Caries and Restoration Prevention
Caries and Restoration Prevention
Caries and Restoration Prevention

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Caries</strong> <strong>and</strong> <strong>Restoration</strong> <strong>Prevention</strong>Ivar A. Mjör, Dorthe Holst <strong>and</strong> Harald M.EriksenJ Am Dent Assoc 2008;139;565-570The following resources related to this article are available online atjada.ada.org ( this information is current as of March 19, 2009 ):Updated information <strong>and</strong> services including high-resolution figures, can befound in the online version of this article at:http://jada.ada.org/cgi/content/full/139/5/565Information about obtaining reprints of this article or about permission toreproduce this article in whole or in part can be found at:http://www.ada.org/prof/resources/pubs/jada/permissions.aspDownloaded from jada.ada.orgon March 19, 2009© 2009 American Dental Association. The sponsor <strong>and</strong> its products are not endorsed by the ADA.
C L I N I C A L P R A C T I C E<strong>Caries</strong> <strong>and</strong> restoration preventionIvar A. Mjör, BDS, MSD, MS, Dr. odont.; Dorthe Holst, C<strong>and</strong>. odont., Dr. odont., MPH;Harald M. Eriksen, C<strong>and</strong>. odont., Dr. odont.Is it possible to maintain lifelongoral health with no or fewrestorations in populationsthat traditionally have hadhigh incidences of caries? Theanswer is yes. Research has led togreat advances in the prevention ofprimary dental caries. According tocurrent knowledge in cariology, thedevelopment of caries to the extentthat it requires surgical interventionlargely can be prevented.Implementation of effective preventiveprograms in general dentalpractice requires the active participationof dentists <strong>and</strong> dentalhygienists, who have the primaryresponsibility for educating <strong>and</strong>training patients in preventivebehaviors. Attention to other factorsunder the control of clinicians,notably criteria regarding when toplace restorations, is important inunderst<strong>and</strong>ing the improvementsrecorded. 1 In addition, patients’motivation <strong>and</strong> compliance areessential to ensure the success ofmost preventive approaches todental caries.Different age groups of patientshave been studied to demonstratethe effect of various preventive <strong>and</strong>restorative programs. The WorldHealth Organization (WHO) hasfocused on 13- <strong>and</strong> 14-year-olds, 2while others have studied 18- to20-year-olds. 3 Studies of thedecrease in caries initially focusedon children <strong>and</strong> adolescents, <strong>and</strong>the question of whether the effectABSTRACTBackground. The authors analyzed studies ofdecayed, missing <strong>and</strong> filled (DMF) rates for surfaces<strong>and</strong> teeth in Norway published during the last 30years. The result of active fluoride therapy combinedwith a change in criteria for when to place restorationsled to a marked reduction in the need for restorations.Methods. The authors reviewed independent, cross-sectional DMFstudies of representative samples of young adults performed every 10years during the period 1973 through 2006. The clinicians involved in thestudies used st<strong>and</strong>ardized <strong>and</strong> calibrated methods. The authors of thisarticle also reviewed an additional series of studies collecting DMF datafrom representative samples of 15-year-old adolescents that also had beencarried out independently from 1979 through 1996. In these studies, theinvestigators examined clinical records <strong>and</strong> bitewing radiographs withattention to progression of carious lesions <strong>and</strong> restorative treatments.Results. The authors noted a marked reduction in the mean decayed,missing <strong>and</strong> filled surface (DMFS) scores from 1973 through 2006 in thetwo adult groups. They also found a significant decrease in treatment ofcaries. The reduction was most marked after the mid-1990s. They notedthat the most dramatic change in the data from the 15-year-olds resultedfrom a change in the treatment criteria during the 1980s. Approximallesions in enamel were monitored by the investigators of those studies incombination with the use of fluoride toothpaste.Conclusion <strong>and</strong> Clinical Implications. A caries treatmentapproach based on active caries-preventive treatment <strong>and</strong> restrictivecriteria for restoration placement are good bases for reducing the need forrestorations as shown in cross-sectional studies reviewed.Key Words. Restorative dentistry; operative; general practice;research; review literature.JADA 2008;139(5):565-570.ARTICLEDr. Mjör is a professor <strong>and</strong> Academy 100 Eminent Scholar, Operative Dentistry, University of FloridaCollege of Dentistry, PO Box 100415, Gainesville, Fla. 32610, e-mail “imjor@dental.ufl.edu”. Addressreprint requests to Dr. Mjör.Dr. Holst is a professor, Community Dentistry, University of Oslo School of Dentistry, Oslo, Norway.Dr. Eriksen is dean, the Institute of Clinical Dentistry, University of Tromsø, Tromsø, Norway.✷C O N TJI N UAI N GDA✷®2I O NE D U C A TDownloaded from jada.ada.org on March 19, 2009Copyright © 2008 American Dental Association. All rights reserved.JADA, Vol. 139 http://jada.ada.org May 2008 565
