09.07.2019
•
Views
Ureters and Bladder – Distended bladder may cause ureteral and pelvicalyceal dilation and rescanning post void is beneficial to exclude obstruction ○ Color Doppler evaluation of bladder helps assess normal ureteral jets and helps exclude complete ureteral obstruction • Bladder ○ Recommend fluid intake prior to examination to ensure optimal distension of urinary bladder – In fully distended state, urinary bladder is easily visualized using transabdominal approach ○ Examine patient in supine position with transabdominal suprapubic approach – Perform scanning in sagittal and transverse planes – Patient may be placed in decubitus position, especially to determine mobility of intravesical masses or debris, if present – With smaller volumes, caudal angulation of transducer is needed to visualize urinary bladder in its retropubic location ○ Nature of cystic structure in pelvis may be ascertained by asking patient to void or by inserting Foley catheter ○ In some instances, transvaginal ultrasound may be used in women for evaluation of suspect bladder neck lesions, UVJ stone, or ureterocele ○ Advantages of ultrasound – Radiation-free, real-time assessment with high spatial resolution of bladder and bladder wall – Real-time assessment of intraluminal masses in bladder for mobility and vascularity – Real-time imaging guidance for bladder intervention, e.g., placement of percutaneous suprapubic catheters – Real-time assessment of ureteral jets using color Doppler imaging; particularly useful in pregnant patients with dilated collecting system • Large midline ovarian or pelvic cystic mass may simulate bladder on transabdominal ultrasound ○ Attention to normal bladder shape, rescanning after voiding to confirm empty bladder, or transvaginal imaging is helpful to differentiate Imaging Pitfalls • Bladder ○ Reverberation artifacts are commonly encountered behind anterior wall of urinary bladder – Appear as regularly spaced lines at increasing depth as a result of repeated reflection of ultrasound signals between highly reflective interfaces close to transducer – May be reduced or avoided by changing scanning angle or by moving transducer or using spacer ○ Underdistended bladder may give false impression of wall thickening and limits intraluminal assessment CLINICAL IMPLICATIONS Clinical Importance • Ureters are at high risk of inadvertent injury during abdominal or gynecological surgery due to close proximity to uterine (in uterosacral ligament) and gonadal arteries (at pelvic brim) • Ectopic ureter ○ Usually (80%) associated with complete ureteral duplication; more common in females ○ Ectopic ureteral insertion in females can occur in urethra, vagina leading to urinary incontinence ○ In complete duplication, upper moeity inserts ectopically inferiorly and distally to lower moeity (Weigert-Meyer rule) and can be associated with ureterocele ○ In duplicated system, upper moiety has higher predisposition to obstruction from ureterocele, while lower moiety has predisposition to vesicoureteral reflux • Ureterocele: Cystic dilation of intramural portion of ureter bulging into bladder ○ Orthotopic: Normal insertion of single ureter ○ Ectopic: Inserts below trigone, mostly in duplicated system • Ureteral duplication ○ Bifid ureter drains a duplex kidney but ureters unite before entering bladder • Extraperitoneal bladder rupture ○ Urine and blood distend prevesical space (Retzius) ○ Urine often tracks posteriorly into presacral space, superiorly into retroperitoneal abdomen ○ Usually caused by pelvic fractures • Intraperitoneal bladder rupture ○ Urine flows up paracolic gutters into peritoneal recesses and surrounds bowel ○ Usually caused by blunt trauma to an overdistended bladder ○ Bladder ruptures along dome, which is in contact with intraperitoneal space • Patent fetal urachus forms conduit between umbilicus and bladder ○ Urachus is normally obliterated to form median umbilical ligament ○ May persist as cyst, diverticulum, or rarely, fistula ○ May become infected or lead to carcinoma (adenocarcinoma) • Bladder diverticula are common ○ Congenital: Hutch diverticulum (near ureterovesical junction) ○ Acquired (usually due to chronic bladder outlet obstruction), associated with trabeculated bladder wall ○ Can lead to infection, stones, tumor SELECTED REFERENCES 1. Demir S et al: Value of sonographic anterior-posterior renal pelvis measurements before and after voiding for predicting vesicoureteral reflux in children. J Clin Ultrasound. ePub, 2014 2. Butler P, Mitchell A, Healy JC. Applied Radiological Anatomy. Cambridge University Press. 2012 3. Shimoya K et al: Diagnosis of ureterocele with transvaginal sonography. Gynecol Obstet Invest. 54(1):58-60, 2002 4. Djavan B et al: Bladder ultrasonography. Semin Urol. 12(4):306-19, 1994 5. Hayden CK Jr et al: Urinary tract infections in childhood: a current imaging approach. Radiographics. 6(6):1023-38, 1986 6. Glassberg KI et al: Suggested terminology for duplex systems, ectopic ureters and ureteroceles. J Urol. 132(6):1153-4, 1984 Anatomy: Pelvis 111
