

CLINICAL EEG and NEUROSCIENCE - Dynamic Memory Lab
CLINICAL EEG and NEUROSCIENCE - Dynamic Memory Lab
CLINICAL EEG and NEUROSCIENCE - Dynamic Memory Lab

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong>Official Journal of the<strong>EEG</strong> <strong>and</strong> Clinical Neuroscience Society (ECNS)Founding EditorFREDERIC A. GIBBS, M.D.Chief EditorNORMAN C. MOORE, M.D.Johnson City, TennesseeAssociate Editorfor NeurologyFRANK H. DUFFY, M.D.Boston, MassachusettsAssociate Editor forPsychiatry <strong>and</strong> PsychologyE. ROY JOHN, Ph.D.New York, New YorkChairmanROBERT L. WEINMANN, M.D.San Jose, CaliforniaEDITORIAL BOARDTreasurerANDREW PIPINGAS, Ph.D.Melbourne, AustraliaHOJJAT ADELI, Ph.D.Columbus, OhioIVAN BODIS-WOLLNER, M.D.New York, New YorkNASH N. BOUTROS, M.D.Detroit, MichiganC. RICHARD CLARK, Ph.D.Adelaide, AustraliaMILES E. DRAKE, JR., M.D.Columbus, OhioSILVANA GALDERISINaples, ItalyJOHN R. HUGHES, M.D.Chicago, IllinoisYOSHIFUMI KOSHINO, M.D.Kanazawa, JapanMICHAEL P. KRIEGER, M.D.Victoria, CanadaALLAN KRUMHOLZ, M.D.Baltimore, Maryl<strong>and</strong>S. KUBICKI, M.D.Berlin, GermanyXIUQIN LIU, M.D.Beijing, ChinaJ. GORDON MILLICHAP, M.D.Chicago, IllinoisERNST NIEDERMEYER, M.D.Baltimore, Maryl<strong>and</strong>WILLIAM J. NOWACK, M.D.Kansas City, KansasANTONINO PAVONE, M.D.Catania, ItalyWALTER S. PRITCHARD, Ph.D.Winston-Salem, North CarolinaMAURICE RAPPAPORT, M.D.San Jose, CaliforniaJAMES J. RIVIELLO, M.D.Boston, MassachusettsR. BART SANGAL, M.D.Troy, MichiganJOYCE G. SMALL, M.D.Indianapolis, IndianaJAMES L. STONE, M.D.Chicago, IllinoisFREDERICK A. STRUVE, Ph.D.West Haven, ConnecticutROBERT THATCHER, Ph.D.St. Petersburg, Florida<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong>is published quarterly: January, April, July <strong>and</strong> October by the <strong>EEG</strong> <strong>and</strong> Clinical Neuroscience Society (ECNS)©<strong>EEG</strong> <strong>and</strong> Clinical Neuroscience Society (ECNS) 2007Production Staff: Catherine Demeter, Managing Editor; Kevin Kjellberg, Production ManagerI
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1BusinessBUSINESS OFFICES:<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> – For all matterspertaining to the Journal Clinical <strong>EEG</strong> <strong>and</strong> Neuroscience,contact:Clinical <strong>EEG</strong> <strong>and</strong> Neuroscience805 W. Liberty DriveWheaton, IL 60187 USAFax: 630-653-6233Email: clinicaleeg@aol.comw w w. e c n s w e b . c o mADMINISTRATIVE – For all matters pertaining to the<strong>EEG</strong> <strong>and</strong> Clinical Neuroscience Society (ECNS), contact:Dr. Nash BoutrosDept. of Psychiatry <strong>and</strong> Behavioral NeurosciencesWayne State UniversityUPC-Jefferson, Suite 3082751 E. JeffersonDetroit, MI 48207 USAPhone: 313-577-0164Fax: 313-577-5900Email: nboutros@med.wayne.eduwww.ecnsweb.com/index.htmBOARD EXAMINATIONwww.ecnsweb.com/ec_aben.htmAdvertising:Acceptance of advertisements in Clinical <strong>EEG</strong> <strong>and</strong>Neuroscience does not imply endorsement of the productsor services offered.Display advertising rates <strong>and</strong> special instructions areavailable from the Business Office.Submit written classified advertisements to the BusinessO ffice with payment in United States funds. Rate: $20.00 forthe first 30 words <strong>and</strong> $0.50 for each additional word.Subscriptions:All subscriptions to Clinical <strong>EEG</strong> <strong>and</strong> Neuroscience a r eon a calendar year basis <strong>and</strong> begin with the January issueof the current volume. Postpaid subscription rates for 2007,volume number 38 are $96 per year U.S.; $116 (U.S. funds)per year elsewhere.Back issues are available post paid for $32 in theU.S., $40 (U.S. funds) elsewhere.Both subscriptions <strong>and</strong> back issues may be orderedthrough the Clinical <strong>EEG</strong> <strong>and</strong> Neuroscience business officeat the address shown above.Address Correction:Please copy your address label exactly including themailing code number. Send the copy <strong>and</strong> your newaddress to the Clinical <strong>EEG</strong> <strong>and</strong> Neuroscience officeaddress shown above.∞This journal has been printed on acid-free paper – effectivewith Volume 16, Number 1.INSTRUCTIONS FOR AUTHORSPurpose:The goal of Clinical <strong>EEG</strong> <strong>and</strong> Neuroscience is to conveyclinically relevant research <strong>and</strong> development in electroencephalography<strong>and</strong> neuroscience. Original articles onany aspect of clinical <strong>EEG</strong> or related work in allied fieldsare invited for publication. Views expressed in articles, editorials,<strong>and</strong> letters represent the opinions of the author(s)<strong>and</strong> do not necessarily reflect the official policy of the institutionwith which the author is affiliated, or the <strong>EEG</strong> <strong>and</strong>Clinical Neuroscience Society (ECNS).Guidelines:Submit articles for publication by email to the BusinessOffice: clinicaleeg@aol.com <strong>and</strong> on computer disk in anyst<strong>and</strong>ard word processing program. Send three hardcopies of the article <strong>and</strong> any other materials to CatherineD e m e t e r, Managing Editor, Clinical <strong>EEG</strong> <strong>and</strong> Neuro -science, 2568 E. Denton Lane, Phoenix, AZ 85016, USA.Manuscripts should be in the form of original articles,editorials, reviews <strong>and</strong> case reports. It is understood thatthese papers will not be concurrently submitted to anyother journal. Authors may propose reviewers for their articles.Authors are to provide a written point by pointresponse to each reviewer with their revisions.Accepted manuscripts become the property of Clinical<strong>EEG</strong> <strong>and</strong> Neuroscience <strong>and</strong> may not be published elsewherewithout written consent of the editor. Authors ofaccepted manuscripts must assign the copyright to Clinical<strong>EEG</strong> <strong>and</strong> Neuroscience.Manuscript Format: (see current issue)Manuscripts should be typewritten, double spaced, oneside, on 8 1 / 2" x 11", leaving ample margins, <strong>and</strong> includeKey Words, Abstract <strong>and</strong> References in numerical order ofappearance in text, following current issue format. Numbereach page <strong>and</strong> identify with title <strong>and</strong> author’s name. Thetitle page should include full title of the article; initials <strong>and</strong>last names of all authors; current positions of each author(title, department, institution, location); phone <strong>and</strong> fax numbers,email <strong>and</strong> mailing address of author to whom reprintrequests are to be sent; acknowledgment if the study wasfunded <strong>and</strong> if it was previously presented at a meeting.For figures, glossy prints are acceptable. Authors willbear the cost of color reproductions. Digital color illustrationsshould be 3x5 or 5x7 <strong>and</strong> at 300dpi, .jpg or .tif.Page Proofs <strong>and</strong> Reprint Orders:Page Proofs <strong>and</strong> reprint orders must be returned within10 days with payment or credit card information to: CatherineD e m e t e r, Managing Editor, Clinical <strong>EEG</strong> <strong>and</strong> Neuroscience,2568 E. Denton Lane, Phoenix, AZ, 85016, USA, or sent byfax directly to Kevin Kjellberg, Production Manager, at Fax:630-653-6233, or email clinicaleeg@aol.com, with promptpayment by check or any major credit card.II
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Special Issues:Previous Special Issues of Clinical <strong>EEG</strong>January 2000A Review of <strong>EEG</strong> BiofeedbackGuest Editor, Norman C. MooreJuly 2001The Re-emergence of Systems NeuroscienceGuest Editor, Ivan Bodis-WollnerBack Issues of theseSpecial Issuesare available atclinicaleeg@aol.comfor $32.00 (US funds)in the US <strong>and</strong>$40.00 (US funds)elsewhere, postpaidJuly 2002P300 <strong>and</strong> Clinical PatientsGuest Editor, John PolichJanuary 2004Current <strong>and</strong> Future Therapeutic Opportunities in theComorbidity Between the Epilepsies <strong>and</strong> Affective DisordersGuest Editor, Phillip C. JobeApril 2005<strong>EEG</strong> Databases in Research <strong>and</strong> ClinicalPractice: Current Status <strong>and</strong> Future DirectionsGuest Editors, Evian Gordon <strong>and</strong> Lukasz M. KonopkaOctober 2005Ultrafast Frequencies <strong>and</strong> Full-B<strong>and</strong> <strong>EEG</strong>Guest Editor, E. NiedermeyerApril 2006Pharmaco-<strong>EEG</strong> at a CrossroadsGuest Editor, S. GalderisiOctober 2006The Electrophysiology of <strong>Memory</strong>: Section I: Basic StudiesGuest Editors, Thomas Grunwald <strong>and</strong> Charan RanganathIII
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1AnnouncementsBOOK REVIEWSClinical <strong>EEG</strong> <strong>and</strong> Neuroscience will publish reviews for any topic thatrelates to clinical electrophysiology of neurological or psychiatric disorders.Basic science books pertaining to cerebral electrophysiology can also be reviewed.Authors interested in having their books reviewed can mail a copy of the book to:Dr. Nash N. BoutrosWayne State UniversityUniversity Psychiatric Clinic2571 E. Jefferson Street, Suite 401Detroit, Michigan 48207We wish to thank the following Reviewers for 2007M. E. Drake, Jr., MDH. W. Goforth, MDT. Harmony, PhDR. Herning, PhDE. R. John, PhDL. M. Konopka, PhDA. Krumholz, MDE. Niedermeyer, MDW. J. Nowack, MDL. M. O’Brien, PhDW. S. Pritchard, PhDE. Rodin, MDR. B. Sangal. MDJ. G. Small, MDH. Stefan, MDS. R. Steinhauer, PhDR. Thatcher, PhDR. Wennberg, MDIV
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Special IssueThe Electrophysiology of <strong>Memory</strong>: Section IIClinical StudiesExploring Human <strong>Memory</strong> ProcessesWith Event-Related PotentialsThomas Grunwald <strong>and</strong> Charan Ranganath, Guest EditorsWelcome to the second in our two-part special issue onthe electrophysiology of memory. In the first installment, weincluded papers reviewing recent findings from studiesaddressing basic questions about human memoryprocesses. In this issue, we will consider electrophysiologicalstudies of memory processes in special populations.As Gabriel García Márquez stated in his epigraph toLiving to Tell the Tale, “life is not what one lived, but whatone remembers (…)”. Indeed, memory functions are criticalfor almost every facet of daily life. Unfortunately memoriesare fragile, <strong>and</strong> memory functioning is highly susceptibleto deterioration through disease or injury. Such memorydeficits can have tragic effects on one’s quality of life.Fortunately, results from event-related potential (ERP)studies have revealed significant insights into the nature ofmemory disorders. ERPs can help to identify time-criticalneuronal processes <strong>and</strong> to relate them to specific cognitiveprocesses. Likewise, ERPs can help delineate functionaldeficits induced by diffuse or localized brain lesions.Because ERP recordings are normally non-invasive <strong>and</strong>comparatively inexpensive, they may eventually wellbecome part of clinical routine investigations. For thesereasons, ERPs are an ideal method for investigating theneural basis of memory <strong>and</strong> its disorders.Here, we will present a series of review papers showingthat ERP studies have revealed significant insights intothe nature of memory disorders. For example, even normalaging is associated with substantial changes in memoryfunctions. Friedman et al. show how ERP studies can helpto underst<strong>and</strong> age-related memory decline. Of course,Alzheimer’s disease is a significant cause of pathologicalmemory disorders among the elderly. In their contribution,Taylor & Olichney ask whether ERP studies can contributeto early detection <strong>and</strong> diagnosis of Alzheimer’s disease.Most clinical assessments of memory focus on verbalmemory functioning. However, Vannucci reviews studiesinto the nature of visual memory deficits, focusing onpatients with temporal lobe epilepsy. In addition to neurologicaldisorders, it is clear that psychiatric conditions canalso have debilitating effects on memory. Pogarell et al.consider the potential of ERP studies for practical psychiatry<strong>and</strong> suggest that ERPs may prove valuable to monitor<strong>and</strong> possibly predict the patient’s response to psychopharmacologicaltreatment.We hope that this two-part Special Issue of Clinical<strong>EEG</strong> <strong>and</strong> Neuroscience will inspire readers to learn moreabout ERP research on memory, <strong>and</strong> we thank all of thecontributing authors for sharing their knowledge with us.Likewise, we thank the editors of this journal for giving usthe opportunity to share our enthusiasm for this field ofbasic <strong>and</strong> clinical research with you.Thomas Grunwald, MD, PhD,Swiss Epilepsy Center, Zurich, Switzerl<strong>and</strong>Charan Ranganath, PhD,Center for Neuroscience <strong>and</strong> Dept. of PsychologyUniversity of California at Davis, Davis, California, USA1
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1<strong>Memory</strong> Encoding <strong>and</strong> Retrieval in the Aging BrainDavid Friedman, Doreen Nessler <strong>and</strong> Ray Johnson, Jr.Key WordsCognitive Aging of <strong>Memory</strong>Encoding <strong>and</strong> RetrievalEpisodic <strong>Memory</strong> (EM) EffectEvent-Related PotentialsLeft Inferior Prefrontal NegativitySemantic SelectionABSTRACTDecline in episodic memory, the encoding <strong>and</strong> retrievalof autobiographical events, is a hallmark of normal cognitiveaging. Although the primary causes of this decline remainelusive, event-related brain potential (ERP) studies havecontributed to an underst<strong>and</strong>ing of age-related episodicmemory failure. These data reveal that, although theretrieval-based episodic memory (EM) effect does not diff e rdramatically between young <strong>and</strong> older adults, the acquisition-relateddata suggest a decline in episodic encoding (i.e.,semantic elaboration) with increasing age. We concludethat, at the current state of knowledge, encoding deficienciesare more important than retrieval deficits in underst<strong>and</strong>ingthe causes of episodic memory decline in the older adult.INTRODUCTIONThe study of how humans encode, store <strong>and</strong> retrievemnemonic information has had a long scientific history,beginning formally with the classical studies of Ebbinghausin the late 19th century. 1 The relatively recent developmentof techniques allowing the investigation of how theseprocesses are instantiated in the brain has provided anunprecedented in vivo window on mnemonic function in theactively performing human. Although much has beenlearned about how (<strong>and</strong> by which brain networks) memoriesare encoded <strong>and</strong> retrieved in the normal young adult,relatively less is known about how aging affects the functioningof these different processes. Normal aging isaccompanied by well-documented failures in episodicm e m o r y, although their root causes are unclear. 2Underst<strong>and</strong>ing the sources of encoding <strong>and</strong>/or retrieval difficultiesis, therefore, critical to a more comprehensiveknowledge of episodic memory function in old age <strong>and</strong>,eventually, for designing remedial programs aimed at amelioratingmnemonic deficiencies in the elderly.Two brain imaging technologies have been used to chartchanges in episodic memory in normally aging older adults,event-related brain potentials (ERPs) <strong>and</strong> event-relatedfunctional magnetic resonance imaging (efMRI). A l t h o u g hthe efMRI technique is highly accurate in localizing areas ofactivation within the brain, the sluggishness of the hemodynamicresponse makes it impossible to determine preciselythe temporal sequence <strong>and</strong> duration of brain region activations.By contrast, the ERP method enables the collection ofvery precise temporal information, at the cost of less accuratespatial resolution than efMRI. The ERP t e c h n i q u e ,therefore, enables the viewing of brain activity related to theformation <strong>and</strong> retrieval of memories in temporal units thatare consistent with the speed of cognitive processes, i.e.,milliseconds. Hence, ERP studies of cognitive aging canprovide detailed information on age-related differences inthe timing <strong>and</strong> duration of specific mnemonic processes thatcontribute to encoding <strong>and</strong> retrieval.Episodic memory is comprised of personal memoriesthat include specific spatio-temporal information about thecontext in which the event occurred. 3 Episodic memory isinvestigated most often using paradigms that assessrecognition memory. In these paradigms, participants aretested by asking them to judge whether each item wasencountered previously during an encoding (i.e., study)phase or is new. Recognition memory is generally thoughtto rely on two processes, one relatively automatic <strong>and</strong> fastacting,labeled familiarity, <strong>and</strong> the other, more effortful,slower <strong>and</strong> requiring conscious deliberation, labeled recollection.4 For example, one can recognize with certainty aperson’s face as having been seen before, but not be ableto recall the contextual details that accompanied the initialepisode (i.e., where <strong>and</strong> when the person was initiallyencountered). This is an instance of a recognition judgmentbased on familiarity in the absence of recollection.Given that the contextual details were encoded during theoriginal event <strong>and</strong> an efficient retrieval strategy, the missingfeatures can often be recalled <strong>and</strong> reintegrated with theinformation provided by the face (i.e., recollected), resultingin a reconstructed episodic memory.Because the retrieval of episodes depends upon howthe information was initially encoded, we first review stud-David Friedman, Professor <strong>and</strong> Research Scientist VII, Doreen Nessler,Associate Research Scientist <strong>and</strong> Research Scientist II, CognitiveElectrophysiology <strong>Lab</strong>oratory, New York State Psychiatric Institute, NewYork, New York, <strong>and</strong> Ray Johnson, Jr., Professor, Department ofPsychology, Queens College, CUNY, Flushing, New York, New York.Address requests for reprints to D. Friedman, PhD, CognitiveElectrophysiology <strong>Lab</strong>oratory, NY Psychiatric Institute, Unit 6, 1051Riverside Drive, New York, N.Y. 10032, USA.Email: df12@columbia.edu2
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1ies of ERP activity recorded during encoding phases forsubsequent recognition testing. We then review the resultsof ERP investigations of retrieval.Encoding-related studiesRelative to non-semantic, or shallow encoding (forexample, processing orthographic features of words),semantic or deep encoding (as when making living/non-livingjudgments about words) leads to a greater likelihoodthat those words will be recognized on a subsequent memorytest. 5 By now, a large number of studies have shownthat the degree to which an item’s memory trace isenriched during encoding is determined by the amount oneelaborates upon the information retrieved from semanticmemory, 6 a phenomenon that can be labeled episodicencoding. Hence, semantic retrieval <strong>and</strong> episodic encodingappear to work in t<strong>and</strong>em, perhaps with semantic retrievaloccurring prior to episodic encoding.ERP investigators have assessed encoding-relatedprocessing by quantifying the differences in neural activityassociated with individual items during an encoding phasebased on whether or not those items are subsequentlyremembered. A subtraction of the ERPs elicited by studyitems that are subsequently forgotten from those that aresubsequently remembered yields the subsequent memoryeffect (SME), a measure of encoding. 7,8 SMEs usually, butnot always, have a positive polarity that is widely distributedacross the scalp. In their investigation, Paller <strong>and</strong> colleagues9 had subjects encode words under deep (e.g., is itliving?) <strong>and</strong> shallow (e.g., does the word contain 2 vowels?)conditions. In accord with Craik <strong>and</strong> Lockhart, 5semantic encoding engendered higher rates of recognitionsuccess compared to non-semantic encoding. Importantly,SMEs, which onset at roughly 400 ms <strong>and</strong> lasted about600 ms, were reliable under semantic but not non-semanticconditions. Hence, SMEs have been associated withsemantic encoding activity because their magnitude is positivelyrelated to the extent of deep encoding processesduring acquisition. 9 The question arises, however, as towhether SMEs are related to subsequent recollectioncomparedto familiarity-based retrievals.One method by which the distinction between recollection<strong>and</strong> familiarity has been demonstrated is with the“Remember/Know” paradigm. 10 In this paradigm, for itemsjudged old, subjects indicate whether their recognition decisionwas accompanied by the retrieval of contextual detail, a“remember” (R) judgment (i.e., a recollection-based retrieval),or was based on a feeling of familiarity with the item, a“know” (K) judgment (i.e., a familiarity-based retrieval).M o r e o v e r, items that are deeply encoded are associatedsubsequently with a greater proportion of R judgments,whereas items that are shallowly encoded are associatedsubsequently with a greater proportion of K responses.The R/K paradigm was used by Friedman <strong>and</strong> Trott 11 toassess whether recollection- <strong>and</strong> familiarity-basedretrievals had their origin during encoding. During the studyphase, participants were asked to memorize two nounsembedded in sentences for a subsequent recognition test.During the recognition test, subjects decided whethernouns were new or old <strong>and</strong>, for old nouns, made an additionalR/K judgment. The study phase ERPs were averagedinto three classes on the basis of subsequent recognitionperformance: 1) subsequently correctly recognized<strong>and</strong> given an R judgment, 2) subsequently correctly recognized<strong>and</strong> given a K judgment, <strong>and</strong> 3) subsequently unrecognized(i.e., a miss). SMEs were computed by subtractingthe ERPs associated with subsequently missed items fromthose associated with subsequent R <strong>and</strong> K judgments. Foryoung adults, reliable SMEs were observed in the intervalfrom 400 - 900 ms for study items associated with subsequentR judgments but not subsequent K judgments.These SME data suggest that recollection- <strong>and</strong> familiaritybasedrecognition judgments at retrieval had their origin inthe type of encoding activity engaged in during study.In addition to young adult participants, Friedman <strong>and</strong>Tr o t t 11 recruited older adults. There was some basis forexpecting age-related differences in ERP activity becausethe elderly had been shown to produce a smaller percentageof remember judgments than the young, 12 <strong>and</strong> to rely moreon familiarity than recollection when these two processesare placed in opposition. 13 , 14 Both findings suggest an agerelatedimbalance in the recollective component of recognitionmemory. Hence, Friedman <strong>and</strong> Tr o t t 11 d e t e r m i n e dwhether aging interacted with the familiarity/recollection distinctionin modulating encoding-related ERP a c t i v i t y. Comparedwith the data of the young described above, for thee l d e r l y, reliable SMEs were observed in association withboth subsequent R <strong>and</strong> K judgments. Friedman <strong>and</strong> Tr o t t 11concluded that, during the study phase, older subjects didnot differentially encode those items that would be subsequentlyassociated with retrieval of contextual details(remember) from those that would not (know). Furthermore,these data implicated age-related deficits in encoding ascontributing to episodic memory deficits in the elderly.These conclusions received some support from the distributionof SME activity across the scalp. For the young, inaddition to positive electrical activity, the SME for R judgmentswas associated with negative activity over left inferiorprefrontal scalp (LIPFS); there was no evidence of negativeactivity over LIPFS in the data of the elderly. 13 Thenegative activity could have reflected retrieval of informationfrom semantic memory, as R. Johnson <strong>and</strong> coworkers15 observed negative-going ERP activity over LIPFS inassociation with semantic but not orthographic decisions.Such results fit well with those of hemodynamic studiesshowing that the retrieval of semantic memories <strong>and</strong> theencoding of episodic memories depend upon activity inregions of the LIPF Cortex (LIPFC 16 ). Assuming that theblood flow <strong>and</strong> ERP data share at least some common3
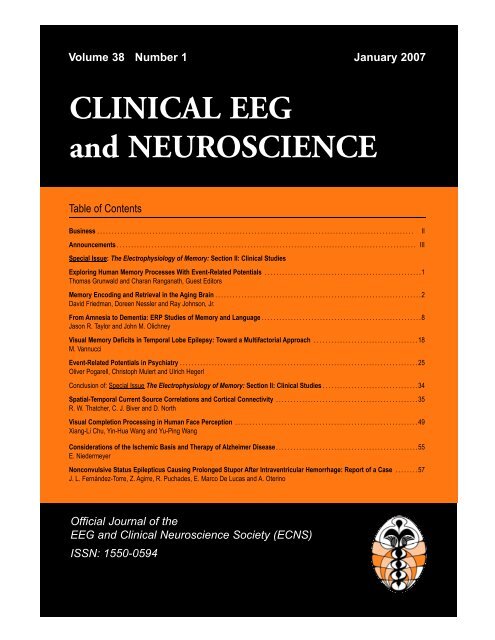
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Figure 1Left panel. Gr<strong>and</strong> mean difference waveforms (High-selection minus Low-selection) recorded over left prefrontal scalp electrodes. Thedata for the young (solid lines) <strong>and</strong> elderly (dashed lines) are superimposed. Early (light gray shading; 400-800 ms) <strong>and</strong> late (dark grayshading; 1200-1400 ms) regions of the waveforms are indicated. Additionally, the black shading in the early interval indicates the regionwhere the ERPs of the young were more negative than those of the elderly. Time lines every 600 ms with arrows indicating stimulusonset. Right panel. Surface potential, spline-interpolated scalp maps (based on the averaged reference computed on a 62-channel,extended 10-20 montage 41 ) are depicted for the early <strong>and</strong> late measured intervals computed on the young <strong>and</strong> elderly waveforms depictedin the left panel. Dots represent the 62 scalp locations.brain generators, together they suggest that the olderadults of the Friedman <strong>and</strong> Trott investigation 11 may havebeen impaired in semantic encoding, which could havebeen responsible for their lower recognition success.Supporting evidence for this conclusion has come frombehavioral investigations documenting that older adults, inthe absence of a specific encoding strategy, do not usesemantic elaboration spontaneously. 17 Hence, becausevolunteers in the Friedman <strong>and</strong> Trott 11 investigation wereasked simply to memorize the nouns without any specificencoding instructions, it is difficult to determine from thosedata whether the putative encoding deficiency in the elderlywas due to a failure of semantic retrieval, a failure ofepisodic encoding or both.To investigate further the nature of encoding processesin the elderly, Nessler <strong>and</strong> colleagues 18,19 exerted greatercontrol over the use of encoding strategies with a semanticselection paradigm adapted from Thompson-Schill <strong>and</strong>coworkers. 20 In our modified version of the object classificationtask described by Thompson-Schill et al., 20 young<strong>and</strong> older participants were asked to study words underLow- <strong>and</strong> High-selection conditions. The Low-selectiontask required a decision as to whether a previously presentedpicture (e.g., lion) matched the meaning of a to-berememberedword (e.g., lion). In the High-selection condition,by contrast, a decision was made concerning whethera previously presented adjective (e.g., heavy) described afeature of the to-be-remembered word (e.g., feather).While both decisions necessitated the retrieval of thesemantic concept, the High-selection decision required, inaddition, the selection of specific semantic features fromseveral alternatives. This design enabled us to assessage-related changes in ERP activity under conditions inwhich young <strong>and</strong> old participants engaged in qualitativelysimilar types of encoding activity (see Rugg <strong>and</strong> Morcom 21for other methodological issues in ERP research on aging).Following the encoding phase, a recognition test on theitems studied under Low- <strong>and</strong> High-selection conditionsenabled us to determine whether the age-related decline inrecognition memory was due to failures in semanticretrieval/selection <strong>and</strong>/or episodic encoding.During the encoding phase, older adults performed aswell as the young adults, indicating that they were well ableto retrieve semantic information <strong>and</strong> select among competingalternatives in the High-selection condition. However,during the subsequent recognition test, older adults performedreliably more poorly than the young adults. Figure 1depicts the encoding-related ERP activity elicited overLIPFS in the young <strong>and</strong> elderly adults obtained by subtractingthe activity elicited in the Low-selection condition fromthat elicited in the High-selection condition. These diff e r-ence waveforms show for both young <strong>and</strong> old adults significantnegative activity in the early period (400-800 ms) overLIPFS. This selection-related effect is sustained in theyoung adult data into the late time interval (1200-1400 ms),but dramatically attenuated in the older adult waveforms.A d d i t i o n a l l y, the young show greater negativity than the elderlyin the early interval. Hence, there appear to be three4
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1negativities: an early, selection-related activity present inboth young <strong>and</strong> old ERPs; an additional, early negativitypresent only in the waveforms of the young; <strong>and</strong> a late,selection-related negativity, again present only in the ERPsof the young. Consistent with their equivalent behavioralperformance, the magnitude of the early, selection-relatednegativity was the same in the young <strong>and</strong> elderly, suggestingthat this brain activity reflects semantic retrieval/selection.As the young outperformed the elderly during recognitiontesting, the additional early negativity <strong>and</strong> the late negativitypresumably reflect episodic encoding, i.e., additionalsemantic elaboration performed on the products of semanticretrieval/selection. On this view, our data support theconclusion that the episodic memory deficit in the elderly inthe current paradigm is a result of a failure to engage inadditional episodic encoding which would have resulted inmore richly encoded memory traces, thereby ensuring ahigher rate of successful retrieval. The topographic mapsillustrated in Figure 1 (right panel) demonstrate dramaticallyattenuated negative activity in the late interval over LIPFSfor the elderly. Hence, the hemodynamic data reviewed earlier<strong>and</strong> these topographic data suggest that the age-relatedencoding difficulties may have resulted from a failure toactivate LIPFC in the late interval.The Friedman <strong>and</strong> Tr o t t 11 <strong>and</strong> Nessler et al. 1 9 d a t asuggest that encoding deficiencies may underlie thewell-documented episodic memory decline in elderlysamples. We turn now to a consideration of ERP d a t arecorded at retrieval.Retrieval-related studiesRecognition processes can be studied by separatelyaveraging the ERP activity elicited by old items that are correctlyrecognized (i.e., hits) <strong>and</strong> new items that are correctlyrejected. A subtraction of the latter from the formerreveals the episodic memory (EM) effect, an index ofr e t r i e v a l . 2 2 In young adults, a series of EM effects with distincttemporal <strong>and</strong> topographic patterns have beenobserved fairly consistently in many investigations of recognitionmemory, suggesting that they reflect unique stages ofmnemonic processing. 2 2 For example, relatively early in theretrieval process, between approximately 300 <strong>and</strong> 500 ms,a medial frontal, positive-going, EM effect has been associatedwith the familiarity component of recognition memory.This association with familiarity is based upon observationsthat its amplitude is similar to 1) correctly recognized olditems regardless of whether they are endorsed with rememberor know judgments, 2 3 2) correctly recognized old itemsregardless of whether the contextual details from the originalepisode are correctly identified, 2 4 <strong>and</strong> 3) correctly recognizedold items <strong>and</strong> falsely recognized items that are highlysimilar to the previously studied old items, i.e., “lures.” 2 5 , 2 6On the other h<strong>and</strong>, later in the retrieval sequence, a subsequentleft parietal, positive-going, EM effect (500-800 ms)has been associated with recollection, as its amplitude islarger to 1) correctly recognized old items associated withremember compared to know judgments, 2 3 2) correctly recognizedold items associated with correct compared toincorrect source judgments, 2 7 <strong>and</strong> 3) correctly recognizedold items compared to falsely recognized, highly similar lurei t e m s . 2 5 Consistent with the medial prefrontal <strong>and</strong> left parietalEM effects reflecting distinct mnemonic processes,recent data have indicated that they are associated withreliably different scalp distributions, suggesting diff e r e n tintracranial generators. 2 4 , 2 8 , 2 9Later-onsetting, longer duration EM effects have alsobeen reported. For example, an asymmetric, positive, rightprefrontal EM effect has been observed, although a consensusregarding its functional significance has yet to bearrived at. It onsets roughly with the diminution of the leftparietal EM effect <strong>and</strong> reaches peak amplitude typically followingmean reaction time for the old/new recognition decision.The post-response timing of this component has ledsome authors to suggest that it may reflect a cognitive controlfunction, such as evaluating the products of retrieval tosupport ongoing memory performance. 30Based on the finding that the elderly rely more on familiaritythan recollection, <strong>and</strong> assuming that the medial prefrontalEM effect reflects familiarity-based processing, oneexpectation is that this EM effect would be of similar magnitudein the ERPs of the young <strong>and</strong> elderly. Unfortunately,few studies have directly assessed age-related changes inthe medial prefrontal EM effect. In the Remember/Knowstudy of Trott et al 23 described above, the medial prefrontalEM effect (300-500 ms) was of similar magnitude <strong>and</strong>topography in the young <strong>and</strong> old adult waveforms in associationwith correctly recognized old items given either R orK judgments (see also Wegesin et al 31 ). Along with a similarpercentage of old items attracting know judgments inthe young <strong>and</strong> elderly, these limited ERP data suggest anintact familiarity mechanism in the elderly.By contrast with the paucity of data on age-relatedchanges in the medial prefrontal EM effect, somewhat moreis known about the left parietal EM effect. Based on thebehavioral literature emphasizing age-related deficits in recollection<strong>and</strong> the ERP data reviewed earlier suggesting thatthe left parietal EM effect indexes contextual retrieval, onemight expect smaller-magnitude left parietal EM effects inthe ERPs of the elderly compared to those of the young. Tothe contrary, this has generally not proven to be the case.Initial investigations by Friedman et al, 3 2 Rugg et al 3 3 a n dSwick <strong>and</strong> Knight 3 4 did not use behavioral indices presumedto reflect familiarity <strong>and</strong> recollection. In later studies, however, measures considered proxies for recollection <strong>and</strong> familiaritywere collected <strong>and</strong>, hence, the results of these investigationsprovide a firmer basis for conclusions about aginge ffects on the left parietal EM effect. Both Mark <strong>and</strong> Rugg 3 5<strong>and</strong> Trott et al 2 3 solicited R <strong>and</strong> K as well as source judgmentsfrom young <strong>and</strong> older adults. In both investigations,5
