Monitoring & Evaluation Plan - Ministry of Health
Monitoring & Evaluation Plan - Ministry of Health
Monitoring & Evaluation Plan - Ministry of Health

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Ministry</strong> <strong>of</strong> <strong>Health</strong>2010 ANNUAL PERFORMANCEMONITORING REPORTMarch, 2011 Second <strong>Health</strong> Sector Support Program, 2009-13MINISTRY OF HEALTHNo. 151-53, Kampuchea Krom BlvdPhnom Penh, Kingdom <strong>of</strong> Cambodia.
in joint partnership with:Second <strong>Health</strong> Sector Support Program, 2009-13Implementing UnitsDepartment <strong>of</strong> AdministrationDepartment <strong>of</strong> Budget and FinanceDepartment <strong>of</strong> Communicable Disease ControlDepartment <strong>of</strong> Drugs, Food and CosmeticsCentral Medical StoresDepartment <strong>of</strong> Hospital ServicesDepartment <strong>of</strong> Human ResourcesDepartment <strong>of</strong> Internal AuditDepartment <strong>of</strong> International CooperationDepartment <strong>of</strong> PersonnelDepartment <strong>of</strong> <strong>Plan</strong>ning and <strong>Health</strong> InformationDepartment <strong>of</strong> Preventive MedicineNational Dengue Control Program (CNM)Helminths Control Program (CNM)National Maternal and Child <strong>Health</strong> Center (NMCHC)National Nutrition ProgramNational Reproductive <strong>Health</strong> Program (NMCHC))National Immunization Program (NMCHC)Prevention <strong>of</strong> Mother to Child Transmission Program (NMCHC)ARI-CDD-Cholera Program (NMCHC)National Center for Blood TransfusionNational Center for <strong>Health</strong> PromotionUniversity <strong>of</strong> <strong>Health</strong> SciencesTechnical School for Medical CareRegional Training Centers (Battambang, Kampot, Kampong Cham, Stung Treng)All Provincial <strong>Health</strong> DepartmentsAll Operational District OfficesMINISTRY OF HEALTHNo. 151-53, Kampuchea Krom BlvdPhnom Penh, Kingdom <strong>of</strong> Cambodia.Tel: 855.(0)23.880.261 Fax: 855.(0)23.880.262 Email: admin.hssp@online.com.kh2
ACRONYMS & ABBREVIATIONSADBAFDAFHAIDSALOSANCAOPAusAIDBCCBORBTCBTRCARECDCCDHSCECECCENATCFRCMSCNMCoCCPACPRCSESCWGCWMDBFDDFDFIDDRFAsian Development BankFrench Cooperation AgencyAction for <strong>Health</strong>Acquired Immune Deficiency SyndromeAverage Length <strong>of</strong> StayAntenatal CareAnnual Operational <strong>Plan</strong>Australian Agency for International DevelopmentBehavior Change CommunicationBed Occupancy RateBelgian Technical CooperationBed Turnover RateCooperative for Assistance and Relief Everywhere, IncCommunicable Disease Control DepartmentCambodia Demographic and <strong>Health</strong> SurveyContinuing EducationContinuing Education CoordinatorsNational Anti-Tuberculosis CenterCase Fatality RateCentral Medical StoresNational Center for MalariaContinuum <strong>of</strong> CareComplementary Package <strong>of</strong> ActivitiesContraceptive Prevalence RateCambodia Socio-Economic SurveyConstruction Working GroupCivil Works ManagerDepartment <strong>of</strong> Budget and FinanceDepartment <strong>of</strong> Drugs and FoodDepartment for International Development (UK)Drug Revolving Fund3
DOTSDPHIDPMEFEmONCEPIFTIGTZHCHCPHEFHISHIVHNIHPHRDHSP1HSP2HSSP1HSSP2HUICBICBAIDAIECIMCIIPDISCIYCFJAPRJICAMCHDirectly Observed Treatment, Short CourseDepartment <strong>of</strong> <strong>Plan</strong>ning and <strong>Health</strong> InformationDepartment <strong>of</strong> Preventive MedicineEquity FundEmergency Obstetric and Neonatal CareExpanded Program <strong>of</strong> ImmunizationsFast Track InitiativeDeutsche Gesellschaft fuer Technische Zusammenarbeit (GermanTechnical Cooperation Agency)<strong>Health</strong> Center<strong>Health</strong> Coverage <strong>Plan</strong><strong>Health</strong> Equity Fund<strong>Health</strong> Information SystemHuman Immuno-Deficiency Virus<strong>Health</strong> Net International<strong>Health</strong> PostHuman Resources Development DepartmentFirst <strong>Health</strong> Sector Strategic <strong>Plan</strong>, 2003-07Second <strong>Health</strong> Strategic <strong>Plan</strong>, 2008-15First <strong>Health</strong> Sector Support Project (ADB, DFID, UNFPA, IDA/TheWorld Bank)Second <strong>Health</strong> Sector Support Program (AFD, AusAID, BTC, DFID,UNFPA, UNICEF, IDA/The World Bank)<strong>Health</strong> UnlimitedInstitutional Capacity BuildingInstitutional Capacity Building AgencyInternational Development Association/The World BankInformation, Education, CommunicationIntegrated Management <strong>of</strong> Childhood IllnessesInpatient DepartmentIntegrated Supervision ChecklistInfant and Young Child FeedingJoint Annual Performance ReviewJapan International Cooperation AgencyMaternal and Child <strong>Health</strong>4
MDGMEFMOEYSMOHMOPMOUMPAMVHLNCHADSNGONHCNIPHNISNMCHCNPNPHNNPODODOOPDOPMPAPPHDPMTCTPOEPRO-TWGHPSIQAQIRACHARGCRHRHACMillennium Development Goals<strong>Ministry</strong> <strong>of</strong> Economy and Finance<strong>Ministry</strong> <strong>of</strong> Education, Youth and Sports<strong>Ministry</strong> <strong>of</strong> <strong>Health</strong><strong>Ministry</strong> <strong>of</strong> <strong>Plan</strong>ningMemorandum <strong>of</strong> UnderstandingMinimum Package <strong>of</strong> ActivitiesMost Vulnerable Households’ ListNational Center for HIV/AIDS, Dermatology, and SexuallyTransmitted InfectionsNon Governmental OrganizationNational <strong>Health</strong> CongressNational Institute <strong>of</strong> Public <strong>Health</strong>National Institute <strong>of</strong> StatisticsNational Center for Maternal and Child <strong>Health</strong>National ProgramNational Pediatric HospitalNational Nutrition ProgramOperational DistrictOperational District OfficeOutpatient DepartmentOxford Policy ManagementPriority Action ProgramProvincial <strong>Health</strong> DepartmentPrevention <strong>of</strong> Mother to Child TransmissionProvincial Office <strong>of</strong> EducationProvincial Technical Working Group <strong>Health</strong>Population Services InternationalQuality AssuranceQuality ImprovementReproductive and Child <strong>Health</strong> AllianceRoyal Government <strong>of</strong> CambodiaReferral HospitalReproductive <strong>Health</strong> Association <strong>of</strong> Cambodia5
RMNCHRTCSCASPFSRCSTD/STISWApSWiMTATBTORTWG-HUNFPAUNICEFURCUSAIDUSDVCCTVHISVHVWBWHOWIFReproductive, Maternal, Newborn and Child <strong>Health</strong>Regional Training CenterSave the Children AustraliaSocial Protection FundSwiss Red CrossSexually Transmitted Diseases/InfectionsSector Wide ApproachSector Wide ManagementTechnical AssistanceTuberculosisTerms <strong>of</strong> ReferenceTechnical Working Group - <strong>Health</strong>United Nations Population FundUnited Nations Children’s FundUniversity Research CompanyU.S. Agency for International DevelopmentU.S. DollarsVoluntary Confidential Counseling and TestingVoluntary <strong>Health</strong> Insurance SchemeVillage <strong>Health</strong> VolunteerThe World Bank/International Development AssociationWorld <strong>Health</strong> OrganizationWeekly Iron Folate supplements6
TABLE OF CONTENTSSECTION A: KEY PROGRAM INFORMATION .......................................................................................... 9OVERVIEW OF SECTOR PROGRESS .............................................................................................................. 10PROGRAM IMPLEMENTATION PROGRESS .................................................................................................. 16KEY IMPLEMENTATION ISSUES .................................................................................................................... 22BASIC PROGRAM DATA ............................................................................................................................... 23PERFORMANCE INDICATOR DASHBOARD ................................................................................................... 24PROGRAM DEVELOPMENT OBJECTIVES INDICATORS, PROVINCIAL LEAGUE TABLE, ................................. 25PROGRAM DEVELOPMENT OBJECTIVES INDICATORS, OPERATIONAL DISTRICT LEAGURE TABLES .......... 31PROVINCIAL REFERRAL HOSPITALS/SPECIAL OPERATING AGENCIES ......................................................... 39PROGRAM PERFORMANCE INDICATORS .................................................................................................... 40PROJECT MONITORING INDICATORS .......................................................................................................... 42EXPENDITURES TO DATE AND PROJECTED CASH REQUIREMENT FOR NEXT TWO QUARTERS (ALLFUNDS) ........................................................................................................................................................ 44OVERALL POOLED FUNDS BUDGET PROJECTIONS ...................................................................................... 45CHAPTER 1: INTRODUCTION AND BASIC DATA .................................................................................. 461.1 INTRODUCTION ............................................................................................................................................................ 46SECTION B: PROGRAM IMPLEMENTATION PROGRESS ....................................................................... 49CHAPTER 2: STRENGTHENING HEALTH SERVICE DELIVERY .................................................................. 502.1 EXPAND COVERAGE OF MPA AND CPA BASED ON HEALTH COVERAGE PLAN AND CLIENT NEEDS .................................. 502.1.1 PROGRESS OF CIVIL WORKS ................................................................................................................................... 502.2 STRENGTHEN HEALTH SERVICE DELIVERY SUPPORT SYSTEMS IN AN INTEGRATED MANNER .............................................. 512.3 TARGET PUBLIC HEALTH SERVICE PROVISION AND PUBLIC HEALTH INTERVENTIONS ACCORDING TO NEED ...................... 532.3.1 REPRODUCTIVE, MATERNAL, NEONATAL, AND CHILD HEALTH ................................................................................. 532.3.2 COMMUNICABLE DISEASES ..................................................................................................................................... 602.4 DEVELOP CONTRACTING MODELS AS COMPREHENSIVE APPROACH TO HEALTH SERVICE DELIVERY.................................. 642.4.1 SPECIAL OPERATING AGENCIES/SERVICE DELIVERY GRANTS .................................................................................... 64CHAPTER 3: HEALTH CARE FINANCING STRATEGY .............................................................................. 773.1 INCREASE GOVERNMENT BUDGET AND IMPROVE EFFICIENCY OF GOVERNMENT RESOURCE ALLOCATION FOR HEALTH…773.2 REDUCE FINANCIAL BARRIERS AT THE POINT OF CARE AND DEVELOP SOCIAL HEALTH PROTECTION MECHANISMS ........... 783.2.1 HEALTH EQUITY FUNDS RESULTS AND ACHIEVEMENTS ............................................................................................ 78CHAPTER 4: HUMAN RESOURCES FOR HEALTH .................................................................................. 864.1 IMPROVE TECHNICAL SKILLS AND COMPETENCE OF HEALTH WORKFORCE ...................................................................... 864.2 STAFF DISTRIBUTION AND RETENTION, WITH PRIORITY TO PERSONNEL ESSENTIAL TO HEALTH SECTOR PRIORITIES .......... 914.3 STAFF TRAINING AT RTCS............................................................................................................................................. 914.4 PERFORMANCE MANAGEMENT SYSTEM ........................................................................................................................ 927
CHAPTER 5: HEALTH INFORMATION SYSTEM ..................................................................................... 94CHAPTER 6: HEALTH SYSTEM GOVERNANCE ...................................................................................... 966.1 HARMONIZATION AND ALIGNMENT WITHIN THE MOH AND ACROSS THE HEALTH SECTOR.............................................. 966.2 PUBLIC-PRIVATE PARTNERSHIPS ................................................................................................................................... 966.3 INSTITUTIONAL DEVELOPMENT ..................................................................................................................................... 966.3.1 POLICY DEVELOPMENT AND IMPLEMENTATION ....................................................................................................... 966.4 STRENGTHEN MOH HEALTH SECTOR STEWARDSHIP THROUGH DECENTRALIZATION AND DECONCENTRATION ................ 976.5 STRENGTHENING COMMUNITY ENGAGEMENT ............................................................................................................... 98CHAPTER 7: PROGRAM MANAGEMENT AND IMPLEMENTATION ..................................................... 1017.1 KEY PROGRAM MANAGEMENT AND IMPLEMENTATION ISSUES ................................................................................... 1017.1.1 EXTERNAL AUDITS ............................................................................................................................................... 1017.1.2 LEGAL COVENANTS ............................................................................................................................................. 1017.1.3 JOINT QUARTERLY MEETINGS .............................................................................................................................. 1017.1.4 INDIGENOUS PEOPLES FRAMEWORK .................................................................................................................... 1017.1.5 GOOD GOVERNANCE FRAMEWORK ..................................................................................................................... 1017.1.6 SOCIAL SAFEGUARDS ........................................................................................................................................... 1037.1.7 ENVIRONMENTAL SAFEGUARDS ........................................................................................................................... 1037.1.8 INVOLUNTARY RESETTLEMENT ............................................................................................................................. 1047.1.9 PROCUREMENT ................................................................................................................................................... 104CHAPTER 8: PROGRAM MONITORING AND EVALUATION ................................................................ 1098.1 PROGRAM MONITORING ACTIVITIES .......................................................................................................................... 1098.2 SERVICE DELIVERY MONITORING GROUP ................................................................................................................... 110ANNEXES ........................................................................................................................................ 113ANNEX A. AGREED ACTIONS TAKEN ON INTERNAL CONTROL BASED ON EXTERNAL AUDIT REPORTS FOR QUARTERS I, II &III 2010 .......................................................................................................................................................................... 113ANNEX B. RECORD OF CONTRACTS FROM CKP ................................................................................................................. 121ANNEX C. ADMINISTRATION OFFICIAL CADRE IN 2010 ..................................................................................................... 124ANNEX D. INDICATOR BY PROVINCE AND OD (NUMERATORS ONLY) ................................................................................. 1268
SECTION A: KEY PROGRAM INFORMATION9