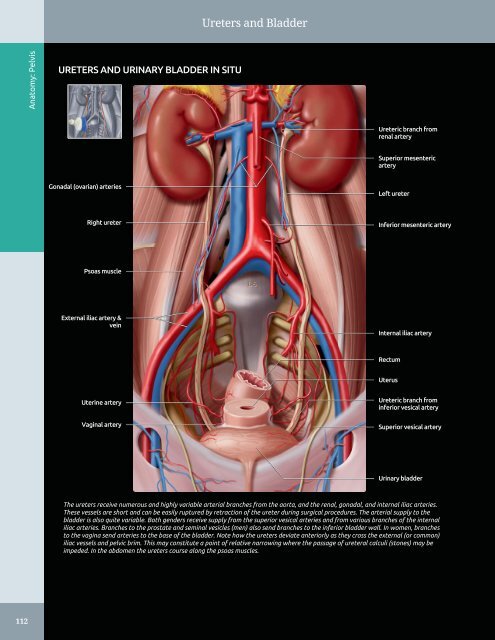
Ureters and Bladder Anatomy: Pelvis URETERS AND URINARY BLADDER IN SITU Ureteric branch from renal artery Superior mesenteric artery Gonadal (ovarian) arteries Left ureter Right ureter Inferior mesenteric artery Psoas muscle External iliac artery & vein Internal iliac artery Rectum Uterus Uterine artery Vaginal artery Ureteric branch from inferior vesical artery Superior vesical artery Urinary bladder The ureters receive numerous and highly variable arterial branches from the aorta, and the renal, gonadal, and internal iliac arteries. These vessels are short and can be easily ruptured by retraction of the ureter during surgical procedures. The arterial supply to the bladder is also quite variable. Both genders receive supply from the superior vesical arteries and from various branches of the internal iliac arteries. Branches to the prostate and seminal vesicles (men) also send branches to the inferior bladder wall. In women, branches to the vagina send arteries to the base of the bladder. Note how the ureters deviate anteriorly as they cross the external (or common) iliac vessels and pelvic brim. This may constitute a point of relative narrowing where the passage of ureteral calculi (stones) may be impeded. In the abdomen the ureters course along the psoas muscles. 112
-
Page 2 and 3:
Diagnostic Ultrasound
-
Page 4 and 5:
Diagnostic Ultrasound Aya Kamaya, M
-
Page 6 and 7:
Dedications To my sweet and support
-
Page 8 and 9:
Asef Khwaja, MD Assistant Professor
-
Page 10 and 11:
Preface
-
Page 12 and 13:
Acknowledgements Text Editors Nina
-
Page 14 and 15:
Sections PART I - Anatomy SECTION 1
-
Page 16 and 17:
TABLE OF CONTENTS VASCULAR CONDITIO
-
Page 18 and 19:
TABLE OF CONTENTS 562 Perigraft Flu
-
Page 20 and 21:
TABLE OF CONTENTS 906 Hyperechoic G
-
Page 22 and 23:
Diagnostic Ultrasound
-
Page 24 and 25:
PART I SECTION 1 Abdomen Liver 4 Bi
-
Page 26 and 27:
Liver ○ Appear as echolucent defe
-
Page 28 and 29:
Liver Coronary ligament HEPATIC ATT
-
Page 30 and 31:
Liver Segment 8 HEPATIC SEGMENTS Se
-
Page 32 and 33:
Liver Rectus abdominis muscle LEFT
-
Page 34 and 35:
Liver Abdominal muscle LEFT LOBE OF
-
Page 36 and 37:
Liver Anterior right portal vein RI
-
Page 38 and 39:
Liver PORTA HEPATIS Anatomy: Abdome
-
Page 40 and 41:
Liver Inferior liver margin OTHER V
-
Page 42 and 43:
Biliary System • Harmonic imaging
-
Page 44 and 45:
Biliary System Left hepatic duct Ri
-
Page 46 and 47:
Biliary System Right rectus muscle
-
Page 48 and 49:
Biliary System COMMON BILE DUCT Ana
-
Page 50 and 51:
Biliary System LEFT INTRAHEPATIC DU
-
Page 52 and 53:
Spleen SPLEEN ANATOMY AND HISTOLOGY
-
Page 54 and 55:
Spleen Fat in splenic hilum Left he
-
Page 56 and 57:
Spleen SPLENIC VESSELS Anatomy: Abd
-
Page 58 and 59:
Spleen Splenosis ANATOMICAL VARIANT
-
Page 60 and 61:
Pancreas PANCREAS IN SITU Anatomy:
-
Page 62 and 63:
Pancreas PANCREAS, TRANSVERSE VIEW
-
Page 64 and 65:
Pancreas Left lobe of liver PANCREA
-
Page 66 and 67:
Kidneys - Normal peak systolic velo
-
Page 68 and 69:
Kidneys KIDNEY ARTERIES AND INTERIO
-
Page 70 and 71:
Kidneys RENAL FASCIA AND PERIRENAL
-
Page 72 and 73:
Kidneys Right hemidiaphragm RIGHT K
-
Page 74 and 75:
Kidneys RIGHT KIDNEY, CT CORRELATIO
-
Page 76 and 77:
Kidneys Right erector spinae muscle
-
Page 78 and 79:
Kidneys RIGHT INTRARENAL ARTERY AND
-
Page 80 and 81:
Kidneys LEFT KIDNEY, CT CORRELATION
-
Page 82 and 83:
Kidneys LEFT KIDNEY, CT CORRELATION
-
Page 84 and 85:
Kidneys Subcutaneous fat Left latis
-
Page 86 and 87:
Kidneys LEFT MAIN RENAL ARTERY AND
-
Page 88 and 89:
Kidneys Right lobe of liver MULTIPL
-
Page 90 and 91:
Bowel - Forms an incomplete ring in
-
Page 92 and 93:
Bowel Falciform ligament STOMACH AN
-
Page 94 and 95:
Bowel SMALL INTESTINE Anatomy: Abdo
-
Page 96 and 97:
Bowel Abdominal wall STOMACH Anatom
-
Page 98 and 99:
Bowel Rectus muscle SMALL BOWEL Ana
-
Page 100 and 101:
Bowel Abdominal wall musculature Ce
-
Page 102 and 103:
Bowel LARGE BOWEL Abdominal wall mu
-
Page 104 and 105:
Bowel Urinary bladder RECTOSIGMOID
-
Page 106 and 107:
Abdominal Lymph Nodes RETROPERITONE
-
Page 108 and 109:
Abdominal Lymph Nodes LYMPHANGIOGRA
-
Page 110 and 111:
Peritoneal Spaces and Structures PE
-
Page 112 and 113:
Peritoneal Spaces and Structures PE