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1the left parietal EM effect in response to correctly recognizedold items attracting R judgments (or correct sourcejudgments) did not differ in magnitude or scalp topographybetween young <strong>and</strong> older adults. Similar phenomena wereobserved by Wegesin <strong>and</strong> coworkers. 31 Despite this similarit y, in all of these investigations older adults showed greaterdecrements in source compared to item memory relative toyoung adults. 36 M o r e o v e r, the temporal precision of the ERPmethod enabled the investigators in all three studies todetermine that the EM effects were prolonged in olderadults by about 100 ms relative to those of the young. T h i sfinding appears to be consistent with the cognitive slowingthat is typically observed in older adults. 37 Although limited,these data collectively suggest that, to the extent that theleft parietal EM effect reflects the retrieval of source-specifyinginformation, older adults, albeit with prolonged processingtime, do not appear to differ from young adults inthis aspect of memory retrieval.The results of age-related investigations of the rightprefrontalEM effect are not at all in agreement. This maynot be surprising given the somewhat imprecise definitionof “post-retrieval processing” that has been ascribed to thisEM effect. In two studies of recognition memory withsource judgments, Trott <strong>and</strong> colleagues 23 <strong>and</strong> Wegesin etal 31 observed robust right prefrontal EM effects in theiryoung adult participants but failed to find similar activity inthe waveforms of their older adults. On the other h<strong>and</strong>,Mark <strong>and</strong> Rugg 35 <strong>and</strong> Li et al, 38 also in source memory paradigms,did observe reliable right prefrontal EM effects intheir older adult waveforms. Given the elusive nature of thebehavioral correlates of this EM effect <strong>and</strong> the contradictoryage-related findings, it is difficult to comment with anyconfidence on the import of this EM effect in underst<strong>and</strong>ingage-associated changes in episodic memory.CONCLUSIONSClearly, there are too few age-related ERP studies ofepisodic memory to permit firm conclusions. Nevertheless,some tentative implications of the studies reviewed herecan be advanced. The available data suggest that encodingdeficiencies may play a larger role in influencingepisodic memory deficits in older adults. This interpretationis consistent with the results of divided attention studies,which demonstrate greater episodic memory deficits inboth young <strong>and</strong> elderly adults when attention is divided atencoding, with a concomitant decrease in LIPFC activity,compared to when it is divided at retrieval. 39 The encodingrelateddata of Friedman <strong>and</strong> Trott 11 <strong>and</strong> Nessler <strong>and</strong> colleagues18,19 suggest that an underlying mechanism may bea lack of spontaneous elaboration of the products retrievedduring semantic processing (i.e., episodic encoding) perhapsresulting from a failure to recruit LIPFC. The limited,retrieval-based ERP data suggest relatively intact familiarity-<strong>and</strong> recollection-based processing in the elderly.However, this does not account for the consistently poorersource memory performance of older relative to youngeradults despite similar-magnitude, left parietal EM effects inyoung <strong>and</strong> elderly samples. This disparity suggests that, inaddition to encoding deficiencies, other, as yet under- orun-explored, retrieval mechanisms might contribute to thisepisodic memory deficit. For example, age-related differencesin retrieval orientation, the differential processing oftest items according to how the items were studied, haverecently been demonstrated. 40 Further study of this type ofphenomenon <strong>and</strong> its impact on age-related episodic memorydecline is clearly warranted. Additionally, future workneeds to address current gaps in knowledge by recordingERP activity during both encoding <strong>and</strong> retrieval phases.Although older adults may not spontaneously elaborateupon the products of semantic retrieval, they do benefitfrom increased processing dem<strong>and</strong>s when given an appropriateencoding strategy. 18,19 Hence, future studies shouldinclude this type of levels of processing manipulation. 6These kinds of investigations will undoubtedly bring uscloser to a better underst<strong>and</strong>ing of the root causes of agerelateddecline in episodic memory.ACKNOWLEDGMENTSThe writing of this manuscript was supported by NIAGrants AG05213 <strong>and</strong> AG09988 <strong>and</strong> by the New York StateDepartment of Mental Hygiene. We are grateful to CharlesL. Brown III for computer programming <strong>and</strong> technicalassistance, Ms. Efrat Schori <strong>and</strong> Ms. Letecia Latif for theirassistance in the recruiting <strong>and</strong> screening of volunteers<strong>and</strong> Mr. Michael Bersick for various aspects of data collection<strong>and</strong> analysis.REFERENCES1. Ebbinghaus H. <strong>Memory</strong>: a contribution to experimental psychology.New York: Dover Publications; 1964.2. Light LL. <strong>Memory</strong> <strong>and</strong> aging: four hypotheses in search ofdata. Ann Rev Psychol 1991; 42: 333-376.3. Tulving E. What is episodic memory? Curr Direct PsycholSci 1993; 2: 67-70.4. Yonelinas A P. The nature of recollection <strong>and</strong> familiarity: areview of 30 years of research. J Mem Lang 2002; 46:4 4 1 - 5 1 7 .5. Craik FIM, Lockhart S. Levels of processing: a frameworkfor memory research. J Verb Learn Verb Behav 1972; 11 :6 7 1 - 6 8 4 .6
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 16. Craik FI. Levels of processing: past, present <strong>and</strong> future?<strong>Memory</strong> 2002; 10: 305-318.7. Paller KA, Wagner AD. Transforming experience into memory:observations of mind <strong>and</strong> brain. Trends Cogn Sci 2002; 6:93-102.8. Sanquist TF, Rohrbaugh JW, Syndulko K, Lindsley DB.Electrocortical signs of levels of processing: perceptualanalysis <strong>and</strong> recognition memory. Psychophysiology 1980;17: 568-576.9. Paller KA, Kutas M, Mayes AR. Neural correlates of encodingin an incidental learning paradigm. ElectroencephalogrClin Neurophysiol 1987; 67: 360-371.10. Tulving E. <strong>Memory</strong> <strong>and</strong> consciousness. Can Psychologist1985; 26: 1-12.11. Friedman D, Trott C. An event-related potential study ofencoding in young <strong>and</strong> older adults. Neuropsychologia 2000;38: 542-557.12. Parkin AJ, Walter BM. Recollective experience, normalaging, <strong>and</strong> frontal dysfunction. Psychol Aging 1992; 7: 290-298.13. Friedman D. Age-associated changes in episodic memory:event-related potential (ERP) investigations of recollection<strong>and</strong> familiarity. In: Zimmer HD, Mecklinger A, Lindenberger U,(eds). Binding in Human <strong>Memory</strong>: A N e u r o c o g n i t i v eApproach. New York: Oxford. In press.14. Jennings JM, Jacoby LL. An opposition procedure for detectingage-related deficits in recollection: telling effects of repetition.Psychol Aging 1997; 12: 352-61.15. Johnson R Jr, Barnhardt J, Grossman S, Adler N, SchindlerD. Levels of processing effects on memory encoding <strong>and</strong>retrieval: an ERP mapping study. Psychophysiology 2001;38: S53.16. Wagner AD, Schacter DL, Koutstaal MRW, Maril A, Dale AM,Rosen BR, et al. Building memories: remembering <strong>and</strong> forgettingof verbal experiences as predicted by brain activity.Science 1998; 281: 1188-1191.17. Hashtroudi S, Parker ES, Luis JD, Reisen CA. Generation<strong>and</strong> elaboration in older adults. Exper Aging Res 1989; 15:73-78.18. Nessler D, Johnson R, Bersick M, Friedman D. On why theelderly have normal semantic retrieval but deficient episodicencoding: a study of left inferior frontal ERP a c t i v i t y.Neuroimage 2006; 30: 299-312.19. Nessler DR, Johnson J, Bersick M, Friedman D. Age-relatedepisodic encoding deficits are associated with early attenuationof a left inferior prefrontal negativity. J Cogn Neurosc2005; 17: 136.20. Thompson-Schill SL, D’Esposito M, Aguirre GK, Farah MJ.Role of left inferior prefrontal cortex in retrieval of semanticknowledge: a reevaluation. Proc Natl Acad Sci USA 1997; 94:14792-14797.21. Rugg MD, Morcom AM. The relationship between brain activity,cognitive performance <strong>and</strong> aging: the case of memory. In:Cabeza R, Nyberg L, Park D, (eds). Cognitive Neuroscienceof Aging: Linking Cognitive <strong>and</strong> Cerebral Aging. New York:Oxford University Press; 2005: 132-154.22. Friedman D, Johnson R. Event-related potential (ERP) studiesof memory encoding <strong>and</strong> retrieval: a selective review.Microsc Res Tech 2000; 51: 6-28.23. Trott CT, Friedman D, Ritter W, Fabiani M, Snodgrass JG.Episodic priming <strong>and</strong> memory for temporal source: eventrelatedpotentials reveal age-related differences in prefrontalfunctioning. Psychol Aging 1999; 14: 390-413.24. Friedman D. ERP studies of recognition memory: differentialeffects of familiarity, recollection <strong>and</strong> episodic priming. CognSci 2004; 1: 81-12125. Curran T. Brain potentials of recollection <strong>and</strong> familiarity. MemCogn 2000; 28: 923-938.26. Nessler D, Mecklinger A, Penney TB. Event related brainpotentials <strong>and</strong> illusory memories: the effects of differentialencoding. Cogn Brain Res 2001; 10: 283-301.27. Wilding EL, Rugg MD. An event-related potential study ofrecognition memory with <strong>and</strong> without retrieval of source.Brain 1996; 119: 889-905.28. Johnson R Jr, Kreiter K, Russo B, Zhu J. A spatio-temporalanalysis of recognition-related event-related brain potentials.Intl J Psychophysiol 1998; 29: 83-104.29. Rugg MD, Yonelinas AP. Human recognition memory: a cognitiveneuroscience perspective. Trends Cogn Sci 2003; 7:313-319.30. Wilding EL, Sharpe H. Episodic memory encoding <strong>and</strong>retrieval: recent insights from event-related potentials. In: ZaniA, Proverbio AM, (eds). The Cognitive Electrophysiology ofMind <strong>and</strong> Brain. New York: Academic Press; 2002: 169-196.31. Wegesin DJ, Friedman D, Varughese N, Stern Y. Age-relatedchanges in source memory retrieval: an ERP replication <strong>and</strong>extension. Cogn Brain Res 2002; 13: 323-338.32. Friedman D, Berman S, Hamberger M. Recognition memory<strong>and</strong> ERPs: age-related changes in young, middle-aged <strong>and</strong>elderly adults. J Psychophysiol 1993; 7: 181-201.33. Rugg MD, Mark RE, Gilchrist J, Roberts RC. ERP repetitioneffects in indirect <strong>and</strong> direct tasks: effects of age <strong>and</strong>interitem lag. Psychophysiology 1997; 34: 572-586.34. Swick D, Knight RT. Event-related potentials differentiate theeffects of aging on word <strong>and</strong> nonword repetition in explicit<strong>and</strong> implicit memory tasks. J Exp Psychol Learn Mem Cogn1997; 23: 123-142.35. Mark RE, Rugg MD. Age effects on brain activity associatedwith episodic memory retrieval: an electrophysiological study.Brain 1998; 121: 861-873.36. Spencer WD, Raz N. Differential effects of aging on memoryfor content <strong>and</strong> context: a meta-analysis. Psychol Aging1995; 10: 527-539.37. Salthouse TA. The processing-speed theory of adult age differencesin cognition. Psychol Rev 1996; 103: 403-428.38. Li J, Morcom AM, Rugg MD. The effects of age on the neuralcorrelates of successful episodic retrieval: an ERP study.Cogn Affect Behav Neurosci 2004; 4: 279-293.39. Anderson ND, Iidaka T, Cabeza R, Kapur S, McIntosh AR,Craik FI. The effects of divided attention on encoding- <strong>and</strong>retrieval-related brain activity: a PET study of younger <strong>and</strong>older adults. J Cogn Neurosci 2000; 12: 775-792.40. Morcom AM, Rugg MD. Effects of age on retrieval cue processingas revealed by ERPs. Neuropsychologia 2004; 42:1525-1542.41. Sharbrough F, Chatrian GE, Lsser RP, Luders H, Nuwer M,Picton T W. Guidelines for St<strong>and</strong>ard Electrode PositionNomenclature Bloomfield: American <strong>EEG</strong> Society; 1990.7
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1From Amnesia to Dementia: ERPStudies of <strong>Memory</strong> <strong>and</strong> LanguageJason R. Taylor <strong>and</strong> John M. OlichneyKey WordsAlzheimer’s DiseaseAmnesiaEvent-Related PotentialsLPCMild Cognitive ImpairmentN400P300P600ABSTRACTCognitive event-related potential (ERP) studies ofmemory <strong>and</strong> language impairments in amnesia <strong>and</strong>A l z h e i m e r’s disease (AD) are reviewed. We l l - c i r c u m-scribed lesions of the medial temporal lobe (MTL) or diencephaloncausing an amnestic syndrome, an inability toencode <strong>and</strong> retrieve episodic memories beyond the briefduration of working memory, appear to produce alteredplasticity of the late positive P600 component, but usuallyspare P300 <strong>and</strong> N400 components. The neuropathology ofAD affects MTL <strong>and</strong> extends to neocortical associationareas, causing deficits of episodic <strong>and</strong> semantic memory.In AD dementia, the P300, N400, <strong>and</strong> P600 all commonlyshow abnormalities. ERP studies of individuals with mildcognitive impairment may reveal neurophysiologicalchanges prior to the emergence of clinical deficits, whichcould advance the early detection <strong>and</strong> diagnosis of AD.INTRODUCTIONTo the cognitive psychologist, time is of the essence;temporal measures such as response time (RT) have providednumerous insights in behavioral research into theprocesses of attention, memory, <strong>and</strong> language. To thebehavioral neurologist <strong>and</strong> the neuropsychologist, relatingbrain regions to cognitive processes is paramount. Theseobjectives are united in event-related brain potential (ERP)investigations of neurologically impaired patients. ERPmeasures provide a real-time record of summated postsynapticelectrical currents time-locked to a particularevent, typically the presentation of a stimulus or the onsetof a behavioral response. The fine temporal resolution ofthe measure, on the order of milliseconds, allows for a precisequantification of the timing <strong>and</strong> duration of the variousstages of cognitive processing. In neurodegenerative disorderssuch as Alzheimer’s disease (AD), ERPs may thereforebe more sensitive to subtle pathophysiologicalchanges than many behavioral or imaging (CT, MRI, PET)measures. Furthermore, unlike functional imaging methods,ERPs are not dependent upon blood-flow or metabolicchanges that are secondary to neural activity <strong>and</strong> proneto alterations in neuro-vascular coupling.Studies of neurological patients have been instrumentalin characterizing the cognitive processes indexed byparticular ERP components <strong>and</strong> in narrowing the searchfor neural generators. Take, for example, individuals withwell-circumscribed amnesia due to medial-temporal lobe(MTL) pathology, reviewed below. In most cases of MTLamnesia, the neuropathology is relatively focal (albeit bilateral),allowing researchers to investigate whether theaffected regions are critical for the generation of particularERP components. This same goal has also been pursuedthrough intracranial recordings of pre-operative patientswith temporal lobe epilepsy. The cognitive deficits presentin MTL amnesia have been well characterized throughbehavioral studies: The encoding <strong>and</strong> storage of new informationinto long-term memory is impaired, whereas thespan <strong>and</strong> duration of working memory are typically unaffected.1 This has allowed researchers to assess the extentto which particular ERP components are dependent uponthose processes that are impaired in MTL amnesia. Forexample, Olichney <strong>and</strong> colleagues 2 found that the P600word-repetition effect (but not the N400 word-repetitioneffect) was diminished in amnesics, supporting the hypothesisthat the P600 component can be a useful index ofrapid forgetting vs. successful encoding.Information also flows in the other direction; ERP studieshave been used to inform models of intact <strong>and</strong> impairedcognitive processing in neurological disorders. T h i sapproach has been applied to AD, also reviewed below.Jason R. Taylor, PhD, Postdoctoral Scholar, is from the Department ofNeurosciences, University of California, San Diego, <strong>and</strong> Veterans MedicalResearch Foundation; John M. Olichney, MD, Associate Professor <strong>and</strong>Staff Neurologist, is from the Department of Neurosciences, University ofCalifornia, San Diego, <strong>and</strong> the VA San Diego Healthcare System. Bothauthors are currently at the Department of Neurology, University ofCalifornia, Davis.Address requests for reprints to John M. Olichney, MD, Center for Mind<strong>and</strong> Brain, 267 Cousteau Place, Davis, CA 95618-5412, USA..Email: jason.taylor@alumni.brown.edu or jmolichney@ucdavis.edu8
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1For example, Auchterlonie <strong>and</strong> colleagues 3 investigatedwhether anomia in AD was attributable to degradation ofthe semantic store or to an independent word-findingdeficit. In that study, the N400 component-sensitive tosemantic processing load, was equally diminished inresponse to named <strong>and</strong> unnamed pictures, suggesting thatanomia <strong>and</strong> semantic deficits are independent in AD.As sensitive measures of cognitive processes <strong>and</strong> theirdisruption due to neuropathology, ERPs have much potentialclinical utility. For example, ERPs may aid in the earlydiagnosis of neurodegenerative disorders such as AD. Wi t hcareful study design, ERPs may be used to isolate relevantcognitive processes <strong>and</strong> to facilitate differential diagnosis. A sdirect measures of synaptic function, ERPs are also potentiallyuseful in the evaluation of pharmacological treatments.The present work is a selective review of cognitive-ERP studies of memory <strong>and</strong> language impairments inamnesia <strong>and</strong> AD. The amnestic syndrome, typically causedby bilateral lesions of the MTL, is characterized by theinability to encode <strong>and</strong> retrieve episodic memories beyondthe brief duration of working memory. The neuropathologyof AD includes MTL structures early in the course of thedisease, <strong>and</strong> a deficit of episodic memory is one of theearly behavioral hallmarks of the disease. However, neocorticalassociation areas are also affected early in AD, <strong>and</strong>patients may present with semantic memory <strong>and</strong> wordfindingdeficits. Therefore, ERP effects that are dependentupon successful encoding <strong>and</strong> retrieval from episodicmemory are expected to be absent or diminished in bothamnesia <strong>and</strong> AD, whereas ERP effects that index semanticprocessing or other higher cognitive functions (e.g.,attention, response selection) may be selectively diminishedin AD. Intracranial <strong>EEG</strong>/ERP studies of pre-surgicaltemporal lobe epilepsy patients provide clues to the neuralgenerators of scalp-recorded ERP components, <strong>and</strong> someof these studies are discussed here. ERP studies of individualswith mild cognitive impairment (MCI), memorydeficits in the absence of functional decline <strong>and</strong> thereforenot meeting the diagnostic criteria for probable AD, arealso discussed, as they may reveal neurophysiologicalchanges that precede clinical deficits. These studies holdgreat potential for the early detection <strong>and</strong> diagnosis of AD.Through this review, we hope to illustrate several keydifferences in the ERP abnormalities in well-circumscribedamnesia compared to dementias such as AD. To anticipate,while well-circumscribed lesions of the MTL or diencephalonappear to produce altered plasticity of the latepositive P600 component, the P300 <strong>and</strong> N400 are usuallyspared. However, with the widespread neuropathologicalchanges in AD, all three of these components commonlyshow abnormalities.P300: OverviewThe P300 (or “P3b”) component is a scalp positivityelicited by low-probability stimuli during stimulus classificationtasks which peaks ~300 ms post-stimulus, maximal overmidline centroparietal sites. In the canonical P300 experiment,the “auditory oddball” task, participants detect a lowprobability“target” (e.g., high-pitched) tone in a stream of“st<strong>and</strong>ard” (e.g., low-pitched) tones, <strong>and</strong> the typical result isa clear P300 for targets with a relatively flat ERP r e s p o n s ein the same latency range for st<strong>and</strong>ards. The P300 has beenextensively studied <strong>and</strong> well characterized in both normal<strong>and</strong> neurologically impaired populations. P300 latency isvariable <strong>and</strong> generally proportional to the complexity of thestimulus evaluation <strong>and</strong> decisional processes dem<strong>and</strong>ed bythe task. It has been suggested that the P300 reflectsprocesses involved in updating working memory, 4 or theprocesses of stimulus discrimination <strong>and</strong> response selecti o n . 5 H o w e v e r, P300 amplitude <strong>and</strong> latency are modulatedby a variety of factors — subjective probability, stimuluss a l i e n c y, availability of attentional resources 6 — <strong>and</strong> itappears to be generated by a distributed network of neuralregions — inferotemporal, perirhinal, prefrontal, cingulate,superior temporal <strong>and</strong> parietal cortices, as well as the hippo c a m p u s 7 , 8 — suggesting that P300 likely indexes a heterogeneousset of cognitive processes. On the other h<strong>and</strong>,studies of patients with damage to the temporo-parietal junctionhave found that the auditory P300 response is eliminated , 9 suggesting that this neocortical region may be critical ingeneration or propagation of the scalp P300.P300 in amnesiaGiven that working memory <strong>and</strong> response selectionprocesses are not typically disturbed in circumscribed medial-temporalamnesia, one might expect the P300 responseto low-probability stimuli to be intact in this population.H o w e v e r, as noted above, intracranial recordings haveshown that the hippocampus <strong>and</strong> paralimbic cortices areamong the brain regions that produce P300-like responses.It remains unknown to what extent the medial-temporalP300 contributes to the P300 recorded at the scalp.Rugg et al 10 studied the P300 response of a single individualwith amnesia due to an infiltrating glioma in the leftMTL. In both auditory <strong>and</strong> visual oddball experiments,Rugg et al found normal P300 effects in this amnesicpatient. Another report of an individual with amnesia due toa lesion of the left MTL found that the P300 was similarlyintact. 11 Two case studies of bilateral medial temporalpathology also found auditory <strong>and</strong> visual P300s that werecomparable to those in normal controls. 12,13 A group studyof five patients with damage restricted to bilateral MTL dueto various etiologies 14 found no significant differences inauditory or visual P300 amplitude or latency between theamnesic patients <strong>and</strong> controls.Honda et al 15studied a heterogeneous group ofamnesic patients <strong>and</strong> found that the integrity of the auditoryP300 response depended on the extent of MTL damageas detected by structural imaging (MRI, CT). Robust P300responses were found in patients in whom no lesions were9
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1evident (two with transient global amnesia <strong>and</strong> one withviral encephalitis), whereas virtually no P300 responsewas found in a patient with small detectable lesions of thebilateral medial temporal lobes due to viral encephalitis.Another patient with detectable MTL lesions due to herpessimplex encephalitis showed no P300 to targets whenstudied 7 months following disease onset, but a small P300response another 2 months later. Finally, a patient withdetectable MTL damage due to anoxia showed no P300after 2 months, <strong>and</strong> a small early positivity to both targets<strong>and</strong> non-targets 6 months later. The authors interpretedthese results cautiously, noting that patients with MTLlesions that were detectable by imaging may have also hadmore diffuse, microscopic lesions that were undetectable.Taken together, studies of MTL involvement in P300 generationsuggest that focal lesions have little effect on theP300 response, but that more diffuse lesions due to viralencephalitis or anoxia may disturb this component.P300 in Alzheimer’s diseaseIn normal aging, the latency of the auditory P300increases ~1-2 ms/year. 16,17 In AD, an even greater latencyincrease (~2 st<strong>and</strong>ard deviations above the mean of normalolder individuals) is commonly reported, <strong>and</strong> somestudies have found that P300 latency may be useful to differentiatebetween AD pathology <strong>and</strong> other disorders (e.g.,depression, schizophrenia 18,19 ). In combination with st<strong>and</strong>ardneuropsychological tests, the clinical utility of theP300 latency measures is enhanced: Goodin 20 found thatin cases of equivocal dementia (50% pretest probability),those with concurrent P300 latency delay showed agreater likelihood of having a dementing illness (estimatedat 90%). P300 amplitude appears to be reduced in AD, butthis is also the case in several other neurological <strong>and</strong> psychiatricdisorders (e.g., vascular dementia, schizophrenia).In contrast, other studies have found P300 latency tobe relatively insensitive in predicting dementia. 21,22 Factorsthat appear to affect the clinical utility of P300 include themethodology used — especially with respect to attentional<strong>and</strong> memory-load dem<strong>and</strong>s — <strong>and</strong> the dementia severityof the patient group (see detailed review in Olichney <strong>and</strong>Hillert 23 ). Abnormal P300 latencies are more likely to bereported in more complex tasks (e.g., counting) rather thanin simple target-detection tasks. It is interesting to note thatthis effect is not simply due to task difficulty per se; Polich<strong>and</strong> Pitzer 24 found that increasing the difficulty of sensorydiscriminations actually decreased the discriminative sensitivityof P300 latency <strong>and</strong> amplitude measures. Althoughthe P300 response has been most commonly studied inthe auditory modality, studies using visual 24 <strong>and</strong> olfactory 25stimuli have reported greater sensitivity to AD pathology.P300 measures appear to be sensitive to dementia severity,showing moderate correlations with mini-mental statusexam (MMSE) scores 22,26 <strong>and</strong> greater sensitivity to moreadvanced stages of dementia.P300 in Mild Cognitive ImpairmentSeveral recent studies have evaluated the auditoryoddball-elicited P300 component in individuals with MCI.Golob et al 27 found significantly longer P300 latency in MCI(mean MMSE = 27.7) relative to controls (mean MMSE =29.2), but no difference in P300 amplitude. In contrast,Frodl et al 28 found that neither P300 amplitude nor latencydiffered between normal controls <strong>and</strong> MCI (mean MMSE =27.5), whereas in mild AD (mean MMSE = 20.8), P300amplitude was reduced <strong>and</strong> latency was delayed relative toboth groups. Golob et al noted that there was great intersubjectvariability in P300 latency in their MCI group, perhapsrelating to the heterogeneity of the group with respectto the unknown presence/absence of AD pathology <strong>and</strong>subsequent conversion to dementia. Indeed, a recent longitudinalstudy of individuals with memory complaintsfound P300 latency differences based on subsequent conversionto AD. 29 Patients who were diagnosed with probableAD within 2 years following the baseline sessionshowed increased P300 latency at baseline relative tothose diagnosed with other dementias (vascular <strong>and</strong> frontotemporal),MCI, or no cognitive impairment. However, itshould be noted that baseline mean MMSE scores weresignificantly lower for the AD-converting group (26.3) thanfor the MCI (28.1) <strong>and</strong> non-impaired (28.6) groups.Summary: P300 oddball effects in AD <strong>and</strong> MCIIt is clear that P300 latency is delayed <strong>and</strong> amplitude isoften decreased in AD. However, because similar P300abnormalities may also be found in other patient populations,the clinical utility of P300 in the differential diagnosisof AD may depend upon the development of more sensitiveparadigms, or perhaps the use of sensory modalitiesother than audition. There is some evidence that P300latency delay in individuals with MCI may indicateincreased risk for subsequent conversion to AD, whichdeserves further investigation.N400: OverviewThe N400 is a scalp negativity elicited in response tomeaningful stimuli that peaks ~400 ms post-stimulus overbilateral temporal channels. The N400 is typically largerover the right hemisphere for visual words, but shows aslight left-hemisphere bias for auditory words. 30 , 31Intracranial recordings have consistently found N400-likepotentials generated in the anterior fusiform <strong>and</strong> parahippocampalgyri bilaterally, 32,33 <strong>and</strong> other c<strong>and</strong>idate N400generators include the superior temporal sulcus, <strong>and</strong> posteriorparietal <strong>and</strong> ventral prefrontal cortices. 34 The N400 issensitive to the semantic congruity of the stimulus with thepreceding context, with amplitude being reduced to stimulithat are presented in a congruous context (e.g., a coherentsentence, a single related word) or if the stimulus is repeated(reviewed in a later section). The effect of semantic congruityon the N400 (the “N400 effect”) has been interpretedas reflecting the reduction in processing effort needed to10
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1access the meaning of a stimulus as a result its appearancein a coherent context. 35,36N400 in Alzheimer’s diseaseThe N400 has been used to evaluate the integrity ofsemantic memory in A l z h e i m e r’s disease. Language dysfunctionis evident relatively early in the course of A D ;patients often present with word-finding deficits <strong>and</strong> performpoorly on tests of letter <strong>and</strong> category fluency. 37 The latter issuggestive of a breakdown of semantic memory 38 ; indeed,behavioral studies (e.g., the triadic word task) have foundevidence that semantic associations are progressivelydegraded in A D . 39 H o w e v e r, it is a matter of debate whetherthe semantic impairment in AD should be characterized asd i fficulty in retrieving information from an intact memorystore or as degradation of the representations themselves. 40In healthy adults, the N400 response to visually presentedwords is sensitive to aging: N400 latency increasesat ~2 ms/year <strong>and</strong> N400 amplitude decreases at ~0.07µV/year across the adult lifespan. 41,42 From ERP studies ofsemantic memory in AD (reviewed below), it is apparentthat the N400 is usually abnormal in AD, typically reducedin amplitude <strong>and</strong> delayed in latency beyond what is expectedin normal aging. Measures of N400 latency may be usefulas a staging tool for dementia progression: Using a linearregression model, Iragui <strong>and</strong> colleagues 43 found thatneuropsychological test scores could be used to predictN400 latency (peak <strong>and</strong> fractional area latency of the differencewave contrasting congruous <strong>and</strong> incongruous conditions;R = .90). The progressive flattening of the N400may be a manifestation of failing N400 generators.N400: semantic congruity effects in ADInvestigations of the N400 congruity effect in sentenceprocessing have produced equivocal results in AD. In anearly study by Hamberger et al, 44 the N400 to visually presentedsentence-ending words was modulated byexpectancy <strong>and</strong> semantic relation to virtually the sameextent in AD patients as in young controls. Older controlsshowed a different pattern of N400 <strong>and</strong> RT effects, whichthe authors attributed to a response strategy. However, ADpatients’ N400 amplitudes were not significantly differentfrom the older controls overall, providing evidence forspared semantic processing in AD. In contrast, in an ERPstudy of spoken sentences, Ford et al 45 found that theN400 expectancy/congruity effect to sentence-terminalwords was significantly reduced (though still greater thanzero) in AD relative to age-matched controls. Similarly,Revonsuo et al 46 found a reduced N400 congruity effect inAD in an auditory sentence paradigm. In that study, noovert response was required of the participants, they weresimply told <strong>and</strong> periodically reminded to attend to the sentences,so the results are unlikely to be “contaminated” bythe P300 component, known to be delayed in AD.Studies using minimal semantic contexts to elicit anN400 effect have generally found that the effect is diminishedin AD. In a study by Schwartz et al, 47 participantsheard a category name, then saw a word, <strong>and</strong> judgedwhether the word belonged to the named category (e.g.,“animal” - “cow”). The N400 effect, greater negativity elicitedby incongruous relative to congruous target words, wassmaller <strong>and</strong> delayed in AD patients relative to age-matchedcontrols. Iragui et al 43 found similar results. In that study,participants heard auditory statements that defined a category(e.g., “a type of flower”) or an antonym relation (e.g.,“the opposite of tall”), then read a word that was either congruousor incongruous with the preceding statement, <strong>and</strong>judged the congruity of the statement <strong>and</strong> target word. TheN400 effect was significantly reduced <strong>and</strong> delayed in ADpatients relative to controls. Reduced N400 effects in ADhave also been found with pictorial stimuli used as primesfor lexical targets 48 as targets following lexical primes, 3 <strong>and</strong>as both prime <strong>and</strong> target. 49,50It is interesting to note that despite the preponderanceof evidence suggesting that the N400 response is impairedin AD, some of the studies reported above have nonethelessfound evidence of normal semantic network structurein AD. Hamberger et al 44 found that AD patients’ N400response followed the expected descending gradient overfour sentence ending conditions: unrelated-nonsense >unrelated-sense > related-sense > best completion.Schwartz et al 47 compared the N400 effect for target wordsprimed by superordinate <strong>and</strong> subordinate category labels<strong>and</strong> found that, in both AD patients <strong>and</strong> controls, the effectwas largest for subordinate labels. Furthermore, two studiesfound evidence that anomia in AD may be independentof the integrity of the semantic system. Auchterlonie et al 3found that the N400 congruity effect for pictures primed bywords was similarly diminished for pictures that were laternamed correctly as for those that were later named incorrectly.Ford et al 48 also found a dissociation between namingbehavior <strong>and</strong> N400 response, albeit the opposite one:AD patients showed small but significant N400 congruityeffects for word targets whether primed by named orunnamed pictures.Summary: N400 semantic congruity effects in ADMost ERP studies of semantic processing in AD haveshown N400 amplitude <strong>and</strong> latency abnormalities withreduced effects of semantic congruity. However, severalstudies have reported that AD patients show a normal gradientof N400 congruity effects over different levels of categoryhierarchy <strong>and</strong> expectancy, suggesting that semanticstructure is relatively preserved in mild AD. Furthermore,ERP evidence has been used to argue that anomia in ADis not simply attributable to impaired semantic processing.The N400 may provide a useful biomarker for monitoringthe stages of disease progression in AD.N400 <strong>and</strong> P600: Effects of repeating meaningful stimuliMany studies in the ERP literature have found that latepotentials, specifically, the N400 (described above) <strong>and</strong>11
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1P600, are modulated by repetition of meaningful stimulisuch as words <strong>and</strong> pictures. The effect of repetition on theN400 is much like the effect of a congruous semantic context:Repeated stimuli normally elicit a smaller negativitythan novel stimuli, or may eliminate the N400 componententirely. The P600 (or late positive component, LPC) is apositivity that peaks ~600 ms after the presentation ofmeaningful stimuli (e.g., words, pictures). Its scalp distributionis similar to that of the P300 elicited by simple tones orshapes — a midline parietal maximum, slightly greaterover the left hemisphere, 51 but the P600 peaks later <strong>and</strong> iselicited by more complex stimuli. Depth recordings in presurgicalepilepsy patients have found P600-like waveformsgenerated in the hippocampus, entorhinal cortex, <strong>and</strong> severalother paralimbic cortices (i.e., cingulate, temporalpole, orbitofrontal cortex 34 ).In word-list memory experiments, the P600 appears toindex verbal episodic memory processes: Larger amplitudeis found on initial exposure to words that are deeply encoded52,53 or subsequently remembered, 54 <strong>and</strong> on repeatedexposure for words correctly identified as “old”. 55 However,words presented in a coherent semantic context (ratherthan a r<strong>and</strong>omized list) have the opposite effect on theP600, producing smaller amplitudes for repeated relativeto initial presentations. The bivalence of these two congruityeffects was reconciled in a model proposed by VanPetten et al 51 in which the P600 reflects the updating ofworking memory with the contents of long term memory. Ina coherent context, semantically predictable words aremore likely to be in working memory at the time of repeatedexposure, obviating the need for updating workingmemory <strong>and</strong> reducing P600 amplitude.In word-repetition studies, it is often difficult to dissociatethe contributions of N400 <strong>and</strong> P600 to the overall repetitioneffect because the components occupy partiallyoverlapping latency ranges, <strong>and</strong> the effect of repetitionmay be the same on both (i.e., decreased negativity ofN400 <strong>and</strong> increased positivity of P600). Therefore, wordrepetitioneffects are typically expressed as an averagepotential over a time window that spans both components.A few studies that have attempted to dissociate N400 <strong>and</strong>P600 repetition effects are discussed later.N400/P600: repetition effects in temporal lobe epilepsyOne research group has reported several intracranial<strong>EEG</strong>/ERP studies of pre-operative patients with temporallobe epilepsy. 56,57 Grunwald et al 56 found a negative componentin the anterior hippocampus, peaking at ~440 mspost-stimulus (referred to as early negativity for words, orENw), that showed a positive shift in response to repeatedwords (continuous old/new task, lag range: 2-18 items).The ENw was smaller on the side of the epileptogenicfocus (subsequently replicated by Helmstaedter et al 57 ). Inaddition to the ENw, Grunwald et al found a late negativity(LNw) in response to repeated words (virtually flat for initialpresentation) in the posterior hippocampus, peaking at~790 ms, which was also smaller ipsilateral to the focus.Further analyses showed that the LNw was apparent onlyfor repeated words that were correctly responded to as“old,” <strong>and</strong> not for unrecognized old words, following thepattern of the scalp-recorded P600 in normal participants.Smith <strong>and</strong> Halgren 58used an ERP word-list memoryparadigm to study epilepsy patients after unilateral temporallobectomy (average repetition lag: 19 items or 50 seconds).Patients with right anterior temporal lobectomyshowed a robust positivity between 250 <strong>and</strong> 650 ms followingold relative to new items; however, left anterior temporallobectomy patients showed a reduced repetition eff e c t .Using a continuous old/new word judgment task with a relativelyshort repetition lag (6 items), Rugg et al 10f o u n ddiminished (not significantly different from zero) ERP r e p e-tition effects in both left <strong>and</strong> right temporal lobectomypatients. In pre-surgical temporal lobe epilepsy patients,E R P repetition effects were intact over midline electrodesbut reduced over the hemisphere ipsilateral to the seizurefocus. Interestingly, when repetition was incidental to thetask (lexical decision), <strong>and</strong> when some words were repeatedimmediately (lag of 0 items), Rugg et al found significantrepetition positivity in all patient groups. This pattern ofresults suggests that, while lesions of anteromedial temporallobe structures may disrupt ERP word repetition eff e c t sthat are dependent upon intact consolidation processes, notall ERP word repetition effects are generated by this region.N400/P600: repetition effects in amnesiaIn a picture-list memory task (line drawings of commonobjects; average repetition lag: 5 items or 20 seconds),Mecklinger et al 59 found no old/new ERP e ffects in patientswith amnesia due to chronic hypoxia, despite above-chance(but impaired) performance on the recognition task. T h eauthors suggest that recognition performance in amnesiamay be supported by a relatively preserved implicit memoryprocess, but that the ERP measure was not sensitive tothis process. Another interesting dissociation, an ERP e ff e c tfor unrecognized items, was found by Lalouschek et al 60 i na study of a single patient with amnesia due to an aneurysmof the anterior cerebral artery. In that study, ERPs for itemsresponded to as “new” were more negative if the “new”response was incorrect (i.e., unrecognized old items) than ifthe response was correct (i.e., correctly rejected new items)in a very late time window (900-1200 ms) over inferotemporalchannels. Note that Cz was used as a reference in thisstudy; therefore, these results are consistent with increasedpositivity over central channels if a linked mastoid or earlobereference had been employed (as in the majority ofstudies reviewed here).Work in the authors’ laboratory has attempted to isolatescalp-recorded N400 <strong>and</strong> P600 effects in amnesia byadding a semantic congruity manipulation to a word-repetitionparadigm. 2 In this procedure, a category statement12
