helps narrow differential diagnosis ○ Most common cause of unilateral obstruction is stone disease ○ Other causes include bladder, ureteral or other pelvic mass, retroperitoneal mass or hemorrhage, aortic aneurysm, retroperitoneal fibrosis, iatrogenic injury • Reflux Into Dilated Renal Pelvis ○ Hydroureter may be present in addition to renal pelvic dilatation ○ VCUG essential in determining reflux – In future, contrast-enhanced voiding urosonography may be used in place of VCUG to evaluate for reflux without use of ionizing radiation • Extrarenal Pelvis ○ Common finding in neonates and often incidentally noted in other age groups – Renal pelvis projects medial to renal sinus ○ Appearance may simulate early obstruction but calyces are not dilated • Physiologic Distension of Renal Pelvis ○ Commonly noted when bladder is distended – Frequent in pregnant patients, most commonly in 3rd trimester; R > L – Fetal pyelectasis can result in mild pelvic dilatation in neonates, which subsequently resolves • Parapelvic Cyst ○ 1-3% of renal parenchymal cysts; usually solitary ○ May be mixed picture, as parapelvic cysts can compress collecting system resulting in true dilatation • Prominent Renal Vessel ○ May mimic pelvic dilatation but color Doppler denotes flow – Protocol advice: Always remember to use color Doppler when concerned about pelvic dilatation or cystic lesion to distinguish from vessel • Urothelial Carcinoma ○ Hypoechoic mass in dilated pelvis, though usually slightly hyperechoic to renal parenchyma ○ Can mimic hemorrhage or pus ○ On color Doppler, note internal vascularity within urothelial carcinoma Helpful Clues for Less Common Diagnoses • Pyonephrosis ○ Debris (pus) in dilated pelvicalyceal system ○ Look for presence of urothelial thickening and cause such as stone • Hemonephrosis ○ Blood within dilated pelvicalyceal system ± blood in bladder ○ Echogenicity variable depending upon age of blood products • Renal Sinus Hemorrhage ○ In absence of trauma, most often secondary to anticoagulation, but can be secondary to occult neoplasm, vasculitis, or blood dyscrasia ○ Cystic lesion of variable echogenicity disrupting normal central echocomplex, with mass effect upon renal pelvis and tension upon infundibula ○ Should spontaneously resolve in 3-4 weeks • Pararenal Fluid Collections ○ May occur in setting of infection, obstruction, or transplantation; include urinoma, hematoma, abscess, and lymphocele near renal hilum • Peripelvic Cyst ○ Lymphatic collection in renal sinus, distinct from parapelvic cyst, which is intraparenchymal ○ Often multiple and bilateral (unlike parapelvic cyst)
- Page 944 and 945: Cystic Pancreatic Lesion Mucinous C
- Page 946 and 947: Solid Pancreatic Lesion ○ Usually
- Page 948 and 949: Solid Pancreatic Lesion Serous Cyst
- Page 950 and 951: Pancreatic Duct Dilatation Chronic
- Page 952 and 953: PART III SECTION 4 Spleen Focal Spl
- Page 954 and 955: Focal Splenic Lesion - Typically mu
- Page 956 and 957: Focal Splenic Lesion Pyogenic Absce
- Page 958 and 959: Focal Splenic Lesion Splenic Infarc
- Page 960 and 961: PART III SECTION 5 Urinary Tract 9
- Page 962 and 963: Intraluminal Bladder Mass Bladder C
- Page 964 and 965: Abnormal Bladder Wall □ Uterine c
- Page 966 and 967: Abnormal Bladder Wall Invasion by P
- Page 968 and 969: PART III SECTION 6 Kidney Enlarged
