ARS WP-011811-d16.indd - MAKO Surgical Corp.
ARS WP-011811-d16.indd - MAKO Surgical Corp.
ARS WP-011811-d16.indd - MAKO Surgical Corp.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Annual Summary of Clinical and Economic Research <strong>MAKO</strong> <strong>Surgical</strong> <strong>Corp</strong>. – 2010Figure 7. Pre-operative AP radiograph of patient with medial OA (left) and post-operativeAP (middle) and lateral (right) radiographs of same patient.Fifty patients (33 female, 17 male;average age 71 ± 10; average BMI26.8 ± 4.5) were enrolled in an IRBapproved study to collect basic clinicaloutcomes. All patients underwenta lateral onlay <strong>MAKO</strong>plasty ® from twosurgeons and were present for clinicalevaluations at pre-op, 6 week, 3month, and 6 month post-operativevisits. Knee Society scores significantlyimproved from 112.6 ± 32.6 preoperativelyto 162 ± 62 at 6 monthspost-operatively. WOMAC scores alsosignificantly improved from 19.2 ±7.0 pre-operatively to 2.3 ± 2.7 at 6months post-operatively. Range ofmotion was full restored to 125 ± 3degrees at 6 months post-operatively 10(Table 3, Fig. 8, 9).Figure 8. Progressive improvement in WOMAC scores with each followup for a series oflateral UKA patients.Womac Score2520151050PainFunctionPre-Op 6 week 3 month 6 monthtibial component for all patients wasan all-poly inlay design.At one, two, three and four year followup, all patients showed significantimprovements, compared to preoperativevalues, in range of motion(p
new bone and tissue sparing implantationtechnique using tactilerobotics. These patients came from foursurgeons at four different hospitals.The average follow-up was six months.Pre- and post-operative radiographswere taken. ROM, KSS and WOMACscores were recorded. The patientshad an average age of 67 yrs (range:45-95), BMI of 29 ± 4kg/m 2 . 47% ofthe patients were male. At only sixweeks follow-up, patients recoveredtheir pre-operative ROM (p=0.37).Knee Society Knee scores (knee andfunction) and WOMAC scores (pain,function and total) significantly improvedfrom pre-operative values atevery follow-up of 6 weeks, 6 monthsand 1 year (p
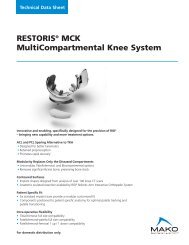
Annual Summary of Clinical and Economic Research <strong>MAKO</strong> <strong>Surgical</strong> <strong>Corp</strong>. – 2010Figure 12. (Below) Contact areas on the tibia and femur in the same specimen during asquatting activity intact, with ACL/PCL sparing bicompartmental arthroplasty, with PCLsparing TKA and with ACL/PCL sacrificing posterior stabilized TKA. (Below) Patellofemoralcontact during the transition from trochlear component to condylar component.These findings indicated that metalbackedonlay components may be abetter option when considering distributionof load despite requiringadditional bone resection 15 (Fig. 13, 14).Bicompartmental KneeArthroplastyAlthough early results with a mono-lithic device are encouraging, use ofa monolithic bicompartmental arthroplastyfor trochlear-medial femoral condylarresurfacing faces some challenges.With this philosophical approachto bicompartmental resurfacing, thevarus–valgus alignment of the componentis determined by the appositionof the lateral transitional edge of thetrochlear component with the lateralfemoral condyle. Given the variabilityin coronal alignment and morphologyof the distal femur, there will be concomitantvariability in how the implantcan be aligned to ensure that the lateraledge of the trochlear prosthesis isflush with the lateral femoral condyle.Whether compromise in the alignmentor position of either of these areas hasFigure 13. (Left) Von Mises stresses for the inlay and onlay components at the interfaceof the bone immediately below the components. Posterior is to the left. (Right) Thestrain values on the surface at the interface. The gray color indicates elevated strainvalues at the inner edge of the metal baseplate.Implant Design/ProductDevelopmentUnicompartmental KneeArthroplastyThere are two main designs used forunicompartmental tibial components.The first design, an all plastic componentcalled an inlay, preserves thecortical bone on the outer edge ofthe tibia. The second design, calledan onlay, removes the tibial edge andincludes a metal backed plate whichrests on the resected tibia. The purposeof this study was to use finiteelement analysis to investigate the hypothesisthat while inlay componentsrequire less bone removal, the stressesand strains at the surface of the bonewill be greater when compared to onlaycomponents.• Results indicated that plastic inlaysgenerated six times more peak stressat the tibial surface when comparedto metal-backed onlays.• Moreover, models using inlay componentsproduced strain valuesgreater than onlay components by afactor of nearly 13.5.Figure 14. (Left) Values of the maximum stress at the interface for 4 individually meshedtibiae. (Right) Values for the maximum strain at the interface.Maximum Stress(more text)2520151050Stress PlotMaximum Stress(more text)Stress PlotPlastic Inlay Metal-Backed Inlay Plastic Inlay Metal-Backed Inlay2501 2 3 4 1 2 3 4Tibia NumberTibia Number72015105