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Figure 1.Gr<strong>and</strong> average waveformsfor congruous words (initial<strong>and</strong> repeated presentations)for normal elderly(n=12), amnesic (n=12),Mild Cognitive Impairment(n=14; mean MMSE=27)<strong>and</strong> mild AD (n=11; meanMMSE=24) groups. TheP600 is indicated in thenormal group waveforms.The congruous repetitioneffect (due to a diminishedP600 to repeated words) isshaded between 300-800ms where present.was spoken (e.g., “A type of wood”) followed by the visualpresentation of a target word (e.g., “cedar”; equal numbersof congruous <strong>and</strong> incongruous trials were presented) <strong>and</strong>participants were required to read the target word <strong>and</strong> verballyindicate whether it belongs to the preceding category.Category statement-target pairs were repeated once (lag:0-3 trials or 10-40 sec later) or twice (lag for each repetition:10-13 items or about 120 sec). This allowed for analysisof N400 congruity effects (initial congruous vs. initialincongruous trials), N400/P600 repetition effects in theabsence of a coherent semantic context (repeated incongruousvs. initial incongruous), <strong>and</strong> isolated P600 repetitioneffects (repeated congruous vs. initial congruous). Thislast comparison allowed for isolation of the P600 becausethe congruity of the category statement <strong>and</strong> the targetessentially eliminated the N400. Amnesic patients showeda significant N400 congruity effect (latency window: 300-500 ms), <strong>and</strong> a significant N400 repetition effect for incongruoustargets, but no P600 effect for repeated congruoustargets (this effect was robust in normal controls from 500-800 ms; see Figure 1).Olichney et al 2 found no correlation between the amplitudesof the N400 <strong>and</strong> P600 repetition effects within theamnesic patient group, supporting the notion that thesetwo components index different cognitive <strong>and</strong> neuralprocesses. Furthermore, the magnitude of the P600 (butnot the N400) repetition effect correlated with neuropsychologicalmeasures of the patients’ verbal memory ability<strong>and</strong> with subsequent cued-recall performance for the presentedstimuli. This work suggests that the N400 is intactin patients with well-circumscribed amnesia, showing bothsemantic congruency <strong>and</strong> repetition effects. Furthermore,the size of their N400 repetition effect showed no relationto explicit memory performance. Thus, the N400 may be aneural correlate of amnesics’ preserved implicit memoryprocesses as observed in conceptual priming tasks. 1 Thediminished P600 repetition effect in amnesia <strong>and</strong> its correlationwith explicit memory performance are consistent withthe interpretation of the P600 as reflecting the updating ofworking memory with the contents of long term memory. Inamnesic patients, this updating was evidently necessaryfor both the new <strong>and</strong> old congruous stimuli.N400/P600: repetition effects in Alzheimer’s diseaseThe neuropathology of AD affects the medial temporallobes early in the course of the disease, <strong>and</strong> deficits ofepisodic memory are usually the earliest presenting symptom.Therefore, one might expect ERP word-repetitione ffects in AD to resemble those of medial-temporalamnesics. However, studies of ERP word-repetition effectsin AD have produced a complex pattern of results.Using a continuous semantic judgment task (buttonpressrequired for “animal” names) with incidental repetitionof non-targets (“non-animal” words were repeated;average lag: 30 sec) in AD, Friedman et al 61 reported preservedlate (700-1000 ms) repetition effects in most (6 of10) mild AD patients. The authors attributed the residualrepetition effects to relatively preserved implicit memoryprocesses in AD. Rugg et al 62 used a similar continuoustask with incidental repetition at somewhat shorter lags(average: 6-21 sec) <strong>and</strong> found ERP repetition effects (300-400 <strong>and</strong> 400-700 ms) in AD that were statistically indistinguishablefrom those in controls, although a trend for asmaller repetition effect with longer lags was noted.In contrast, Tendolkar et al 6 3 employed an explicit wordlistmemory task <strong>and</strong> a longer inter-item lag (~5 minutes) <strong>and</strong>found very different results. In that study, controls exhibiteda large repetition positivity for correctly recognized old itemsin both early (300-600 ms) <strong>and</strong> late (700-900 ms) latencywindows. This effect was further enhanced for items forwhich source memory was also correctly retrieved (wordshad been displayed in one of two colors) from 600-900 ms,supporting an association between late positivity (P600) <strong>and</strong>conscious retrieval processes. In AD patients, no repetitione ffect was present in the late time window, <strong>and</strong> an effect in13
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Figure 2.Gr<strong>and</strong> averagewaveforms forincongruous words(initial <strong>and</strong> repeatedpresentations) fromYear 1 for normalold controls (n=16),<strong>and</strong> from Years 1<strong>and</strong> 2 for MCI-stable(n=10; meanMMSE=28.0 at Year1) <strong>and</strong> MCI-to-ADconverters (n=16;mean MMSE=27.3at year 1). The N400is indicated on righttemporalchannels.The incongruousrepetition effect (dueto a diminishedN400 to repeatedwords) is shadedbetween 300-600ms where present.0 400 800 0 400 800 0 400 800 ms 0 400 800 0 400 800 msearly latency windows (300-500 ms) showed a distinctlyfrontal distribution. The authors attributed this frontal old/newe ffect to familiarity because of its resemblance to an eff e c tfound in a prior study. 5 5 Furthermore, patients’ source memorywas at chance, suggesting that their above-chancerecognition performance (62%) was due to a sense of familiarity(or another such implicit process) <strong>and</strong> not to recollectionof the study event. Schnyer et al 6 4 found further evidencefor deficient ERP word repetition effects in AD. Usinga continuous lexical decision task with incidental repetition atlong lags (>90 items or >7.5 minutes), Schnyer et al found arepetition positivity from 300 to 650 ms in controls, but nodiscernable effect in AD patients.A study in our laboratory 65 applied the same semanticcongruity-plus-repetition paradigm described in the previoussection 2 to patients with mild AD. As in patients withchronic amnesia, patients with mild AD had significantlyreduced P600 word-repetition effects (see Figure 1). Inaddition, patients with mild AD showed a significant diminutionof the N400 word-repetition effect. In fact, both theP600 <strong>and</strong> N400 repetition effects were “absent” in the ADgroup, in that there were no statistically significant effectsfor these potentials. The loss of the N400 repetition effectmay correspond to abnormal semantic/conceptual priming,as has been found in several behavioral studies of mildAD. 66 Furthermore, when 10th percentile (in normal elderly)cutoffs for the P600 <strong>and</strong> N400 word-repetition effectswere applied, all 11 mild AD patients were correctly classifiedas abnormal on one or both measures (sensitivity:100%; specificity: 82%), suggesting that this paradigm haspromise for use in the diagnosis or early detection of AD.N400/P600: repetition effects inMild Cognitive ImpairmentAnother study in the authors’ laboratory used the congruity-plus-repetitionparadigm to evaluate N400 <strong>and</strong> P600repetition effects in MCI. 67 In MCI, target words that followedcongruous category statements elicited a robustpositive shift in N400 amplitude relative to incongruouspairings. Analysis of the fractional area latency of this N400congruity effect showed that it was delayed in MCI relativeto controls. The N400 repetition effect, initial vs. repeatedincongruous pairings, was present but delayed in MCI. TheP600 repetition effect, initial vs. repeated congruous pairings,was not significantly different from zero in the MCIgr<strong>and</strong> average (see Figure 1). Post-hoc analyses revealedthat in MCI individuals who were subsequently diagnosedwith probable AD (n=7; “converters”), the P600 repetitioneffect was virtually absent, whereas in the MCI participantswho remained at risk (n=6; “MCI stable”) the effect waspresent but delayed relative to controls. Longitudinal ERPstudy of this cohort has shown that the N400 repetitioneffect is diminished <strong>and</strong> spatially restricted in converters atbaseline (Year 1), then absent in the group average data 1year later (Year 2; see right column in Figure 2). It is noteworthythat the P600 repetition effect at baseline could beused to discriminate MCI-to-AD converters from MCI-stablecases over the next 3 years with high accuracy (e.g.,85% or 11 of the 13 MCI participants included in Olichney14
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1et al 67 ), despite statistically indistinguishable MMSE scores(means 26.6 <strong>and</strong> 27.5 respectively).Summary: N400/P600 repetition effectsRecent work dissociating N400 <strong>and</strong> P600 repetitione ffects has found that MTL amnesics, whose ability toencode events into long term memory is compromised,show intact N400 but impaired P600 effects. This pattern offindings supports the notion that implicit <strong>and</strong> explicit retrievalprocesses are indexed by N400 <strong>and</strong> P600, respectively. InAD, both N400 <strong>and</strong> P600 repetition effects are severelydiminished. In MCI, the conjunction of reduced N400 <strong>and</strong>P600 repetition effects may be useful in identifying thoseindividuals at highest risk for subsequent conversion to A D .CONCLUSIONIntegrating across the ERP studies reviewed above,some useful generalizations can be made. The sensitivityof cognitive ERPs can be greatly increased by looking atmodulations of components, rather than expecting anabsence or near ablation of late components such as theP300, N400, <strong>and</strong> P600, all of which have multiple, distributedneural generators. Patients with a “pure” amnesticsyndrome usually have normal P300s (at least on the auditory“oddball” paradigm), but occasionally, abnormal P300shave been observed among those with more diffuse braininjuries. While memory was the only cognitive domain witha clinical deficit, the P300 abnormalities likely reflect subclinicalabnormalities in attention <strong>and</strong> working/immediatememory. Amnesic patients usually have normal N400effects, but an important exception is that of MCI “converters”with incipient AD. In contrast to the relatively normaleffects of word repetition on the N400, severe decrementsof the P600/LPC word repetition effect are present in wellcircumscribedamnesia.Patients with mild AD can usually generate reasonablysized P300 <strong>and</strong> N400 amplitudes, but quantitative analysesoften show subtle abnormalities beyond that attributableto aging. Across N400 experiments, the precise paradigmused appears to be very important <strong>and</strong> may lead todifferential sensitivity to amplitude or latency abnormalities.In mild AD, both N400 <strong>and</strong> P600 components demonstratea loss of normal word repetition effects. This suggests amore generalized failure of synaptic plasticity than inpatients with pure amnesia. Biomarkers of failed synapticplasticity should be of great value in AD, a disease thatsome leading investigators view as a primary disorder ofsynaptic function. 68,69 Studies of transgenic AD animal modelsoften find synaptic dysfunction prior to the appearanceof amyloid plaques or extensive neurofibrillary pathology.70,71 Clinico-neuropathological studies have found thatthe density of cortical presynaptic terminals is one of thestrongest predictors of dementia severity. 72ERPs may also provide a useful non-invasive tool forstaging the extent of AD pathology. In the mild to moderatestages of AD, the P300 <strong>and</strong> N400 potentials usually deterioratemarkedly, but with relative sparing of earlier sensorycomponents. 16 This is as one would predict based on thetypical staged progression of AD pathology. 73 Predilectionsites in early AD include the medial temporal lobe, otherlimbic areas, <strong>and</strong> multimodal association cortices withsparing of primary sensory areas. Unimodal associationcortex is involved in AD, but not as heavily as multimodalcortex. As more effective treatments emerge for AD, includingsome capable of reducing amyloid burden (e.g., A-βvaccination <strong>and</strong> γ-secretase inhibitors), biomarkers sensitiveto the reversal of cognitive processing deficits will be ofincreasing importance.ACKNOWLEDGMENTSSupported by National Institute on Aging (NIH grants#R01 AG18442 to J.M.O. <strong>and</strong> P50 AG05131 to J.R.T. )<strong>and</strong> the Department of Veterans A ff a i r s .REFERENCES1. Squire LR, Knowlton B, Musen G. The structure <strong>and</strong> organizationof memory. Annu Rev Psychol 1993; 44: 453-495.2. Olichney JM, Van Petten C, Paller K, Salmon DP, Iragui VJ,Kutas M. Word repetition in amnesia: electrophysiologicalmeasures of impaired <strong>and</strong> spared memory. Brain 2000; 123:1948-1963.3. Auchterlonie S, Phillips PA, Chertkow H. Behavioral <strong>and</strong>electrical brain measures of semantic priming in patientswith A l z h e i m e r’s disease: implications for access failure versusdeterioration hypotheses. Brain Cogn 2002; 48(2-3):2 6 4 - 2 6 7 .4. Donchin E, Coles MGH. Is the P300 component a manifestationof context updating? Behav Brain Sci 1988; 11 ( 3 ) :3 5 7 - 3 7 4 .5. Verleger, R. Event-related potentials <strong>and</strong> cognition: a critiqueof the context updating hypothesis <strong>and</strong> an alternative interpretationof P3. Behav Brain Sci 1988; 11: 343-356.6. Johnson R Jr. A triarchic model of P300 amplitude. Psychophysiology1986; 23(4): 367-384.7. Halgren E, Marinkovic K, Chauvel P. Generators of the latecognitive potentials in auditory <strong>and</strong> visual oddball tasks.Electroencephalogr Clin Neurophysiol 1998; 106(2): 156-164.8. Guillem F, Rougier A, Claverie B. Short- <strong>and</strong> long-delayintracranial ERP repetition effects dissociate memory systemsin the human brain. J Cogn Neurosci 1999; 11(4): 437-458.9. Yamaguchi S, Knight RT. Effects of temporal-parietal lesionson the somatosensory P3 to lower limb stimulation. ElectroencephalogrClin Neurophysiol 1992; 84(2): 139-148.15
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 110. Rugg MD, Pickles CD, Potter DD, Roberts RC. Normal P300following extensive damage to the left medial temporal lobe.J Neurol Neurosurg Psychiatry 1991; 54(3): 217-222.11. Tachibana H, Miyata Y, Takeda M, Minamoto H, Sugita M,Okita T. Auditory event-related potentials in an amnesicpatient with a left temporal lobe lesion. J Neurol Sci 1999;168(1): 52-56.12. Onofrj M, Gambi D, Fulgente T, Bazzano S, Colamartino P.Persistence of a P3 component in severe amnestic syndrome.Electroencephalogr Clin Neurophysiol 1991; 78(6):480-484.13. Potter D, Pickles C, Roberts R, Rugg M, Paller K, Mayes A .Visual <strong>and</strong> auditory P300 in a case of bilateral destruction ofthe medial temporal lobes following viral encephalitis. In:Heinze HJ, Munte T, Mangun G, (eds). Cognitive Electrophysiology:Event-related Brain Potentials in Basic <strong>and</strong>Clinical Research. Boston: Birkhauser Books; 1993: 303-311 .14. Polich J, Squire LR. P300 from amnesic patients with bilateralhippocampal lesions. Electroencephalogr Clin Neurophysiol1993; 86(6): 408-417.15. Honda M, Suwazono S, Nagamine T, Yonekura Y, ShibasakiH. P300 abnormalities in patients with selective impairmentof recent memory. J Neurol Sci 1996; 139(1): 95-105.16. Goodin DS, A m i n o ff MJ. Electrophysiological diff e r e n c e sbetween subtypes of dementia. Brain 1986; 109(6): 11 0 3 - 1113.17. Ford JM, Pfefferbaum A. Age-related changes in event-relatedpotentials. Advances Psychophysiology 1985; 1: 301-339.18. Squires KC, Chippendale TJ, Wrege KS, Goodin DS, Starr A.Electrophysiological assessment of mental function in aging<strong>and</strong> dementia. In: Poon L, (ed). Aging in the 1980s.Washington, DC: American Psychology Association; 1980:125-134.19. Gordon E, Kraiuhin C, Harris A, Meares R, Howson A. Thedifferential diagnosis of dementia using P300 latency. BiologPsychiatry 1986; 21: 1123-1132.20. Goodin DS. Clinical utility of long latency “cognitive” eventrelatedpotentials (P3): the pros. Electroencephalogr ClinNeurophysiol 1990; 76(1): 2-5.21. Pfefferbaum A, Wenegrat BG, Ford JM, Roth WT, Kopell BS.Clinical application of the P3 component of event-relatedpotentials. II: Dementia, depression <strong>and</strong> schizophrenia.Electroencephalogr Clin Neurophysiol 1984; 59(2), 104-124.22. Patterson JV, Michalewski HJ, Starr A. Latency variability ofthe components of auditory event-related potentials to infrequentstimuli in aging, Alzheimer-type dementia, <strong>and</strong>depression. Electroencephalogr Clin Neurophysiol 1988;71(6): 450-460.23. Olichney JM, Hillert DG. Clinical applications of cognitiveevent-related potentials in Alzheimer’s disease. Phys MedRehabil Clin N Am 2004; 15(1): 205-233.24. Polich J, Pitzer A. P300 <strong>and</strong> Alzheimer’s disease: Oddballtask difficulty <strong>and</strong> modality effects. Electroencephalogr ClinNeurophysiol 1999; (suppl) 50: 281-287.25. Morgan CD, Murphy C. Olfactory event-related potentials inA l z h e i m e r’s disease. J Int Neuropsychol Soc 2002; 8(6):7 5 3 - 7 6 3 .26. Tanaka F, Kachi T, Yamada T, Sobue G. Auditory <strong>and</strong> visualevent-related potentials <strong>and</strong> flash visual evoked potentials inAlzheimer’s disease: correlations with Mini-Mental StateExamination <strong>and</strong> Raven’s Coloured Progressive Matrices. JNeurol Sci 1998; 156(1): 83-88.27. Golob EJ, Johnson JK, Starr A. Auditory event-related potentialsduring target detection are abnormal in mild cognitiveimpairment. Clin Neurophysiol 2001; 113(1): 151-161.28. Frodl T, Hampel H, Juckel G, Burger K, Padberg F, Engel RR,Moller HJ, Hegerl U. Value of event-related P300 subcomponentsin the clinical diagnosis of mild cognitive impairment<strong>and</strong> Alzheimer’s Disease. Psychophysiology 2002; 39(2):175-181.29. Gironell A, Garcia-Sanchez C, Estevez-Gonzalez A, BoltesA, Kulisevsky J. Usefulness of P300 in subjective memorycomplaints: a prospective study. J Clin Neurophysiol 2005;22(4): 279-284.30. Kutas M, Hillyard SA. Reading senseless sentences: brainpotentials reflect semantic incongruity. Science 1980;207(4427): 203-205.31. Kutas M, Neville HJ, Holcomb PJ. A preliminary comparisonof the N400 response to semantic anomalies during reading,listening <strong>and</strong> signing. Electroencephalogr Clin Neurophysiol(suppl) 1987; 39: 325-330.32. McCarthy G, Nobre AC, Bentin S, et al. Language-relatedfield potentials in the anterior-medial temporal lobe: 1.Intracranial distribution <strong>and</strong> neural generators. J Neurosci1995; 15(2): 1080-1089.33. Nobre AC, Allison T, McCarthy G. Word recognition in thehuman inferior temporal lobe. Nature 1994; 372(6503):2 6 0 - 2 6 3 .34. Halgren E, Baudena P, Heit G, et al. Spatio-temporal stagesin face <strong>and</strong> word processing: depth recorded potentials in thehuman occipital <strong>and</strong> parietal lobes. J Physiol (Lond) 1994;88: 1-50.35. Kutas M, Van Petten C. Event-related brain potential studiesof language. In: Ackles PK, Jennings JR, Coles MGH, (eds),Advances in Psychophysiology, vol.3. Greenwich, CT: JAIPress; 1988: 139-187.36. Osterhout L, Holcomb PJ. Event-related potentials <strong>and</strong> languagecomprehension. In: Rugg MD, Coles MGH, (eds).Electrophysiology of Mind: Event-related Brain Potentials<strong>and</strong> Cognition. Oxford, UK: Oxford University Press; 1995:171-215.37. Monsch AU, Bondi MW, Butters N, Salmon DP, Katzman R,Thal LJ. Comparisons of verbal fluency tasks in the detectionof dementia of the Alzheimer type. Arch Neurol 1992; 49(12):1253-1258.38. Salmon DP, Butters N, Chan AS. The deterioration of semanticmemory in Alzheimer’s disease. Can J Exp Psychol 1999;53(1): 108-117.39. Chan AS, Butters N, Salmon DP: The deterioration of semanticnetworks in patients with Alzheimer’s disease: a crosssectionalstudy. Neuropsychologia 1997 35(3): 241-248.40. Ober BA, Shenaut GK. Semantic priming in Alzheimer’s disease:meta analysis <strong>and</strong> theoretical evaluation. In: Allen PA,Bashore TR, (eds). Advances in Psychology: Age Differencesin Word <strong>and</strong> Language Processing. Amsterdam: Elsevier;1995: 247-271.41. King J, Kutas M. Do the waves begin to waver? ERP studies oflanguage processing in the elderly. In: Allen PA, Bashore T R ,(eds). Advances in Psychology: Age Differences in Word <strong>and</strong>Language Processing. Amsterdam: Elsevier; 1995: 314-344.42. Kutas M, Iragui V. The N400 in a semantic categorizationtask across 6 decades. Electroencephalogr Clin Neurophysiol1998; 108: 456-471.16
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 143. Iragui V, Kutas M, Salmon DP: Event-related brain potentialsduring semantic categorization in normal aging <strong>and</strong> seniledementia of the Alzheimer’s type. Electroencephalog ClinNeurophysiol 1996; 100: 392-406.44. Hamberger MJ, Friedman D, Ritter W, Rosen J. Event-relatedpotential <strong>and</strong> behavioral correlates of semantic processingin Alzheimer’s patients <strong>and</strong> normal controls. Brain Lang1995; 48(1): 33-68.45. Ford JM, Woodward SH, Sullivan EV, Isaacks BG,Tinklenberg JR, Yesavage JA, Roth WT. N400 evidence ofabnormal responses to speech in A l z h e i m e r’s disease.Electroencephalogr Clin Neurophysiol 1996; 99(3): 235-246.46. Revonsuo A, Portin R, Juottonen K, Rinne JO. Semantic processingof spoken words in Alzheimer’s disease: an electrophysiologicalstudy. J Cogn Neurosci 1998; 10(3): 408-420.47. Schwartz TJ, Kutas M, Butters N, et al. Electrophysiologicalinsights into the nature of the semantic deficit in Alzheimer’sdisease. Neuropsychologia 1996; 34(8): 827-841.48. Ford JM, Askari N, Mathalon DH, Menon V, Gabrieli JD,Tinklenberg JR, Yesavage J. Event-related brain potentialevidence of spared knowledge in A l z h e i m e r’s disease.Psychol Aging 2001; 16(1): 161-176.49. Castañeda M, Ostrosky-Solís F, Pérez M, Bobes MA, RangelLE. ERP assessment of semantic memory in Alzheimer’s disease.Int J Psychophysiol 1997; 27(3): 201-214.50. Ostrosky-Solís F, Castañeda M, Pérez M, Castillo G, BobesMA. Cognitive brain activity in Alzheimer’s disease: electrophysiologicalresponse during picture semantic categorization.J Int Neuropsychol Soc 1998; 4(5): 415-425.51. Van Petten C, Kutas M, Kluender R, Mitchiner M, McIsaac H.Fractionating the word repetition effect with event relatedpotentials. J Cogn Neurosci 1991; 3: 131-150.52. Paller KA, Kutas M. Brain potentials during memory retrievalprovide neurophysiological support for the distinction betweenconscious recollection <strong>and</strong> priming. J Cogn Neurosci 1992; 4:3 7 5 - 3 9 1 .53. Paller KA, Kutas M, Mayes AR. Neural correlates of encodingin an incidental learning paradigm. ElectroencephalogrClin Neurophysiol 1987; 67: 360-371.54. Fern<strong>and</strong>ez G, Weyerts H, Tendolkar I, Smid HG, Scholz M,Heinze HJ. Event-related potentials of verbal encoding intoepisodic memory: dissociation between the effect of subsequentmemory performance <strong>and</strong> distinctiveness. Psychophysiology1998; 35: 709-720.55. Rugg MD, Mark RE, Walla P, Schloerscheidt AM, Birch CS,Allan K. Dissociation of the neural correlates of implicit <strong>and</strong>explicit memory. Nature 1998; 392: 595-598.56. Grunwald T, Elger CE, Lehnertz K, Van Roost D, Heinze HJ.Alterations of intrahippocampal cognitive potentials in temporallobe epilepsy. Electroencephalogr Clin Neurophysiol1995; 95(1): 53-62.57. Helmstaedter C, Grunwald T, Lehnertz K, Gleissner U, ElgerCE. Differential involvement of left temporolateral <strong>and</strong> temporomesialstructures in verbal declarative learning <strong>and</strong>memory: evidence from temporal lobe epilepsy. Brain Cogn1997; 35(1): 110-131.58. Smith ME, Halgren E. Dissociation of recognition memorycomponents following temporal lobe lesions. J Exp PsycholLearn Mem Cogn 1989; 15: 50-60.59. Mecklinger A, von Cramon DY, Matthes-von Cramon G.Event-related potential evidence for a specific recognitionmemory deficit in adult survivors of cerebral hypoxia. Brain1998; 121 (Pt 10): 1919-1935.60. Lalouschek W, Goldenberg G, Marterer A, Beisteiner R,Lindinger G, Lang W. Brain/behaviour dissociation on old/newdistinction in a patient with amnesic syndrome. ElectroencephalogrClin Neurophysiol 1997; 104(3): 222-227.61. Friedman D, Hamberger M, Stern Y, Marder K. Event-relatedpotentials (ERPs) during repetition priming in Alzheimer’spatients <strong>and</strong> young <strong>and</strong> older controls. J Clin Exp Neuropsychol1992; 14(4): 448-462.62. Rugg MD, Pearl S, Walker P, Roberts RC, Holdstock JS.Word repetition effects on event-related potentials in healthyyoung <strong>and</strong> old subjects, <strong>and</strong> in patients with Alzheimer-typedementia. Neuropsychologia 1994; 32(4): 381-398.63. Tendolkar I, Schoenfeld A, Golz G, Fern<strong>and</strong>ez G, Kuhl KP,Ferszt R, Heinze HJ. Neural correlates of recognition memorywith <strong>and</strong> without recollection in patients with A l z h e i m e r’sdisease <strong>and</strong> healthy controls. Neurosci Lett 1999; 263(1):4 5 - 4 8 .64. Schnyer DM, Allen JJ, Kaszniak AW, Forster KI. An eventrelatedpotential examination of masked <strong>and</strong> unmaskedrepetition priming in A l z h e i m e r’s disease: implications fortheories of implicit memory. Neuropsychology 1999; 13(3):3 2 3 - 3 3 7 .65. Olichney JM, Riggins BR, Morris SK, Salmon DP, Kutas M,Iragui VJ. Reduced effects of word repetition on the N400<strong>and</strong> LPC event-related potentials are common in mildAlzheimer’s disease <strong>and</strong> Mild Cognitive Impairment converters.Neurology 2002, 58 (suppl 3) A216.66. Keane M, Gabrieli J, Fennema A, et al. Evidence for a dissociationbetween perceptual <strong>and</strong> conceptual priming inAlzheimer’s disease. Behav Neurosci 1991; 105: 326-342.67. Olichney JM, Morris SK, Ochoa C, Salmon DP, Thal LJ,Kutas M, Iragui VJ. Abnormal verbal event-related potentialsin mild cognitive impairment <strong>and</strong> incipient AD. J NeurolNeurosurg Psychiatry 2002; 73: 377-384.68. Selkoe DJ. Alzheimer’s disease is a synaptic failure. Science2002 Oct 25; 298(5594): 789-791.69. Mesulam MM. Neuroplasticity failure in Alzheimer’s disease:bridging the gap between plaques <strong>and</strong> tangles. Neuron 1999;24(3): 521-529.70. Moechars D, Dewachter I, Lorent K, et al. Early phenotypicchanges in transgenic mice that overexpress diff e r e n tmutants of amyloid precursor protein in brain. J Biol Chem1999; 274(10): 6483-6492.71. Rowan MJ, Klyubin I, Cullen WK, Anwyl R. Synaptic plasticityin animal models of early Alzheimer’s disease. PhilosTrans R Soc Lond B Biol Sci 2003; 358(1432): 821-828.72. Terry RD, Masliah E, Salmon DP, Butters N, DeTeresa R, HillR, Hansen LA, Katzman R. Physical basis of cognitive alterationsin A l z h e i m e r’s disease: synapse loss is the major correlateof cognitive impairment. Ann Neurol 1991; 30(4): 572-580.73. Braak H, Braak E. Neuropathological stageing of A l z h e i m e r -related changes. Acta Neuropathol (Berl) 1991; 82(4): 239-259.17
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Visual <strong>Memory</strong> Deficits in Temporal LobeEpilepsy: Toward a Multifactorial ApproachM. VannucciKey WordsEvent-Related PotentialsHippocampus<strong>Memory</strong>Right Temporal LobeTemporal Lobe EpilepsyVisual <strong>Memory</strong>ABSTRACTTemporal lobe epilepsies (TLE) are associated withmaterial-specific memory deficits depending on the side ofseizure origin. However, while verbal memory deficits havebeen consistently reported in patients with left-sided TLE,the relationship between visual memory deficits <strong>and</strong> rightsidedTLE is more complex. Here, we review factors thatinfluence the pattern of lateralization <strong>and</strong> the nature ofvisual memory impairments in TLE <strong>and</strong> discuss the possiblerelationship between these deficits <strong>and</strong> perceptualimpairments in TLE patientsINTRODUCTIONLearning <strong>and</strong> memory impairments are the most frequentneuropsychological correlates of TLE. Thus, it maynot be surprising that recordings of event-related potentials(ERPs) from depth electrodes within the temporal lobeshave found reduced responses on the side of the epileptogenicfocus in verbal memory tasks. 1 However, up to nowit has not been possible to lateralize the functional deficitby depth ERPs when pictures were used as stimuli. 2,3These findings raise the question of whether verbal <strong>and</strong>non-verbal memory may be organized in different ways.One of the most influential <strong>and</strong> debated neuropsychologicalmodels of memory in TLE is the material-specificmemory model, originally proposed by Milner, Kimura <strong>and</strong>their co-workers. 4-6 This model differentiated between verbal<strong>and</strong> non-verbal memory <strong>and</strong> suggested for the first timethat the left temporal lobe supports memory for verbalmaterial while the right temporal lobe participates in nonverballearning <strong>and</strong> memory. This model has been veryinfluential during the last 30 years. Extensive research hasconfirmed its predictions concerning verbal memory,demonstrating both pre- <strong>and</strong> post-operative verbal memorydeficits in patients with left-sided TLE. However, conflictingresults of studies on visual memory have contradictedthe original model indicating a more complex relationshipbetween visual memory processes <strong>and</strong> the right temporallobe (for a review see 7,8 ). Recent studies suggest a multifactorialmodel of visual memory in which the nature of thedeficits <strong>and</strong> their lateralization depend on specific memorysubprocesses (tasks), the particular temporal lobe regionsinvolved (structures), <strong>and</strong> subject characteristics likeseizure-history, language dominance, <strong>and</strong> sex (subjectsvariables). Moreover, evidence from many studies suggeststhat non-verbal memory is not a unitary construct butthat visual <strong>and</strong> spatial memory are different subsystemsboth functionally <strong>and</strong> in terms of their neural bases. Here,we will focus on visual memory, i.e. memory for the structure<strong>and</strong> shape of complex visual patterns, in contrast tospatial memory, which refers to the spatial position of complexpatterns (objects) in an array of discrete stimuli. 9 Indoing so, we will concentrate on memory impairments inpre- or non-surgical TLE, <strong>and</strong> we will refer to post-surgicalpatients only briefly (for a review on post-operative effectsof right anterior temporal lobectomy see 8,10 ).The Original “Material-specific <strong>Memory</strong>” ModelMilner, Kimura <strong>and</strong> their co-workers developed the“material-specific memory” model at the MontrealNeurological Institute from their studies of cognitive effectsof unilateral temporal lobectomy performed in TLE patientsto control their medically intractable seizures. These studiesconsistently revealed material-specific memory deficitsrelated to the side of the resection: Left temporal lobe surgeryselectively impaired memory for verbal material 4,11while contralateral resections resulted in impaired learning<strong>and</strong> memory for non-verbal visual <strong>and</strong> auditory patternsthat could not be easily verbalized. Deficits were found intasks of learning <strong>and</strong> recall of complex visual patterns <strong>and</strong>abstract designs, maze learning, block tapping task <strong>and</strong>face recognition. 6,12-14 In particular, Kimura found visuallearning deficits using a visual learning task in which non-M. Vannucci is from the Department of Psychology, University ofFlorence, Italy, <strong>and</strong> the Department of Epileptology, Bonn UniversityMedical Center, Germany.Address requests for reprints to Dr. Manila Vannucci, PhD, AssistantProfessor, Department of Psychology, Via S.Niccolò 93, 50125 Firenze,Italy.Email: manila.vannucci@psico.unifi.it18
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1sense figures were repeatedly presented among othernon-recurring designs. 6 In this task, right temporal lobectomypatients showed marked difficulties in learning to distinguishbetween recurrent <strong>and</strong> non-recurrent nonsense patterns.Lateralized material-specific memory deficits werealso found in pre- or non-surgical TLE patients, eventhough in this group the pattern of double-dissociation wasless striking. 14These results had strong implications for clinical neuropsychologicalstudies aiming to lateralize or even localizethe epileptogenic focus, <strong>and</strong> many experiments wereperformed to replicate <strong>and</strong> further investigate this model.H o w e v e r, while it proved to be successful <strong>and</strong> reliable forverbal memory, the original findings were not always replicatedfor visual memory for which conflicting results werereported: Some studies, mainly with post-operative T L Epatients, confirmed the right temporal lobe superiority forvisual memory, but many others failed to find it. Over thelast 30 years, several studies have tried to identify factorsthat may explain these inconsistencies thus elaboratingthe original model. Especially, some variables concerningmaterials <strong>and</strong> tasks, different temporal lobe substructuresinvolved in memory processes, <strong>and</strong> patient characteristicswere found to influence the pattern of lateralization forvisual memory.Toward a Multifactorial ModelMultiple visual memory processesThe coarse distinction between verbal <strong>and</strong> visual memorymay not suffice to explain visual memory deficits inTLE. In fact, these may be caused by impairments of differentsubprocesses like encoding/learning, consolidation, orretrieval. Converging evidence indicates that these subprocessesthemselves may be lateralized differentially.Depending on the tasks used <strong>and</strong> the specific aspects ofvisual memory that these tasks tapped, different patternsof lateralization have been found. According to Barr, 7 thesetasks can be grouped into two main classes: Figural reproductiontests <strong>and</strong> figural learning tests.Both scientific experiments <strong>and</strong> routine clinical studiesperformed in epilepsy centers usually apply figural reproductiontests. These comprise a copy or immediate reproductionof some visual pictures followed by a seconddelayed reproduction, as in the Rey Osterrieth ComplexFigure (ROCF), Benton Visual Retention test (BVRT ) ,Visual Reproduction subtest from the Wechsler <strong>Memory</strong>Scale (WMS-VR) <strong>and</strong> from the Wechsler <strong>Memory</strong> Scale-Revised (VR-WMS-R), the Family Pictures <strong>and</strong> the supplementaltest of visual reproduction from the most recentWechsler <strong>Memory</strong> Scale Third Edition (WMS-III). By contrast,figural learning tests include a learning phase, inwhich a supraspan set of visual stimuli is to be recognisedor recalled over repeated trials, <strong>and</strong> a subsequent delayed(after 30-40 minutes) recognition or recall phase. Most frequentlyused are the abstract design list (ADL) learning <strong>and</strong>recall paradigm introduced by Jones-Gotman 15 <strong>and</strong> st<strong>and</strong>ardizedtests as the revised versions of the Diagnosticumfür Cerebralschädigungen (DCS-R; revised diagnostic testsfor cerebral lesions), the Rey’s Visual Design Test (RV D T ),<strong>and</strong> the Visual-Spatial Learning Test (VSLT ).Compared to figural reproduction tests, visual learning<strong>and</strong> memory tasks appear to be more sensitive to effectsof right temporal lobe lesions, especially with respect todelayed retention, in both post-operative 16-18 <strong>and</strong> pre-operativepatients 19-23 (but see 24 ). In one of the first studies,Helmstaedter et al 19 found impaired immediate recall,learning capacity <strong>and</strong> mean visual learning performance inpre-surgical patients with right as compared to left TLE.Similarly, Jones-Gotman et al 18 found that right temporallobectomy patients were impaired in visual learning, ascompared to controls, while no significant differencesbetween the groups were found in the retention (delayedrecall) of visual information.By contrast, less consistent <strong>and</strong> mostly negative resultson laterality effects have been found in studies using figuralreproduction tests: Only few studies reported significantd i fferences in the delayed reproduction performance ofROCF <strong>and</strong> VR-WMS-R between both pre- <strong>and</strong> post-surgicalpatients with right or left TLE (e.g. 25 - 27 ). Other studies didnot find any deficits in figural reproduction in right (or left)T L E . 28 - 30 R e c e n t l y, Barr et al 31 also reported negative findingsin a multicenter study with 757 epilepsy surgery c<strong>and</strong>idatesfrom 8 epilepsy centers, in which both ROCF <strong>and</strong> VR-WMS were applied. The few studies that examined the visualmemory subtests of the most recent Wechsler <strong>Memory</strong>Scale, III Edition reported conflicting findings. 32 , 33According to Barr, the lack of laterality effects reportedin most studies using figural reproduction tests may, atleast in part, be due to some confounding variables. 31Visual stimuli of some figural reproduction tests can easilybe encoded verbally (e.g., stimuli of VS-WMS-R, FamilyPictures of WMS-III), thus making compensatory verbalizationstrategies possible <strong>and</strong> therefore questioning the exactnature of the memory processes measured by the task.Moreover, reproduction requires intact motor <strong>and</strong> higherlevelconstructional abilities, so that impairments in eitherof these functions could confound the results.Unfortunately, not all studies on visual memory have controlledfor these functions.Although at present researchers <strong>and</strong> clinicians are stillsearching for “psychometrically sound <strong>and</strong> clinically usefulmeasures that are sensitive to material specific deficits,particularly visual memory processing,” 34 these studiesindicate some of the requirements that a test should haveto assess memory functions associated with the right temporallobe: It should include a learning phase in addition toan immediate <strong>and</strong> delayed recall or recognition phase, <strong>and</strong>it should be carefully constructed to avoid effects of confoundingvariables. Unfortunately, many clinical tests used19
