Platelet Rich Plasma for Hamstring Tears - Prolotherapy
Platelet Rich Plasma for Hamstring Tears - Prolotherapy
Platelet Rich Plasma for Hamstring Tears - Prolotherapy

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
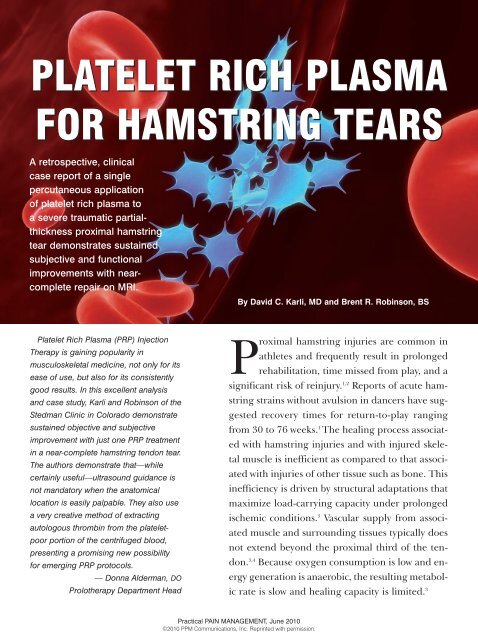
<strong>Platelet</strong> <strong>Rich</strong> <strong>Plasma</strong> <strong>for</strong> <strong>Hamstring</strong> <strong>Tears</strong>Tendons are damaged when subjectedto loads that exceed their tensile or physiologicthreshold. This can occur in responseto massive trauma or to repetitiveoverload if insufficient time is allowed <strong>for</strong>tissue recovery. The risk <strong>for</strong> tendon ruptureis highest when tension is appliedrapidly and obliquely. 3 The highest <strong>for</strong>ceshave been recorded during eccentric contraction.3,5 Tendons respond to this nonphysiologicoverload with tendon sheathinflammation, intratendinous degeneration,or a combination of both. 1,6Muscle and tendon recover from injurythrough tissue remodeling that can leadto inefficient regeneration and infiltrationby scar tissue. 7,8 The first phase involvesan increase in vascular permeability,initiation of angiogenesis, chemotacticmigration of inflammatory cells (notablyneutrophils initially then followed bymacrophages) to the region of injury, andinduction of local tenocytes to synthesizecollagen and extracellular matrix (ECM). 7,8After several days, type III collagen synthesispeaks as tenocyte proliferation continues.At roughly six weeks, the healingtissue begins to remodel. Regional cellularitydecreases as up-regulation of synthesisof collagen and other proteins takesplace. Tissue gradually transitions fromcellular to fibrous in nature as tenocytesalign in the direction of stress <strong>for</strong>ces. Productionof collagen type I increases as productionof type III drops off. At approximately10 weeks, fibrous tissue begins toremodel and mature. These processescontinue through the course of a full year,resulting in tendon tissue with scar-likeproperties. As tissue matures, tenocytemetabolism decreases—either throughintrinsic mechanisms contained within anintact peritenon or through extrinsicmechanisms involving invasion by cellsfrom the surrounding tissue. Extrinsicpathways related to peritenon disruptionand more severe injuries lead to greaterscarring and adhesion and resultant disruptionof the normal gliding of the tendonwithin the sheath. 9,10Traditional hypotheses have attributedpain in tendinopathy to an inflammatoryprocess. Studies of chronically painfulachilles and patellar tendons have shownno evidence of inflammation. Histologically,healing appears to be disorderedand haphazard, with an absence of inflammatorycells but presence of hypercellularity,scattered vascular in-growth, andcollagen degeneration. The etiology ofFIGURE 1A. Pre-procedure MRI — demonstrationof subject proximal hamstring tissueavulsion and hemorrhagic and inflammatorychanges in the sub-acute period.pain within tendons has not been conclusivelyelucidated, but evidence suggeststhat mechanical collagen breakdown, abnormallactate levels, neurotransmitterimbalance, the presence of pro-inflammatoryprostaglandins, and neural centralizationmay be involved. 3Tendon recovery is frequently incompletein severe or full-thickness tears, dueto the proliferation and up-regulation offibroblasts, which induce <strong>for</strong>mation of excessivescar tissue that leads to suboptimaltissue integrity and functionality. 8 Researchsuggests that throughout tendonrepair, trophic substances, such as growthfactors released from damaged tissue,may regulate the healing response. It hasbeen hypothesized that autologousgrowth factors found in platelets may augmentthe healing of musculoskeletal softtissueabnormalities. 