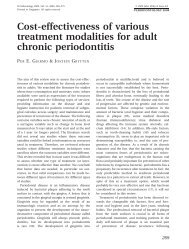
C L I N I C A L P R A C T I C ENUMBER OF TOOTH SURFACES8060402001973 1984 1993 2003STUDY YEARnoted was merely a postponement of the onset ofthe caries remained at issue until it was shownthat the caries decline was maintained intoadulthood. 4This article interprets published data <strong>and</strong>trends in oral health development <strong>and</strong> change intreatment criteria across more than 30 years. Itfocuses on the caries <strong>and</strong> restoration situation inNorway, but the situation is much the same in allthe Sc<strong>and</strong>inavian countries <strong>and</strong> in some non-Sc<strong>and</strong>inavian countries. Aside from this geographicalfocus, the clinical <strong>and</strong> science aspects ofour assessment should be comparative betweencountries.Filled SurfacesMissing SurfacesDecayed SurfacesFigure 1. Cross-sectional decayed, missing, <strong>and</strong> filled surfaces’ data for representative samplesof 35-year-olds in Oslo, Norway, during a 30-year period from 1973 through 2003.Source: Skudutyte-Rysstad <strong>and</strong> Eriksen. 5METHODS AND MATERIALSThis article focuses on published cross-sectionaldata regarding decayed, missing <strong>and</strong> filled surfaces(DMFS)/decayed, missing <strong>and</strong> filled teeth(DMFT) from 1973 through 2006. We based ourselection of the age groups on the assumptionthat the adult groups comprising people aged 35to 44 years were considered to represent thedental care provided well into adulthood <strong>and</strong> thatpeople aged 15 years represent the outcome ofdental care in childhood.We present data on the adults first becausethey represent the endpoint of the outcome of thedental restorative care in this review. One groupwas from an urban area 5 <strong>and</strong> the other from arural area. 6 We present results from the 15-yearoldage group 7 to assess if theimprovements noted in thedecayed, missing <strong>and</strong> filled(DMF) data regarding theadults’ teeth <strong>and</strong> tooth surfacesare consistent with the resultsfrom the 15-year-olds <strong>and</strong> if theyconform to the relatively rapidimprovements noted in the adultgroups.RESULTSThe adult groups. Data onrepresentative samples of 35-year-olds in Oslo, the capital cityof Norway, have been recordedby investigators 5 every 10 yearsfor several decades as part of ahealth survey of people in thisage group. DMFS/DMFT datahave been recorded by theseinvestigators since 1973, <strong>and</strong> thelast examination was completed in 2003. Thus,cross-sectional data across a 30-year period areavailable. 5 The criteria for recording caries werest<strong>and</strong>ardized (WHO criteria), <strong>and</strong> the clinicalexaminers’ methods were calibrated at each of theexaminations across the 30-year period.The DMFS data from this urban population in1973 showed that, on average, 70 tooth surfaceshad been restored or were missing or carious(Figure 1). 5 The restored surfaces constituted byfar the largest component of the DMF index;almost 50 surfaces involving 16 teeth had beenrestored. Decay, including primary <strong>and</strong> secondary(recurrent) caries, averaged 6.5 surfaces on 3.2teeth, <strong>and</strong> 2.8 teeth were missing. Third molarswere not included in the DMF index.A marked decrease in the DMF index did notbecome apparent until the 1993 survey, <strong>and</strong> thedecrease continued in the 2003 investigations.From 1973 to 2003, the data showed a 62 percentreduction in DMFS, an 83 percent decrease in themean number of carious lesions <strong>and</strong> a decrease of73 percent of missing teeth. The number ofrestored surfaces decreased by 56 percent. Primary<strong>and</strong> secondary caries together, on average,were diagnosed in less than one tooth surface perABBREVIATION KEY. DMF: Decayed, missing <strong>and</strong>filled. DMFS: Decayed, missing <strong>and</strong> filled surfaces.DMFT: Decayed, missing <strong>and</strong> filled teeth. WHO:World Health Organization.Downloaded from jada.ada.org on March 19, 2009566 JADA, Vol. 139 http://jada.ada.org May 2008Copyright © 2008 American Dental Association. All rights reserved.