OVERVIEW OF SECTOR PROGRESSThis discussion <strong>of</strong> overall sector progress during the first semester, 2010 draws heavily from thePreliminary Report <strong>of</strong> the Cambodia Demographic and <strong>Health</strong> Survey 2010, and the MOH’sReport prepared for the 32 nd National <strong>Health</strong> Congress and 9 th Joint Annual PerformanceReview conducted on 14-15 March, 2011. Additional information has been drawn fromindividual MOH Program Task Force reports and presentations, as well as sub-sector andnational program specific reports such as the Annual <strong>Health</strong> Financing Report, NationalNutrition Program Annual Report, etc.OVERALL SECTOR PROGRESSIn March, 2011 the <strong>Ministry</strong> <strong>of</strong> <strong>Health</strong> released the Preliminary Report <strong>of</strong> the CambodiaDemographic and <strong>Health</strong> Survey 2010 jointly conducted by National Institute <strong>of</strong> Statistics,<strong>Ministry</strong> <strong>of</strong> <strong>Plan</strong>ning, the MOH’s Directorate General for <strong>Health</strong>, and the MEASURE DHS Projectimplemented by ICF Macro, with financial assistance from the HSSP2 Program, USAID, UNFPA,UNICEF, and JICA. The 2010 CDHS follows the successful CDHS surveys conducted in 2000 and2005 and provides Cambodia with three data points over the past decade to track progresstoward the targets contained in the National Strategic Development <strong>Plan</strong>, and the CambodiaMillennium Development Goals.Infant and child mortality estimates from CDHS 2010 continue to show significant declineswitnessed from the previous CDHS surveys. The infant mortality rate has declined from 95 forthe 1996-2000 period to 65 in the 2001-05 period to 45 in the 2006-10 period. Similarly, under5 mortality has declined from 124 per 1,000 live births to 83 to 54 over the same periods. Thismeans that currently, about 1 in 20 children born in Cambodia dies before reaching their fifthbirthday. The total fertility rate also shows the steady declines witnessed from past surveys.The 2010 CDHS found that the TFR was 3.0 children per married woman <strong>of</strong> reproductive age,down from 4.0 in 2000 and 3.4 in 2005. Concomitant with this decline, the contraceptiveprevalence rate for modern methods has climbed from 19% in 2000, to 27% in 2005, to 35% inthe 2010 CDHS.Several utilization and coverage indicators for maternal and child health also show substantialimprovement, including deliveries by trained health pr<strong>of</strong>essionals which has climbed from 32%in 2000 to 44% in 2005 and 71% in 2010, and deliveries at health facilities from 10% in 2000 to22% in 2005, and 54% in 2010. The percent <strong>of</strong> pregnant women with at least one antenatal carevisit has also increased 38% in 2000, to 69% in 2005 and 89% in 2010. Similarly, the fullimmunization rate measured for children 12-23 months increased from 40% in 2000 to 67% in2005 and 79% in 2010.The nutritional status <strong>of</strong> children under 5 years <strong>of</strong> age, however, continues to be <strong>of</strong> someconcern. Based on the recalculation <strong>of</strong> the 2005 CDHS data applying the new growth standardsadopted by WHO in 2006, it appears that the rate <strong>of</strong> stunting (height-for-age) has declined onlymarginally from 43% in 2005 to 40% in 2010, while wasting (weight-for-height) was 8% in 2005and 11% in 2010, and underweight (weight-for-age) remained stationary at 28% in both CDHSs.Anemia also is common among children in Cambodia: 55% <strong>of</strong> children 6-59 months were foundto be anemic, with nearly all children either moderately anemic (26%) or mildly anemic (28%),and 1% severely anemic. In contrast to children’s nutritional status, several behavioral andutilization indicators show significant improvement. The exclusive breastfeeding rate has10
climbed from 60% in 2005 to 74% in 2010. In 2010, approximately two thirds <strong>of</strong> infants werebreastfed within one hour <strong>of</strong> birth (65%), and 89% within one day <strong>of</strong> birth. The coverage <strong>of</strong>vitamin A supplements for children 6-59 months increased from 35% in 2005 to 71% in 2010,while the proportion receiving deworming medication increased from 27% in 2005 to 57% in2010. It should be noted that the Preliminary Report does not contain any breakdowns onthese national indicators in terms <strong>of</strong> wealth quintiles; that analysis is awaited in the FinalReport due in July, 2011. It is very likely that the summary indicators presented above willcontinue to show wide disparities across wealth quintiles as was found in the 2005 CDHS.Reproductive, Maternal, Newborn and Child <strong>Health</strong> In terms <strong>of</strong> Program 1: Reproductive,Maternal, Newborn, and Child <strong>Health</strong>, in general good progress was made in 2010. Of a total <strong>of</strong>19 performance indicators 7 had achieved their targets by year’s end, with achievement formost <strong>of</strong> the others only a few percentage points below prescribed targets. The 7 indicators forwhich targets were achieved include number <strong>of</strong> health facilities providing adolescent youthfriendly services (226 against a target <strong>of</strong> 135), proportion <strong>of</strong> deliveries at health facilities (50.2%against 50%), proportion <strong>of</strong> HIV positive pregnant women receiving ART for prevention <strong>of</strong>maternal to child transmission 57.3% against 50%), proportion <strong>of</strong> pregnant women attendingANC services receiving HIV testing and results 81.1% against 80%), proportion <strong>of</strong> children 12-59months <strong>of</strong> age receiving mebendazole supplements every 6 months (92% against 88%), number<strong>of</strong> OPD visits per capita for children under 5 years <strong>of</strong> age, new cases only, (1.51 against 1.3), andpercent <strong>of</strong> health centers implementing IMCI services (100% against 80%). Achievements for 9additional indicators were within 5 percentage points <strong>of</strong> their targets, including proportion <strong>of</strong>ANC2 visits (80% against 85%), proportion <strong>of</strong> deliveries by trained health pr<strong>of</strong>essionals, also aJoint <strong>Monitoring</strong> Indicator for the health sector as part <strong>of</strong> RGC-donor coordination (69.8%against 70%), proportion <strong>of</strong> pregnant women receiving iron folate supplements, 90 tablets (80%against 83%), proportion <strong>of</strong> postpartum women receiving iron folate supplements, 42 tablets(73% against 75%), proportion <strong>of</strong> postpartum women receiving one dose <strong>of</strong> vitamin Asupplements within 6 weeks <strong>of</strong> delivery (73% against 75%), proportion <strong>of</strong> children 6-59 months<strong>of</strong> age receiving two doses <strong>of</strong> vitamin A supplements within the past 6 months (95.5% against98%), number <strong>of</strong> referral hospitals providing comprehensive EmONC services (25 against 26),proportion <strong>of</strong> children under one year <strong>of</strong> age immunized with DPT3-HepB3 vaccine 92% against96%), and proportion <strong>of</strong> children under one year <strong>of</strong> age immunized against measles (93%against 95%). Only 3 indicators may be considered to have significantly failed to achieve theirtargets, including modern contraceptive method use (30% versus 40% - note that theachievement figure includes data from RHAC clinics; also, note that the 2010 CDHS preliminaryestimate for this indicator was 35% which covered public and private sector users), C-sectionrate (2% versus 2.5%), and number <strong>of</strong> referral hospitals and health centers functioning as basicEmONC facilities (19 versus 34%).Task Force 1 responsible for RMNCH services identified key enabling factors for successfulachievements as high level <strong>of</strong> commitment from government and health partners, expandingRMNCH priorities in AOP formulation to include IMCI and IYCF/BFCI packages, and availability <strong>of</strong>HSSP2 funding for all 24 provinces. Additional factors included expansion <strong>of</strong> HEFs to 57 ODs andCBHI to 18 schemes thus improving accessibility and affordability <strong>of</strong> RMNCH services to poorand vulnerable sections <strong>of</strong> the population, strong leadership at health center level withimproved transparency <strong>of</strong> user fees, HEF funding and live birth incentive payments,commitment from PHD toward improved deployment <strong>of</strong> midwives, and good participation fromcommunities and local authorities through increased utilization <strong>of</strong> RMNCH services and promptreferrals for emergencies.11
For nutrition, TF1 identified key priorities as scaling up systemic management <strong>of</strong> acuteundernutrition with community-based screening and facility level management, promotingappropriate infant and young child feeding practices through enforcement <strong>of</strong> the sub-decree onmarketing <strong>of</strong> IYCF products, and expansion <strong>of</strong> the IYCF/BFCI package and communicationcampaigns on breastfeeding and complementary feeding, improving the micronutrient status <strong>of</strong>children 6-24 months, women <strong>of</strong> reproductive age, and pregnant/postpartum women throughmicronutrient supplementation including in-home fortification with multi-micronutrientpowder, scaling up the weekly supplementation <strong>of</strong> IFA for women <strong>of</strong> reproductive age, andstrengthened behavior change communication on appropriate food intake. Priorities forreproductive health include expanding use <strong>of</strong> long term contraceptive methods and communitybased distribution, mobilizing resources to ensure modern methods availability beyond 2012,scaling up safe abortion services under the Abortion Law, and continuing expansion <strong>of</strong>adolescent youth friendly services with strengthened collaboration between communities andhealth facilities. Under maternal and newborn health, key priorities include strengtheningmaternal death audits, increasing the number <strong>of</strong> CEmONC and BEmONC health facilities,improving coverage and quality <strong>of</strong> ANC, delivery and postpartum care, and updating newborncare standard guidelines and training curriculum. Finally, TF1 highlighted the importance <strong>of</strong>increasing the coverage and quality <strong>of</strong> PMTCT services through expansion <strong>of</strong> HIV and othertesting among pregnant women, birth spacing for HIV positive women, ARV prophylaxis amongHIV positive women, and strengthening the system for early diagnosis and follow-up <strong>of</strong> HIVexposed infants.In terms <strong>of</strong> child health, key priorities for the 2011-12 period include strengthening IMCIservices through antibiotic treatment for pneumonia, management <strong>of</strong> diarrhea with lowosmolarityORS and zinc, and management <strong>of</strong> newborns; promoting appropriate home-basedcare <strong>of</strong> sick children and recognition and timely care seeking for danger signs, improving quality<strong>of</strong> pediatric care in hospitals, eliminating measles and maternal and neonatal tetanus,sustaining high immunization coverage with a focus on low performing ODs so as to achievenational targets, systems strengthening for immunizing specific target groups such as childrenin high risk and vulnerable groups, and the urban poor, and increasing coverage <strong>of</strong> Hepatitis Bvaccine at birth. The NIP in particular, has identified 4 main disease prevention and controlpriorities for the coming year including eradication <strong>of</strong> measles and tetanus (both mother andchild), combatting Hepatitis B, and maintaining the “no polio” status <strong>of</strong> the country.Communicable Disease Prevention and Control The MOH’s communicable diseaseprevention and control efforts made significant gains in 2010 with targets on most keyindicators being achieved. The proportion <strong>of</strong> people with advanced HIV infection receiving ARVcombination therapy (HAART) was 92% against the target <strong>of</strong> >95%, which represented amarginal decline over the 2009 achievement <strong>of</strong> 98%. The proportion <strong>of</strong> people living withHIV/AIDS on ART who survived beyond 12 months was 90% versus the target <strong>of</strong> >85%. For theTB program the case detection rate for smear positive pulmonary TB was 66% versus thestandard target <strong>of</strong> 70%; this represented a 4 percentage point increase in achievement over theprevious year. The TB cure rate on the other hand, was 91%, well over the 2010 target <strong>of</strong> >85%.The number <strong>of</strong> malaria cases treated at public health facilities per 1,000 population was 4.07against the target <strong>of</strong> 6.0, and well below the previous year’s achievement <strong>of</strong> 6.22. Finally, thecase fatality rate for dengue hemorrhagic fever reported from public health facilities was 0.3%in 2010 against the target <strong>of</strong> 0.6% and declined marginally from the 2009 CFR <strong>of</strong> 0.32%.12
Task Force 2 overseeing communicable disease prevention and control identified a number <strong>of</strong>factors responsible for the success <strong>of</strong> its strategy and interventions in 2010. These includefunding support from government and health partners, establishment <strong>of</strong> the Special OperatingAgencies, incentive payments to health workers, waiving user fees for treatment <strong>of</strong> emergingdiseases, availability <strong>of</strong> trained CDC staff at all levels <strong>of</strong> the health system, improved datatransmission and management, and monitoring and supervision activities. For HIV/AIDS, the TFidentified the following key priorities for the medium term (2011-14) period: maintainingcomprehensive (continuum <strong>of</strong> care) HIV/AIDS care and treatment for PLHA; strengthening HIVprevention among most at risk populations, and scaling up the linked response betweenHIV/AIDS, and reproductive, maternal and child health programs and interventions. The TBprogram will support refresher training on DOTS, and laboratory services, strengthen thecapacity to diagnose smear negative TB, extra pulmonary TB, and TB among children, andconduct national TB conference and annual program review. Malaria prevention and controlactivities over this period will focus on establishing a surveillance system for migrants,supplying adequate equipment for surveillance, case management, and vector control,supporting active case investigation <strong>of</strong> D3 positive cases: community early detection andtreatment through mobile malaria workers, containing malaria on Thai-Cambodian border(artesunate and mefloquine resistant parasites), and promoting community and school-baseddengue preventive activities with intensified surveillance and case management. Masslarviciding will be conducted in high risk provinces with two rounds per year for dengue control,along with broadcasts through TV and radio with dengue prevention and control messages.Anti-helminths interventions will include monitoring <strong>of</strong> chronic lymphatic filariasis patients forself-hygiene, monitoring prevalence <strong>of</strong> schistosomiasis through Kato-Katz technique andserology, and annual mass drug administration to people living in schistosomiasis endemicareas. Overall priorities will include developing the Communicable Disease Law asrecommended by HE Samdech Prime Minister, improving laboratory capacity to supportoutbreak response, supply laboratory equipment to rapid response teams, establish S&Rsystem for zoonoses, conduct training and refresher training on avian influenza awareness,surveillance, investigation and control, and finalize the Pandemic Preparedness <strong>Plan</strong> andformulate associated provincial plans.Non Communicable Disease Prevention and Control During this reporting period theMOH, in collaboration with the University <strong>of</strong> <strong>Health</strong> Sciences and with financial and technicalsupport from WHO, conducted the nationwide STEP survey to estimate the prevalence <strong>of</strong> riskfactors for noncommunicable diseases, and establish baseline information for prevention andcontrol interventions in the country. 1 Survey data were obtained from 5,433 adult participantsaged 25-64 years with a response rate <strong>of</strong> 96.3% through interviews, and physical andbiochemical measurements. Findings showed that 1 in every 10 respondents had newly andpreviously diagnosed mild hypertension (SBP ≥140 and/or DBP ≥90 mmHg); this proportion wassignificantly higher for urban and male respondents as compared to rural and femalerespondents, and increased with age. The prevalence <strong>of</strong> impaired fasting glycemia and diabeteswas 1.4% and 2.9% respectively. Prevalence <strong>of</strong> diabetes in urban areas was 2.4 times that inrural areas. Also, 1 in every 5 respondents had raised total cholesterol levels and thisproportion increased with age, was higher in women than men, and in urban as opposed torural areas. Finally, the survey showed that 8 <strong>of</strong> every 10 persons had one to two risk factors fordeveloping NCDs, whereas 1 in 10 had three or more risk factors. The proportion <strong>of</strong>1 <strong>Ministry</strong> <strong>of</strong> <strong>Health</strong> and University <strong>of</strong> <strong>Health</strong> Sciences, 2010. “Prevalence <strong>of</strong> Non-Communicable Disease Risk Factors in Cambodia, STEPS SurveyCountry Report,” September.13
espondents with three or more risk factors was 2.2 times higher in men versus women, 1.7times higher in urban than in rural areas, and increased with age.During this reporting period, continued progress was made toward the targets for the NCDprogram. The number <strong>of</strong> diabetes patients receiving treatment per 1,000 patients in publichealth facilities (data from 9 sentinel sites in the country) was 29 compared to the target <strong>of</strong> 30for the year. The number <strong>of</strong> hypertension cases receiving treatment per 1,000 population was20 which exactly equaled the target. The number <strong>of</strong> newly diagnosed cervical cancer cases per100,000 women over the age <strong>of</strong> 25 years was 33 as opposed to a target <strong>of</strong>