8,11-13An understanding of the role ofplatelets in tissue healing has led to theuse of autologous platelet concentrates<strong>for</strong> therapeutic purposes. Degranulationand subsequent release of growth factorsfrom platelets can be induced and the isolatedgrowth factors can be delivered directlyinto injured tissue to stimulate aphysiologic response. <strong>Platelet</strong>-rich plasma(PRP) is easy to produce through centrifugationof peripheral blood and separationof the resulting component. As anFIGURE 1B. Post-procedure MRI — demonstrationof interval healing following percutaneousimplantation of PRP, PPP and AT.autologous substrate, PRP has limited potentialto harm. 11,14 The therapeutic responseof the percutaneous implantationof PRP into tendon, muscle, ligament, cartilage,intervertebral disc, and fascia hasgenerally been positive. 15Numerous growth-factor peptides havebeen identified in both the dense granulesand the alpha granules of platelets,which bind to membrane-bound receptors,thereby activating intracellular second-messengerpathways. 11,16,17 Bioactivefunctions associated with platelet-derivedgrowth factors (PDGFs) include angiogenesis,chemotaxis, cell recruitment, cellularproliferation, cellular differentiation, andECM synthesis. 12 Some researchers havesuggested that, due to the complexity ofhealing pathways and tissue regeneration,the synergistic interaction of multiplegrowth factors at physiologic concentrationsmay be superior to the action of asingle exogenous growth factor. 12,18Case ReportA 48-year-old female sustained a severeleft proximal hamstring tear while waterskiing. Her left leg became hyperextendedwhen she attempted to drop her rightski and the ski caught the water, aggressively<strong>for</strong>cing her left hip into eccentrichyperflexion. Subsequently, she felt atearing sensation localized to the left ischialtuberosity region at the origin of theleft common hamstring tendon. She immediatelyexperienced pain and transientnumbness in the left lower extremity. Ini-Practical PAIN MANAGEMENT, June 2010©2010 PPM Communications, Inc. Reprinted with permission.11
<strong>Platelet</strong> <strong>Rich</strong> <strong>Plasma</strong> <strong>for</strong> <strong>Hamstring</strong> <strong>Tears</strong>FIGURE 2A. Autologous thrombin. Removal ofthe clot following the addition of 10%Calcium Chloride.FIGURE 2B. Autologous thrombin. Harvestingof autologous thrombin prior to injection.tially, she did not seek care, instead relyingon rest and oral nonsteroidal anti-inflammatorydrugs (NSAIDs) <strong>for</strong> two andone-half weeks. During this time, althoughsymptom intensity decreased,pain and dysfunction persisted with ambulation,prolonged sitting, and exertionalactivity. Nocturnal pain interrupted thepatient’s sleep patterns. In addition, thepatient experienced subjective weaknessand instability of the affected leg as wellas localized swelling at the site of injury.Sixteen days after the injury, the patientconsulted an orthopaedic surgeon becauseof the persistence of pain and functionallimitation. The consulting physicianidentified pain on palpation, whichwas localized to the left buttock and aggravatedby resisted knee flexion. Lefthamstring strength was rated 4/5 and leftlower extremity sensory and vascularexams were normal.Radiographs of the pelvis revealed nobony defects at the hamstring insertioninto the ischial tuberosity or evidence ofany other hip-joint abnormality. MRI confirmeda full-thickness tear of the proximalsemimembranosis tendon near themyotendinous junction. Tendon-fiber retractionwas measured to be 3 cm. A partial-thicknesstear of the conjoined bicepsfemoris and semitendinosus tendon at theischial tuberosity insertion was also reported.No bone marrow edema wasnoted. A diffuse hematoma within the regionwas also appreciated (see Figure 1a).After discussion of the surgical and nonsurgicaloptions, the patient opted <strong>for</strong> PRPinjection in an attempt to facilitate healingand recovery in the setting of