Family Planning in Asia and the Pacific - International Council on ...
Family Planning in Asia and the Pacific - International Council on ... Family Planning in Asia and the Pacific - International Council on ...
Qualitative assessments by a number of researchers
FigureFigure67Relationship between ideal number of children
- Page 334 and 335: TableTable6TableTable7TableTable832
- Page 336 and 337: TableTable11326
- Page 338 and 339: TableTable14TableTable15TableTable1
- Page 340 and 341: TableTable19Laws and</stron
- Page 342 and 343: worker and hours w
- Page 344 and 345: 334
- Page 346 and 347: 336
- Page 348 and 349: includin</
- Page 350 and 351: TableTable1Contraceptive prevalence
- Page 352 and 353: These results suggest that about 70
- Page 354 and 355: 2 The (period) TFR is the</
- Page 356 and 357: 346
- Page 358 and 359: FigureThe existence of traditional
- Page 360 and 361: Guinea case by <st
- Page 362 and 363: The establishment of provin
- Page 364 and 365: provide family plannin</str
- Page 366 and 367: Figurelegal requirement nor a condi
- Page 368 and 369: FigureTableTable5TableTable6Figure4
- Page 370 and 371: modern method and
- Page 372 and 373: married or in unio
- Page 374 and 375: Figureolder. Both the</stro
- Page 376 and 377: TableTable15The immediate past Nati
- Page 378 and 379: out that the “ne
- Page 380 and 381: Commodity securitySupply cha<strong
- Page 382 and 383: is able to achieve. In Papua New Gu
- Page 386 and 387: increasin<
- Page 388 and 389: service delivery poin</stro
- Page 390 and 391: Population: Views from Men
- Page 392 and 393: 1545-1730Day 2: December 9Session 2
- Page 394 and 395: Day 3, December 10Session 50830-100
- Page 396 and 397: 15Mr. Tong Sithen1
- Page 398 and 399: 54Ms. Shadiya IbrahimAssistant Repr
- Page 400 and 401: 93Mr. Melkie AntonProject OfficerUn
- Page 402 and 403: 131Dr. John P. SkibiakDirectorRepro
- Page 404: International <str
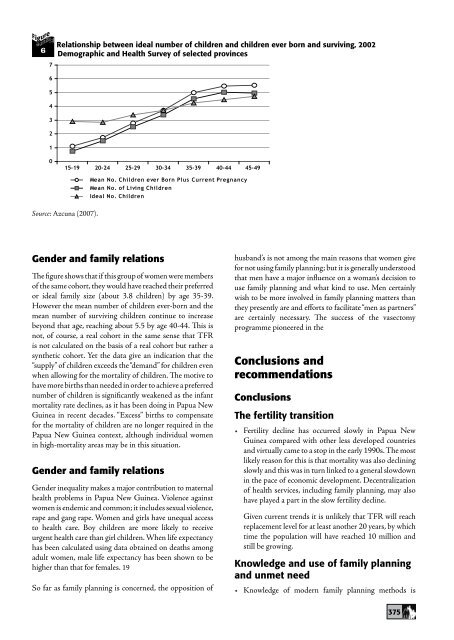
FigureFigure67Relati<strong>on</strong>ship between ideal number of children <str<strong>on</strong>g>and</str<strong>on</strong>g> children ever born <str<strong>on</strong>g>and</str<strong>on</strong>g> surviv<str<strong>on</strong>g>in</str<strong>on</strong>g>g, 2002Demographic <str<strong>on</strong>g>and</str<strong>on</strong>g> Health Survey of selected prov<str<strong>on</strong>g>in</str<strong>on</strong>g>ces654321015-19 20-24 25-29 30-34 35-39 40-44 45-49Mean No. Children ever Born Plus Current PregnancyMean No. of Liv<str<strong>on</strong>g>in</str<strong>on</strong>g>g ChildrenIdeal No. ChildrenSource: Azcuna (2007).Gender <str<strong>on</strong>g>and</str<strong>on</strong>g> family relati<strong>on</strong>sThe figure shows that if this group of women were membersof <str<strong>on</strong>g>the</str<strong>on</strong>g> same cohort, <str<strong>on</strong>g>the</str<strong>on</strong>g>y would have reached <str<strong>on</strong>g>the</str<strong>on</strong>g>ir preferredor ideal family size (about 3.8 children) by age 35-39.However <str<strong>on</strong>g>the</str<strong>on</strong>g> mean number of children ever-born <str<strong>on</strong>g>and</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g>mean number of surviv<str<strong>on</strong>g>in</str<strong>on</strong>g>g children c<strong>on</strong>t<str<strong>on</strong>g>in</str<strong>on</strong>g>ue to <str<strong>on</strong>g>in</str<strong>on</strong>g>creasebey<strong>on</strong>d that age, reach<str<strong>on</strong>g>in</str<strong>on</strong>g>g about 5.5 by age 40-44. This isnot, of course, a real cohort <str<strong>on</strong>g>in</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> same sense that TFRis not calculated <strong>on</strong> <str<strong>on</strong>g>the</str<strong>on</strong>g> basis of a real cohort but ra<str<strong>on</strong>g>the</str<strong>on</strong>g>r asyn<str<strong>on</strong>g>the</str<strong>on</strong>g>tic cohort. Yet <str<strong>on</strong>g>the</str<strong>on</strong>g> data give an <str<strong>on</strong>g>in</str<strong>on</strong>g>dicati<strong>on</strong> that <str<strong>on</strong>g>the</str<strong>on</strong>g>“supply” of children exceeds <str<strong>on</strong>g>the</str<strong>on</strong>g> “dem<str<strong>on</strong>g>and</str<strong>on</strong>g>” for children evenwhen allow<str<strong>on</strong>g>in</str<strong>on</strong>g>g for <str<strong>on</strong>g>the</str<strong>on</strong>g> mortality of children. The motive tohave more births than needed <str<strong>on</strong>g>in</str<strong>on</strong>g> order to achieve a preferrednumber of children is significantly weakened as <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>in</str<strong>on</strong>g>fantmortality rate decl<str<strong>on</strong>g>in</str<strong>on</strong>g>es, as it has been do<str<strong>on</strong>g>in</str<strong>on</strong>g>g <str<strong>on</strong>g>in</str<strong>on</strong>g> Papua NewGu<str<strong>on</strong>g>in</str<strong>on</strong>g>ea <str<strong>on</strong>g>in</str<strong>on</strong>g> recent decades. “Excess” births to compensatefor <str<strong>on</strong>g>the</str<strong>on</strong>g> mortality of children are no l<strong>on</strong>ger required <str<strong>on</strong>g>in</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g>Papua New Gu<str<strong>on</strong>g>in</str<strong>on</strong>g>ea c<strong>on</strong>text, although <str<strong>on</strong>g>in</str<strong>on</strong>g>dividual women<str<strong>on</strong>g>in</str<strong>on</strong>g> high-mortality areas may be <str<strong>on</strong>g>in</str<strong>on</strong>g> this situati<strong>on</strong>.Gender <str<strong>on</strong>g>and</str<strong>on</strong>g> family relati<strong>on</strong>sGender <str<strong>on</strong>g>in</str<strong>on</strong>g>equality makes a major c<strong>on</strong>tributi<strong>on</strong> to maternalhealth problems <str<strong>on</strong>g>in</str<strong>on</strong>g> Papua New Gu<str<strong>on</strong>g>in</str<strong>on</strong>g>ea. Violence aga<str<strong>on</strong>g>in</str<strong>on</strong>g>stwomen is endemic <str<strong>on</strong>g>and</str<strong>on</strong>g> comm<strong>on</strong>; it <str<strong>on</strong>g>in</str<strong>on</strong>g>cludes sexual violence,rape <str<strong>on</strong>g>and</str<strong>on</strong>g> gang rape. Women <str<strong>on</strong>g>and</str<strong>on</strong>g> girls have unequal accessto health care. Boy children are more likely to receiveurgent health care than girl children. When life expectancyhas been calculated us<str<strong>on</strong>g>in</str<strong>on</strong>g>g data obta<str<strong>on</strong>g>in</str<strong>on</strong>g>ed <strong>on</strong> deaths am<strong>on</strong>gadult women, male life expectancy has been shown to behigher than that for females. 