referral form - Shodair Children's Hospital
referral form - Shodair Children's Hospital
referral form - Shodair Children's Hospital

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
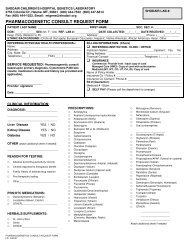
2755 Colonial Drive, PO Box 5539, Helena, MT 59604(406) 444-7500 1-800-447-6614 FAX (406) 444-7536Admission Assessment FormDate: ________________ Referring Party: ____________________________________________________ Phone#: ________________________Patient Living Arrangement: Parents Group Home Foster Home JDC Shelter Other: ____________________________Patient’s Name: ____________________________________________________________ Patient DOB: _____________________ Age: __________Patient’s SSN: ________________________________ Male Female Is youth emancipated, married or had a child? Yes NoName Adult(s) Legally Responsible:Father: ________________________________ Rights? Yes / No Hm# _________________ Cell#________________ SSN____________________Mother: _______________________________ Rights? Yes / NoHm# _________________ Cell#________________ SSN____________________Other #1: ______________________________Other #2: ______________________________POA or ________ Hm# _________________ Cell#________________ SSN____________________POA or ________ Hm# _________________ Cell#________________ SSN____________________DFS or Tribal: ________________________________________ TIA TLC Full Custody Cell#________________ Work#__________________Assaultive behavior? No Yes Suicidal behavior? No Yes Is patient an imminent danger to self or others? No YesReason for Admission: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________Mental Health Case Manager? No Yes Name: ________________________________________________ Phone# ___________________CSCT Organization/Therapist Name/Credentials/Ph#: ______________________________________________________________________________Outpatient Therapist? No Yes Name/Credentials/Ph#: ______________________________________________________________________Start Date: _____________ Last Appt. _____________ Frequency: Weekly Bi-Monthly MonthlyModality: Indiv. Family GroupPrevious <strong>Hospital</strong>izations (Where/When): ________________________________________________________________________________________Past Psychiatric Diagnoses Identified: ___________________________________________________________________________________________Current Meds/Doses: _________________________________________________________________________________________________________Meds Prescribed by: _____________________________________________________________________Phone # ___________________________Family Doctor/Pediatrician: ________________________________________________________________ Phone # ___________________________Physical Health Problems? No Yes MRSA? Identify: _______________________________________________________________________Medication Allergies: ______________________________________________ Other Allergies: ______________________________________________Alcohol or Drug Use? _______________________________________________Prior Treatment Provider(s): _________________________________Victim of Sexual Abuse? No Yes History of sexualized behaviors? No Yes Describe: ____________________________________History of Sexual Offenses No Yes Prior Treatment Provider(s): ______________________________________________________________Legal History? No Yes List: ____________________________________ Probation Officer/Ph #_____________________________________Cognitive or Developmental Delays? No Yes Identify: _______________________________ School: _______________________________Medicaid or Insurance? List: __________________________________________ Subscriber's Name/DOB: __________________________________Reviewed by Dr.____________________ Approved for Admit? ________ Recommendation: Acute Residential/Unit: ________________NOT approved:Process #: _____________________Page 1 Rev 5/2012
SHODAIR CHILDREN’S HOSPITALPsychosocial and Family AssessmentPatient SiblingsPlease list all known siblings of the patient (include name, age, residence): ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Describe patient's relationship with each sibling: ______________________________________________________________________________________________________________________________________________________________________________________________________________Patient Living ArrangementLiving arrangement prior to hospitalization: Biological Parent Other Biological Family Group Home Adoptive ParentsFoster CareJuvenile DetentionAddress: ____________________________________________________________ City/State/Zip: ___________________________________________List individuals living with patient and indicate relationship to patient: ____________________________________________________________________________________________________________________________________________________________________________________________How long has the patient lived in the current residence?____________________________________________________________________________Where else has the patient lived in the past 5 years?________________________________________________________________________________Does patient have access to firearms in the home? Yes No Are firearms kept locked and secured? Yes NoFamily History of Mental IllnessBiological mother's history (check all that apply):Depression Bipolar PTSD Anxiety Substance Use SchizophreniaHistory of Suicide Attempts History of Completed Suicide History of Psych. <strong>Hospital</strong>izationLearning Disability None known Other____________________________________________________________________________Biological father's history (check all that apply):Depression Bipolar PTSD Anxiety Substance Use SchizophreniaHistory of Suicide Attempts History of Completed Suicide History of Psych. <strong>Hospital</strong>izationLearning Disability None known Other____________________________________________________________________________Patient Developmental HistoryDevelopmental History (check all that apply):Pregnancy Problems Prenatal Substance Use Pre-term Birth Regression Postpartum DepressionTemper Tantrums Delay Motor Development Speech Delays Disrupted AttachmentsTrouble Making Friends Developmental Disability Genetic Abnormalities Delay toilet trainingSeparation Anxiety Sensory Difficulties No ConcernsAny significant medical issues or treatment patient has had? Yes NoAt what age did the patient do each of the following: Walk? ______ Talk?_____ Toilet Train?_______Page 3 Rev 5/2012
SHODAIR CHILDREN’S HOSPITALPsychosocial and Family AssessmentPatient Behavioral ProfileBehavior Profile (check all that have EVER been present)Sexually Active Suicidal Ideation Homicidal Ideation History of Suicide AttemptsSelf Harm Physical Aggression Verbal Aggression Psychosis (visual or auditory)Irritability Depression Poor Hygiene IsolationSleeping Less Sleeping More Hard to Wake Up NightmaresLoss of Appetite Excessive Appetite Poor Concentration Racing ThoughtsMood Swings Fire Setting Theft Running AwayLying Recent Losses Property Destruction Cruelty to AnimalsAnxiety School Refusal Bullying Others Being BulliedConflicts w/Peers Abnormal Toileting Habits Suspensions/Expulsions Difficulty w/AuthorityInappropriate Sexual BehaviorOther____________________________________________________________________Previous treatment for mental health or behavioral issue (check all that apply)ER Visit Acute <strong>Hospital</strong>ization Residential Treatment PRTF WaiverGroup Home Neurological Evaluation Psych Med Monitor Psych TestingOutpatient Ind. Therapy Partial Hos/Day Treatment Outpatient Family Therapy Group TherapyNoneList providers, dates of treatment, and length of stay:_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Neglect and Abuse HistoryHas the patient every experienced any of the following? (check all that apply)Physical Abuse Physical Abuse to Another Sexual Abuse Sexual Abuse to Another NeglectVerbal Abuse Verbal Abuse to Another Witnessed Domestic Abuse NoneExplain: _________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Has Department of Family Services ever been involved? Yes NoList dates, allegations, and findings: _____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Any legal charges filed or in process due to allegations? Yes NoPage 4 Rev 5/2012
SHODAIR CHILDREN’S HOSPITALPsychosocial and Family Assessment Page 4Legal HistoryWhat is the current legal status of the patient's probation? Formal In<strong>form</strong>al NoneProbation Officer: ___________________________________________________________ Phone Number:_________________________________Mark all that have EVER applied or CURRENTLY apply: Juvenile Detention Formal Probation In<strong>form</strong>al ProbationChemical Use HistoryMark ALL substances patient HAS used or IS using:Not Applicable Alcohol Marijuana Amphetamines Cocaine NarcoticsLSD PCP Methamphetamine Ecstasy Steroids InhalantsNicotine Over-the- Counter Meds Tranquilizers/Sedatives Prescription Meds-OthersPrevious treatment for chemical use issues: (check all that apply)Chemical Dependency Eval. Inpatient Outpatient Intensive Outpatient NonePlease list dates and length of stay of above services: ______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Access to other(s) prescription or over the counter meds at home? Yes NoAre medications locked and secure? Yes NoSchool HistorySchool Name: _________________________________________________ Contact Person: ________________________________ Grade: _______CSCT: Yes No CSCT Organization Name: ____________________________________________________________________CSCT Therapist/Credentials:____________________________________________________________________ Phone: ________________________Mark all that apply: IEP 504 No ServicesCategory: ___________________________________________________________________________________________________________________Conflicts with Peers/Adults? Yes NoPrevious Truancy Patterns: _____________________________________________________________________________________________________Preferred Learning Method: Auditory Visual TactileDetentions/Suspensions/Expulsions: Yes NoPage 5 Rev 5/2012
SHODAIR CHILDREN’S HOSPITALPsychosocial and Family Assessment Page 5Cultural and Spiritual NeedsSpiritual Affiliation: Yes No____________________________________________________________________________________________________________________________Active in cultural or spiritual activities? Yes No____________________________________________________________________________________________________________________________Cultural/environmental factors impeding treatment? Yes No____________________________________________________________________________________________________________________________Special requests for spiritual or cultural needs:________________________________________________________________________________________________________________________________________________________________________________________________________________Leisure/Recreational InterestsWhat are the patient's hobbies/interests and strengths?__________________________________________________________________________________________________________________________________________________________________________________________________________How many hours of TV, video games, or computer per week: _ Less than 10 _ 10-25 _ Greater than 25Environmental NeedsPlacement option/stable housing after treatment: Yes NoAccess to adequate and reliable transportation: Yes NoIs patient's neighborhood safe: Yes NoFinancial NeedsDoes the family receive public assistance: Yes NoIs the family Medicaid eligible: Yes NoOther financial needs:_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________Community ResourcesWhat support systems does the family have access to?Church Mental Health Services DPHHS ProbationCommunity Center After School Program Extended Family Advocacy GroupNeighbors Rec Center NoneOther support systems for family: ___________________________________________________________________________________________________________________________________________________________________________________________________________________________Page 6 Rev 5/2012
SHODAIR CHILDREN’S HOSPITALPsychosocial and Family Assessment Page 6Family ConsiderationsWhat are the strengths and assets of the family? ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________What is your hope for this hospitalization?________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Any other special needs of the family?___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Any additional in<strong>form</strong>ation? _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________XSignature of Person Completing FormDate**Please fax completed <strong>form</strong> to <strong>Shodair</strong> <strong>Children's</strong> <strong>Hospital</strong> (406)444-1039 or return in person upon admissionPage 7 Rev 5/2012