C L I N I C A L P R A C T I C Epatient <strong>and</strong> constituted 0.7teeth in the sample of35-year-olds in 2003.The investigators independentlycollected DMFdata from the rural adultgroup by using the WHOcriteria every 10 years from1973 through 2006 (Figure2). 6 The 35- to 44- year-oldsubjects in this groupshowed similar results tothose reported in the urbanpopulation. The investigatorsnoted a decrease inthe mean number of DMFS/DMFT in 1994, <strong>and</strong> thedecrease continued asshown in the 2006 recordings.6 The mean number ofrestored teeth remainedsimilar from 1973 throughMEAN NUMBER OF SURFACESOR TEETH90807060504030201001983. After a slight increase in 1994 in the numberof restored teeth, the investigators noted adecrease in the 2006 recordings. 6 A comparison ofthe DMF recordings from the urban (Figure 1) <strong>and</strong>rural (Figure 2) adult populations indicates thedecreasing trends are similar in the two populations,although the DMF values are higher for therural population than for the urban population.The 15-year-old age group. The crosssectionalDMF data for the 15-year-old subjectswere available from the same urban population towhich the adult group belonged (Figure 3). 7Researchers reviewed DMF data regarding representativesamples of 15-year-olds during theperiod from 1979 through 1996, paying specialattention to the presence of caries that receivedrestorative treatment. 7 They r<strong>and</strong>omly selectedtreatment records, including the radiographsobtained immediately before the clinical examination,from those of the sample group of 15-yearolds.The radiographic examination was limitedto approximal surfaces from the distal surface ofthe first premolar to the mesial surfaces of thesecond permanent molars. Researchers performedradiography under st<strong>and</strong>ardized conditions, <strong>and</strong>carious lesions were recorded as being in theouter or inner one-half of the enamel or in theouter or inner one-half of the dentin. 7 Theresearchers noted surfaces missing owing tocaries <strong>and</strong> restored surfaces in the same locations<strong>and</strong> compared them with those observed at the1973 1983 1994 2006STUDY YEARDecayed, Missing<strong>and</strong> Filled SurfacesDecayed, Missing<strong>and</strong> Filled TeethFilled TeethFigure 2. Cross-sectional data on decayed, missing <strong>and</strong> filled surfaces; decayed, missing <strong>and</strong> filledteeth; <strong>and</strong> filled teeth data in 35- to 44-year-olds from a rural county in Norway from 1973 until2006. Source: Holst <strong>and</strong> colleagues. 6previous treatment session. 7 The researchersassessed changes in treatment criteria by comparingthe depth of the carious lesions that hadbeen restored during the next treatment session. 7The number of restored surfaces was reduceddramatically in the 1980s because of a change in thecriteria for placement of restorations in the treatmentof enamel lesions (Figure 3). 7 The number ofrestored surfaces decreased by 92 percent becauseclinicians were treating caries in the enamel preventivelyinstead of by placing restorations.DISCUSSIONFluoride plays an important role in the preventionof caries <strong>and</strong> consequently in restorationplacement, but attention to other factors, notablycriteria for when to place restorations, is essentialto underst<strong>and</strong> the improvements recorded in theadult populations reviewed here. 5,6 A number ofinteracting conditions must be in place to ensurethe success of caries-preventive programs thatinvolve easy access to fluorides, including dailyuse of fluoridated toothpaste; the engagement<strong>and</strong> supervision of caries progression by dentalpractitioners <strong>and</strong> dental hygienists; a publicinterested in good oral health <strong>and</strong> aiming to prioritizeoral hygiene; <strong>and</strong> restrictive criteria forplacement of restorations.A combination of the aforementioned factors iskey, but other factors—such as an increased levelof education, access to dental care <strong>and</strong> enhancedDownloaded from jada.ada.org on March 19, 2009JADA, Vol. 139 http://jada.ada.org May 2008 567Copyright © 2008 American Dental Association. All rights reserved.
