VERTEBRAL BONE COLLAPSE IN SICKLE CELL DISEASE: A ...
VERTEBRAL BONE COLLAPSE IN SICKLE CELL DISEASE: A ...
VERTEBRAL BONE COLLAPSE IN SICKLE CELL DISEASE: A ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
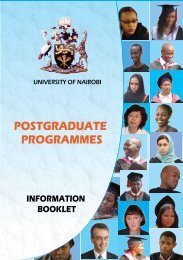
August 2001 EAST AFRICAN MEDICAL JOURNAL 445East African Medical Journal Vol. 78 No. 8 August 2001<strong>VERTEBRAL</strong> <strong>BONE</strong> <strong>COLLAPSE</strong> LN <strong>SICKLE</strong> <strong>CELL</strong> <strong>DISEASE</strong>: A REPORT OF TWO CASESJ. I. Emodi. FMCPaed, Consultant Paediatrician, Department of Paediatrics, and I. J. Okoye, FMCR. Consultant Radiologist. Department of Radiology. University ofNigeria Teaching Hospital, P.M.B. 01280, Enugu. NigeriaRequest for reprints to: Dr. J. I. Emodi, University of Nigeria Teaching Hospital, P.M.B. 01280, Enugu, Nigeria<strong>VERTEBRAL</strong> <strong>BONE</strong> <strong>COLLAPSE</strong> <strong>IN</strong> <strong>SICKLE</strong> <strong>CELL</strong> <strong>DISEASE</strong>: A REPORT OF TWO CASESJ. I. EMODI and 1. J. OKOYESUMMARYWe describe two female children both nine years of age with sickle cell anaemia andcompression deformity of three successive lumbar vertebrae in one child and collapse of onelumbar vertebra in the other. Management for the two children included analgesics,antibiotics and application of a lumbar jacket for stabilisation of the spine. In both patientsthe vertebral bodies remodelling with re-generation of the tissue. This report is being madeto highlight the improved chances of response with early detection and adequate management.<strong>IN</strong>TRODUCTIONSickle cell haemoglobinopathy is common inNigeria,affecting 2-3% ofchildren(l,2). The disease process affectsall the bones in the body and its effect on the vertebralbones have been described. Radiological features of thesevertebral bodies include a coarse trabecular pattern,persistent anterior vertebral notching, biconcavity of thebodies, step ladder effect, massive collapse of the 'centra',and compression deformities(3.4). Most previous reportshave focused on the pathological processes, none haslooked into the management with a view of maximizingthe reparative process and so prevent further damage(5-7).These case reports are presented to illustrate an aspect ofmanagement that has not been previously described forchildren with sickle cell anaemia.hour. There was no malaria parasite and mantoux result was 3mm. Spinal radiograph (Figure I) showed complete resorptionof the anterior vcrtcbral end plate of the residual box of L] .Therewere areas of calcification within the dead bone with loss ofLI -2 disc space and involvement of the contigous surface of thebody of L2. There was generalised thinning of the cortices ofTI 2-L3 vertebral bodies with widened intervertebral spaces andthickening of the trabeculae with a resultant coarse bone texture.Biconcave discs were noted to varying extent throughout thethoraco-lumbar spine.Figure 1Lateral spirurl rctdiogrclphs showir~g verrebrcil body colllp.ve of Ll onthe LEFTund remodelling ofL1 with loss r,f' height otz the RIGHTCASE REPORTSCase I: A nine year old female, N C, presented with a oneweek history of waist pain, intermittent fever and inability tobend forward at the waist. The child's genotype was unknown.Therc was no history of trauma. The pain was dull in characterand non-radiating. Fever which was worse in the eveningsresponded to antipyretics. Mobility atthewaist wasimpaired andthe child walked stiffly. There was no prior history of similarillness, bone pains orjaundice. She was fully immunised and hadno history of contact with any one with tuberculosis.On physical examination, at presentation, she was found tobe of an asthenic build, mildly pale, anicteric, a febrile and notin any obvious distress. She was walking with a marked lumbarlordosis and a stiff gait. The muscle tone and power in the lowerlimbs were normal, thedeep tendon reflexes were not exaggeratedand sensation was intact. There was mild tenderness over thelumbar spine but no gibbus was discernible.She had a splenomegaly cxtending 4 cm below the leftcostal margin. All other systems were essentially normal.Laboratory investigations revealed PCV of 24% genotypeSS, White cell count 10,400 mm3 with a neutrophil of 68%,lymphocyte of 29% and oeosinophil of 3%.The erythrocyte sedimentation tale was 35 mm in the firstShe was managed with antimalarials, analgesics and alumbar jacket was applied initially for six months. Removalresulted in a relapse needing a further two months of the jacket.Spinal radiograph done after 10 months showed Ll vertebralbody remodelling neatly withpersistingL 1-2 disc space loss andloss of height of the anterior portion of L1 (Figure 1).Twelve months after the lumbar jacket was removed shehad no further problems.Case 2: A nine yearold female, 00 presented in this hospitalwith a three week history of waist pain with fever and a four day
