Private clinic and A&E: the interface
Private clinic and A&E: the interface
Private clinic and A&E: the interface

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Private</strong> <strong>clinic</strong> <strong>and</strong> A&E: <strong>the</strong> <strong>interface</strong>Dr TSUI Sik Hon 徐 鍚 漢 ,FRCP Edin, FRCS Edin, FHKCEMConsultant & Chief of ServiceAccident & Emergency DepartmentQueen Mary HospitalHong Kong1
Contents• Discussion on emergency cases that mayturn up in private <strong>clinic</strong>s• What will happen to such patients after<strong>the</strong>y are referred to A&E?• How private doctors help to improvepatients’ outcome by providing <strong>the</strong>appropriate initial management?• Follow up of cases that are referred backto your <strong>clinic</strong>3
Medical conditionsHypertension• A 45 year old lady presented with URTI<strong>and</strong> high BP was found: 200/120• Patient is referred to A&E• What will be her journey like?4
A&E Triage System• Patient will be triaged by <strong>the</strong> nurses afterregistration• To established priority of care• Base on patient’s general condition, vitalsigns, brief history <strong>and</strong> referral notes (ifavailable)• According to disease urgency <strong>and</strong> severity• Nurse initiated investigations <strong>and</strong>treatments5
Triage CategoriesTriage Category Patient condition Target response time1. Critical危 殆Suffering from a life threateningconditionWith unstable vital signs requiringresuscitationImmediate2. Emergency危 急3. Urgent緊 急4. Semi-urgent次 緊 急5. Non-urgent非 緊 急Suffering from a potentially lifethreatening conditionBorderline vital signs with risk ofrapid deteriorationSuffer from a major condition withpotential risk of deteriorationSuffer from acute but stableconditionSuffer from minor <strong>and</strong> stablecondition
Hypertension• BP in A&E: 220/120, P: 92/min• Patient had mild dizziness• Triaged as Cat 3• The key to manage this case:– Establish if this case is hypertensiveemergency or hypertensive urgency7
• Hypertensive emergency:– Severe elevation in BP with complicated byevidence of progressive target org<strong>and</strong>ysfunction• Hypertensive urgency:– Severe elevation in BP without target org<strong>and</strong>ysfunction8
Target organ dysfunction• Coronary ischaemia• Acute pulmonary oedema• Acute renal failure• Aortic dissection•Stroke• Hypertensive encephthalopathy9
Evaluation• CNS: headache, vomiting, impairedconscious level, seizure, neurologicaldeficit, coma• CVS: chest pain, SOB• Renal: haematuria, proteinuria, decreasedurine output• Retina: haemorrhage, exudates,papilloedema10
Investigations•ECG•CXR• Urinalysis•RFT• +/- CT brain11
Management• HT Emergency– Manage in CCU/ICU/Stroke Unit– Rapid <strong>and</strong> smooth BP control by parental<strong>the</strong>rapy12
Management• HT Urgency (much more common)– Rest <strong>and</strong> repeated BP measurement– Not very urgent actually– Start oral anti-HT as indicated– Monitor response to resting or treatment inObservation Ward or EM Ward– Nifedipine SL NOT recommended because ofrapid drop in BP followed by rebound13
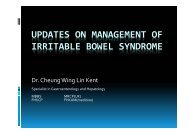
Case 2• A 55 years old gentleman presented toyou with retrosternal dull aching chest painfor 1 hour• Chronic smoker, good past health• You perform ECG in your <strong>clinic</strong>……14
Can you identify anyabnormality?15
AMIActions for you:• Call ambulance (27353355) <strong>and</strong> give clearinformation to ambulance controller• Advise against self-transport to hospital• Drugs you can consider to give whilewaiting:– Aspirin ~300mg (check allergy <strong>and</strong> contraindications– Morphine IV, maxalon IV– TNG (check contra-indications)16
What happens next?• Ambulance equipped with defibrillator willsoon arrive• Rapid transfer to hospital• Alert A&E en-route• Triage Cat 1, immediate attention•Aim for early PPCI or thrombolysis;depending on availability of expertise <strong>and</strong>indications17
A&E Management of STEMI• Patient evaluation: focused Hx <strong>and</strong> PE• Define symptom onset time• Establish diagnosis; rule out AMI mimics• Ix: ECG 12 leads, right side, post leads• Ix: CBP, LRFT RG, AP/APTT, type &screen• Set IV access•Tx: MONA• Communication: activate AMI pathway 18
ECG ED R side leads
ECG ED posterior leads
Reperfusion <strong>the</strong>rapyChance of survival• Better with early reperfusion <strong>the</strong>rapy (timeis muscle)• Better with PPCI than thrombolytics• International bench mark:– DNT ≤ 30min–DBT ≤ 90min• Consider PPCI if DBT-DNT < 60min• Also depends on availability of expertise21
No Left SystemTotal Blocked LADMechanical VentilationShock, IABPBalloon time : 13:35 3/11/07Door-to-Balloon Time : 87minNormal FlowRe-establishedPt in ICU ARF 6wFull recovered22