C L I N I C A L P R A C T I C EPERCENTAGE OF RESTOREDENAMEL LESIONS10090807060504030201001979 1989 1993 1996STUDY YEARFigure 3. Cross-sectional data showing the percentage of enamelcaries lesions that were restored in a representative sample of15-year-olds in the School Dental Service in the city of Oslo, Norway,during a 17-year period. Note the dramatic reduction in the numberof restorations placed between 1979 <strong>and</strong> 1989. This reduction isconsidered to be due primarily to a change in the criteria for restorationplacement in the treatment of primary caries lesions—that is,noncavitated caries lesions limited to enamel were treated preventively<strong>and</strong> not with restorations. Source: Gimmestad <strong>and</strong> colleagues. 7living conditions, including increased personalincome—also play a role in the success of cariesprevention programs. Such effects are expected tohave greater potential significance in the UnitedStates, where a part of the population cannotafford dental treatment, while in some otherindustrialized countries, virtually everybodyseeks <strong>and</strong> receives regular dental care. 8,9 Our ownexperience during the last 40 to 50 years indicatesthe positive effect of caries <strong>and</strong> restorationprevention in practice in Norway. The caries- <strong>and</strong>restoration-preventive achievements that affectthe entire population in Sc<strong>and</strong>inavian generaldental practices have not reached all parts of theworld, including the United States.The demineralization of the dental tissues is themain basis for the detection <strong>and</strong> characterizationof caries lesions. Primary caries lesions on theproximal surfaces of teeth most often are detectedclinically, especially when supplemented by examinationof bitewing radiographs. In this way, cavitated<strong>and</strong> noncavitated lesions can be diagnosed.Other smooth-surface lesions are identified solelyby means of clinical examination. The diagnosis ofocclusal primary lesions is more difficult than thatof lesions on other surfaces because of the convoluteddistribution of enamel making up the pit<strong>and</strong>-fissurepattern of the occlusal surface.Primary caries lesions are classified as eitherenamel or dentin lesions. Enamel lesions may besubdivided into outer- <strong>and</strong> inner-enamel lesions.<strong>Caries</strong> that have reached dentin are classified asbeing in either the outer or the inner dentin;alternatively, the dentin lesions may be dividedinto three depth categories: outer, middle or innerdentin. An important question in the discussion ofrestoration prevention is the decision of whenrestorative therapy should be started in the treatmentof caries. The restrictive attitude towardrestoration decisions among dentists shown inthis review (that is, not treating enamel lesionssurgically) has been confirmed in other studies. 9-13This restrictive trend gradually has entered generaldental practice. A comparison of results fromsimilar studies in 1983 <strong>and</strong> 1995 shows anincrease from 66 to 82 percent of practitioners inNorway not treating enamel lesions surgically. 13Also, the reduction in the number of restored surfacesoccurred at a time when caries lesions ingeneral were decreasing; that is, the reduction inrestorations cannot be entirely credited to therestrictive criteria for placing restorations. Furthermore,fewer restorations placed to treat primarycaries will result in fewer replacements offailed restorations.The decision to place the first restoration in apreviously unrestored surface of a tooth is a crucialevent in the life of a tooth, because a permanentrestoration, in the true sense of the term“permanent,” does not exist. Every dentist recognizesthat restorations, once placed, will requirereplacement or repair after some time. Repair oflocalized lesions are indicated to save tooth structurelost owing to repeated replacements, butmany teaching programs <strong>and</strong> clinicians considerrepair of localized lesions an inferior, “patchwork”type of restorative treatment, despite good clinicalexperience <strong>and</strong> positive outcome of repair inclinical studies. 14,15Clinicians may need to be reminded thatremoval of carious tissues <strong>and</strong> placing of restorationsper se cannot be a permanent solution to thecaries problem. <strong>Restoration</strong> treats the effect of thedisease but does not focus on the cause of caries.If only the carious tissue is removed, not thereason for the development of the lesions, carieswill prevail <strong>and</strong> occur both on previously unrestoredsurfaces or adjacent to restorations as secondarycaries.One country’s fight against caries. SoonDownloaded from jada.ada.org on March 19, 2009568 JADA, Vol. 139 http://jada.ada.org May 2008Copyright © 2008 American Dental Association. All rights reserved.