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1in TLE patients do not respect these criteria <strong>and</strong> only fewcenters use figural learning tests as part of their routineneuropsychological assessment battery, 35even thoughsome efforts have been made over the recent years tobridge the long-st<strong>and</strong>ing gaps between research <strong>and</strong> clinicalwork. 36 In particular, in two recent studies, two new (ormodified) versions of visuo-spatial supraspan learningtests, including a learning phase <strong>and</strong> a delayed retrieval,have been performed with TLE patients: The modified versionof DCS (mDCS; 22 ) <strong>and</strong> the Biber Figure Learning Test-Extended (BFLT-E; 23 ). Both were compared with st<strong>and</strong>ardfigural reproduction tests <strong>and</strong> demonstrated the clinical utilityof learning tests in discriminating between right <strong>and</strong> leftTLE <strong>and</strong> their superiority to figural reproduction tests.Multiple temporal lobe structuresApart from the lateralization of visual memory, studiesin TLE patients have also addressed the question of whereexactly these processes are localized. The temporal lobesinclude different neo-cortical <strong>and</strong> medial temporal regions,<strong>and</strong> TLE can be caused by different pathologies affectingselectively one or more of these structures. Since Milner’s 4pioneering study of amnesic patients the hippocampus hasbeen suggested to play a crucial role in declarative episodicmemory, <strong>and</strong> the hippocampus has become the maintarget of research into the neural basis of visual memoryimpairments in TLE.Historically, the first approach to study hippocampalinvolvement in visual memory was to compare visual memoryperformance of different groups of unilateral temporallobectomy patients, classified according to the side <strong>and</strong>extent of surgery. These comparisons revealed a significantpositive association between the severity of visualmemory impairment <strong>and</strong> the extent of right hippocampalresection. 13,15 With the development of more tailored surgicalprocedures like the selective amygdalo-hippocampectomy(SAH) sparing the temporal neo-cortex, or the neocorticectomy(NCE) sparing both amygdala <strong>and</strong> hippocampus,it has been possible to better investigate the relativecontributions of medial <strong>and</strong> neo-cortical temporal structuresto visual memory. In these studies conflicting resultswere found: Some studies reported a more pronouncedimpairment in visuo-spatial learning <strong>and</strong> memory after rightanterior temporal lobectomy than after right SAH, 37,38 thussuggesting an additional contribution of neo-cortical structuresto visual memory processes, but others did not. 18,39 Inparticular, Jones-Gotman et al 18 found a similar pattern ofvisual learning impairments in patients who underwentright-sided ATL, SAH, or NCE, which suggested that theintegrity of the whole circuit is the essential factor for normallearning, storage <strong>and</strong> retrieval of visual information.Over the last decades a more direct approach to studythe role of the hippocampus has become possible byinvestigating the specific effects of hippocampal sclerosison pre- <strong>and</strong> post-operative memory functions. To identifyhippocampal functions the behavioral performance of unilateralTLE patients with hippocampal sclerosis has beencompared with the performance of TLE patients withouthippocampal sclerosis. 10,17,40-42 These studies consistentlyreported poorer performance in visual memory tasks inpatients with hippocampal sclerosis compared to patientswith extramesial pathology. Moreover, a different pattern oflateralization has been found depending on the tasks: Nosignificant differences between patients with left <strong>and</strong> righthippocampal sclerosis were found with figural reproductiontests, 40,41 while a poorer performance in visual learningtasks was reported in patients with right as compared to lefthippocampal sclerosis. 17H o w e v e r, since the severity of hippocampal atrophy <strong>and</strong>sclerosis may vary one may ask whether visual memoryimpairments are related to the severity of pathology.Histopathological cell-counts <strong>and</strong> the development of moresophisticated non-invasive quantitative MRI techniques (hippocampalvolumetry <strong>and</strong> T2 relaxation time measurement)have made it possible to use more accurate measures of thestructural integrity <strong>and</strong> extent of hippocampal pathology inTLE <strong>and</strong> to relate these structural measures to behavioralperformance in memory tasks (e.g. 43 ). Nevertheless, moststudies failed to find any correlations between pre-surgicalvisual memory performance <strong>and</strong> cell counts in the right hippo c a m p u s 44 , 45or right hippocampal volume measureme n t s . 46 - 52 Only in one of the cell-count studies a correlationbetween cell density of CA4 in right TLE <strong>and</strong> performance atB V RT was found. 53 Using MRI, Trenerry et al 48 found presurgicalright hippocampal volumes to be correlated withpost- but not pre-operative visual memory performance,whereas Baxendale et al 49found right hippocampal MRImeasures to correlate with visual learning <strong>and</strong> delayedrecall. However, this relationship depended on the interactionof demographic <strong>and</strong> epilepsy-related variables.Most MRI studies have concentrated on the hippocampus.Only two recent studies extended volume measurementsto extrahippocampal structures like amygdala,mammillary body <strong>and</strong> fornix <strong>and</strong> found a significant correlationbetween right amygdala volume <strong>and</strong> performance invisual memory tasks. 50,51 In sum, these studies suggestedfor a role of the hippocampus in visual memory processes<strong>and</strong> specify the original material-specific memory model byhighlighting the role of the right hippocampus as source ofthe right temporal superiority in visual learning processes.However, the hippocampal measures described so far arestructural parameters. Further insight into hippocampal<strong>and</strong> extrahippocampal contributions to visual memoryimpairments may be made possible by functional (e.g.,fMRI) measures. These techniques allow the observationof medial temporal lobe structures in action both during distinctvisual memory processes as encoding <strong>and</strong> retrieval<strong>and</strong> during distinct phases like learning <strong>and</strong> delayed recallor recognition. fMRI is currently being used to study the20
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1neural basis of “normal” memory functioning but there areonly few fMRI studies in TLE patients. Moreover, up to nowno study has compared the activity of hippocampal <strong>and</strong>extrahippocampal structures during different memory subprocessesin TLE patients with visual memory deficits.Multiple subject variablesAs Baxendale et al 49have shown, demographic <strong>and</strong>epilepsy-related factors interact with the extent <strong>and</strong> lateralityof hippocampal pathology in shaping visual memory performance.In particular, the authors found that poor visuallearning was associated with hippocampal atrophy in olderpatients. Older age at the time of testing, long duration ofepilepsy <strong>and</strong> smaller right hippocampal volume were associatedwith poorer delayed recall in a figure recall task.Recently it has been suggested that the pattern of lateralizationfor visual memory is affected by subject characteristicslike seizure-history variables (age of onset, duration ofepilepsy <strong>and</strong> seizure frequency), language dominance <strong>and</strong>sex diff e r e n c e s . 54 - 59Among seizure-history variables, theage of onset may have the strongest influence. Since thereis evidence that normal lateralization of cognitive functionsis defined by age 5, 60 an early onset of epilepsy before theage of 5 years may be expected to modify <strong>and</strong> to interferewith the normal functional organization of the brain.Lespinet et al 54 studied the effects of age of onset onverbal <strong>and</strong> visual memory in pre-operative right <strong>and</strong> leftLTLE patients. They found that an early onset of seizuresbefore the age of 5 years was more strongly associatedwith reduced recall performance in the Rey OsterriethComplex Figure test than with other measures of verbalmemory. Thus visual memory may be more sensitive to theage of onset than verbal memory. Moreover, the age ofonset affected the material-specific pattern of lateralization:An early onset, of either right or left TLE, was associatedwith both verbal <strong>and</strong> visual impairments, while a late onsetwas associated with lateralized material-specific memorydeficits depending on the site of the lesion.Two further subject variables have recently been foundto affect the pattern of memory lateralization: Hemisphericlanguage dominance <strong>and</strong> sex differences. It is widelyaccepted that hemispheric language dominance is animportant variable affecting hemispheric specialization indifferent cognitive functions. However, in several studieson memory functions in TLE the pattern of hemispheric languagedominance was not taken into account, <strong>and</strong> only fewstudies directly addressed the question of whether a differentpattern of language dominance was associated with adifferent pattern of material-specific memory functions.Some of these studies found no lateralization of eitherverbal or visuo-spatial memory in patients with atypical languagedominance (right or “non-left”. 55,56 ) Some, however,found an inverse pattern of memory deficits 20,57 : In patientswith left-sided TLE <strong>and</strong> atypical hemispheric languagedominance, verbal memory was preserved while visualmemory was extremely impaired — more than in patientswith left-sided TLE <strong>and</strong> left hemispheric language dominance,<strong>and</strong> even more than in patients with right-sided TLE<strong>and</strong> left hemispheric language dominance. This atypicalpattern of visual memory impairments in left-sided TLE hasbeen explained in terms of a “crowding phenomenon”:When both verbal <strong>and</strong> visual information are to beprocessed in the right hemisphere competition for space orthe incompatibility between different ways of informationprocessing results in the suppression of right hemisphericfunctions, including visual memory.Several studies suggest that the female brain is moreplastic <strong>and</strong> less lateralized with respect to language functions.61-63 Are material-specific memory impairments thereforeless lateralized in women (as compared to men)? Thisquestion has been addressed in a study by Helmstaedteret al 58 (see also 59 ) in which verbal <strong>and</strong> visual memory wereassessed in male <strong>and</strong> female left TLE patients who allunderwent both a left <strong>and</strong> right intracarotidal amobarbytaltest (“Wada-test”) to evaluate cerebral language dominance<strong>and</strong> left- <strong>and</strong> right-hemispheric contributions tomemory processes. The authors found sex differences infigural learning <strong>and</strong> memory of left TLE-patients, withwomen showing the poorest performance. Moreover, in leftTLE in patients with atypical language dominance, womenshowed a greater capacity of the healthy right temporallobe to compensate for verbal memory deficits than men,resulting a impaired figural memory. This suggests a morepronounced “crowding effect” due to the greater plasticityof the right temporal lobe in women related to the greaterinterhemispheric plasticity for language.Visual memory <strong>and</strong> visual object processingIn her original studies Milner 4 , 5 found non-verbal memorydeficits in TLE patients after right temporal lobectomies.However, she also found perceptual impairmentsin experiments in which the normal redundancy of visualstimuli was reduced (e.g., by a short presentation) <strong>and</strong> intasks requiring the discrimination of small differences inthe contours of abstract complex objects. This suggestedthat the right temporal lobe may also “aid in rapid visualidentification.” These findings were replicated by Kimura 6who found that both pre- <strong>and</strong> post-operative right T L Epatients were impaired in two tachistoscopic tests of perceptualprocessing: Perception of overlapping nonsenseobjects (complex patterned figures) <strong>and</strong> of groups of dots.H o w e v e r, patients were unimpaired in perceptual testswith verbalizable material (letters <strong>and</strong> familiar visualobjects). Perceptual impairments were slight <strong>and</strong> less pronouncedthan memory deficits <strong>and</strong> could only be revealedby perceptual dem<strong>and</strong>ing tasks. Nevertheless, these findingsraise the questions of whether the same temporallobe structures may subserve both visual perceptual <strong>and</strong>memory processes <strong>and</strong> whether deficits in visual processingin TLE patients may contribute to visual memory21
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Figure 1.Gr<strong>and</strong> averages of hippocampal response in the non-focal (A)<strong>and</strong> focal temporal lobe (B). Solid line: nonsense objects;dashed line: real objects.impairments. In fact, functional brain imaging studies withhealthy subjects have recently shown that medial temporallobe structures are not only involved in episodic memoryformation but also in visual object processing: T h e yare active during tasks requiring the processing of complexvisual stimuli without any explicit learning <strong>and</strong> memorydem<strong>and</strong>s. 6 4 - 6 6Neuropsychological research into temporal lobe epilepsyhas still not addressed visual processing, <strong>and</strong> clinicalneuropsychological assessments of TLE patients usuallypay little attention to perceptual processes in comparison toother higher cognitive functions. Therefore, we performed astudy asking whether the hippocampus contributes to theprocessing of visual objects <strong>and</strong> whether the epileptogenicprocess affects the processing of figurative material. 6 7In 12 unilateral TLE patients, we recorded limbic ERPsinvasively from within the hippocampus proper referencedagainst extracranially linked mastoids. Using a visualobject decision task we asked our patients to distinguishpictures of real objects from those of nonsense objects. Asshown in Figure 1, non-epileptic hippocampus differentiatedreliably between nonsense <strong>and</strong> real objects <strong>and</strong>responded differentially to both kinds of stimuli, startingfrom around 200 ms after stimulus onset. A negative potentialpeaking around 350 ms was significantly higher inamplitude in response to nonsense objects than whenelicited by pictures of real objects. Moreover, whileresponses to nonsense stimuli were characterized by aslow negative component from 500 to 900 ms, real objectselicited a high amplitude positivity peaking around 650 ms.By contrast, the limbic ERPs generated within the epileptichippocampus did not differentiate between the two classesof complex visual stimuli: Hippocampal responses to nonsenseobjects were reduced within the epileptic temporallobe, thus eliminating the specific effect of meaning of visualstimuli found on the non-focal side. These findings suggestthat the hippocampus participates in the semantic processingof complex visual objects <strong>and</strong> show that an epileptogenicfocus within the medial temporal lobe does interferewith the neural processing of figurative material.Future studies are necessary to investigate further the neuropsychologicalcorrelates of this pattern of response <strong>and</strong>,in particular, to verify whether this pattern of response isrelated to visual memory impairments.CONCLUSIONThe relationship between visual memory <strong>and</strong> right temporallobe is more complex than hypothesized in the originalmaterial-specific memory model. The specific pattern oflateralization for visual memory depends on multiple interactingvariables including memory subprocesses, temporallobe structures <strong>and</strong> subject characteristics. At presentthere is no unitary model of visual memory impairment inTLE, <strong>and</strong> the relationship between visual memory deficits<strong>and</strong> perceptual impairments in TLE patients is still unclear.Future studies combining basic <strong>and</strong> clinical research arenecessary to enhance our knowledge on memory impairments<strong>and</strong> “normal” visual memory functioning.REFERENCES1. Grunwald T, Kurthen M, Elger CE. Event-related potentials intemporal lobe epilepsy. In: Lüders HO, (ed). Epilepsy Surgery.Philadelphia: Lippincott Raven Publishers; 2001: 513-519.2. Puce A, Andrewes DG, Berkovic SF, Bladin PF. Visual recognitionmemory. Neurophysiological evidence for the role ofwhite matter in man. Brain 1991; 114: 1647-1666.3. Guillem F, N’Kaoua B, Rougier A, Claverie B. Effects of temporalversus temporal plus extra-temporal lobe epilepsies onhippocampal ERPs: physiopathological implications forrecognition memory studies in humans. Brain Res CognBrain Res 1995; 2: 147-153.4. Milner B. Psychological defects produced by temporal lobeexcision. Res Publ Assoc Res Nerv Ment Dis 1958; 36: 244-257.5. Milner B Visual recognition <strong>and</strong> recall after right temporalexcision in man. Neuropsychologia 1968; 6: 191-209.6. Kimura D. Right temporal lobe damage. Arch Neurol 1963; 8:48-55.7. Barr WB. Examining the right temporal lobe’s role in nonverbalmemory. Brain Cogn 1997; 35: 26-41.8. McDermid Vaz S. Nonverbal memory functioning followingright anterior temporal lobectomy: a meta-analytic review.Seizure 2004; 13: 446-452.9. Abrahams S, Pickering A, Polkey C E, Morris R G. Spatialmemory deficits in patients with unilateral damage to theright hippocampal formation. Neuropsychologia 1998; 35:11 - 2 4 .22
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 110. Gleissner U, Helmstaedter C, Elger CE. Right hippocampalcontribution to visual memory: a presurgical <strong>and</strong> postsurgicalstudy in patients with temporal lobe epilepsy. J NeurolNeurosurg Psychiat 1998; 65: 665-669.11. Meyer E Y, Yates A H J. Intellectual changes following temporallobectomy for psychomotor epilepsy. J. Neurol NeurosurgPsychiat 1955; 18: 44-52.12. Milner B. Visually-guided maze learning in man: effects ofbilateral hippocampal, bilateral frontal, <strong>and</strong> unilateral cerebrallesions. Neuropsychologia 1965; 3: 317-338.13. Milner B. Visual recognition <strong>and</strong> recall after right temporalexcision in man. Neuropsychologia 1968; 6: 191-209.14. Milner B. Interhemispheric differences in the localization of psychologicalprocesses in man. Br Med Bull 1971; 27: 272-277.15. Jones-Gotman M. <strong>Memory</strong> for designs: the hippocampalcontribution. Neuropsychologia 1986a; 24: 193-203.16. Jones-Gotman M. Right hippocampal excision impairs learning<strong>and</strong> recall of a list of abstract designs. Neuropsychologia1986b; 24: 659-670.17. Jones-Gotman M. Psychological evaluation for epilepsys u r g e r y. In: Shorvon S, Dreifuss F, Fish D, Thomas D (eds).The Treatment of Epilepsy. Oxford: Blackwell Science;1996: 621-630.18. Jones-Gotman M, Zatorre RJ, Olivier A, Andermann F,Cendes F, Staunton H, et al. Learning <strong>and</strong> retention of words<strong>and</strong> designs following excision from medial or lateral temporal-lobestructures. Neuropsychologia 1997; 5: 963-973.19. Helmstaedter C, Pohl C, Hufnagel A, Elger C.E. Visual learningdeficits in nonresected patients with right temporal lobeepilepsy. Cortex 1991; 27: 547-555.20. Helmstaedter C, Kurthen M, Linke DB, Elger CE. Right hemisphererestitution of language <strong>and</strong> memory functions in righthemisphere language-dominant patients with left temporallobe epilepsy. Brain 1994; 117: 729-737.21. Giovagnoli AR, Casazza M, Avanzini G. Visual learning on aselective reminding procedure <strong>and</strong> delayed recall in patientswith temporal lobe epilepsy. Epilepsia 1995; 36: 704-711.22. Dige N, Wik G. A visual learning <strong>and</strong> memory test for preoperativeevaluation of patients with temporal lobe epilepsy. IntJ Neurosci 2001; 111: 167-174.23. Glosser G, Saykin A J, Deutsch K, O’Connor M J, Sperling MR. Neural organization of material specific memory functionsin temporal lobe epilepsy patients as assessed by intracaroticamobarbital test. Neuropsychology 1995; 9: 449-456.24. Lee GP, Loring DW, Thompson JL. Construct validity of material-specificmemory measures following unilateral temporallobe ablations. Psych Assessment 1989; 1: 192-197.25. Fedio P, Mirsky, AF. Selective intellectual deficits in childrenwith temporal lobe or centrencephalic epilepsy. Neuropsychologia1969; 7: 287-300.26. Taylor, LB. Localisation of cerebral lesions by psychologicaltesting. Clin Neurosurg 1969; 16: 269-287.27. Delaney RC, Rosen AJ, Mattson RH, Novelly RA. <strong>Memory</strong>function in focal epilepsy: a comparison of non-surgical, unilateraltemporal lobe <strong>and</strong> frontal lobe samples. Cortex 1980;16: 103-117.28. Mayeux R, Br<strong>and</strong>t J, Rosen J, Benson DF. Interictal memory<strong>and</strong> language impairment in temporal lobe epilepsy.Neurology 1980; 30: 120-125.29. Novelly RA, Augustine EA, Mattson RH, Glaser GH,Williamson PD, Spencer DD, Spencer SS. Selective memoryimprovement <strong>and</strong> impairment in temporal lobectomy forepilepsy. Ann Neurol 1984; 15: 64-67.30. Chelune GJ, Naugle RI, Luders H, Awad IA. Prediction ofcognitive change as a function of preoperative ability statusamong temporal lobectomy patients seen at 6-month followup.Neurology 1991; 41: 399-404.31. Barr WB, Chelune GJ, Hermann BP, Loring DW, Perrine K,Strauss E, et al. The use of figural reproduction tests asmeasures of nonverbal memory in epilepsy. J IntNeuropsychol Soc 1997; 3: 435-443.32. Wilde N, Strauss E, Chelune GJ, Loring DW, Martin RC,Hermann BP, et al. WMS-III performance in patients with temporallobe epilepsy: group differences <strong>and</strong> individual classification.J Int Neuropsychol Soc 2001; 7: 881-891.33. Lacritz LH, Barnard HD, Van Ness P, Agostini M, Diaz-Arrastia R, Cullum CM. Qualitative analysis of WMS-IIILogical <strong>Memory</strong> <strong>and</strong> Visual Reproduction in temporal lobeepilepsy. J Clin Exp Neuropsychol 2004; 26: 521-530.34. Doss RC, Chelune G, Naugle RI. WSM-III performance inepilepsy patients following temporal lobectomy. J IntNeuropsychol Soc 2004; 10: 173-179.35. Camara WJ, Nathan J, Puente AE. Psychological test usage:implications for professional psychology. ProfessionalPsychol Res Pract 2000; 31: 141-154.36. Barr W, Morrison C, Zaroff C, Devinsky O. Use of the BriefVisuospatial <strong>Memory</strong> Test-Revised (BVMT-R) in neuropsychologicalevaluation of epilepsy surgery c<strong>and</strong>idates.Epilepsy Behav 2004; 5: 175-179.37. Wieser HG, Yasargil MG. Selective amygdalohippocampectomyas a surgical treatment of mesiobasal limbic epilepsy.Surgical Neurol 1982; 17: 445-457.38. Goldstein LH, Polkey CE. Everyday memory after unilateraltemporal lobectomy or amygdalo-hippocampectomy. Cortex1992; 28: 189-201.39. Goldstein LH, Polkey CE. Short-term cognitive changes afterunilateral temporal lobectomy or unilateral amygdalo-hippocampectomyfor the relief of temporal lobe epilepsy. JNeurol Neurosurg Psychiat 1993; 56: 135-140.40. Miller LA, Munoz DG, Finmore M. Hippocampal sclerosis <strong>and</strong>human memory. Arch Neurol 1993; 50: 391-394.41. Hermann BP, Seidenberg M, Schoenfeld J, Davies K.Neuropsychological characteristics of the syndrome of mesialtemporal lobe epilepsy. Arch Neurol 1997; 54: 369-376.42. Guerreiro C, Cendes F, Li LM, Jones-Gotman M, AndermannF, Dubeau F, et al. Clinical patterns of patients with temporallobe epilepsy <strong>and</strong> pure amygdalar atrophy. Epilepsia 1999;40: 453-461.43. Baxendale SA. The hippocampus: functional <strong>and</strong> structuralcorrelations. Seizure 1995; 4: 105-117.44. Sass KJ, Sass A, Westerveld M. Russell’s adaptation of theWechsler <strong>Memory</strong> Scale as an index of hippocampal pathology.J Epil 1992; 5: 24-30.45. Rausch R, Babb TL. Hippocampal neuron loss <strong>and</strong> memoryscores before <strong>and</strong> after temporal lobe surgery for epilepsy.Arch Neurol 1993; 50: 812-817.46. Lencz T, McCarthy G, Bronen RA, Scott TM, Inserni JA, SassKJ, et al. Quantitative magnetic resonance imaging in temporallobe epilepsy: relationship to neuropathology <strong>and</strong> neuropsychologicalfunction. Ann Neurol 1992; 31: 629-637.23
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 147. Loring DW, Murro AM, Meador KJ, Lee GP, Gratton CA,Nichols ME, et al. Wada memory testing <strong>and</strong> hippocampalvolume measurements in the evaluation for temporal lobectomy.Neurology 1993; 43: 1789-1793.48. Trenerry MR, Jack CR Jr, Ivnik RJ, Sharbrough FW, CascinoGD, Hirschorn KA, et al. MRI hippocampal volumes <strong>and</strong>memory function before <strong>and</strong> after temporal lobectomy.Neurology 1993; 43: 1800-1805.49. Baxendale SA, van Paesschen W, Thompson PJ, ConnellyA, Duncan JS, Harkness WF, Shorvon S.D. The relationshipbetween quantitative MRI <strong>and</strong> neuropsychological functioningin temporal lobe epilepsy. Epilepsia 1998; 39: 158-166.50. Martin RC, Hugg WJ, Roth DL, Bilir E, Gilliam FG, Faught E,Kuzniecky RI. MRI extrahippocampal volumes <strong>and</strong> visualmemory: correlations independent of MRI hippocampal volumesin temporal lobe epilepsy patients. J Int NeuropsycholSoc 1999; 5: 540-548.51. Pegna AJ, Caldara-Schnetzer AS, Perrig SH, Lazeyras F,Khateb A, Mayer E, et al. Is the right amygdala involved invisuospatial memory? Evidence from MRI volumetric measures.Eur Neurol 2002; 47: 148-155.52. Griffith HR, Pyzalski RW, O’Leary D, Magnotta V, Bell B, DowC, Hermann B, Seidenberg M.A. Controlled quantitative MRIvolumetric investigation of hippocampal contributions toimmediate <strong>and</strong> delayed memory performance. J Clin ExpNeuropsychol 2003; 25: 1117-1127.53. Matkovitch S, Oxbury M, Hiorns JH. Hippocampal neuronaldensity correlates with preoperative verbal memory inpatients with temporal lobe epilepsy. Epilepsia 1995; 36 (S3):1 2 1 .54. Lespinet V, Bresson C, N’Kaoua B, Rougier A, Claverie B.Effect of age of onset of temporal lobe epilepsy on the severity<strong>and</strong> the nature of preoperative memory deficits. Neuropsychologia2002; 40: 1591-1600.55. Glosser G, Saykin AJ, Deutsch GK, O’Connor MJ, SperlingMR. Neural organization of material-specific memory functionsin temporal lobe epilepsy patients as assessed by intracarotidamobarbital test. Neuropsychology 1995; 9: 449-456.56. Kim H, Sangdoe Y, Eun IS, Jieun K. Material-specific memoryin temporal lobe epilepsy: effects of seizure laterality <strong>and</strong>language dominance. Neuropsychology 2003; 17: 59-68.57. Strauss E, Satz P, Wada J. An examination of the crowdinghypothesis in epileptic patients who have undergone thecarotid amytal test. Neuropsychologia 1990; 28: 1221-1227.58. Helmstaedter C, Kurthen M, Elger C E. Sex differences inmaterial-specific cognitive functions related to languagedominance: an intracarotid amobarbital study in left temporallobe epilepsy. Laterality 1999; 4: 51-63.59. Helmstaedter C, Brosch T, Kurthen M, Elger CE. The impactof sex <strong>and</strong> language dominance on material-specific memorybefore <strong>and</strong> after left temporal lobe surgery. Brain 2004;127: 1518-1525.60. Iaccino JF. Are there developmental differences in brain lateralization?In: Left brain-right brain differences: Inquiries,evidence, <strong>and</strong> new approaches. Hillsdale, New Jersey:Lawrence Erlbaum Assoc Publ; 1993: 183-203.61. Shaywitz BA, Shaywitz SE, Pugh KR, Constable RT,Skudlarski P, Fulbright RK, et al. Sex differences in the functionalorganization of the brain for language. Nature 1995;373: 607-60962. Kansaku K, Yamaura A, Kitazawa S. Sex differences in lateralizationrevealed in the posterior language areas. CerebCortex 2000; 10: 866-872.63. Fern<strong>and</strong>ez G, Weis S, Stoffel-Wagner B, Tendolkar I, ReuberM, Beyenburg S, et al. Menstrual cycle-dependent neuralplasticity in the adult human brain is hormone, task, <strong>and</strong>region specific. J Neurosci 2003; 23: 3790-3795.64. Martin A, Wiggs C.L, Weisberg J. Modulation of human medialtemporal lobe activity by form, meaning <strong>and</strong> experience.Hippocampus 1997; 7: 587-593.65. Martin A. Automatic activation of the medial temporal lobeduring encoding: lateralized influences of meaning <strong>and</strong> novelty.Hippocampus 1999; 9: 62-70.66. Vuilleumier P, Henson, RN, Driver J, Dolan R.J. Multiple levelsof visual object constancy revealed by event-related fMRIof repetition priming. Nat Neurosci 2002; 5: 491-499.67. Vannucci M, Dietl T, Pezer N, Viggiano MP, Helmstaedter C,Schaller C, Elger CE, Grunwald T. Hippocampal function <strong>and</strong>visual object processing in temporal lobe epilepsy. Neuroreport2003; 14: 1489-1492.24
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Event-Related Potentials in PsychiatryOliver Pogarell, Christoph Mulert <strong>and</strong> Ulrich HegerlKey WordsAlzheimer’s DiseaseCNVDepressionEvent-Related PotentialsLDAEPMMNP50P300PsychiatrySchizophreniaSensory GatingABSTRACTElectrophysiological assessments of psychiatric disordershave produced a number of promising, highly replicablefindings <strong>and</strong> thus carry the potential of becoming clinicallyutilizable in the diagnostic or prognostic evaluation ofpsychopathological conditions. The procedures involvedare rather complex technically <strong>and</strong> the interpretation of thefindings require a combined neurophysiological <strong>and</strong> clinicalexpertise. On the other h<strong>and</strong>, electrophysiological techniquesare in general non-invasive <strong>and</strong> relatively inexpensive,<strong>and</strong> neurophysiology laboratories are widely availablein the clinical setting.Among these techniques, event-related potentials(ERPs) are of major interest in psychiatry, particularlysince these tools can indicate cortical neuronal dysfunctions,which play a major role in various neuropsychiatricdisorders.INTRODUCTIONDecades ago reports on event-related potentials(ERPs) such as Contingent Negative Variation (CNV) 1 <strong>and</strong>P300 2 stimulated the interest of both psychiatrists <strong>and</strong> psychologistsin these neurophysiology techniques. ERPs inpsychiatry, however, did not gain comparable clinical relevanceas early sensory evoked potentials in neurology, <strong>and</strong>rather remained a tool for basic research.Regarding clinical applicability ERP studies were hamperedby the fact that most of these parameters were diagnosticallyunspecific <strong>and</strong> not reliable enough to be usefulfor the individual patient. On the other h<strong>and</strong>, the relationshipbetween ERPs <strong>and</strong> circumscribed cognitive functionswas another attractive approach. For example, interestingcorrelations between late evoked positivities <strong>and</strong> memory,N400 <strong>and</strong> semantic processes, or the latencies of ERPs<strong>and</strong> the timing of cognitive processes have beendescribed. This research is of considerable interest fortesting information processing models in cognitive psychologybecause ERPs might be useful indicators of cognitiveprocesses <strong>and</strong> dysfunctions not accessible tobehavioral testing. Concerning psychiatry, this approachmay deepen the underst<strong>and</strong>ing of pathophysiology in awide range of psychiatric disorders. Nevertheless, it isunlikely that such studies will lead to results with broadclinical relevance.In recent years the focus of ERPs research in psychiatryhas shifted to other fields. A unique advantage of ERPsis the fact that cortical function <strong>and</strong> reactivity can beassessed with high temporal resolution (e.g., as comparedto functional MRI) in both a sensitive <strong>and</strong> noninvasive manner.This offers the possibility to monitor changes of brainfunction, e.g., during medication with psychotropic drugsby serial recordings. Another promising approach is tostudy ERP parameters as indicators of central neurochemicalfunction <strong>and</strong> as predictors of the patients´ responses topsychopharmacotherapy, since ERPs directly reflect postsynapticeffects of cortically released neurotransmitters(e.g., GABA, glutamate) <strong>and</strong> indirect modulatory effects ofneuromodulators (e.g., serotonin, acetylcholine) on corticalneuronal function. ERP parameters indicating the functionof neurochemical systems would be of considerable clinicalvalue due to the fact that subgroups of patients withcertain neurochemical dysfunctions could be identified <strong>and</strong>could be treated more specifically. The increasing knowledgeabout anatomical structures <strong>and</strong> cellular processesunderlying event-related potentials <strong>and</strong> methodologicaladvances in ERP data analysis may help to bridge the gapbetween ERPs <strong>and</strong> basic physiological processes.The P300 event related potentialP300 is a positive ERP which occurs with a latency ofabout 300 ms after presentation of task relevant stimuliOliver Pogarell, Christoph Mulert, Ulrich Hegerl are from the Departmentof Psychiatry, Division of Clinical Neurophysiology, Ludwig-Maximilians-University of Munich.Address requests for reprints to Oliver Pogarell, MD, Dept. of Psychiatry,Div. of Clinical Neurophysiology, Ludwig-Maximilians-University of Munich,Nussbaumstr. 7, D-80336 Munich, Germany.Email: oliver.pogarell@med.uni-muenchen.de25