446 EAST AFRICAN MEDICAL JOURNAL August 2001had been made at the age of four years. ?he waist pain interferedwith the child's mobility and was worsened by movement at thehips, lower limbs and by standing, but was relieved by the childlying down. The fever was high grade, intermittent and worse inthe evenings. She was initially treated at the emergency room'with intravenousfluids, analgesics, antimalarials and transfusionof one unit of packed cells. She was discharged after 96 hours butfour days later the child was unable to sit up in bed or stand withor without support on account of the pain.On admission into the ward she was found to be fairly wellnourished with the typical sickle cell facies of bossing,gnathopathyandasthenia. Shewaspale, febrile witha temperatureof 38.6"C and anicteric. She was fully conscious and alert,Kemig's sign was negative and the cranial nerves were intact.She had a gibbus over the lower spine and her lower limbs werehyptertonic with hyperreflexia, power was grade 4 and hersensation was intact.There wasa hepatomegaly of8 cm below thecostalmargin,the liver was soft, non tender with a sharp edge and smoothsurface.Investigations disclosed anaemia uith PCV of 23%Erythrocyte sedimentation rateof 150 mln in the first hour, whitebloodcellcountof 17,500mm3 withnetltrophil.479k lymphocyte51%, eosinophils 2%. Mantoux test was negative. Spinalradiographs showed multiple osteolytic les~ons involving thebodies of L3-5 with loss of height of affected vertebral bodies.Therewas reduction in thedisc space between L2-3 and wideningof L3.4 disc space. The pedicles were intact. There was normalalignment of the vertebral body which also showed coarsetraberculae. Blood culture grew stapi~ylococ:cus aureus.A lumbar jacket was applied and the child treated withintravenous antibiotics, initially, followed with oral antibiotics,for a total of six weeks, bed rest and analgesics. The lumbarjacket was removedafterthree months when thespinal radiographsshowed marked healing of the lumbar vertebral bodies withmarked regeneration of the bony tissue.CONCLUSIONMost case reports on vertebral bone destruction insickle cell haemoglobinopathy has focussed on the pathologyand causative factors(4-7). There has been no report maderegarding management of this condition. In view of thereported vanishing of the vertebral bone in a young malefrom thisenvironment, possibly as aresult oflate presentationwhich prevented adequate management(6), we report thesecases where management included application of lumbarjackets to stabilise their spines.The ability of vertebral and other bones, in cases ofsickle cell haemoglobinopathy, to regenerate has beennoted by several authors(3,4). Application of a lumbarjacket might not necessarily hasten this process but wouldhasten ambulation of a patient and allow for outpatientmanagement, especially in this er~vironment whereeconomic factors contribute greatly to patient care. Itwould also help in immobilising the :spine of the patientand prevent further deterioration and loss of bone, therebyimproving the affected patient's well being.One wonders whether the patient, in the report byOzoh et al(6) would have saved his vertebra had he beentreated with a lumbar jacket. The discrepancy in theduration of application of jackets in these two patientscould possibly arise from the causative factors (infectionvs infarct~on) involved in the collapse of the vertebralbodies.ACKNOWLEDGEMENTWe wish to thank Mrs. Jane Atuonwu for her secretarial assistance andMr. Okolo for his photography.REFERENCESI. Kaine W.N. and Udeozo I.O.K. Incidence of sickle cell wait andanaemia in tbo-pre-school children. Nix. J. Puediut. 1981 ; 8:87 -91.2. Hendrickse R.G. Sickle cell anaemia in Nigerian children. Afr. J.Med. 1960: 6: 45-7.3. Serjeant G.R. Bone and Joint Lesions In: Sicklc cell disease.Serjeant GR ed. Oxford University Press, 1985; 168-195 .4. Reynolds J. The skull and spine. Sem. h~ Roet 1987: 22: 168- 175.5. Kooy. A de Heide L.J.. ten Tije A.J., Mulder A.H.. Tanghe H.L.,Kluytlnans. J.A. and Michiels, I.J. Vertebral bone destruction insickle cell diseases infection, infarction or both. Neth. J Med.1996.48:227-31.6. Ozoh.J.O.,Onugbo,M.A.,Nwankwo,N., Ukabarn.S.0.. Umerah,B.C. and Ezenwa. C.C. "Vanishing" of vertebra in a patient withsickle cell haemoglobinopathy. Brit. Med. J. 1990; 301:1368-9.7. Al-Awamy, B., Sumer, T., Nnaeem, MA. and Al-Mouzan M.Pathological fracture ofvertebral colum~~ in aqsociation withsicklecell anaemia in Saudi Arabia. Trop. Ceq. Med. 19x6; 38:421-4.
August 200 1 EAST AFRICAN MEDICAL JOURNAL IXDON'T GAMBLEWITHYOUR CAREER,GET MPSPROFESSIONALPROTECTIONWHY TAKE CHANCESWITH YOUR FUTURE?Medical professionals are constantly atrisk from the consequences of medico-legal mishaps. Don't take chances withyour professional future. Join the MPSnow and get proper professionalprotection:<strong>IN</strong>DEMNiTY to pay your legal costs anddamages in medical negligence claims.REPRESENTATION at inquests,Medical Council and hospital discipliiaryproceedings.ASSISTANCE with complaints andinquiries, and criminal matters arisingfrom your professional practice.ADVICE on ethical problems, medico-legal matters, or anything else that affectsyour professional interests.rs------------------------1 For more information about the MPS please phone Nairobi Name:884350, Pager No. 551 Tel: 247365 now or fill in the couponI1 and send to:- Branch Administrator, The Medical Protection Title:ISociety, P.O. Box 24349, Nairobi; E-mail: mps@africaonline.co.keI HomdPractice or Hospital Address:IIIIIIIIIIIFounded 1892IIL,--------------------------------The Medical Protection Society1A
e certain,.-Count on tneinjectable cephalosporinThe world's top seWg injectable antibiotic'The top d ing hospital product worldwide1Morethan20y&ofexcellent clinical experieneMore than 64 million peopletreated worldwidetocephineftriaxone