

Advanced Trauma Life Support ATLS Student Course Manual 2018

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
COLD INJURY: LOCAL TISSUE EFFECTS 181<br />
5. Chemical burns<br />
6. Inhalation injury<br />
7. Burn injury in patients with preexisting medical<br />
disorders that could complicate management,<br />
prolong recovery, or affect mortality (e.g.,<br />
diabetes, renal failure)<br />
8. Any patient with burns and concomitant trauma<br />
(e.g., fractures) in which the burn injury poses<br />
the greatest risk of morbidity or mortality.<br />
In such cases, if the trauma poses the greater<br />
immediate risk, the patient may be initially<br />
stabilized in a trauma center before being<br />
transferred to a burn unit. Physician judgment<br />
is necessary in such situations and should be<br />
considered in concert with the regional medical<br />
control plan and triage protocols.<br />
9. Burned children in hospitals without qualified<br />
personnel or equipment for the care of children<br />
10. Burn injury in patients who will require special<br />
social, emotional, or rehabilitative intervention<br />
Because these criteria are so comprehensive, clinicians<br />
may elect to consult with a burn center<br />
and determine a mutually agreeable plan other<br />
than transfer. For example, in the case of a partialthickness<br />
hand or face burn, if adequate wound care<br />
can be taught and oral pain control tolerated, followup<br />
at an outpatient burn clinic can avoid the costs of<br />
immediate transfer to a burn center.<br />
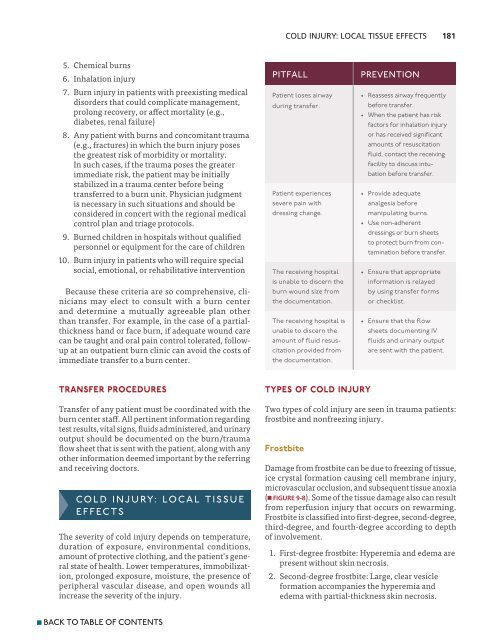
Pitfall<br />
Patient loses airway<br />
during transfer.<br />
Patient experiences<br />
severe pain with<br />
dressing change.<br />
The receiving hospital<br />
is unable to discern the<br />
burn wound size from<br />
the documentation.<br />
The receiving hospital is<br />
unable to discern the<br />
amount of fluid resuscitation<br />
provided from<br />
the documentation.<br />
prevention<br />
• Reassess airway frequently<br />
before transfer.<br />
• When the patient has risk<br />
factors for inhalation injury<br />
or has received significant<br />
amounts of resuscitation<br />
fluid, contact the receiving<br />
facility to discuss intubation<br />
before transfer.<br />
• Provide adequate<br />
analgesia before<br />
manipulating burns.<br />
• Use non-adherent<br />
dressings or burn sheets<br />
to protect burn from contamination<br />
before transfer.<br />
• Ensure that appropriate<br />
information is relayed<br />
by using transfer forms<br />
or checklist.<br />
• Ensure that the flow<br />
sheets documenting IV<br />
fluids and urinary output<br />
are sent with the patient.<br />
Transfer Procedures<br />
Transfer of any patient must be coordinated with the<br />
burn center staff. All pertinent information regarding<br />
test results, vital signs, fluids administered, and urinary<br />
output should be documented on the burn/trauma<br />
flow sheet that is sent with the patient, along with any<br />
other information deemed important by the referring<br />
and receiving doctors.<br />
Cold Injury: Local Tissue<br />
Effects<br />
The severity of cold injury depends on temperature,<br />
duration of exposure, environmental conditions,<br />
amount of protective clothing, and the patient’s general<br />
state of health. Lower temperatures, immobilization,<br />
prolonged exposure, moisture, the presence of<br />
peripheral vascular disease, and open wounds all<br />
increase the severity of the injury.<br />
Types of Cold Injury<br />
Two types of cold injury are seen in trauma patients:<br />
frostbite and nonfreezing injury.<br />
Frostbite<br />
Damage from frostbite can be due to freezing of tissue,<br />
ice crystal formation causing cell membrane injury,<br />
microvascular occlusion, and subsequent tissue anoxia<br />
(n FIGURE 9-8). Some of the tissue damage also can result<br />
from reperfusion injury that occurs on rewarming.<br />
Frostbite is classified into first-degree, second-degree,<br />
third-degree, and fourth-degree according to depth<br />
of involvement.<br />
1. First-degree frostbite: Hyperemia and edema are<br />
present without skin necrosis.<br />
2. Second-degree frostbite: Large, clear vesicle<br />
formation accompanies the hyperemia and<br />
edema with partial-thickness skin necrosis.<br />
n BACK TO TABLE OF CONTENTS