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1<strong>and</strong> which is related to psychological aspects like cognitionor attention (information processing). There are atleast two distinct P300 subcomponents which overlap atthe scalp. The P3b has a more centro-parietal distribution<strong>and</strong> corresponds to the classical P300 recorded within anoddball paradigm after rare <strong>and</strong> task relevant events. T h eP3a occurs after novel events independently of task relevance<strong>and</strong> is characterized by a more frontal distribution,a shorter latency <strong>and</strong> a fast habituation. These subcomponentsreflect functionally different processes. Whereas theP3a has been interpreted as an orienting response, theP3b was related to psychological constructs such as controlledinformation processing, the information content ofthe event, memory processes, the reorganization of aninternal expectancy model (“context updating”) or the“context closure.” 3The physiological interpretation of P300 is limited bythe fact that knowledge about the neuronal structures <strong>and</strong>processes involved in the generation of P300 are still insufficient.However, knowledge has increased considerably inthe last years. Intracerebral recordings in patients withepilepsy have shown that the parietal <strong>and</strong> temporal cortexare involved in the generation of the auditory P3b.Concerning P3a the superior temporal plane, the associationcortices, limbic structures, <strong>and</strong> frontal as well as prefrontalcortices appear to play a major role. 4-6 With localrecording, the hippocampus shows the largest P300.However, because the hippocampus is an electricallyclosed field, this structure probably does not contribute in arelevant manner to the P300 recorded at the scalp.A further progress in this respect might be the simultaneousrecording of ERPs under functional magnetic resonanceimaging (fMRI). Both fMRI <strong>and</strong> <strong>EEG</strong> are complementarymethods for the analysis of brain activity witheach method having its strength where the other one haslimits: the spatial resolution in the range of millimeters infMRI <strong>and</strong> the time resolution in the range of millisecondsin <strong>EEG</strong>.Mulert et al 7 have shown that high quality <strong>EEG</strong> recordingsare feasible inside the scanner with adequate eliminationof artifacts (e.g., originating from MR gradients) fromthe <strong>EEG</strong> signal. Therefore, not only an optimal temporalresolution of brain activity (as recorded via ERPs/<strong>EEG</strong> fromthe scalp) but also a precise spatial allocation of the underlyingstructures has been made possible.Regarding the neurochemical background, it is widelyaccepted that P300 potentials recorded at the scalp resultfrom intracortical currents induced by postsynaptic potentials.Neuronal cortical processing is influenced by corticallyreleased modulatory neurotransmitters (serotonin,dopamine, noradrenaline, <strong>and</strong> acetylcholine). Therefore itis not surprising that these transmitters are also related toP300. Because of the close interaction between the differentneuromodulatory systems, a highly specific relationshipbetween P300 parameters <strong>and</strong> a certain neuromodulatorcannot be expected. Most consistent are the results concerningP300 <strong>and</strong> the cholinergic system. Anticholinergicinterventions induce a latency increase <strong>and</strong> amplitudereduction of P300 whereas the opposite is observed aftercholine agonists. 8-15 This is in line with the robust findingthat Alzheimer’s disease, which is associated with cholinergichypofunction, is associated with reduced amplitude<strong>and</strong> prolonged latency of P300.Influences of the noradrenergic <strong>and</strong> the dopaminergicsystem on P300 16-19 have also been described. The serotonergicsystem appears to play only a minor role for thegeneration of the P300. 12,20P 300 in psychiatric disordersSchizophreniaThe heterogeneity of schizophrenic disorders regardings y m p t o m a t o l o g y, course <strong>and</strong> outcome is expected toreflect heterogeneity of various underlying pathophysiologicalprocesses. In this respect physiological parameterscould be helpful to define subgroups that are more homogeneousnot only concerning clinical <strong>and</strong> therapeutic variablesbut also the pathophysiological mechanisms. Withrespect to schizophrenic disorders P300 is among themost intensively studied ERPs.It is a robust finding that the P300 amplitude is smallerin schizophrenic patients than in healthy controls. This hasbeen demonstrated in acutely ill, remitted, medicated <strong>and</strong>unmedicated patients. 21-26 Neuroleptics have only a relativelysmall effect on P300 amplitudes, which is supportedby studies comparing patients with high versus low plasmalevels of neuroleptics or by a longitudinal study in patientswho discontinued neuroleptic treatment. 27The amplitude reduction of the auditory P300 in schizophrenicpatients is not merely reflecting state dependentaspects but also has to be considered as a trait marker.This is supported by studies showing that the reduction ofP300 amplitude is not influenced in a relevant manner byneuroleptic medication <strong>and</strong> can also be found in remittedschizophrenics. 22 Furthermore, children of schizophrenicparents <strong>and</strong> other subjects at risk of developing schizophreniashowed P300 abnormalities. Studies in children ofschizophrenic parents showed a prolongation of P300latencies (auditory oddball paradigm) <strong>and</strong>/or smaller P300amplitudes as compared to matched controls. 28It has been postulated that patients with a neurodevelopmentalschizophrenia form a subgroup characterized bypoor premorbid adjustment with cognitive disturbances,early <strong>and</strong> insidious onset, a chronic <strong>and</strong> deterioratingcourse of the disease, negative symptoms <strong>and</strong> a tendencyto develop tardive dyskinesia. 29 There are several studiessupporting the assumption that schizophrenic patientswith small P300 correspond to this subgroup of schizophrenics.In a study on stabilized schizophrenic patientsthe subgroup with a small P300 showed more residual26
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1symptoms, more perinatal complications, poor premorbidadjustment <strong>and</strong> a higher risk of developing tardive dyskinesia.The majority of patients showing tardive dyskinesiaat the time of the recording also presented with a smallP300. Even more interesting is the finding that patientswho developed tardive dyskinesias during a 2 years follow-upperiod had already significantly smaller P300 at thebeginning of the prospective study. 3 0 A small P300 hasbeen found to predict nonresponse to neuroleptics concerningpositive symptoms <strong>and</strong> a prolonged P300 latencyhas been found to predict non-response concerning negativesymptoms. 2 3 S i m i l a r l y, Strik et al 3 1 - 3 3 found thatpatients with a “cycloid psychosis” (according to the classificationby Leonhard), which is characterized by a favorabletherapeutic response <strong>and</strong> long-term prognosis, haveno reduction of P300 amplitude or even an increase inamplitude compared to healthy subjects. Furthermore, instudies on stabilized schizophrenic outpatients it is a quiteconsistent finding that patients with small P300 have moreresidual symptoms, mainly negative symptoms <strong>and</strong>thought disorders.P300 <strong>and</strong> psychopathologyFor the evaluation of the relationship between P300<strong>and</strong> psychopathology, it is of crucial importance to independentlystudy stabilized patients <strong>and</strong> acutely psychoticpatients. In stabilized patients, it is a quite consistent findingthat P300 amplitude is negatively correlated with residualsymptoms. This association does not reflect statedependent effects of residual symptoms on P300 butrather the poor outcome of a subgroup of patients withsmall P300. This interpretation is supported by a study ofschizophrenic patients, retested after 9 months. Here theintra-individual changes of psychopathology were not relatedto the corresponding changes of P300 amplitude. 27However, the P300 component reflects both trait <strong>and</strong>state aspects such as psychopathology. Several studies onacutely psychotic patients reported positive correlationsbetween P300 amplitudes <strong>and</strong> the severity of positivesymptoms. However, the literature is not entirely consistenton this issue, which can be explained by differences in theseverity of the acute symptomatology. It has to be expectedthat patients with severe acute symptoms leading toimpaired attention, will have difficulties to cooperate <strong>and</strong> toperform the P300 oddball paradigm. 34-36In summary, a small P300 in schizophrenic patientshas been found to be a vulnerability marker characterizinga subgroup of patients with a poor premorbid adjustment,an enhanced risk of developing tardive dyskinesia, moreresidual symptoms <strong>and</strong> a poor outcome. Concerning theevaluation of the relationship between psychopathology<strong>and</strong> P300, it is of importance to control the studies forremitted versus acutely psychotic patients, predominanceof positive versus negative symptoms <strong>and</strong> to differentiatethe P300 subcomponents P3a <strong>and</strong> P3b.Affective disordersAn amplitude reduction of P300 has been found indepressed patients although the literature is not consistenton this issue. Some authors found changes of P300 only ina subgroup of patients, mainly in those with severe or psychoticdepression. 37,38It is a replicated finding that patients with depressive disorderswith suicide attempts showed smaller P300 amplitudesthan depressive patients without suicide attempts. Inaddition a correlation has been reported between acute suicidality<strong>and</strong> P300 amplitude. 3 9 A convincing explanation forthis relationship has not been given up to now.Alzheimer’s diseaseP300 is an interesting instrument for studyingA l z h e i m e r’s disease, because latency <strong>and</strong> amplitude ofP300 are closely related to cognitive processes <strong>and</strong> tocholinergic function. Furthermore P300 is cortically generated<strong>and</strong> A l z h e i m e r’s disease impairs especially cortical functioning.It is therefore not surprising that A l z h e i m e r’s diseaseis related in a consistent manner with smaller P300amplitudes <strong>and</strong> prolonged P300 latencies. Such changescan be observed even in patients with mild A l z h e i m e r’s disea s e . 4 0 , 4 1 In studies, comparing demented patients with psychiatric<strong>and</strong> neurological patients without dementia, thespecificity of P300 latencies was above 80 % whereas thesensitivity was relatively poor, ranging between 15 <strong>and</strong>80%. As expected, studies with more severely dementedpatients reported higher sensitivities. Auditory P300 latencieswere superior to visual P300 latencies concerning therecognition of patients with A l z h e i m e r’s disease.In a prospective, confirmatory study to evaluate the clinicalrelevance of the P300 in the early diagnosis of A D ,Frodl et al 4 2 investigated patients with AD, mild cognitiveimpairment (MCI) <strong>and</strong> healthy controls (HC) using P300assessments with dipole source analysis. The authorscould demonstrate that the amplitudes of temporo-basaldipoles (equivalent to the P3b subcomponent) were statisticallysignificantly decreased in AD as compared to both HC<strong>and</strong> MCI. Furthermore, the latencies of superior temporaldipoles (equivalent to P3a) were significantly prolonged inAD compared with HC. The significant differences remainedstable after stratification of the patients regarding the severityof the disease: Even patients with mild AD showedmarked, significant reductions in P300 amplitudes. T h esensitivity <strong>and</strong> specificity for the differentiation of A Dpatients <strong>and</strong> HC using temporo-basal P300-amplitudes <strong>and</strong>superior temporal P300-latencies were as high as 86.7%,<strong>and</strong> 88.5%, respectively, which is comparable to other(often less validated) biological diagnostic markers in A D .The P300 is related to cholinergic neurotransmission<strong>and</strong> may therefore be useful to identify subgroups with amore circumscribed cholinergic dysfunction. This subgroupmay turn out to show a favorable response to a treatmentwith cholinesterase inhibitors.27
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1In addition, P300 as a non-invasive instrument mightbe a useful method for the assessment of changes in corticalfunction during follow-up by serial recordings.Regarding treatment monitoring, i.e., detection of neurobiologicaleffects of pharmacotherapy with cholineesterase inhibitors (CEI) in AD, Thomas et al 43 coulddemonstrate in a study of 60 subjects with AD treated witheither the choline esterase inhibitors donepezil or rivastigmineor with vitamine E, that only the treatment with CEI(both rivastigmine or donepezil) led to a significantdecrease in P300 latencies, which was correlated to a clinicalimprovement of cognitive performance. The data havebeen replicated after stratification of the subjects accordingto severity of the dementia. 44In a study by another group on 40 patients with moderateAD who underwent a 12 week controlled treatment witheither CEI or placebo medication, the investigators couldprovide preliminary evidence for the value of P300 measurementsregarding prediction of treatment response. 45The subjects received electrophysiological evaluations(P300, auditory oddball paradigm, dipole source analysis)during a 12 week double-blind, placebo-controlled treatmentwith donepezil. Treatment response (as assessed bya maintenance or improvement in scoring on dementia ratingscales) was analyzed after stratification of donepezil<strong>and</strong> placebo patients according to high/low P300 amplitudesat baseline. In this study there was a significantassociation between the P300 parameters at baseline <strong>and</strong>the mean change in ADAS-cog scores after 12 weeks ontreatment: patients with high P300 amplitudes at baselineshowed a statistically significant better treatment responseafter 12 weeks on verum medication. The correspondinganalyses in the placebo group did not show statistically significantdifferences.Thus these studies provide preliminary evidence thatthe event-related P300 might represent a reliable, noninvasive<strong>and</strong> clinically practicable auxiliary tool, offeringcomplementary information on brain functional aspects.The data on P300 in patients with Alzheimer’s dementiashow that ERPs may provide useful tools not only for diagnosisbut also for treatment monitoring <strong>and</strong>/or prediction oftreatment response in cognitive dysfunction.Contingent negative variation (CNV)CNV is a negative potential that slowly develops in thetime-interval between a warning stimulus <strong>and</strong> a relatedimperative stimulus, which requires a motor or mentalresponse. When longer time-intervals are used betweenthe warning <strong>and</strong> the imperative stimulus (inter-stimulusinterval: 3-8 sec.) an initial CNV (iCNV) with a more frontaldistribution <strong>and</strong> a terminal CNV (tCNV) with a maximumover central regions can be distinguished. Empirical as wellas theoretical arguments indicate that this negativity isrelated to the depolarization of apical cortical dendrites <strong>and</strong>to an enhanced cortical excitability. This interpretation issupported by the more recent observation that the reactiontime to sensory stimuli falling in the phase of the developingnegativity is shorter <strong>and</strong> the evoked neuroelectricresponse is larger as compared to stimuli falling outside ofthis negativity. 46,47 CNV has originally been related toexpectancy. However, it depends on several unspecificpsychological factors such as attention or motivation. Aclear relation to psychological constructs is difficult. Onereason is the fact that CNV is not a uniform component.Concerning iCNV, an overlap of late effects of the warningstimuli to processes related to the imperative stimulus haveto be considered, <strong>and</strong> concerning tCNV, there may be anoverlap between non-motoric pre-imperative processes(e.g., anticipation) <strong>and</strong> the Bereitschaftspotential 48 relatedto the preparation of a motor response.In schizophrenic patients it is a quite consistent findingthat CNV at central regions is reduced. An interesting observationhas been that in schizophrenic patients, especially inthe acute psychotic state, the CNV after the imperative stimulusis not going down to baseline or is going down mores l o w l y. This post imperative negative variation (PINV), howev e r, is not specific for schizophrenia, but has also beenfound in other psychiatric disorders, such as dementia ormania. In patients with affective disorders a reduction ofCNV has been reported although it is controversial, whetheror not this reduction is state dependent or a trait marker. It isof interest that depressed patients with an enhanced risk ofsuicide have a smaller CNV <strong>and</strong> a larger PINV th<strong>and</strong>epressed patients without enhanced risk of suicide. 39 , 49Mismatch negativity (MMN)MMN is a negativity over fronto-central brain regionswith a latency of 250 ms, which develops after stimuli thatare deviant with regard to physical stimulus properties(e.g., loudness, duration, frequency). MMN is mostlyshown as the difference wave between the response to thefrequent <strong>and</strong> the deviant stimuli. This component is independentof attention <strong>and</strong> seems to reflect a largely automaticdeviance detecting process of sensory cortex. In theauditory modality the MMN is generated mainly by thesupratemporal cortex. 50 The sum activity of this structure isoriented perpendicularly to the cortical surface <strong>and</strong> istherefore projecting to frontal electrodes. This explains thefrontal distribution of the MMN. Animal experiments haveshown that the MMN is blocked by competitive as well asnon-competitive NMDA-receptor antagonists whereas earlierobligatory components are not influenced by suchdrugs. 51 This indicates that MMN depends on the currentflow induced by the opening of cortical NMDA-channels<strong>and</strong> therefore on glutamatergic neurotransmission. Theevaluation of the specificity of this relationship is difficult atthe moment. It has been observed that histamine-receptorsalso influence the MMN. 52Medicated <strong>and</strong> unmedicated schizophrenic patientsshowed a reduction of the MMN. 53-56 This indicates that a28
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1neurophysiological deficit in schizophrenia can be foundalready at the level of the sensory cortex <strong>and</strong> not onlyinvolves association cortices <strong>and</strong> limbic structures. Thisfinding is also of interest considering the hypothesis of glutamatergichypofunction in schizophrenic disorders. Thisglutamatergic hypofunction could be an explanation for thereduction of the MMN, because the relevance of NMDAreceptorfunction for the electrogenesis of MMN has beenshown in animal experiments.MMN responses were related to negative but not topositive symptoms <strong>and</strong> correlated with neuropsychologicalimpairments. 54,57 Since MMN reflects a basal detectionmechanism for deviant sensory events, a dysfunction inthis process could be the physiological correlate for thereduced reactivity to external stimuli in schizophrenicpatients with negative symptoms. A recent study showedthat MMN deficits are linked to global impairments in everydayfunctioning in patients with schizophrenia. MMNseems to represent a core neurophysiological dysfunction<strong>and</strong> might therefore be useful as a measure for predictingthe functional outcome. 58 In addition, mismatch negativitygeneration has been reported to be impaired in subjects atrisk for the later development of psychosis. 59P50 sensory gatingP50 sensory gating paradigms have been extensivelyused in patients with schizophrenia, where various degreesof abnormalities <strong>and</strong> deficits have been described. 60 - 63Sensory gating means the pre-attentional habituation ofresponses to repeated stimuli of the same sensory quality.In normal controls there is an inhibition of responsivenessto these repetitive stimuli. The P50 wave is the event relatedpotential used for the assessment of sensory gating. T h edecrease or inhibition of this component upon a second ofa pair of stimuli serves as the neurophysiological correlateof activated inhibitory mechanisms to block out irrelevant,meaningless or redundant stimuli.Most patients with schizophrenia have an impairmentof P50 sensory gating, i.e., a diminished P50 reduction inthe respective paradigms. Human <strong>and</strong> animal studies havesuggested that alterations of cholinergic (nicotinic) receptorsmight be the neurochemical background of sensorygating deficits in schizophrenia. 60,64-68 P50 sensory gatingabnormalities in schizophrenia have just recently beenextensively reviewed by Potter et al. 61 There is a large bodyof literature; however, the presented data are not overallconsistent regarding clinical correlates, medication effects,control for confounding effectors, etc. There is strong evidenceof an association of P50 data with measures of vigilance<strong>and</strong> attention, whereas there are no clear <strong>and</strong> explicitcorrelations with the severity of clinical schizophrenic featuressuch as positive or negative symptoms. Regardingtreatment effects, it has been shown, mainly in openuncontrolled studies, that P50 sensory gating deficits areunchanged under typical neuroleptic medication, whereasatypical antipsychotics seem to improve this neurophysiologicalparameter. 69 - 71Among the second generationantipsychotics, clozapine has been shown to even normaliseP50 ratios. 69,71,72 Besides schizophrenics, subjectswith prodromal symptoms <strong>and</strong> at risk for the developmentof schizophrenia have been shown to present withimpaired sensory gating, 73 <strong>and</strong> P50 gating deficits appearto be a genetic trait in schizophrenia patients that is alsofound in first degree relatives. 63,74-76In conclusion, the P50 sensory gating paradigm is animportant research tool for the investigation of patients withschizophrenia <strong>and</strong> their relatives, since it reflects essentialfunctions of information processing protecting the brainfrom overflow <strong>and</strong> that might be disturbed in psychosis.However, more research is required in terms of the clinicalsignificance of P50 impairments <strong>and</strong> their improvementsupon different types of medication.The intensity dependence ofauditory evoked potentials (IDAEP)Interindividual differences in the intensity dependenceof sensory evoked potentials were first investigated withinthe augmenting/reducing concept proposed for evokedpotentials by Buchsbaum <strong>and</strong> Silverman. 77 In these studiesmainly visual evoked potentials (VEP) were used. A flat ornegative slope of the amplitude stimulus intensity function(reducing) was seen as reflecting a central mechanismregulating the sensitivity in all sensory modalities <strong>and</strong> protectingthe organism from sensory overstimulation. Thisgeneral augmenting/reducing concept has been criticized,because the augmenting/reducing characteristic wasshown to depend on many methodological aspects such asthe parameterization of the intensity dependence, therecording site or the intensity range or modality of the stimuli.78-80 Converging arguments from clinical <strong>and</strong> preclinicalstudies support the hypothesis that the loudness dependenceof the auditory evoked N1/P2 response (LDAEP) isregulated by the level of central serotonergic neurotransmission.81 More specifically, animal studies suggest thatinhibition or activation of the serotonergic neurons in thedorsal raphe nucleus influence the loudness dependencein the primary but not in the secondary auditory cortex. 82,83With dipole source analysis or tomographic current sourcedensity analysis activity of the primary <strong>and</strong> secondary auditorycortex can (at least in parts) be separated. 84 , 85R e c e n t l y, with functional magnetic resonance imaging(fMRI) loudness dependence could be demonstrated mainlyfor the primary <strong>and</strong> only to a lesser degree for the secondaryauditory cortex. 86,87In clinical studies an increased LDAEP has beenshown in MDMA users, 88,89 <strong>and</strong> in patients with borderlinepersonality disorder, 90 indicative of a serotonergic dysfunctionin these subjects. In depressed patients a high LDbefore drug treatment has been associated with a favorableresponse to serotonergic medication. 91-9329
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Regarding the validation of the assumed serotonergicproperties of LDAEP in vivo combined studies with SinglePhoton Emission Computed Tomography (SPECT) usingthe monoaminergic (serotonergic <strong>and</strong> dopaminergic) radiolig<strong>and</strong>β-CIT, a marker of Serotonin- <strong>and</strong> Dopamintransporters(SERT, <strong>and</strong> DAT) have been performed. SPECT<strong>and</strong> β-CIT allow to semiquantitatively assess SERT <strong>and</strong>DAT availabilities within the brainstem/pons (SERT) <strong>and</strong> inthe striatum (DAT). In such studies it has been demonstratedthat the loudness dependence was highly significantlycorrelated with both nuclear imaging markers of the serotonergic<strong>and</strong> dopaminergic system, which is a first direct invivo evidence that LDAEP is associated with centralmonoaminergic function in psychiatric patients. 94The observation that allelic variants of the serotonintransporter gene differ with respect to the LD further supportsthe hypothesis of an association between the serotonergicsystem <strong>and</strong> neurophysiological measures. 95Nevertheless, the complexity of central monoaminergicsystems, which are strongly interconnected <strong>and</strong> showinteractions between different neurochemical subdivisions,has to be taken into account. Therefore, only a relativespecificity of this indicator for certain functional aspects,e.g., in terms of the serotonergic system can be expected.In spite of these limitations, the studies on psychiatricpatients treated with serotonergic agents suggest that theloudness dependence of the N1/P2 activity may well beclinically useful for a more carefully directed individualpharmacotherapy in neuropsychiatry. 96Affective disordersReports in the literature as well as own results indicatethat a pronounced LDAEP predicts a favorable response toSSRI treatment. Paige et al 97 reported that depressedpatients who responded to SSRI had a strong LDAEP (P2-component) before starting medication. During medication,no reduction of the LDAEP was observed. These findingswere supported by using a dipole source analysis ofLDAEP. Depressed patients responding to SSRI (sertraline,paroxetine) had a stronger LDAEP (N1/P2 component)at baseline, i.e., before starting medication. 93 Thisindicates that the LDAEP could give valuable informationto the clinician concerning the probability of individualresponse to SSRI in depressed patients. It remains unclearwhether or not LDAEP predicts response or nonresponsespecifically to SSRI or also to alternative therapies. Paigeet al 98 reported that a strong LDAEP also predicts favorableresponse to the noradrenergic <strong>and</strong> dopaminergic agentbuproprion, which supports the predictive quality of theLDAEP concerning response to antidepressants whereasthe specificity of this tool concerning serotonergic antidepressantsremains to be elucidated.Lithium has serotonin-agonistic eff e c t s , 9 9 which are supposedto be relevant for its acute antidepressant <strong>and</strong> antimanicas well as its relapse preventing effects. Therefore, itcan be assumed that especially those patients with lowserotonergic function, indicated by a strong LDAEP, will belithium responders. Several studies consistently reportedthat patients with a strong intensity dependence of sensoryevoked potentials (VEP, SEP) are responders to acute antidepressiveor antimanic lithium therapy. 7 7 , 1 0 0 - 1 0 2These findings have stimulated research on the predictivequality of LDAEP concerning clinical response to preventivelithium treatment. Predictors of response or nonresponseto preventive lithium medication would be especiallyvaluable, because of the high rate of nonresponse (up to45%), the long observation time needed to evaluate clinicalresponse <strong>and</strong> the risks of long-term lithium medication.In our laboratory, Hegerl et al found that patients with affectivepsychoses responding to preventive lithium medicationwere indeed characterized by a strong LDAEP. 103 Patientswere classified as responders, when they had no recurrenceleading to hospitalization under lithium during thepreceding 5 years. This finding was replicated in anotherretrospective study: responders to preventive lithium treatmentwere again characterized by a significantly strongerLDAEP. 104CONCLUSIONERPs are unique tools for evaluating the reactivity of corticalneuronal activity in psychiatric patients. Due to a closerelationship between ERPs <strong>and</strong> cortical release of neurotransmitters,ERPs are at least in part useful indicators ofneurochemical dysfunction. Therefore, these techniquesmight contribute to the prediction of response to pharmacotherapyor monitoring changes in brain function duringp s y c h o p h a r m a c o t h e r a p y. These approaches have led toconsistent results, which are not only of value for the developmentof pathogenetic models or to establish a sub classificationof psychiatric disorders, but also are of relevance forclinical <strong>and</strong> therapeutic decisions in psychiatric practice.30
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1REFERENCES1. Walter WG, Cooper R, Aldridge VJ, McCallum WC, WinterAL. Contingent negative nariation: an electric sign of sensorimotorassociation <strong>and</strong> expectancy in the human brain.Nature 1964; 203: 380-384.2. Sutton S, Braren M, Zubin J, John ER. Evoked-potential correlatesof stimulus uncertainty. Science 1965; 150(700):1187-1188.3. Verleger R. Event related potentials <strong>and</strong> cognition: a critiqueof the context updating hypothesis <strong>and</strong> an alternative interpretationof P3. Behav Br Sci 1988; 11: 343-356.4. Halgren E, Baudena P, Clarke JM, Heit G, Liegeois C,Chauvel P, et al. Intracerebral potentials to rare target <strong>and</strong>distractor auditory <strong>and</strong> visual stimuli. I. Superior temporalplane <strong>and</strong> parietal lobe. Electroencephalogr Clin Neurophysiol1995; 94(3): 191-220.5. Halgren E, Baudena P, Clarke JM, Heit G, Marinkovic K,Devaux B, et al. Intracerebral potentials to rare target <strong>and</strong>distractor auditory <strong>and</strong> visual stimuli. II. Medial, lateral <strong>and</strong>posterior temporal lobe. Electroencephalogr Clin Neurophysiol1995; 94(4): 229-250.6. Baudena P, Halgren E, Heit G, Clarke JM. Intracerebralpotentials to rare target <strong>and</strong> distractor auditory <strong>and</strong> visualstimuli. III. Frontal cortex. Electroencephalogr Clin Neurophysiol1995; 94(4): 251-264.7. Mulert C, Jager L, Schmitt R, Bussfeld P, Pogarell O, MollerHJ, et al. Integration of fMRI <strong>and</strong> simultaneous <strong>EEG</strong>: towardsa comprehensive underst<strong>and</strong>ing of localization <strong>and</strong> timecourseof brain activity in target detection. Neuroimage 2004;22(1): 83-94.8. Dierks T, Frolich L, Ihl R, Maurer K. Event-related potentials<strong>and</strong> psychopharmacology: cholinergic modulation of P300.Pharmacopsychiatry 1994; 27(2): 72-74.9. Antal A, Bodis-Wollner I, Ghilardi MF, Glover A, Mylin L, ToldiJ. The effect of levo-acetyl-carnitine on visual cognitiveevoked potentials in the behaving monkey. ElectroencephalogrClin Neurophysiol 1993; 86(4): 268-274.10. Br<strong>and</strong>eis D, Naylor H, Halliday R, Callaway E, Yano L.Scopolamine effects on visual information processing, attention,<strong>and</strong> event-related potential map latencies. Psychophysiology1992; 29(3): 315-336.11. Meador KJ. Cholinergic, serotonergic, <strong>and</strong> GABAergiceffects on the ERP. Electroencephalogr Clin Neurophysiol(suppl) 1995; 44: 151-155.12. Meador KJ, Loring DW, Davis HC, Sethi KD, Patel BR,Adams RJ, et al. Cholinergic <strong>and</strong> serotonergic effects on theP3 potential <strong>and</strong> recent memory. J Clin Exp Neuropsychol1989; 11 (2): 252-260.13. Harrison JB, Buchwald JS, Kaga K, Woolf NJ, Butcher LL.“Cat P300” disappears after septal lesions. ElectroencephalogrClin Neurophysiol 1988; 69(1): 55-64.14. Hammond EJ, Meador KJ, Aung-Din R, Wilder BJ.Cholinergic modulation of human P3 event-related potentials.Neurology 1987; 37(2): 346-350.15. Callaway E, Halliday R, Naylor H, Schechter G. Effects oforal scopolamine on human stimulus evaluation. Psychopharmacology(Berl) 1985; 85(2): 133-138.16. Pineda JA, Foote SL, Neville HJ. Effects of locus coeruleuslesions on auditory, long-latency, event-related potentials inmonkey. J Neurosci 1989; 9(1): 81-93.17. Blum K, Braverman ER, Dinardo MJ, Wood RC, Sheridan PJ.Prolonged P300 latency in a neuropsychiatric population withthe D2 dopamine receptor A1 allele. Pharmacogenetics1994; 4(6): 313-322.18. Noble EP, Berman SM, Ozkaragoz TZ, Ritchie T. ProlongedP300 latency in children with the D2 dopamine receptor A1allele. Am J Hum Genet 1994; 54(4): 658-668.19. Gallinat J, Bajbouj M, S<strong>and</strong>er T, Schlattmann P, Xu K, FerroEF, et al. Association of the G1947A COMT (Val (108/158)Met) gene polymorphism with prefrontal P300 during informationprocessing. Biol Psychiatry 2003; 54(1): 40-48.20. Pritchard WS, Raz N, August GJ. No effect of chronic fenfluramineon the P300 component of the event-related potential.Int J Neurosci 1987; 35(1-2): 105-110.21. Shutara Y, Koga Y, Fujita K, Takeuchi H, Mochida M,Takemasa K. An event-related potential study on the impairmentof automatic processing of auditory input in schizophrenia.Brain Topogr 1996; 8(3): 285-289.22. Rao KM, Ananthnarayanan CV, Gangadhar BN,Janakiramaiah N. Smaller auditory P300 amplitude in schizophrenicsin remission. Neuropsychobiology 1995; 32(3):171-174.23. Ford JM, White P, Lim KO, Pfefferbaum A. Schizophrenicshave fewer <strong>and</strong> smaller P300s: a single-trial analysis. BiolPsychiatry 1994; 35(2): 96-103.24. Laurent A, Garcia-Larrea L, Dalery J, Terra JL, D’Amato T,Marie-Cardine M, et al. The P 300 potential in schizophrenia.[In French] Encephale 1993; 19(3): 221-227.25. Eikmeier G, Lodemann E, Zerbin D, Gastpar M. Event-relatedpotentials in schizophrenic patients in the acute phase <strong>and</strong> inremission. [In German] <strong>EEG</strong> EMG Z ElektroenzephalogrElektromyogr Verw<strong>and</strong>te Geb 1991; 22(1): 15-20.26. Blackwood DH, St Clair DM, Muir WJ, Duffy JC. AuditoryP300 <strong>and</strong> eye tracking dysfunction in schizophrenic pedigrees.Arch Gen Psychiatry 1991; 48(10): 899-909.27. Juckel G, Muller-Schubert A, Gaebel W, Hegerl U. Residualsymptoms <strong>and</strong> P300 in schizophrenic outpatients. PsychiatryRes 1996; 65(1): 23-32.28. Schreiber H, Stolz-Born G, Kornhuber HH, Born J. Eventrelatedpotential correlates of impaired selective attention inchildren at high risk for schizophrenia. Biol Psychiatry 1992;32(8): 634-651.29. Murray RM, O’Callaghan E, Castle DJ, Lewis SW. A neurodevelopmentalapproach to the classification of schizophrenia.Schizophr Bull 1992; 18(2): 319-332.30. Hegerl U, Juckel G, Muller-Schubert A, Pietzcker A, GaebelW. Schizophrenics with small P300: a subgroup with a neurodevelopmentaldisturbance <strong>and</strong> a high risk for tardive dyskinesia?Acta Psychiatr Sc<strong>and</strong> 1995; 91(2): 120-125.31. Strik WK, Dierks T, Franzek E, Maurer K, Beckmann H.Differences in P300 amplitudes <strong>and</strong> topography betweencycloid psychosis <strong>and</strong> schizophrenia in Leonhard’s classification.Acta Psychiatr Sc<strong>and</strong> 1993; 87(3): 179-183.32. Strik WK, Dierks T, Maurer K. Amplitudes of auditory P300 inremitted <strong>and</strong> residual schizophrenics: correlations with clinicalfeatures. Neuropsychobiology 1993; 27(1): 54-60.33. Strik WK, Fallgatter AJ, Stoeber G, Franzek E, Beckmann H.Specific P300 features in patients with cycloid psychosis.Acta Psychiatr Sc<strong>and</strong> 1996; 94(6): 471-476.31