Figure 15. The reconstructed femurs were brought into a standardized alignment basedon the identification of 10 control points defining the articular surfaces and epicondyles.From this standard alignment, sagittal arcs were fit to the medial condyle and the patellararticular sulcus, and the arc centers and radii were determined (black circles on rightfigure).deleterious effects on patellar trackingand midterm performance of the implantis not yet known.A recent study by Banks 16 and colleaguesexamined the morphologyof the reconstructed CT scans of 117knees and found that the anteroposterior(AP) and proximodistal (PD) relationshipsbetween the condylar andtrochlear arc centers were highly variable.There was no significant correlationbetween the AP femur size andthe AP distance from condylar to PFarc centers or between the mediolateral(ML) femur size and the AP distancefrom condylar to PF arc centers.The standard errors for these regressionswere at least 4.5mm. There werestatistically significant relationshipsbetween the AP and ML femur sizeand the PD distance from condylar toPF arc centers; however the standarderrors were also at least 4mm. Thesedata show that the geometric relationshipbetween the femoral condylesand patellar trochlea is highly variable.A multicompartment resurfacing approachmight better restore femoralanatomy compared to a monoblockapproach, with the potential to provideenhanced arthroplasty function whilemaintaining the functional integrity ofthe natural lateral compartment.<strong>Surgical</strong> Technique/Robotic Arm Use/IndicationsAre Partial Knee ReplacementCandidates Receiving a TKA?Radiographic studies have shown thatmost osteoarthritis of the knee affectsonly one or two compartments, rarelyall three 17-18 . A recent study by Arno 19et al looked at the resected bones of97 varus TKA patients visually to assessthe cartilage integrity using theWeidow grading scale 20 . The operativereports were also reviewed for possiblecontraindications to early interventionprocedures. It was found that 61% ofthe cases had healthy lateral compartmentcartilage. When strictly applyingKozinn and Scott indications forUKA 21 , it was found that 21% of thecases could have been treated with aUKA, with of course this percentagepotentially higher if the patients weretreated earlier.In another study, we retrospectively reviewedpre- and post-operative notesfrom 406 consecutive TKA patientsfrom a single surgeon 22 . Intra-operativedata included the integrity of thethree compartments and ACL. Firstly,the ACL was intact in 66% of thesecases. Based on these data alone, 16%of these TKA patients were indicatedfor a unicompartmental arthroplasty,12% medial UKA, 3% lateral UKAand 1% PFA. In addition, 31% wereindicated for bicompartmental arthroplastywith 4% bicondylar (medialand lateral UKA), 6% lateral UKA andPFA and 21% medial UKA and PFA.While these data don’t yet account forfixed versus flexible deformities,excessive osteophytes or other contraindications,it seems clear that thediseased knee often treated with aTKA does not actually involve all threecompartments.8Cartilage Health and AssessmentThe question remains whether the lateralcartilage in these cases had adequatemechanical properties to sustainphysiologic loading should a medialUKR procedure have been performed.One measure of this is the indentationstiffness of the cartilage. Others haveobtained this information through theuse of a device such as the Artscan200 and the Actaeon Probe. Bothwere designed for short-duration indentationtesting of the cartilage inorder to assess cartilage viability. Theauthors designed and constructed anindentor, with similar objectives to theabove devices, optimized for use in alab setting, to measure the resistiveforce as an indentor was pressed intothe cartilage surface at a prescribeddistance. By analyzing the lateralcartilage of resection samples fromTKR cases the authors sought to determineif cases found to be visuallyand histologically healthy had resistiveforce values which were also indicativeof healthy cartilage and thereforecould have sustained loading had aUKR been performed. 23 In this study,twenty two bone resection samplespresenting with predominantly medialOA were obtained within 24 hours ofsurgery were examined visually, histologicallyand mechanically. There wasstrong agreement between the visualand indentation results. This is significantin that it suggests that cases thatappear to have normal cartilage wouldalso have the capability of sustainingload.Tibial Slope Leveling in Medial UKAfor ACL DeficiencyPatients with anterior cruciate ligament(ACL) deficiency may have increasedfailure rates with UKA as a resultof abnormal contact stresses andaltered knee kinematics. Variations inthe slope of the tibial component inUKA may alter tibiofemoral translation,and affect outcomes. A recentcadaveric study evaluated tibiofemoraltranslation during the Lachman andpivot shift tests after changing theslope of the unicondylar tibial component(Fig. 16).
