Application for License to Operate a Hospital - CHD-Davao Region
Application for License to Operate a Hospital - CHD-Davao Region
Application for License to Operate a Hospital - CHD-Davao Region

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
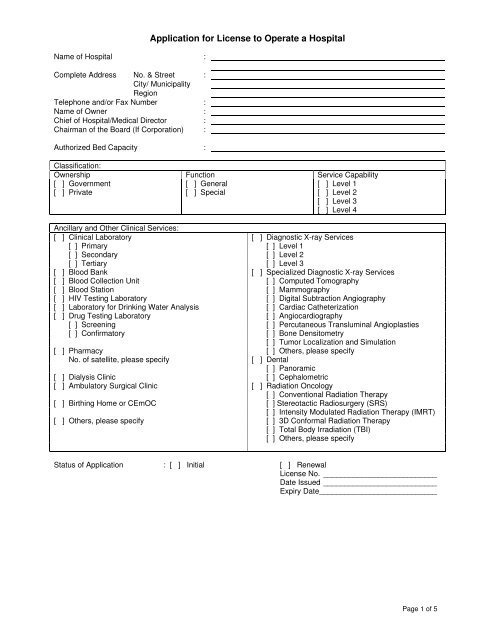
Name of <strong>Hospital</strong> :Complete Address No. & Street :City/ Municipality<strong>Region</strong>Telephone and/or Fax Number :Name of Owner :Chief of <strong>Hospital</strong>/Medical Direc<strong>to</strong>r :Chairman of the Board (If Corporation) :Authorized Bed Capacity :<strong>Application</strong> <strong>for</strong> <strong>License</strong> <strong>to</strong> <strong>Operate</strong> a <strong>Hospital</strong>Classification:Ownership Function Service Capability[ ] Government[ ] Private[ ] General[ ] Special[ ] Level 1[ ] Level 2[ ] Level 3[ ] Level 4Ancillary and Other Clinical Services:[ ] Clinical Labora<strong>to</strong>ry [ ] Diagnostic X-ray Services[ ] Primary [ ] Level 1[ ] Secondary [ ] Level 2[ ] Tertiary [ ] Level 3[ ] Blood Bank [ ] Specialized Diagnostic X-ray Services[ ] Blood Collection Unit [ ] Computed Tomography[ ] Blood Station [ ] Mammography[ ] HIV Testing Labora<strong>to</strong>ry [ ] Digital Subtraction Angiography[ ] Labora<strong>to</strong>ry <strong>for</strong> Drinking Water Analysis [ ] Cardiac Catheterization[ ] Drug Testing Labora<strong>to</strong>ry [ ] Angiocardiography[ ] Screening [ ] Percutaneous Transluminal Angioplasties[ ] Confirma<strong>to</strong>ry [ ] Bone Densi<strong>to</strong>metry[ ] Tumor Localization and Simulation[ ] Pharmacy [ ] Others, please specifyNo. of satellite, please specify[ ] Dental[ ] Panoramic[ ] Dialysis Clinic [ ] Cephalometric[ ] Ambula<strong>to</strong>ry Surgical Clinic [ ] Radiation Oncology[ ] Conventional Radiation Therapy[ ] Birthing Home or CEmOC [ ] Stereotactic Radiosurgery (SRS)[ ] Intensity Modulated Radiation Therapy (IMRT)[ ] Others, please specify [ ] 3D Con<strong>for</strong>mal Radiation Therapy[ ] Total Body Irradiation (TBI)[ ] Others, please specifyStatus of <strong>Application</strong> : [ ] Initial [ ] Renewal<strong>License</strong> No. ___________________________Date Issued ___________________________Expiry Date ____________________________Page 1 of 5
Checklist of <strong>Application</strong> Documents1) For INITIAL or RENEWAL, please tick () the appropriate boxes under column B or C and provide necessary documents.2) Items shaded are not required. However, if there are changes in in<strong>for</strong>mation upon RENEWAL, please tick () theappropriate boxes under column C and provide necessary documents.ADocumentsRequired For All <strong>Hospital</strong>s1. <strong>Hospital</strong>1.1. Notarized duly accomplished <strong>Application</strong> <strong>for</strong> <strong>License</strong> <strong>to</strong> <strong>Operate</strong> a<strong>Hospital</strong> (this <strong>for</strong>m)1.2. List of Personnel (use ANNEX A)1.3. Pho<strong>to</strong>copies of the following:1.3.1. Proof of qualification1.3.1.1. PRC ID1.3.1.2. Certificate of Training1.4. List of Equipment/ Instrument (use ANNEX B)1.5. Location map <strong>for</strong> the hospital1.6. Pho<strong>to</strong>graphs of the exterior and interior of the hospital1.7. Annual <strong>Hospital</strong> Statistical ReportBInitial<strong>Application</strong>CRenewal<strong>Application</strong>2. Clinical Labora<strong>to</strong>ry2.1. List of Personnel (use ANNEX A)2.2. Pho<strong>to</strong>copies of the following:2.2.1. Proof of qualification of pathologist and medical technologist2.2.1.1. PRC ID2.2.1.2. Specialty Board Certificate (<strong>for</strong> pathologist)2.2.1.3. Certificate of Training2.3. List of Equipment, Reagent, Labora<strong>to</strong>ry Ware and Materials <strong>for</strong>Specific Test (use ANNEX C)2.4. Quality Manual (<strong>to</strong> be fully implemented by January 1, 2009) Submitchanges only2.5. Certificate of Participation in External Quality Assurance Program2.6. Memorandum of Agreement, if not owned by the hospital3. Pharmacy3.1. List of Personnel (use ANNEX A)3.2. Pho<strong>to</strong>copies of the following:3.2.1. Proof of qualification of pharmacist3.2.1.1. PRC ID3.2.1.2. Certificate of Training in Licensing of DrugEstablishments and Outlets3.3. List of Products (use ANNEX D)3.4. Memorandum of Agreement, if not owned by the hospital4. Radiology4.1. List of Diagnostic Radiology and Radiation Oncology Services byCategory (use ANNEX E)4.2. List of Personnel <strong>for</strong> Diagnostic Radiology and Radiation OncologyServices (use ANNEX F)4.3. For diagnostic radiology services, pho<strong>to</strong>copies of the following:4.3.1. Proof of qualification of radiologist and radiologic/ x-raytechnologist4.3.1.1. PRC ID4.3.1.2. Specialty Board Certificate (<strong>for</strong> radiologist)4.3.1.3. Certificate of Training4.4. For radiation oncology services, pho<strong>to</strong>copies of the following:4.4.1. Proof of qualification of radiation oncologist/ medicalphysicist/ radiotherapy technologistPage 2 of 5
ADocuments4.4.1.1. PRC ID (<strong>for</strong> radiation oncologist and radiotherapytechnologist)4.4.1.2. Specialty Board Certificate (<strong>for</strong> radiation oncologist)4.4.1.3. Masters Degree in Medical Physics (<strong>for</strong> medicalphysicist)4.4.1.4. Certificate of Training4.5. List of X-ray Machines (use ANNEX G)4.6. Acceptance/Per<strong>for</strong>mance Test Result <strong>for</strong> Computed Tomography andMammography x-ray machines4.7. Pho<strong>to</strong>copy of official receipt from PNRI <strong>for</strong> new film badgesubscription <strong>for</strong> one year4.8. Pho<strong>to</strong>copy of film badge personal dose evaluation reports within thevalidity period of the hospital license4.9. Certificate of compliance with pre-operational requirements <strong>for</strong>medical linear accelera<strong>to</strong>r facility4.10. Facility report on the installation and commissioning of the equipmentduly signed by the facility’s qualified medical physicist and thetechnical representative of the equipment manufacturer/supplier4.11. Con<strong>for</strong>mance testing report of the BHDT medical physics team on thex-ray units in the medical linear accelera<strong>to</strong>r facility4.12. Quality audit report of the BHDT health physics team on the medicallinear accelera<strong>to</strong>r facilityWhen Provided by the <strong>Hospital</strong>5. Dialysis Clinic5.1. List of Personnel (use ANNEX A)5.2. Pho<strong>to</strong>copies of the following:5.2.1. Proof of qualification of medical and paramedical staff5.2.1.1. PRC ID5.2.1.2. Certificate of Training5.3. List of Equipment/ Instrument (use ANNEX B)5.4. Manual of Operations/ SOP5.5. Annual Summary Report of Patients Registered <strong>to</strong> the Renal DiseaseRegistry (Certificate of Compliance)5.6. Documented Quality Assurance Program (QAP)6. Blood Station/ Blood Collection Unit6.1. List of Personnel (use ANNEX A)6.2. Pho<strong>to</strong>copies of the following:6.2.1. Proof of qualification of medical technologist and donorrecruitment officer6.2.1.1. PRC ID6.2.1.2. Certificate of Training6.3. List of Equipment, Labora<strong>to</strong>ry Ware and Materials (use ANNEX H)6.4. Documented Blood Transfusion Committee6.5. Certificate of Inclusion in the Official Blood Services Network ofNVBSP6.6. Recommendation from the Zonal/ <strong>Region</strong>al Blood Services Network6.7. Annual Accomplishment Report using NVBSP Form7. Blood Bank7.1. List of Personnel (use ANNEX A)7.2. Pho<strong>to</strong>copies of the following:7.2.1. Proof of qualification of medical technologist and donorrecruitment officer7.2.1.1. PRC ID7.2.1.2. Certificate of Training7.3. List of Equipment, Labora<strong>to</strong>ry Ware and Materials (use ANNEX H)BInitial<strong>Application</strong>CRenewal<strong>Application</strong>Page 3 of 5
