Diagnostic Ultrasound - Abdomen and Pelvis
Mucinous Cystic Pancreatic Tumor (Left) Transverse transabdominal ultrasound shows a well-defined, anechoic, cystic lesion in the body of the pancreas with a few hyperechoic peripheral foci ſt. Note the normal pancreas st. (Right) Corresponding axial CECT shows an oval, cystic mass in the body of the pancreas with an enhancing capsule st. The lesion contained internal septations not seen on CT. Diagnoses: Pancreas (Left) Coronal CECT demonstrates a wellcircumscribed, round cystic mass in the tail of the pancreas with subtle internal septations ſt. (Right) Corresponding endoscopic ultrasound demonstrates a large cystic mass with internal septations ſt and a small mural nodule (calipers), which was not well seen on CT. (Left) Axial CECT shows a wellcircumscribed, rounded, cystic mass in the tail of the pancreas with subtle enhancing internal septations st. (Right) Endoscopic ultrasound demonstrates a well-defined, multilocular cystic lesion in the tail of the pancreas with internal septations ſt. 369
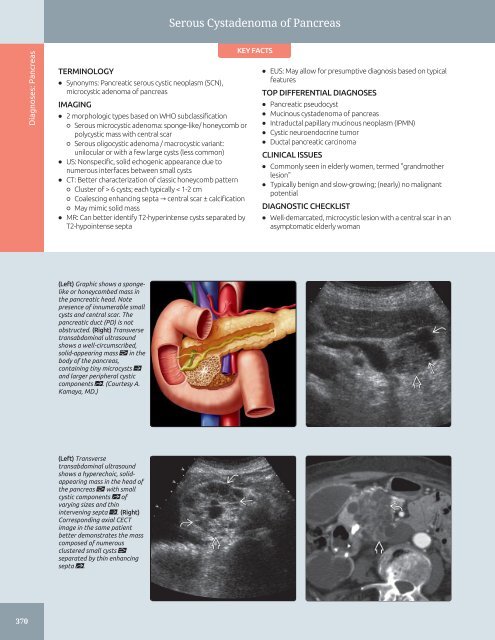
Serous Cystadenoma of Pancreas Diagnoses: Pancreas TERMINOLOGY • Synonyms: Pancreatic serous cystic neoplasm (SCN), microcystic adenoma of pancreas IMAGING • 2 morphologic types based on WHO subclassification ○ Serous microcystic adenoma: sponge-like/ honeycomb or polycystic mass with central scar ○ Serous oligocystic adenoma / macrocystic variant: unilocular or with a few large cysts (less common) • US: Nonspecific, solid echogenic appearance due to numerous interfaces between small cysts • CT: Better characterization of classic honeycomb pattern ○ Cluster of > 6 cysts; each typically < 1-2 cm ○ Coalescing enhancing septa → central scar ± calcification ○ May mimic solid mass • MR: Can better identify T2-hyperintense cysts separated by T2-hypointense septa KEY FACTS • EUS: May allow for presumptive diagnosis based on typical features TOP DIFFERENTIAL DIAGNOSES • Pancreatic pseudocyst • Mucinous cystadenoma of pancreas • Intraductal papillary mucinous neoplasm (IPMN) • Cystic neuroendocrine tumor • Ductal pancreatic carcinoma CLINICAL ISSUES • Commonly seen in elderly women, termed "grandmother lesion" • Typically benign and slow-growing; (nearly) no malignant potential DIAGNOSTIC CHECKLIST • Well-demarcated, microcystic lesion with a central scar in an asymptomatic elderly woman (Left) Graphic shows a spongelike or honeycombed mass in the pancreatic head. Note presence of innumerable small cysts and central scar. The pancreatic duct (PD) is not obstructed. (Right) Transverse transabdominal ultrasound shows a well-circumscribed, solid-appearing mass in the body of the pancreas, containing tiny microcysts ſt and larger peripheral cystic components st. (Courtesy A. Kamaya, MD.) (Left) Transverse transabdominal ultrasound shows a hyperechoic, solidappearing mass in the head of the pancreas with small cystic components st of varying sizes and thin intervening septa ſt. (Right) Corresponding axial CECT image in the same patient better demonstrates the mass composed of numerous clustered small cysts separated by thin enhancing septa st. 370
- Page 340 and 341: Gallbladder Carcinoma TERMINOLOGY A
- Page 342 and 343: Gallbladder Carcinoma (Left) Sagitt
- Page 344 and 345: Biliary Ductal Dilatation IMAGING G
- Page 346 and 347: Choledochal Cyst TERMINOLOGY Synony
- Page 348 and 349: Choledochal Cyst (Left) Longitudina
- Page 350 and 351: Choledocholithiasis TERMINOLOGY Abb
- Page 352 and 353: Choledocholithiasis (Left) A single
- Page 354 and 355: Biliary Ductal Gas TERMINOLOGY Syno
- Page 356 and 357: Cholangiocarcinoma TERMINOLOGY Syno
- Page 358 and 359: Cholangiocarcinoma (Left) Ultrasoun
- Page 360 and 361: Ascending Cholangitis TERMINOLOGY S
- Page 362 and 363: Ascending Cholangitis (Left) Longit
- Page 364 and 365: Recurrent Pyogenic Cholangitis TERM
- Page 366 and 367: Recurrent Pyogenic Cholangitis (Lef
- Page 368 and 369: AIDS-Related Cholangiopathy TERMINO
- Page 370 and 371: PART II SECTION 3 Pancreas Introduc
- Page 372 and 373: Approach to Pancreatic Sonography C
- Page 374 and 375: Approach to Pancreatic Sonography (
- Page 376 and 377: Acute Pancreatitis TERMINOLOGY Abbr