Annual Summary of Clinical and Economic Research <strong>MAKO</strong> <strong>Surgical</strong> <strong>Corp</strong>. – 2010Figure 16. Reproducible and quantifiabletechnique for applying the pivot shift test.Figure 17. Anteroposterior translation withACL deficiency measured with a UKA placein neutral and with 4° more and 4° lessposterior slope.AP Translation (mm)15105Medial Compartment Translation During Lachman TestOver- and under-correction of the mechanicalalignment is associated withearly failure of the femoral and tibialcomponents in UKA. A recent studyhypothesized that robotic arm technologywould provide improved controlover the amount of mechanical alignmentcorrection achieved dependingon the pre-operative deformity. 72 patientsprospectively underwent roboticarm medial UKA by a single surgeonbetween 2007 and 2009. Radiographicmechanical alignment measurementswere performed in all patientswith pre-operative and 3-month postoperativefull-leg standing radiographs(n=39). The mean changes were in prevspost-operative mechanical alignmentwere calculated and the amountof correction achieved depending onthe severity of the pre-operative deformity(A=9° varus)was analyzed with ANOVA and linearregression (α=0.05). Mean correctionin the combined groups was 3.12°(SD=2.76) from 7.09° varus pre-operatively(SD = 4.33°) to 3.97° varuspost-operatively (SD=3.51º) (p
properties of articular cartilage, aswell as local thickness. Medical andengineering software is now availablewhereby three dimensional modelscan be made from MRI scans, togetherwith analyses of thickness and volume.These techniques can have a usefulapplication in studying the progressof osteoarthritis (OA) and in planningand designing Early Intervention (EI)treatments. While many studies havebeen carried out on the end-stage ofOA, there have been few reports ofthe progress of the cartilage loss fromthe earliest stages. A recent study byWalker et al. 26 determined the locationsand magnitudes of the cartilageloss of the knee joint, and the progressionof OA in order to understand themechanical factors involved. Further,from this data, types of EI treatments,such as small implant components,which could be employed to arrest theprogress of the OA process were determined.The MRI scans (3T Siemens,Malvern, PA) from 18 patients withsymptomatic early OA were analyzed.The femoral and tibial cartilage modelswere subdivided into 6 regions. Eachregion then underwent thickness analysisdisplayed with a colorcoded thicknessmap in RapidForm. From the 18cases, 4 representative examples withincreasing K-L grades were selected toshow the progression of the cartilageloss (Fig. 19).Results showed that most early OA inthe knee presented in the distal regionof the medial femoral articular cartilage,leaving the posterior condyles intact.The medial tibia also matched thewear shown on the femoral condylebut did not present a consistent regionof wear, which may be explainedby the variations in ligament laxity andthe condition of the meniscus. Thesepatterns of cartilage loss are consistentwith the impact forces generatedat the heel strike and the toe off phasesof walking. The information fromthis study is crucial for the design offuture EI implants, as it points to theopportunity of preserving maximal viablecartilage while resurfacing onlythe damaged areas. Such early interventiontechniques could significantlydelay the progression of knee osteoarthritisand thus improve the quality oflife of many patients.Figure 19. Cartilage degeneration over the increasing K-L grades from 4 representativeknee MRI scans at 00 flexion.Cartilage Damage and ClinicalSymptomsThe most commonly used radiographicalgrading method is the KellgrenLawrence (KL) classification 27 . Thismethod defines severity of osteoarthritis(OA) primarily by the amount ofjoint space narrowing, the presence ofosteophytes and the condition of theunderlying bone. While KL grade assessesthe condition