implementation <strong>of</strong> the new 3 year direct entry associate in midwifery program with anexpected 460 graduates from public institutions in 2011, provision <strong>of</strong> continuing education toupdate knowledge and skills <strong>of</strong> public health pr<strong>of</strong>essionals, and staff incentives providedthrough Special Operating Agencies and for midwives successfully attending a live birth.Bed occupancy rates were 77.3% nationally against the annual target <strong>of</strong> 75%. For essentialdrugs stockouts, as against a national target <strong>of</strong> 5% for 15 listed items, the national achievementwas 5.35%, down from 6.45 % in 200914 provinces had stockout rates above 5%. Against thenational annual target <strong>of</strong> 0.6 for OPD per capita, the national average was 0.63 for thisreporting period. Twelve <strong>of</strong> 24 provinces reported an OPD per capita rate below the nationalaverage, and only 9 provinces achieved their prescribed targets (targets ranged from a low <strong>of</strong>0.32 for Phnom Penh to a high <strong>of</strong> 1.62 for Otdar Meanchey). In terms <strong>of</strong> licensing <strong>of</strong> privateentities, including polyclinics, consultation cabinets, maternities, dental clinics etc. butexcluding pharmacies, 93% were licensed in 2010 versus a target <strong>of</strong> 77% for the sector. Forlicensed pharmacies, the achievement in 2010 was 94%, marginally below the national target <strong>of</strong>100%. The annual national budget for health has shown steady increases over the past fewyears: the adjusted budget has increased by 23% from 2008 to 2009, and by 16.41% in 2010 (CR645,138,220,000 or USD 161,284,555). Seventy one percent <strong>of</strong> this adjusted budget wasallocated to the central level, with the remaining allocated to the provincial level. Budgetdisbursement rates also show steady improvement: at the central level it was 94.8% while atthe provincial level it was 99.5% in 2010.<strong>Health</strong> equity fund and government subsidy schemes at referral hospitals have expandedcoverage across the provinces with 77% coverage <strong>of</strong> the population in 2010, as against 67% in2009. Seventy two percent or 57 referral hospitals were implementing HEF/subsidy schemes,and 29% or 291 HCs. All <strong>of</strong> the national hospitals also had similar schemes. There are now atotal <strong>of</strong> 18 community based health insurance schemes operating in the country covering atotal beneficiary population <strong>of</strong> 170,490 persons. Ninety five percent <strong>of</strong> PHDs had submittedtimely, accurate and complete HIS reports to the central HIS database in 2010, as against theannual target <strong>of</strong> 100%. This marked an improvement <strong>of</strong> 5 percentage points over 2009.Under this program, the key priorities for 2011-12 for health service delivery includestrengthening medical equipment maintenance and management system, improving quality <strong>of</strong>care at all health facilities utilizing the quality <strong>of</strong> care assessment tool developed by thedepartment <strong>of</strong> hospital services, improving laboratory services, and strengthening infectionprevention and control at health facilities.For health care financing, priorities include developing a <strong>Health</strong> Financing Policy through arevision <strong>of</strong> the 1996 National Charter for <strong>Health</strong> Financing, improving the evidence base forevaluation <strong>of</strong> HEFs, formulating a standard model for social health protection and preparing aplan for expansion <strong>of</strong> social health insurance in the country, developing guidelines on thebenefit package and provider payment methods, continuing collaboration with the Council onAdministrative Reform to update and finalize the Social <strong>Health</strong> Protection Master <strong>Plan</strong>, andstrengthening the links between SHP and quality <strong>of</strong> care.A key priority under human resource development includes the review <strong>of</strong> the Second National<strong>Health</strong> Workforce Development <strong>Plan</strong>, 2006-15 and strengthening the national HR informationsystem. Other priorities include continuing deployment <strong>of</strong> secondary midwives at HCs,expanding and upgrading clinical practicum sites (particularly referral hospitals located in towns15
Cat. No.with RTCs), enhancing the capacity building skills <strong>of</strong> teaching staff through the establishment <strong>of</strong>the Center for Educational Development for <strong>Health</strong> Pr<strong>of</strong>essionals, speeding up the introduction<strong>of</strong> a licensing and registration system for health pr<strong>of</strong>essionals through the development <strong>of</strong> aregulatory framework, strengthening staff pr<strong>of</strong>essional ethics under the management <strong>of</strong>pr<strong>of</strong>essional councils, and continuing to provide incentives to midwives for safe deliveries.Initiatives to be undertaken to strengthen the health information system include reviewingstandard HIS forms to make them more user friendly for private providers and NGOs, linkingdata reporting to the licensing process and enforcing it in collaboration with local authorities(no licensing without submittal <strong>of</strong> complete, accurate and timely HIS data), improving dataanalysis and use for decision making e.g., AOP formulation, providing training on datacollection, reporting, and database s<strong>of</strong>tware to private entities, and an assessment <strong>of</strong> thesector-wide need for IT support. Finally, key priorities under health system governance includestrengthening inter-ministerial collaboration as well as inter-departmental at provincial anddistrict levels for combatting counterfeit drugs and illegal practices, improving rational use,drug management and supervision at PHD and OD levels, strengthening accountability throughclient satisfaction surveys, and strengthening monitoring and accountability <strong>of</strong> SOAs (ODs andPRHs).PROGRAM IMPLEMENTATION PROGRESS1. Sector Wide Management: Following agreement between JPIG partners and MOH topmanagement on moving planning and monitoring functions to the Department <strong>of</strong> <strong>Plan</strong>ning and<strong>Health</strong> Information, the secretariat has been working extensively on aligning planning andreporting with the existing MOH established system. Currently, the planning function (exceptfor the mid-year review <strong>of</strong> the budget) has been fully integrated at all levels which has reducedthe role <strong>of</strong> secretariat in converting the approved plans into the Program approval format andbudget lines, following the HSSP2 financial management system. The recent updated programmonitoring framework is fully aligned with the HSP2 frame work except for a few monitoringindicators required by the World Bank’s portfolio projects.2. Most <strong>of</strong> the data for the indicators cited in this report have been taken from the National<strong>Health</strong> Congress Report presented at the NHC and JAPR meetings on 14-15 March, 2011, aswell as the HIS. In addition, for a few indicators such as “Percent <strong>of</strong> HIV positive pregnantwomen receiving ART for PMTCT” which are not available in the HIS, the data have beencompiled directly from the relevant national program.3. The 2010 Annual Operational <strong>Plan</strong> for the Program was $26,847,376 which included:Category NamePool AFD BTC UNFPA UNICEF TOTALSDG 1 5,014,202 803,407 0 0 0 5,817,609HEF Grant 2 1,970,000 0 0 400,000 84,000 2,694,000MBPI-related payment 3 137,904 0 9,217 0 0 147,121Goods 4A 1,961,137 1,500 10,000 0 130,400 2,103,037Civil Works 4B 92,000 000 0 92,00016
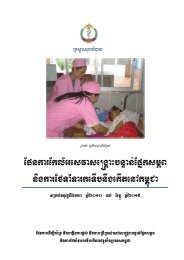
IDA/PoolMDTF/PoolUNICEF/PoolUNFPA /PoolTotal PooledUNICEF DiscreteUNFPA DiscreteBTC DiscreteAFD DiscreteRGCFCat. No.Category NamePool AFD BTC UNFPA UNICEF TOTALConsultant Services 4C 1,773,162 486,417 95,000 13,350 63,000 2,430,929Operating Costs 4D 6,493,818 109,125 39,000 883,876 377,485 7,903,304Training 4E 5,016,010 76,201 115,149 254,438 197,578 5,659,376Grand Total by Cat. Codes /Funding Sources22,458,234 1,476,650 268,366 1,551,664 852,463 26,847,3764. SUMMARY OF EXPENDITURESEXPENDITURES BY SOURCE OF FUNDS, 2010SourcesBudgetExpenditures Percent(millions US$)(millions US$)IDA/Pool 10.29 6.08 59%MDTF/Pool 17.22 10.18 59%UNICEF/Pool 0.53 0.31 59%UNFPA /Pool 0.73 0.43 59%Total Pooled 28.76 17.01 59%UNICEF Discrete 0.49 0.42 86%UNFPA Discrete 1.37 1.29 94%BTC Discrete 0.29 0.26 88%AFD Discrete 1.47 1.87 127%RGCF 0.90 1.04 116%Total 33.29 21.89 66%PERCENT EXPENDITURE AGAINST ALLOCATION BY SOURCE140%120%100%80%60%59% 59% 59% 59% 59%86%94%88%127%116%40%20%0%% Spent17
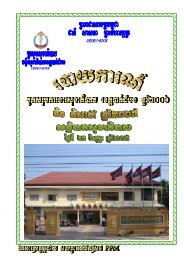
EXPENDITURES BY IMPLEMENTING UNITSPROVINCESMONPRVBTBPercent <strong>of</strong> AOP Budget Expended, 201087%116%115%97%116%117%84%128%122%UNFPAUNICEFPFOverallPURSHVKRTBMC88%85%90%127%134%145%142%158%144%148%145%0% 20% 40% 60% 80% 100% 120% 140% 160% 180%OMCKALPHNPLNKCHHSTGKCMKTHTKOPercent <strong>of</strong> AOP Budget Expended, 201062%98%69%79%79%71%89%83%89%89%110%85%91%89%93%92%100%82%99%94%71%104%96%98%97%58%109%99%87%291%103%0% 50% 100% 150% 200% 250% 300%AFDBTCUNFPAUNICEFPFOverall18
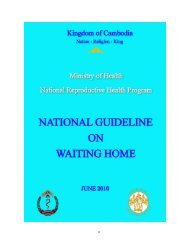
RATKPSKEPKKGSVRKPTSIRPVHPercent <strong>of</strong> AOP Budget Expended, 201052%47%49%60%65%65%70%70%94%73%74%72%92%75%65%76%76%39%76%77%78%87%78%79%0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%BTCUNFPAUNICEFPFOverallDEPARTMENTS, NATIONAL PROGRAMS, AND CENTRAL INSTITUTIONSPercent <strong>of</strong> AOP Budget Expended, 2010UNFPAUNICEFDengueNNPNRHP12%25%65%73%73%110%113%PFOverallPMTCTTU-MCHNIP97%97%100%100%96%47%54%0% 20% 40% 60% 80% 100% 120%19
Percent <strong>of</strong> AOP Budget Expended, 2010BTCST RTCKPT RTCKCM RTCBTB RTC5%12%28%23%22%50%44%57%80%101%122%UNFPAUNICEFPFNCHP92%92%HLFPC50%50%0% 20% 40% 60% 80% 100% 120% 140%Percent <strong>of</strong> AOP Budget Expended, 2010UNFPAADMIN84%84%PFUHS-TSMC7%7%OverallST RTC28%23%KPT RTC22%101%122%KCM RTC12%50%44%BTB RTC5%57%80%NCHP92%92%0% 20% 40% 60% 80% 100% 120% 140%20
Percent <strong>of</strong> AOP Budget Expended, 2010DIC23%23%PFDHS39%39%OverallDDF90%90%DBF61%61%CMS52%52%CDC36%36%0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%HSSPHRDPD12%13%15%15%42%Percent <strong>of</strong> AOP Budget Expended, 2010201%119%109%145%148%AFDBTCUNFPAUNICEFPFOverallIAD37%37%DPMDPHI60%60%89%50%52%0% 50% 100% 150% 200% 250%21
KEY IMPLEMENTATION ISSUESDelay in decision on overall budget for civil works resulted in delay in recruitment <strong>of</strong> civilworks design and management firm. The budget and package for civil works have beenapproved by WB, but procurement <strong>of</strong> civil works will likely take long and procurement<strong>of</strong> civil works firm will also take at least 6 monthsCurrently we have an Infrastructure Coordinator to coordinate construction <strong>of</strong> nationallaboratory, Preah Vihear RH, and other packages. However, there is a need for andadditional civil works engineer and Autocad designerThe scaling up <strong>of</strong> SDGs and HEFs from 2011 will require additional funds or reductionfrom other Program activities. Short-term contracts for <strong>Health</strong> Equity Funds (HEFs)result in increasing workload on procurement and delays in implementation. The newarrangement for 2 year contracts seems to be more efficient.Budget envelope for all IUs has helped them to prepare appropriate AOPs withinresource constraints <strong>of</strong> the Program. Timely approval <strong>of</strong> AOP before the end <strong>of</strong> the fiscalyear would allow the Program to prepare the procurement plan and start theprocurement process without delay. In 2010, AOP approval was delayed significantly;however, the 2011 AOP was approved in January indicating improvementIt was not possible to prepare a consolidated training plan for 2010. The 2011 planformat was endorsed in early 2011 and we are still awaiting formal submittal from IUs.Currently, recruitment <strong>of</strong> training coordinator is under short listingStaff issue in secretariat exists due to staff turnover which has affected timelycompletion <strong>of</strong> work due to time taken to recruit new staff, and for them to becomepr<strong>of</strong>icient in their workDespite several workshops, key issues regarding SDGs are still pending or were subjectto delay such as procurement by SOAs under operating costs, staff bonus paymentmodalities, etc. Target setting methods for SOAs were approved in 4 th quarter, 2010 andSOAs trained in application <strong>of</strong> the methods in a workshop in Kampong Cham inDecember, 2010. However, there was delay in approval <strong>of</strong> 2011 targets due to detailedreview conducted for each SOA, and suggestions for alternate targetsIn 2010 there were several short term extensions for HEFs; the situation has nowimproved with contracts for HEFOs being executed for 2 yearsWe need to pay attention to closing date <strong>of</strong> AFD and BTC components <strong>of</strong> HSSP2. Weneed to make sure <strong>of</strong> smooth transition to the new financing; under AFD funding, civilwork plans and medical equipment need to be completed before closing dateSDG payments to SOAs shifted from monthly replenishment to two quarter advancepayments in 2011 based on certification from SDMG on performance achievementsThe Financial Management Unit will collaborate more closely with the FMIP team, DBF,and DPHI to review possible ways to use common reporting formats for the <strong>Health</strong>Financing Bureau22
BASIC PROGRAM DATAJPA PARTNERSI. Pooled FundSourceAmountBudget Estimate fromPAD (US$)Budget Available byGrant Agreements(US$)MDTF (may increase) $ 52,092,675.00 52,092,675.00AusAID (2009 to June 2011. 37.150000 AU$ Million 30,000,000.00Future funding to beconfirmed)DFID (2009-2013) 35 GBP Million 50,000,000.00IDA (5 years) SDR 18,500,000.00 30,000,000.00UNICEF (2009 and 2010) 1,159,000.00UNFPA (2009 and 2010) 1,120,000.00Sub-Total Pooled Funds: 84,371,675.00II. Discrete FundsAFD (2008 – 2013) 7 Euro Million 10,000,000.00 10,000,000.00BTC (2009 – 2011) 3 Euro Million 4,500,000.00 4,285,714.00UNFPA (2009 and 2010) 8.867 USD Million 8,867,000.00 4,105,772.00UNICEF (2009 and 2010) 4 USD Million 4,000,000.00 3,413,778.00Sub-Total Discrete Funds: 21,805,264.00TOTAL JPA Partners 106,176,939.00RGC COUNTERPART FUNDSRGC-CF for Pooled Funds 8.9 USD Million 8,900,000.00 8,900,000.00RGC-CF for BTC Discrete Fund 2.5 USD Million 2,500,000.00 2,500,000.00TOTAL RGC-CF 11,400,000.00GRAND TOTAL 117,576,93923
PERFORMANCE INDICATOR DASHBOARDPROGRAM INDICATORS BASELINE CURRENTREPRODUCTIVE, MATERNAL, NEWBORN AND CHILD HEALTH FAST TRACK INITIATIVECONTINUUM OF CARE COVERAGEBaseline CurrentInfant mortality rate66 45Neonatal mortality rate 28 27Under 5 mortality rate 83 54Maternal mortality ratio 472 461Total fertility rate 3.4 3Stunting 43 40Wasting 8 11Underweight 28 28Exclusive breastfeeding 66 74Body mass index, women, 15-49 20.3 16.1HIV prevalence rate, 15-49 0.9 0.5TB prevalence all forms per100,000Malaria case fatality rateRoad traffic accidents headtrauma cases treated617 5907.3 4.55NA 39%PROGRAM DEVELOPMENT OBJECTIVE INDICATORS, 20102003 2004 2005 2006 2007 2008 2009 20101 Trained attendance at delivery 22.14 32.97 40.57 35.87 46.00 58.00 63.00 69.602 Deliveries at public health facilities 10.60 16.34 24.14 17.77 25.54 39.00 44.00 52.103 Modern contraceptive method use 18.46 20.03 21.02 22.49 23.64 26.00 28.00 30.004 DPT3-HepB3 vaccinations 73.00 85.00 79.00 80.00 82.00 92.00 95.00 92.005 Pregnant women PMTCT 0.00 0.00 0.00 7.50 11.20 27.00 32.30 57.306 TB cure rate 89.00 90.00 90.00 89.00 87.00 91.00 92.00 92.007 Malaria cases treated per 1,000 10.80 7.50 5.50 7.20 4.20 4.10 5.30 4.078 Vitamin A supplements, 6-59 mos. 39.00 73.50 72.00 78.50 88.00 88.50 100.00 96.009 Pregnant women iron folate 0.00 0.00 0.00 69.00 63.00 69.00 83.00 80.0010 Mebendazole, 12-59 mos. 71.00 86.00 92.00in joint partnership with:24
PROGRAM DEVELOPMENT OBJECTIVES INDICATORS, PROVINCIAL LEAGUENOTE: OPD = OUTPATIENT DEPARTMENT; DTS = DELIVERIES BY TRAINED STAFF; DHF = DELIVERIES AT HEALTH FACILITIES; MMU = MODERN METHOD USE (CONTRACEPTIVES); ANC2 = ANTENATAL CARE, 2 VISITS; IFA = IRON FOLATE SUPPLEMENTS; PMTCT =PREVENTION OF MOTHER TO CHILD TRANSMISSION;25
In a change from the previous report, the provincial league table for Program DevelopmentObjective indicators on the previous page contains data for each indicator for the years 2008-10.This is per the specific request <strong>of</strong> JPIG as approved by the MOH, allowing the reader to tracktrends in performance against targets for the past three years. In some cases, for both targets andindicator values, we have entered ‘NA’ to indicate that the relevant figures are not available.Targets have been derived from the AOP 2010 Mid Year Review and 3 Year Rolling <strong>Plan</strong>s <strong>of</strong> theprovinces, whereas the indicator values have been compiled from the HIS and entered into theprogram database.It should be noted that considerable difficulties were encountered in accessing and verifying HISdata due to the ongoing development <strong>of</strong> the web based database system over the past ninemonths contracted to an external agency. Figures in the database tended to be updated on almosta weekly basis requiring repeated visits to the web site to cross check and download the correctedfigures. The database has been effectively shut down since March, 2011 for further work, but it isexpected that it will be fully functional soon. A fuller discussion <strong>of</strong> developments in respect <strong>of</strong> theHIS is available in Chapter 5 below.Also in response to JPIG’s request, the Annex contains detailed tables for all <strong>of</strong> the PDO indicatorsfor the past three years for provinces and ODs in terms <strong>of</strong> numerators only, thus circumventingthe issue <strong>of</strong> accurate population denominators, whether based on Census 2008 projections, or theCommune Database.Of the 12 PDO indicators presented in the table, achievements <strong>of</strong> three indicators vis-à-vis theirtargets cannot be assessed, since only numerators are available in the HIS database. Theseinclude: OPD