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 134. Blackwood D. P300, a state <strong>and</strong> a trait marker in schizophrenia.Lancet 2000; 355(9206): 771-772.35. Mathalon DH, Ford JM, Pfefferbaum A. Trait <strong>and</strong> stateaspects of P300 amplitude reduction in schizophrenia: a retrospectivelongitudinal study. Biol Psychiatry 2000; 47(5):434-449.36. Frodl-Bauch T, Gallinat J, Meisenzahl EM, Moller HJ, HegerlU. P300 subcomponents reflect different aspects of psychopathologyin schizophrenia. Biol Psychiatry 1999; 45(1):116-126.37. Santosh PJ, Malhotra S, Raghunathan M, Mehra YN. A studyof P300 in melancholic depression-correlation with psychoticfeatures. Biol Psychiatry 1994; 35(7): 474-479.38. Bruder GE, Towey JP, Stewart JW, Friedman D, Tenke C,Quitkin FM. Event-related potentials in depression: influenceof task, stimulus hemifield <strong>and</strong> clinical features on P3 latency.Biol Psychiatry 1991; 30(3): 233-246.39. Hansenne M, Pitchot W, Gonzalez Moreno A, Zaldua IU,Ansseau M. Suicidal behavior in depressive disorder: anevent-related potential study. Biol Psychiatry 1996; 40(2):116-122.40. Polich J, Ladish C, Bloom FE. P300 assessment of earlyAlzheimer’s disease. Electroencephalogr Clin Neurophysiol1990; 77(3): 179-189.41. Pfefferbaum A, Ford JM, Kraemer HC. Clinical utility of longlatency “cognitive” event-related potentials (P3): the cons.Electroencephalogr Clin Neurophysiol 1990; 76(1): 6-12; discussion1.42. Frodl T, Hampel H, Juckel G, Burger K, Padberg F, Engel RR,et al. Value of event-related P300 subcomponents in the clinicaldiagnosis of mild cognitive impairment <strong>and</strong> Alzheimer’sDisease. Psychophysiology 2002; 39(2): 175-181.43. Thomas A, Iacono D, Bonanni L, D’Andreamatteo G, OnofrjM. Donepezil, rivastigmine, <strong>and</strong> vitamin E in Alzheimer disease:a combined P300 event-related potentials/neuropsychologicevaluation over 6 months. Clin Neuropharmacol2001; 24(1): 31-42.44. Onofrj M, Thomas A, Luciano AL, Iacono D, Di Rollo A ,D’Andreamatteo G, et al. Donepezil versus vitamin E inA l z h e i m e r’s disease: II. mild versus moderate-severeA l z h e i m e r’s disease. Clin Neuropharmacol 2002; 25(4):2 0 7 - 2 1 5 .45. Pogarell O, Schulz C, Juckel G, Mueller-Siecheneder F, LauxG, Bahra R, et al. Auditory evoked P300 <strong>and</strong> treatmentresponse to donepezil in patients with Alzheimer´s disease.World J Biol Psychiatry 2001; 2: 264.46. Rockstroh B, Muller M, Wagner M, Cohen R, Elbert T. Eventrelated<strong>and</strong> motor responses to probes in a forewarned reactiontime task in schizophrenic patients. Schizophr Res 1994;13(1): 23-34.47. Wagner M, Rendtorff N, Kathmann N, Engel RR. CNV, PINV<strong>and</strong> probe-evoked potentials in schizophrenics. ElectroencephalogrClin Neurophysiol 1996; 98(2): 130-143.48. Kornhuber HH, Deecke L. Changes in the brain potential involuntary movements <strong>and</strong> passive movements in man: readinesspotential <strong>and</strong> reafferent potentials. Pflugers A r c hGesamte Physiol Menschen Tiere 1965; 284: 1-17.49. Ashton CH, Marshall EF, Hassanyeh F, Marsh VR, Wright-Honari S. Biological correlates of deliberate self-harm behaviour:a study of electroencephalographic, biochemical <strong>and</strong>psychological variables in parasuicide. Acta Psychiatr Sc<strong>and</strong>1994; 90(5): 316-323.50. Javitt DC, Steinschneider M, Schroeder CE, Vaughan HG,Jr., Arezzo JC. Detection of stimulus deviance within primateprimary auditory cortex: intracortical mechanisms of mismatchnegativity (MMN) generation. Brain Res 1994; 667(2):192-200.51. Javitt DC, Schroeder CE, Steinschneider M, Arezzo JC,Ritter W, Vaughan HG, Jr. Cognitive event-related potentialsin human <strong>and</strong> non-human primates: implications for thePCP/NMDA model of schizophrenia. Electroencephalogr ClinNeurophysiol 1995; (suppl) 44: 161-175.52. Serra JM, Escera C, Sanchez-Turet M, Sanchez-Sastre J,Grau C. The H1-receptor antagonist chlorpheniraminedecreases the ending phase of the mismatch negativity of thehuman auditory event-related potentials. Neurosci Lett 1996;203(2): 77-80.53. Javitt DC, Doneshka P, Grochowski S, Ritter W. Impairedmismatch negativity generation reflects widespread dysfunctionof working memory in schizophrenia. Arch GenPsychiatry 1995; 52(7): 550-558.54. Catts SV, Shelley AM, Ward PB, Liebert B, McConaghy N,Andrews S, et al. Brain potential evidence for an auditorysensory memory deficit in schizophrenia. Am J Psychiatry1995; 152(2): 213-219.55. Shelley AM, Ward PB, Catts SV, Michie PT, Andrews S,McConaghy N. Mismatch negativity: an index of a preattentiveprocessing deficit in schizophrenia. Biol Psychiatry 1991;30(10): 1059-1062.56. Rosburg T, Kreitschmann-Andermahr I, Sauer H. Mismatchnegativity in schizophrenia research. An indicator of earlyprocessing disorders of acoustic information. [In German]Nervenarzt 2004; 75(7): 633-641.57. Baldeweg T, Klugman A, Gruzelier J, Hirsch SR. Mismatchnegativity potentials <strong>and</strong> cognitive impairment in schizophrenia.Schizophr Res 2004; 69(2-3): 203-217.58. Light GA, Braff DL. Mismatch negativity deficits are associatedwith poor functioning in schizophrenia patients. Arch GenPsychiatry 2005; 62(2): 127-136.59. Brockhaus-Dumke A, Tendolkar I, Pukrop R, Schultze-LutterF, Klosterkotter J, Ruhrmann S. Impaired mismatch negativitygeneration in prodromal subjects <strong>and</strong> patients with schizophrenia.Schizophr Res 2005; 73(2-3): 297-310.60. Adler LE, Olincy A, Waldo M, Harris JG, Griffith J, Stevens K,et al. Schizophrenia, sensory gating, <strong>and</strong> nicotinic receptors.Schizophr Bull 1998; 24(2): 189-202.61. Potter D, Summerfelt A, Gold J, Buchanan RW. Review of clinicalcorrelates of P50 sensory gating abnormalities in patientswith schizophrenia. Schizophr Bull 2006; 32(4): 692-700.62. Adler LE, Waldo MC, Freedman R. Neurophysiologic studiesof sensory gating in schizophrenia: comparison of auditory <strong>and</strong>visual responses. Biol Psychiatry 1985; 20(12): 1284-1296.63. Siegel C, Waldo M, Mizner G, Adler LE, Freedman R. Deficitsin sensory gating in schizophrenic patients <strong>and</strong> their relatives:evidence obtained with auditory evoked responses.Arch Gen Psychiatry 1984; 41(6): 607-612.64. Leonard S, Gault J, Hopkins J, Logel J, Vianzon R, Short M,et al. Association of promoter variants in the alpha7 nicotinicacetylcholine receptor subunit gene with an inhibitory deficitfound in schizophrenia. Arch Gen Psychiatry 2002; 59(12):1085-1096.32
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 165. Leonard S, Breese C, Adams C, Benhammou K, Gault J,Stevens K, et al. Smoking <strong>and</strong> schizophrenia: abnormal nicotinicreceptor expression. Eur J Pharmacol 2000; 393(1-3):237-242.66. Leonard S, Gault J, Adams C, Breese CR, Rollins Y, AdlerLE, et al. Nicotinic receptors, smoking <strong>and</strong> schizophrenia.Restor Neurol Neurosci 1998; 12(2-3): 195-201.67. Leonard S, Adams C, Breese CR, Adler LE, Bickford P,Byerley W, et al. Nicotinic receptor function in schizophrenia.Schizophr Bull 1996; 22(3): 431-445.68. Freedman R, Adler LE, Bickford P, Byerley W, Coon H,Cullum CM, et al. Schizophrenia <strong>and</strong> nicotinic receptors.Harv Rev Psychiatry 1994; 2(4): 179-192.69. Nagamoto HT, Adler LE, Hea RA, Griffith JM, McRae KA,Freedman R. Gating of auditory P50 in schizophrenics: uniquee ffects of clozapine. Biol Psychiatry 1996; 40(3): 181-188.70. Freedman R, Adler LE, Waldo MC, Pachtman E, Franks RD.Neurophysiological evidence for a defect in inhibitory pathwaysin schizophrenia: comparison of medicated <strong>and</strong> drugfreepatients. Biol Psychiatry 1983; 18(5): 537-551.71. Nagamoto HT, Adler LE, McRae KA, Huettl P, Cawthra E,Gerhardt G, et al. Auditory P50 in schizophrenics on clozapine:improved gating parallels clinical improvement <strong>and</strong>changes in plasma 3-methoxy-4-hydroxyphenylglycol.Neuropsychobiology 1999; 39(1): 10-17.72. Adler LE, Olincy A, Cawthra EM, McRae KA, Harris JG,Nagamoto HT, et al. Varied effects of atypical neuroleptics onP50 auditory gating in schizophrenia patients. Am JPsychiatry 2004; 161(10): 1822-1828.73. Myles-Worsley M, Ord L, Blailes F, Ngiralmau H, FreedmanR. P50 sensory gating in adolescents from a pacific isl<strong>and</strong>isolate with elevated risk for schizophrenia. Biol Psychiatry2004; 55(7): 663-667.74. Waldo MC, Carey G, Myles-Worsley M, Cawthra E, Adler LE,Nagamoto HT, et al. Codistribution of a sensory gating deficit<strong>and</strong> schizophrenia in multi-affected families. Psychiatry Res1991; 39(3): 257-268.75. Clementz BA, Geyer MA, Braff DL. Poor P50 suppressionamong schizophrenia patients <strong>and</strong> their first-degree biologicalrelatives. Am J Psychiatry 1998; 155(12):1691-1694.76. Freedman R, Olincy A, Ross RG, Waldo MC, Stevens KE,Adler LE, et al. The genetics of sensory gating deficits inschizophrenia. Curr Psychiatry Rep 2003; 5(2):155-161.77. Buchsbaum M, Silverman J. Stimulus intensity control <strong>and</strong>the cortical evoked response. Psychosom Med 1968; 30(1):12-22.78. Connolly JF, Gruzelier JH. Amplitude <strong>and</strong> latency changes inthe visual evoked potential to different stimulus intensities.Psychophysiology 1982; 19(6): 599-608.79. Dragutinovich S. Measurement <strong>and</strong> definition of changes inthe visual evoked potential to different stimulus intensities. IntJ Psychophysiol 1987; 5(2): 125-133.80. Carrillo-de-la-Pena MT. ERP augmenting/reducing <strong>and</strong> sensationseeking: a critical review. Int J Psychophysiol 1992;12(3): 211-220.81. Hegerl U, Gallinat J, Juckel G. Event-related potentials. Dothey reflect central serotonergic neurotransmission <strong>and</strong> dothey predict clinical response to serotonin agonists? J AffectDisord 2001; 62(1-2): 93-100.82. Juckel G, Csepe V, Molnar M, Hegerl U, Karmos G. Intensitydependence of auditory evoked potentials in behaving cats.Electroencephalogr Clin Neurophysiol 1996; 100(6): 527-537.83. Juckel G, Hegerl U, Molnar M, Csepe V, Karmos G. Auditoryevoked potentials reflect serotonergic neuronal activity—astudy in behaving cats administered drugs acting on 5-HT1Aautoreceptors in the dorsal raphe nucleus. Neuropsychopharmacology1999; 21(6): 710-716.84. Naatanen R, Picton T. The N1 wave of the human electric<strong>and</strong> magnetic response to sound: a review <strong>and</strong> an analysis ofthe component structure. Psychophysiology 1987; 24(4):375-425.85. Hegerl U, Gallinat J, Mrowinski D. Intensity dependence ofauditory evoked dipole source activity. Int J Psychophysiol1994; 17(1): 1-13.86. Brechmann A, Baumgart F, Scheich H. Sound-level-dependentrepresentation of frequency modulations in human auditorycortex: a low-noise fMRI study. J Neurophysiol 2002;87(1): 423-433.87. Mulert C, Jager L, Propp S, Karch S, Leicht G, Pogarell O, etal. Loudness dependence of the primary auditory cortex asan indicator of central serotonergic transmission: combinationof <strong>EEG</strong> <strong>and</strong> fMRI. Neuroimage 2004; 22: (suppl 1),TU356.88. Tuchtenhagen F, Daumann J, Norra C, Gobbele R, Becker S,Pelz S, et al. High intensity dependence of auditory evokeddipole source activity indicates decreased serotonergic activityin abstinent ecstasy (MDMA) users. Neuropsychopharmacology2000; 22(6): 608-617.89. Croft RJ, Klugman A, Baldeweg T, Gruzelier JH.Electrophysiological evidence of serotonergic impairment inlong-term MDMA (“ecstasy”) users. Am J Psychiatry 2001;158(10):1687-1692.90. Norra C, Mrazek M, Tuchtenhagen F, Gobbele R, Buchner H,Sass H, et al. Enhanced intensity dependence as a marker oflow serotonergic neurotransmission in borderline personalitydisorder. J Psychiatr Res 2003; 37(1): 23-33.91. Hegerl U, Juckel G. Intensity dependence of auditoryevoked potentials as an indicator of central serotonergicneurotransmission: a new hypothesis. Biol Psychiatry 1993;33(3): 173-187.92. Mulert C, Juckel G, Augustin H, Hegerl U. Comparisonbetween the analysis of the loudness dependency of theauditory N1/P2 component with LORETA <strong>and</strong> dipole sourceanalysis in the prediction of treatment response to the selectiveserotonin reuptake inhibitor citalopram in major depression.Clin Neurophysiol 2002; 113(10): 1566-1572.93. Gallinat J, Bottlender R, Juckel G, Munke-Puchner A, StotzG, Kuss HJ, et al. The loudness dependency of the auditoryevoked N1/P2-component as a predictor of the acute SSRIresponse in depression. Psychopharmacology (Berl) 2000;148(4): 404-411.94. Pogarell O, Tatsch K, Juckel G, Hamann C, Mulert C, PopperlG, et al. Serotonin <strong>and</strong> dopamine transporter availabilitiescorrelate with the loudness dependence of auditory evokedpotentials in patients with obsessive-compulsive disorder.Neuropsychopharmacology 2004; 29(10):1910-1917.95. Gallinat J, Senkowski D, Wernicke C, Juckel G, Becker I,S<strong>and</strong>er T, et al. Allelic variants of the functional promoterpolymorphism of the human serotonin transporter gene isassociated with auditory cortical stimulus processing.Neuropsychopharmacology 2003; 28(3): 530-532.33
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 196. Pogarell O, Poepperl G, Mulert C, Hamann C, Sadowsky N,Riedel M, et al. SERT <strong>and</strong> DAT availabilities under citalopramtreatment in obsessive-compulsive disorder (OCD). EurN e u r o p s y c h o p h a r m a c o l o g y. In press.97. Paige SR, Fitzpatrick DF, Kline JP, Balogh SE, Hendricks SE.Event-related potential amplitude/intensity slopes predictresponse to antidepressants. Neuropsychobiology 1994;30(4): 197-201.98. Paige SR, Hendricks SE, Fitzpatrick DF, Balogh S, Burke WJ.Amplitude/intensity functions of auditory event-related potentialspredict responsiveness to bupropion in major depressived i s o r d e r. Psychopharmacol Bull 1995; 31(2): 243-248.99. Muller-Oerlinghausen B. Lithium long-term treatment—does itact via serotonin? Pharmacopsychiatry 1985; 18(2): 214-217.100. Baron M, Gershon ES, Rudy V, Jonas WZ, Buchsbaum M.Lithium carbonate response in depression: prediction byunipolar/bipolar illness, average-evoked response, catechol-O-methyl transferase, <strong>and</strong> family history. Arch GenPsychiatry 1975; 32(9): 1107-1111.101. Buchsbaum M, Goodwin F, Murphy D, Borge G. AER in affectivedisorders. Am J Psychiatry 1971; 128(1): 19-25.102. McKnew DH, Cytryn L, Buchsbaum MS, Hamovit J, LamourM, Rapoport JL, et al. Lithium in children of lithium-respondingparents. Psychiatry Res 1981; 4(2): 171-180.103. Hegerl U, Ulrich G, Muller-Oerlinghausen B. Auditory evokedpotentials <strong>and</strong> response to lithium prophylaxis.Pharmacopsychiatry 1987; 20(5): 213-216.104. Hegerl U, Wulff H, Muller-Oerlinghausen B. Intensity dependenceof auditory evoked potentials <strong>and</strong> clinical response toprophylactic lithium medication: a replication study. PsychiatryRes 1992; 44(3): 181-190.Conclusion of:Special IssueThe Electrophysiology of <strong>Memory</strong>: Section IIClinical Studies34
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Spatial-Temporal Current SourceCorrelations <strong>and</strong> Cortical ConnectivityR. W. Thatcher, C. J. Biver <strong>and</strong> D. NorthKey WordsCortical ConnectionsCortico-cortical Connectivity ModelIntra-hemispheric AsymmetryLORETASource CorrelationsABSTRACTThe purpose of this study was to explore spatial-temporalcorrelations between 3-dimensional current density estimatesusing Low Resolution Electromagnetic Tomography(LORETA).The electroencephalogram (<strong>EEG</strong>) was recorded from19 scalp locations from 97 subjects. LORETA current densitywas computed for 2,394 gray matter pixels. The graymatter pixels were grouped into 33 left hemisphere <strong>and</strong> 33right hemisphere regions of interest (ROIs) based ongroupings of Brodmann areas. The average source currentdensity in a given region of interest (ROI) was computedfor each 2 second epoch of <strong>EEG</strong> <strong>and</strong> then a Pearson productcorrelation coefficient was computed over the timeseries of successive 2 second epochs of current densitybetween all pairwise combinations of ROIs during the restingeyes-closed <strong>EEG</strong> session.Rhythmic changes in source correlation as a function ofdistance were present in all regions of interest. Also, maximumcorrelations at certain frequencies were presentindependent of distance. The occipital regions exhibitedthe highest short distance correlations <strong>and</strong> the frontalregions exhibited the highest long distance correlations. Ingeneral, the right hemisphere exhibited higher intra-hemisphericsource correlations than the left hemisphere especiallyin the temporal, parietal <strong>and</strong> occipital cortex. Thestrongest left vs. right hemisphere differences were in thealpha frequency b<strong>and</strong> (8-12 Hz) <strong>and</strong> in the gamma frequencyb<strong>and</strong> (37-40 Hz).The pattern of spatial frequencies in different corticallobules is consistent with differences in neural packing density<strong>and</strong> the operation of ‘U’ shaped fiber systems. The generalconclusions were: 1- the higher the packing densitythen the greater the intra-cortical connection contribution toL O R E TA source correlations, 2- spatial frequencies are primarilydue to intra-cortical ‘U’ shaped fiber connections <strong>and</strong>long distance fiber connections, 3- posterior <strong>and</strong> temporalcortical intra-hemispheric coupling is generally stronger inthe right hemisphere than in the left hemisphere.INTRODUCTIONNeural dynamics involves the generation of electricalcurrents by populations of synchronously active neuronswithin local regions of the brain which are coupled throughaxonal connections to other populations of neurons. 1 - 4Anatomical analyses of the cerebral white matter haveshown that there are three general categories of corticocortcalconnections: 1- intra-cortical unmyelinated connectionswithin the gray matter on the order of 1 mm to approximately3 mm, 2- short-distance ‘U’ shaped fibers in thecerebral white matter located beneath the gray matter (10mm to approx. 30 mm) <strong>and</strong>, 3- long distance fasciculi locatedin the deep white matter below the ‘U’ shaped fibers withdistances from 30 mm to approx. 170 mm. 3 , 4 Measures of<strong>EEG</strong> coherence <strong>and</strong> phase delays from the scalp surfacecommonly detect the presence of two compartments withan approximate correspondence with the short distance<strong>and</strong> long distance fiber systems. 1 , 2 , 5 - 7 For example, studiesby Nunez 1 <strong>and</strong> Thatcher et al 5 showed that <strong>EEG</strong> coherencedecreases as a function of distance from any electrode site,thus characterizing the short distance compartment <strong>and</strong>coherence increases as a function of distance beyondapproximately 10-14 cm, which characterizes the long distancecompartment. Studies of changes of <strong>EEG</strong> coherencewith distance are usually explained by a decrease in thenumber of connections as a function of distance from anygiven population of neurons, while increased coherencewith distance is explained by an increase of connectionsbetween two populations through axons <strong>and</strong> fasciculi of thedeep cerebral white matter. 1 - 6A deeper underst<strong>and</strong>ing of cortical coupling is possibleby studying the correlations between current sourcesderived from the surface <strong>EEG</strong> using an inverse method. 8 - 1 0Thatcher et al 8 recorded <strong>EEG</strong> during voluntary finger move-From the Department of <strong>EEG</strong> <strong>and</strong> NeuroImaging <strong>Lab</strong>oratory (R. W.Thatcher, C. J. Biver, D. North) Bay Pines VA Medical Center, St.Petersburg, Florida, <strong>and</strong> the Department of Neurology (R. W. Thatcher),University of South Florida College of Medicine, Tampa, Florida.Addresss requests for reprints to Robert W. T h a t c h e r, PhD,NeuroImaging <strong>Lab</strong>oratory, Research <strong>and</strong> Development Service-151,Veterans Administration Medical Center, Bay Pines, Florida 33744, USA.Email: rwthatcher@yahoo.comReceived: February 13, 2006; accepted: May 14, 2006.35
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1KeyInstituteTMatrixAverage theCorrelations invoxels withineach non-Reference ROISource Correlation Flow Chart19 ChannelsCross-SpectrumSq Rootof Sum ofSquares ofx, y, zMomentsEach voxel& frequencyRepeat forall ROIs &All frequenciesReplaceEach voxelin referenceROI withThe averageCurrentDensityOrder ROIsBy distanceFrom theReference ROIComputeCorrelationBetween theReferenceROI <strong>and</strong> theRemainingvoxelsFigure 1.Flow chart of the procedures to compute LORETA source correlations.ments <strong>and</strong> derived three dipoles in the sensory-motor corticalregions that accounted for approximately 97% of the varianceof the surface <strong>EEG</strong> <strong>and</strong> were validated using PET a n dMRI. A pseudo-inverse procedure was then used to derivethree different time series from each of the three dipoles,<strong>and</strong> coherence <strong>and</strong> phase delays were computed betweenthe various combinations of dipole time series. Stable butrapid changes in correlations between sources were shownto be time locked to voluntary motor movements in the supplementalmotor cortex <strong>and</strong> the contra-lateral motor cortex. 8 , 9Hoechstetter et al 1 0 used a multiple dipole source solution forscalp <strong>EEG</strong> electrical potentials <strong>and</strong> then used coherence tocompute the correlation between the 3-dimensional currentsources <strong>and</strong> demonstrated changes in the correlationbetween current sources related to different tasks. Pascual-Marqui et al 11 used low resolution electromagnetic tomography(LORETA) to compute current sources <strong>and</strong> then used acorrelation coefficient to explore differences in source correlationsbetween a normal control group <strong>and</strong> a group of schizophrenicpatients. All of these studies revealed interesting<strong>and</strong> reproducible relations between current sources <strong>and</strong> networkconnectivity that provide a deeper underst<strong>and</strong>ing of thesurface <strong>EEG</strong> dynamics.A general limitation of all LORETA studies is the use of a“Low Resolution” point spread function by the Laplacianoperator when using 19 scalp electrodes. 1 2 For example, thespatial correlation of magnitudes is approximately unitybetween nearby voxels <strong>and</strong> decreases as a smooth <strong>and</strong>monotonic function of distance. However, the point spreadfunction is not a major difficulty when spatial correlations arecomputed over intervals of time, because the null hypothesisis that spatial frequency is constant over time <strong>and</strong>approximates a monotonic function. Significant deviationsfrom a monotonic function of distance are independent of thee ffects of a point-spread <strong>and</strong> therefore must be explained byother factors such as the anatomical location of spatio-temporallyassociated ROIs. A method employed in this study isto minimize the effects of point spread by clustering groupsof nearby voxels as “Regions of Interest” (ROIs) <strong>and</strong> thencompute the time covariance of current density magnitudes.The point-spread is constant over time, <strong>and</strong> thus spatial frequenciesof correlations can not be explained by a simplepoint-spread model of any <strong>EEG</strong> inverse solution.The purpose of the present paper is to evaluate the useof low resolution electromagnetic tomography (LORETA) tocompute the spatio-temporal correlation coefficient or temporalcovariance of current source density betweenregions of interest as defined by Brodmann areas. Specificexperimental hypotheses are: 1- source correlationsdecrease smoothly as a function of distance from a givenregion of interest (point-spread null hypothesis), 2- sourcecorrelations are isomorphic or uniform as a function of frequency(uniform resonance null hypothesis) <strong>and</strong> , 3- thereare no differences in intra-hemispheric source correlationsbetween homologous left <strong>and</strong> right hemisphere locations(hemispheric null hypothesis).METHODSSubjectsA total of 97 normal adults ranging in age from 5 to 37(male = 58, mean age = 10.41 years, st<strong>and</strong>ard deviation ofage = 4.66) were included in this study. The subjects in thestudy were selected based on no history of neurologicaldisorders such as epilepsy, head injuries <strong>and</strong> reported normaldevelopment <strong>and</strong> successful school performance. AWechsler Intelligence test was administered to all subjects<strong>and</strong> the range of full scale I.Q. was 120 to 154. The agerange <strong>and</strong> gender proportion is the result of including allsubjects that met the no clinical disorder criteria <strong>and</strong> withI.Q. scores > 120.<strong>EEG</strong> recordingThe <strong>EEG</strong> was recorded from 19 scalp locations basedon the International 10/20 System of electrode placement,using linked ears as a reference. Each <strong>EEG</strong> record wasplotted <strong>and</strong> visually examined <strong>and</strong> then edited to removeartifact. The amplifier b<strong>and</strong>widths were nominally 0.5 to 40Hz, the outputs being 3 db down at these frequencies, <strong>and</strong>the sample rate was 128 Hz. Split-half <strong>and</strong> test-re-test reliabilitymeasures were conducted on the edited <strong>EEG</strong> segments<strong>and</strong> only records with > 95% reliability were enteredinto the spectral analyses. <strong>EEG</strong> was acquired in the eyesclosedconditions <strong>and</strong> record lengths varied from 58.6 secondsto 120 seconds.Cross-spectral analysis <strong>and</strong> LORETA computationThe temporal covariance or correlation of LORETAcurrent density between successive 2 second FFTepochs over the 58 second to 120 seconds is the subjectof this study. The steps to compute the desired spatialtemporalcorrelations between regions of interest aredescribed in Figure 1. First step is the digitized <strong>EEG</strong> samplesdivided into successive 2 second epochs of 256sample points of the edited <strong>EEG</strong> then FFT c r o s s - s p e c t r a lanalysis using a cosine taper window according to st<strong>and</strong>ardprocedures for LORETA frequency analyses. 1 3 - 1 5 I n36
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Table 1Examples of spatial ordering of ROIs for the superior frontal gyrus <strong>and</strong> the middle occipital gyrusSuperior Frontal GyrusMiddle Occipital GyrusRegion (mm) Region (mm)MFG Medial Frontal Gyrus 17.63 IOG Inferior Occipital Gyrus 13.96MidFG Middle Frontal Gyrus 20.82 SOG Superior Occipital Gyrus 20.47AC Anterior Cingulate 26.24 AG Angular Gyrus 29.91IFG Inferior Frontal Gyrus 40.21 LG Lingual Gyrus 30.03EN Extra-Nuclear 48.66 Cu Cuneus 31.64PreCG Precentral Gyrus 52.96 PC Posterior Cingulate 38.38SG Subcallosal Gyrus 51.08 SMG Supramarginal Gyrus 43.02CG Cingulate Gyrus 53.33 FG Fusiform Gyrus 44.56OG Orbital Gyrus 51.68 PCu Precuneus 45.84RG Rectal Gyrus 52.77 MTG Middle Temporal Gyrus 48.94In Insula 55.48 IPL Inferior Parietal Lobule 50.95SubG Sub-Gyral 70.97 SPL Superior Parietal Lobule 52.28TTG Transverse Temporal Gyrus 70.06 SubG Sub-Gyral 58.55PCG Postcentral Gyrus 72.97 PHG Parahippocampal Gyrus 59.42STG Superior Temporal Gyrus 71.42 ITG Inferior Temporal Gyrus 60.37Un Uncus 72.51 PCG Postcentral Gyrus 63.26PCL Paracentral Lobule 76.40 STG Superior Temporal Gyrus 63.46PHG Parahippocampal Gyrus 76.13 TTG Transverse Temporal Gyrus 67.00IPL Inferior Parietal Lobule 88.27 In Insula 72.50MTG Middle Temporal Gyrus 87.54 PCL Paracentral Lobule 74.46ITG Inferior Temporal Gyrus 89.62 CG Cingulate Gyrus 80.05SMG Supramarginal Gyrus 95.80 PreCG Precentral Gyrus 81.57PC Posterior Cingulate 96.81 Un Uncus 83.70FG Fusiform Gyrus 96.36 EN Extra-Nuclear 91.62SPL Superior Parietal Lobule 102.72 SG Subcallosal Gyrus 93.98PCu Precuneus 104.04 IFG Inferior Frontal Gyrus 103.83AG Angular Gyrus 108.61 MidFG Middle Frontal Gyrus 111.36LG Lingual Gyrus 115.04 AC Anterior Cingulate 114.05Cu Cuneus 119.81 MFG Medial Frontal Gyrus 116.70SOG Superior Occipital Gyrus 122.93 RG Rectal Gyrus 119.03MOG Middle Occipital Gyrus 122.70 SFG Superior Frontal Gyrus 122.70IOG Inferior Occipital Gyrus 127.90 OG Orbital Gyrus 133.22order to reduce the number of variables, adjacent frequency0.5 Hz b<strong>and</strong>s were averaged to produce a 1 Hzresolution thus yielding a total of 40 frequency b<strong>and</strong>sfrom 1 to 40 Hz. The Key Institute software was used tocompute the T matrix according to the Talairach A t l a scoordinates of the Montreal Neurological Institute’s MRIaverage of 305 brains. 1 2 - 1 6 Based on the equations of theKey Institute 1 5 the diagonal elements (autospectrum) ofthe Hermitian cross-spectral matrix were multiplied by theT matrix at each 1 Hz frequency b<strong>and</strong> for each 2 secondepoch. The T matrix is a 3-dimensional matrix of x, y <strong>and</strong>z current source moments in each of the 2,394 gray matterpixels. The resultant current source vector at eachvoxel was computed as the square root of the sum of thesquares for the x, y <strong>and</strong> z source moments for each 1 Hzfrequency b<strong>and</strong>.Regions of interest (ROIs)The anatomical names <strong>and</strong> Brodmann areas that correspondto each of the 2,394 gray matter pixels in TalairachAtlas coordinates was provided by Lancaster et al 16 asused by the Key Institute software, Pascual-Marqui. 15 TheKey Institute’s first best match to a given region of interest(ROI) was used for both Brodmann area values <strong>and</strong>anatomical names. After computing the LORETA sourcecurrents for each of the 2,394 gray matter pixels the Key-Talairach table of gray matter pixels was sorted by anatomicalname <strong>and</strong> an average current source density for agiven ROI was computed by summing the current valuesfor each of the gray matter pixels in an ROI <strong>and</strong> then dividingby the number of pixels. This resulted in a total of 66different averages of current source density for each 2 secondepoch (33 ROIs from the left hemisphere <strong>and</strong> 33 ROIs37
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1from the homologous right hemisphere). A second level ofaveraging involved averaging the current source densitiesin the four general Brodmann lobules of frontal, temporal,parietal <strong>and</strong> occipital, which yielded eight lobules of averagedcurrent source density, four left <strong>and</strong> four right hemispherelobules. An example of the spatial ordering <strong>and</strong>designations of regions of interest for the superior frontalgyrus <strong>and</strong> the middle occipital gyrus are shown in Table 1.Source correlationsThe current values within a selected ROI were averaged<strong>and</strong> each voxel in the selected ROI was replaced withthe average value <strong>and</strong> the ROI with average current densityvalues is called a “reference ROI.” Then a PearsonProduct correlation coefficient was computed between thereference ROI average current value <strong>and</strong> the current densityvalues in the remainder of the 2,394 pixels as thecovariance of magnitudes over the time series of 2 secondepochs. The average correlation between a given referenceROI <strong>and</strong> a different ROI was computed by averagingthe correlation coefficients between the reference ROI <strong>and</strong>the individual voxels that comprise a given ROI. This procedurewas repeated for each of the 66 ROIs. The averagecorrelation values range from -1 to +1, <strong>and</strong> the statisticalsignificance level is determined by the number of degreesof freedom or the total number of 2 second epochs thatspan a given time series. For example, the time seriesdegrees of freedom in this study ranged from 29 to 60 forthe range of 58 seconds to 120 seconds <strong>EEG</strong> recordings.Figure 1 is a diagrammatic illustration of the computationalmethods used to compute the Pearson product sourcecorrelations over the time interval of the recording period.The computational steps are shown in separate blocks.Distance metric of current source correlationsA Euclidean distance metric was computed for eachregion of interest in two steps. Step one computed a separateaverage of the x, y <strong>and</strong> z Talairach atlas coordinatesof each voxel within a region of interest. Step two involvedcomputing the square root of the sum of the squares ofabsolute distance between the average x, y <strong>and</strong> z coordinatesof a reference ROI with respect to a different ROI.The computation of the absolute distance is the diff e r e n c ebetween the average X of a reference ROI (i.e., X 1 ) <strong>and</strong>the average X coordinate of a second ROI (i.e., X 2 ) <strong>and</strong>the same for the Y <strong>and</strong> Z coordinates. The diff e r e n c ebetween the x, y <strong>and</strong> z coordinates is then squared <strong>and</strong>the square root was computed on the sum of the squaresas shown in equation 1.Eq. 1 - D = √ (X_1 - X_ 2 )2 + (Y _ 1 - Y_ 2 )2 + (Z _ 1 - Z_ 2 )2Where the bar above x, y <strong>and</strong> z denotes the average x,y <strong>and</strong> z coordinate value for a given ROI, therefore, a centerof mass coordinate value for each ROI.The ROIs were then ordered as a function of Euclide<strong>and</strong>istance with respect to a given reference ROI. Examplesof the spatial ordering of ROIs are shown in Table 1 for referenceROIs being the superior frontal gyrus <strong>and</strong> the middleoccipital gyrus.RESULTSSpatial <strong>and</strong> temporal heterogeneityof source correlationsFigures 2 <strong>and</strong> 3 are examples of contour maps of sourcecorrelations from two different subjects for the left <strong>and</strong> righthemisphere frontal ROIs <strong>and</strong> left <strong>and</strong> right hemisphereoccipital ROIs. Because of space limitations it was not possibleto show contour maps of all 97 subjects. The two subjectsselected are exemplars <strong>and</strong> typical of the source correlationsfound in all of the subjects. There was great consistency<strong>and</strong> similarity across subjects. These are examples ofthe general pattern of maximal source correlations at shortdistance distances (e.g., 13 mm to approx. 3 cm) in occipitalregions <strong>and</strong> maximal source correlations at longer distancesin frontal cortical regions (e.g., 3 cm to approx. 13 cm). It canbe seen in Figures 2 <strong>and</strong> 3 that there are higher short distancecorrelations when using the occipital reference ROIthan the frontal reference ROI. All of the subjects in thisstudy exhibited horizontal b<strong>and</strong>s <strong>and</strong> spatial frequencies ora pattern of increasing <strong>and</strong> decreasing correlations as afunction of distance from the reference ROI.In occipital regions, the frequency of maximal shortdistance source correlations was essentially uniform from1 to approximately 40 Hz with longer distance high sourcecorrelations between 35 to 40 Hz. In contrast, frontal corticalregions exhibited more heterogeneity with maximalsource correlations at different frequencies <strong>and</strong> at a varietyof intra-hemispheric distances. All cortical regionstended to show higher correlations between 35 to 40 Hzthan at lower frequencies.Figure 4 shows increases <strong>and</strong> decreases as a functionof distance with respect to the middle occipital gyrus(dashed lines) <strong>and</strong> middle temporal gyrus (solid lines) fromthe left hemisphere (left) <strong>and</strong> right hemisphere (right). In allsubjects, the occipital regions exhibited maximum sourcecorrelations at short distances with a rhythmic decline incorrelation as a function of distance. In contrast, the temporalregions showed maximal source correlations at longdistances <strong>and</strong> a pronounced rhythmic pattern as a functionof distance.Hemispheric differences in source correlationsFigure 5, top left, shows average source correlationsacross all subjects (N = 97) from the left superior frontalgyrus, top right are the average source correlations fromthe homologous right superior frontal gyrus <strong>and</strong> in the middleare the results of t-tests between the source correlationsin the left <strong>and</strong> right intra-hemispheric superior frontalgyrus. The z-axis is color scaled as shown by the color bar.The x-axis is frequency (Hz), <strong>and</strong> the y-axis are regions ofinterest that were ordered as a function of distance fromthe superior frontal gyrus. The ordered distances betweenthe reference ROI (superior frontal gyrus) <strong>and</strong> the remain-38
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Subjects:Left FrontalLeft Occipital1.IOGSOGMOGCuLGAGSPLPCuSMGFGPCIPLMTGITGPCGPCLTTGSTGPHGSubGUnPreCGInCGENOGRGIFGSGMidFGSFGAC5 10 15 20 25 30 35 40OGSFGRGMidFGMFGIFGACENSGPreCGUnInITGTTGSTGPCGCGMTGPHGSubGPCLIPLFGSMGSPLAGIOGPCuMOGSOGPCLG5 10 15 20 25 30 35 40FREQUENCY (Hz)FREQUENCY (Hz)2.CuIOGLGOGMOGSOGRGPCuPCSPLAGUnFGPCLACSGMFGITGPHGSFGCGMTGSMGIPLIFGENSubGMidFGSTGInTTGPCG5 10 15 20 25 30 35 40OGSFGMidFGMGFRGACIFGENPreCGSGUnPCGInTTGCGPCLSTGIPLITGSMGSPLMTGSubGPHGAGFGPCuSOGMOGIOGPCCu5 10 15 20 25 30 35 40FREQUENCY (Hz)FREQUENCY (Hz)3.CuSOGMOGIOGPCuLGSPLAGPCPCLSMGIPLFGPCGCGMTGITGPHGTTGSubGOGSTGUnSFGPreCGMFGRGACSGInMidFGENOGSFGMidFGMGFRGACIFGENPreCGSGUnPCGInTTGCGPCLSTGIPLITGSMGSPLMTGSubGPHGAGFGPCuSOGMOGIOGPCCu5 10 15 20 25 30 35 40 5 10 15 20 25 30 35 40FREQUENCY (Hz)FREQUENCY (Hz)Figure 2.Two-dimensional contour maps of the source correlations from two typical or examplar subjects from the left hemisphere superior frontalgyrus (left column) <strong>and</strong> the left hemisphere middle occipital gyrus (right column). The x-axis is frequency (1 to 40 Hz), the y-axis areROIs that are ordered as a function of distance from the left superior frontal ROI (left column) <strong>and</strong> the left hemisphere middle occipitalgyrus (right column). The z-axis is the magnitude of correlation as represented by the color bar under each contour map. The distancesin the left column vary from 17.63 mm starting with the left hemisphere medial frontal gyrus that is the nearest ROI to the farthest distantROI which is the left hemisphere inferior occipital gyrus (127.90 mm distant). The distances from the middle occipital gyrus in the rightcolumn vary from 13.96 mm for the left inferior occipital gyrus that is the nearest ROI to the most distant ROI which is the left hemisphereorbital frontal gyrus (132.22 mm distant). It can be seen that the occipital region exhibits shorter distance high source correlationsthan does the frontal region. See Table 1 for the names of the abbreviated ROIs <strong>and</strong> the distances from the reference ROI in millimeters.39
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Right Superior Frontal Gyru sRight Middle Occipital Gyru sIOGSOGMOGCuLGAGPCuSPLSMGPCFGIPLITGMTGPCLPHGPCGSTGSubGUnTTGInCGPreCGRGSGOGENIFGACMidFGMFG5 10 15 20 25 30 35 40OGSFGRGMFGACMidFGIFGSGENUnPreCGCGPCLInTTGSTGPCGITGSubGPHGSPLIPLMTGPCuFGSMGPCCuLGAGSOGIOG5 10 15 20 25 30 35 40IOGSOGMOGCuLGAGPCuSPLSMGPCFGIPLITGMTGPCLPHGPCGSTGSubGUnTTGInCGPreCGRGSGOGENIFGACMidFGMFGFREQUENCY (Hz)FREQUENCY (Hz)OGSFGRGMFGACMidFGIFGSGENUnPreCGCGPCLInTTGSTGPCGITGSubGPHGSPLIPLMTGPCuFGSMGPCCuLGAGSOGIOG5 10 15 20 25 30 35 40 5 10 15 20 25 30 35 40FREQUENCY (Hz)FREQUENCY (Hz)Figure 3.Two-dimensional contour maps of the source correlations from the same two subjects as in Figure 2 but from the homologous righthemisphere superior frontal gyrus (left column) <strong>and</strong> the homologous right hemisphere middle occipital gyrus (right column). The x-axis isfrequency (1 to 40 Hz), the y-axis are ROIs that are ordered as a function of distance from the superior frontal ROIt (left column) <strong>and</strong> themiddle occipital gyrus (right column). The z-axis is the magnitude of correlation as represented by the color bar under each contour map.The distances in the left column vary from 17.63 mm starting with the right hemisphere medial frontal gyrus that is the nearest ROI tothe farthest distant ROI which is the right hemisphere inferior occipital gyrus (127.90 mm distant). The distances from the middle occipitalgyrus in the right column vary from 13.96 mm for the left inferior occipital gyrus that is the nearest ROI to the most distant ROI whichis the left hemisphere orbital frontal gyrus (132.22 mm distant). It can be seen that the occipital region exhibits shorter distance highsource correlations than does the frontal region. It can be seen that the right occipital region exhibits high source correlations at shorterdistances than does the right hemisphere frontal region. See Table 1 for the names of the abbreviated ROIs. See Table 1 for the namesof the abbreviated ROIs <strong>and</strong> the distances from the reference ROI in millimeters.ing ROIs are shown in Table 1. T-test values less than P >.05 are colored green, while t-test differences where leftintra-hemispheric source correlations are greater than thehomologous right intra-hemispheric source correlations(positive) are colored orange to red. T-test differenceswhere the right hemisphere source correlations weregreater than the homologous left hemisphere source correlations(negative) are colored blue to purple. It can be seenthat left superior frontal gyrus source correlations are significantlygreater than right hemisphere source correlations(i.e., orange <strong>and</strong> red colors) especially at short distances<strong>and</strong> at frequencies greater than 20 Hz. The long distancesource correlations (96 mm to 127 mm) are greater in theright superior frontal gyrus (i.e., blue <strong>and</strong> purple colors)than in the homologous left superior frontal gyrus, especiallybetween 1 <strong>and</strong> 20 Hz.Figure 6 top left are average source correlations (N =97) from the left middle occipital gyrus, top right are theaverage source correlations from the homologous rightmiddle occipital gyrus, <strong>and</strong> the middle are the results of t-tests between the source correlations in the left <strong>and</strong> righthemispheric middle occipital gyrus. The axes <strong>and</strong> colorscaling are the same as in Figure 5. T-test values less thanP > .05 are colored green while t-test differences where lefthemisphere source correlations are greater than thehomologous right hemisphere source correlations (posi-40