of the joint, selfassessmentquestionnaires, such asWOMAC and SF-36, are often used todetermine a patient’s level of discomfort.There is currently little researchwhich compares the condition of thecartilage itself to the KL grade andWOMAC scores. (Fig. 19) A study usedmagnetic resonance imaging of patientswith various stages of osteoarthritisto determine if thickness andvolume mapping of the cartilage wouldcorrelate with KL grade and WOMACscores. This retrospective study included50 cases with primary medial OArandomly selected from the R01 NIHstudy AR052873. As part of enrollmentin this study, patients had undergoneT1 weighted fat suppressed 3Dgradient echo 3T MRI scans (Siemens,Malvern, PA). There were 18 males and32 females, with a mean age of 60.8 ±10.6 and mean body mass index (BMI)of 26.8 ± 3.6. The study also included12 normal cases selected from a departmentfunded study at our center.As part of that study volunteers hadundergone T1 weighted non-fat suppressed3D gradient echo 7T MRIscans (Siemens, Malvern, PA). All normalcases were male with a mean ageof 29.1 ± 3.2 and a mean BMI of 24.9± 2.9. All MRI scans were reviewed byan experienced musculoskeletal radiologistand classified using the (KL)scale. The results above confirm that10KL grade is a valid metric for describingthe state of cartilage especially forthe volumes of the medial distal femur,medial posterior femur, and medialtibia when compared to their lateralcounterparts. However, comparing thevolume ratios to the WOMAC scoresindicated that self-assessment maynot indicate the status of the cartilageand extent of osteoarthritis. Therefore,although they are important to learnmore about the patients’ perceptionof pain, etc., self-assessment shouldcontinue to be considered secondaryto KL grade when determining the extentof a patient’s osteoarthritis 28 .Patterns of Cartilage Loss andMeniscal FunctionThe medial meniscus is known to transmitat least 50% of the load across thejoint surfaces. A meniscus which isdamaged or where the material propertieshave degenerated 29 would causean increase of cartilage stresses in thecentral regions of the condyles, leadingto cartilage wear. This has beensupported by the finding of meniscalsubluxation in cases of early osteoarthritis30 . From MRIs of symptomatic osteoarthritis(OA) patients of differentKellgren Lawrence (KL) grades, a recentstudy analyzed the cartilage thicknessmaps to determine whether cartilageloss was consistent with a dysfunctionalmeniscus. This study included 50 caseswith primary medial OA.In normal knees, the thickest cartilagewas in a central band of the distalfemoral condyle, and the central areaof the tibia. Cartilage wear progressedpredominantly in these areas. This isconsistent with a medial meniscuswhich is no longer carrying load, suchthat all the joint load becomes con-
Annual Summary of Clinical and Economic Research <strong>MAKO</strong> <strong>Surgical</strong> <strong>Corp</strong>. – 2010centrated centrally. As the severity increased,wear moved outwards on thetibia, indicative of varus deformity andmedial femoral subluxation, and anextruded meniscus. Further researchon the mechanisms of meniscal dysfunctionare indicated 31 (Fig. 20).Figure 20. Six cases representative of the change in thickness observed as OA severityincreased.Health Care EconomicsOperative Time and Length ofHospital StayA review of 169 patients who receivedrobotic arm assisted UKA had an averagehospital length of stay of 1.3days 32 . In another study, 56 robotic armUKA’s were compared to 57 manuallyimplanted mobile bearing UKA’s. Theaverage length of stay for the roboticarm group was 1.4 days compared to3.2 days for the manual mobile bearinggroup (p
