2010 BC Guide in Determining Fitness to Drive
2010 BC Guide in Determining Fitness to Drive 2010 BC Guide in Determining Fitness to Drive
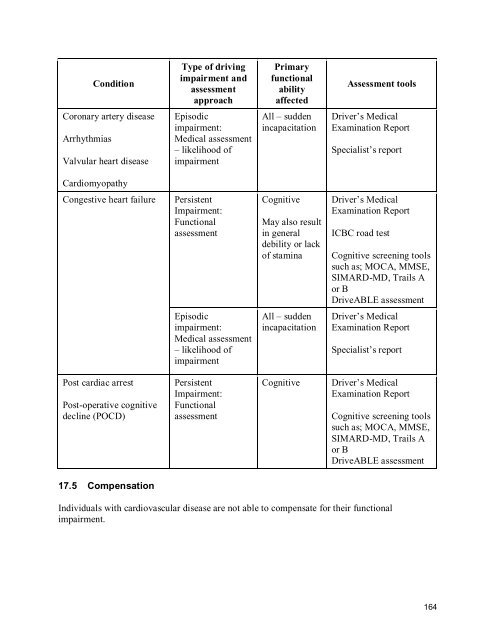
ConditionType of drivingimpairment andassessmentapproachPrimaryfunctionalabilityaffectedAssessment toolsCoronary artery diseaseArrhythmiasValvular heart diseaseEpisodicimpairment:Medical assessment– likelihood ofimpairmentAll – suddenincapacitationDriver’s MedicalExamination ReportSpecialist’s reportCardiomyopathyCongestive heart failurePersistentImpairment:FunctionalassessmentCognitiveMay also resultin generaldebility or lackof staminaDriver’s MedicalExamination ReportICBC road testCognitive screening toolssuch as; MOCA, MMSE,SIMARD-MD, Trails Aor BDriveABLE assessmentEpisodicimpairment:Medical assessment– likelihood ofimpairmentAll – suddenincapacitationDriver’s MedicalExamination ReportSpecialist’s reportPost cardiac arrestPost-operative cognitivedecline (POCD)PersistentImpairment:FunctionalassessmentCognitiveDriver’s MedicalExamination ReportCognitive screening toolssuch as; MOCA, MMSE,SIMARD-MD, Trails Aor BDriveABLE assessment17.5 CompensationIndividuals with cardiovascular disease are not able to compensate for their functionalimpairment.164
GUIDELINES17.6 Policy rationaleThese guidelines are based primarily on recommendations contained in the final report of the2003 Canadian Cardiovascular Society (CCS) Consensus Conference Assessment of the CardiacPatient for Fitness to Drive and Fly. The CCS recommendations focus exclusively on thepotential episodic impairments associated with cardiovascular diseases.Additional guidelines have been added to address potential persistent cognitive impairmentcaused by congestive heart failure, and the potential for co-morbid cognitive impairment inrelation to cardiac arrest, and post-operative cognitive decline (POCD) following coronary arterybypass graft (CABG) surgery. Where guidelines have been added or changed, the rationale isincluded in the table.17.7 Private and commercial drivers with congenital heart defectsApplicationAssessment guidelinesFitness guidelinesOSMV determinationguidelinesConditionsRestrictionsRe-assessmentguidelinesPolicy rationaleThese guidelines apply to driver fitness determinations for privateand commercial drivers who have a congenital heart defect.If further information regarding an individual’s medical condition isrequired, OSMV will request: a Driver’s Medical Examination Report additional information from the treating physician, or an assessment from a cardiologist.Individuals may drive if they meet any guidelines related to a specificcardiovascular condition or event.Individuals are fit to drive.No conditions are required.No restrictions are required.If the defect has been repaired and the treating physician does notindicate any concerns, no re-assessment, other than routinecommercial or age-related re-assessment, is required. If the defecthas not been repaired, OSMV will re-assess every 5 years, unlessroutine commercial or age-related re-assessment applies.Congenital heart defects are not specifically addressed in the CCSguidelines. It is included here in recognition that a congenital heartdefect may be reported to OSMV. The nature of congenital heartdefects and their treatment is variable; therefore there are no specificfitness guidelines for them.165
- Page 127 and 128: Deep-vein thrombosisDeep-vein throm
- Page 129 and 130: Aneurysms less than 5 cm in diamete
- Page 131 and 132: GUIDELINES12.6 Private and commerci
- Page 133 and 134: 12.7 Private drivers who have an an
- Page 135 and 136: 12.9 Commercial drivers who have an
- Page 137 and 138: Chapter 13: Musculoskeletal Conditi
- Page 139 and 140: ConditionType of drivingimpairment
- Page 141 and 142: GUIDELINES13.6 Private and commerci
