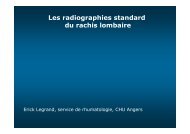
Quel est la fréquence d’un AIT ?
Les Accidents Ischémiques Transitoires.pdf
Les Accidents Ischémiques Transitoires.pdf
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Quel</strong> <strong>est</strong> <strong>la</strong> <strong>fréquence</strong> <strong>d’un</strong> <strong>AIT</strong> ?1 million de sujets500 <strong>AIT</strong>2400 AVCDont 600 récidives/an480 DCD à 1 mois700 décédésà 1 an600 dépendantsà 1 anHankey et al Lancet 1999
Différentes causes d’ischémie
<strong>Quel</strong>le définition ?• Déficit neurologique focal ou rétinien de survenuebrutale, d’origine ischémique, de topographievascu<strong>la</strong>ire régressant en moins de 24h ?• Déficit bref de dysfonction neurologique dû à uneischémie focale cérébrale ou rétinienne (dont lessymptômes durent typiquement moins <strong>d’un</strong>eheure), sans preuve d’infarctus aigu ? (HAS 2004, ASA 2009)
Le diagnostic de l’<strong>AIT</strong>• Parfois difficile : pas de marqueur• Mauvaise reproductibilité inter-observateurs• Interrogatoire du patient et de l’entourage +++• Chronologie• Circonstances de survenue• <strong>AIT</strong> probable, <strong>AIT</strong> possible
Le diagnostic de l’<strong>AIT</strong>• 4 éléments importants :– Déficitaire– Brutal (< 2min)– D’emblée maximal– Focal
Le diagnostic de l’<strong>AIT</strong>• <strong>AIT</strong> probable :Territoire carotidien Territoire Vertebro-basi<strong>la</strong>ire :CarotidienVertebro-basi<strong>la</strong>ire- Cécité monocu<strong>la</strong>ire transitoire (CMT)- Troubles du <strong>la</strong>ngage(aphasie)- Déficit moteur et/ou sensitifuni<strong>la</strong>téraux touchant <strong>la</strong> faceet/ou les membres *- Troubles moteurs et/ou sensitifsbi<strong>la</strong>téraux ou à bascule touchant <strong>la</strong> faceet/ou les membres- hémianopsie <strong>la</strong>térale homonyme** oucécité corticale* Ces symptômes, en l’absence d’autres signes, ne permettent pas de trancher entre unterritoire carotidien ou vertebrobasi<strong>la</strong>ire** L’HLH peut également s’observer dans le territoire carotidien
Le diagnostic de l’<strong>AIT</strong>• <strong>AIT</strong> Possible (compatibles avec un <strong>AIT</strong> mais ne doivent pasfaire évoquer le diagnostic en première intension si isolés) :– Vertige– Diplopie– Dysarthrie– Troubles de <strong>la</strong> déglutition– Perte de l’équilibre– Troubles sensitifs isolés ne touchant qu’une partie<strong>d’un</strong> membre ou <strong>d’un</strong>e hémiface– Drop-attack
Le diagnostic de l’<strong>AIT</strong>• Les symptômes suivants ne doivent pas faire évoquerune <strong>AIT</strong> :– Altération de <strong>la</strong> conscience isolée– Confusion mentale isolée– Étourdissement isolé– Amnésie isolée– Faiblesse généralisée– Lypothimie– Scotome scintil<strong>la</strong>nt– Acouphènes isolés– Trouble aigu du comportement– Progression des symptômes
Le diagnostic de l’<strong>AIT</strong>Autre difficulté : nombreuxdiagnostics différentiels– Aura migraineux– Epilepsie partielle– Hématome intra cérébral– Hématome sous-dural– Malformation vascu<strong>la</strong>ire cérébrale– Ictus amésique– Sclérose en p<strong>la</strong>ques– Myasthénie– Tumeur cérébrale– Hypoglycémie– Vertige ORL– Hystérie– ……Devant une CMT• HTA maligne• G<strong>la</strong>ucome aigu• HTIC• Thrombose de <strong>la</strong> veinecentrale de <strong>la</strong> rétine• NORB• Décollement de <strong>la</strong> rétine