Annual Summary of Clinical and Economic Research at <strong>MAKO</strong> <strong>Surgical</strong> <strong>Corp</strong>. – 2010References:1. Lonner JH, John TK and Conditt MA. Robotic ArmAssisted UKA Improves Tibial Component Alignment.Clin Orthop Relat Res, 2009.2. Coon T, Driscoll MD, Horowitz S, Conditt M. RoboticallyAssisted UKA is More Accurate than ManuallyInstrumented UKA. Presented at American Academyof Orthopedic Surgeons. New Orleans, LA. 2010.3. Pearle AD, O’Loughlin PF, and Kendoff DO: RobotAssisted Unicompartmental Knee Arthroplasty. JArthroplasty, 2008.4. Argenson J-NA, Parratte S, Bertani A, AubaniacJ-M, Lombardi AV, Berend KR, Adams JB, LonnerJH, Mahoney OM, Kinsey TL, John TK and Conditt MA:The New Arthritic Patient and Arthroplasty TreatmentOptions. J Bone Joint Surg Am, 91-A: 43-48 2009.5. Dunbar NJ, Pearle AD, Kenoff D, Conditt M, Banks S. IsUKA More Accurate With Robotic Assistance?Presented at the Orthopedic Research Society. NewOrleans, LA. 2010.6. Roche M, Dunbar NJ, Park B, Bank S, HorowitzS, Conditt M. Accuracy of UKA Component Placementwith Dynamically Referenced Tactile Robotics. Presentedat the American Academy of Orthopedic Surgeons.San Diego, CA. 2011.7. Callanan M, Jarrett B, Bragdon C, Zurakowski D,Rubash H, Freilberg A, Malchau H. Risk Factors for CupMalpositioning: Quality Improvement Through a JointRegistry at a Tertiary Hospital. Clin Orthop Relat Res.August 2010.8. Padgett DE, Dorr LD, Pagnano MW, Trousdale RT,Jamieson ML, Thompson MT, Conditt MA. Accuracy ofRobotically Assisted Acetabular Cup Implantation.78th Annual Meeting of the American Academy for OrthopedicSurgeons. San Diego, CA. 2011.9. Roche MW, Horowitz S, Conditt MA. Four YearOutcomes of Robotically Guided UKA. 23rd AnnualCongress of ISTA, Dubai, UAE, 2010.10. Velyvis J, Roche MW, Horowitz S, Conditt MA.Robotic Arm Guidance to Improve Lateral UKA Accuracy.78th Annual Meeting of the American Academyfor Orthopedic Surgeons. San Diego, CA. 2011.11. Lonner JH, John TK and Conditt MA. Early clinicaloutcomes of modular bicompartmental arthroplasty.22nd Annual Congress of ISTA, Big Island, Hawaii,2009.12. Velyvis. J, Coon TM, Kreuzer S, Roche M, HorowitzS, Conditt MA. Early Outcomes of Robotically GuidedBicompartmental Arthroplasty. 23rd Annual Congressof ISTA, Dubai, UAE, 2010.13. Watanabe T, Banks SA, Kreuzer S, Leffers KJ, MunetaT. Deep Flexion Kinematics with Robotic ModularKnee Arthroplasty. Submitted to the Japanese OrthopedicAssociation. Pacifico Yokohama, Japan, 2011.14. Yildirim G, Walker PS, Conditt MA, Horowitz S,Madrid I. Cadaveric Evaluation of the <strong>MAKO</strong> MultiCompartmental Knee Kinematics. Annual Meeting ofthe Orthopaedic Research Society. Long Beach, California,2011.15. Walker PS, Parakh DS, Chaudhary ME, Wei CS.Comparison of Interface Stresses and Strains for Onlayand Inlay Unicompartmental Tibial Components. AnnualMeeting of the Orthopaedic Research Society.Long Beach, California, 2011.16. Banks SA, Abbasi A, van Vorhis R, Chan R, Otto Jand Conditt MA. Morphology of the Distal Femur forBicompartmental Arthroplasty. 77th Annual Meetingof the American Association of Orthopedic Surgeons,New Orleans, LA, 2010.17. Duncan RC, Hay EM, Saklatvala J and Croft PR.Prevalence of radiographic osteoarthritis–it all dependson your point of view. Rheumatology (Oxford),45(6): 757-60, 2006.18. Ledingham J, Regan M, Jones A and Doherty M.Radiographic patterns and associations of osteoarthritisof the knee in patients referred to hospital. AnnRheum Dis,52(7): 520-6, 1993.19. Arno S, Maffei D, Walker PS, Schwarzkopf R, DesaiP and Steiner G. Could unicompartmental knee replacementsbe used more frequently? J Arthroplasty.In Press.20. Weidow J, Pak J, and Karrholm J. Different patternsof cartilage wear in medial and lateral gonarthrosis.Acta Orthop Scand, 73(3): 326-9, 2002.21. Kozinn SC and Scott R. Unicondylar knee arthroplasty.J Bone Joint Surg Am, 71(1): 145-50, 198922. Kreuzer S, Leffers K, Jamieson ML, Conditt MA.How Many TKA Patients Could be Treated With EarlyIntervention Procedures? Submitted to the 78th AnnualMeeting of the American Academy for OrthopedicSurgeons. San Diego, CA. 2011.23. Kuo L, John D, Arno S, Walker PS. Comparison ofvisual, histological, and indentation analysis of cartilagein the osteoarthritic knee. Annual Meeting of the OrthopaedicResearch Society. Long Beach, California, 2011.24. Suero E, Citak M, Conditt M, Pearle A. Effect ofMedial UKA Tibial Component Slope on ACL DeficientKnee Stability. 