conservativetherapy. At this point, she was referredto the author <strong>for</strong> the procedure,which was per<strong>for</strong>med on post-injury day16, after all of the risks and details of theprocedure were explained to the patientand consent had been obtained.PROCEDUREProduction of <strong>Platelet</strong> <strong>Rich</strong> <strong>Plasma</strong>With sterile technique, 60mL of wholeblood was collected by peripheral phlebotomyinto a syringe containing 6 cc ofthe anticoagulant citrate dextrose solutionA (ACD-A, Cytosol Laboratories,Braintree, MA). The specimen wasprocessed with a Harvest ® SmartPReP ®centrifugation system and 60mL disposablekit (Harvest Technologies, Plymouth,MA). The blood sample was loaded, centrifuged,and harvested following themanufacturer’s protocol. The initial60mL of whole blood yielded 7mL of PRP,which was drawn into a sterile syringe.The red blood cell fraction was discarded,and the platelet-poor plasma (PPP) wassaved <strong>for</strong> the production of autologousthrombin (AT).Activation of <strong>Platelet</strong>-Poor <strong>Plasma</strong> andProduction of Autologous ThrombinSupernatantOnce the whole blood was separated, 7mLof the PPP was added to each of two 10-mL glass BD Vacutainer tubes (BD,Franklin Lakes, NJ), both of which hadbeen pre-dosed with 0.15mL of 10% calciumchloride (American Regent, Inc.,Shirley, NY) to reverse the effects of theanticoagulant. The tubes were vigorouslyshaken <strong>for</strong> 60 seconds to adequately mixthe contents and then left to stand <strong>for</strong> 15minutes. After the rest period, a thick, softclot <strong>for</strong>mation was noted within each tube.Under sterile conditions, the clot wasmanually broken apart to produce a clearsupernatant, which was harvested (seeFigure 2a) and drawn into a sterile syringe(Figure 2b). Consistent with reports describedby Everts and other authors, theresulting supernatant following PPP activationhas been demonstrated to containautologous thrombin protein. 19,20PRP ImplantationThe patient was placed in a prone position.The left gluteal and proximal hamstringregion was prepared and drapedunder sterile conditions. With the tendonat rest and with concentric contraction,the areas of maximal tenderness and thesite of proximal insertion of the hamstringinto the ischial tuberosity were identifiedby palpation.Contact with and isolation of the targetregion was maintained through applicationof isometric contraction with manualsoft tissue depression by the second andthird digits of the examiner’s nondominanthand. Local anesthesia was achievedby placing 1% preservative-free Xylocaine(2-3mL) into the soft tissue of the proximalhamstring.While constant pressure was maintainedwith the nondominant hand, a 22-gauge, 1.5-inch needle was inserted towardthe ischial tuberosity. Once periostealcontact was made, the PRP wasplaced at the insertion site in a fanlike distributionwith a radius of several centimetersand also along the proximal 3-5 cmof the common tendon tissues utilizing 4-5 needle fenestrations of the tendon andmyotendinous junction. After negative aspirations,all 7mL of PRP was infiltrated.The PRP syringe was disconnected, the activatedPPP/AT-filled syringe was attached,and then 7mL of PPP/AT was infiltratedinto the tissue in a similar fashion. A steriledressing was applied to the region, andthe patient was discharged home.Post-Procedure ProtocolA two-week period of relative rest and activityrestriction was recommended.Weight-bearing and ambulation as toleratedwere allowed but any aggressivestretching or concentric or eccentricloading of the tendon was not. The patientwas advised to avoid NSAIDs or anyother anti-inflammatory medication <strong>for</strong>at least two weeks. At week three, the patientwas permitted to increase her activ-12 Practical PAIN MANAGEMENT, June 2010©2010 PPM Communications, Inc. Reprinted with permission.