19So far as family plann<str<strong>on</strong>g>in</str<strong>on</strong>g>g is c<strong>on</strong>cerned, <str<strong>on</strong>g>the</str<strong>on</strong>g> oppositi<strong>on</strong> ofhusb<str<strong>on</strong>g>and</str<strong>on</strong>g>’s is not am<strong>on</strong>g <str<strong>on</strong>g>the</str<strong>on</strong>g> ma<str<strong>on</strong>g>in</str<strong>on</strong>g> reas<strong>on</strong>s that women givefor not us<str<strong>on</strong>g>in</str<strong>on</strong>g>g family plann<str<strong>on</strong>g>in</str<strong>on</strong>g>g; but it is generally understoodthat men have a major <str<strong>on</strong>g>in</str<strong>on</strong>g>fluence <strong>on</strong> a woman’s decisi<strong>on</strong> touse family plann<str<strong>on</strong>g>in</str<strong>on</strong>g>g <str<strong>on</strong>g>and</str<strong>on</strong>g> what k<str<strong>on</strong>g>in</str<strong>on</strong>g>d to use. Men certa<str<strong>on</strong>g>in</str<strong>on</strong>g>lywish to be more <str<strong>on</strong>g>in</str<strong>on</strong>g>volved <str<strong>on</strong>g>in</str<strong>on</strong>g> family plann<str<strong>on</strong>g>in</str<strong>on</strong>g>g matters than<str<strong>on</strong>g>the</str<strong>on</strong>g>y presently are <str<strong>on</strong>g>and</str<strong>on</strong>g> efforts to facilitate “men as partners”are certa<str<strong>on</strong>g>in</str<strong>on</strong>g>ly necessary. The success of <str<strong>on</strong>g>the</str<strong>on</strong>g> vasectomyprogramme pi<strong>on</strong>eered <str<strong>on</strong>g>in</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g>C<strong>on</strong>clusi<strong>on</strong>s <str<strong>on</strong>g>and</str<strong>on</strong>g>recommendati<strong>on</strong>sC<strong>on</strong>clusi<strong>on</strong>sThe fertility transiti<strong>on</strong>Fertility decl<str<strong>on</strong>g>in</str<strong>on</strong>g>e has occurred slowly <str<strong>on</strong>g>in</str<strong>on</strong>g> Papua NewGu<str<strong>on</strong>g>in</str<strong>on</strong>g>ea compared with o<str<strong>on</strong>g>the</str<strong>on</strong>g>r less developed countries<str<strong>on</strong>g>and</str<strong>on</strong>g> virtually came to a stop <str<strong>on</strong>g>in</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> early 1990s. The mostlikely reas<strong>on</strong> for this is that mortality was also decl<str<strong>on</strong>g>in</str<strong>on</strong>g><str<strong>on</strong>g>in</str<strong>on</strong>g>gslowly <str<strong>on</strong>g>and</str<strong>on</strong>g> this was <str<strong>on</strong>g>in</str<strong>on</strong>g> turn l<str<strong>on</strong>g>in</str<strong>on</strong>g>ked to a general slowdown<str<strong>on</strong>g>in</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> pace of ec<strong>on</strong>omic development. Decentralizati<strong>on</strong>of health services, <str<strong>on</strong>g>in</str<strong>on</strong>g>clud<str<strong>on</strong>g>in</str<strong>on</strong>g>g family plann<str<strong>on</strong>g>in</str<strong>on</strong>g>g, may alsohave played a part <str<strong>on</strong>g>in</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> slow fertility decl<str<strong>on</strong>g>in</str<strong>on</strong>g>e.Given current trends it is unlikely that TFR will reachreplacement level for at least ano<str<strong>on</strong>g>the</str<strong>on</strong>g>r 20 years, by whichtime <str<strong>on</strong>g>the</str<strong>on</strong>g> populati<strong>on</strong> will have reached 10 milli<strong>on</strong> <str<strong>on</strong>g>and</str<strong>on</strong>g>still be grow<str<strong>on</strong>g>in</str<strong>on</strong>g>g.Knowledge <str<strong>on</strong>g>and</str<strong>on</strong>g> use of family plann<str<strong>on</strong>g>in</str<strong>on</strong>g>g<str<strong>on</strong>g>and</str<strong>on</strong>g> unmet needKnowledge of modern family plann<str<strong>on</strong>g>in</str<strong>on</strong>g>g methods is375


