HIV/AIDS+WORK Swaziland
HIV/AIDS, work and development - (NERCHA), the Info Centre
HIV/AIDS, work and development - (NERCHA), the Info Centre
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
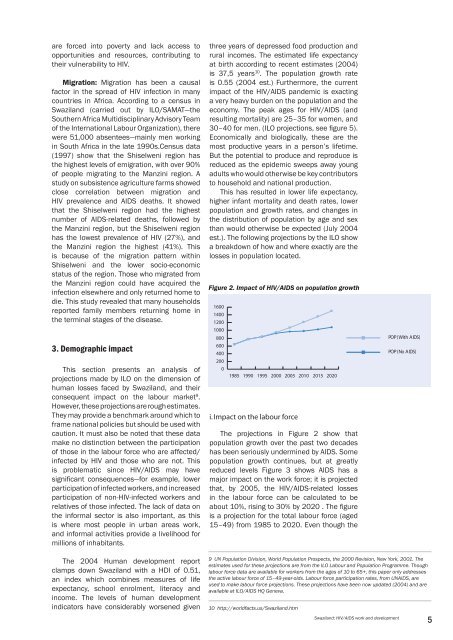
are forced into poverty and lack access toopportunities and resources, contributing totheir vulnerability to <strong>HIV</strong>.Migration: Migration has been a causalfactor in the spread of <strong>HIV</strong> infection in manycountries in Africa. According to a census in<strong>Swaziland</strong> (carried out by ILO/SAMAT—theSouthern Africa Multidisciplinary Advisory Teamof the International Labour Organization), therewere 51,000 absentees—mainly men workingin South Africa in the late 1990s.Census data(1997) show that the Shiselweni region hasthe highest levels of emigration, with over 90%of people migrating to the Manzini region. Astudy on subsistence agriculture farms showedclose correlation between migration and<strong>HIV</strong> prevalence and AIDS deaths. It showedthat the Shiselweni region had the highestnumber of AIDS-related deaths, followed bythe Manzini region, but the Shiselweni regionhas the lowest prevalence of <strong>HIV</strong> (27%), andthe Manzini region the highest (41%). Thisis because of the migration pattern withinShiselweni and the lower socio-economicstatus of the region. Those who migrated fromthe Manzini region could have acquired theinfection elsewhere and only returned home todie. This study revealed that many householdsreported family members returning home inthe terminal stages of the disease.3. Demographic impactThis section presents an analysis ofprojections made by ILO on the dimension ofhuman losses faced by <strong>Swaziland</strong>, and theirconsequent impact on the labour market 9 .However, these projections are rough estimates.They may provide a benchmark around which toframe national policies but should be used withcaution. It must also be noted that these datamake no distinction between the participationof those in the labour force who are affected/infected by <strong>HIV</strong> and those who are not. Thisis problematic since <strong>HIV</strong>/AIDS may havesignificant consequences—for example, lowerparticipation of infected workers, and increasedparticipation of non-<strong>HIV</strong>-infected workers andrelatives of those infected. The lack of data onthe informal sector is also important, as thisis where most people in urban areas work,and informal activities provide a livelihood formillions of inhabitants.three years of depressed food production andrural incomes. The estimated life expectancyat birth according to recent estimates (2004)is 37,5 years 10 . The population growth rateis 0.55 (2004 est.) Furthermore, the currentimpact of the <strong>HIV</strong>/AIDS pandemic is exactinga very heavy burden on the population and theeconomy. The peak ages for <strong>HIV</strong>/AIDS (andresulting mortality) are 25–35 for women, and30–40 for men. (ILO projections, see figure 5).Economically and biologically, these are themost productive years in a person’s lifetime.But the potential to produce and reproduce isreduced as the epidemic sweeps away youngadults who would otherwise be key contributorsto household and national production.This has resulted in lower life expectancy,higher infant mortality and death rates, lowerpopulation and growth rates, and changes inthe distribution of population by age and sexthan would otherwise be expected (July 2004est.). The following projections by the ILO showa breakdown of how and where exactly are thelosses in population located.Figure 2. Impact of <strong>HIV</strong>/AIDS on population growth160014001200100080060040020001985 1990 1995 2000 2005 2010 2015 2020i. Impact on the labour forceThe projections in Figure 2 show thatpopulation growth over the past two decadeshas been seriously undermined by AIDS. Somepopulation growth continues, but at greatlyreduced levels Figure 3 shows AIDS has amajor impact on the work force; it is projectedthat, by 2005, the <strong>HIV</strong>/AIDS-related lossesin the labour force can be calculated to beabout 10%, rising to 30% by 2020 . The figureis a projection for the total labour force (aged15–49) from 1985 to 2020. Even though thePOP(With AIDS)POP(No AIDS)The 2004 Human development reportclamps down <strong>Swaziland</strong> with a HDI of 0.51,an index which combines measures of lifeexpectancy, school enrolment, literacy andincome. The levels of human developmentindicators have considerably worsened given9 UN Population Division, World Population Prospects, the 2000 Revision, New York, 2001. Theestimates used for these projections are from the ILO Labour and Population Programme. Thoughlabour force data are available for workers from the ages of 10 to 65+, this paper only addressesthe active labour force of 15–49-year-olds. Labour force participation rates, from UNAIDS, areused to make labour force projections. These projections have been now updated (2004) and areavailable at ILO/AIDS HQ Geneva.10 http://worldfacts.us/<strong>Swaziland</strong>.htm<strong>Swaziland</strong>: <strong>HIV</strong>/AIDS work and development5