<strong>Platelet</strong> <strong>Rich</strong> <strong>Plasma</strong> <strong>for</strong> <strong>Hamstring</strong> <strong>Tears</strong>ities slowly and progressively as pain allowedher to tolerate.Post-Procedure Clinical CourseThe patient reported no significant increasein pain after the intervention. Subjectiveimprovement in pain was noticeableat one week, and functionality beganto improve gradually about the same time.By week four, the patient was able to ambulatewithout pain or antalgia and to sitpain-free <strong>for</strong> reasonable periods. In addition,the quality of her sleep had also improveddue to resolution of nocturnalpain and she no longer required NSAIDsor other analgesics. She was able to resumelight exercise, including treadmill–walking,at week six and was able totolerate stationary bicycling at moderateexertion by week eight. When followed upby phone at 20 weeks, the patient reportedno return of discom<strong>for</strong>t during the interim.As of six months post-procedure,she was continuing to progressively increaseactivities and was preparing tobegin more aggressive concentric and eccentricstrengthening activities. Her goalwas ultimately to resume alpine and waterskiing.The patient underwent follow-up MRIjust under four months following the injury.The radiologist who had interpretedthe pre-procedure study reported the followingat follow-up:1. “Significant interval healingresponse within both the semimembranosistendon and the conjoinedtendon of biceps femoris and semitendinosus.Mild granulation tissueand contour irregularity persistswithin the proximal tendons. Thereis persistent partial, but not complete,avulsion of the conjoined tendonfrom the ischial tuberosity. Thesemimembranosis tendon origin isintact.2. Interval complete resolution of thehamstring muscle strains and posteriorthigh hematoma” (see Figure1b).DiscussionTraditional nonsurgical therapies <strong>for</strong>acute and chronic tendon injuries havelimited potential to alter the long-termcourse of the disease process. If acute orrepetitive tendon trauma results in fibrosisof the intratendinous tissue, chronicityusually develops and results in pain,functional limitation, and risk of reinjury.In a study of transected Achilles tendonin sheep, histologic and biomechanicalproperties of spontaneously-healed tendonsdid not match those of intact noninjuredtendons. At 12 months, rupture<strong>for</strong>ce in the transected group rated only56.7% of that in the normal group. 21 Peritendinousscar <strong>for</strong>mation has also beenobserved to produce sciatic nerve irritationand lower extremity sensorimotorsymptoms. 3,22 Disappointing clinical resultshave led to a growing interest in thepotential of anabolic and regenerativetherapies which, in theory, may be able toaugment the capability of tissues <strong>for</strong> repair.PRP represents a simple, low-cost, lowrisk,autologous regenerative biotherapeuticagent whose utility in treating softtissuepathology remains under investigation.Thus far, its safety profile has beenstrong. No serious adverse event relatedto PRP application has been reported inthe literature. The author’s experience,which includes more than 1,500 percutaneouscases, has been similar, with theemergence of a solid safety record, as wellas a trend toward therapeutic success.To date, research has suggested thesame trends of utility and favorable outcomes<strong>for</strong> the application of PRP in basicorthopedic conditions, such as lateral epicondylitis,achilles tendinopathy, patellartendinopathy, rotator cuff injury, muscleinjury, osteoarthritis, ligament injury, andintervertebral disc pathology. 15 Researchcontinues not only to validate the therapeuticeffect of PRP under the strictest ofscientific criteria but also to elucidate theintracellular effects of PDGFs on exposedtissue. Controversy exists regarding theneed <strong>for</strong> the addition of autologousthrombin to improve efficiency of plateletdegranulation versus reliance on nativecollagen or exposed tissue to achievemaximal platelet degranulation. Quantificationof autologous thrombin rangeswithin activated PPP using the methodsdescribed above would be helpful in determiningadvantage and necessity.Questions remain regarding optimaltherapeutic PRP concentration versuswhole blood and the effect of white bloodcell inclusion within the PRP injectate.Everts et al 23 have suggested a 4- to 5-foldincrease in platelet concentration versuswhole blood based on the anabolic effectsof PRP on soft tissues and bone healing.Whether higher PRP concentrations leadto incremental increases in anabolic tissuestimulation is currently unclear. Some authorshave suggested that higher concentrationscould contribute to deleteriouseffects, although this has not been substantiated.Accuracy of percutaneous