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Figure 4.In the left column are meansource correlations from theleft hemisphere middle temporalgyrus (solid line) <strong>and</strong>the left hemisphere middleoccipital gyrus (dotted lines)at 9 Hz. In the right columnare mean source correlationsfrom the homologousright hemisphere middletemporal gyrus (solid line)<strong>and</strong> the right hemispheremiddle occipital gyrus (dottedlines) at 9 Hz. The y-axis is mean source correlation<strong>and</strong> the x-axis is theordered distance (millimeters)from the middle temporal<strong>and</strong> middle occipitalgyri to the remaining ROIs.A linear decline in source1.0000.9000.8000.7000.6000.5000.4000.3000.2000.100LO R E TA MEAN SOURCE CORRELATIONs at 9HzLeft HemisphereTEMPORALMiddle Temporal Gyrus0.0001 4 8 12 16 20 24 28 32ORDERED DISTANCEs (mm)OCCIPITALMiddle Occipital GyrusRight Hemispherecorrelation is seen with occipital reference ROIs (dotted lines) where as there is a more complex spatial relationship with the temporal referenceROIs (solid line).1.0000.9000.8000.7000.6000.5000.4000.3000.2000.1000.0001 4 8 12 16 20 24 28 32ORDERED DISTANCEs (mm)tive) are colored orange to red. T-test differences wherethe right hemisphere source correlations were greater thanthe homologous left hemisphere source correlations (negative)are colored blue to purple. In contrast to the superiorfrontal gyrus, the right middle occipital gyrus source correlationsare significantly greater than left hemispheresource correlations (i.e., blue <strong>and</strong> purple colors) especiallyat middle to long distances (43 mm to 94 mm) especially inthe 1 to 15 Hz range. In general, the right hemisphereoccipital source correlations are greater than the lefthomologous left hemisphere occipital regions.Hemispheric differences in regionsof interest independent of frequencyIn order to evaluate <strong>and</strong> summarize the strength of thehemispheric differences in source correlations the number ofstatistically significant t-tests (P < .05) were tabulated for thefour lobules (frontal, temporal, parietal <strong>and</strong> occipital) by combiningregions of interest that are contained within a givenlobule. Figure 7 shows the tabulation of statistically significantt-tests in lobules independent of frequency. The ROIsthat comprise a given lobule are on the x-axis <strong>and</strong> the numberof statistically significant t-tests (P < .05) are on the y-axis. T-tests where the left hemisphere source correlationswere significantly greater than the homologous right hemisphereare represented by the open bars <strong>and</strong> t-tests wherethe right hemisphere source correlations were significantlygreater than the homologous left hemisphere are representedby the black bars. The total number of t-tests equals thenumber of ROIs or 32 times the 40 frequencies = 1,280. Onewould expect 64 statistically significant t-tests by chancealone at P < .05. It can be seen that only the frontal lobulesexhibited greater left than right hemisphere source correlations,with the exception of the pre-central gyrus whichexhibited greater right hemisphere source correlations thanleft hemisphere. All other lobules (temporal, parietal <strong>and</strong>occipital) exhibited greater right hemisphere source correlationsthan the left hemisphere. The greatest right hemisphereasymmetry in the temporal lobule was in the inferiortemporal gyrus (ITG), the greatest right hemisphere asymmetryin the parietal lobule was in the superior parietal lobule(SPL), <strong>and</strong> the greatest right hemisphere asymmetry inthe occipital lobule was in the middle occipital gyrus (MOG).Hemispheric differences in frequencyindependent of regions of interestFigure 8 shows the total number of statistically significantt-tests (P < .05) from 1 to 40 Hz for all ROIs combined.The total number of t-tests in this analysis equals the numberof ROIs or 33 times the remaining regions that are correlatedwith each region = 32 <strong>and</strong> 33 x 32 = 1,056. Onewould expect 53 statistically significant t-tests by chancealone at P < .05. The dashed lines represent right hemispheregreater than left hemisphere significant differences<strong>and</strong> the solid lines represent left hemisphere greater thanright. It can be seen that the alpha frequency b<strong>and</strong> (8 to 12Hz) exhibited the greatest right > left hemispheric differences.In contrast, the left hemisphere exhibited greatersource correlations than the homologous right hemispherein the higher frequency range, 37 - 40 Hz.Figure 9 shows a break down of the overall summary ofstatistically significant t-tests as a function of lobule <strong>and</strong>frequency. The total number of t-tests in this analysis is differentfor each lobule, because each lobule has a different41
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Frontal – Superior Frontal Gyru sSOGMOGIOGCuLGAGPCuSFGFGPCSMGITGMTGIPLPHGPCLUnSTGPCGTTGSubGInRGOGCGSGPreCGENIFGACMidFGMFGLEFTIOGSOGMOGCuLGAGPCuSPLSMGPCFGIPLITGMTGPCLPHGPCGSTGSubGUnRIGHTMidFGMFG5 10 15 20 25 30 35 40 5 10 15 20 25 30 35 40TTGInCGPreCGRGSGOGENSFGAGF R E QUENCY (Hz)F R E QUENCY (Hz)T-TESTs @ P = .05SOGMOGIOGCuLGAGPCuSFGFGPCSMGITGMTGIPLPHGPCLUnSTGPCGTTGSubGInRGOGCGSGPreCGENIFGACMidFGMFG5 10 15 20 25 30 35 40F R E QUENCY (Hz)Figure 5.Top left are mean source correlations from the left intra-hemisphere superior frontal gyrus <strong>and</strong> the top right are the mean source correlationsfrom the homologous right superior frontal gyrus. The y-axis are ROIs that are ordered as a function of distance from the superiorfrontal gyrus. The x-axis is frequency from 1 to 40 Hz <strong>and</strong> the z-axis is the magnitude of correlation as shown by the color bar. The middlecontour map are t-test values between the left <strong>and</strong> right hemisphere superior frontal gyrus. The z-axis is the magnitude of the t-valuesas shown in the color bar. See Table 1 for the listing of ROIs.number of ROIs. For the frontal lobule the total number oft-tests = 11 x 32 = 352 (18 by chance alone), parietal lobes= 9 x 32 = 288 (14 by chance alone), temporal lobes = 8 x32 = 256 (13 by chance alone) <strong>and</strong> the occipital lobes = 5x 32 = 160 (8 by chance alone). It can be seen that thereis a maximum in the alpha frequency range (8 - 12 Hz) inall lobules <strong>and</strong> the direction of differences in the alphab<strong>and</strong> is always right greater than left. With the exception ofthe occipital lobule, the left hemisphere source correlationsare greater than the homologous right hemisphere in thehigher frequency range (37 - 40 Hz).DISCUSSIONThe results of this study demonstrated spatial-temporalpatterns of correlation between <strong>EEG</strong> current sources withinspecific regions of the cortex. Contrary to a monotonic pointspreadfunction, spatial <strong>and</strong> temporal patterns were presentin all subjects as well as in averages from all ROIs. Spatialheterogeneity <strong>and</strong> anatomical specificity were consistentlydemonstrated by spatial rhythms of correlations at specificfrequencies that varied according to the location of the referenceregion of interest. Therefore, all three uniform nullhypotheses discussed in the Introduction can be rejected.42
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Occipital – Middle Occipital Gyru sLEFTRIGHTOGSFGOGSFGRGRGMFGMFGACMidFGACMidFGIFGIFGSGSGENENUnUnPreCGPreCGCGCGPCLPCLInInPCGTTGTTGSTGSTGPCGITGITGPHGSubGSubGPHGSPLSPLIPLIPLMTGMTGPCuPCuSMGFGFGSMGPCPCAGCuCuLGLGAGSOGSOGIOG5 10 15 20 25 30 35 40IOG5 10 15 20 25 30 35 40F R E QUENCY (Hz)F R E QUENCY (Hz)T-TESTs @ P = .05OGSFGRGMFGACMidFGIFGSGENUnPreCGCGPCLInPCGTTGSTGITGPHGSubGSPLIPLMTGPCuSMGFGPCAGCuLGSOGIOG5 10 15 20 25 30 35 40F R E QUENCY (Hz)Figure 6.Top left are mean source correlations from the left hemisphere middle occipital gyrus <strong>and</strong> the top right are the mean source correlationsfrom the right hemisphere middle occipital gyrus. The y-axis are ROIs that are ordered as a function of distance from the middle occipitalgyrus. The x-axis is frequency from 1 to 40 Hz <strong>and</strong> the z-axis is the magnitude of correlation as shown by the color bar. The middle contourmap are t-test values between the left <strong>and</strong> right hemisphere middle occipital gyrus. The z-axis is the magnitude of the t-values asshown in the color bar.The finding of spatio-temporal heterogeneity was observedin all of the individual subjects (Figures 2, 3, 4, 5). The occipitallobes exhibited maximum correlation at short distances(10 mm to approx. 20 mm) while the frontal lobes exhibitedmaximum correlations at longer distances (50 mm to 105mm), <strong>and</strong> the temporal <strong>and</strong> parietal lobes exhibited a mixtureof short <strong>and</strong> long distance correlations. All regions of interestexhibited rhythmic increases <strong>and</strong> decreases in spatial-temporalcorrelation as a function of distance. In this study thetemporal dimension is the correlation of current source densityfrom successive 2 second samples of alert eyes-closed<strong>EEG</strong> over an interval of time that varied between 58.6 to 120seconds. Similar heterogeneities were also observed inunpublished analyses of eyes-open <strong>EEG</strong> data. Importantly,each ROI exhibited maximum correlations to other ROIs atd i fferent frequencies. In general, short distance correlationstended to be frequency independent while long distance correlationswere more frequency specific. Further, longer interregiondistances were most strongly associated with higherfrequencies (20 - 40 Hz). These findings are similar to thosereported by Shen et al 7 using <strong>EEG</strong> coherence recorded fromarrays of subdural electrodes. For example, Shen et al 743
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Total Significant T- Tests @ P = .05 of Left with Right HemisphereFrontal Lobu l eTe m p o ral Lobu l eREGIONs of I N T E R E S TParietal Lobu l eREGIONs of I N T E R E S TOccipital Lobu l eREGIONs of I N T E R E S TREGIONs of I N T E R E S TFigure 7.Total number of statistically significant t-tests (P < .05) between the left <strong>and</strong> right hemisphere source correlations for different ROIs.Number of negative t-values is Right hemisphere > Left hemisphere <strong>and</strong> number of positive t-values is Left hemisphere > Right hemisphere.Top left are the number of statistically significant source correlations in different ROIs between the left <strong>and</strong> right frontal lobules.Top right are the number of statistically significant source correlations in different ROIs between the left <strong>and</strong> right temporal lobules.Bottom left are the number of statistically significant source correlations in different ROIs between the left <strong>and</strong> right parietal lobule <strong>and</strong>the bottom right are the number of statistically significant source correlations in different ROIs between the left <strong>and</strong> right occipital lobules.Oblique columns are positive t-values in which the left hemisphere source correlations are greater than the homologous right hemispheresource correlations. Black columns are negative t-values in which the right hemisphere source correlations are greater than thehomologous left hemisphere source correlations.reported that lower frequencies were associated with shortinterelectrode distances, <strong>and</strong> that specific locations in thesubdural grid of electrodes were associated with distantlocations at specific frequencies.Limitations of this studyAs mentioned in the Introduction a general limitation ofall LORETA studies is the use of a “Low Resolution” pointspread function by the Laplacian operator when using 19scalp electrodes (Pascual-Marqui. 12 A point-spread meansthat the spatial correlation is approximately unity betweennearby voxels <strong>and</strong> decreases as a monotonic function ofdistance. The design of the present study minimized theeffects of the point spread of current density estimates byclustering hundreds of nearby voxels into “Regions ofInterest” This strategy appears effective since if the pointspread function were dominant then there should alwaysbe high correlations near to the reference ROI, which iscontrary to the finding that only the occipital regions <strong>and</strong>not frontal regions exhibited short distance spatial correlations.In addition, the point spread function can not explainthe presence of spatial frequencies <strong>and</strong> maxima at longdistances (see Figures 2-8), because the correlations inthis study are spatial covariances of the time series of currentdensities <strong>and</strong> the point-spread function is constant asa function of time. Another limitation is the use of thePearson product correlation for the time series of magnitudesover time rather than the computation of coherence<strong>and</strong> phase. Coherence <strong>and</strong> phase are more fundamentalto the measures of oscillator coupling than is a spatial-temporalPearson product correlation coefficient of magni-44
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1400350300250200150100500Total Significant T- Tests using @ P = .05o f Left with Right Hemisphere Figure 8.Total number of statistically significantt-tests between the left <strong>and</strong> righthemisphere source correlations as afunction of frequency. The solid lineis positive t-values in which the lefthemisphere source correlations aregreater than the homologous right1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39F R E QUENCY (Hz)TOTAL SIG POS +TOTAL SIG NEG -hemisphere source correlations. Thedotted line is the number of negativet-values in which the right hemispheresource correlations aregreater than the homologous lefthemisphere source correlations. They-axis is the number of statisticallysignificant t-values (P < .05) <strong>and</strong> thex-axis is frequency from 1 to 40 Hz.tudes. Nevertheless, the Pearson product correlation coefficientis a valid measure especially when the intent is toestimate the covariance of magnitudes over a relative longinterval of time. Coherence <strong>and</strong> phase are valuable measures<strong>and</strong> we plan to implement these measures in thefuture. A passive condition such as eyes-closed resting isanother possible limitation because active task dynamicsmay be related to the strength <strong>and</strong> modulation of coupling.Source correlations <strong>and</strong> cortico-cortical connectivityThere were several consistent <strong>and</strong> distinct features inthe source correlations observed in this study. One distinctfeature was that all source correlations showed rhythmicincreases <strong>and</strong> decreases in the strength of correlation as afunction of distance from a ROI (Figures 2-9). Another distinctfeature was that the occipital lobes showed thestrongest correlations at short distances (2 mm to 20 mm)while the frontal lobes exhibited longer peak-to-peak correlationdistances than the occipital lobes. These findings areconsistent with the higher packing density of occipital lobescompared to the frontal lobes 17,18 <strong>and</strong> with distance estimatesof cortico-cortical ‘U’ shaped fiber bundles that connectcortical gyri <strong>and</strong> sulci. The findings are consistent witha ‘U’ shaped cortico-cortical connection system in the cerebralcortex.This model assumes that the short distance horizontalb<strong>and</strong>s, e.g., 1 cm to 3 cm observed in Figures 2 <strong>and</strong> 3 areinfluenced by the ‘U’ shaped cortico-cortical fiber systemsstudied by Schulz <strong>and</strong> Braitenberg 4 <strong>and</strong> Braitenberg 3 . Forexample, Schulz <strong>and</strong> Braitenberg 4 showed that there arethree categories of cortico-cortical connections in thehuman brain: 1- intra-cortical connections which representthe majority of cortical connections <strong>and</strong> are on the order of1 mm to approximately 5 mm <strong>and</strong> involve collateral axonalconnections that do not enter the cerebral white matter; 2-‘U’ shaped myelinated fibers representing the majority ofthe cerebral white matter that connect cortical gyri <strong>and</strong>sulci <strong>and</strong> are on the order of 3 mm to 3 cm <strong>and</strong>, 3- deeplylocated long distance fiber systems referred to as fasciculiwith connections from approximately 3 to 15 cm that representapproximately 4% of the cerebral white matter.The intra-cortical fiber system is too short at 1 to 3 mmfor the 19 lead or even 512 lead <strong>EEG</strong> to resolve at the scalpsurface (see system ‘A’ in Figure 10). Nonetheless, thee ffects of the intra-cortical system on the amplitude of the<strong>EEG</strong> are very strong, because fiber bundles carry actionpotentials that terminate that produce excitatory post-synapticpotentials <strong>and</strong> thereby synchronize activation of small tolarge domains of cells which produce currents that arerecorded electrically as the surface <strong>EEG</strong>. The LORETAinverse solution of the scalp-recorded <strong>EEG</strong> uses a Laplacianoperator to emphasize the contribution of distributed <strong>and</strong>synchronous current source activation, which must as a matterof physics be influenced by neuronal packing density,e.g., resulting in high occipital short distance correlations.The contribution of the ‘U’ shaped fiber system is seenbest in the horizontal b<strong>and</strong>s of high correlation at 30 mm toapproximately 60 mm such as in Figures 2 <strong>and</strong> 3. Supportfor a cortico-cortical ‘U’ shaped fiber hypothesis in the presentstudy is the finding of peak-to-peak correlation distancesthat ranged from approximately 20 mm to 40 mm (seeFigures 2-8), which is in the range of distances known toexist for the ‘U’ shaped fiber systems of the human brain.The ‘U’ shaped cortico-cortical fiber hypothesis is also supportedby the finding of a much smaller contribution by thelong distance connection system that was also observed,especially in frontal <strong>and</strong> occipital ROIs, <strong>and</strong> was on the orderof 8 to 12 cm, which is consistent with Schulz <strong>and</strong>B r a i t e n b e r g 4 (see Figures 2 <strong>and</strong> 3). Figure 10 is an illustra-45
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1F RO N TAL LO B E sFREQUENCY (HZ)TEMPORAL LO B E sT- Tests @ P = .05PA R I E TAL LO B E sFREQUENCY (HZ)O C C I P I TAL LO B E sFigure 9.Total number of statistically significantt-values (P < .05) betweenthe left <strong>and</strong> right hemispheresource correlations in four differentlobules at different frequencies.Negative t-values means the righthemisphere correlations > the lefthemisphere <strong>and</strong> positive t-valuesmean the left hemisphere correlations> right hemisphere. The topleft is from the frontal lobes, thetop right is from the parietal lobes,the bottom left is from the temporallobes <strong>and</strong> the bottom right is fromthe occipital lobes. The y-axis isthe number of statistically significantt-values (P < .05) <strong>and</strong> the x-axis is frequency from 1 to 40 Hz.FREQUENCY (HZ)FREQUENCY (HZ)CGSFGMFGRGACPCLMidFGSPLPCuCuCGPCGSGIFGLGSOGPCAGMOGENUnPCGIPLPreCGSMGInPGHTTGSubGFGITGSTGFigure 10.Diagrammatic illustration of a cortico-cortical connection model. Top is the organization of intra-cortical connections according to Schulz<strong>and</strong> Braitenberg. 4 A = gray matter intra-cortical connections, B = ‘U’ shaped white matter connections <strong>and</strong> C = long distance white matterconnections. Bottom is an exemplar contour map of source correlations in which the horizontal b<strong>and</strong>s of increasing <strong>and</strong> decreasingsource correlations correspond to the different cortico-cortical connection systems as described in the top of the figure.46
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1tion of a cortico-cortical connection model based on Shultz<strong>and</strong> Braitenberg 3 to explain the source correlation findings inthis study. Additional support for a cortico-cortical hypothesisis the finding of no difference in left <strong>and</strong> right hemispherepeak-to-peak spatial oscillations of source correlations,which is consistent with studies by Schulz <strong>and</strong> Braitenberg 4who failed to find significant hemispheric differences in thelength of the long distance <strong>and</strong> ‘U’ shaped fiber connections.The lack of difference in the distances between interpeakcorrelations in left <strong>and</strong> right hemispheres in the presentstudy indicates that the intrinsic fiber connection systemis an invariant <strong>and</strong> stable variable, which is similar forthe left <strong>and</strong> right hemispheres. Significantly, while interpeakdifferences are the same between left <strong>and</strong> right hemispheresthe magnitude of source correlations is generallygreater in the right hemisphere than in the left hemisphere(see Figures 7 <strong>and</strong> 8). This indicates that the number orstrength of intra-hemispheric connections, i.e., couplingmagnitude, is generally greater in the right hemispherethan in the left hemisphere. The exception is in the frontallobes <strong>and</strong> higher <strong>EEG</strong> frequencies.Evidence of cortico-cortical multiplexingAnother distinct feature of the correlation contour mapswas the presence of vertical b<strong>and</strong>s of high or low correlationat specific frequencies (see Figures 2-8). The alphafrequency b<strong>and</strong> was often prominent in occipital <strong>and</strong> parietalROIs <strong>and</strong> less prominent in temporal <strong>and</strong> frontal ROIs.The frontal <strong>and</strong> temporal ROIs often showed maximal correlationsat higher frequencies (e.g., 30-40 Hz), but eachROI showed maximal correlations at specific frequencieswith single or a particular group of ROIs (see Figures. 2, 3,4, 5, 7 <strong>and</strong> 11). These findings are similar to those reportedby Shen et al 7 using coherence of <strong>EEG</strong> recorded fromsubdural electrodes in which specific locations in the electrodegrid exhibited high coherence to another location butat a specific frequency. In fact, the authors reported thateach subdural electrode exhibited a unique spatial-frequencyrelationship to all other locations in the grid of electrodes;they presented a type of multiplexing model inwhich each domain of neurons communicated with allother domains but at specific frequencies. The presentfindings are consistent with the Shen et al 7 “spatial-spectralsignature of cortical synchrony” model of cortico-corticalcoupling. According to this model, each ROI is connectedto all other ROIs but a given region communicates at specificfrequencies.As presented previously, the individual subject findings<strong>and</strong> the statistically significant covariance between distantlocations of the brain over time at a specific frequency isevidence of a stable resonance. If we assume that the connectionsbetween two ensembles are stable <strong>and</strong> mediatedby axonal fibers which conduct all frequencies, then resonanceat a specific frequency occurs when phase lockingbetween the two connected neuronal ensembles is optimal.A model of the spatial frequency of current densityvariation between two distant locations at a given temporalfrequency is consistent with a stable ‘U’ shaped fiber system<strong>and</strong> long distance fasciculi in which all frequencies areconducted with the number of synapses <strong>and</strong> dendritic locationof synapses <strong>and</strong> thalamo-cortical synchronizing mechanismsgoverning the spatial covariances of a given ROI.Hemispheric differences in cortico-cortical connectivityThe results of this study showed that, in general, theright hemisphere exhibited higher intra-hemispheric sourcecorrelations than the left hemisphere, with the exception ofthe frontal lobes. Right greater than left was especially thecase for parietal <strong>and</strong> occipital lobules. The frontal <strong>and</strong> temporallobules showed higher left intra-hemispheric sourcecorrelations than in the homologous right hemispherebetween 1 to 5 Hz, 15 Hz <strong>and</strong> 35-40 Hz. The right intrahemisphericcorrelations were significantly greater than thehomologous left hemisphere at 10 Hz in all lobules. Theoccipital lobes were unique in that there were greater rightintra-hemispheric significant correlations than the homologousleft hemisphere at all frequencies.The largest hemispheric asymmetries were in the superiorparietal lobule <strong>and</strong> the inferior parietal lobule with greaterright intra-hemispheric source correlations than in thehomologous left hemisphere (see Figure 9). A rank orderingof the most statistically significant intra-hemispheric asymmetriesof the right greater than left hemisphere is: superiorparietal gyrus > inferior parietal gyrus > pre-central gyrus >middle occipital gyrus > inferior temporal gyrus > insula.The finding of greater right intra-hemispheric sourcecorrelations than in the left hemisphere is consistent withcoherence studies of the surface <strong>EEG</strong> in which there isgreater right hemispheric coherence than in the left hemispherein both longitudinal <strong>and</strong> cross-sectional studies.5,19,20 The LORETA current density findings in the presentstudy <strong>and</strong> the surface <strong>EEG</strong> findings are also consistentwith MRI studies showing a higher white matter to graymatter ratio in the right hemisphere in comparison to theleft. 21 For example, the left hemisphere is more highly fissuredthan the right 22 with a higher density of cells in the leftthan in the right hemisphere, 23 as well as a longer planumtemporale <strong>and</strong> longer sylvian fissure in the left hemisphere.24,25 The findings from these studies <strong>and</strong> the presentstudy when taken as a whole indicate that the organizationof the left hemisphere favors processing or transfer withincortical regions, whereas the right hemisphere is morespecialized for the processing or integration of informationacross regions. Given these considerations, the findings inthe present study are consistent with functional differencesbetween the human left <strong>and</strong> right hemispheres in which theleft hemisphere is involved in analytical <strong>and</strong> sequential processingin contrast to the right hemisphere which is moreinvolved in synthesis <strong>and</strong> integration <strong>and</strong> relational functions.26 More specifically, the left hemisphere has been47
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1shown to be strongly involved in analytical <strong>and</strong> sequentialprocessing, which would presumably require a high degreeof local differentiation, whereas the right hemisphere ismore involved in synthesis <strong>and</strong> relational functions whichwould require more intrahemispheric fibers to coordinate<strong>and</strong> relate the outputs of the distributed local processors.The finding of greater spatial correlations in the right hemispherecompared to the left hemisphere is consistent withthese functional models of hemispheric specialization.The use of source correlation <strong>and</strong> source coherencehas been shown to be a useful method for exploring cortico-corticalconnectivity as well as the temporal-spatialdynamics involved in cognition <strong>and</strong> clinical applications. 8 - 11The present study further supports the use of source correlation<strong>and</strong> source coherence as a reliable <strong>and</strong> clinically usefuldigital signal processing tool. Finally, interhemisphericcorrelations were not explored in the present study. Shultz<strong>and</strong> Braitenberg 4 estimate that only approximately 3% ofthe cerebral white matter involves direct hemispheric connectionssuch as through the corpus callosum, <strong>and</strong> theapplication of source correlations to interhemispheric relationshipswill be the subject of a future study.REFERENCES1. Nunez P. Electrical Fields of the Brain. New York: OxfordUniversity Press; 1981.2. Nunez P. Neocortical <strong>Dynamic</strong>s <strong>and</strong> Human <strong>EEG</strong> Rhythms.New York: Oxford University Press; 1994.3. Braitenberg, V. Cortical architectonics: general <strong>and</strong> areal. In:Brazier MAB, Petsche H, (eds). Architectonics of theCerebral Cortex. New York: Raven Press; 1978: 443-465.4. Schulz A, Braintenberg V. The human cortical white matter:quantitative aspects of cortico-cortical long-range connectivity.In: Schultz A, Miller R, (eds). Cortical Areas: Unity <strong>and</strong>Diversity. Conceptual Advances in Brain Research, London,2002: 377-386.5. Thatcher RW, Krause P, Hrybyk M. Corticocortical associationfibers <strong>and</strong> <strong>EEG</strong> coherence: a two compartmental model.Electroencephalogr Clin Neurophysiol 1986; 64: 123-143.6. Thatcher RW, Biver C, McAlaster R, Salazar AM. Biophysicallinkage between MRI <strong>and</strong> <strong>EEG</strong> coherence in traumatic braininjury. NeuroImage 1998; 8(4): 307-326.7 Shen B, Nadkarni M, Zappulla RA. Spatial-spectral signatureof human cortical synchrony. <strong>EEG</strong> Clin Neurophysiol 1999;110(1): 115-125.8. Thatcher R, Wang B, Toro C, Hallett M. Human neural networkdynamics using multimodal registration of <strong>EEG</strong>, PET<strong>and</strong> MRI. In: Thatcher R, Hallett M, Zeffiro T, John E, HuertaM, (eds). Functional Neuroimaging: Technical Foundations.New York: Academic Press; 1994.9. Thatcher RW. Tomographic electroencephalography/magnetoecephalography:dynaics of human neural network switching.J Neuroimag 1995; 5: 35-45.10. Hoechstetter K, Bornfleth H, Weckesser D, Ille N, Berg P,Scherg M. BESA source coherence: a new method to studycortical oscillatory coupling. Brain Topogr 2004; 16: 233-238.11. Pascual-Marqui RD, Koukkou M, Lehmann D, Kochi K.Functional localization <strong>and</strong> functional connectivity with LORE-TA comparison of normal controls <strong>and</strong> first episode drug naïveschizophrenics. J Neurotherapy 2001; 4(4): 35-37.12. Pascual-Marqui RD. Review of methods for solving the <strong>EEG</strong>inverse problem. Int J Bioelectromagnetism 1999; 1:75-86.13. Gomez J, Thatcher RW. Frequency domain equivalencebetween potentials <strong>and</strong> currents using LORETA. Int JNeurosci 2001; 107: 161-171.14. Frei E, Gamma A, Pascual-Marqui RD, Lrhmsnn D, Hell D,Vollenweider FX. Localization of MDMA-induced brain activityin healthy volunteers using low resolution electromagnetictomography (LORETA). Human Brain Map 2001; 14: 152-165.15. Pascual-Marqui RD. Free software <strong>and</strong> documentation fromthe Key Institute that was downloaded from http://w w w. u n i z h . c h / k e y i n s t / N e w L O R E TA / S o f t w a r e / S o f t w a r e . h t m .June, 2003.16. Lancaster JL, Woldorff MG, Parsons LM, Liotti M, Freitas CS,Rainey L, et al. Automatice Talairach atlas labels for functionalbrain mapping. Human Brain Map 2000; 10: 120-13117. Blinkov SM, Glezer I. The Human Brain in Figures <strong>and</strong>Tables: A Quantitative H<strong>and</strong>book. New York: Basic Books,Plenum Press; 1968.18. Carpenter MB, Sutin J. Human Neuroanatomy. 8th ed.Baltimore, Maryl<strong>and</strong>: Williams <strong>and</strong> Wilkins; 1983.19. Tucker DM, Dawson SL, Roth DL, Penl<strong>and</strong> JG. Regionalchanges in <strong>EEG</strong> power <strong>and</strong> coherence during cognition:intensive study of two individuals. Behav Neurosci 1985;99(3):564-77.20. Tucker DM, Roth DL, Blair TB. Functional connectionsamong cortical regions: Topography of <strong>EEG</strong> coherence.Electroenceph Clin Neurophysiol 1986; 63: 242-250.21. Gur RC, Packer IK, Hungerbuhler JP, Reivich M, Obrist WD,Amarnek WS, Sacheim HA. Differences in the distribution ofgray <strong>and</strong> white matter in human cerebral hemispheres.Science 1980; 207: 1226-1228.22. Connelly CJ. External Morphology of the Primate Brain.Springfield, IL: Charles C Thomas; 1950.23. Galaburda AM, LeMay M, Kemper TL, Geschwind N. Rightleftasymmetries in the brain. Science 1978; 199: 852-856.24. Geschwind N, Levitski W. Human brain: left-right asymmetriesin temporal speech region. Science 1968; 161: 186-187.25. Chi HJG, Dooling ES, Giles FH. Gyral development of thehuman brain. Ann Neurol 1977; 1: 86-94.26. Kinsbourne M. Mechanisms of hemisphere interaction inman. In: Kinsbourne M, Smith L, (eds). HemisphericDisconnection <strong>and</strong> Cerebral Function. Thomas, Springfield,IL: Charles C Thomas; 1974: 71-86.48
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Visual Completion Processing in Human Face PerceptionXiang-Li Chu, Yin-Hua Wang <strong>and</strong> Yu-Ping WangKey WordsEvent-related PotentialFace PerceptionNegativityN1Visual CompletionABSTRACTSubjects discriminated whether two sequentially presentedhuman face pictures (S1 <strong>and</strong> S2) were identicalwhile event-related potentials were recorded to explore theneural basis of visual completion for occluded objects.Four kinds of stimulus trials were employed: S2 <strong>and</strong> S1were identical (match-complete); S2 <strong>and</strong> S1 were identical,but S2 was partially occluded (match-incomplete); S2 wasa different face from S1 (mismatch-complete); S2 was differentfrom S1, <strong>and</strong> was partially occluded (mismatchincomplete).Incomplete faces enhanced the amplitude ofN1 compared with complete faces. The peak latency of N2elicited by incomplete faces was delayed about 20 mscompared with complete faces. The enhancement of N1 isrelated to visual completion processing that requires additionaltime.INTRODUCTIONVisual completion is described as a process thatboundaries <strong>and</strong> surfaces of objects are perceived in locationswhere no local information is present. That is, whenone object is partly occluded by another, its occluded partsare perceptually “filled in,” <strong>and</strong> the occluded object appearsto be continuous behind its occluder. It is known as amodalcompletion. 1 Completion of partly occluded objects hassometimes been considered to be more cognitive in origin,perhaps not explainable by truly sensory or perceptualmechanisms at all. 2 However, single unit recording studiesshowed that cells of area V2 were activated by amodalcompletion that occurred when a contour passed behindan occluder. 3 A recent fMRI study showed that the lateraloccipital cortex is the central site involved in the visualcompletion process. 4 Sekuler <strong>and</strong> Palmer 5 studied the timecourse of completion by means of the primed matchingparadigm <strong>and</strong> discovered that a partially occluded figure isperceptually represented as complete with a quite shortperiod of time ( no longer than 200 ms).Faces represent highly meaningful non-linguistic stimuli,providing much more perceptually derived information.The recognition of faces is very accurate <strong>and</strong> eff o r t l e s sdespite changes in viewing angle, expression, age, or paraphernalia.There is strong evidence indicating that the perceptionof faces is mediated by extrastriate mechanismsspecifically tuned to process physiognomic information. 6 , 7This view is supported by single-cell recordings in primates 8<strong>and</strong> intracranial recordings of event-related potentials(ERPs) in humans. 6 Recent electrophysiological studies onface perception have focused on the N170 (N1), a negativecomponent of ERPs, peaking between 140 <strong>and</strong> 180 ms,which typically distributes over bilateral occipitotemporalscalp regions 9 , 10 <strong>and</strong> is considered as a face-specific ERPc o m p o n e n t . 10 In these studies the amplitude of N1 elicitedby faces was larger than that elicited by other complex visualobjects such as buildings, cars, furniture, etc. 10 B e c a u s ethe face specific N1 component is not affected by facef a m i l i a r i t y 11 , 12but by face inversion or scrambling of theinternal facial features, 13 , 14 it has been argued that the N1reflects the perceptual encoding of face components ratherthan the processing of face identification. 13Electrophysiological research revealed that incomplete3-dimensional objects elicited an enhanced N1 in occipitotemporalarea, which indicates that N1 may be the negativityrelated to visual completion. 1 5 M o r e o v e r, some findingsshowed that faces are processed holistically: they areprocessed as a whole rather than as a collection of independentfeatures. 1 6 , 1 7 We can hypothesize that the completionfor occluded faces should be similar to the occluded 3-dimensional object, <strong>and</strong> the N1 should be altered when theincomplete faces are presented <strong>and</strong> the visual completionprocess is activated. In the present study, we recorded ERPresponses while subjects performed a face-matching task.From the Department of Neurology (X.-L. Chu, Y.-H. Wang), FirstHospital of Peking University, Beijing, China, <strong>and</strong> the Department ofNeurology (Y.-P. Wang), Xuanwu Hospital, Capital University of MedicalSciences, Beijing, China.Address requests for reprints to Dr. Yu-Ping Wang, Department ofNeurology, Xuanwu Hospital, Capital University of Medical Sciences, #45Changchun Street, Beijing 100053, China.Email: wangyupi@public.bta.net.cnReceived: January 21, 2006; accepted: July 15, 2006.49