Patient with chestpain/discomfort• A common presentation to A&E• Long list of differential diagnosis• History is <strong>the</strong> KING, ECG is a MUST• First is to exclude life threatening causes:– Acute coronary syndrome (ACS)– Aortic dissection– Pulmonary embolism– Tension pneumothorax23
Chest pain protocol• After brief history, PE, vital signs; identify<strong>the</strong> group of patients with:– Atypical chest pain– Stable angina with non-specific or normalECG• Consider risk factors for ACS• Low to moderate risk: admit EMW orObservation ward for monitoring, serialECG <strong>and</strong> Troponin24
Rationale for chest pain protocol• A normal ECG does not exclude ACS• Elderly patients <strong>and</strong> diabetics are more prone to atypicalor silent presentation of ACS• Epigastric or upper abdominal pain may be apresentation of inferior myocardial ischaemia• Response to GI cocktail does not rule out ACS• Reproducible chest wall pain does not rule our ACS• Patient with chest pain <strong>and</strong> an abnormal ECG should notbe sent home before fur<strong>the</strong>r assessment25
Neurological Problem• A 71 year old gentleman with history ofDM presented to your <strong>clinic</strong> in <strong>the</strong> morningwith facial asymmetry <strong>and</strong> slurring ofspeech• Is this a case of stroke?26
Acute Stroke• Stroke is a syndrome characterized by asudden neurological deficit caused byintracranial haemorrhage or ischaemia• In <strong>the</strong> era of thrombolytic <strong>the</strong>rapy, timelydiagnosis <strong>and</strong> appropriate <strong>the</strong>rapyrequires close collaboration of variousparties27
Chain of optimal recovery of acute stroke patientsEarlyrecognitionEarly EMSactivationFamily doctor has a role hereEarly EDevaluation<strong>and</strong>interventionEarly accessto neurologyexpertise
Chain of optimal recovery of acute stroke patientsEarly ED evaluation <strong>and</strong> interventionInter-department collaboration to shorten:Door to Triage timeEarlyoptimalsupportivecareDoor to Doctor timeDoor to CT timeDoor to Stroke Unit timert-PA30
Respiratory case• A 25-year old man with history of asthmawho appears very dypsnoeic comes toyour <strong>clinic</strong>• You detect a lot of wheeze on PE• You decide to refer him to A&E• What treatment will you give in your <strong>clinic</strong>?32
Unfavorable historyBritish ThoracicSociety Guidelines201233
Severity Assessment34
Discharge arrangement36
Blood sugar• 73 year old man, known DM on Diamicron80mg OM• Presented to you with mild dizziness <strong>and</strong>dry mouth• RG by bedside glucometer: 22 mmol/L• Would you like to refer to A&E or managethis patient yourself?37
A&E Approach• Hyperglycaemia with minimal or nosymptom• Rule out life-threatening complications:– DKA: <strong>clinic</strong>al, urine/blood ketones, ABG– Hyperosmolar hyperglycaemic non-ketoticsyndrome: <strong>clinic</strong>al <strong>and</strong> blood test– Underlying diseases: ACS, infection…38
Hyperglycaemia• Manage in EMW/Observation Unit forselected cases– Check diet compliance– Check drug compliance– Await investigation results– Input from DM nurse, Dietitian etc if serviceavailable– Dosage adjustment <strong>and</strong> FU39
Allergy• A 23 year old lady with low back painreceived a shot of diclofenac injection inyour <strong>clinic</strong>• She has no history of drug allergy• She comes back to you 15 min later withgeneralised urticarial rash, peri-oralswelling, SOB <strong>and</strong> dizziness40
Are you worried?• PE: BP 80/30, Pulse 120/minchest: wheeze noted• Yes, this is a severe presentation of drugallergy: acute anaphylaxis• Need to call for help41
Urgent Treatments to begiven in A&E• IV fluid replacement• Adrenaline is <strong>the</strong> main stay of treatment;IV is needed for such presentation,o<strong>the</strong>rwise SC for milder cases• Anti-histamine• Steroid• Salbutamol• Expected response will be fast42
The worst scenario for you….• While you are busy seeing patient in your<strong>clinic</strong>, your assistant called you for help: apatient collapses suddenly in your waitingarea• You find an old gentleman, unconsciouswith no spontaneous respiration <strong>and</strong> nopulse• What should you do?43
Don’t forget to call for help• Update on American Heart Associationguidelines 2010 on CPR– Emphasize on chest compression (C-A-Binstead of A-B-C)– High quality: at least 5cm depth, at least100/min– Allow chest compression alone CPR foruntrained byst<strong>and</strong>er– Chest compression alone is much better thannothing44
For trained personnel• Delay of chest compression is to beavoided• Look, listen <strong>and</strong> feel for breathing• Briefly check for no response <strong>and</strong> nobreathing• Activate EMS• Spend no more than 10s to check pulse• Chest compression <strong>and</strong> rescue breath– 30:2 45