- Page 970 and 971: Enlarged Kidney - Nonneoplastic cau
- Page 972 and 973: Enlarged Kidney Perinephric Fluid C
- Page 974 and 975: Small Kidney ○ Pseudotumors from
- Page 976 and 977: Small Kidney Postobstructive Atroph
- Page 978 and 979: Hypoechoic Kidney • Multiple Myel
- Page 980 and 981: Hypoechoic Kidney Acute Renal Arter
- Page 982 and 983: Hyperechoic Kidney ○ Echogenic co
- Page 984 and 985: Hyperechoic Kidney Chronic Glomerul
- Page 986 and 987: Cystic Renal Mass ○ Associated wi
- Page 988 and 989: Cystic Renal Mass Multicystic Dyspl
- Page 990 and 991: Solid Renal Mass • Horseshoe Kidn
- Page 992 and 993: Solid Renal Mass Renal Lymphoma Ren
- Page 996 and 997: Dilated Renal Pelvis • Intrarenal
- Page 998 and 999: Dilated Renal Pelvis Pyonephrosis P
- Page 1000 and 1001: PART III SECTION 7 Abdominal Wall/P
- Page 1002 and 1003: Diffuse Peritoneal Fluid Hemoperito
- Page 1004 and 1005: Solid Peritoneal Mass - Higher dens
- Page 1006 and 1007: Solid Peritoneal Mass Mimics Benign
- Page 1008 and 1009: Cystic Peritoneal Mass ○ Women of
- Page 1010 and 1011: Cystic Peritoneal Mass Pseudomyxoma
- Page 1012 and 1013: PART III SECTION 8 Prostate Enlarge
- Page 1014 and 1015: Enlarged Prostate Benign Prostatic
- Page 1016 and 1017: Focal Lesion in Prostate ○ Variab
- Page 1018 and 1019: Focal Lesion in Prostate Müllerian
- Page 1020 and 1021: PART III SECTION 9 Bowel Bowel Wall
- Page 1022 and 1023: Bowel Wall Thickening - Distal ileu
- Page 1024 and 1025: Bowel Wall Thickening Crohn Disease
- Page 1026 and 1027: Bowel Wall Thickening Clostridium D
- Page 1028 and 1029: PART III SECTION 10 Scrotum 1008
- Page 1030 and 1031: Diffuse Testicular Enlargement Test
- Page 1032 and 1033: Decreased Testicular Size Testicula
- Page 1034 and 1035: Testicular Calcifications Sertoli C
- Page 1036 and 1037: Focal Testicular Mass - Most common
- Page 1038 and 1039: Focal Testicular Mass Testicular Ly
- Page 1040 and 1041: Focal Extratesticular Mass - 3-50 m
- Page 1042 and 1043: Focal Extratesticular Mass Inguinal
Renal Pseudotumor<br />
Column of Bertin<br />
Column of Bertin<br />
(Left) Longitudinal color<br />
Doppler ultrasound of the<br />
right kidney shows a lesion st<br />
that is isoechoic to cortex with<br />
no internal color flow. (Right)<br />
Coronal CECT of the same<br />
patient confirms that the<br />
lesion st represents cortical<br />
tissue as it was isodense to<br />
cortex on all phases of the<br />
multiphasic CECT.<br />
Differential Diagnoses: Kidney<br />
Fetal Lobulation<br />
Focal Pyelonephritis/Abscess<br />
(Left) Longitudinal ultrasound<br />
of the left kidney in a neonate<br />
shows fetal lobulation. The<br />
cortical indentations ſt are<br />
located between pyramids .<br />
(Right) Longitudinal<br />
ultrasound of right kidney<br />
shows a focal wedge-shaped<br />
area of increased cortical<br />
echogenicity ſt in a patient<br />
with fever <strong>and</strong> pain from acute<br />
pyelonephritis.<br />
Dromedary Hump<br />
Dromedary Hump<br />
(Left) Longitudinal ultrasound<br />
of the left kidney shows an<br />
exophytic hump on the<br />
anterior mid pole ſt. There is<br />
mild hydronephrosis with a<br />
calyx st extending into the<br />
hump. (Right) Longitudinal<br />
color Doppler ultrasound of<br />
the same kidney shows no<br />
distortion of vascular supply in<br />
the dromedary hump ſt.<br />
973