ADocuments7.4. Certificate of Inclusion in the Official Blood Services Network ofNVBSP7.5. List of Blood Stations and Blood Collection Units within the network7.6. Documented Blood Transfusion Committee7.7. Annual Accomplishment Report using NVBSP Form8. HIV Testing Labora<strong>to</strong>ry8.1. List of Personnel (use ANNEX A)8.2. Pho<strong>to</strong>copies of the following:8.2.1. Proof of qualification of medical technologist8.2.1.1. PRC ID8.2.1.2. Certificate of Training8.3. List of Testing Materials (use ANNEX I)9. Labora<strong>to</strong>ry <strong>for</strong> Drinking Water Analysis9.1. List of Personnel (use ANNEX A)9.2. Pho<strong>to</strong>copies of the following:9.2.1. Proof of qualification of analyst9.2.1.1. PRC ID9.2.1.2. PSP Certificate, if applicable9.2.1.3. Certificate of Training9.3. List of Parameters <strong>for</strong> Each Service Capability (use ANNEX J9.4. List of Equipment, Reagent, Labora<strong>to</strong>ry Ware and Materials <strong>for</strong>Specific Test (use ANNEX K)9.5. Quality Manual <strong>for</strong> Drinking Water Analysis10. Drug Testing Labora<strong>to</strong>ry10.1. List of Personnel (use ANNEX A)10.2. Pho<strong>to</strong>copies of the following:10.2.1. Proof of qualification of head of the labora<strong>to</strong>ry, analyst andauthorized specimen collec<strong>to</strong>r10.2.1.1. PRC ID10.2.1.2. PAM Registration, if applicable10.2.1.3. Certificate of Training10.3. List of Equipment/ Instrument (use ANNEX B)10.4. Documentation of Chain of Cus<strong>to</strong>dy10.5. Quality Control Program (<strong>for</strong> screening labora<strong>to</strong>ry) ORCertification <strong>for</strong> Quality Standard System by a DOH recognized certifyingbody (<strong>for</strong> confirma<strong>to</strong>ry labora<strong>to</strong>ry)10.6. Certificate of Proficiency/ Proficiency Testing Result10.7. Procedure Manual11. Ambula<strong>to</strong>ry Surgical Clinic11.1. List of Personnel (use ANNEX A)11.2. Pho<strong>to</strong>copies of the following:11.2.1. Proof of qualification11.2.1.1. PRC ID11.2.1.2. Specialty Board Certificate11.2.1.3. Certificate of Training11.3. List of Equipment/ Instrument (use ANNEX B)11.4. List of Surgical Operations/ Procedures11.5. Documented Quality Assurance ProgramBInitial<strong>Application</strong>CRenewal<strong>Application</strong>12. Birthing Home or Comprehensive Emergency Obstetric Care (CEmOC)12.1. List of Personnel (use ANNEX A)12.2. Pho<strong>to</strong>copies of the following:12.2.1. Proof of qualification12.2.1.1. PRC ID12.2.1.2. Specialty Board Certificate12.2.1.3. Certificate of TrainingPage 4 of 5
ADocuments12.3. List of Equipment/ Instrument (use ANNEX B)BInitial<strong>Application</strong>CRenewal<strong>Application</strong>Page 5 of 5
ANNEX MRepublic of the Philippines )City/Municipality of _______________ ) S. S.AcknowledgementI, ____________________________, ____________________________, of legal age,Civil StatusNameDesignation______________, a resident of __________________________________________________,Home Addressafter having been sworn in accordance with law hereby depose and say that I am executing thisaffidavit <strong>to</strong> attest <strong>to</strong> the completeness and truth of the <strong>for</strong>egoing in<strong>for</strong>mation and the attacheddocuments and <strong>to</strong> the hospital’s compliance with all standards and requirements <strong>for</strong> theRegistration and Initial/ Renewal of <strong>License</strong> <strong>to</strong> <strong>Operate</strong> a <strong>Hospital</strong> as set by the Department ofHealth._____________________________SignatureBe<strong>for</strong>e me, this _______ day of ______________ 2007 in the City/ Municipality of_____________________, Philippines, personally appeared the above affiant with CommunityTax Certificate No. _____________________ issued on _____________________ at_____________________, known <strong>to</strong> me <strong>to</strong> be the same person/s who executed the <strong>for</strong>egoinginstrument and they acknowledge <strong>to</strong> me that the same is their free act and deed.IN WITNESS WHEREOF, I have hereun<strong>to</strong> set my hands this _________day of_______________ 2007.Doc. No. _________ ;Page No. ________ ;Book No. ________ ;Series of 20 _______NOTARY PUBLICMy Commission ExpiresDecember 31, 20______