delivery ofPRP appears to be critical in providing the“PRP represents a simple, low-cost, low-risk, autologousregenerative biotherapeutic agent whose utility in treating softtissuepathology remains under investigation. Thus far, its safetyprofile has been strong. No serious adverse event related to PRPapplication has been reported in the literature.”maximal possible therapeutic effect. Ultrasoundand fluoroscopic guidance havegained favor among practitioners whoprovide PRP interventions and, in the author’sexperience, these imaging techniqueshave merit. The site of the injuryreported above was easily identified withmanual palpation, but ultrasound needlelocalization could have been used to verifyimplantation of the PRP within viabletendon tissue and in peritendinous regionsat the site of avulsion.If PRP as a useful therapeutic optionstands the test of scientific validation,practitioners would have a clinical tool topromote faster and more complete healingof acutely injured tissue and to preventchronic tissue pathology by stimulatingregeneration of healthy tissue thatwould not otherwise <strong>for</strong>m spontaneously.The implications <strong>for</strong> traditional approachesto sports injury are obvious.Chronic injury and its attendant per<strong>for</strong>manceimpairment could be avoided, andinjury progression through continuedPractical PAIN MANAGEMENT, June 2010©2010 PPM Communications, Inc. Reprinted with permission.13
<strong>Platelet</strong> <strong>Rich</strong> <strong>Plasma</strong> <strong>for</strong> <strong>Hamstring</strong> <strong>Tears</strong>play would no longer be a risk.If its safety profile continues to be favorable,PRP may represent a safer alternativeto more traditional treatments,such as steroidal and nonsteroidal medications—whetherinjected or deliveredorally. In a study evaluating the histopathologicchanges in proximal hamstringtendinopathy, Lempainen et al 22concluded that with corticosteroid application,chronic tendinopathy was likely todevelop and usually only short-term reliefwas provided.PRP infiltration could also complementrehabilitation programs that are so oftenused to treat soft-tissue disorders. Postprocedureactivity-modification and rehabilitationprotocols have yet to be clearlydefined. Most clinical research has suggestedthe need <strong>for</strong> a period of tissuerest—due to the sustained bioactivity andrelease of growth factors—followed bygraded return to activity and training atdifferent intervals. 24The case presented here demonstratesthe potential therapeutic effects of PRP. Asingle infiltration of PRP promoted thehealing of a severe, near-complete–thickness,traumatic hamstring tendon disruptionthat otherwise would likely have facedsurgical debridement and reimplantation.As of six months post-procedure(after a single application), the outcomecontinues to be good in terms of bothsymptoms and function. MRI follow-uphas suggested that limited residual scartissue has <strong>for</strong>med. In contrast, to judgefrom histologic research data, the likelihoodof scarred, dysfunctional tissue followingspontaneous tissue repair of an injuryof this magnitude would have beenhigh.The exact mechanism of anabolic stimulationwith PRP or PDGFs has yet to beelucidated. It may, in fact, reflect a complexinteraction of cellular and noncellularevents. The stage of the healingprocess during which PRP is effective alsoremains unclear. Without question, furtherresearch is required not only to validatethe biotherapeutic effects and clinicalresults of PRP therapy but also to unveilthe physiologic mechanisms of action.SummaryPercutaneous, autologous platelet richplasma injection was selected as a conservativetreatment option <strong>for</strong> a proximalhamstring injury within the setting of aprivate orthopedic surgical practice. Subjectiveimprovement post-procedure wasmonitored through six months. Pre-injuryMRI was per<strong>for</strong>med at approximately twoweeks after the initial injury. At fourmonths post-treatment, a follow up MRIwith the same parameters was repeatedand reviewed by the same radiologist toevaluate healing and tissue integrity. Thepatient subjectively reported a decrease inpain at one week post-procedure. Reductionin pain and improvements in functionalitycontinued through weeks 4, 6, 8,20 and at final follow-up at six months.The improvements noted by the patientcoincided with significant tissue healingas reported by the evaluating radiologiston follow-up MRI.