- Page 378 and 379: Acute Pancreatitis (Left) Transvers
- Page 380 and 381: Pancreatic Pseudocyst TERMINOLOGY D
- Page 382 and 383: Pancreatic Pseudocyst (Left) Transv
- Page 384 and 385: Chronic Pancreatitis TERMINOLOGY Ab
- Page 386 and 387: Chronic Pancreatitis (Left) Transve
- Page 388 and 389: Mucinous Cystic Pancreatic Tumor TE
- Page 392 and 393: Serous Cystadenoma of Pancreas TERM
- Page 394 and 395: Serous Cystadenoma of Pancreas (Lef
- Page 396 and 397: Intraductal Papillary Mucinous Neop
- Page 398 and 399: Intraductal Papillary Mucinous Neop
- Page 400 and 401: Intraductal Papillary Mucinous Neop
- Page 402 and 403: Pancreatic Ductal Carcinoma TERMINO
- Page 404 and 405: Pancreatic Ductal Carcinoma (Left)
- Page 406 and 407: Pancreatic Neuroendocrine Tumor TER
- Page 408 and 409: Pancreatic Neuroendocrine Tumor (Le
- Page 410 and 411: Solid Pseudopapillary Neoplasm TERM
- Page 412 and 413: Solid Pseudopapillary Neoplasm (Lef
- Page 414 and 415: PART II SECTION 4 Spleen Introducti
- Page 416 and 417: Approach to Splenic Sonography sple
- Page 418 and 419: Approach to Splenic Sonography (Lef
- Page 420 and 421: Approach to Splenic Sonography (Lef
- Page 422 and 423: Splenomegaly TERMINOLOGY Abbreviati
- Page 424 and 425: Splenomegaly (Left) US in a 92-year
- Page 426 and 427: Splenic Cyst TERMINOLOGY Definition
- Page 428 and 429: Splenic Cyst (Left) Grayscale US of
- Page 430 and 431: Splenic Tumors TERMINOLOGY Definiti
- Page 432 and 433: Splenic Tumors (Left) Longitudinal
- Page 434 and 435: Splenic Tumors (Left) A solid, hypo
- Page 436 and 437: Splenic Infarct TERMINOLOGY Abbrevi
- Page 438 and 439: Splenic Infarct (Left) Power Dopple
Serous Cystadenoma of Pancreas<br />
Diagnoses: Pancreas<br />
TERMINOLOGY<br />
• Synonyms: Pancreatic serous cystic neoplasm (SCN),<br />
microcystic adenoma of pancreas<br />
IMAGING<br />
• 2 morphologic types based on WHO subclassification<br />
○ Serous microcystic adenoma: sponge-like/ honeycomb or<br />
polycystic mass with central scar<br />
○ Serous oligocystic adenoma / macrocystic variant:<br />
unilocular or with a few large cysts (less common)<br />
• US: Nonspecific, solid echogenic appearance due to<br />
numerous interfaces between small cysts<br />
• CT: Better characterization of classic honeycomb pattern<br />
○ Cluster of > 6 cysts; each typically < 1-2 cm<br />
○ Coalescing enhancing septa → central scar ± calcification<br />
○ May mimic solid mass<br />
• MR: Can better identify T2-hyperintense cysts separated by<br />
T2-hypointense septa<br />
KEY FACTS<br />
• EUS: May allow for presumptive diagnosis based on typical<br />
features<br />
TOP DIFFERENTIAL DIAGNOSES<br />
• Pancreatic pseudocyst<br />
• Mucinous cystadenoma of pancreas<br />
• Intraductal papillary mucinous neoplasm (IPMN)<br />
• Cystic neuroendocrine tumor<br />
• Ductal pancreatic carcinoma<br />
CLINICAL ISSUES<br />
• Commonly seen in elderly women, termed "gr<strong>and</strong>mother<br />
lesion"<br />
• Typically benign <strong>and</strong> slow-growing; (nearly) no malignant<br />
potential<br />
DIAGNOSTIC CHECKLIST<br />
• Well-demarcated, microcystic lesion with a central scar in an<br />
asymptomatic elderly woman<br />
(Left) Graphic shows a spongelike<br />
or honeycombed mass in<br />
the pancreatic head. Note<br />
presence of innumerable small<br />
cysts <strong>and</strong> central scar. The<br />
pancreatic duct (PD) is not<br />
obstructed. (Right) Transverse<br />
transabdominal ultrasound<br />
shows a well-circumscribed,<br />
solid-appearing mass in the<br />
body of the pancreas,<br />
containing tiny microcysts ſt<br />
<strong>and</strong> larger peripheral cystic<br />
components st. (Courtesy A.<br />
Kamaya, MD.)<br />
(Left) Transverse<br />
transabdominal ultrasound<br />
shows a hyperechoic, solidappearing<br />
mass in the head of<br />
the pancreas with small<br />
cystic components st of<br />
varying sizes <strong>and</strong> thin<br />
intervening septa ſt. (Right)<br />
Corresponding axial CECT<br />
image in the same patient<br />
better demonstrates the mass<br />
composed of numerous<br />
clustered small cysts <br />
separated by thin enhancing<br />
septa st.<br />
370