C L I N I C A L P R A C T I C Eafter World War I, legislation was passed inNorway providing free dental services to childrenaged 7 to 14 years. At that time, Norway was apoor European country. This service, whichbecame known as the School Dental Service, wasnot effective before World War II because of theinsufficient numbers of dentists due to the lack oftraining <strong>and</strong> education. The School DentalService improved gradually in quality <strong>and</strong> quantityof coverage, <strong>and</strong> it became part of Norway’sNational Public Dental Service. Today, it coverschildren <strong>and</strong> adolescents from birth to age 18years. Adults are treated on a fee-for-service basissimilar to that in private practice anywhere inthe world. However, the sparse population ofsome parts of the country does not provide apatient pool large enough to support private practice.The dental service, therefore, was developedinto a combined public dental health care systembased on free dental treatment for children <strong>and</strong>special groups (such as people with disabilities<strong>and</strong> older adults) <strong>and</strong> a fee-for-service system foradults with a fee schedule similar to that in privatepractice.Virtually all children voluntarily participate inthe National Public Dental Service, so preventiveservices reach the entire population from birth to18 years of age. Because dental offices in Norwayusually are located in school buildings, the conditionsfor introducing preventive programs areclose to ideal. A private practice setting, in whichmost children in the United States receive dentalcare, requires initiative by the patient or parent,<strong>and</strong>, thus, compliance is less certain. While notdetailed here, the threshold for when to intervenesurgically also varies between U.S. <strong>and</strong> Sc<strong>and</strong>inavi<strong>and</strong>entists. 16Numerous studies <strong>and</strong> public health servicestatistics in Norway during the last three decadeshave demonstrated the effectiveness of therestorative services provided. Yet, the body of evidenceindicates that caries was not <strong>and</strong> cannot becured by placing restorations. One example of theeffectiveness of the restorative system was astudy of 18- to 20-year-old Norwegians in the late1950s. These young adults had, on average, aDMFS score approaching 50 <strong>and</strong> the filled componentwas by far the largest proportion for those3, 17who had received regular dental care.Oral hygiene has long been emphasized inNorway, <strong>and</strong> 94 to 97 percent of studentsreported toothbrushing more than once a day. 8,18In the prefluoride era, it seemed like the dentists<strong>and</strong> the patients were fighting a losing battle. Asa consequence of the improved oral health, thefrequency of dental examinations have increasedgradually. 9,18As fluoride entered caries-preventive programs,significant positive changes arose. Initialprograms involved supervising students’ rinsingwith a fluoride solution as an alternative to theprofessional topical application of sodium fluoridesolution. Soon these regimens were followed byprescription of fluoride tablets. Fluoride clearlyhad a positive effect, but it was not until after1971, when fluoride toothpaste could be purchasedwithout a prescription, that the beneficialeffects of fluoride could be demonstrated on a populationbasis. This event was a major breakthroughin caries prevention for the entire population.Attention also was focused on a number ofother areas later, including the diagnostic criteria<strong>and</strong> at what stage in the caries development restorationswere indicated for the treatment of thecaries. The findings demonstrated that thechange in the criteria for when to place restorations,combined with access to fluoride primarilyvia toothpaste, resulted in a positive reduction inthe number of restorations needed. Additionaleffects likely also have played a role, including ahigher level of education, improved living conditions<strong>and</strong> higher personal income. 10 Naturallyoccurring <strong>and</strong> artificially fluoridated water fluoridationprograms <strong>and</strong> supplies are rare in Norway.CONCLUSIONS<strong>Restoration</strong> prevention is linked closely to cariesprevention. A number of factors play a role in preventiveapproaches. Our literature review focusedon access to fluoride <strong>and</strong> restrictive criteria forwhen to place restorations once the disease hasoccurred. Provided initial carious lesions diagnosedin enamel are subjected to active preventivetreatment, a marked, long-term reduction inthe number of restorations can be achieved. ■Disclosure. The authors reported no disclosures.This review was supported in part by National Institute of Dental<strong>and</strong> Craniofacial Research/National Institutes of Health grantU01-DE-16746.1. Bille J, Thylstrup A. Radiographic diagnosis <strong>and</strong> clinical tissuechanges in relation to treatment of approximal carious lesions. <strong>Caries</strong>Res 1982;16(1):1-6.2. Holst D. The relationship between prevalence <strong>and</strong> incidence ofdental caries: some observational consequences. Community DentHealth 2006;23(4):203-208.3. Mjör IA. Dentistry in the 21st century with emphasis on operativedentistry. In: Simonsen RJ, ed. Dentistry in the 21st Century: A GlobalPerspective. Chicago.: Quintessence; 1991:199-206.Downloaded from jada.ada.org on March 19, 2009JADA, Vol. 139 http://jada.ada.org May 2008 569Copyright © 2008 American Dental Association. All rights reserved.
