A G E N D A 1. APOLOGIES FOR ABSENCE Ian Metcalfe 2 ...
A G E N D A 1. APOLOGIES FOR ABSENCE Ian Metcalfe 2 ... A G E N D A 1. APOLOGIES FOR ABSENCE Ian Metcalfe 2 ...
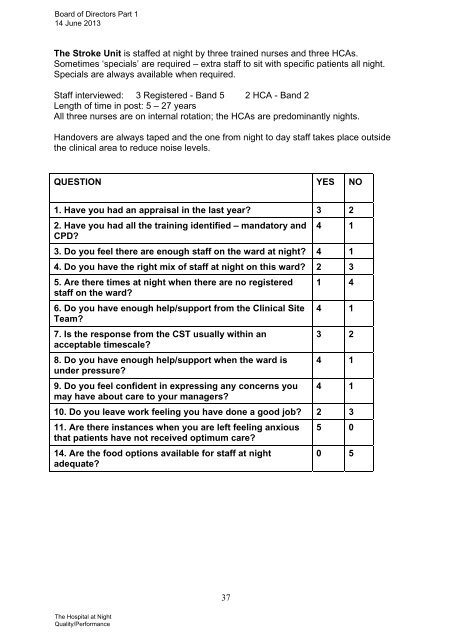
Board of Directors Part 114 June 2013The Stroke Unit is staffed at night by three trained nurses and three HCAs.Sometimes ‘specials’ are required – extra staff to sit with specific patients all night.Specials are always available when required.Staff interviewed: 3 Registered - Band 5 2 HCA - Band 2Length of time in post: 5 – 27 yearsAll three nurses are on internal rotation; the HCAs are predominantly nights.Handovers are always taped and the one from night to day staff takes place outsidethe clinical area to reduce noise levels.QUESTION YES NO1. Have you had an appraisal in the last year? 3 22. Have you had all the training identified – mandatory andCPD?4 13. Do you feel there are enough staff on the ward at night? 4 14. Do you have the right mix of staff at night on this ward? 2 35. Are there times at night when there are no registeredstaff on the ward?6. Do you have enough help/support from the Clinical SiteTeam?7. Is the response from the CST usually within anacceptable timescale?8. Do you have enough help/support when the ward isunder pressure?9. Do you feel confident in expressing any concerns youmay have about care to your managers?1 44 13 24 14 110. Do you leave work feeling you have done a good job? 2 311. Are there instances when you are left feeling anxiousthat patients have not received optimum care?14. Are the food options available for staff at nightadequate?5 00 537The Hospital at NightQuality/Performance
BOARD OF DIRECTORSMeeting Date and Part: 14 June 2013 Part 1Subject:Section:Executive with OverallResponsibilityAuthor of Paper:Details of previousdiscussion and/ordissemination:Key Purpose:Action required by BoD:Monitor’s Enforcement GuidanceDiscussionTony Spotswood, Chief ExecutiveKaren Flaherty, Trust SecretaryN/APatient Safety Health & Safety Performance StrategyXFor informationExecutive Summary:This guidance describes the enforcement powers that Monitor has under the National HealthService Act 2006 in relation to the licensing of providers and also its powers in relation tocompetition law.The powers in relation to licensing include informal action, providers giving enforcementundertakings, imposing discretionary requirements (including monetary penalties up to 10% ofthe provider’s turnover in England), imposing new licence conditions, requiring a trust to remove,suspend or disqualify directors and/or governors and revoking a provider’s licence. Thesepowers may be exercised by Monitor where it finds that a provider is breaching, or hasbreached, one or more of its licence conditions or an enforcement undertaking, or has not met arequirement to hold a licence, or has failed to provide Monitor with information it requires or, inthe case of enforcement undertakings, it has reasonable grounds to suspect that a provider hasdone these things. In relation to compeition law, Monitor’s powers include giving directions tobring an infringement to an end and imposing financial penalties and these powers are heldconcurrently with the Office of Fair Trading.The guidance also sets out how Monitor will prioritise its enforcement action.Strategic Goals & Objectives:AllLinks to CQC Registration:(Outcome reference)Links to AssuranceFramework/Key Risks:Type of Assurance: Internal External
- Page 30 and 31: Board of Directors Part 114th June
- Page 32 and 33: Area Indicator Measure Target Monit
- Page 34 and 35: Trust Performance Dashboard - Quali
- Page 36 and 37: Board of DirectorsJune 2013Financia
- Page 38 and 39: Board of DirectorsJune 20138. Recom
- Page 40 and 41: BOARD OF DIRECTORSMeeting Date and