In terms <strong>of</strong> deliveries by trained staff, 13 provinces failed to meet their individual targets, one <strong>of</strong>them, Takeo, by as much as 15 percentage points. Since Takeo’s target was set at 85% (whileachievement was 69.9%) it is likely that the target itself was overly ambitious. The highest levelsachieved for this indicator were 77.5% by Siem Reap and 77.15% by Svay Rieng, and the lowestwere Stung Treng (32.8%) and Kratie (32.9%). Both Ratanakiri and Krong Kep’s achievements werealso low at 35.6% and 39.4% respectively, yet both achieved/exceeded their targets. In general, allprovinces exhibit steadily increasing achievements across the past 3 years with minor variations.Eight provinces failed to achieve their targets for deliveries at health facilities including: KampongChhnang, Kampong Speu, Kandal, Koh Kong, Krong Pailin, Krong Preah Sihanouk, Stung Treng, andTakeo. The target to achievement gap was greatest for Kandal (45.8% achievement versus a target<strong>of</strong> 70%), and Krong Preah Sihanouk (47.1% achievement versus a target <strong>of</strong> 60%). With theadoption <strong>of</strong> rational target setting methods by the sector for the 2012 AOP based on the methodsfirst adopted by the SOAs, it is likely that such enormous gaps will disappear, and targets will bemore realistic and relevant. Similar to the DTS indicator above, in general all provinces show asteadily increasing trend in achievements along with minor variations.Ten <strong>of</strong> 22 provinces (the other two, Krong Kep and Koh Kong did not set any targets) did notachieve their individual targets in terms <strong>of</strong> C-sections. In some cases, the gap is pr<strong>of</strong>oundly high:Stung Treng’s target was 8% versus an achievement <strong>of</strong> 0.5%, and Phnom Penh’s was 7.7 versus anachievement <strong>of</strong> 0.87%. The best performers were Krong Preah Sihanouk at 4.83% considerablyabove its target <strong>of</strong> 3%, and Ratanakiri at 3.22% (against a target <strong>of</strong> 1%). For modern contraceptivemethod use, as many as 15 provinces failed to reach their individual targets. Examination <strong>of</strong> past 3year trends shows that only Kampong Thom shows a steadily declining trend across all 3 yearsfrom 30% in 2008, 27.9% in 2009, and 25.9% in 2010. Both Preah Vihear and Siem Reap showdramatic declines between 2008 and 2009. For Preah Vihear, achievement in 2008 was 35.4%while in 2009 it was only 0.76%. Similarly, for Siem Reap, achievement in 2008 was 21.5% whereasin 2009 it fell sharply to 5.04%. It remains to be investigated whether these declines representdata discrepancies, or genuine declines in current users <strong>of</strong> modern methods.Overall, the sector failed to reach the ANC2 visits target <strong>of</strong> 88%, achieving only 80.3% and this ismirrored in the fact that 17 <strong>of</strong> 24 provinces also failed to reach their individual targets. Despitebeing in a remote location <strong>of</strong> the country, Otdar Meanchey was the highest achiever with 91.2%coverage, a little higher than its ambitious target <strong>of</strong> 90%. In terms <strong>of</strong> the 3 year trends, many <strong>of</strong>the provinces seem to show a decline from the levels achieved in 2009 to those in 2010. OtdarMeanchey and Preah Vihear appear to be the only provinces whose 3 year trends show substantialincrease over the period. Similar to ANC2 visits, 18 provinces failed to achieve their 2010 targetsfor coverage <strong>of</strong> iron folate supplements. Krong Kep was the best performer with 91.1% along withKrong Pailin at 88.6%. A substantial majority <strong>of</strong> the provinces show a decline in achievement from2008 to 2009, although most <strong>of</strong> them seemed to have bounced back in 2010. For prevention <strong>of</strong>transmission <strong>of</strong> HIV/AIDS from mother to child, a uniform target <strong>of</strong> 50% coverage <strong>of</strong> estimatedHIV+ pregnant women was applied across all <strong>of</strong> the provinces. All provinces show a steady orsignificant increase in coverage from 2009 to 2010 per the program’s database. Overall, the sectorachievement was 57.3% against a target <strong>of</strong> 50%.As already noted above, the HIS database now contains only the numerators for DPT3-HepB3, as aresult, achievement against individual provincial coverage targets cannot be determined. For thecountry as a whole, the NHC/JAPR reported an achievement <strong>of</strong> 92% against the sector target <strong>of</strong>96%, and an achievement <strong>of</strong> 95% in 2009. Across the three year period, the number <strong>of</strong> infants29
immunized with DPT3-HepB3 vaccine has steadily increased from 297,510 in 2008 to 298,678 in2009, to 339,911 in 2010. It is possible that the slight decline in coverage rates from 2009 to 2010(95% and 92% respectively) may simply be a function <strong>of</strong> an overestimated populationdenominator based on Census projections. The matter will be investigated after the database isfully functional. Eleven <strong>of</strong> the 24 provinces show slight declines in numbers <strong>of</strong> infants immunized,either from 2008 to 2009 (8 provinces), or 2009 to 2010 (3 provinces).For measles immunization, national achievement was 93% against the sector target <strong>of</strong> 96%, asreported in the NHC/JAPR. This was marginally above the 2009 achievement <strong>of</strong> 91%. The HISdatabase also shows steady increases across the 3 year period from 2008-10, although theachievement <strong>of</strong> 114.1% in 2010 obviously suggests some deficiencies with the populationdenominator used for the calculation (based on Census projections). This issue again will beinvestigated once the database is ready. Only 5 provinces show declines in coverage over the2008-10 period either from the years 2008-09 or from 2009-10 – all others show increasingcoverage. Please note that the Annex contains numerators for this and all other PDO Indicators byprovince and OD for the 2008-10 period as taken from the HIS.There appears to be very high variation across provinces and the 3 year period under review in thenumbers <strong>of</strong> children 6-59 months <strong>of</strong> age provided with Vitamin A supplements. As many as 18provinces show declines, some significant, for the 3 year period, either from 2008 to 2009 or from2009 to 2010. The NHC/JAPR reported a Round 1 achievement <strong>of</strong> 95% and a Round 2 achievement<strong>of</strong> 96% versus a target <strong>of</strong> 98% for both rounds. This was slightly below the 2009 achievement <strong>of</strong>98% for Round 1, and 100% for Round 2.30
PROGRAM DEVELOPMENT OBJECTIVES INDICATORS, OPERATIONAL DISTRICT LEAGURE TABLES31
PROVINCIAL REFERRAL HOSPITALS/SPECIAL OPERATING AGENCIES39
NoPROGRAM PERFORMANCE INDICATORSIndicatorsBaseline2008Target2013Target2010COMPONENT A: HEALTH SERVICE DELIVERY1 OPD all cases 0.54 0.6 0.6 0.58 0.642 OPD under 5 cases 1.1 1.5 1.3 1.0 195,2693 ANC 2 visits 81 94 85 83 289,8914 C-section rate 2 3.2 2.5 1.4 2.035 TB case detection rate>7069(2011)>70 62 666 % <strong>of</strong> people living in highmalaria endemic areas (
NoIndicators8 Number <strong>of</strong> individuals insuredunder CBHI schemes9 Government healthexpenditure per capita (USD)COMPONENT C: HUMAN RESOURCES DEVELOPMENT1 Secondary midwives per10,000 per location:- Country ratio- Provincial average- Provincial medianCOMPONENT D: STEWARDSHIP AND INSTITUTIONSBaseline2008Target2013Target201073,828 NA NA7.77 NA 8.32 8.64 10.511.351.401.74 NA NAAchievement2009 2010 2011 2012 2013130,397 170,4901.341.381.261.321.371.201 Percent <strong>of</strong> external funds forNA* NA* NA* NA* NA*health included in AOPs2 Percent <strong>of</strong> functioning HCMCs NA NA NA NA 100%3 Percent <strong>of</strong> Licensed privatePharmacies and Depots49 89 66 59 944 Percent <strong>of</strong> private entities(polyclinics, consultationcabinets, maternity clinics,56 82 77 72 93dental clinics, etc.) that arelicensedNOTE: *Although this indicator is included in the HSP2 M&E Framework (updated 12 March, 2011) no values are cited; thetarget for 2010 is shown as 100%. The MOH’s Annual <strong>Health</strong> Financing Report 2010 states on page 11 that there are severalconstraints to collecting financial information from health partners, and that figures are only available for two externallyfunded programs: HSSP2, and the Global Fund (GFATM).41
PROJECT MONITORING INDICATORSNoIndicators1 Technical content and results-focus <strong>of</strong> AOP processimproves based on MTR and Final <strong>Evaluation</strong>Baseline2008NATarget2013Improvementsince MTRAchievement2009 2010 2011 2012 2013NANA2 Number and percentage <strong>of</strong> MOH central institutionsand provinces submitting AOP and 3YRPs accordingto schedule and in MOH format79%(2008)95%+ NA 100%3 AOP resource allocation <strong>of</strong> program budgetsreflecting HSP2 and JAPR priorities (1.MCH; 2.CDs;and 3.NCDs)4 Rate <strong>of</strong> Program execution for Government funds pooled DP5 Share <strong>of</strong> operating cost budget reaching contractingODs6 Proportion <strong>of</strong> ODs implementing SDGs and internalcontracting meeting at least 80% <strong>of</strong> theirperformance targetsNA NA MCH: $24.3mill(8.9%)CDC: $52.8 mill(19.4%)NCD: $6 mill(2.2%)NA105%(JAPR 2009)95%95%RGC: 63%DP(HSSP2):41%RGC: 94.8%DP(HSSP2):59%0 40% 100%0 100% NA 9%7 Financial Management Improvement <strong>Plan</strong>developed and implementedNAFMIPimplementedFMIPimplementedFMIPimplemented8 Number <strong>of</strong> MOH staff receiving POC paymentsfinanced by Project.0 NA 0 042
NoIndicators9 Annual health planning summits (JAPR and JAPA)conducted with wide stakeholder participationBaseline2008NATarget2013JAPA and JAPRconductedAchievement2009 2010 2011 2012 2013JAPA and JAPR andJAPRJAPAconducted conducted inMarch, 201110 Percentage <strong>of</strong> HSP2 indicators that have baselines77%83%98%targets69%73%90%11 Selected key HSP2 indicators disaggregated bylocation and sexPHDs: NoSex disagg: NoPHDs: YesSex disagg: YesPHDs: YesSex disagg:NoPHDs: YesSex disagg:No12 <strong>Health</strong> personnel receiving training through theProject (number)NA NA 43,989 20,35913 <strong>Health</strong> facilities constructed, renovated, and/orequipped through the Project.NA NA NA 643
EXPENDITURES TO DATE AND PROJECTED CASH REQUIREMENT FOR NEXT TWO QUARTERS (ALL FUNDS)Funds Receivedto dateFunds Expendedto dateBalance Fundto dateBudget plan forQ1 & Q2, 2011Commitmentamounts tobe paidduring thenext quarterTotal FundsRequiredBudget <strong>Plan</strong>2010 (incl.procurementbroughtforward)Year toDateExpenditure%Actualvs.Budgeta b c = a - b d e f = d+e-c g h i=h/g1. Service Delivery Grants 6,831,521 4,729,312 2,102,209 2,850,735 1,000,605 1,749,131 5,817,609 4,134,503 71%2. HEF Grants (direct benefit cost) 6,655,716 6,544,984 110,733 2,881,694 - 2,770,961 2,819,422 4,132,401 147%3. MBPI and related payment 318,464 270,571 47,893 - - (47,893) - -4. Others - - - - - - - -Goods 4,089,270 1,453,356 2,635,914 573,342 2,796,698 734,127 5,515,189 892,750 16%Works 323,837 278,521 45,316 - - (45,316) 92,000 278,521 303%Services 4,612,663 3,043,157 1,569,506 622,500 667,949 (279,056) 4,701,618 2,212,386 47%Operating Costs 11,689,602 9,304,903 2,384,699 5,025,188 - 2,640,490 8,047,473 5,460,458 68%Training 9,684,028 7,732,330 1,951,698 1,471,011 125,709 (354,978) 6,299,479 4,779,113 76%TOTAL 44,205,101 33,357,134 10,847,967 13,424,470 4,590,961 7,167,465 33,292,789 21,890,133 66%The Interim Financial Report (IFRs) is contained in the Annex.44
14,000,00012,000,00010,000,0008,000,0006,000,0004,000,0002,000,000ReceivedSpent0OVERALL POOLED FUNDS BUDGET PROJECTIONSThe table is yet to be compiled by the Secretariat’s Financial Management unit and will becompleted in the Final Report.2009 2010 2011 2012 2013Budget CategoriesTotal<strong>Plan</strong> Disb <strong>Plan</strong> Disb <strong>Plan</strong> <strong>Plan</strong> <strong>Plan</strong>SDG 1.19 1.40 5.01 3.91 5.01 5.01 5.01 21.44 19%HEF 1.19 1.18 1.97 2.82 3.23 3.23 3.23 12.84 12%MBPI/POC 0.70 0.29 0.5 0.5 1.29 1%Civil Works & 0.46 1.09 0.09 2.96 7 5 3 16.18 15%medical equipmentConsulting Services 2.84 0.6 1.77 3.05 1.7 1.7 1.7 7.47 7%Training 5.15 3.97 5.02 4.56 3 3 3 17.99 16%Operating Costs 5.94 4.34 6.49 5.4 5 5 5 25.83 23%Sub total 12.87 20.85 22.7 25.44 22.94 20.94 103.04 94%Grand totalUnallocated performance based funds 6.96 6%110.00100%45
CHAPTER 1: INTRODUCTION AND BASIC DATA1.1 INTRODUCTIONThis Performance <strong>Monitoring</strong> Report (PMR) is the fourth since the launching <strong>of</strong> HSSP2 in early2009 and covers the 2010 annual reporting period.Following the extensive modifications to the format and contents <strong>of</strong> the Report as contained inthe 2009 Annual Performance <strong>Monitoring</strong> Report which were approved by HSSP2 partners, thisReport contains some additional changes aimed at streamlining the presentation <strong>of</strong> keyinformation: Revision <strong>of</strong> the Indicators contained in the Program’s <strong>Monitoring</strong> and <strong>Evaluation</strong>Framework as originally listed in the Annex to the Program’s Operational Manual basedon consultations with MOH departments, national programs, and central institutions, aswell as with JPIG partners. The main changes arise from the effort to align HSSP2indicators more closely to the HSP2 M&E Framework requiring addition, deletion ormodification <strong>of</strong> existing indicators, and addition <strong>of</strong> a few indicators that are linkedclosely to the Program’s focus. Inclusion <strong>of</strong> an OD League Table in addition to the Provincial League Table for the pastthree years (2008-10); a practice that will now be followed routinely in subsequentreports, allowing readers to identify high and low performers among the ODs for the keyPerformance Development Objective indicators, as well as observe trends over time. Inclusion <strong>of</strong> Provincial and OD league tables in the Annex that cite only the numeratorsfor the key PDO Indicators for the past three years; this allows the reader to ascertaintrends in the key Indicators without the complicating factor <strong>of</strong> possibly inaccuratepopulation denominators, due to overestimates <strong>of</strong> target population growth rates Addition <strong>of</strong> sector reporting and analysis for relevant sections <strong>of</strong> the PMR is drawndirectly from presentations and reports made at the National <strong>Health</strong> Congress and JointAnnual Performance Review conducted on 14-15 March, 2011, and the PreliminaryReport <strong>of</strong> the Cambodia Demographic and <strong>Health</strong> Survey 2010 released in February,2011, as well as IU reports in approved format Comments specific to the PMR that were contained in the Draft Technical Audit Reportsubmitted in February, 2011 have not been included, pending approval by JPIG. JPIG forwarded suggestions in early 2011 for incorporation in future PMRs; JPIG M&Etechnical lead also followed up with a meeting with secretariat staff in March, 2011.Below is a list <strong>of</strong> JPIG suggestions in bullet format, with comments from secretariatregarding compliance in italics:o For data on use modern contraceptives for example, the 2010 JAPR reported havingcollected service utilization data at private sector and NGOs, which could beincorporated into progress reports and JAPR reports. Where available, please includeNGO data.Indicator now includes reporting from RHAC.oInstead <strong>of</strong> presenting the provincial and national average at the bottom <strong>of</strong> the provincialtable, we suggest national hospitals and grand total would be more informative.Complied with.46
We suggest adding results from 2008 and 2009 to this table to enable trend analysis <strong>of</strong>ODs. JPIG is aware there might be s<strong>of</strong>tware and denominator issues and that changes indenominators make it difficult to look at trends accurately. JPIG suggests an annex with3 years’ data by OD with only numbers, not percentages for key indicators.Complied with. % <strong>of</strong> external funds for health included in AOPs: for the annual report please elicitinformation from the sector AOP in 2008, 2009 and 2010 to fill in the data.Data for 2010 have been included; 2008 and 2009 data will be included in the FinalReport. Target Public <strong>Health</strong> Service Provision: it is suggested to include in the format a verybrief summary (one paragraph) on major results beyond the indicators, such as xx policyhas been reviewed and is to be finalized …, YY protocol has been developed and to befinalized by…. in each programme and sub programme. This helps us to understandmore progresses on key policy, strategy, and other important documents in addition tothe results based on indicators.Every attempt has been made to collect such information from IUs for this annual report.Typically, copies <strong>of</strong> key policies or protocols from different IUs at central level are notautomatically made available to the secretariat, as JPIG M&E Technical Lead wasapprised in follow-up meeting. We will continue to try and collect all relevantinformation. Reproductive <strong>Health</strong> Information and Services: The current draft report only shows theabortion component, but in HSP2, there are two more components – family planningand adolescent reproductive health services. Please include these two morecomponents in future reports.Note that the separate report from the RMMP project on safe abortion services fundedby DFID is no longer included since the project has ended. Information on FP and ARHS isincluded with indicator and other reporting. Secretariat has worked closely with NRHPassistant to add relevant information. Maternal and Newborn Services and Family Care Practices: As in the comment on point2.3 above, this section could have a narrative description (max. one paragraph) on safemotherhood protocols, waiting home guidelines, EmONC assessment and improvementplan, etc. in addition to the list <strong>of</strong> indicators, targets and achievements. NRHP canprovide the data for achievement for Indicator # 7 in this section.Information from NRHP has been included. For future reports, JPIG suggests adding a table with the number <strong>of</strong> PRH, ODs and HCswhere HSSP2 pooled and discrete funds support HEF schemes.Complied with Only data on medical staff trained in RTCs is included in the report. In order to see thewhole picture <strong>of</strong> medical staff trained, training at TSMC and at International Universitycould also be included.Information from TSMC has been included; HRD department stated they did not haveany data from IU The performance report says that the HEFs cover 73% <strong>of</strong> the poor population and that 3millions <strong>of</strong> USD has been spent in public health centres. Future semi annual and annualperformance reports could show: the amount paid by CBHI, HEF, and OOP at nationallevel and unit costs by broad category – OPD and IPD the differences in the per capitaconsumption <strong>of</strong> these different categories <strong>of</strong> purchasers. Going towards universalcoverage, the amount <strong>of</strong> money paid by third parties / total amount <strong>of</strong> money receivedby health facilities is an interesting financial indicator:[Amount <strong>of</strong> US dollars paid by CBHI + Amount <strong>of</strong> US $ paid by HEF]-----------------------------------------------------------------47