C L I N I C A L P R A C T I C E4. Eriksen HM. Has caries merely been postponed? Acta OdontolSc<strong>and</strong> 1998;56(3):173-175.5. Skudutyte-Rysstad R, Eriksen HM. Changes in caries experienceamong 35-year-old Oslo citizens, 1973-2003. Acta Odontol Sc<strong>and</strong>2007;65(2):72-77.6. Holst D, Schuller AA, Dahl KE. Bedre tannhelse for alle?Tannhelseutvikling i den voksne befolkning i Nord-Trøndelag fra 1973til 2006. [Improved oral health for everybody? Oral health developmentin the adult population in the county of North Trøndelag from 1973 to2006]. Nor Tannlaegeforen Tid 2007;117:804-811.7. Gimmestad AL, Holst D, Fylkesnes K. Changes in restorativecaries treatment in 15-year-olds in Oslo, Norway, 1979-1996. CommunityDent Oral Epidemiol 2003;31(4):246-251.8. Åstrøm AN, Samdal O. Time trends in oral health behaviorsamong Norwegian adolescents: 1985-97. Acta Odontol Sc<strong>and</strong>2001;59(4):193-200.9. Holst D, Varren A, Hogsnes T, Jacobsen HN. Innkallingsintervallerfor barn og unge i Den offentlige tannhelsetjenesten [Length ofrecall intervals for children <strong>and</strong> adolescents in the Public HealthService]. Nor Tannlaegeforen Tid 2007;117:942-947.10. Mejare I, Sundberg H, Espelid I, Tveit AB. <strong>Caries</strong> <strong>and</strong> restorativetreatment thresholds by Swedish dentists. Acta Odontl Sc<strong>and</strong> 1999;57(3):149-154.11. Holst D. Tannhelsen i dynamisk endring: fra sykdomsrisiko tilhelspotential [Oral health in a dynamic change: from risk of disease tohealth potential]. Nor Tannlaegeforen Tid 2004;114:866-871.12. Maltz M, Barbachan e Silva B, Carvalho DQ, Volkweis A. Resultsafter two years of non-operative treatment of occlusal surface in childrenwith high caries prevalence. Braz Dent J 2003;14(1):48-54.13. Tveit AB, Espelid I, Skodje F. Restorative treatment decisions onapproximal caries in Norway. Int Dent J 1999;49(3):165-172.14. Gordan VV, Shen, C, Riley, J III, Mjör IA. Two-year clinicalevaluation of alternative treatments to replacement of defective compositerestorations. J Esthet Restor Dent 2006;18(3):145-155.15. Gordan VV, Riley JL 3rd, Blaser PK, Mjör IA. 2-year clinicalevaluation of alternative treatments to replacement of defectiveamalgam restorations. Oper Dent 2006;31(4):418-425.16. Gordan VV, Bader J, Garvan C, et al.; for the DPBRN CollaborativeGroup. The diagnosis <strong>and</strong> treatment of primary caries by dentalPBRN dentists (abstract). In: AADR annual meeting program; April 2,2008; Dallas.17. Mjör IA. Interpretations of DMF registrations of Norwegianrecruits with emphasis on previous treatment experience. CommunityDent Oral Epidemiol 1974;2(3):98-103.18. Skau I, Holst D, Grytten J. Beh<strong>and</strong>lingspanorama oginnkallingsintervaller i privat allmennpraksis [Treatment panorama<strong>and</strong> length of recall intervals in private dental practice]. NorTannlaegeforen Tid 2005;115:764-768.Downloaded from jada.ada.org on March 19, 2009570 JADA, Vol. 139 http://jada.ada.org May 2008Copyright © 2008 American Dental Association. All rights reserved.