

The Journal of Dermatology Vol.31 No.6
The Journal of Dermatology Vol.31 No.6
The Journal of Dermatology Vol.31 No.6

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
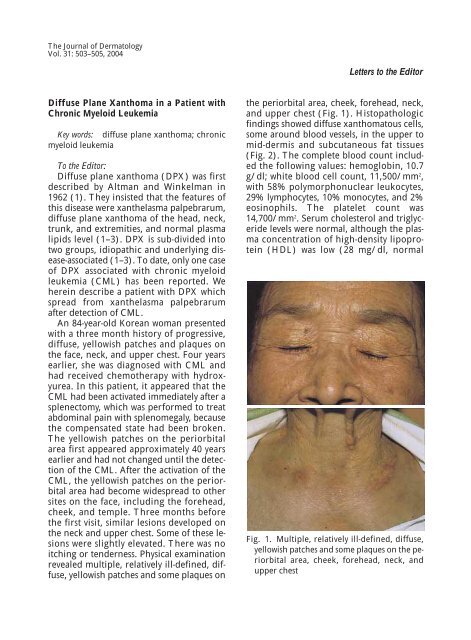
<strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Dermatology</strong>Vol. 31: 503–505, 2004Letters to the EditorDiffuse Plane Xanthoma in a Patient withChronic Myeloid LeukemiaKey words: diffuse plane xanthoma; chronicmyeloid leukemiaTo the Editor:Diffuse plane xanthoma (DPX) was firstdescribed by Altman and Winkelman in1962 (1). <strong>The</strong>y insisted that the features <strong>of</strong>this disease were xanthelasma palpebrarum,diffuse plane xanthoma <strong>of</strong> the head, neck,trunk, and extremities, and normal plasmalipids level (1–3). DPX is sub-divided intotwo groups, idiopathic and underlying disease-associated(1–3). To date, only one case<strong>of</strong> DPX associated with chronic myeloidleukemia (CML) has been reported. Weherein describe a patient with DPX whichspread from xanthelasma palpebrarumafter detection <strong>of</strong> CML.An 84-year-old Korean woman presentedwith a three month history <strong>of</strong> progressive,diffuse, yellowish patches and plaques onthe face, neck, and upper chest. Four yearsearlier, she was diagnosed with CML andhad received chemotherapy with hydroxyurea.In this patient, it appeared that theCML had been activated immediately after asplenectomy, which was performed to treatabdominal pain with splenomegaly, becausethe compensated state had been broken.<strong>The</strong> yellowish patches on the periorbitalarea first appeared approximately 40 yearsearlier and had not changed until the detection<strong>of</strong> the CML. After the activation <strong>of</strong> theCML, the yellowish patches on the periorbitalarea had become widespread to othersites on the face, including the forehead,cheek, and temple. Three months beforethe first visit, similar lesions developed onthe neck and upper chest. Some <strong>of</strong> these lesionswere slightly elevated. <strong>The</strong>re was noitching or tenderness. Physical examinationrevealed multiple, relatively ill-defined, diffuse,yellowish patches and some plaques onthe periorbital area, cheek, forehead, neck,and upper chest (Fig. 1). Histopathologicfindings showed diffuse xanthomatous cells,some around blood vessels, in the upper tomid-dermis and subcutaneous fat tissues(Fig. 2). <strong>The</strong> complete blood count includedthe following values: hemoglobin, 10.7g/dl; white blood cell count, 11,500/mm 2 ,with 58% polymorphonuclear leukocytes,29% lymphocytes, 10% monocytes, and 2%eosinophils. <strong>The</strong> platelet count was14,700/mm 2 . Serum cholesterol and triglyceridelevels were normal, although the plasmaconcentration <strong>of</strong> high-density lipoprotein(HDL) was low (28 mg/dl, normalFig. 1. Multiple, relatively ill-defined, diffuse,yellowish patches and some plaques on the periorbitalarea, cheek, forehead, neck, andupper chest
504Kim et alFig. 2. Many xanthomatous cells in upper tomid-dermis (H & E, ×400).value; 45–65). A diagnosis <strong>of</strong> diffuse planexanthoma associated with CML was made.To date, most reported cases <strong>of</strong> DPX havebeen associated with underlying systemicdiseases. <strong>The</strong>se include multiple myeloma,monoclonal gammopathy, leukemia, lymphoma,Sezary syndrome, Castleman’s disease,Waldenstrom’s macroglobulinemia,cryoglobulinemia, Langerhans cell histiocytosis,and POEMS syndrome (1, 2, 4–9).However, some authors have suggested thatthis phenomenon may be explained on thebasis <strong>of</strong> authors tending to report only thosepatients with a significant association. Patientswithout underlying disorders may beunder-reported (3, 9). Recently, Marcovel etal.(9) reported that only three <strong>of</strong> eight patientshad a reticuloendothelial disease andthat the true incidence <strong>of</strong> an underlying diseaseseemed to be lower than expected.However, patients with DPX must be clinicallyfollowed because this disease can precedethe occurrence <strong>of</strong> an associated condition.Various types <strong>of</strong> leukemia have beenknown to be associated with DPX; these includechronic myelomonocytic leukemia,chronic lymphocytic leukemia, chronicmonoblastic leukemia, chronic granulocyticleukemia, and CML (1, 2, 4–7, 9). Amongthese, only one case <strong>of</strong> CML associated DPXwas described in 1964 by Freud et al.