-
Page 114 and 115:
Peritoneal Spaces and Structures Li
-
Page 116 and 117:
Peritoneal Spaces and Structures IN
-
Page 118 and 119:
Abdominal Wall ANTERIOR ABDOMINAL W
-
Page 120 and 121:
Abdominal Wall MUSCLES OF BACK IN S
-
Page 122 and 123:
Abdominal Wall Subcutaneous fat Rig
-
Page 124 and 125:
Abdominal Wall Right lobe of liver
-
Page 126 and 127:
Abdominal Wall Right rectus abdomin
-
Page 128 and 129:
Abdominal Wall Subcutaneous fat Rig
-
Page 130 and 131:
PART I SECTION 2 Pelvis Ureters and
-
Page 134 and 135:
Ureters and Bladder URINARY BLADDER
-
Page 136 and 137:
Ureters and Bladder CT UROGRAM CORR
-
Page 138 and 139:
Ureters and Bladder Liver URETER An
-
Page 140 and 141:
Ureters and Bladder WEIGERT-MEYER L
-
Page 142 and 143:
Prostate ○ Sac-like structures su
-
Page 144 and 145:
Prostate ZONAL ANATOMY OF THE PROST
-
Page 146 and 147:
Prostate SEMINAL VESICLES AND VAS D
-
Page 148 and 149:
Prostate PROSTATE ANATOMY Anatomy:
-
Page 150 and 151:
Testes ○ Internal oblique muscle
-
Page 152 and 153:
Testes EPIDIDYMIS AND SCROTAL WALL
-
Page 154 and 155:
Testes TESTIS, SAGITTAL VIEW Anatom
-
Page 156 and 157:
Testes Scrotal wall EPIDIDYMIS, HEA
-
Page 158 and 159:
Testes TESTICULAR AND EPIDIDYMAL AP
-
Page 160 and 161:
Testes ARTERIAL AND VENOUS SUPPLY A
-
Page 162 and 163:
Uterus ARTERIES OF UTERUS AND ADJAC
-
Page 164 and 165:
Uterus NORMAL VARIATIONS, UTERINE P
-
Page 166 and 167:
Uterus UTERINE VARIATIONS WITH AGE
-
Page 168 and 169:
Uterus CYCLIC CHANGES OF ENDOMETRIU
-
Page 170 and 171:
Uterus FALLOPIAN TUBE Anatomy: Pelv
-
Page 172 and 173:
Cervix GRAPHICS OF CERVIX ANATOMY A
-
Page 174 and 175:
Cervix TRANSVAGINAL ULTRASOUND OF C
-
Page 176 and 177:
Cervix CHANGES OF CERVIX DURING PRE
-
Page 178 and 179:
Vagina GRAPHICS OF NORMAL VAGINAL A
-
Page 180 and 181:
Vagina Urinary bladder TRANSVERSE U
-
Page 182 and 183:
Vagina SPECTRAL WAVEFORM OF VAGINAL
-
Page 184 and 185:
Ovaries Mesosalpinx LIGAMENTOUS SUP
-
Page 186 and 187:
Ovaries Transvaginal transducer NOR
-
Page 188 and 189:
Ovaries Ovarian artery SPECTRAL WAV
-
Page 190 and 191:
Ovaries CYCLIC CHANGES OF OVARY Ana
-
Page 192 and 193:
Ovaries CYCLIC CHANGES OF INTRAOVAR
-
Page 194 and 195:
Liver Transplant Hepatic Artery Ste
-
Page 196 and 197:
Approach to Hepatic Sonography (Lef
-
Page 198 and 199:
Approach to Hepatic Sonography (Lef
-
Page 200 and 201:
Acute Hepatitis TERMINOLOGY Definit
-
Page 202 and 203:
Acute Hepatitis (Left) Transverse g
-
Page 204 and 205:
Hepatic Cirrhosis TERMINOLOGY Defin
-
Page 206 and 207:
Hepatic Cirrhosis (Left) Longitudin
-
Page 208 and 209:
Hepatic Steatosis TERMINOLOGY Synon
-
Page 210 and 211:
Hepatic Steatosis (Left) Transverse
-
Page 212 and 213:
Hepatic Schistosomiasis TERMINOLOGY
-
Page 214 and 215:
Venoocclusive Disease TERMINOLOGY A
-
Page 216 and 217:
Venoocclusive Disease (Left) Graysc
-
Page 218 and 219:
Hepatic Cyst TERMINOLOGY Synonyms
-
Page 220 and 221:
Hepatic Cyst (Left) Transverse and
-
Page 222 and 223:
Biliary Hamartoma TERMINOLOGY Synon
-
Page 224 and 225:
Biliary Hamartoma (Left) Ultrasound
-
Page 226 and 227:
Caroli Disease TERMINOLOGY Synonyms
-
Page 228 and 229:
Caroli Disease (Left) Oblique abdom
-
Page 230 and 231:
Biloma TERMINOLOGY Definitions •
-
Page 232 and 233:
Biliary Cystadenoma/Carcinoma TERMI
-
Page 234 and 235:
Biliary Cystadenoma/Carcinoma (Left
-
Page 236 and 237:
Pyogenic Hepatic Abscess TERMINOLOG
-
Page 238 and 239:
Pyogenic Hepatic Abscess (Left) Obl
-
Page 240 and 241:
Amebic Hepatic Abscess TERMINOLOGY
-
Page 242 and 243:
Amebic Hepatic Abscess (Left) Longi
-
Page 244 and 245:
Hepatic Echinococcus Cyst TERMINOLO
-
Page 246 and 247:
Hepatic Echinococcus Cyst (Left) Ob
-
Page 248 and 249:
Hepatic Diffuse Microabscesses TERM
-
Page 250 and 251:
Peribiliary Cyst TERMINOLOGY Synony
-
Page 252 and 253:
Ciliated Hepatic Foregut Cyst TERMI
-
Page 254 and 255:
Hepatic Cavernous Hemangioma TERMIN
-
Page 256 and 257:
Hepatic Cavernous Hemangioma (Left)
-
Page 258 and 259:
Hepatic Cavernous Hemangioma (Left)
-
Page 260 and 261:
Focal Nodular Hyperplasia TERMINOLO
-
Page 262 and 263:
Focal Nodular Hyperplasia (Left) Tr
-
Page 264 and 265:
Hepatic Adenoma TERMINOLOGY Synonym
-
Page 266 and 267:
Hepatic Adenoma (Left) Transverse t
-
Page 268 and 269:
Hepatocellular Carcinoma TERMINOLOG
-
Page 270 and 271:
Hepatocellular Carcinoma (Left) Tra
-
Page 272 and 273:
Hepatocellular Carcinoma (Left) Tra
-
Page 274 and 275:
Hepatic Metastases TERMINOLOGY Defi
-
Page 276 and 277:
Hepatic Metastases (Left) Transvers
-
Page 278 and 279:
Hepatic Lymphoma TERMINOLOGY Defini
-
Page 280 and 281:
Hepatic Lymphoma (Left) Transverse
-
Page 282 and 283:
Transjugular Intrahepatic Portosyst