[Amount <strong>of</strong> US dollars paid by CBHI + Amount <strong>of</strong> US $ paid by HEF + User fees + other cashmoney received]HEF section has been expanded with additional information and graphs designed by M & E unitand completed by HF adviser; additional information will be forthcoming in future reports. CDHS data: this is now available and can be included in the progress report.Relevant information from the CDHS 2010 Preliminary Report has been included in section onOverview <strong>of</strong> Sector Progress.48
SECTION B: PROGRAM IMPLEMENTATION PROGRESS49
CHAPTER 2: STRENGTHENING HEALTH SERVICE DELIVERY2.1 EXPAND COVERAGE OF MPA AND CPA BASED ON HEALTH COVERAGE PLANAND CLIENT NEEDSBy December, 2010 the health coverage plan showed a total <strong>of</strong> 77 ODs, HCs increase from 984in 2009 to 997 in 2010, HPs increase from 111 in 2009 to 117 in 2010. It is expected that thenumber <strong>of</strong> HCs will increase to 1023 in 2011. 10 HCs in Kandal province have been handedover to Municipality <strong>of</strong> Phnom Penh according to new provincial administrative arrangement.There are currently 89 Referral Hospitals including 8 nationals <strong>of</strong> which CP3 (26), CPA2 (30)and CPA1 (33).2.1.1 PROGRESS OF CIVIL WORKSJPIG has approved civil works budget as follows:Proposed Prioritization According to EmONC <strong>Plan</strong>1. Additional Delivery Rooms (79) 790,000.002. EmONC at ODs 200,000.003. EmONC at RHs 3,135,000.004. RTCs 2,955,000.00 Cost for 2 only5. Water and electricity 2,000,000.006. New HC construction (100) 6,500,000.00Total Construction and Upgrading 15,580,000.00Total scope for design contract16,570,000.00 Includes all 4 RTCcostsAfter very careful assessment MOH has proposed construction <strong>of</strong> 102 HCs, 6 HPs, RTCBattambang and RTC Stung Treng starting from 2011 while the construction/renovation <strong>of</strong>RHs and water supply and sanitation could be started from 2012. The detailed names <strong>of</strong>facilities and civil work plan are in the Annex.The civil works completed under HSSP1 in 2010 are listed below:50
SUMMARY LIST OF DISBURSEMENT ON CWsDescription <strong>of</strong> Consturction Contract price Variation Disbursed Final Costs Completion % Contract Balance*Contract No.HSSP/WB/ICB/CW/Phase 2-Lot 2/07-Rebid (Mohaprum Co., Ltd.O Chrouv RH 1,061,939.40 1,063,795.07 1,063,795.07 100% (1,855.67)*Contract No.CAKH088 (Lot 4B) (Mohaprum Co., Ltd.(Sampov Meas RH , Pursat Province) 403,588.36 396,292.60 396,292.60 100% 7,295.76*Contract No. CAKH088 (Lot 2B), (Kim Mex)Stung Treng RH 1,180,218.30 24,230.07 1,204,448.10 1,204,448.10 100% 0.27*Contract No. CAKH088 (Lot 1B), (Kim Mex)Kampot RH 1,237,596.33 20,196.54 1,257,792.87 1,257,793.52 100% (0.65)*Contract No.HSSP/WB/NCB/CW/Preah Vihea/10 (Kry Huy)Temporary Surgical Facility for Tbeng Meanchey 71,176.31 RH (PVH) 5,033.00 75,853.93 75,853.93 100% 355.38*Contract No.HSSP1-CKP-NCB-W001(Kry Huy)Kulen HC 41,912.74 40,561.46 40,561.46 100% 1,351.28Chrach HC 56,785.05 12,729.53 22% 44,055.52Kampong SraLoa HC 44,561.73 15,571.45 35% 28,990.28Kdak HP 19,980.10 18,300.46 18,300.46 100% 1,679.64Thnal Koang HP 18,696.02 17,473.54 17,473.54 100% 1,222.48Sre Veal HP 20,180.10 3,435.93 17% 16,744.17Ta Bors HP 20,180.10 2,898.90 14% 17,281.20Bang Korn HP 20,180.10 0.00 0% 20,180.10*Contract No.HSSP-CKP-ICB-W002 (Borei kamkor)Tbeng Meanchey RH 2,009,063.57 524,364.98 26% 1,484,698.59CONSTRAINTSProcurement <strong>of</strong> medical equipment for newly built RHs needs to be expeditedConstruction <strong>of</strong> 3 HCs and 5 HPs as a whole is lagging behind schedule; 1 HC and 2 HPshave been handed over to end usersThe onset <strong>of</strong> rainy season may slow down construction in Preah Vihear requiringinvocation <strong>of</strong> liquidated damagesThe have been some slight delays in the submittal <strong>of</strong> updated and accurate constructionprograms from contractorsClashes between Thai-Cambodian troops in Preah Vihear in February 2011 have causedconcern about retention <strong>of</strong> foremen, workers, and casual labor at isolated sites2.2 STRE NGTHE N HE A LTH SE RV ICE DE LIVE RY SU PPORT SYSTEMS IN AN INTE GRA TED MANNE RINTEGRATED SUPERVISIONThe table below reports on integrated supervision (ISC) activities conducted during the 1 stsemester. As can be seen, a total <strong>of</strong> 501 visits were conducted from PHDs to ODs versus 586,101 visits from PHDs to RHs versus 182 planned and 4,204 visits from ODs to HCs versus 4,902planned. Detailed reasons with explanations for under-achievement <strong>of</strong> numbers <strong>of</strong> visitsplanned are listed in the “Comments” column below.51
NoDescriptionPHD to ODs PHD to RHs OD to HCs<strong>Plan</strong> Ach <strong>Plan</strong> Ach <strong>Plan</strong> AchCommentISC Supervision1BanteayMeanchey24 12 24 12 636 636Team <strong>of</strong> other programswere busy with othertasks outside province2 Battambang 30 18 24 14 900 8443 Kg Speu 18 15 18 9 600 6004 Kg Thom 9 9 9 9 600 5505 Kampot 24 8 24 8 612 4556 Kep 6 2 36 27PHD staff busy with WS &meetings. OD team hasno problem, but reportingfrom OD supervision waslateLack <strong>of</strong> Budget forSuperv,Team was busywith other tasks outsideprovince.Lack <strong>of</strong> Budget, Members<strong>of</strong> team have many othertasks and missions.Members <strong>of</strong> team werebusy with lot <strong>of</strong> workmissions7 Kratie 12 2 12 2 276 187 Team was busy withdiarrhea outbreak8 Odor Meanchey 24 10 216 180Members <strong>of</strong> team had alot <strong>of</strong> roles and missions9 Pailin 6 6 72 36 Lack <strong>of</strong> budget forSupervision10 Pursat 12 10 12 12 384 28811 Preah Vihear 6 3 6 4 168 37Lack <strong>of</strong> Budget forSuperv,Team was busywith other tasks outsideprovince.Lack <strong>of</strong> Budget, Lack <strong>of</strong>competent humanresources12 Stung Treng 6 NA 168 30 Members <strong>of</strong> team had alot <strong>of</strong> roles and missions13 Kg. Cham 6 6 6 6 1,548 1,548Time constraint inimplementation <strong>of</strong> AOPactivities, therefore someactivities have not beendone14 Kg. Chhnang 18 18 18 16 482 453 Not as planned due to theA/H1N1 campaign in the1st quarter15 Kandal 0 0 0 0 0 016 Koh Kong 12 11 5 4 0 0ISC activities were notincluded in 2010 AOPMembers <strong>of</strong> Teams had alot <strong>of</strong> duties andgeographical factors aswell52
17 Mondulkiri 4 3 4 3 48 35 During the rainy season,roads were difficultISC activities wereincluded but notapproved in 2010 AOPand the ISC activities18 Phnom Penh 24 24 6 6 126 60 carried out but notfunded by HSSP2. SomeODs had no activities <strong>of</strong>ISC, because HC managershad been changed.19 Preah Sihanouk 0 0 108 97 No time due to being busywith MCH Survey andA/H1N1 CampaignLack <strong>of</strong> <strong>of</strong>ficials and20 Prey Veng 42 18 21 12 676 592inadequate time. Budgetapproval is not followingAOP.PBB budget used andHSSP2 budget not21 Ratanakiri 0 0 0 0 132 118approved for PHD to HCs.Not achieved as planneddue to business withcholera outbreak22 Siem Reap 4 3 4 3 816 81623 Svay Rieng 18 18 18 18 456 45624 Takeo 30 11 30 11 316 146Total 24 PHDsISC293 189 283 167 9,376 8,191ISC activities were carriedout but not funded byHSSP2Many meetings andworkshops <strong>of</strong> NationalPrograms requiringpostponement <strong>of</strong>provincial plans wheninvitations arrived, andoverlap <strong>of</strong> schedule forAH1N1 vaccinationcampaignISC members had severalother tasks and timesand teams were notaltogether.Please note that program-specific supervision visits were carried out separately as well,although they are not reported here.2.3 TARGE T PU BLIC HE A LTH SE RV ICE PROVISION AND PU BLIC HEALTH INTERVENTIONSACCORD ING TO NEED2.3.1 REPRODUCTIVE, MATERNAL, NEONATAL, AND CHILD HEALTH2.3.1.1 NUTRITION OF WOMEN AND CHILDRENMain financial support for the nutrition programs for 2010 were from the 2 nd <strong>Health</strong> SectorSupport Program (HSSP2) and the MDG-F Joint Program for Children, Food Security andNutrition in Cambodia thought UNICEF and WHO, plus support from FAO, USAID and NGOs(RACHA, HKI, RHAC, WVC, IRD, VSO, MAGNA, URC, SHARE, SP, GRET, Malteser International,and etc). The total budget <strong>of</strong> the NNP Annual Operational <strong>Plan</strong> (AOP) for 2010 was aroundtwo millions dollars. Of this total amount, ~ USD 700,000 was from HSPP2 and ~ USD 1.353
million from MDG-F. Most <strong>of</strong> activities planned in 2010 were implemented. Highlights andachievements <strong>of</strong> 2010 included:• Launch <strong>of</strong> the first National Nutrition Strategy 2009-2015 in May. Participants includedrelevant government partners from national, provincial and operational district level anddevelopment partners.• Launch <strong>of</strong> the National Communication Strategy to Promote the Use <strong>of</strong> Iron/Folic AcidSupplementation for Pregnant and Postpartum Women: 2010-2013 in September andthe implementation started in October.• Launch <strong>of</strong> the MDG-F Joint Program for Children, Food Security and Nutrition inCambodia in June 2010.• Completion and dissemination <strong>of</strong> results <strong>of</strong> the Good Food for Children study(Combating Anemia and Micronutrient Deficiencies among Young Children in RuralCambodia through In-home Fortification and Nutrition Education) in October.• Development <strong>of</strong> the National Interim Guidelines for the Management <strong>of</strong> AcuteMalnutrition throughout 2010.• Development <strong>of</strong> Training Materials for the Management <strong>of</strong> Acute Malnutritionthroughout 2010.• Development <strong>of</strong> Initial Implementation <strong>Plan</strong> for the Management <strong>of</strong> Acute Malnutritionin July-August and the commencement <strong>of</strong> the initial implementation <strong>of</strong> the Management<strong>of</strong> acute malnutrition in late September.• Development <strong>of</strong> the (Draft) National Policy and Guidelines for the MicronutrientSupplementation to Prevent and Control Deficiencies in Cambodia in November.• Update <strong>of</strong> the National Communication Strategy to Promote Vitamin A to cover newperiod <strong>of</strong> 2011-2015 started in September.• Development <strong>of</strong> the Communication for Behavioral Impact (COMBI) Campaign toPromote Complementary Feeding in Cambodia: 2011-2013 started in 2008 and thefinalized in 2010.• Approval for the introduction <strong>of</strong> MSc in Nutrition under the National Institute <strong>of</strong> Public<strong>Health</strong> (NIPH) in late 2010. The <strong>Ministry</strong> <strong>of</strong> <strong>Health</strong> (MoH) has agreed and has formed aWorking Group to establish a master program in nutrition in Cambodia under the NIPH.A consultant supported by WHO has drafted a proposal and curriculum for MSc inNutrition for Cambodia in November and December.NoCore PerformanceIndicatorAchievement2007Achievement2008Achievement2009Achievement2010Target20111 Number/proportion <strong>of</strong>Baby Friendly Hospitals7(cumulative)7(cumulative)9(cumulative)10 152 Number/proportion <strong>of</strong>Baby FriendlyCommunities (based on14,000 villages)2,787 villages(cumulative)21%3,038 villages(cumulative)23%3,700 villages(cumulative)26%4,421(cumulative)32%3503 Vitamin A coverage forchildren 6-59 months88% (R1 100%& R2 76%)89% (R1 88%,& R2 89%)99% (R1 98%& R2 100%)96% (R1 95 &R2 96 )R 98% & R298%)4 Vitamin A coverage forpostpartum mothers60% 68% 71% 73% 78%54
within 6 weeks afterdelivery5 Iron/Folic Acid coverage<strong>of</strong> pregnant women (90tablets)6 Iron/Folic Acid coverage<strong>of</strong> postpartum women(42 tablets)63% 69% 83% 80% 85%45% 53% 68% 73% 78%7 Number or proportion <strong>of</strong>health centers trained inMPA10 (based on 966HCs)575= 60%(cumulative)690= 71%(cumulative)722= 75%(cumulative)788= 82%(cumulative)100%8 Number <strong>of</strong> referral andnational hospitalsmanaging <strong>of</strong> severemalnutrition9(cumulative)15(cumulative)20(cumulative)29(cumulative)299 Number <strong>of</strong> health centersimplementingmanagement <strong>of</strong> acutemalnutritionN/A N/A N/A 5(InitialImplementation)24CONSTRAINTSThe NNP continued to be very busy with the expansion <strong>of</strong> existing nutrition interventions andmany new initiatives and developments in 2010. Insufficient qualified staff has continued tobe a big challenge for the NNP to match the current and future workload. Two majordevelopments in 2010 that have taken a lot <strong>of</strong> time and effort <strong>of</strong> the NNP staff were:- The development <strong>of</strong> the National Interim Guidelines, Training Materials and the InitialImplementation for the Management <strong>of</strong> Acute Malnutrition- The development <strong>of</strong> the National Policy and Guidelines for the MicronutrientSupplementation to Prevent and Control Deficiencies in Cambodia in NovemberSome specific constraints included:• IFA coverage (80% for 2010) was lower than target set for 2010 (83%) and lower than2009. Vitamin A coverage has also slightly decreased. The following are some seasonswhy IFA coverage has decreased:• Some health centers did not distribute IFA during outreach sessions because they wantedto encourage pregnant women to attend ANC at health center.• There might be some problem with numerator, denominator and the expected pregnancyin total population (2.56% <strong>of</strong> total population), especially with the new findings from 2008Census.• Recording and reporting <strong>of</strong> IFA distribution for pregnant women in hospital has not beenincluded in hospital reporting; HO2 form.55
• New MPA 10 provinces did not have enough funding to conduct the training <strong>of</strong> healthcenter staff, despite the effort to strengthen annual operational planning in nutrition atnational and sub-national. As a result, the target set for the training <strong>of</strong> MPA 10 was notmet.• Recording and reporting <strong>of</strong> nutrition activities were still problematic; very slow to get thereport from the HIS on vitamin A and iron/folic acid coverage and difficult to get thecorrect number <strong>of</strong> villages implementing BFCI.NEXT STEPSThe NNP has achieved most <strong>of</strong> its objectives set out in the 2010 AOP. All <strong>of</strong> the studies wereconducted as planned and reports were prepared and shared with key partners. New policies,guidelines and strategies were developed and disseminated.• Conduct an assessment <strong>of</strong> the Initial Implementation <strong>of</strong> Management <strong>of</strong> AcuteMalnutrition.• Use findings from the assessment to revise the National Interim Guidelines and TrainingMaterials for the Management <strong>of</strong> Acute Malnutrition. Expand the management <strong>of</strong> acutemalnutrition program to 19 new health centers.• Finalize the National Policy and Guidelines for the Micronutrient Supplementation toPrevent and Control Deficiencies Among Women and Children in Cambodia. Use this newpolicy and guidelines to expand MNPs in two provinces; kampong Speu and Svay Riengand expand WIFS in six provinces; Kep, Kampot, Kampong Speu, Kampong Thom, Pursatand Svay Rieng.• Continue to work National Center for <strong>Health</strong> promotion and development partners todevelop IEC/BCC materials for the Communication for Behavioral Impact (COMBI)Campaign to Promote Complementary Feeding in Cambodia: 2011-2013. The launch andimplementation <strong>of</strong> the campaign will be conducted in July.• Develop new indicators for the new three nutrition interventions to be incorporated intothe HIS; Management <strong>of</strong> Acute Malnutrition, MNPS and WIFS. Develop Tally Sheets andReporting Forms for all levels and pilot using these recording and reporting forms in twoprovinces; Kampong Speu and Svay Rieng.• Continue to work as a member <strong>of</strong> the MOH Working Group on MSc in Nutrition under theNational Institute <strong>of</strong> Public <strong>Health</strong> (NIPH).• Develop training package and job aids for all micronutrient supplementation programs tobe incorporated into the MPA 10 training materials.• Finalize the revision <strong>of</strong> the National Communication Strategy to Promote Vitamin A anddevelop IEC/BCC materials needed for the implementation <strong>of</strong> this communicationstrategy.• Continue to work with the Department <strong>of</strong> Drugs and Food and other line ministries toimplement the Joint Prakas on the Implementation <strong>of</strong> the Sub-decree on Marketing <strong>of</strong>Products for Infant and Young Child Feeding. Conduct two meetings to review theimplementation and enforcement <strong>of</strong> the sub-decree.• Continue to implement the National Communication Strategy to Promote the Use <strong>of</strong>Iron/Folic Acid Supplementation for Pregnant and Postpartum Women: 2010-2013• Participate in the Mid-term Review <strong>of</strong> the Strategic Framework for Food Security andNutrition in Cambodia 2008-201256