78th Annual Meeting of the AmericanAcademy for Orthopedic Surgeons. San Diego, CA.2011.25. Suero EM, Citak M, Cross MB, Conditt MA, PearleAP. Mechanical Malalignment Correction in RoboticUnicompartmental Knee Arthroplasty. Submitted to JBone Joint Surg Am, 2011.26. Yildirim G, Arno S, Khmelnitska E, Regatte R,Walker PS. MRI Analysis of the Progression of ArticularCartilage Loss in Knee Osteoarthritis Patients. AnnualMeeting of the Orthopaedic Research Society. New Orleans,Louisiana, 2010.27. Schiphof D, Boers M, Bierma-Zeinstra SMA. Differencesin descriptions of Kellgren and Lawrence gradesof knee osteoarthritis. Ann Rheum Dis 67:1034-1036.2008.28. Arno S, Walker PS, Samuels J, Krasnokutsky S, LiangS, Yildirim G, Regatte R, Recht M, Abramson S.Quantitative MRI of articular cartilage of the knee:correlation with severity of medial OA and self-assessment.Annual Meeting of the Orthopaedic ResearchSociety. Long Beach, California, 2011.29. Hunter DJ, Zhang YQ, Niu JB, Tu X, Amin S, ClancyM, Guermazi A, Grigorian M, Gale D, Felson DT. Theassociation of meniscal pathologic changes with cartilageloss in symptomatic knee osteoarthritis. ArthritisRheum. Mar;54(3):795-801. 2006.30. Gale DR, Chaisson CE, Totterman SM, Schwartz RK,Gale ME, Felson D. Meniscal subluxation: associationwith osteoarthritis and joint space narrowing. OsteoarthritisCartilage. Nov;7(6):526-32. 1999.31. Walker PS, Arno S, Krasnokutsky S, Samuels J,Abramson SB, Regatte R, Recht M, Liang S, YildirimG. Patterns of cartilage loss in knee OA and relation tomeniscal function. J Orthop Res, Under Review.32. Data on file33. Jinnah R, Poehling G. A Comparative study of RoboticAssisted and conventional manual implantationof unicompartmental knee replacements. Presented atthe Southern Orthopedic Association Annual Meetingin Kiawah Island, South Carolina. 2009.34. Agency for Healthcare Research and Quality. (2010)H-CUP web-based database. Retrieved December 23,2010, from http://hcupnet.ahrq.gov/HCUPnet.jsp35. Candrilli S, Mauskopf J (2006) RTI Health Solutions,How Much Does a Hospital Day Cost? Retrieved December23, 2010, from http://www.rtihs.org/request/index.cfm?fuseaction=display&PID=646536. Data on file37. Bozic KJ, Rubash HE, Sculco TP, Berry DJ, An Analysisof Medicare Payment Policy for Total Joint Arthroplasty.J Arthroplasty 23(6 Suppl 1): 133-138. 2008.38. Cleveland Clinic. (2010). Patient Price InformationSheet. Retrieved December 23, 2010, from http://my.clevelandclinic.org/Documents/Patients/HB197_MAIN_2010.pdf39. Musculoskeletal Clinical Regulatory Advisers, LLC.(2011). Physician and Hospital Coding Guide, Hip andKnee Procedures. Fort Lauderdale, FL: <strong>MAKO</strong> <strong>Surgical</strong><strong>Corp</strong>.40. Bozic KJ, Kurtz SM, Lau E, Ong K, Vail TP, Berry DJ.The Epidemiology of Revision Total Hip Arthroplasty inthe United States. J Bone Joint Surg Am 91(1): 128-133. 2009.41. Ong KL, Mowat FS, Chan N, Lau E, Halpern MT,Kurtz SM. Economic Burden of Revision Hip and KneeArthroplasty in Medicare Enrollees. Clin Orthop RelatRes. 446:22-28. 2006.42. Upadhyay A, York S, Macaulay W, McGrory B, RobbennoltJ, Bal BS. Medical Malpractice in Hip and KneeArthroplasty. J Arthroplasty 22(6 Suppl 2): 2-7. 2007.43. Cobb, J., J. Henckel, et al. (2006). “Hands-on roboticunicompartmental knee replacement: a prospective,randomised controlled study of the acrobot system.”J Bone Joint Surg Br 88(2): 188-197.The third party trademarks used herein are property of their respective owners.© <strong>MAKO</strong> <strong>Surgical</strong> <strong>Corp</strong>. 205125 r00 02/11 www.makosurgical.com