New Patient Questionnaire - Sleep
New Patient Questionnaire - Sleep
New Patient Questionnaire - Sleep

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
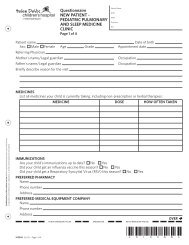
<strong>Questionnaire</strong>new patient, sleep -pediatric pulmonaryand sleep medicineclinicPage 1 of 4<strong>Patient</strong> NameDOBMRNPhysicianFIN<strong>Patient</strong> nameDate of birthSex: Male Female Age Grade Appointment dateReferring PhysicianMother's name/Legal guardianOccupationFather's name/Legal guardianOccupationBriefly describe reason for the visitMedicinesList all medicines your child is currently taking, including non-prescription or herbal therapies:M E D I mediCine dose HOW OFTEN TAKENConfidentiality of this medical record shall be maintained except when use or disclosureis required or permitted by law, regulation, or written authorization by the patient.PREFERRED PHARMACYNamePhoneAddressPREFERRED MEDICAL EQUIPMENT COMPANYNamePhoneAddressBIRTH INFORMATIONBirth weightGestational ageDelivery methodAdditional birth informationdo not mark below this line barcode zone do not mark below this lineover X15301 (6/12) – Page of 4*X15301*
new patient, sleep - pediatric pulmonary and sleep medicine clinic(CONTINUED)Page 2 of 4GENERAL SLEEP INFORMATIONSLEEP HISTORYDoes your child have a regular bedtime routine? No YesDoes your child have his/her own bed? No YesDoes your child have his/her own bedroom? No YesIs a parent present when your child falls asleep? No YesWhere does your child usually fall asleep?His/her room, own bed (alone) Parent room, own bed Parent room, parent bedSibling room, own bed Sibling room, sibling bed OtherWhere does your child usually spend most of the night?His/her room, own bed (alone) Parent room, own bed Parent room, parent bedSibling room, own bed Sibling room, sibling bed OtherWhere does your child usually wake up in the morning at?His/her room, own bed (alone) Parent room, own bed Parent room, parent bedSibling room, own bed Sibling room, sibling bed OtherWho is your child usually put to bed by: Mother Father Both parents Self OtherDoes your child resist going to bed? No Yes If yes, do you feel this is a problem? No YesDoes your child have difficultyfalling asleep? No Yes If yes, do you feel this is a problem? No YesDoes your child awaken duringthe night? No Yes If yes, do you feel this is a problem? No YesAfter nighttime waking, child hasdifficulty falling back to sleep? No Yes If yes, do you feel this is a problem? No YesIs your child difficult to wake upin the morning? No Yes If yes, do you feel this is a problem? No YesIs your child is a poor sleeper? No Yes If yes, do you feel this is a problem? No YesSLEEP SCHEDULEWhat is the amount of time the child spends in their bedroom before going to sleep?X15301 (6/12) – Page of 4minutesWhat is the amount of time your child sleeps during a 24-hour period on weekdays? hours minutesWhat is your child's usual bedtime on weekday nights? :What is your child's usual waketime on weekday nights? :What is the amount of time your child sleeps during a 24-hour period on weekendsand holidays? hours minutesWhat is your child's usual bedtime on weekend/holiday nights? :What is your child's usual waketime on weekday/holiday nights? :What is in the number of days per week your child has a nap?days per weekIf your child naps, write in the usual nap time(s): Nap 1: : AM/ PM to : AM/ PMNap 2: : AM/ PM to : AM/ PMcontinue to next page Confidentiality of this medical record shall be maintained except when use or disclosureis required or permitted by law, regulation, or written authorization by the patient.
Confidentiality of this medical record shall be maintained except when use or disclosureis required or permitted by law, regulation, or written authorization by the patient.CURRENT SLEEP SYMPTOMS (check the appropriate column for each symptom)Difficulty breathing during sleepStops breathing during sleepSnoresRestless sleepSweating during sleepDaytime sleepinessNightmares<strong>Sleep</strong>walking<strong>Sleep</strong>talkingScreaming during sleepKicks legs during sleepWakes up at nightGets out of bed at nightTrouble staying in their bedResists going to bedTeeth grindingWets bedUncomfortable feeling in legs(ie. "creepy-crawly)Trouble getting up in the morningFalls asleep in schoolNaps after schoolDaytime sleepinessFeels weak or loses control of theirwith strong emotionsReports feeling unable to move whenfalling asleep or upon waking upSees frightening visual images beforefalling asleep or upon waking upMorning headachesX15301 (6/12) – Page of 4new patient, sleep -pediatric pulmonaryand sleep medicineclinic (CONTINUED)Page 3 of 4<strong>Patient</strong> NameDOBMRNPhysicianFINNever Not often sometimes Often Always Unsure(less than (1 to 2 (3 to 5 (6 to 71 day/week) days/week) days/week) days/week)over
new patient, sleep - pediatric pulmonary and sleep medicine clinic(CONTINUED)Page 4 of 4MEDICAL HISTORYHas your child ever had any of the following?Abnormal chest x-ray No YesAllergies No YesAnemia No YesAsthma No YesBronchiectasis No YesChronic bronchitis No YesCoughing up blood No YesDevelopmental delay No YesDiabetes No YesDown's syndrome No YesDysphagia No YesEpilepsy/Seizures No YesEczema No YesOther medical historyFrequent ear infections No YesGastrointestinal reflux No YesHeart problems No YesHives No YesHigh blood pressure No YesNeuromuscular problem No YesObesity No YesPneumonia No YesPoor weight gain No YesPremature No YesPulmonary embolism/blood clot No Yes<strong>Sleep</strong> apnea No YesTuberculosis No YesList any other doctors or therapists involved in your child's careAllergistSurgical history with datesAdenoidectomy? No Yes on Bronchoscopy? No Yes onCircumcision? No Yes on Ear tubes? No Yes onGastric tube? No Yes on Lobectomy? No Yes onNissen fundoplication? No Yes on Sinus surgery? No Yes onTonsillectomy? No Yes on Other? No Yes onFAMILY HISTORYRelationship name AGEM=MaternalP=PaternalMotherFatherSisterBrotherM AuntM UncleP AuntP UncleM GrandmotherM GrandfatherP GrandmotherP GrandfatherOtherOther Social HistoryDoes your child live with his/her parents(s)? No Yes Who lives in the home?Is your child adopted? No Yes If yes, at what age?Name of person completing the formDateX15301 (6/12) – Page of 4SignatureAsthmaAllergiesGERDHeart DiseaseDepressionHypertensionStrokeDiabetesADHDObstructive<strong>Sleep</strong> ApneaSnoringRestless legsyndromeNarcolepsyEpilepsyConfidentiality of this medical record shall be maintained except when use or disclosureis required or permitted by law, regulation, or written authorization by the patient.