- Page 143 and 144: ConditionsRestrictionsRe-assessment
- Page 145 and 146: 14.3 Chronic renal disease and adve
- Page 147 and 148: GUIDELINES14.6 Private and commerci
- Page 149 and 150: 14.8 Private drivers with end-stage
- Page 151 and 152: 14.10 Private and commercial driver
- Page 153 and 154: Level ofImpairmentMildlyImpairedMod
- Page 155 and 156: GUIDELINES15.6 Private and commerci
- Page 157 and 158: 15.8 Commercial drivers with modera
- Page 159 and 160: 15.10 Commercial drivers with sever
- Page 161 and 162: Policy rationaleDrivers who require
- Page 163 and 164: Chapter 16: Vestibular DisordersBAC
- Page 165 and 166: One study identified that 32.5% of
- Page 167 and 168: ConditionType ofdrivingimpairmentan
- Page 169 and 170: Re-assessmentguidelinesPolicy ratio
- Page 171 and 172: 16.8 Private and commercial drivers
- Page 173 and 174: 16.10 Private and commercial driver
- Page 175 and 176: Individuals who have undergone valv
- Page 177: Episodic impairmentThe potential ep
- Page 181 and 182: 17.9 Commercial drivers with corona
- Page 183 and 184: 17.11 Private drivers who have had
- Page 185 and 186: 17.13 Private and commercial driver
- Page 187 and 188: 17.15 Private drivers who have vent
- Page 189 and 190: 17.17 Private and commercial driver
- Page 191 and 192: 17.19 Private drivers who have sust
- Page 193 and 194: 17.21 Commercial drivers who have s
- Page 195 and 196: 17.23 Private and commercial driver
- Page 197 and 198: 17.25 Private and commercial driver
- Page 199 and 200: 17.27 Private drivers with atrioven
- Page 201 and 202: 17.28 Commercial drivers with atrio
- Page 203 and 204: 17.29 Private drivers with permanen
- Page 205 and 206: 17.31 Private drivers who have decl
- Page 207 and 208: 17.33 Private drivers where ICD the
- Page 209 and 210: 17.35 Commercial drivers who have d
- Page 211 and 212: 17.37 Commercial drivers with inher
- Page 213 and 214: 17.39 Commercial drivers with medic
- Page 215 and 216: 17.41 Private drivers with surgical
- Page 217 and 218: 17.43 Private drivers with mitral v
- Page 219 and 220: 17.45 Private drivers with congesti
- Page 221 and 222: 17.46 Commercial drivers with conge
- Page 223 and 224: 17.47 Private drivers with left ven
- Page 225 and 226: 17.49 Private drivers with a heart
- Page 227 and 228: 17.51 Private drivers with hypertro
ConditionType of driv<strong>in</strong>gimpairment andassessmentapproachPrimaryfunctionalabilityaffectedAssessment <strong>to</strong>olsCoronary artery diseaseArrhythmiasValvular heart diseaseEpisodicimpairment:Medical assessment– likelihood ofimpairmentAll – sudden<strong>in</strong>capacitation<strong>Drive</strong>r’s MedicalExam<strong>in</strong>ation ReportSpecialist’s reportCardiomyopathyCongestive heart failurePersistentImpairment:FunctionalassessmentCognitiveMay also result<strong>in</strong> generaldebility or lackof stam<strong>in</strong>a<strong>Drive</strong>r’s MedicalExam<strong>in</strong>ation ReportIC<strong>BC</strong> road testCognitive screen<strong>in</strong>g <strong>to</strong>olssuch as; MOCA, MMSE,SIMARD-MD, Trails Aor B<strong>Drive</strong>ABLE assessmentEpisodicimpairment:Medical assessment– likelihood ofimpairmentAll – sudden<strong>in</strong>capacitation<strong>Drive</strong>r’s MedicalExam<strong>in</strong>ation ReportSpecialist’s reportPost cardiac arrestPost-operative cognitivedecl<strong>in</strong>e (POCD)PersistentImpairment:FunctionalassessmentCognitive<strong>Drive</strong>r’s MedicalExam<strong>in</strong>ation ReportCognitive screen<strong>in</strong>g <strong>to</strong>olssuch as; MOCA, MMSE,SIMARD-MD, Trails Aor B<strong>Drive</strong>ABLE assessment17.5 CompensationIndividuals with cardiovascular disease are not able <strong>to</strong> compensate for their functionalimpairment.164