-
Page 284 and 285:
Transjugular Intrahepatic Portosyst
-
Page 286 and 287:
Portal Vein Occlusion TERMINOLOGY A
-
Page 288 and 289:
Portal Vein Occlusion (Left) Color
-
Page 290 and 291:
Budd-Chiari Syndrome TERMINOLOGY Ab
-
Page 292 and 293:
Budd-Chiari Syndrome (Left) Color D
-
Page 294 and 295:
Portal Vein Gas TERMINOLOGY Abbrevi
-
Page 296 and 297:
Liver Transplant Portal Vein Stenos
-
Page 298 and 299:
Liver Transplant Biliary Stricture
-
Page 300 and 301:
PART II SECTION 2 Biliary System In
-
Page 302 and 303:
Approach to Biliary Sonography hosp
-
Page 304 and 305:
Approach to Biliary Sonography (Lef
-
Page 306 and 307:
Approach to Biliary Sonography (Lef
-
Page 308 and 309:
Cholelithiasis TERMINOLOGY Synonyms
-
Page 310 and 311:
Cholelithiasis (Left) Longitudinal
-
Page 312 and 313:
Cholelithiasis (Left) Abdominal rad
-
Page 314 and 315:
Echogenic Bile TERMINOLOGY Synonyms
-
Page 316 and 317:
Echogenic Bile (Left) Transverse ul
-
Page 318 and 319:
Gallbladder Cholesterol Polyp TERMI
-
Page 320 and 321:
Gallbladder Cholesterol Polyp (Left
-
Page 322 and 323:
Acute Calculous Cholecystitis TERMI
-
Page 324 and 325:
Acute Calculous Cholecystitis (Left
-
Page 326 and 327:
Acute Acalculous Cholecystitis TERM
-
Page 328 and 329:
Acute Acalculous Cholecystitis (Lef
-
Page 330 and 331:
Chronic Cholecystitis TERMINOLOGY D
-
Page 332 and 333:
Xanthogranulomatous Cholecystitis T
-
Page 334 and 335:
Porcelain Gallbladder TERMINOLOGY A
-
Page 336 and 337:
Hyperplastic Cholecystosis (Adenomy
-
Page 338 and 339:
Hyperplastic Cholecystosis (Adenomy
-
Page 340 and 341:
Gallbladder Carcinoma TERMINOLOGY A
-
Page 342 and 343:
Gallbladder Carcinoma (Left) Sagitt
-
Page 344 and 345:
Biliary Ductal Dilatation IMAGING G
-
Page 346 and 347:
Choledochal Cyst TERMINOLOGY Synony
-
Page 348 and 349:
Choledochal Cyst (Left) Longitudina
-
Page 350 and 351:
Choledocholithiasis TERMINOLOGY Abb
-
Page 352 and 353:
Choledocholithiasis (Left) A single
-
Page 354 and 355:
Biliary Ductal Gas TERMINOLOGY Syno
-
Page 356 and 357:
Cholangiocarcinoma TERMINOLOGY Syno
-
Page 358 and 359:
Cholangiocarcinoma (Left) Ultrasoun
-
Page 360 and 361:
Ascending Cholangitis TERMINOLOGY S
-
Page 362 and 363:
Ascending Cholangitis (Left) Longit
-
Page 364 and 365:
Recurrent Pyogenic Cholangitis TERM
-
Page 366 and 367:
Recurrent Pyogenic Cholangitis (Lef
-
Page 368 and 369:
AIDS-Related Cholangiopathy TERMINO
-
Page 370 and 371:
PART II SECTION 3 Pancreas Introduc
-
Page 372 and 373:
Approach to Pancreatic Sonography C
-
Page 374 and 375:
Approach to Pancreatic Sonography (
-
Page 376 and 377:
Acute Pancreatitis TERMINOLOGY Abbr
-
Page 378 and 379:
Acute Pancreatitis (Left) Transvers
-
Page 380 and 381:
Pancreatic Pseudocyst TERMINOLOGY D
-
Page 382 and 383:
Pancreatic Pseudocyst (Left) Transv
-
Page 384 and 385:
Chronic Pancreatitis TERMINOLOGY Ab
-
Page 386 and 387:
Chronic Pancreatitis (Left) Transve
-
Page 388 and 389:
Mucinous Cystic Pancreatic Tumor TE
-
Page 390 and 391:
Mucinous Cystic Pancreatic Tumor (L
-
Page 392 and 393:
Serous Cystadenoma of Pancreas TERM
-
Page 394 and 395:
Serous Cystadenoma of Pancreas (Lef
-
Page 396 and 397:
Intraductal Papillary Mucinous Neop
-
Page 398 and 399:
Intraductal Papillary Mucinous Neop
-
Page 400 and 401:
Intraductal Papillary Mucinous Neop
-
Page 402 and 403:
Pancreatic Ductal Carcinoma TERMINO
-
Page 404 and 405:
Pancreatic Ductal Carcinoma (Left)
-
Page 406 and 407:
Pancreatic Neuroendocrine Tumor TER
-
Page 408 and 409:
Pancreatic Neuroendocrine Tumor (Le
-
Page 410 and 411:
Solid Pseudopapillary Neoplasm TERM
-
Page 412 and 413:
Solid Pseudopapillary Neoplasm (Lef
-
Page 414 and 415:
PART II SECTION 4 Spleen Introducti
-
Page 416 and 417:
Approach to Splenic Sonography sple
-
Page 418 and 419:
Approach to Splenic Sonography (Lef
-
Page 420 and 421:
Approach to Splenic Sonography (Lef
-
Page 422 and 423:
Splenomegaly TERMINOLOGY Abbreviati
-
Page 424 and 425:
Splenomegaly (Left) US in a 92-year
-
Page 426 and 427:
Splenic Cyst TERMINOLOGY Definition
-
Page 428 and 429:
Splenic Cyst (Left) Grayscale US of
-
Page 430 and 431:
Splenic Tumors TERMINOLOGY Definiti
-
Page 432 and 433:
Splenic Tumors (Left) Longitudinal
-
Page 434 and 435:
Splenic Tumors (Left) A solid, hypo
-
Page 436 and 437:
Splenic Infarct TERMINOLOGY Abbrevi
-
Page 438 and 439:
Splenic Infarct (Left) Power Dopple
-
Page 440 and 441:
Vascular Conditions Renal Artery St
-
Page 442 and 443:
Approach to Urinary Tract Sonograph
-
Page 444 and 445:
Approach to Urinary Tract Sonograph
-
Page 446 and 447:
Column of Bertin, Kidney TERMINOLOG
-
Page 448 and 449:
Renal Junction Line TERMINOLOGY Syn
-
Page 450 and 451:
Renal Ectopia TERMINOLOGY Abbreviat
-
Page 452 and 453:
Renal Ectopia (Left) Grayscale ultr
-
Page 454 and 455:
Horseshoe Kidney TERMINOLOGY Defini
-
Page 456 and 457:
Horseshoe Kidney (Left) Longitudina
-
Page 458 and 459:
Ureteral Duplication TERMINOLOGY Sy
-
Page 460 and 461:
Ureteral Duplication (Left) Longitu
-
Page 462 and 463:
Ureteral Ectopia TERMINOLOGY Abbrev
-
Page 464 and 465:
Ureteral Ectopia (Left) Coronal T2
-
Page 466 and 467:
Ureteropelvic Junction Obstruction
-
Page 468 and 469:
Ureteropelvic Junction Obstruction
-
Page 470 and 471:
Urolithiasis TERMINOLOGY Abbreviati
-
Page 472 and 473:
Urolithiasis (Left) Longitudinal US
-
Page 474 and 475:
Urolithiasis (Left) Intravenous pye
-
Page 476 and 477:
Nephrocalcinosis TERMINOLOGY Abbrev
-
Page 478 and 479:
Nephrocalcinosis (Left) Coronal MIP
-
Page 480 and 481:
Hydronephrosis TERMINOLOGY Synonyms
-
Page 482 and 483:
Hydronephrosis (Left) Longitudinal
-
Page 484 and 485:
Simple Renal Cyst TERMINOLOGY Defin
-
Page 486 and 487:
Simple Renal Cyst (Left) Longitudin
-
Page 488 and 489:
Complex Renal Cyst TERMINOLOGY Defi
-
Page 490 and 491:
Complex Renal Cyst (Left) Transvers
-
Page 492 and 493:
Cystic Disease of Dialysis TERMINOL
-
Page 494 and 495:
Cystic Disease of Dialysis (Left) L
-
Page 496 and 497:
Multilocular Cystic Nephroma TERMIN
-
Page 498 and 499:
Acute Pyelonephritis TERMINOLOGY Ab
-
Page 500 and 501:
Acute Pyelonephritis (Left) Longitu
-
Page 502 and 503:
Renal Abscess TERMINOLOGY Definitio
-
Page 504 and 505:
Emphysematous Pyelonephritis TERMIN
-
Page 506 and 507:
Emphysematous Pyelonephritis (Left)
-
Page 508 and 509:
Pyonephrosis TERMINOLOGY Definition
-
Page 510 and 511:
Xanthogranulomatous Pyelonephritis
-
Page 512 and 513:
Tuberculosis, Urinary Tract TERMINO
-
Page 514 and 515:
Tuberculosis, Urinary Tract (Left)
-
Page 516 and 517:
Renal Cell Carcinoma TERMINOLOGY Ab
-
Page 518 and 519:
Renal Cell Carcinoma (Left) Longitu
-
Page 520 and 521:
Renal Metastases IMAGING General Fe
-
Page 522 and 523:
Renal Angiomyolipoma TERMINOLOGY Ab
-
Page 524 and 525:
Renal Angiomyolipoma (Left) Longitu
-
Page 526 and 527:
Upper Tract Urothelial Carcinoma TE
-
Page 528 and 529:
Upper Tract Urothelial Carcinoma (L
-
Page 530 and 531:
Renal Lymphoma TERMINOLOGY Abbrevia
-
Page 532 and 533:
Renal Lymphoma (Left) Longitudinal
-
Page 534 and 535:
Renal Artery Stenosis TERMINOLOGY A
-
Page 536 and 537:
Renal Artery Stenosis (Left) Obliqu
-
Page 538 and 539:
Renal Vein Thrombosis TERMINOLOGY A
-
Page 540 and 541:
Renal Vein Thrombosis (Left) Longit
-
Page 542 and 543:
Renal Infarct TERMINOLOGY Definitio
-
Page 544 and 545:
Perinephric Hematoma TERMINOLOGY De
-
Page 546 and 547:
Prostatic Hyperplasia TERMINOLOGY A
-
Page 548 and 549:
Prostatic Hyperplasia (Left) Axial
-
Page 550 and 551:
Prostatic Carcinoma TERMINOLOGY Abb
-
Page 552 and 553:
Prostatic Carcinoma (Left) Transver
-
Page 554 and 555:
Prostatic Carcinoma (Left) Transver
-
Page 556 and 557:
Bladder Carcinoma TERMINOLOGY Defin
-
Page 558 and 559:
Bladder Carcinoma (Left) Transverse
-
Page 560 and 561:
Ureterocele TERMINOLOGY Definitions
-
Page 562 and 563:
Ureterocele (Left) Transabdominal l
-
Page 564 and 565:
Bladder Diverticulum TERMINOLOGY Ab
-
Page 566 and 567:
Bladder Diverticulum (Left) Transab
-
Page 568 and 569:
Bladder Calculi TERMINOLOGY Synonym
-
Page 570 and 571:
Schistosomiasis, Bladder TERMINOLOG
-
Page 572 and 573:
PART II SECTION 6 Kidney Transplant
-
Page 574 and 575:
Approach to Sonography of Renal All
-
Page 576 and 577:
Approach to Sonography of Renal All
-
Page 578 and 579:
Approach to Sonography of Renal All
-
Page 580 and 581:
Allograft Hydronephrosis TERMINOLOG
-
Page 582 and 583:
Allograft Hydronephrosis (Left) Lon
-
Page 584 and 585:
Perigraft Fluid Collections TERMINO
-
Page 586 and 587:
Perigraft Fluid Collections (Left)
-
Page 588 and 589:
Transplant Renal Artery Stenosis TE
-
Page 590 and 591:
Transplant Renal Artery Stenosis (L
-
Page 592 and 593:
Transplant Renal Artery Thrombosis
-
Page 594 and 595:
Transplant Renal Vein Thrombosis TE
-
Page 596 and 597:
Renal Transplant Arteriovenous (AV)
-
Page 598 and 599:
Renal Transplant Pseudoaneurysm TER
-
Page 600 and 601:
Renal Transplant Rejection IMAGING
-
Page 602 and 603:
Delayed Renal Graft Function TERMIN
-
Page 604 and 605:
PART II SECTION 7 Adrenal Gland Adr
-
Page 606 and 607:
Adrenal Hemorrhage TERMINOLOGY Abbr
-
Page 608 and 609:
Adrenal Hemorrhage (Left) Longitudi
-
Page 610 and 611:
Myelolipoma TERMINOLOGY Definitions
-
Page 612 and 613:
Myelolipoma (Left) Longitudinal US
-
Page 614 and 615:
Adrenal Adenoma TERMINOLOGY Synonym
-
Page 616 and 617:
Adrenal Adenoma (Left) Longitudinal
-
Page 618 and 619:
Adrenal Cyst TERMINOLOGY Definition
-
Page 620 and 621:
Pheochromocytoma TERMINOLOGY Defini
-
Page 622 and 623:
Pheochromocytoma (Left) Longitudina
-
Page 624 and 625:
Adrenal Carcinoma TERMINOLOGY Synon
-
Page 626 and 627:
Adrenal Carcinoma (Left) Transverse
-
Page 628 and 629:
PART II SECTION 8 Abdominal Wall/Pe
-
Page 630 and 631:
Approach to Sonography of Abdominal
-
Page 632 and 633:
Approach to Sonography of Abdominal
-
Page 634 and 635:
Abdominal Wall Hernia TERMINOLOGY D
-
Page 636 and 637:
Abdominal Wall Hernia (Left) Transv
-
Page 638 and 639:
Abdominal Wall Hernia (Left) Transv
-
Page 640 and 641:
Groin Hernia TERMINOLOGY Definition
-
Page 642 and 643:
Groin Hernia (Left) Graphic shows a
-
Page 644 and 645:
Groin Hernia (Left) Longitudinal ul
-
Page 646 and 647:
Ascites TERMINOLOGY Definitions •
-
Page 648 and 649:
Ascites (Left) Transverse ultrasoun
-
Page 650 and 651:
Peritoneal Carcinomatosis TERMINOLO
-
Page 652 and 653:
Peritoneal Carcinomatosis (Left) Lo
-
Page 654 and 655:
Peritoneal Carcinomatosis (Left) Tr
-
Page 656 and 657:
Peritoneal Space Abscess TERMINOLOG
-
Page 658 and 659:
Peritoneal Space Abscess (Left) Tra
-
Page 660 and 661:
Segmental Omental Infarction TERMIN
-
Page 662 and 663:
PART II SECTION 9 Bowel Approach to
-
Page 664 and 665:
Approach to Bowel Sonography Given
-
Page 666 and 667:
Approach to Bowel Sonography (Left)
-
Page 668 and 669:
Appendicitis TERMINOLOGY Definition
-
Page 670 and 671:
Appendicitis (Left) Axial ultrasoun
-
Page 672 and 673:
Appendicitis (Left) Axial ultrasoun
-
Page 674 and 675:
Appendiceal Mucocele TERMINOLOGY De
-
Page 676 and 677:
Appendiceal Mucocele (Left) Sagitta
-
Page 678 and 679:
Intussusception TERMINOLOGY Definit
-
Page 680 and 681:
Intussusception (Left) Transverse t
-
Page 682 and 683:
Epiploic Appendagitis TERMINOLOGY A
-
Page 684 and 685:
Epiploic Appendagitis (Left) Graysc
-
Page 686 and 687:
Diverticulitis TERMINOLOGY Definiti
-
Page 688 and 689:
Diverticulitis (Left) Acute diverti
-
Page 690 and 691:
Crohn Disease TERMINOLOGY Synonyms
-
Page 692 and 693:
Crohn Disease (Left) Long-axis ultr
-
Page 694 and 695:
Crohn Disease (Left) Long-axis ultr
-
Page 696 and 697:
Large Bowel Malignancy TERMINOLOGY
-
Page 698 and 699:
Large Bowel Malignancy (Left) Hepat
-
Page 700 and 701:
PART II SECTION 10 Scrotum Introduc
-
Page 702 and 703:
Approach to Scrotal Sonography (Lef
-
Page 704 and 705:
Testicular Germ Cell Tumors TERMINO
-
Page 706 and 707:
Testicular Germ Cell Tumors (Left)
-
Page 708 and 709:
Gonadal Stromal Tumors, Testis TERM
-
Page 710 and 711:
Gonadal Stromal Tumors, Testis (Lef
-
Page 712 and 713:
Testicular Lymphoma/Leukemia TERMIN
-
Page 714 and 715:
Epidermoid Cyst TERMINOLOGY Synonym
-
Page 716 and 717:
Tubular Ectasia of Rete Testis TERM
-
Page 718 and 719:
Testicular Microlithiasis TERMINOLO
-
Page 720 and 721:
Testicular Microlithiasis (Left) Tr
-
Page 722 and 723:
Testicular Torsion/Infarction TERMI
-
Page 724 and 725:
Testicular Torsion/Infarction (Left
-
Page 726 and 727:
Undescended Testis TERMINOLOGY Syno
-
Page 728 and 729:
Epididymitis/Orchitis TERMINOLOGY S
-
Page 730 and 731:
Epididymitis/Orchitis (Left) Sagitt
-
Page 732 and 733:
Scrotal Trauma TERMINOLOGY Definiti
-
Page 734 and 735:
Scrotal Trauma (Left) Transverse gr
-
Page 736 and 737:
Hydrocele TERMINOLOGY Definitions
-
Page 738 and 739:
Spermatocele/Epididymal Cyst TERMIN
-
Page 740 and 741:
Adenomatoid Tumor TERMINOLOGY Defin
-
Page 742 and 743:
Varicocele TERMINOLOGY Definitions
-
Page 744 and 745:
Non-Ovarian Cystic Masses Hydrosalp
-
Page 746 and 747:
Approach to Sonography of the Femal
-
Page 748 and 749:
Nabothian Cyst TERMINOLOGY Synonyms
-
Page 750 and 751:
Nabothian Cyst (Left) Longitudinal
-
Page 752 and 753:
Cervical Carcinoma IMAGING General
-
Page 754 and 755:
Cervical Carcinoma (Left) Longitudi
-
Page 756 and 757:
Cervical Carcinoma (Left) Longitudi
-
Page 758 and 759:
Adenomyosis TERMINOLOGY Synonyms
-
Page 760 and 761:
Adenomyosis (Left) Longitudinal tra
-
Page 762 and 763:
Leiomyoma TERMINOLOGY Abbreviations
-
Page 764 and 765:
Leiomyoma (Left) Transvaginal ultra
-
Page 766 and 767:
Leiomyoma (Left) Transverse transab
-
Page 768 and 769:
Uterine Anomalies TERMINOLOGY Abbre
-
Page 770 and 771:
Uterine Anomalies (Left) 3D ultraso
-
Page 772 and 773:
Uterine Anomalies (Left) Graphic of
-
Page 774 and 775:
Hematometrocolpos TERMINOLOGY Abbre
-
Page 776 and 777:
Hematometrocolpos (Left) Transverse
-
Page 778 and 779:
Endometrial Polyp TERMINOLOGY Abbre
-
Page 780 and 781:
Endometrial Polyp (Left) Longitudin
-
Page 782 and 783:
Endometrial Polyp (Left) Transabdom
-
Page 784 and 785:
Endometrial Carcinoma TERMINOLOGY A
-
Page 786 and 787:
Endometrial Carcinoma (Left) Longit
-
Page 788 and 789:
Endometritis TERMINOLOGY Synonyms
-
Page 790 and 791:
Endometritis (Left) Longitudinal tr
-
Page 792 and 793:
Intrauterine Device TERMINOLOGY Abb
-
Page 794 and 795:
Intrauterine Device (Left) Longitud
-
Page 796 and 797:
Tubal Ectopic Pregnancy TERMINOLOGY
-
Page 798 and 799:
Tubal Ectopic Pregnancy (Left) Tran
-
Page 800 and 801:
Tubal Ectopic Pregnancy (Left) Sagi
-
Page 802 and 803:
Unusual Ectopic Pregnancies TERMINO
-
Page 804 and 805:
Unusual Ectopic Pregnancies (Left)
-
Page 806 and 807:
Unusual Ectopic Pregnancies (Left)
-
Page 808 and 809:
Failed First Trimester Pregnancy TE
-
Page 810 and 811:
Failed First Trimester Pregnancy (L
-
Page 812 and 813:
Failed First Trimester Pregnancy (L
-
Page 814 and 815:
Retained Products of Conception TER
-
Page 816 and 817:
Retained Products of Conception (Le
-
Page 818 and 819:
Gestational Trophoblastic Disease T
-
Page 820 and 821:
Gestational Trophoblastic Disease (
-
Page 822 and 823:
Functional Ovarian Cyst TERMINOLOGY
-
Page 824 and 825:
Functional Ovarian Cyst (Left) Typi
-
Page 826 and 827:
Hemorrhagic Cyst TERMINOLOGY Abbrev
-
Page 828 and 829:
Hemorrhagic Cyst (Left) Using color
-
Page 830 and 831:
Ovarian Hyperstimulation Syndrome T
-
Page 832 and 833:
Ovarian Hyperstimulation Syndrome (
-
Page 834 and 835:
Serous Ovarian Cystadenoma/Carcinom
-
Page 836 and 837:
Serous Ovarian Cystadenoma/Carcinom
-
Page 838 and 839:
Mucinous Ovarian Cystadenoma/Carcin
-
Page 840 and 841:
Mucinous Ovarian Cystadenoma/Carcin
-
Page 842 and 843:
Ovarian Teratoma TERMINOLOGY Synony
-
Page 844 and 845:
Ovarian Teratoma (Left) Ultrasound
-
Page 846 and 847:
Polycystic Ovarian Syndrome TERMINO
-
Page 848 and 849:
Endometrioma TERMINOLOGY Synonyms
-
Page 850 and 851:
Endometrioma (Left) Longitudinal en
-
Page 852 and 853:
Hydrosalpinx TERMINOLOGY Definition
-
Page 854 and 855:
Hydrosalpinx (Left) Longitudinal tr
-
Page 856 and 857:
Tubo-Ovarian Abscess TERMINOLOGY De
-
Page 858 and 859:
Tubo-Ovarian Abscess (Left) Longitu
-
Page 860 and 861:
Parovarian Cyst TERMINOLOGY Abbrevi
-
Page 862 and 863:
Peritoneal Inclusion Cyst TERMINOLO
-
Page 864 and 865:
Peritoneal Inclusion Cyst (Left) Sa
-
Page 866 and 867:
Bartholin Cyst TERMINOLOGY Definiti
-
Page 868 and 869:
Gartner Duct Cyst TERMINOLOGY Abbre
-
Page 870 and 871:
Gartner Duct Cyst (Left) Longitudin
-
Page 872 and 873:
Sex Cord-Stromal Tumor TERMINOLOGY
-
Page 874 and 875:
Sex Cord-Stromal Tumor (Left) Trans
-
Page 876 and 877:
Sex Cord-Stromal Tumor (Left) Sagit
-
Page 878 and 879:
Adnexal/Ovarian Torsion TERMINOLOGY
-
Page 880 and 881:
Adnexal/Ovarian Torsion (Left) Long
-
Page 882 and 883:
Ovarian Metastases Including Kruken
-
Page 884 and 885:
Ovarian Metastases Including Kruken
-
Page 886 and 887:
PART III SECTION 1 Liver Hepatomega
-
Page 888 and 889:
Hepatomegaly - Firm consistency (du
-
Page 890 and 891:
Hepatomegaly Lymphoma Lymphoma (Lef
-
Page 892 and 893:
Diffuse Liver Disease Acute/Chronic
-
Page 894 and 895:
Cystic Liver Lesion ○ May be soli
-
Page 896 and 897:
Cystic Liver Lesion Peribiliary Cys
-
Page 898 and 899:
Hypoechoic Liver Mass - Adjacent he
-
Page 900 and 901:
Hypoechoic Liver Mass Infected Bilo
-
Page 902 and 903:
Echogenic Liver Mass • Fibrolamel
-
Page 904 and 905:
Echogenic Liver Mass Hepatic Ligame
-
Page 906 and 907:
Target Lesions in Liver Hepatic Met
-
Page 908 and 909:
Multiple Hepatic Masses ○ Cluster
-
Page 910 and 911:
Multiple Hepatic Masses Cirrhosis W
-
Page 912 and 913:
Hepatic Mass With Central Scar Foca
-
Page 914 and 915:
Periportal Lesion Helpful Clues for
-
Page 916 and 917:
Periportal Lesion Peribiliary Cyst
-
Page 918 and 919:
Irregular Hepatic Surface Subcapsul
-
Page 920 and 921:
Portal Vein Abnormality Bland Porta
-
Page 922 and 923:
PART III SECTION 2 Biliary System
-
Page 924 and 925:
Diffuse Gallbladder Wall Thickening
-
Page 926 and 927:
Diffuse Gallbladder Wall Thickening
-
Page 928 and 929:
Hyperechoic Gallbladder Wall Porcel
-
Page 930 and 931:
Focal Gallbladder Wall Thickening/M
-
Page 932 and 933:
Echogenic Material in Gallbladder S
-
Page 934 and 935:
Dilated Gallbladder ○ Distended n
-
Page 936 and 937:
Dilated Gallbladder Mucocele/Hydrop
-
Page 938 and 939:
Intrahepatic and Extrahepatic Duct
-
Page 940 and 941:
PART III SECTION 3 Pancreas Cystic
-
Page 942 and 943:
Cystic Pancreatic Lesion Helpful Cl
-
Page 944 and 945:
Cystic Pancreatic Lesion Mucinous C
-
Page 946 and 947:
Solid Pancreatic Lesion ○ Usually
-
Page 948 and 949:
Solid Pancreatic Lesion Serous Cyst
-
Page 950 and 951:
Pancreatic Duct Dilatation Chronic
-
Page 952 and 953:
PART III SECTION 4 Spleen Focal Spl
-
Page 954 and 955:
Focal Splenic Lesion - Typically mu
-
Page 956 and 957:
Focal Splenic Lesion Pyogenic Absce
-
Page 958 and 959:
Focal Splenic Lesion Splenic Infarc
-
Page 960 and 961:
PART III SECTION 5 Urinary Tract 9
-
Page 962 and 963:
Intraluminal Bladder Mass Bladder C
-
Page 964 and 965:
Abnormal Bladder Wall □ Uterine c
-
Page 966 and 967:
Abnormal Bladder Wall Invasion by P
-
Page 968 and 969:
PART III SECTION 6 Kidney Enlarged
-
Page 970 and 971:
Enlarged Kidney - Nonneoplastic cau
-
Page 972 and 973:
Enlarged Kidney Perinephric Fluid C
-
Page 974 and 975:
Small Kidney ○ Pseudotumors from
-
Page 976 and 977:
Small Kidney Postobstructive Atroph
-
Page 978 and 979:
Hypoechoic Kidney • Multiple Myel
-
Page 980 and 981:
Hypoechoic Kidney Acute Renal Arter
-
Page 982 and 983:
Hyperechoic Kidney ○ Echogenic co
-
Page 984 and 985:
Hyperechoic Kidney Chronic Glomerul
-
Page 986 and 987:
Cystic Renal Mass ○ Associated wi
-
Page 988 and 989:
Cystic Renal Mass Multicystic Dyspl
-
Page 990 and 991:
Solid Renal Mass • Horseshoe Kidn
-
Page 992 and 993:
Solid Renal Mass Renal Lymphoma Ren
-
Page 994 and 995:
Renal Pseudotumor Column of Bertin
-
Page 996 and 997:
Dilated Renal Pelvis • Intrarenal
-
Page 998 and 999:
Dilated Renal Pelvis Pyonephrosis P
-
Page 1000 and 1001:
PART III SECTION 7 Abdominal Wall/P
-
Page 1002 and 1003:
Diffuse Peritoneal Fluid Hemoperito
-
Page 1004 and 1005:
Solid Peritoneal Mass - Higher dens
-
Page 1006 and 1007:
Solid Peritoneal Mass Mimics Benign
-
Page 1008 and 1009:
Cystic Peritoneal Mass ○ Women of
-
Page 1010 and 1011:
Cystic Peritoneal Mass Pseudomyxoma
-
Page 1012 and 1013:
PART III SECTION 8 Prostate Enlarge
-
Page 1014 and 1015:
Enlarged Prostate Benign Prostatic
-
Page 1016 and 1017:
Focal Lesion in Prostate ○ Variab
-
Page 1018 and 1019:
Focal Lesion in Prostate Müllerian
-
Page 1020 and 1021:
PART III SECTION 9 Bowel Bowel Wall
-
Page 1022 and 1023:
Bowel Wall Thickening - Distal ileu
-
Page 1024 and 1025:
Bowel Wall Thickening Crohn Disease
-
Page 1026 and 1027:
Bowel Wall Thickening Clostridium D
-
Page 1028 and 1029:
PART III SECTION 10 Scrotum 1008
-
Page 1030 and 1031:
Diffuse Testicular Enlargement Test
-
Page 1032 and 1033:
Decreased Testicular Size Testicula
-
Page 1034 and 1035:
Testicular Calcifications Sertoli C
-
Page 1036 and 1037:
Focal Testicular Mass - Most common
-
Page 1038 and 1039:
Focal Testicular Mass Testicular Ly
-
Page 1040 and 1041:
Focal Extratesticular Mass - 3-50 m
-
Page 1042 and 1043:
Focal Extratesticular Mass Inguinal
-
Page 1044 and 1045:
Focal Extratesticular Mass Liposarc
-
Page 1046 and 1047:
Extratesticular Cystic Mass Varicoc
-
Page 1048 and 1049:
PART III SECTION 11 Female Pelvis
-
Page 1050 and 1051:
Cystic Adnexal Mass □ Hemorrhagic
-
Page 1052 and 1053:
Cystic Adnexal Mass Dermoid (Mature
-
Page 1054 and 1055:
Solid Adnexal Mass - May masquerade
-
Page 1056 and 1057:
Solid Adnexal Mass Fibrothecoma Hem
-
Page 1058 and 1059:
Extraovarian Adnexal Mass Helpful C
-
Page 1060 and 1061:
Extraovarian Adnexal Mass Paraovari
-
Page 1062 and 1063:
Extraovarian Adnexal Mass Lymph Nod
-
Page 1064 and 1065:
Enlarged Ovary - Often bilateral (5
-
Page 1066 and 1067:
Enlarged Ovary Theca Lutein Cysts T
-
Page 1068 and 1069:
Enlarged Uterus Leiomyoma Adenomyos
-
Page 1070 and 1071:
Abnormal Endometrium ○ Multiple e
-
Page 1072 and 1073:
Abnormal Endometrium Pregnancy and
-
Page 1074 and 1075:
Abnormal Endometrium Tamoxifen-Indu
-
Page 1076 and 1077:
INDEX A Abdominal aorta, 34, 40, 42
-
Page 1078 and 1079:
INDEX - myelolipoma vs., 590 - stag
-
Page 1080 and 1081:
INDEX Biliary cyst. See Choledochal
-
Page 1082 and 1083:
INDEX Caroli disease, 204-207 - bil
-
Page 1084 and 1085:
INDEX - solid renal mass vs., 968 -
-
Page 1086 and 1087:
INDEX diagnostic checklist, 839 dif
-
Page 1088 and 1089:
INDEX Efferent ductules, 130 Ejacul
-
Page 1090 and 1091:
INDEX Focal myometrial contraction
-
Page 1092 and 1093:
INDEX - hydrocele vs., 715 - sperma
-
Page 1094 and 1095:
INDEX Hepatocellular carcinoma (HCC
-
Page 1096 and 1097:
INDEX Inflammatory pseudotumor, sol
-
Page 1098 and 1099:
INDEX - focal extratesticular mass
-
Page 1100 and 1101:
INDEX irregular hepatic surface vs.
-
Page 1102 and 1103:
INDEX Normal postpartum, enlarged u
-
Page 1104 and 1105:
INDEX Pararenal fat, posterior, 64
-
Page 1106 and 1107:
INDEX - inflammatory, gallbladder c
-
Page 1108 and 1109:
INDEX Pyelogenic cyst - dilated ren
-
Page 1110 and 1111:
INDEX Renal infection - renal lymph
-
Page 1112 and 1113:
INDEX - macrocystic variant, mucino
-
Page 1114 and 1115:
INDEX - right, 92 lesser sac, 93 Su
-
Page 1116 and 1117:
INDEX Tunica albuginea cyst - calci
-
Page 1118:
INDEX X Xanthogranulomatous cholecy