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Table 1Mean accuracy scores <strong>and</strong> reaction times (RT) in four conditions (mean ± SD)MatchMismatchComplete Incomplete Complete IncompleteRT 495±102 553±97* 578±78* 571±78*Accuracy 97.0% ± 5.0% 91.2% ± 8.9%* 95.5% ± 3.4% 94.0% ± 5.2%* Significantly different from match-completeMATERIALS AND METHODSSubjectsSixteen right-h<strong>and</strong>ed healthy subjects (7 females)between the ages of 23 <strong>and</strong> 27 years participated in thisstudy as paid volunteers. None of them had any history ofneurological or psychiatric diseases. All subjects hadreached a university education level <strong>and</strong> had normal orcorrected-to normal vision. Written informed consent wasobtained from each participant. They were fully informed ofthe recording technique that is noninvasive.Trial design <strong>and</strong> taskVisual stimuli were photographs of faces (front view)from college yearbooks. Females <strong>and</strong> clean-shaven maleswere equally presented, <strong>and</strong> none had extraneous featuressuch as spectacles or jewelry. The faces were unfamiliar tothe participants. In our experiments, we used digitallyscanned grayscale photographs with equal brightness <strong>and</strong>contrast. The vertical <strong>and</strong> horizontal visual angles were2.74° <strong>and</strong> 2.28°, respectively. These photos were eitherintact or incomplete (partially occluded). The occluded part,occupied a visual angle of 1.37° X 1.14°, was the left-topquadrant of the pictures. Stimuli were presented centrallyon a computer monitor in front of a black background. Ablack board occluded the invisible quadrant. The first (S1)<strong>and</strong> the second (S2) stimulus pictures in a pair flashed 300ms in sequence, with an onset inter-stimulus interval of1000 ms. The inter-pair interval was 3 s. Four conditions ofstimulus pairs were r<strong>and</strong>omly employed with equal probability:S2 was the same face picture as S1 (match-complete);S2 was the same face picture as S1, but S2 was anincomplete face with an occluded part (match-incomplete);S2 was a different face picture from S1 (mismatch-complete);S2 with an invisible part was a different face picturefrom S1 (mismatch-incomplete).Following electrode application, subjects sat in a comfortablechair located in a shielded room <strong>and</strong> were asked tofix their eyes on a cross marker in the center of a computermonitor located 100 cm away from their eyes. They wereinformed to discriminate whether the two stimuli in a pairwere the same face or not <strong>and</strong> to ignore whether the faceswere intact or not. Subjects pressed one button of a pushpadas fast <strong>and</strong> accurately as possible when S2 was consideredthe same face picture as S1, <strong>and</strong> pressed anotherbutton when S2 was considered to be different from S1.Following 10 practice trials, a total of 160 stimulus trials,divided into two sessions (each of 5 min), were presented.The response h<strong>and</strong>s were counterbalanced in the secondsession for all subjects. A short break was allowed betweensessions to prevent subjects from fatigue. The reactiontime (RT) <strong>and</strong> the frequency of their correct responseswere recorded by the STIM system.Electrode placement <strong>and</strong> recording<strong>EEG</strong> was recorded with Ag-AgCl electrodes from FP1,FP2, F3, F4, F7, F8, Fz, C3, C4, Cz, P3, P4, Pz, T3, T4,T5, T6, O1, O2 <strong>and</strong> Oz (according to the International 10-20 System), referenced to an electrode positioned on thetip of the nose. Impedance was kept below 5KΩ. Verticalelectrooculogram (EOG) was recorded through electrodesabove <strong>and</strong> below the left eye. Horizontal EOG was recordedthrough electrodes at the outer canthi of both eyes.<strong>EEG</strong> was amplified with a b<strong>and</strong> pass of 0.05-100 Hz, sampledat 1000 Hz, <strong>and</strong> stored on a hard disk for off-lineanalysis. The ERPs were averaged for each channel <strong>and</strong>each condition. The averaged ERPs were digitally filteredwith a b<strong>and</strong> pass from 0.1 to 40 Hz. The averaged epochwas 1000 ms <strong>and</strong> the measurement 200 ms prior to theonset of S2 served as a baseline. Any trials containingincorrect responses were excluded from the averages.Epochs with <strong>EEG</strong> or EOG exceeding ±100 µV were alsoexcluded from the averages. The average number ofaccepted sweeps was: 37.2 ± 1.2 for match-complete;35.8 ± 1.3 for match-incomplete; 36.9 ± 1.8 for mismatchcomplete;36.3 ± 2.5 for mismatch-incomplete.Statistical analysisThe component of interest was N1 <strong>and</strong> N2, over theposterior temporo-occipital areas (T5, T6, O1 <strong>and</strong> O2). Theamplitude of N1 was accessed as the mean amplitudebetween 120 to 190 ms from stimulus onset at T5, T6, O1<strong>and</strong> O2 where the N1 was most conspicuous according tothe gr<strong>and</strong>-averaged ERPs. The peak latencies were measuredat the maximum of N1 <strong>and</strong> N2 at O1 <strong>and</strong> O2. Thereaction time <strong>and</strong> the frequency of correct responses aswell as electrophysiological measures were investigated byrepeated measures ANOVAs. The significance level for allstatistical tests was p < 0.05.RESULTSBehavioral dataThe mean reaction times (RT) <strong>and</strong> the percentage of correctresponses are shown in Table 1. The 2 x 2 A N O VA ( t w o50
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Figure 1.Gr<strong>and</strong>-averaged ERPs elicited by four conditions (match <strong>and</strong> complete, match <strong>and</strong> incomplete, mismatch <strong>and</strong> complete, mismatch <strong>and</strong>incomplete). Incomplete faces elicited larger N1 than complete faces. The latency of N2 elicited by incomplete faces was delayed comparedwith complete faces.Table 2The mean amplitude (µV) of N1 in 120-190 ms tie windows for each condition (mean ± SD)MatchMismatchSite Complete Incomplete Complete IncompleteO1 3.7 ± 5.2 2.9 ± 5.9 3.7 ± 5.5 3.0 ± 5.5O2 2.4 ± 4.3 -1.3 ± 5.9*# 1.9 ± 6.0 -1.6 ± 5.8*#T5 1.9 ± 4.2 1.3 ± 4.5 1.1 ± 4.1 1.3 ± 4.3T6 0.7 ± 2.8 -2.2 ± 3.6*# -0.1 ± 4.7 -2.0 ± 3.5*#* Significantly different from match-complete# Significantly different from mismatch-completefactors: “Match” <strong>and</strong> “Completion”) of these data showedthat “Match” x “Completion” interaction had a significante ffect on RT (F(1, 15)=36.96, p < 0.001). Post-hoc comparisonshowed that the RT to the match-complete was shorterthan that to the match-incomplete (p < 0.05). The RT i nmismatch conditions did not show any difference betweencomplete <strong>and</strong> incomplete trials. The RT in the match conditionswas shorter than in the mismatch conditions (F(1, 15)=14.56, p < 0.002). The 2 x 2 A N O VA showed the frequencyof correct responses was higher when the second facewas complete than when it was incomplete (F(1, 15)= 11.97, p < 0.004). Post-hoc comparison showed that theaccuracy in the match-complete conditions was higher thanthe match-incomplete conditions (p < 0.002).ERP dataFigure 1 shows the gr<strong>and</strong>-averaged ERP waveformsfrom the lateral temporal <strong>and</strong> occipital electrodes. N1amplitude, quantified as mean amplitude within 120-190ms post-stimulus window, was analyzed by repeatedmeasures ANOVAs with the factors: Match (match versusmismatch), Completion (complete versus incomplete),Hemisphere (left versus right), <strong>and</strong> Electrode site (T5, T6,O1 <strong>and</strong> O2) (Table 2). Compared with complete faces,incomplete faces elicited a larger N1 as reflected by a highlysignificant main effect of “Completion” (F(1, 15)=6.36,p
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Figure 2.A: Topographical map of difference wave between match-incomplete<strong>and</strong> match-complete. B: Topographical map of differencewave between mismatch-incomplete <strong>and</strong> mismatch-complete.Table 3The peak latencies of ERP components in four conditions (mean ± SD) (ms)MatchMismatchSite Complete Incomplete Complete IncompleteN1 O1 155 ± 8 157 ± 7 157 ± 11 157 ± 9O2 156 ± 9 158 ± 6 156 ± 9 157 ± 9N2 O1 240 ± 6 257 ± 6* 254 ± 16* 271 ± 20*#&O2 243 ± 9 264 ± 9* 246 ± 9& 268 ± 12*#* Significantly different from match-complete# Significantly different from mismatch-complete& Significantly different from match-incompletetopographical mapping of the difference potentials wereobtained at N1 latency level.Figure 2A shows the distribution of the difference activitybetween match-incomplete <strong>and</strong> match-complete <strong>and</strong>Figure 2B between mismatch-incomplete <strong>and</strong> mismatchcomplete.The enlarged N1 elicited by incomplete facesdistributes on the right occipitotemporal scalp obviouslywhether the faces in a pair were matched or mismatched.LatencyFigure 1 shows a shift in latency of N2 elicited by incompletefaces as compared with complete faces while the shiftof N1 latency is absent. This effect is distinct in the occipitalarea (O1 <strong>and</strong> O2). N2 latency was quantified as the negativepeak latency between 225 <strong>and</strong> 275 ms post-stimulus.N2 peak latency to incomplete faces was longer than that tocomplete faces, <strong>and</strong> this was reflected in highly significante ffects of “Completion” (F(1, 15)=12.12, p0.05).DISCUSSIONThe present study investigated the effects of “Completion”on N1 as well as the subsequent ERP component usingthe occluded faces as stimuli. We found that N1 to incompletefaces was larger than N1 to complete faces. Thepeak latency of the subsequent N2 elicited by incompletefaces was delayed compared with complete faces.Visual completion is an inherent property of visualrecognition in which partially occluded objects can beaccurately perceived. Previous studies revealed that lateraloccipital cortex is the crucial site involved in thisprocess. 4,18 Again, Lerner <strong>and</strong> her colleagues 19 discovereda hierarchical axis oriented anterior-posteriorly in theorganization of ventral object areas. The axis, along ventraloccipitotemporal object areas, starts in early visual areasthrough retinotopic areas V4/V8 <strong>and</strong> continues into the lateraloccipitalsulcus dorsally <strong>and</strong> the posterior fusiformgyrus ventrally, in which the neuronal sensitivity shifts fromlocal object features to a more global representation. Thelateraloccipital sulcus dorsally <strong>and</strong> the posterior fusiformgyrus together correspond to the previously describedobject-related lateral occipital cortex, 18,20 which was confirmedto be selectively involved in face perception. 19,21,22Therefore, there is a large overlap between the face-selectivecortex <strong>and</strong> the object-selective cortex. 19The research pertaining to the occluded object completionrevealed that the lateral occipital cortex (both the lateraloccipitalsulcus dorsally <strong>and</strong> the posterior fusiform gyrussubdivisions) was activated by completion process. 4 In thepresent study, relative to complete faces, incomplete faceselicited an enlarged N1. Perception of occluded picturesrequires visual completion processing to “fill-in” the absentinformation. Therefore, the enhanced N1 could be related to52
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1visual completion. Another study showed that illusory perceptsproduced larger N1 in bilateral occipital areas <strong>and</strong> proposedthat N1 is the electrophysiological index for the illusorycontour perception. 23 Therefore, illusory contour completion(modal completion) <strong>and</strong> occluded object completion(amodal completion) may have a similar neural mechanism. 1Sekuler <strong>and</strong> Palmer 5 have found that completion interpretationdevelops over time, <strong>and</strong> a partially occluded figure isperceptually represented as complete within a short periodof 200 ms. All of these results indicate that N1 peaking at~180 ms in the occipitotemporal areas may be the electrophysiologicalindex for visual completion process. Moreover,N1 amplitude difference between complete faces <strong>and</strong>incomplete faces was significant at the right occipitotemporalarea. This agrees with the previous findings showing thatoccluded 3-dimensional objects elicited a larger N1 in theright occipitotemporal area. 15There is evidence of hemisphericasymmetry for perceptual closure 24 <strong>and</strong> for face proce s s i n g . 25 , 26 In our further unpublished study (16 right-h<strong>and</strong>edsubjects involved), the visual stimuli included two kinds offace pictures: complete <strong>and</strong> incomplete. Instead, the facesoccluded one of the four quadrants r<strong>and</strong>omly served asincomplete face stimuli. We have found the consistentresults that the right occipitotemporal cortex is moreengaged in the completion process than the left. T h e r e f o r e ,it is possible that the right occipitotemporal cortex may playa more important role in visual completion. Further studiesare necessary to provide more information on this issue.The prevailing view is that N1 is related to the configuralencoding of faces because the inverted faces elicited adelayed N1. 27 The highest possibility is that the loss of configuralinformation through inversion slows down the earlyface processing. In our studies, the incomplete facesenlarged but not delayed the N1 compared with the completefaces. This suggested that the incomplete face processingis, to some extent, different from the inverted faceprocessing. The incomplete face processing may beinvolved in a more general visual completion process thatis reflected by the enhanced N1.The latency of the following component N2 elicited byincomplete faces was on average 20 ms later than thatelicited by complete faces while the latency of N1 was notaffected. This indicates that visual completion processtakes place before the stage represented by N2, whichrequires additional processing time.In the present study, subjects performed a face matchingtask, irrespective of the configuration (complete orincomplete) of the stimuli. The effect of “completion” ratherthan “match” reached significance on the amplitude of N1.This suggests that the visual completion for occluded facesarises automatically <strong>and</strong> is irrelevant to the task at h<strong>and</strong>.CONCLUSIONA series of ERP components can be elicited by thecomplex visual stimuli — complete faces <strong>and</strong> incompletefaces. Visual completion processes for incomplete facescan enhance the amplitude of N1. Visual completionprocess is an automatic process that consumes additionalprocessing time.ACKNOWLEDGMENTSThis research was supported by the National NaturalScience Foundation of China (30370477).REFERENCES1. Kellman PJ, Yin C. A common mechanism for illusory <strong>and</strong>occluded object completion. J Exper Psychol 1998; 24: 859-869.2. Gregory RL. Vision with isoluminant color contrast: a projectiontechnique <strong>and</strong> observation. Perception 1977; 6: 113-119.3. Bakin JS, Nakayama K, Gilbert CD. Visual responses inmonkey area V1 <strong>and</strong> V2 to three-dimensional surface configurations.J Neurosci 2000; 20: 8188-8198.4. Lerner Y, Hendler T, Malach R. Object-completion effects inthe human lateral occipital complex. Cereb Cortex 2002; 12:163-177.5. Sekuler AB, Palmer SE. Perception of partly occluded objects:a microgenetic analysis. J Exp Psychol Gen 1992; 121:95-111.6. Allison T, Ginter H, McCarthy G, Nobre A, Puce A, Luby M,Spencer DD. Face recognition in human extrastriate cortex.J Neurophysiol 1994, 71: 821-825.7. Allison T, Puce A, Spencer DD, McCarthy G. Electrophysiologicalstudies of human face perception: potentials generatedin occipitotemporal cortex by face <strong>and</strong> non-face stimuli.Cereb Cortex 1999; 9: 415-430.8. Desimone R. Face-selective cells in the temporal cortex ofmonkeys. J Cogn Neurosci 1991; 3: 1-8.9. Eimer M. The face-specific N170 component reflects latestages in the structural encoding of faces. NeuroReport2000; 11:2319-2324.10. Bentin S, Allison T, Puce A, Perez E, McCarthy G. Electrophysiologicalstudies of face perception in humans. J CognNeurosci 1996; 8: 551-565.11. Eimer M. Effects of face inversion on the structural encoding<strong>and</strong> recognition of faces evidence from event-related brainpotentials. Cogn Brain Res 2000; 10: 145-158.12. Eimer M. Event-related brain potentials distinguish processingstages involved in face perception <strong>and</strong> recognition. ClinNeurophysiol 2000; 111: 694-705.53
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 113. Rossion B, Gauthier I. How does the brain process upright<strong>and</strong> inverted faces? Behav Cogn Neurosci 2000; 11: 67-74.14. Rossion B, Delvenne JF, Debatisse D, Goffaux V, Bruyer R,Crommelinck M, Guérit JM. Spatio-temporal localization ofthe face inversion effect: an event-related potentials study.Bio Psychol 1999; 50: 173-189.15. Wang Y, Zhang Y, Wang H, Cui L, Tian S. Brain potentialselicited by matching global <strong>and</strong> occluded 3-dimensional contours.Brain Cogn 2003; 53: 28-33.16. Sagiv N, Bentin S. Structural encoding of human <strong>and</strong>schematic faces: holistic <strong>and</strong> part-based processes. J CognNeurosci 2001; 13: 937-951.17. Gr<strong>and</strong> Le R, Mondloch CJ, Maurer D, Brent HP. Impairmentin holistic face processing following early visual deprivation.Psychol Sci 2004; 15: 762-768.18. Doniger GM, Foxe JJ, Murray MM, Higgins BA, SnodgrassJG, Schroeder CE, Javitt DC. Activation timecourse of ventralvisual stream object-recognition areas: high density electricalmapping of perceptual closure processes. J Cogn Neurosci2000; 14: 615-621.19. LernerY, HendlerT, Ben-Bashat D, Harel M, Malach R. A hierarchicalaxis of object processing stages in the human visualcortex. Cereb Cortex 2001; 11: 287- 297.20. Grill-Spector K, Kushnir T, Hendler T, Edelman S, Itzchak Y,Malach R. A sequence of object-processing stages revealedby fMRI in the human occipital lobe. Hum Brain Map 1998; 6:316-328.21. Halgren E, Dale A, Sereno M, Tootell R, Marinkovic K, RosenB. Location of human face-selective cortex with respect toretinotopic areas. Hum Brain Map 1999; 7: 29-37.22. Kanwisher N, McDermott J, Chun M. The fusiform face area:a module in human extrastriate cortex specialized for faceperception. J Neurosci 1997; 17: 4302-4311.23. Proverbio AM, Zani A. Electrophysiological indexes of illusorycontours perception in humans. Neuropsychologia 2002;40: 479-491.24. Lewis RS, Kamptner LN. Sex differences in spatial task performanceof patients with <strong>and</strong> without unilateral cerebrallesion. Brain Cogn 1987; 6: 142-152.25. Puce A, Allison T, Asgari M, Gore JC, McCarthy G.Differential sensitivity of human visual cortex to faces, letterstrings,<strong>and</strong> textures: a functional magnetic resonance imagingstudy. J Neurosci 1996; 16: 5205-5215.26. Gr<strong>and</strong> Le R, Mondloch CJ, Maurer D, Brent HP. Expert faceprocessing requires visual input to the right hemisphere duringinfancy. Nat Neurosci 2003; 6: 462-474.27. Rossion B, Delvenne JF, Debatisse D, Goffaux V, Bruyer R,Crommelinck M, Guérit JM. Spatio-temporal localization ofthe face inversion effect: an event-related potentials study.Bio Psychol 1999; 50: 173-189.54
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Considerations of the Ischemic Basis<strong>and</strong> Therapy of Alzheimer DiseaseE. NiedermeyerKey WordsAlzheimer DiseaseCerebral Ischemia, PrimaryHead-Down TherapyProphylaxis vs. TreatmentTreatment vs. ProphylaxisABSTRACTA recently presented concept of Alzheimer disease(AD) is based on a primarily ischemic (rather than degenerative)type of brain disease. Etiologically, this new conceptis presumed to be related to the human upright gaitalong with individual predisposition.The proposed treatment — head-down therapy (HDT)— is the centerpoint of this presentation: a simple <strong>and</strong> generallyaccessible type of therapy, with monitoring by neuropsychologicalquestioning, electroencephalography, <strong>and</strong>transcranial Doppler. As a treatment of AD (limited to stage1), HDT is expected to be helpful. It is possible, however,that its prophylactic use may be of even greater importance.INTRODUCTIONThe concept of Alzheimer Disease (AD) as a primarilyischemic disorder (without true vascular disease) hasopened the door for therapeutic action. 1 The primaryischemia causing AD might be a price to be paid for ourupright gait: in predisposed persons as early as age 40years (with a prevalence climbing from 0.4% to 30% atage 80).Paramount is the strict separation of AD from othertypes of dementia <strong>and</strong>, above all, from the dementias associatedwith cerebrovascular disorder (multi-infarct dementia).Whenever a patient with suspected AD has a history ofhigh blood pressure, coronary disease/myocardial infarction<strong>and</strong> any type of stroke, the associated dementia isthen most unlikely to be of the AD type. Furthermore, nicotinismwith its well known cardiac, cerebral <strong>and</strong> peripheralarterial effects is hardly compatible with AD. To underst<strong>and</strong>AD, underst<strong>and</strong> first its limitations!THE THERAPEUTIC APPROACH:HEAD-DOWN THERAPY“Head down!” sums it up. The patient lying on the back,being placed on a tiltable bed with the head below the horizontal.How much lowered? The treatment must be donewithin the limits of safety <strong>and</strong> comfort. When the head islowered between 1 to 5 degrees, the therapeutic sessionsof 1 hour duration are likely to be well tolerated. Steeperlowering of the head (5-20 degrees) should be done withreduction of duration.HEAD-DOWN THERAPY AND STAGE OF DISEASEAdvanced stages of AD are certainly too late for the initiationof head-down therapy (HDT). Once memory is notthe only affected function any more <strong>and</strong> signs of speechdisturbance (paraphasias) are becoming prominent, thewidespread neuronal loss will make HDT useless.Is stage 1 of AD therefore the ideal period for HDT?Certainly, as long as the presence of AD is the only criterion.But it is quite possible that HDT will turn out to be evenmore successful in the prevention of AD in patients withmild or marked cognitive decline yet without evidence ofAD. It is quite possible, if not likely, that such prophylactictherapy will find a much greater number of HDT users. Thefear of AD has always fostered anxieties in healthy middleagedpersons concerned about their decline of memory —be this within or above normal limits.Therefore, the use of HDT may spread far beyond thedomain of hospitals <strong>and</strong> similar institutions. In the homesetting, it may become a “do-it-yourself” treatment. Thismay prove to be an effective preventive method, but it mustnot turn into a mere fad. Using an ordinary bed, with thepatient lying on a flat surface, the feet can be lifted to a reasonableheight of about 4" by raising the foot section of thebed, placing its rear posts on blocks of such size.Will this not amount to veritable chaos in a field wherescientific exactitude ought to reign supreme? Of course itwill — but as long as the do-it-yourselfers note improvement,one will have to be tolerant. As long as strictly scientificprojects are going on in the hospital setting with monitoredHDT, the door should remain open for those who,driven by anxieties, rush to the homemade treatment.From the Departments of Neurology <strong>and</strong> Neurosurgery, The JohnsHopkins University School of Medicine, The Division of Neurology, TheSinai Hospital, Baltimore, Maryl<strong>and</strong>.Address requests for reprints to Ernst Niedermeyer, MD, 305 ColonialCourt, Towson, Maryl<strong>and</strong>, 21204-4318, USA.Received: August 15, 2006; accepted: August 22, 2006.55
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1At this time — in the absence of data — it is stillunknown if HDT is more successful in the prophylaxis thanin the treatment of AD.Hearsay has it that advanced Yoga exercisers whost<strong>and</strong> on their head every day — a position usually notlonger tolerable than 1 minute — never become victims ofAD. If this turns out to be more than hearsay — if this iscorrect — such a strong argument should remove furtherobstacles on the route to widespread prevention of AD.THERAPEUTIC SESSIONS WITH MONITORINGIn the clinical setting, the treatment should be monitoredby the following methods: a) Neuropsychologicalquestioning, b) <strong>EEG</strong>, <strong>and</strong> c) Transcranial Doppler. Forthose experienced in the P300 methodology, that methodcan be recommended for the monitoring of AD. 2Neuropsychological questioningNeuropsychological questioning — ideally done by anexperienced clinical neuropsychologist — can be performedin many ways. If familiar with the patient’s family situation,names of children <strong>and</strong> gr<strong>and</strong>children, dates of theirlives, their schools, their husb<strong>and</strong>s/wives, <strong>and</strong> informationabout cousins <strong>and</strong> other relatives, are quite appropriate.Does the patient know his/her birthday or wedding day? Inwhat town is he now, where did he live before? Then, ofcourse, there are the usual questions about the presentpresident of the USA <strong>and</strong> his predecessors. Presenting picturesof presidents may reveal a form of agnosia (usuallybeginning in the second stage of AD, a stage that could betoo late for the use of HDT). Whatever is being questionedin the course of a therapeutic session should have beenasked before HDT for comparison.ElectroencephalographyIn stage 1 of AD, slowing of the <strong>EEG</strong> gradually increases,starting with a 4-7/sec <strong>and</strong> some 1.5-3/sec activity overthe temporal area. The posterior basic rhythm graduallyslows down to 6-8/sec. Temporal slowing may be intermingledwith sharp potentials (almost always unassociatedwith clinical seizures).In the head-down position, a reduction of slowingshould be expected. The use of computerized frequencyanalysis may or may not provide further informative data.Transcranial DopplerIn view of suspected major neurocirculatory problems,sonography, transcranial Doppler has been used in recentAD studies by Silvestrini et al. 3 <strong>and</strong>, in particular, byRuitenberg et al. 4 who were impressed with the diminishedcerebral blood flow velocity. This method has to be warmlyrecommended.If possible, all three of these methods should beused. For practical purposes, it might be reasonable to useone of them in the morning session <strong>and</strong> one of the othertwo during the afternoon treatment.A new concept — still without dataWithout data?! — a horrifying prospect in modern clinicalmedicine! But the concept had to come first becausethe reigning concept is flawed <strong>and</strong> has to be mended.“Concept before data” is a normal situation for physicists<strong>and</strong> chemists. Yes, it is true: those scientists smile oreven laugh at the total data-dependence in biomedicine.Data will come to prove the new concept right — or wrong.But as long as a concept is based on logical thought, thereis nothing to fear.REFERENCES1. Niedermeyer E. Alzheimer disease: caused by primary deficiencyof the cerebral blood flow. Clin <strong>EEG</strong> Neurosci 2006;37: 175-177.2. Pogarell O, Mulert C, Heger U. Event-related potentials <strong>and</strong>fMRI in neuropsychopharmacology. Clin <strong>EEG</strong> Neurosci 2006;37: 99-107.3. Silvestrini M, Pasqualetti P, Baruffaldi R, Bartolini M,H<strong>and</strong>ouk Y, Matteis M, Moffa F, Provinciali L, Vernieri F.Cerebrovascular reactivity <strong>and</strong> cognitive decline inpatients with Alzheimer disease. Stroke 2006; 37: 1010-1 0 1 5 .4. Ruitenberg A, den Heuer T, Bakker SLM, Van Swieten JC,Koudstall PJ, Hofman A, Breteler MMB. Cerebral hypoperfusion<strong>and</strong> clinical onset of dementia: the Rotterdam Study.Ann Neurol 2005; 57: 789-794.56
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Nonconvulsive Status Epilepticus Causing Prolonged StuporAfter Intraventricular Hemorrhage: Report of a CaseJ. L. Fernández-Torre, Z. Agirre, R. Puchades, E. Marco De Lucas <strong>and</strong> A. OterinoKey WordsElderly PatientsElectroencephalographyIntraventricular HemorrhageNonconvulsive Status EpilepticusStuporABSTRACTWe describe the case of an octogenarian woman whoexperienced a severe alteration of mental state due to nonconvulsivestatus epilepticus (NCSE) complicating an intraventricularhemorrhage. Our report emphasizes that NCSEmay be the cause of unexplained neurological deteriorationin elderly patients with acute brain injury.INTRODUCTIONNonconvulsive status epilepticus (NCSE) is a wellknowncause of altered mental state whose diagnosis maybe particularly difficult in elderly people. 1 Cerebrovasculardisease is considered a frequent etiology of epilepsy inolder patients, however, intraventricular hemorrhage is anunreported condition associated with NCSE.CASE REPORTAn 88-year-old woman was admitted to our hospitalbecause of acute alteration of consciousness, nausea <strong>and</strong>vomiting. She had antecedents of hypertension <strong>and</strong> hadsuffered from an ischemic infarction in the territory of theleft middle cerebral artery that had caused a mild righthemiparesis. On examination, she was slightly confused,oriented in person <strong>and</strong> disoriented in time <strong>and</strong> place. Herspeech was not fluent <strong>and</strong> there was a discrete weaknessof the right limbs. Plantar responses were flexor. A computedtomography (CT) scan of the brain revealed a left intraventricularhemorrhage <strong>and</strong> a small hematoma localized inthe left thalamus (Figure 1).During the next 72 hours, her level of consciousnessworsened dramatically, <strong>and</strong> she became stuporous.Although the clinical worsening was thought secondary torebleeding, cerebral edema or hydrocephalus, an electroencephalogram(<strong>EEG</strong>) was requested. The <strong>EEG</strong> showed theexistence of continuous epileptiform discharges involvingthe entire left hemisphere in keeping with the diagnosis oflocalization-related (partial) NCSE (Figure 2a). Despite theonset of treatment with intravenous phenytoin (100 mg/8 h),the clinical state of the patient was unmodified for the next 3days. Three consecutive <strong>EEG</strong>s carried out over those daysrevealed generalized continuous epileptiform activity compatiblewith a secondarily generalized NCSE (Figure 2b).The patient’s metabolic status throughout the courseof the disease was carefully controlled, <strong>and</strong> particularinterest was paid to avoid metabolic disturbances such ashyponatremia or hypokalemia, which are known predisposingfactors of NCSE. Antiepileptic therapy with valproate(1000 mg/24 h) <strong>and</strong> clonazepam (1.0 mg/24h) wasadded to her previous treatment. On the following 17days, her level of consciousness was fluctuant rangingfrom somnolence to profound stupor. Several <strong>EEG</strong>sshowed the persistence of ongoing generalized epileptiformdischarges during these days. On day 23 afteradmission, she was conscious <strong>and</strong> able to underst<strong>and</strong>simple comm<strong>and</strong>s. At that time, an <strong>EEG</strong> disclosed featurescompatible with a moderate diffuse encephalopathy<strong>and</strong> resolution of NCSE (Figure 2c). Finally, she was dischargedto another hospital for chronic pathology.DISCUSSIONIntraventricular hemorrhage is a rarely described causeof NCSE. 2,3 Recently, Dennis et al. 3 carried out the firstinvestigation studying the frequency <strong>and</strong> clinical features ofNCSE among comatose patients with subarachnoid hemorrhage.Eight out of 26 patients who underwent continuouselectroencephalographic monitoring were diagnosedas having NCSE. In 4 patients, a bilateral intraventricularhemorrhage was observed. Evaluation of persistent comaor neurological deterioration was the reason for which continuous<strong>EEG</strong> monitoring was carried out. Despite the factthat NCSE was controlled in 5 cases, none of those subjectsexperienced a significant clinical improvement <strong>and</strong> allFrom the Department of Clinical Neurophysiology (J. L. Fernández-Torre,MD, Z. Agirre, MD), Internal Medicine (R. Puchades), Radiology (E. MarcoDe Lucas, MD) <strong>and</strong> Neurology (A. Oterino, MD); University Hospital“Marqués de Valdecilla”; Sant<strong>and</strong>er, Cantabria, Spain.Address requests for reprints to Dr. José L. Fernández-Torre, Departmentof Clinical Neurophysiology, University Hospital “Marqués deValdecilla,” Avda. Valdecilla, s/n. 39008 Sant<strong>and</strong>er, Cantabria. Spain.Email: jlfern<strong>and</strong>ez@humv.es; ftorrenfc@hotmail.com.Received: February 6, 2006; accepted: April 2, 2006.57
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Figure 1.A CT scan of the brain revealed the existence of a large intraventricularhemorrhage occupying the left ventricle.Figure 2A.An <strong>EEG</strong> performed 72 fours after admission showed the presence of continuous epileptiform discharges (arrow) involving the entire lefthemisphere. Vertical bar: 100 µV; Horizontal bar: 1 second; Low filter: 0.5. High filter: 30 Hz.of them died. Similarly, a sudden neurological worseningwas the reason for performing an <strong>EEG</strong> in our case, <strong>and</strong>NCSE was refractory to conventional antiepileptic treatment.Moreover, NCSE remained uncontrolled for severaldays, <strong>and</strong> <strong>EEG</strong> was the unique method to demonstrate thepersistence of ongoing epileptic activity.It could be argued that in our case the long period ofobtundation may have simply been related to the intraventricularhemorrhage <strong>and</strong> the electroencephalographicanomalies constituted only an epiphenomenon.Nevertheless, the behavioral improvement was closelyassociated with the abolition of the epileptiform activity on58
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1Figure 2B.On the next days, several <strong>EEG</strong>s revealed generalized continuous epileptiform activity in keeping with a secondarily generalized NCSE.Vertical bar: 100 µV; Horizontal bar: 1 second; Low filter: 0.5. High filter: 30 Hz.Figure 2C.An <strong>EEG</strong> carried out 23 days after admission showed findings in keeping with a diffuse encephalopathy with resolution of NCSE, but withsome scattered spikes maximal on the right anterior temporal region. A significant improvement of the neurological state of the patientwas observed at that time. Vertical bar: 100 µV; Horizontal bar: 1 second; Low filter: 0.5; High filter: 30 Hz.59
<strong>CLINICAL</strong> <strong>EEG</strong> <strong>and</strong> <strong>NEUROSCIENCE</strong> ©2007 VOL. 38 NO. 1the <strong>EEG</strong>, suggesting strongly that clinical symptoms had agenuine epileptic origin. Some speculation exists in relationto the pathophysiologic mechanism originating theNCSE in this case. Likely, the small hematoma localized inthe left thalamus could be the epileptogenic source of theipsilateral hemispheric continuous epileptiform discharges.However, an intrinsic epileptogenicity associated with theintraventricular hemorrhage per se, or acute hydrocephalusthrough disruption of cortico-subcortical pathways,may not be completely ruled out. Thus, it is wellknownthat the existence of seizures <strong>and</strong> pathological <strong>EEG</strong>features in neonates with severe intraventricular hemorrhageare considered markers of brain injury. Our patienthad also a previous history of an ipsilateral middle cerebralartery territory infarction, which could have predisposedthe occurrence of seizures from left hemispheric origin.Prolonged localization-related (partial) NCSE is aharmless epileptic condition, which may cause, particularlyin the setting of acute brain disorders, permanent braindamage. 4-6 Therefore, an early diagnosis <strong>and</strong> rapid treatmentwill avoid additional deficits. Although the prognosisof our patient was more favorable than described byDennis et al., 3 the clinical improvement was markedly slow<strong>and</strong> neurological outcome poor. Unfortunately, it is not possibleto perform continuous <strong>EEG</strong> monitoring in critically illpatients with altered mental status in our hospital.However, we are aware that this rapidly exp<strong>and</strong>ing electrophysiologictechnique is the method of choice for evaluatingsubjects with cerebral damage <strong>and</strong> unexplained persistentconfusion or coma. 7To summarize, NCSE is a possible severe neurologicalcomplication in older patients suffering from intraventricularhemorrhage. Since an unexplained deterioration of consciousnesslevel may be the sole clinical sign of NCSE inthese subjects, a high level of suspicion <strong>and</strong> an urgent <strong>EEG</strong>will be the cornerstone of an early <strong>and</strong> accurate diagnosis.REFERENCES1. Fernández-Torre JL, Díaz-Castroverde AG. Non-convulsivestatus epilepticus in elderly individuals: report of four representativecases. Age Ageing 2004; 33: 78-81.2. Begemann M, Rowan AJ, Tuhrim S. Treatment of refractorycomplex-partial status epilepticus with propofol: case report.Epilepsia 2000; 41: 105-109.3. Dennis LJ, Claassen J, Hirsch LJ, Emerson RG, ConnollyES, Mayer SA. Nonconvulsive status epilepticus after subarachnoidhemorrhage. Neurosurgery 2002; 51: 1136-1140.4. Wasterlain CG, Fujikawa DG, Penix L, Sankar R. Pathophysiologicalmechanisms of brain damage from statusepilepticus. Epilepsia 1993; 34(suppl 1): S37-S53.5. Krumholz A, Sung GY, Fisher RS, Barry E, Bergey GK,Grattan LM. Complex partial status epilepticus accompaniedby serious morbidity <strong>and</strong> mortality. Neurology 1995; 45:1499-1504.6. F e r n á n d e z - Torre JL, Figols J, Martínez-Martínez M,González-Rato J, Calleja J. Localized-nonconvulsive statusepilepticus: further evidence of permanent cerebral damage.J Neurology 2006; 253: 392-395.7. Hirsh LJ. Continuous <strong>EEG</strong> monitoring in the intensivecare unit: an overview. J Clin Neurophysiology 2004; 21:3 3 2 - 3 4 0 .60

