

MALARIA ELIMINATION IN ZANZIBAR - Soper Strategies
MALARIA ELIMINATION IN ZANZIBAR - Soper Strategies
MALARIA ELIMINATION IN ZANZIBAR - Soper Strategies

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
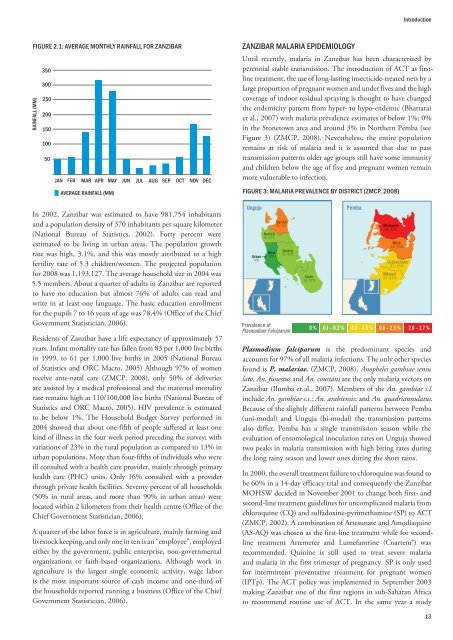
FIGURE 2.1: AVERAGE MONTHLY RA<strong>IN</strong>FALL FOR <strong>ZANZIBAR</strong><br />
RA<strong>IN</strong>FALL (MM)<br />
350<br />
300<br />
250<br />
200<br />
150<br />
100<br />
50<br />
JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC<br />
AVERAGE RA<strong>IN</strong>FALL (MM)<br />
In 2002, Zanzibar was estimated to have 981,754 inhabitants<br />
and a population density of 370 inhabitants per square kilometer<br />
(National Bureau of Statistics, 2002). Forty percent were<br />
estimated to be living in urban areas. The population growth<br />
rate was high, 3.1%, and this was mostly attributed to a high<br />
fertility rate of 5.3 children/women. The projected population<br />
for 2008 was 1,193,127. The average household size in 2004 was<br />
5.5 members. About a quarter of adults in Zanzibar are reported<br />
to have no education but almost 76% of adults can read and<br />
write in at least one language. The basic education enrollment<br />
for the pupils 7 to 16 years of age was 78.4% (Office of the Chief<br />
Government Statistician, 2006).<br />
Residents of Zanzibar have a life expectancy of approximately 57<br />
years. Infant mortality rate has fallen from 83 per 1,000 live births<br />
in 1999, to 61 per 1,000 live births in 2005 (National Bureau<br />
of Statistics and ORC Macro, 2005) Although 97% of women<br />
receive ante-natal care (ZMCP, 2008), only 50% of deliveries<br />
are assisted by a medical professional and the maternal mortality<br />
rate remains high at 110/100,000 live births (National Bureau of<br />
Statistics and ORC Macro, 2005). HIV prevalence is estimated<br />
to be below 1%. The Household Budget Survey performed in<br />
2004 showed that about one-fifth of people suffered at least one<br />
kind of illness in the four week period preceding the survey; with<br />
variations of 23% in the rural population as compared to 13% in<br />
urban populations. More than four-fifths of individuals who were<br />
ill consulted with a health care provider, mainly through primary<br />
health care (PHC) units. Only 16% consulted with a provider<br />
through private health facilities. Seventy percent of all households<br />
(50% in rural areas, and more than 90% in urban areas) were<br />
located within 2 kilometers from their health centre (Office of the<br />
Chief Government Statistician, 2006).<br />
A quarter of the labor force is in agriculture, mainly farming and<br />
livestock keeping, and only one in ten is an “employee”, employed<br />
either by the government, public enterprise, non-governmental<br />
organizations or faith-based organizations. Although work in<br />
agriculture is the largest single economic activity, wage labor<br />
is the most important source of cash income and one-third of<br />
the households reported running a business (Office of the Chief<br />
Government Statistician, 2006).<br />
<strong>ZANZIBAR</strong> <strong>MALARIA</strong> EPIDEMIOLOGY<br />
Until recently, malaria in Zanzibar has been characterized by<br />
perennial stable transmission. The introduction of ACT as first-<br />
line treatment, the use of long-lasting insecticide-treated nets by a<br />
large proportion of pregnant women and under fives and the high<br />
coverage of indoor residual spraying is thought to have changed<br />
the endemicity pattern from hyper- to hypo-endemic (Bhattarai<br />
et al., 2007) with malaria prevalence estimates of below 1%; 0%<br />
in the Stonetown area and around 3% in Northern Pemba (see<br />
Figure 3) (ZMCP, 2008). Nevertheless, the entire population<br />
remains at risk of malaria and it is assumed that due to past<br />
transmission patterns older age groups still have some immunity<br />
and children below the age of five and pregnant women remain<br />
more vulnerable to infection.<br />
FIGURE 3: <strong>MALARIA</strong> PREVALENCE BY DISTRICT (ZMCP, 2008)<br />
Unguja<br />
Urban<br />
0%<br />
North B<br />
0.1 - 0.2%<br />
West<br />
0%<br />
North A<br />
0.6 - 2.5%<br />
Central<br />
0.1 - 0.2%<br />
Prevalence of<br />
Plasmodium Falciparum<br />
South<br />
0.1 - 0.2%<br />
0%<br />
Pemba<br />
Michewni<br />
2.6 - 3.7%<br />
Wete<br />
0.6 - 2.5%<br />
Chakechake<br />
0.3 - 0.5%<br />
Mikoani<br />
0.3 - 0.5%<br />
Introduction<br />
0.1 - 0.2% 0.3 - 0.5% 0.6 - 2.5% 2.6 - 3.7%<br />
Plasmodium falciparum is the predominant species and<br />
accounts for 97% of all malaria infections. The only other species<br />
found is P. malariae. (ZMCP, 2008). Anopheles gambiae sensu<br />
lato, An. funestus and An. coustani are the only malaria vectors on<br />
Zanzibar (Ilumba et al., 2007). Members of the An. gambiae s.l.<br />
include An. gambiae s.s.; An. arabiensis; and An. quadriannulatus.<br />
Because of the slightly different rainfall patterns between Pemba<br />
(uni-modal) and Unguja (bi-modal) the transmission patterns<br />
also differ. Pemba has a single transmission season while the<br />
evaluation of entomological inoculation rates on Unguja showed<br />
two peaks in malaria transmission with high biting rates during<br />
the long rainy season and lower ones during the short rains.<br />
In 2000, the overall treatment failure to chloroquine was found to<br />
be 60% in a 14-day efficacy trial and consequently the Zanzibar<br />
MOHSW decided in November 2001 to change both first- and<br />
second-line treatment guidelines for uncomplicated malaria from<br />
chloroquine (CQ) and sulfadoxine-pyrimethamine (SP) to ACT<br />
(ZMCP, 2002). A combination of Artesunate and Amodiaquine<br />
(AS-AQ) was chosen as the first-line treatment while for secondline<br />
treatment Artemeter and Lumefantrine (Coartem®) was<br />
recommended. Quinine is still used to treat severe malaria<br />
and malaria in the first trimester of pregnancy. SP is only used<br />
for intermittent preventative treatment for pregnant women<br />
(IPTp). The ACT policy was implemented in September 2003<br />
making Zanzibar one of the first regions in sub-Saharan Africa<br />
to recommend routine use of ACT. In the same year a study<br />
13