new patient form - Helen DeVos Children's Hospital
new patient form - Helen DeVos Children's Hospital
new patient form - Helen DeVos Children's Hospital

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
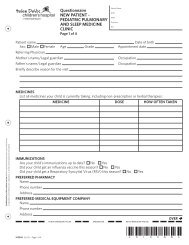
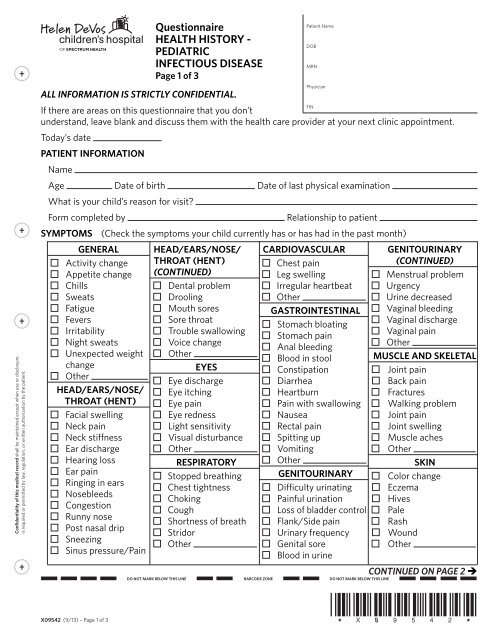
HEALTH HISTORY -PEDIATRICINFECTIOUS DISEASE(CONTINUED)Page 2 of 3Patient NameDOBMRNPhysicianFINSYMPTOMS (CONTINUED)NEUROLOGICALDizzinessFacial weaknessHeadachesLightheadednessNumbnessSeizuresSpeech difficultyFaintingTremorsWeaknessOther(Check the symptoms your child currently has or has had in the past month)HEMTOLOGICSwollen lymph nodesAnemiaBruises/Bleeds easilyGum bleedingOtherBEHAVIORALAgitatedAnxietyBehavioral problemConfusionBEHAVIORAL(CONTINUED)DecreasedconcentrationDepressionHallucinationsHyperactiveNervous/AnxiousTries to injure selfSleep disturbanceSuicidal ideasOtherSLEEPTeeth grindingGasping/pausingSnoringOtherMEDICINES List medicines child is currently takingALLERGIES/SENSITIVITIES/REACTIONConfidentiality of this medical record shall be maintained except when use or disclosureis required or permitted by law, regulation, or written authorization by the <strong>patient</strong>.FAMILY HISTORYX09542 (9/13) – Page 2 of 3(Fill in health in<strong>form</strong>ation about your child’s family)Relation to Child Age State of HealthFatherMotherBrother/ SisterBrother/ SisterBrother/ SisterBrother/ SisterBrother/ SisterBrother/ SisterBrother/ SisterBrother/ SisterBrother/ SisterBrother/ SisterBrother/ SisterBrother/ SisterCheck if your child’s blood relatives have had any of thefollowing:DiseaseRelation to ChildAllergiesArthritisAsthmaBlood disease (e.g. sicklecell trait/disease)Drug use/abuseHIVImmunodeficiencyMRSARheumatological/Autoimmune(lupus, sarcoidosis)TuberculosisOtherCONTINUED ON PAGE 3
HEALTH HISTORY -PEDIATRICINFECTIOUS DISEASE(CONTINUED)Page 3 of 3Patient NameDOBMRNPhysicianHOSPITALIZATIONSYear <strong>Hospital</strong> Reason for <strong>Hospital</strong>izationand OutcomeFINBIRTH HISTORYBirth weight: lb ozType of delivery:Premature Full TermVaginal birth C-sectionDid the child’s mother have anyinfections during pregnancy? No YesIf yes, describeHas your child ever had a blood transfusion? No YesIf yes, give approximate datesDid the baby go home with the motherafter she gave birth? No YesIf no, state reasonSERIOUS ILLNESS / INJURIES DATE OUTCOMEOther in<strong>form</strong>ation about your child you would like to shareConfidentiality of this medical record shall be maintained except when use or disclosureis required or permitted by law, regulation, or written authorization by the <strong>patient</strong>.SOCIAL HISTORY OF YOUR CHILDActivities/InterestsSchool levelPer<strong>form</strong>anceRecent stressors/Traumatic events? No Yes If yes, listOther concernsPharmacy namePhoneRecently traveled? No Yes If yes, whereIs your child adopted? No Yes If yes, from where WhenPets in the house? No Yes Type of petI certify that the above in<strong>form</strong>ation is correct to the best of my knowledge. I will not hold my child’s doctor orany members of his/her staff responsible for any errors or omissions that I may have made in the completionof this <strong>form</strong>.Time Date Person Completing Questionnaire signatureRelationship to childTIME DATE Reviewed byX09542 (9/13) – Page 3 of 3