• Get a defibrillator if available• Some malls in HK have installedAutomated External Defibrillator (AED)• Easy to operate46
Use of Automated ExternalDefibrillatorsPads, <strong>the</strong>nPlug in CableAutomatic AnalysisNeed to PRESS to shock if advised to Do So.47
Resuscitation drugs <strong>and</strong> equipmentyou may wish to stock• For discussion– IV drugs: adrenaline, piriton, hydrocortisone– ?ATP, atropine– Aspirin, ?morphine– Dextrose, Salbutamol (Neb/Puff/IV)– IV Antibiotics, your choice?48
Orthopaedic Cases• A young man sprained his ankle whileplaying football• He walks with limping gait, withtenderness <strong>and</strong> swelling around ankle• He does not want to have XR or bereferred to A&E49
Ottawa Ankle Rule50
Ano<strong>the</strong>r Orthopaedic Case• F/56, known DM• Presents to you with left leg swelling <strong>and</strong>pain• There is fever• You see this• Are you worried?51
• Don’t mistaken this case as cellulitis• Features that suggests NecrotizingFasciitis:– Systemic symptoms– Disproportionate pain <strong>and</strong> tenderness over <strong>the</strong><strong>clinic</strong>al signs– Purplish discoloration– Blister formation52
TreatmentPrognosis depends on• High index of <strong>clinic</strong>al suspicion ofattending doctor• Early diagnosis• Early involvement of O&T, ICU <strong>and</strong>Microbiology Team• Early surgical treatment53
A case of head injury• 61 year old man with IHD <strong>and</strong> PTCAperformed 2 months ago• On aspirin <strong>and</strong> pravix• He had syncope after micturition <strong>and</strong> felllast night, sustained head injury, brief LOC• See you in <strong>the</strong> morning• You note a 2cm haematoma on occiput• Will you refer this case to A&E?54
Decision for CT Brain55
High Risk HistoryHigh Risk PE• Mechanism of injury• LOC• Amnesia• Anticoagulants (Pravix)• Coagulopathy• Vomiting• Seizure• Focal neurologicalsigns• Asymmetric pupils• Distracting injuries• Intoxication• Large extra cranialhaematoma• Signs of skull #56
Paediatric case• A 6 years old girl presented to you withfever for 2 days• She developed rash this morning• Temp: 39C, patient looks lethargic• This rash is notblanchable57
MeningococcaemiaYour action• Personal protection• Call ambulance• Give one dose of antibiotics beforesending patient away: Cefotaxime(Claforan) or Ceftriaxone (Rocephin)50mg/kg IV• Early antibiotics saves life58
Traffic light system for identifying risk of serious illnessfor children with feverColour• Pale/mottled/ashen/blueActivityRespirationHydrationO<strong>the</strong>rs• No response to social cues• Appears ill to a HCP• Unable to rouse or if roused does not stay awake• Weak, high-pitched or continuous cry•Grunting• Tachypnoea: RR > 60 breaths/minute• Moderate or severe chest indrawing• Reduced skin turgor•0–3 months: ≥ 38˚C;3–6 months: ≥ 39˚C•Non-blanching rash• Bulging fontane• Neck stiffness• Status epilepticus• Focal neurological signs• Focal seizures•Bile stained vomitus
Traffic light system for identifying risk of serious illnessColour• Pallor reported by parent/carerActivity • Not responding normally to social cues• Wakes only with prolonged stimulation• Decreased activity• No smileRespirationHydrationO<strong>the</strong>rs•Nasal flaring• Tachypnoea:RR > 50 breaths/minute age 6–12 monthsRR > 40 breaths /minute age > 12 months• Oxygen saturation ≤ 95% in air• Crackles• Dry mucous membrane• Poor feeding in infants• CRT ≥ 3 seconds• Reduced urine output•Fever ≥ 5 days•Swelling of a limb or joint•Non-weight bearing/not using an extremity
Traffic light system for identifying risk of serious illnessColourActivityRespiration•Normal colour of skin, lips <strong>and</strong> tongue•Responds normally to social cues•Content/smiles•Stays awake or awakens quickly•Strong normal cry/not crying•NormalHydration•Normal skin <strong>and</strong> eyes•Moist mucous membranesO<strong>the</strong>rs•None of <strong>the</strong> amber/ red symptoms orsignsNICE <strong>clinic</strong>al guideline 47 : Feverish illness in children: Assessment <strong>and</strong>initial management in children younger than 5 years
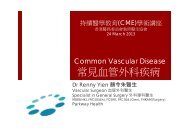
Last case• 16 year old girl repeated presented to youfor UTI symptoms• Several courses of antibiotics have beengiven• This time she also C/O epigastric pain withis quite severe; cramping in nature62
Ketamine associated cystitisnormal ketamine abuser x 4 yrs Ketamine abuser x 7 yrsABCourtesy of Dr Peggy Chu, TMH63
Ketamine Associated AbdominalPain• Onset a few hours after taking ketamine• Lasted for 1 to a few days• Epigastric pain, dull <strong>and</strong> persistent or cramping– Associated nausea <strong>and</strong> vomiting• Partial relief by buscopan / opioid, but notantacid• Abnormal LFT (~15% HKPIC cohort)
The endThank you for your attention!Questions are welcome65