- Page 42 and 43: Board of Directors Part 114 June 20
- Page 44 and 45: Board of Directors Part 114 June 20
- Page 46 and 47: Board of Directors Part 114 June 20
- Page 48 and 49: Board of Directors Part 114 June 20
- Page 50 and 51: Board of Directors Part 114 June 20
- Page 52 and 53: Board of Directors Part 114 June 20
- Page 54 and 55: Board of Directors Part 114 June 20
- Page 56 and 57: Board of Directors Part 114 June 20
- Page 58 and 59: Board of Directors Part 114 June 20
- Page 60 and 61: Board of Directors Part 114 June 20
- Page 62 and 63: Board of Directors Part 114 June 20
- Page 64 and 65: Board of Directors Part 114 June 20
- Page 66 and 67: Board of Directors Part 114 June 20
- Page 68 and 69: Board of Directors Part 114 June 20
- Page 70 and 71: Board of Directors Part 114 June 20
- Page 72 and 73: Board of Directors Part 114 June 20
- Page 74 and 75: Board of Directors Part 114 June 20
- Page 76 and 77: Board of Directors Part 114 June 20
- Page 78 and 79: Board of Directors Part 114 June 20
- Page 82 and 83: EnforcementGuidance28 March 2013Mon
- Page 84 and 85: ForewordThe Health and Social Care
- Page 86 and 87: 1 IntroductionThe Health and Social
- Page 88 and 89: Table 1.1 Monitor’s enforcement p
- Page 90 and 91: Licence enforcementDiscretionary re
- Page 92 and 93: Competition lawMonitor has concurre
- Page 94 and 95: 2 PrioritisationThis chapter sets o
- Page 96 and 97: We also recognise that the actions
- Page 98 and 99: 3 Imposing discretionary requiremen
- Page 100 and 101: SeriousnessMonitor will take into a
- Page 102 and 103: Deterring similar breaches by other
- Page 104 and 105: An important objective of imposing
- Page 106 and 107: 4 Enforcement - case procedures4.1
- Page 108 and 109: provide regular case updates to par
- Page 110 and 111: including in the application eviden
- Page 112 and 113: In certain circumstances, Monitor m
- Page 114 and 115: Non-compliance penaltiesUnder sched
- Page 116 and 117: Notice of Intent (section 90)Where
- Page 118 and 119: • any incidental or consequential
- Page 120 and 121: Monitor will have concurrent powers
- Page 122 and 123: the first two decision-making point
- Page 124 and 125: Non-compliance penaltiesA provider
- Page 126 and 127: AnnexMonitor’s powers of enforcem
- Page 128 and 129: a) has provided, or is providing, a
Board of Directors Part 114 June 2013The Stroke Unit is staffed at night by three trained nurses and three HCAs.Sometimes ‘specials’ are required – extra staff to sit with specific patients all night.Specials are always available when required.Staff interviewed: 3 Registered - Band 5 2 HCA - Band 2Length of time in post: 5 – 27 yearsAll three nurses are on internal rotation; the HCAs are predominantly nights.Handovers are always taped and the one from night to day staff takes place outsidethe clinical area to reduce noise levels.QUESTION YES NO<strong>1.</strong> Have you had an appraisal in the last year? 3 22. Have you had all the training identified – mandatory andCPD?4 13. Do you feel there are enough staff on the ward at night? 4 14. Do you have the right mix of staff at night on this ward? 2 35. Are there times at night when there are no registeredstaff on the ward?6. Do you have enough help/support from the Clinical SiteTeam?7. Is the response from the CST usually within anacceptable timescale?8. Do you have enough help/support when the ward isunder pressure?9. Do you feel confident in expressing any concerns youmay have about care to your managers?1 44 13 24 14 110. Do you leave work feeling you have done a good job? 2 31<strong>1.</strong> Are there instances when you are left feeling anxiousthat patients have not received optimum care?14. Are the food options available for staff at nightadequate?5 00 537The Hospital at NightQuality/Performance