2.3.1.2 REPRODUCTIVE HEALTH INFORMATION AND SERVICES2.3.1.3 MATERNAL AND NEWBORN SERVICES AND FAMILY CARE PRACTICESNATIONAL REPRODUCTIVE HEALTH PROGRAMIn 2010, the National Reproductive <strong>Health</strong> Program (NRHP) had implemented the majorevents which planned in the Annual Operational <strong>Plan</strong> (AOP). Those events included in thetraining activities for the provincial trainers, meetings and workshop:Training activities:- Training <strong>of</strong> Trainers on Implant for PHD MCH staff for all 24 provinces- Training <strong>of</strong> Trainers on PNC Packages- Training <strong>of</strong> Trainers on IPPC- Training on IUD insertion- Training <strong>of</strong> Trainers for Physician on EmONC- Training <strong>of</strong> Midwifes on EmONC (One month)- Training <strong>of</strong> Physician on EmONC (Three months)- Training for Physician on how to use Manual Vaccum Extractor- Training for Midwife on how to use Manual Vaccum Extractor- Training <strong>of</strong> Trainers <strong>of</strong> CBDMeeting/Workshop:- Workshop to review the achievement <strong>of</strong> the National Reproductive <strong>Health</strong> Program forthe first six months <strong>of</strong> 2010- Workshop to develop the Annual Operational <strong>Plan</strong> 2011 <strong>of</strong> the National Reproductive<strong>Health</strong> Program- Dissemination workshop on the EmONC improvement <strong>Plan</strong> at the provincial level- Meeting to update the Safe Motherhood Protocol for <strong>Health</strong> Center- Preparation ceremony <strong>of</strong> the Cambodia Midwife Association 2010- Sub-TW Meeting for Maternal and Child <strong>Health</strong>- Workshop to review the Checklist for the Adolescent and Reproductive <strong>Health</strong>- National Symposium for the Maternal and Child <strong>Health</strong>- Workshop on <strong>Monitoring</strong> and <strong>Evaluation</strong> on EmONC- Dissemination workshop on Safe Motherhood Protocol for <strong>Health</strong> Centers andNational Waiting Home guidelines- Meeting on the Cambodia Midwife Association committees- High Level Midwifery Taskforce Meeting and the secretariat meeting- CBD Dissemination WorkshopNo12INDICATORContraceptivePrevalence Rate(Modern Method)Two and moreantenatal careconsultationQuarter 1 Quarter 2 Quarter 3 Quarter4 ANNUALTarget Ach Target Ach Target Ach Target Ach Target AchNA NA NA 29.32% NA NA NA 45% 29%NA NA NA 38.45% NA NA NA 85% 83%57
34Delivery by healthtrained providerDelivery by trainedhealth provider inhealth facilitiesNA NA NA 27.97% NA NA NA 70% 63%NA NA NA 24.22% NA NA NA 50% 53%5 Delivery by C-section NA NA NA 0.68% NA NA NA 2.50% 1%67% <strong>of</strong> public healthfacilities provide safeabortion 93/967% <strong>of</strong> public healthfacilities provideADSRH services41/967NA NA NA56%-RH11%-HCNA NA NA82%-RH11%-HC5%82%-RH11%-HCNA NA NA NA NA NA 5 5%CONSTRAINT AND NEXT STEPS• Printing <strong>of</strong> documents to share with health centers has been delayed• There were too many TOT training workshops at national and PHD levels which adversely affected monitoand supervision activities from the national level to HCs• Incentives for government staff were not available throughout the yearPREVENTION OF MOTHER TO CHILD TRANSMISSION (PMTCT PROGRAM)NoINDICATOR1 Number <strong>of</strong> Pregnantwomen who received HIVtest and received theirresult.2 Number <strong>of</strong> pregnantwomen whose testare positive.3 Number <strong>of</strong> known HIVpositive pregnant womenwho are referred forPMTCT.4Number <strong>of</strong> delivered HIVpositivemothers whoreceived ARV for PMTCT.5 Number <strong>of</strong> babies born toHIV infected mothersreceived ARV prophylaxisfor PMTCT.6 % <strong>of</strong> HIV infect-mothersreceived ARVtreatment/prophylaxis forPMTCTQuarter 1 Quarter 2 Quarter 3 Quarter 4 ANNUALTarget Ach Target Ach Target Ach Target Ach Target Ach26,500 27,531 29,000 29,789 31,500 32,176 34,000 50,893 121,000 140,389100 112 100 114 100 143 100 119 400 488120 119 120 93 120 116 120 104 480 432175 164 175 171 175 192 175 205 700 732175 171 175 183 175 196 175 198 700 7481 158
CONSTRAINTS1 Different data forms given to the HF create double work for the staff at primary levels.2 While PMTCT services are more available in HC and RH, report to be collected becomeslower than before. This means that it takes time for the MCH manager collect informationfrom the HFs.3 Data form from NCHADS and from NMCHC will put together into only one form. So that staffinter data only one time.2.3.1.4 CHILD HEALTH SERVICES AND FAMILY CARE PRACTICESNATIONAL IMMUNIZATION PROGRAMNoINDICATORQuarter 1 Quarter 2 Quarter 3 Quarter 4 ANNUALTarget Ach Target Ach Target Ach Target Ach Target Ach1 BCG 24.50% 25% 24.50% 23% 24.50% 22% 24.50% 24% 98% 94%HepB birth dose2 95% coverage) Reduce HepB prevalence to 80% PAB for TT) Over 90% DTP-HepB-Hib coverage every district by 2015 Identify high risk groups and reduce immunization drop out through micro planning12. Improved vaccine management through training activities59
2.3.2 COMMUNICABLE DISEASES2.3.2.1 DENGUESince the beginning <strong>of</strong> this year, 2010 the dengue situation is quiet better than last previousthree years, but a little bit higher than last year 2009. During the 1 st three months (week 1-12), the dengue situation is more or less stable and after that up to week 26 ( around April,May and June ), the overall dengue situation are more safe. The number <strong>of</strong> dengue suspectedcases by week were jumping up 1.1 to 1.4 times and always over the lower limit ( the casesare over the 5 years mean: LLL) : alert situation and got a peak level by touching the 5 yearsmeans + 2 Standard deviation line ( the ULL), on week 31 (July). During 2010 period, thesuspected dengue cases reported and admitted at Public <strong>Health</strong> facilities were 12,500 cases inwhich with 38 died ( case fatality rate: 0.3%). If we compared with last year, 2009 with thesame period only 11,699 cases in which with 38 died. In 2010, during the first quarter, theaverage per month was only 157 dengue and dengue haemorrhagic fever, but these levels <strong>of</strong>infection are jumping up to three to four fold times every quarter. In the 2 nd quarter theaverage number <strong>of</strong> cases was reported from April to June were 737 cases per month. Thepeak <strong>of</strong> cases occurred in week 31 ( end <strong>of</strong> July), when 835 cases were reported (Graph 2).The incidence per 100,000 population during 12 months period was 89.10 that was littlehigher than last year 2009 (83.40 per 100,000 population) but five times lower than 2007 (437per 100,000 population). However, we observed some dengue outbreaks have been occurredat urban, suburban and rural remotes areas in some provinces like: Battambang - Siem Reap-Phnom-Penh City- Kandal- Kg Cham- Kg Chhnang- Kg Thom- Kampot- Kep- Takeo- PrahSihanouk- Prey Veng- Banteay Mean Chey- Kg Speu- Oddor Mean Chey- Svay Rieng- Pursat-Koh Kong- Prah Vihea Provinces (Map1).60
Cases NumberCFR (%)Cumulative Incidence <strong>of</strong> Dengue cases byDistrict in Cambodia 2010Distribution <strong>of</strong> Dengue Reported Cases & Cases Fatality Rate by Age and Gender,Cambodia-2010 (52 weeks, n=12500/38)Female Male CFR300025000.4273625270.50.450.4200015001996 20060.3146814900.40.350.30.250.210005000.11111660.150.10.050≤4 ys 5 to 9 ys 10 to 14 ys 15+Age groups0MONITORING INDICATORSNoINDICATOR1 Dengue incidence rateTarget< 70 per100.000ANNUALAchieved89.1 per 100,0002 Dengue case-fatality rate 0.80% 0.30%For better control the situation specially during the transmission season, the National DengueControl Programme under the strong support from MOH and WHO, and financial supportfrom ADB_CDC2 and HSSP2_Pooled Fund, closely collaboration with all high risk dengue61
Provincial <strong>Health</strong> Departments, Operational Districts with strong commitment from <strong>Health</strong>Centers staff, carried-out rapid community-based vector control response activities( investigation, health education/ mobile health education, sources reduction, larviciding andULV space spraying if needed). The aim <strong>of</strong> the rapid intervention is to identify the nature <strong>of</strong>the outbreak, containment and reduce the speed <strong>of</strong> dengue transmission, slow down dengueincidence and reduce case-fatality rate.Dengue supervision is one essential dengue tool for better management and efficientlymonitor <strong>of</strong> dengue situation before, during and after dengue outbreak. This strategy can allowus to go around and monitor to the high risk localities <strong>of</strong> each provinces, specially high riskprovinces such as high population density localities, former dengue outbreak localities. theNational Dengue Control Programme, under the financial support from HSSP2_Poleed Fund,has been conducted dengue supervision in some high risk and outbreak provinces such asBanteay Mean Chey, Kg Cham, Kandal, Prey Vaeng, Prah Sihanuok, Svay Rieng, Kampot, SiemReap, Pursat, Kg Thom, Kg Chhnang, Takeo, Stung Traeng, Kg Speu, Kratie, Battambang andOddor Mean Chey provinces.To make sure on availability <strong>of</strong> drugs and Insecticide at all provincial levels, the NationalDengue Control Programme in collaboration with the Central Medical Store, MOH have beenprepared list for drugs and insecticide supplies and sent to all 24 Provincial <strong>Health</strong> Departmentper Table below:Provinces1RAbate Quantity(Kg)1R BTI Quantity(kgs)2RAbate Quantity (Kg)Alpha Cypermethrine10% (1L)1 Phnom-Penh 5,000 14,000 502 Kg Cham.. 3,500 1,500 503 Kandal 2,700 504 Siem Reap 7,000 8,000 405 Banteay Mean Chey 8,000 8,000 306 Battambang 7,300 6,700 307 Pailin 1,200 1,2508 Otdar Mean Chey 1,800 1,8009 Pursat 6,200 3,00010 Kg Chhnang 1,300 1,300 3011 Kg Thom 2,700 0 3012 Preah Vihear 2,600 2,600 3013 Prey Veng 12,000 0 5014 Kg Speu 6,300 7,000 3015 Preah Sihanuok 1,300 2,00062
16 Koh Kong 2,200 2,500 3017 Ratanakiri 1,900 0 3018 Mondolkiri 1,00019 Stung Treng 1,800 0 3020 Takeo 9,200 4,000 5021 Kampot 6,100 3,000 5022 Kep 1,000 1,00023 Svay Rieng 4,800 4,000 3024 Kratie 3,200 3,200 3025 National Program 5,000 120Total 102,400 2,500 74,850 600CONSTRAINTS Fund not enough to cope with the overall dengue situation, No or not adequate equipment and supplies for surveillance system ( computers,phone, Fax machines) and clinical management monitoring, specially at intensive careunits <strong>of</strong> Provincial Referral Hospitals ( CBC machines, vital signs monitoring machines,Centrifuge machines, Blood Pressures (at least up to HCs level, etc) Not enough reagents for lab and Rapid diagnosis tests (PANOIO tests) to supportinvestigation activities, during dengue epidemic,o Not enough resource persons for data collection and management, HE coverage still low for community and school-based (TV/radio broadcasting, IECmaterials production). Less supervision/Follow-up activities for HE ( school-community-based), surveillancesystem and clinical management, The application <strong>of</strong> IVM as rapid response activities in some localities <strong>of</strong> some dengueoutbreak provinces not properly done on-time. In some localities, less or no participation/responsibility from local authority/parents.NEXT STEPS Funds should be increased so as to cover all dengue strategy/ activities for effectiveprevention and control Equipment and supplies for surveillance system and for clinical managementmonitoring should be available and enough Reagents for lab and Rapid diagnosis tests (PANOIO tests) have to supply supportinvestigation activities, during dengue epidemic63
Resource persons for data collection and management should be trained andmotivated them HE coverage should be extend to all or at least cover high risk community and schoolbased(TV/radio broadcasting, IEC materials production) Supervision/Follow-up activities for HE ( school-community-based), surveillancesystem and clinical management should be improve The allocation <strong>of</strong> some budget as a package for rapid response activities as IVMstrategy should be considered2.3.2.2 HELMINTHSNo123456INDICATORNumber new Lymphaticfilariasis case stay athospital per year% <strong>of</strong> school age childrenreceive deworming tablets% <strong>of</strong> children aged 23-59months receive dewormingtablets% <strong>of</strong> pregnant women in >2nd trimester and lactatingwomen get dewormingtabletsThe prevalence <strong>of</strong> S.mekongi in endemic areas% <strong>of</strong> eligible populationreceived Mass drugadministration inschistosomiasis endemicareasQuarter 1 Quarter 2 Quarter 3 Quarter 4 ANNUALTarget Ach Target Ach Target Ach Target Ach Target Ach0case100%1case100% 0case 100% 1case 100%2cases100%42% 100% 50% 100% 22% 100% 70% 100% 92% 100%15% 100% 70% 100% 15% 100% 70% 100% 85% 100%25% 85% 25% 91% 25% 94% 25% 82% 87% 100%
IntroductionIn 2010 there were a total <strong>of</strong> 30 Special Operating Agencies (SOAs), including 22 operationalDistricts and 8 Provincial Referral Hospitals. The table below shows the status <strong>of</strong> each SOA in2010.No. OD/RH Pop. 2010SDG /Capita($US)ContractMOH-PHDContractPHD withPRH or ODSDGImplementationDate(SDG) 12monthscontractbudget65ReceivedAdvancePayment1.Kampong Cham1 Kg. Cham PRH 285,406 NA4-Aug-09 1-Jan-10 385,885.00 yes2 Memut OD 135,316 1.24 24-Jul-09 1-Jul-09 166,325.00 yes3 Punhea Krek OD 216,132 1.24 24-Jul-09 1-Jul-09 252,226.00 Yes1-Apr-094 Cheung Prey OD 199,816 1.24 28-Jul-09 1-Jan-10 241,752.00 yes5 Chamkar Leu OD 163,856 1.24 28-Jul-09 1-Jan-10 199,112.00 yes6 Prey Chhor OD 187,959 1.24 31-Dec-09 1-Jan-10 232,000.00 yes2.Takeo7 Ta Keo PRH na Na7-Jul-10 1-Jun-10 200,000.00 yes8 Daun Keo OD 219,515 1.24 9-Jul-10 1-Jun-10 217,759.00 yes9 Prey Kabas OD 161,667 1.24 9-Jul-10 1-Jun-10 200,467.00 yes1-Apr-0910 Baty OD 198,970 1.24 7-Jul-10 1-Jun-10 246,723.00 yes11 Kirivong OD 229,475 1.24 16-Jul-09 1-Jul-09 276,633.00 yes12 Ang Rokar OD 139,231 1.24 16-Jul-09 1-Jul-09 168,262.00 yes3. Koh Kong13 Koh Kong PRH24-Jul-09 1-Aug-09 81,647.00 yes14 Smach Meanchey OD 57,570 3.28 1-Apr-09 24-Jul-09 1-Aug-09 122,471.00 yes15 Sre Ambel OD 59,911 3.28 24-Jul-09 1-Aug-09 254,075.00 yes4. Ratanak Kiri16 Ratanakiri PRH28-Jul-09 1-Aug-10 96,711.00 yes1-Apr-0917 Ban Lung OD 158,674 3.52 28-Jul-09 1-Aug-10 145,066.00 yes5. Mondul Kiri18 Mondulkiri PRH24-Jul-09 1-Oct-09 95,935.00 yes1-Apr-0919 Sen Mnorum OD 62,818 4.64 24-Jul-09 1-Oct-09 186,228.00 yes6. Preah Vihear20 Preah Vihear PRH17-Jul-09 1-Oct-09 209,892.00 yes1-Apr-0921 Tbeng Meanchey OD 177,317 3.51 17-Jul-09 1-Oct-09 391,650.00 yes7. Otdar Meanchey22 Otdar Meanchey PRHand Anlong Veng RH21-Oct-0921-Apr-10 1-Jan-10 116,000.0023 Samrong OD 219,316 2.65 23-Oct-09 1-Jan-10 580,000.00 yes24 8. Siem Reap24 Siem Reap PRH9-Apr-10 1-Jan-10 191,620.00 No25 Siem Reap OD 303,383 1.24 9-Apr-10 1-Jan-10 338,575.00 No26 Sotnikum OD 292,860 1.24 1-Oct-09 20-Apr-10 1-Jan-10 360,000.00 No27 Angkor Chum OD 218,889 1.24 20-Apr-10 1-Jan-10 271,422.00 No28 Krolanh OD 127,104 1.24 9-Apr-10 1-Jan-10 157,609.00 No.9. Prey Veng29 Preah Sdach OD 119,180 1.2414-Jul-09 1-Jul-09 146,470.00 yes30Pearaing OD 201,710 1.241-Apr-0914-Jul-09 1-Jul-09 239,401.00yes30 SOAs 4,136,075 9 contracts 20 13 6,771,916.00 -
Service Delivery Grant Allocations to SOAs, 2010-11The table below shows the SDG allocations by SOA for the years 2010 and 2011. Theallocations were based on a review and revision <strong>of</strong> the original formula, and extensivediscussions with JPIG. AFD accorded its approval on 2 March, 2011 while World Bank accordedits approval on 16 March, 2011.No SOA 2010 (USD) 2011 (USD)1 Memut OD 169,326 177,7922 Punhea Krek OD 268,000 254,6003 Cheung Prey OD 250,000 237,5004 Chamkar Leu OD 200,000 200,0005 Prey Chhor OD 232,000 243,6006 Daun Keo OD 217,759 217,7587 Prey Kabas OD 200,467 200,4678 Baty OD 264,723 246,7239 Kirivong OD 276,632 262,80110 Ang Rokar OD 168,264 159,84911 Smach Meanchey OD (60%) 115,354 109,58612 Sre Ambel OD 211,747 201,16013 Ban Lung OD (60%) 348,158 330,75114 Sen Mnorum OD (67%) 195,288 185,52515 Tbeng Meanchey OD (68%) 438,498 416,57316 Samrong OD (80%) 464,000 440,80017 Siem Reap OD (90%) 338,575 270,86018 Sotnikum OD 360,000 342,00019 Angkor Chum OD 271,422 257,85120 Krolanh OD 157,609 149,72921 Preah Sdach OD 147,784 140,39422 Pearaing OD 250,120 237,61423 PRH Takeo 200,000 200,00024 PRH Kampong Cham 165,000 165,00025 PRH Siem Reap 191,619 182,03826 PRH Koh Kong 76,903 73,05827 PRH Ratanakiri 232,106 220,50128 PRH Mondulkiri 96,187 91,37829 PRH Preah Vihear 206,352 196,03430 PRH Otdar Meanchey 116,000 110,200Total 6,829,893 6,522,14266