<strong>Platelet</strong> rich plasma represents a simple,low-cost, low-risk, autologous regenerativebiotherapy whose utility in treatingsoft-tissue pathology remains underinvestigation. This case report demonstratessustained subjective and functionalimprovements with near-completerepair on MRI with a single applicationof platelet-rich plasma in a severe tendoninjury. ■DisclosureThe authors certify that no party havinga direct interest in the results of the researchsupporting this article has or willconfer a benefit on the authors or on anyorganization with which the authors areassociated.David Karli, MD, is currently a physicianpartner at the Steadman Clinic in Vail, Colorado,where he has practiced since 2003. Hereceived his residency training at HarvardMedical School and medical degree throughthe University of Maryland. His research interestsare focused on clinical applications andbasic science mechanisms of autologous regenerativebiotechnologies, including platelet richplasma.Brent Robinson, BS, is a research associatein Regenerative Orthopaedics at the SteadmanClinic. His background in regenerative medicineand stem cell research began at the ColoradoState University Veterinary TeachingHospital.References1. Askling C, Saartok T, Thorstensson A. Type ofacute hamstring strain affects flexibility, strength, andtime to return to pre-injury level. Br J of Sports Med.2006. 40: 40-44.2. Connell D, Schneider-Kolsky M, Hoving J, et al.Longitudinal study comparing sonographic and MRIassessments of acute and healing hamstring injuries.Am Roentgen Ray Society. 2004. 183: 975-984.3. Sharma P and Maffulli N. Biology of tendon injury:healing, modeling, and remodeling. J MusculoskeletNeuronal Interact. 2006. 6: 181-190.4. Naito M and Ogata K. The blood supply of the tendonwith a paratenon: an experimental study usinghydrogen washout technique. Hand. 1983;15:9-14.5. Fyfe I, Stanish WD. The use of eccentric trainingand stretching in the treatment and prevention of tendoninjuries. Clin Sports Med. 1992. 11: 601-624.6. Benazzo F and Maffulli N. An operative approachto Achilles tendinopathy. Sports Med Arthroscopy Rev.2000. 8: 96-101.7. Jarvinen T, Jarvinen T, Kaariainen M, et al. Muscleinjuries: optimizing recovery. Best Practice & ResearchClinical Rheumatology. 2006. 21: 317-331.8. Menetrey J, Kasemkijwattana C, Day C, et al.Growth factors improve muscle healing in vivo. J ofBone and Joint Surg [Br]. 2000. 82: 131-137.9. Koob TJ and Summers AP. Tendon-bridging thegap. Comp Biochem Physiol: A Mol Inter Physiol.2002. 133: 905-909.10. Strickland JW. Flexor tendons: acute injuries. InGreen D, Hotchkiss R, Pedersen W. eds, Green’s operativehand surgery. Churchill Livingstone. New York.1999. pp 1851-1897.11. Crane D and Everts P. <strong>Platelet</strong> <strong>Rich</strong> <strong>Plasma</strong> (PRP)Matrix Graphs. Pract Pain Manag. 2008. 8(1): 12-26.12. Foster T, Puskas B, Mandelbaum B, et al. <strong>Platelet</strong>rich plasma from basic science to clinicalapplications. 2009. 37: 2259-2272.13. Hall M, Band P, Meislin R, et al. <strong>Platelet</strong>-rich plasma:current concepts and application in sports medicine.J Am Acad Orthop Surgeons. 2009. 17:602-608.14. Bielecki TM, Gazdzik TS, and Arendt J. Antibacterialeffect of autologous platelet gel enriched withgrowth factors and other active substances: an invitro study. J of Bone and Joint Surg. 2007. 89:417-420.15. Sampson S, Gerhardt M, Mandelbaum B. <strong>Platelet</strong>rich plasma injection grafts <strong>for</strong> musculoskeletal injuries:a review. Curr Rev Musculoseletal Med. 2008.1: 165-174.16. Chambers RL and McDermott JC. Molecularbasis of skeletal muscle regeneration. Can J ApplPhysiol. 1996. 21: 155-184.17. Grounds MD. Towards understanding skeletalmuscle regeneration. Path Res Pract. 1991. 187: 1-22.18. Molloy T, Wang Y, and Murrell G. The roles ofgrowth factors in tendon and ligament healing. SportsMed. 2003. 33: 381-394.19. DeRossi R, Coelho A, de Mello G, et al. Effects ofplatelet-rich plasma gel on skin healing on surgicalwound in horses. Acta Cir Bras. 2009. 24: 276-281.20. Giacco F, Perruolo G, D’Agostino E, et al. Thrombin-activatedplatelets induce proliferation of humanskin fibroblasts by stimulating autocrine production ofinsulin-like growth factor-1. FSEB J. 2006. 20: 2402-2404.21. Bruns J, Kampen J, Kahrs J, et al. Achilles tendonrupture: experimental results on spontaneous repairin a sheep-model. Knee Surg Sports TraumatolArthrosc. 2000. 8: 364-369.22. Lempainen L, Sarimo J, Mattila K, et al. Proximalhamstring tendinopathy: results of surgical managementand histopathologic findings. Am J Sports Med.2009. 37: 727-734.23. Everts P, Knape J, Weibrich, et al. <strong>Platelet</strong> richplasma and platelet gel: a review. J Extra CorporTechn. 2006. 38: 174-187.24. Van Den Dolder J, Mooren R, Vloon A, et al.<strong>Platelet</strong>-<strong>Rich</strong> <strong>Plasma</strong>: Quantification of Growth FactorLevels and the Effect on Growth and Differentiation ofRat Bone Marrow Cells. Tissue Eng Part A. 2010. 16:1021-1029.14 Practical PAIN MANAGEMENT, June 2010©2010 PPM Communications, Inc. Reprinted with permission.