(4).Our patient may be the second case <strong>of</strong> DPXwith CML.<strong>The</strong> pathogenesis <strong>of</strong> DPX remains unknown.However, some possible hypotheseshave been suggested (3, 7). In cases associatedwith monoclonal gammopathy, it is assumedthat paraprotein-lipoprotein complexesmay be recognized by scavenger receptorson macrophages, resulting in thedevelopment <strong>of</strong> cutaneous xanthomas (10).A second hypothesis is that DPX is a histiocytosis-derivedxanthomatosis in the spectrum<strong>of</strong> non-X histiocytosis (9). Otherwise,Vail et al.(7) suggested that the cells in theskin lesions represent direct cutaneous infiltrationby the same leukemic cells found inother organs. Our patient had had periorbitalxanthelasma for about 40 years. <strong>The</strong>selesions had been silent until the CML wasdetected, and then they spread to other siteson the face, neck, and upper chest immediatelyafter the CML was activated. We thinkthat this clinical course may support theabove third hypothesis by Vail et al. Furthermore,this case also suggests that abruptspread <strong>of</strong> pre-existing xanthelasma shouldbe followed by full-examination for the detection<strong>of</strong> any underlying systemic disease.Our case had a low level <strong>of</strong> high-densitylipoprotein (HDL) although her triglycerideand cholesterol levels were within normallimits. Although the exact roles <strong>of</strong> HDLin the xanthoma have not yet been established,HDL is thought to exert a protectiveeffect against tissue cholesterol deposition,and a low plasma level <strong>of</strong> HDL results in adefective removal <strong>of</strong> intracellular cholesterol(11). <strong>The</strong>refore, it is not surprisingthat low levels <strong>of</strong> HDL have been reportedin some patients with xanthelasma andtuberous xanthoma (11). To date, however,there has been no research regarding therole <strong>of</strong> HDL in DPX. It would be worth examiningthe effects <strong>of</strong> HDL in the development<strong>of</strong> DPX.Kyoung Jin KimDeuk Pyo LeeHo Seok Suh*
Diffuse Plane Xanthoma with Chronic Myeloid Leukemia505Mi Woo LeeJee Ho ChoiKee Chan MoonJai Kyoung KohDepartment <strong>of</strong> <strong>Dermatology</strong>Asan Medical CenterUniversity <strong>of</strong> Ulsan College <strong>of</strong> MedicineSeoul, Korea*Department <strong>of</strong> <strong>Dermatology</strong>Ulsan University Hospital, Ulsan, KoreaCorrespondence to: Kyoung Jin Kim, M.D.,Ph.D.Department <strong>of</strong> <strong>Dermatology</strong>Asan Medical CenterUniversity <strong>of</strong> Ulsan College <strong>of</strong> Medicine388-1, Poongnap-dong, Songpa-guSeoul 138-736, KoreaReferences1) Altman J, Winkelmann RK: Diffuse normolipemicplane xanthoma: Generalized xanthelasma, ArchDermatol, 85: 633–640, 1962.2) Lynch PJ, Winkelmann RK: Generalized planexanthoma and systemic disease, Arch Dermatol,93: 639–646, 1966.3) Akhyani M, Daneshpazhooh M, Seirafi H,Naraghi ZS: Diffuse plane xanthoma in an otherwisehealthy woman, Clin Exp Dermatol, 26:405–407, 2001.4) Freud P, Plachta A, Speer FD, Luhby AL:Leukemic xanthomatosis, Amer J Dis Child, 88:43–61, 1964.5) Stockman A, Delanghe J, Geerts M, Naeyaert JM:Diffuse plane normolipaemic xanthomatosis in apatient with chronic lymphatic leukaemia andmonoclonal gammopathy, <strong>Dermatology</strong>, 204:351–354, 2002.6) Derrick EK, Price ML: Plane xanthomatosis withchronic lymphatic leukemia, Clin Exp Dermatol,18: 259–260, 1993.7) Vail JT, Adler KR, Rothenberg J: Cutaneous xanthomasassociated with chronic myelomonocyticleukemia, Arch Dermatol, 121: 1318–1320, 1985.8) Chang SE, Choi JH, Sung KJ, Moon KC, Koh JK,Ro JY: POEMS syndrome with xanthomatouscells, Am J Dermatopathol, 21: 567–570, 1999.9) Marcoval JM, Moreno AM, Bordas X, Gallardo F,Peyri J: Diffuse plane xanthoma: Clinicopathologicstudy <strong>of</strong> 8 cases, J Am Acad Dermatol, 39:439–442, 1998.10) Loo DS, Kang S: Diffuse normolipidemic planexanthomas with monoclonal gammopathy presentingas urticarial plaques, J Am Acad Dermatol,35: 829–832, 1996.11) Parker F: Normocholesterolemic xanthomatosis,Arch Dermatol, 122: 1253–1257, 1996.