

Signup- Splash Canyon 2018.docx
Mandatory Return
Mandatory Return

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
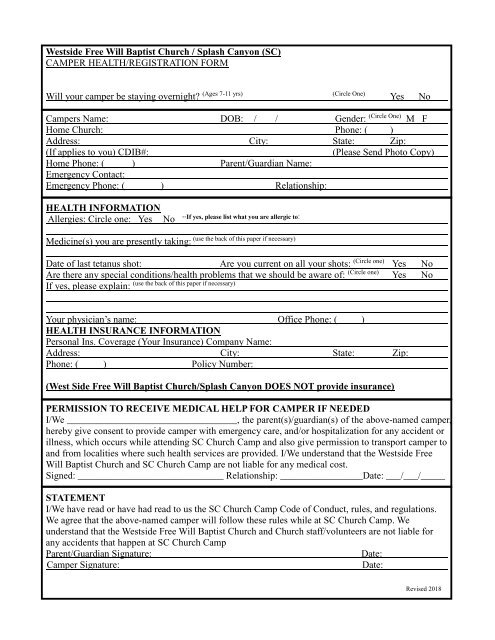
Westside Free Will Baptist Church / <strong>Splash</strong> <strong>Canyon</strong> (SC)<br />
CAMPER HEALTH/REGISTRATION FORM<br />
Preregistration cutoff date is Sunday, April 30 th . Registering before this date qualifies your spy in<br />
training for a free International Spy Academy T-SHIRT!<br />
Will your camper be staying overnight? (Ages 7-11 yrs) (Circle One) Yes No<br />
Campers Name: DOB: / / Gender: (Circle One) M F<br />
Home Church: Phone: ( )<br />
Address: City: State: Zip:<br />
(If applies to you) CDIB#:<br />
(Please Send Photo Copy)<br />
Home Phone: ( ) Parent/Guardian Name:<br />
Emergency Contact:<br />
Emergency Phone: ( ) Relationship:<br />
HEALTH INFORMATION<br />
Allergies: Circle one: Yes<br />
No<br />
--If yes, please list what you are allergic to:<br />
(use the back of this paper if necessary)<br />
Medicine(s) you are presently taking:<br />
Date of last tetanus shot: Are you current on all your shots: (Circle one) Yes No<br />
Are there any special conditions/health problems that we should be aware of: (Circle one) Yes No<br />
(use the back of this paper if necessary)<br />
If yes, please explain:<br />
Your physician’s name: Office Phone: ( )<br />
HEALTH INSURANCE INFORMATION<br />
Personal Ins. Coverage (Your Insurance) Company Name:<br />
Address: City: State: Zip:<br />
Phone: ( ) Policy Number:<br />
(West Side Free Will Baptist Church/<strong>Splash</strong> <strong>Canyon</strong> DOES NOT provide insurance)<br />
PERMISSION TO RECEIVE MEDICAL HELP FOR CAMPER IF NEEDED<br />
I/We ___________________________________, the parent(s)/guardian(s) of the above-named camper,<br />
hereby give consent to provide camper with emergency care, and/or hospitalization for any accident or<br />
illness, which occurs while attending SC Church Camp and also give permission to transport camper to<br />
and from localities where such health services are provided. I/We understand that the Westside Free<br />
Will Baptist Church and SC Church Camp are not liable for any medical cost.<br />
Signed: ______________________________ Relationship: _________________Date: ___/___/_____<br />
STATEMENT<br />
I/We have read or have had read to us the SC Church Camp Code of Conduct, rules, and regulations.<br />
We agree that the above-named camper will follow these rules while at SC Church Camp. We<br />
understand that the Westside Free Will Baptist Church and Church staff/volunteers are not liable for<br />
any accidents that happen at SC Church Camp<br />
Parent/Guardian Signature:<br />
Date:<br />
Camper Signature:<br />
Date:<br />
Revised 2018
ADDITIONAL MEDICAL INFO/INSTRUCTIONS.<br />
FOR:



