Chapter 514 - Nursing Facility Services - DHHR - State of West ...
Chapter 514 - Nursing Facility Services - DHHR - State of West ...
Chapter 514 - Nursing Facility Services - DHHR - State of West ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
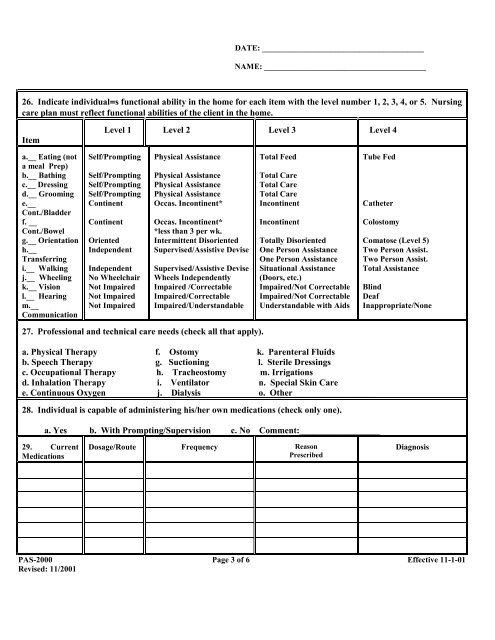
DATE: ________________________________________NAME: ________________________________________26. Indicate individual=s functional ability in the home for each item with the level number 1, 2, 3, 4, or 5. <strong>Nursing</strong>care plan must reflect functional abilities <strong>of</strong> the client in the home.ItemLevel 1 Level 2 Level 3 Level 4a.__ Eating (nota meal Prep)b.__ Bathingc.__ Dressingd.__ Groominge.__Cont./Bladderf. __Cont./Bowelg.__ Orientationh.__Transferringi.__ Walkingj.__ Wheelingk.__ Visionl.__ Hearingm.__CommunicationSelf/PromptingSelf/PromptingSelf/PromptingSelf/PromptingContinentContinentOrientedIndependentIndependentNo WheelchairNot ImpairedNot ImpairedNot ImpairedPhysical AssistancePhysical AssistancePhysical AssistancePhysical AssistanceOccas. Incontinent*Occas. Incontinent**less than 3 per wk.Intermittent DisorientedSupervised/Assistive DeviseSupervised/Assistive DeviseWheels IndependentlyImpaired /CorrectableImpaired/CorrectableImpaired/UnderstandableTotal FeedTotal CareTotal CareTotal CareIncontinentIncontinentTotally DisorientedOne Person AssistanceOne Person AssistanceSituational Assistance(Doors, etc.)Impaired/Not CorrectableImpaired/Not CorrectableUnderstandable with AidsTube FedCatheterColostomyComatose (Level 5)Two Person Assist.Two Person Assist.Total AssistanceBlindDeafInappropriate/None27. Pr<strong>of</strong>essional and technical care needs (check all that apply).a. Physical Therapy f. Ostomy k. Parenteral Fluidsb. Speech Therapy g. Suctioning l. Sterile Dressingsc. Occupational Therapy h. Tracheostomy m. Irrigationsd. Inhalation Therapy i. Ventilator n. Special Skin Caree. Continuous Oxygen j. Dialysis o. Other __________________28. Individual is capable <strong>of</strong> administering his/her own medications (check only one).a. Yes b. With Prompting/Supervision c. No Comment:__________________29. CurrentMedicationsDosage/Route Frequency ReasonPrescribedDiagnosisPAS-2000 Page 3 <strong>of</strong> 6 Effective 11-1-01Revised: 11/2001