<strong>Quel</strong> <strong>est</strong> le risque après un <strong>AIT</strong> ?• Jusqu’à 20 % des infarctus cérébraux sontprécédés <strong>d’un</strong> <strong>AIT</strong>Chandratheva et al Neurology 2009
Peut-on <strong>est</strong>imer le risque après un <strong>AIT</strong> ?• Le score ABCD 2 :– Age ≥ 60 ans 1– Pression artérielle :• Systolique > 140 et/ou diastolique > 90mmHg 1– Clinique :• Déficit moteur uni<strong>la</strong>téral 2• Trouble de <strong>la</strong> parole sans déficit moteur1– Durée :• ≥ 60 min 2• De 10 à 59 min 1• < 10 min 1– Diabète 1ATTENTION !!!Jonhston et al, Lancet 2007
Intérêt <strong>d’un</strong> traitement précoce après un <strong>AIT</strong>• 2 Etudes : EXPRESS et SOS-TIARisque de récidive d’AVCdiminué de 80%Rothwell et al Lancet 2007, Amarenco et al Lancet neuro 2007
Faut-il hospitaliser les patients ayant fait un <strong>AIT</strong> ?Circu<strong>la</strong>ire ministérielle 22 mars 2007• Recommandations ANAES 2004 :– L’hospitalisation en service spécialisé <strong>est</strong> recommandée :• si elle permet d’obtenir plus rapidement les examens complémentaires ;• en cas d’<strong>AIT</strong> récidivants et récents et d’<strong>AIT</strong> survenant sous traitementantiagrégant p<strong>la</strong>quettaire ;• si le terrain le justifie (comorbidité, âge, isolement social).• Recommandations Américaines (ASA 2009) :– It is reasonable to hospitalize patients with TIA if they present within 72hours of the event and any of the following criteria are present:• ABCD 2 score of 3 (C<strong>la</strong>ss IIa, Level of Evidence C).• ABCD 2 score of 0 to 2 and uncertainty that diagnostic workup can be completed within 2days as an outpatient (C<strong>la</strong>ss IIa, Level of Evidence C).• ABCD 2 score of 0 to 2 and other evidence that indicates the patient’s event was caused byfocal ischemia (C<strong>la</strong>ss IIa, Level of Evidence C).
<strong>Quel</strong>le conduite à tenir devant un <strong>AIT</strong>?• Bi<strong>la</strong>n rapide ++++ (< 24h) :– Imagerie cérébrale (IRM>TDM)– NFS, p<strong>la</strong>quettes, iono sang urée créat, TP, TCA, BH,CRP– Bi<strong>la</strong>n lipidique– ECG– Doppler TSA• Puis– ± Echographie cardiaque, PL, artério……..
<strong>Quel</strong>le conduite à tenir devant un <strong>AIT</strong>• Traitement en Urgence :– Aspirine 160 à 300 mg (après l’imagerie)• Traitement de prévention secondaire :– Fonction de <strong>la</strong> cause :• AVK : Cardioembolique, dissection, causes rares…• Antiagrégants : athérome, microangiopathie, sanscause (aspirine, clopidogrel, asasantine)• Anti-hypertenseurs : tout type d’AVC (preuve avecperindopril + indapamide LP)• Statine : causes non-cardioemeboliques avec pourobjectif LDL < 1g/l (preuve avec atorvastatine 80mg)?
Conclusion• L’<strong>AIT</strong> <strong>est</strong> une urgence thérapeutique• Diagnostic d’interrogatoire• Hospitalisation des <strong>AIT</strong> :– Récents– Récidivants– Sous aspirine– ABCD 2 ≥ 3– Sujet jeune• Ttt précoce par aspirine ++++ après imagerie en urgence
MERCI DE VOTRE ATTENTION