Performance <strong>of</strong> SOA and Non-SOA Operational DistrictsThe tables and linked graphs below show average performance <strong>of</strong> SOA and non-SOA ODs for aperiod <strong>of</strong> 3 years from 2008-10 for 7 key contractual indicators. Note that all the data arefrom the HIS and have not been independently verified. However, it should be noted thatthese are data that have been entered by the OD themselves into the web-based HISdatabase now under construction by an external agency. The data are updated from thoseused for the measurement <strong>of</strong> performance and presented to JPIG in February, 2011. At thattime it was pointed out some <strong>of</strong> the ODs (SOA and non-SOA) had not submitted all <strong>of</strong> thereports in respect <strong>of</strong> their health facilities, and that the tables and graphs would be updatedsubsequently. The secretariat now is in the process <strong>of</strong> cross-checking these data against thosecontained in the newly approved contracts, and is also in the process <strong>of</strong> checking populationdenominators used for calculation <strong>of</strong> coverage and utilization indicators. Results will bereported to JPIG as soon as they are finalized.1. OPD per capita for All New Cases2008 2009 2010SOA (All) 0.59 0.65 0.76Non-SOA (All) 0.39 0.46 0.53National 0.45 0.54 0.64Difference SOA vs Non-SOA 0.19 0.19 0.23Difference SOA vs National 0.14 0.11 0.12Annual % Increase SOA (2008-09, 2009-10) 10.13% 16.99%Annual % Increase Non-SOA (2008-09, 2009-10) 15.38% 15.24%80%70%60%50%OPD PER CAPITA, 2008-201040%30%20%10%2008200920100%SOA (All)NoN-SOA(All)NationalDifferenceSOA vs Non-SOADifferenceSOA vsNationalAnnual %Increase SOA(2008-09,2009-10)Annual %IncreaseNon-SOA(2008-09,2009-10)67
2. Deliveries by Trained Staff2008 2009 2010SOA (All) 45.38% 53.38% 57.91%NoN-SOA (All) 40.27% 47.41% 51.44%National 53.14% 64.48% 69.76%Difference SOA vs Non-SOA 5.11% 5.97% 6.47%Difference SOA vs National -7.76% -11.10% -11.85%Annual % Increase SOA (2008-09, 2009-10) 17.63% 8.49%Annual % Increase Non-SOA (2008-09, 2009-10) 17.73% 8.50%80%70%60%50%DELIVERIES BY TRAINED STAFF, 2008-1040%30%20%10%2008200920100%-10%-20%SOA (All) NoN-SOA(All)National DifferenceSOA vsNon-SOADifferenceSOA vsNational68
3. Deliveries at <strong>Health</strong> Facilities2008 2009 2010SOA (All) 33.53% 43.60% 48.00%NoN-SOA (All) 25.11% 35.60% 43.35%National 34.89% 50.2% 58.61%Difference SOA vs Non-SOA 8.42% 7.99% 4.65%Difference SOA vs National -1.36% -6.60% -10.61%Annual % Increase SOA (2008-09, 2009-10) 30.03% 10.09%Annual % Increase Non-SOA (2008-09, 2009-10) 41.78% 21.76%Annual % Increase Non-SOA (2008-09, 2009-10)Annual % Increase SOA (2008-09, 2009-10)DELIVERIES AT HEALTH FACILITIES, 2008-10Difference SOA vs NationalDifference SOA vs Non-SOANational201020092008NoN-SOA (All)SOA (All)-20% -10% 0% 10% 20% 30% 40% 50% 60%69
4. C-sections2008 2009 2010SOA (All) 0.42% 0.57% 1.05%NoN-SOA (All) 0.50% 0.65% 0.63%National 0.77% 1.69% 2.03%Difference SOA vs Non-SOA -0.07% -0.08% 0.41%Difference SOA vs National -0.35% -1.12% -0.99%Annual % Increase SOA (2008-09, 2009-10) 35.47% 82.80%Annual % Increase Non-SOA (2008-09, 2009-10) 30.68% -2.16%Annual % Increase Non-SOA (2008-09, 2009-10)Annual % Increase SOA (2008-09, 2009-10)C-SECTIONS, 2008-10Difference SOA vs NationalDifference SOA vs Non-SOANational201020092008NoN-SOA (All)SOA (All)-10% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90%5. Modern Method Use2008 2009 2010SOA (All) 29.58% 26.11% 34.24%NoN-SOA (All) 23.37% 22.44% 26.95%Whole Country ( National) 24.76% 22.22% 28.1%Difference SOA vs Non-SOA 6.21% 3.67% 7.29%Difference SOA vs National 4.82% 3.89% 6.14%Annual % Increase SOA (2008-09, 2009-10) -11.71% 31.10%Annual % Increase Non-SOA (2008-09, 2009-10) -3.97% 20.09%70
Annual % Increase Non-SOA (2008-09, 2009-10)Annual % Increase SOA (2008-09, 2009-10)MODERN METHOD USE, 2008-10Difference SOA vs NationalDifference SOA vs Non-SOAWhole Country ( National)201020092008NoN-SOA (All)SOA (All)-20% -10% 0% 10% 20% 30% 40%2008 2009 2010SOA (All) 72.28% 82.51% 77.64%NoN-SOA (All) 64.49% 77.86% 68.31%Whole Country ( National) 75.23% 88.43% 80.31%Difference SOA vs Non-SOA 7.79% 4.65% 9.33%Difference SOA vs National -2.95% -5.92% -2.67%Annual % Increase SOA (2008-09, 2009-10) 14.15% -5.89%Annual % Increase Non-SOA (2008-09, 2009-10) 20.73% -12.26%71
6. ANC2 VisitsANC2 VISITS, 2008-10Annual % Increase Non-SOA (2008-09,2009-10)Annual % Increase SOA (2008-09, 2009-10)Difference SOA vs NationalDifference SOA vs Non-SOAWhole Country ( National)201020092008NoN-SOA (All)SOA (All)-20% 0% 20% 40% 60% 80% 100%7. Measles Vaccinations2008 2009 2010SOA (All) 82.91% 98.28% 114.19%NoN-SOA (All) 80.31% 99.41% 111.26%Whole Country ( National) 93.45% 100.23% 114.11%Difference SOA vs Non-SOA 2.60% -1.14% 2.93%Difference SOA vs National -10.54% -1.95% 0.08%Annual % Increase SOA (2008-09, 2009-10) 18.54% 16.19%Annual % Increase Non-SOA (2008-09, 2009-10) 23.78% 11.91%72
MEASLES IMMUNIZATIONS, 2008-10140%120%100%80%60%200840%200920%20100%-20%SOA (All)NoN-SOA(All)WholeCountry (National)DifferenceSOA vs Non-SOADifferenceSOA vsNationalAnnual %Increase SOA(2008-09,2009-10)Annual %IncreaseNon-SOA(2008-09,2009-10)Revision <strong>of</strong> the SDG ManualDuring this reporting period and extending into the 1 st quarter <strong>of</strong> 2011, the MOH began theprocess <strong>of</strong> conducting a review and revision <strong>of</strong> the SDG manual to include the following items: Target setting methods for SOAs Quarterly monitoring tools Quarterly reporting formats (including financial reports) Cash projections Procurement proceduresTarget Setting MethodsDiscussion on establishing appropriate methods for targets setting for contractual indicatorsby SOAs was first presented and discussed at the Preah Sihanoukville Workshop in July, 2011.Subsequently, in the final quarter <strong>of</strong> 2010 the MOH finalized a policy note on target setting forSOAs based on extensive discussions with all stakeholders, including JPIG. The need forestablishing standard target setting methods was occasioned by joint monitoring visits to theSOAs by JPIG and MOH teams which discovered that some SOAs had contract performancetargets that were lower than the previous year’s achievements; also, there was little or no linkwith national targets and achievements. Two methods were finalized and approved by theMOH and JPIG, and in December 2010 a target Setting Workshop was conducted in KampongCham to train PHD Commissioners and SOAs in the applying the methods. Subsequently, theSDMG carried out a comprehensive review <strong>of</strong> SOA targets contained in the draft 2011contracts and <strong>of</strong>fered their suggestions for revision in quite a few cases. These suggestionsalong with all other targets were then reviewed by JPIG and consolidated suggestions forrevision were then forwarded to PHD Commissioners to make appropriate changes in thedraft contracts. The approved methods for target setting were subsequently adopted by theMOH for inclusion in the AOP 2012 Guidelines and a half day session to train PHDs and ODs inthe methods was conducted by the M&E adviser following the AOP 2012 Guidelines workshopon 5 April, 2011.73
Quarterly <strong>Monitoring</strong> ToolsThe need for standard quarterly monitoring tools for use by SDMG, PHD Commissioner andSOA monitoring teams was identified shortly after the reconstitution <strong>of</strong> the SDMG in the firstsemester, 2010. Subsequently, the secretariat in collaboration with key SDMG membersdeveloped draft tools that were reviewed at the July 2010 workshop in Sihanoukville. Thesedraft tools were then field tested by different SDMG teams during their monitoring visits inthe 3 rd and 4 th quarters <strong>of</strong> 2010. Based on suggestions and feedback from all stakeholdersincluding JPIG, the revised tools were presented at the SDMG Workshop on 22 March, 2011for use by the different levels in the health system.Quarterly Reporting FormatsThese were first drafted at the Preah Sihanoukville workshop in July 2011 by a working group<strong>of</strong> workshop participants led by DPHI. Final reporting formats including quarterly financialswere approved for use by PHD Commissioners and SOAs at the 22 March, 2011 SDMGQuarterly Workshop.Cash ProjectionsFrom January 2011, the Program adopted a two quarter advance payment system for theSDGs linked to certification by the SDMG on performance achievements by each SOA for theprevious quarter. This system replaced the earlier cash release system that was based onmonthly replenishment without any linkage to SOA performance.Procurement ProceduresDevelopment <strong>of</strong> procurement procedures for the SOAs under operating costs was finalizedduring this reporting period and clarifications issued to all participants at the SDMG quarterlyworkshop on 22 March, 2011.Additional Revisions to the SDG ManualThe SDMG with support from the Secretariat is in the process <strong>of</strong> developing an approvedbonus payment scheme, methods verification <strong>of</strong> SOA performance, and a detailed M&EPerformance Indicator matrix to provide guidance to SDMG monitoring teams, PHDCommissioners and SOAs themselves. It is expected that policy options/proposals in theserespects will be presented and reviewed at the forthcoming SDMG Consultative Workshop on10 May, 2011.Tracking <strong>of</strong> PBB Budget for SOAsThe tables below show the tracking tables for the PBB budget releases to the SOAs. Thetracking is carried out by the DBF and reported quarterly to the secretariat.74
STATUS OF PBB BUDGET FOR SPECIAL OPERATING AGENCYFor Quarter 2, 2010NoSOARequested(in Riel)FromSOADate sentrequesttoDBFDepartment Budget & Finance(DBF) - MOHMandatefrom DBFto DG(Ad/F)DBFreceivedDate sentmandate tocomptrollerMEFDate sentmandate toMEFMEFDate sentmandatetoNTMEF CashMgmtCommitteeCashReleasesentto DBFMOHMOH /DBFAllocatecashSOA toNTNationalTreasury( NT)DatePaymentpreparedfor SOASOAReceivedon#DaysProcessExpendidurereport inQuarterSent toDBF1 OD Memut 258,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 1482OD PonHeaKrek 320,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 1483OD PreahSdech 130,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 1484 OD Pearaing 186,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 1485 OD Ang Roka 144,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 1486 OD Kirivong 220,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 1487 OD Banlung 163,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 1488OD TbegMeanchey 172,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 1489ODSenmonorum 132,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 14810OD SmachMeanchey 93,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 14811 OD Sre Ambel 112,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 14812 RH Ratanakiri 112,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 14813 RH 16 Makara 108,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 148RH14 Senmonorum 80,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 14815 RH Koh Kong 110,000,000 23-Mar-2010 1-Apr-2010 2-Apr-10 30-Jul-10 30-Jul-10 3-Aug-10 3-Aug-10 18-Aug-10 1482,340,000,000 Average Number <strong>of</strong> Days 14875
STATUS OF PBB BUDGET FOR SPECIAL OPERATING AGENCYFor Quarter 3, 2010NoName's SOARequested(in Riel)FromSOADatesentrequesttoDBFDepartment Budget & Finance(DBF) - MOHDBF Mandate Date sentreceive from DBF mandate tod to DG controler(Ad/F) MEFDate sentmandate toMEFMEFDate sentmandate toNTMEF CashMgmtCommitteeCashRelease sentto DBFMOHMOH / DBFAllocatecashSOA toNTNationalTreasury( NT)DatePaymentpreparedfor SOASOAReceivedon#DaysProcessExpendidurereport inQuarterSent toDBF1 OD Memut 103,200,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 942 OD Pongea Krek 102,600,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 943 OD Preah Sdech 78,000,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 944 OD Pearaing 128,040,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 945 OD Ang Roka 86,400,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 946 OD Kirivong 131,040,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 947 OD Banlung 82,860,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 948 OD Tbeg Meanchey 76,200,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 949 OD Senmonorum 69,600,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 94OD Smach10 Meanchey 66,480,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 9411 OD Sre Ambel 93,000,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 9412 RH Ratanakiri 48,000,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 9413 RH 16 Makara 38,880,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 9414 RH Senmonorum 32,700,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 9415 RH Koh Kong 48,000,000 10-Aug-10 18-Aug-10 23-Aug-10 20-Oct-10 20-Oct-10 3-Nov-10 3-Nov-10 12-Nov-10 941,185,000,000Average Number <strong>of</strong>Days 9476
CHAPTER 3: HEALTH CARE FINANCING STRATEGY3.1 INC REASE GOVE RNMENT BUD GE T A ND IMPROVE EFFIC IENC Y OF GOVERNMENT RE SOU RCEALLOCA TION FOR HEALTHKey <strong>Health</strong> Financing Indicators 2008 2009 2010Government Budget for <strong>Health</strong> (Riels) 450,629,639,800 549,534,152,000 645,138,220,000% <strong>of</strong> Budget for Central Level 70.15% 69.84% 71.74%% <strong>of</strong> Budget for Provincial Level 29.85% 30.16% 28.56%% <strong>of</strong> GDP for <strong>Health</strong> 1.05% 1.11 NA<strong>Health</strong> Budget as % <strong>of</strong> current national disbursement 12.54% 11.11 12.83%Total Government health disbursement (Riels) 425,949,210,030 522,926,557,167 611,357,559,206Total Population (Census 2008) 13,388,910 13,614,706 13,840,370Exchange Rate per USD 4,000 4,100 4,100Government <strong>Health</strong> Disbursement per capita (Riels) 31,814 38,408 44,172Government <strong>Health</strong> Disbursement per capita (USD) 7.95 9.36 10.77% Government spending Adjusted Budget 94.50% 95.16% 94.8%% <strong>of</strong> spending at central 95.30% 96% 96.7%% <strong>of</strong> spending at Provinces 92.60% 91% 90.0%% <strong>of</strong> Government Disbursement/Total disbursement byprovincePHDO 34% 32.00% NA at this time(Depend onissue <strong>of</strong> 2010Expenditurebook.)ODO 10% 9.00% NA at this timeRH 25% 27.00% NA at this timeHC 31% 32.00% NA at this timeOOP Disbursement per capita to public health facility viauser fee(USD) 0.52 1.17 0.60OOP per capita to public and private 25 25 25 (based 2005)Donor fund into health sector (USD) 110,731,129 129,601,479 88,196,043Donor fund per capita (USD) 8.27 9.52 6.37Total <strong>Health</strong> Expenditures per capita (USD) 40 40 40Number <strong>of</strong> health facility with SOA 0 15 30Number <strong>of</strong> National Hospitals with subsidy schemes 1 6 6Number <strong>of</strong> RH with HEF-subsidy schemes 52 52 57Number <strong>of</strong> HC with HEF-subsidy schemes 80 140 229Percentage poor people coverage by HEF 68 73 77Number <strong>of</strong> National Hospitals with VHIS (CBHI) schemes 2 2 2Number <strong>of</strong> RHs with VHIS schemes 12 13 18Number <strong>of</strong> VHIS beneficiaries 79,873 12hm2,829 170,490Source: Department <strong>of</strong> Budget and Finance, and Department <strong>of</strong> <strong>Plan</strong>ning and <strong>Health</strong> Information77
3.2 REDUCE FINA NCIAL BA RRIE RS A T THE POINT OF CARE AND DEVE LOP SOCIA L HEALTHPROTECTION ME CHA NISMSThe National Social Protection Strategy for the Poor and Vulnerable <strong>of</strong> HSSP2 (2009-2013)includes (i) Master <strong>Plan</strong> for Social <strong>Health</strong> Protection and (ii) <strong>Health</strong> Equity Fund Guidelines. TheRoyal Government <strong>of</strong> Cambodia (RGC) has identified improving social protection for the poorand vulnerable as a policy priority in the Rectangular Strategy, in the NSDP Update, and at the2008 Cambodia Development Cooperation Forum.From 2009-to date the RGC has undertaken a consultation process to develop the NationalSocial Protection Strategy for the Poor and Vulnerable. An Interim Working Group (IWG) onSocial Safety Nets (under TWG–Food Security & Nutrition) led by Council for Agricultural andRural Development (Chair) and with participation from MEF/SNEC, MOP, MOI, MOH, MOEYS,MOSAVY, MOLVT, MRD, and development partners. This IWG has developed sharedunderstanding <strong>of</strong> the concepts, produced an inventory <strong>of</strong> existing interventions, held NationalForum on Social Safety Nets with closing address by Samdech Prime Minister Hun Sen, and ledtechnical consultations on various social protection topics.The RGC is developing the draft Strategy for consultation in March and April. The draft Strategywill be presented for consultation with RGC central and line ministries, development partners,NGOs and other stakeholders; and in June 2010 the Strategy will be presented at the 2010Cambodia Development Cooperation Forum.A Social <strong>Health</strong> Protection (SHP) Master <strong>Plan</strong> has been developed with overall goal <strong>of</strong> providingeffective and equitable access to affordable quality <strong>of</strong> health services for all Cambodians by2015 and aims to developing and implementing a sustainable national system for social healthprotection by ensuring (i) social health protection coverage to all with priority for the poor; (ii)basic package <strong>of</strong> responsive health care benefits at an affordable price; (iii) accessible healthcare services with client-oriented quality; through consolidation <strong>of</strong> existing schemes andbuilding a national system that will make possible move towards universal coverage under anational health insurance agency.3.2.1 HEALTH EQUITY FUNDS RESULTS AND ACHIEVEMENTSThere were a total <strong>of</strong> 53 health equity funds (HEFs) operating in the sector, including 9subsidized directly by Government (excluding the 6 national hospitals), with the rest beingsupported by a variety <strong>of</strong> health development partners including USAID and HSSP2 partners. Itis estimated that coverage <strong>of</strong> HEFs amounted to 73% <strong>of</strong> the total population <strong>of</strong> the country or9.7 million people. Pre-identified beneficiaries included 980,431 persons, while post-identifiedpersons amounted to 1.3 million. The total number <strong>of</strong> cases directly supported by HEFs hasshown an increase from 2007 through this reporting period as <strong>of</strong> 16 September 2010, with thegreatest increase occurring from 2007 to 2008 when the number <strong>of</strong> HEF schemes that wereoperational increased due to JFPR/ADB funded HEFs coming on stream.Overall, during this reporting period, $2.99 million was incurred as total benefit costs (user fees,transport costs, food costs, and non-food costs), and $427,751 as total administration andprogram development costs. Utilization included a total <strong>of</strong> 202,121 (204,268 based on totalsheet 2010) OPD visits, 45,524 (46,118 based on total sheet 2010) IPD cases, and 9,986 (total78
sheet 2010) deliveries. Of the total benefit costs <strong>of</strong> $1,449,748, payments for transport costsare $189,262.List <strong>of</strong> <strong>Health</strong> Equity Funds, 2010No Scheme Source <strong>of</strong> Fund Operators Coverage Pop.2010 BeneficiaryHSSP/WB/USAID1 Mongkol Borey HSSP/WB/USAID URC-CHS 242,683 75,2322 Ochrov HSSP/WB/USAID URC-CHS 187,907 58,2513 Preahnetpreah HSSP/WB/USAID URC-CHS 133,429 41,3634 Mongrussei HSSP/WB/USAID URC-AFH 190,523 59,0625 Battambang HSSP/WB/USAID URC-AFH 333,064 103,2506 Sampeo Meas HSSP/WB/USAID URC-CHS 273,527 84,7937 Bakan HSSP/WB/USAID URC-CHS 124,611 38,6298 Sihanouk Vill HSSP/WB/USAID URC-RHAC 232,786 72,1649 Chhlong HSSP/WB/USAID URC-AFH 90,324 28,00110 Kratie HSSP/WB/USAID URC-AFH 227,091 70,398HSSP/WB and OtherDonors11 Kg. Thom HSSP/WB AFH 267,280 82,85712 Staung HSSP/WB AFH 137,744 42,70113 Preah Vihear HSSP/WB AFH 183,718 56,95314 Memot HSSP/ URC-AFH 134,589 41,72315 Ponhear Krek-Dambe HSSP/ URC-AFH 213,150 66,07616 Smach Mean Chey HSSP/ URC-RHAC 57,036 17,68117 Srae Ambel HSSP/ URC-RHAC 78,005 24,18218 Kirivong HSSP/ URC-BFH 226,269 70,14319 AngRokar HSSP/ URC-BFH 139,231 43,16220 Sen Monorom HSSP/ URC-AFH 69,101 21,42121 Ratnakiri (Banlong) HSSP/ URC-AFH 164,848 51,10322 PreahSdach HSSP/ URC-AFH 117,734 36,49723 Pearaing HSSP/ URC-AFH 196,500 60,91524 Kampong Siem BTC CHHRA 283,549 87,90025 Prey Chhor BTC CHHRA 185,290 57,44026 Cheung Prey BTC CHHRA 195,799 60,69827 Chamka Leu BTC CHHRA 161,264 49,99228 Samrong USAID/BTC/CHRA CHHRA 219,316 67,988Anlong Veng USAID/BTC/CHRA CHHRA29 Sotrnikum USAID/BTC/CHRA CHHRA 285,616 88,54130 SiemReap USAID/BTC/CHRA CHHRA 930,479 288,44831 Krolanh USAID/BTC/CHRA CHHRA 123,956 38,42632 Steungtreng VSO33 SvayRieng UNICEF34 Municipal Hospital (Kandal) USAID/URC FHDCroix-rouge USAID/URC FHDKhm-Soviet USAID/URC FHD35 OD Choeung(A Kgnan-K.9) USAID/URC FHD79
UNFPA36 OD Lech (Pochentong) USAID/URC FHD37 OD Tbong (Cdong, Chakanre) URC/FHD FHD38 Daunkeo SRC CRC39 Angkor Chum UNFPA RHAC 225,041 69,76340 Tbong Khmum-kroch chhmar UNFPA RHAC 207,277 64,25641 Kg. Chhnang (RPH) UNFPA RHAC 206,899 64,13942 Kg. Tralach UNFPA RHAC 164,671 51,04843 Boribo UNFPA RHAC 113,342 35,136Govt/Subsidy-ODO and National HospitalsCBHI44 Kampong Trach Gvt Subsidy ODO45 Ankorchey Gvt Subsidy ODO46 Kampong Trabek Gvt Subsidy ODO47 Romeas Hek Gvt Subsidy ODO48 Kg. Speu Gvt Subsidy ODOKg. Chhang Gvt Subsidy ODO49 Takmao Gvt Subsidy ODO50 Ksach Kandal Gvt Subsidy ODO51 Pailin Gvt Subsidy ODO52 National Pediatric Gvt Subsidy NH53 Ang. Dong Gvt Subsidy NH54 Kampuchea Sviet Gvt Subsidy NH55 Kossamak Gvt Subsidy NH56 Calmet Gvt Subsidy NH57 MCH Gvt Subsidy NHKampot GRET/SKY 138,878Ang Rokar GRET/SKY 139,231Batie GRET/SKY 198,970Kirivong GRET/SKY 226,269Takeo RH/Daun Keo GRET/SKY 218,076Prey Kabass GRET/SKY 148,538Phnom Penh/Kandal GRET/SKY 275,658The graphs below show the patterns <strong>of</strong> utilization and costs incurred for groups <strong>of</strong> HEFs bysource <strong>of</strong> funding for the year 2010. 3As could be observed from Figure 1, during 2007, 2008 and early 2009 the number <strong>of</strong> <strong>Health</strong>Equity Fund Beneficiaries varied between less than a thousand to 2000. However the utilization<strong>of</strong> the HEF beneficiaries has been constantly increasing from 2009 onwards and it has taken apick stage during September 2010. This shows a significant improvement in the utilization overthe years.3 Source: Bureau <strong>of</strong> <strong>Health</strong> Economics and Financing, Department <strong>of</strong> <strong>Plan</strong>ning and <strong>Health</strong> Information.80
Figure 1: Comparison <strong>of</strong> cases Pre and Post ID during 2007-201060005000Total Pre-ID40003000200010000Nov-10Sep-10Jul-10May-10Mar-10Jan-10Nov-09Sep-09Jul-09May-09Mar-09Jan-09Nov-08Sep-08Jul-08May-08Mar-08Jan-08Nov-07Sep-07Jul-07May-07Mar-07Jan-07It may be noted that the HEF beneficiaries are usually poor people identified through a Pre-IDprocess which is usually done by <strong>Ministry</strong> <strong>of</strong> <strong>Plan</strong>ning (MoP). However, the MoP is not able toidentify all the poor people and sometimes it so happens that a patient arriving at the hospitaldoes not have the ability to pay the care. There is a process <strong>of</strong> identifying these poor by the HEFoperator. The people identified through this process are called Post-ID patients. As the figuredepicts, over the years the number <strong>of</strong> Pre-ID beneficiaries have increased and there isproportionate increase in Post-ID cases also. However during 2009 and 2010 the number <strong>of</strong>post ID cases has come down significantly. Figure 1.Figure 2: Cost per Pre-ID Poor Individual 2007-2010.1210Cost/Pre-ID Poor Individual86420Nov-10Sep-10Jul-10May-10Mar-10Jan-10Nov-09Sep-09Jul-09May-09Mar-09Jan-09Nov-08Sep-08Jul-08May-08Mar-08Jan-08Nov-07Sep-07Jul-07May-07Mar-07Jan-07Figure 2 shows the average monthly cost for Pre-ID poor. As could be seen from the figure, theaverage cost per Pre-ID poor has declined over the years. This is mostly due to increasedutilisation by the poor. Moreover the indirect cost component has not increased compared tothe direct cost component.81
Figure 3: Average cost per IPD – Direct cost, indirect cost and Administrative cost605040Direct BenefitsIndirect BenefitsAdministration3020100Nov-10Sep-10Jul-10May-10Mar-10Jan-10Nov-09Sep-09Jul-09May-09Mar-09Jan-09Nov-08Sep-08Jul-08May-08Mar-08Jan-08Nov-07Sep-07Jul-07May-07Mar-07Jan-07As a result <strong>of</strong> increased utilisation, the direct benefit cost such as user fees, food, transport,non-food and grants has increased substantially over the years. There is a steep increase inaverage direct benefit cost from 2009 onwards. As could be seen from the figure 4, higherAverage Length <strong>of</strong> Stay (ALOS) has also been a major contributing factor for the rise in directbenefit cost. As far as the indirect costs are concerned there is sharp decline in these costsbecause <strong>of</strong> economies <strong>of</strong> scale (Figures 3 and 4)Figure 4: Comparison <strong>of</strong> Trends in ALS for HEF Beneficiaries versus Non-Beneficiaries98ALOS HEF BeneficiariesALOS Non Beneficiaries76543210Nov-10Sep-10Jul-10May-10Mar-10Jan-10Nov-09Sep-09Jul-09May-09Mar-09Jan-09Nov-08Sep-08Jul-08May-08Mar-08Jan-08Nov-07Sep-07Jul-07May-07Mar-07Jan-07Figure 4 depicts the difference <strong>of</strong> ALS between HEF beneficiaries and non-beneficiaries. Amongseveral reasons, two reasons seem to be important; first: providing better quality <strong>of</strong> care to thepoor patients by keeping them longer, second: keeping the bed occupancy rate high, thus82
getting more user fees from the HEF beneficiary patients. However, the exact reason for higherALS for HEF beneficiaries needs to be studied carefully by taking the case mix and casecomplexity issues into consideration.Figure 5: Percent <strong>of</strong> HEF IPD Beneficiaries to Total IPD Patients in HEF supported RHs60%50%Percent HEF40%30%20%10%0%Nov-10Sep-10Jul-10May-10Mar-10Jan-10Nov-09Sep-09Jul-09May-09Mar-09Jan-09Nov-08Sep-08Jul-08May-08Mar-08Jan-08Nov-07Sep-07Jul-07May-07Mar-07Jan-07It is observed that the percentage <strong>of</strong> HEF IPD beneficiaries has increased over the years,especially from the first quarter <strong>of</strong> 2009. This is mostly due to the efforts <strong>of</strong> the implementerson IEC/BCC activities. Due to awareness <strong>of</strong> the community about the health equity fund, theutilisation has increased substantially over the years. However, much needs to be done in thisregard to enhance the utilisation by poor. (Figure 5)Figure 6: Trends in Direct Benefit Costs400000350000300000250000200000150000100000500000Direct Benefits per MonthNov-10Sep-10Jul-10May-10Mar-10Jan-10Nov-09Sep-09Jul-09May-09Mar-09Jan-09Nov-08Sep-08Jul-08May-08Mar-08Jan-08Nov-07Sep-07Jul-07May-07Mar-07Jan-07As already known, increase in direct benefit cost indicates higher utilization, thus betterprogram implementation. As the number <strong>of</strong> beneficiaries increases, the direct cost componentsincrease. As could be seen from figure 6, the direct benefit cost has been increasing constantly.One can easily observe that the direct benefit cost component has suddenly increased during83
the period 2009 and 2010. This may be due to expansion <strong>of</strong> the program and greater awarenessamong the population. (Figure 7)Figure 7: Management Costs/Total Costs40%35%Management Costs/Total Costs30%25%20%15%10%5%0%Nov-10Sep-10Jul-10May-10Mar-10Jan-10Nov-09Sep-09Jul-09May-09Mar-09Jan-09Nov-08Sep-08Jul-08May-08Mar-08Jan-08Nov-07Sep-07Jul-07May-07Mar-07Jan-07As it is already known that management cost is the indirect cost and it remains fixed till it isutilized to an optimal level. After that point if the program has to expand, then themanagement cost need to be increased. As could be observed from the graph at the initial levelthis cost component consumed 25-30 per cent <strong>of</strong> the total fund allocation. During the initialphases <strong>of</strong> the program the cost remained high because <strong>of</strong> low utilization <strong>of</strong> the health carefacilities. From 2009 onwards there is a sharp decline in this component. (Figure 7)84
HEALTH EQUITY FUNDS MANAGEMENT AND TECHNICAL CHALLENGESDuring this period, two key workshops were conducted: a consultative meeting on HEFs on 18March, 2010 at the Phnom Penh Intercontinental Hotel, and then a regional workshop from 6-8June, 2010 in Banteay Meanchey. The sub-sections below summarize the outcomes from bothsets <strong>of</strong> meetings.Evidence from past experience suggests that HEFs are an effective means <strong>of</strong> targeting the poorby reducing financial and physical barriers and providing access to quality health services forthe poor. Pre-identification <strong>of</strong> poor families appears to be more effective than postidentificationin minimizing inclusion and exclusion errors, and ensuring complete coverage <strong>of</strong>the poor. HEFs can improve underutilization <strong>of</strong> health facilities, and provide additional revenuesand incentives for staff motivation. They contribute to improved quality <strong>of</strong> services throughlonger opening hours and improvements in staff attitudes and behavior. Finally, HEFs can helpreduce but may not completely eliminate household debt arising from health expenditures.Major concerns that the meetings highlighted included the fact that inclusion and exclusionerrors continue to be higher than warranted and that coverage needs to expand more quickly,particularly to HCs and HPs. Certain sections <strong>of</strong> the poor like the homeless and migrantscontinue to be excluded and special initiatives may be needed to enable them to access theseservices. Benefit packages need to be expanded to cover targeted services such as chronicdiseases and others. Currently, there is a lack <strong>of</strong> feedback and analysis and use <strong>of</strong> data fromreporting systems. Administrative systems are overloaded due to the need for supportingdocumentation for each case receiving HEF support.Other issues <strong>of</strong> concern include the ID Poor scheme: a combination <strong>of</strong> pre- and postidentificationmay result in fewer exclusion and inclusion errors; the process <strong>of</strong> distribution <strong>of</strong>ID cards to the poor needs to be reviewed carefully; and verification <strong>of</strong> poor households shouldbe carried out with the involvement <strong>of</strong> health staff, VHSGs, and HEF operators, with the leadtaken by the Commune Councils. These concerns should also be relayed to the MOP for furtheraction. To expand coverage <strong>of</strong> HEFs which is currently dependent on facilities obtaining aminimum assessment score, it may be necessary to grant approval based on conditions thatentail quick improvements in the identified weaknesses.A key recommendation emanating from the consultative meetings emphasized the need for aninstitutional home for social health protection that will cover the current roles and functions <strong>of</strong>HEF implementers. The meetings called for a nationally representative, random samplehousehold survey to be conducted to determine the impact <strong>of</strong> HEFs on household wealth statusand poverty reduction, household health expenditures, and health seeking behavior. To thisshould be added a blind independent national evaluation <strong>of</strong> HEFI, HEFO and SUBO performanceso that it can provide the evidence base for establishment <strong>of</strong> uniform procedures and thecreation <strong>of</strong> a national HEF agency. Development partner support, both financial and technicalshould continue in close consultation with the MOH.85
CHAPTER 4: HUMAN RESOURCES FOR HEALTH4.1 IMP ROVE TECHNICA L SKILLS AND COMPETE NCE OF HEALTH WORKFORCEPROGRESS OF CAPACITY BUILDING ACTIVITIESNoType <strong>of</strong> TrainingTotal No <strong>of</strong>SexStaff Trained MF1 MCH/NNP 12,817 4,207 8,61024 PHDs 11,889 3,649 8,240Central-National Program 928 558 3702 MCH/ R. <strong>Health</strong> 3,544 636 2,90824 PHDs 3,160 566 2,594Central-National Program 384 70 3143 MCH/ PMTCT 506 61 44524 PHDs 328 25 303Central-National Program 178 36 1425 NIP 5,298 3,123 2,17524 PHDs 5,137 3,000 2,37Central-National-Program 161 123 384 <strong>Health</strong> Promotion 3,994 1,980 2,01424 PHDs 3,817 1,856 1,961Central-National Program 177 124 535 Dengue 5,372 3,805 1,56724PHDs 2,990 1,841 1,149Central-National Program 2,382 1,964 4186 Helminth 387 299 8824PHDs 35 17 18Central-National Program 352 282 707 Drugs Management 100 79 2124PHDs 100 79 21DDF dpt N/A N/A N/A8 Management 1,622 1,142 48024PHDs 1,622 1,142 4809 Administration 187 128 5924PHDs 75 57 18Adm Dpt 112 71 4110 Accounting/ Finance 51 38 1324 PHDs 51 38 1311 Language 14 12 224 PHDs 14 12 212 Computer Training 12 12 024 PHDs 12 12 086
Total No <strong>of</strong>SexNoType <strong>of</strong> TrainingStaff Trained MF13 Training in RTCs 513 275 23814 Other Training 6,130 3,005 3,12524 PHDs 6,130 3,005 3,125Trained staff in all Departments 6,047 3,810 2,23715 Audit 21 18 316 PersDpt 984 452 53217 PMD 1265 819 44618 DPHI 740 373 36719 CDC 1742 1388 35420 DBF 6 4 221 HRD 177 102 7522 HSD 1118 658 460Total 46,594 22,612 23,982RTCs Training Activities ReportNo Description Total M F1 Battambang RTC 57 44 132 Kg Cham RTC 150 87 633 Kampot RTC 245 111 1344 Stung Treng RTC 61 33 28Total 513 275 238SUMMARY OF TRAINING ACTIVITIES UNDER FINANCIAL MANAGEMENT IMPROVEMENT PLAN (FMIP) FOR 2010No1TrainingDate18-22JanuaryNo<strong>of</strong>Days5TrainingModuleBasicAccounting& InternalControlProvince Participant group Male Female TotalKampongChhnangChief accountant, accountant,and cashier from OD MonkulBorei, OD Pres Net Preas, ODThmor Pouk, OD Or Chrov, ODThmar Koul, OD Mong Russey, ODSampov Loun, OD Battambang,OD Sangke, OD Kampong Cham,OD Kroch Chhmar, OD O ReangOv, OD Srei Santhor, OD TbongKhmum, RH Banteay Meanchey,RH Battambang, RH KampongChhnang33 18 5187
23458-12February22-26February15-19March29 March-02 April55556 19-23 April 5Budget &CashManagementBasicAccounting& InternalControlBudget &CashManagementBasicAccounting& InternalControlBudget &CashManagementKampongChhnangKampongChamKampongChamSiemReapKampongChhnangChief accountant, accountant,and cashier fromOD Monkul Borei, OD Preah NetPreah, OD Thmar Pouk, OD OrChrov, OD Thmar Koul, OD MongRossey, OD Sompov Loun, ODBattambang, OD Sangke, ODKompong Cham, OD KrouchChmar, OD O Reang Ov, OD SreiSanthor, OD Tbong Khmum, PRHBaneay Meanchey, PRHbattambang, and PRH KompongChhnag.Chief accountant, accountant,and cashier from OD KampongChhnang, OD Kampong Tralach,OD Kampong Speu, OD KorngPisey, OD Oudong, OD BaraySantuk, OD Kampong Thom, ODStoung, OD Ankor Chey, ODChhouk, OD Kampong Trach, ODKampot, OD Ang Snoul, RHKampong Speu, RH KampongThom, RH Kampot, RH Kandal.Chief accountant, accountant,and cashier from OD KampongChhnang, OD Kampong Tralach,OD Kampong Speu, OD KorngPisey, OD Oudong, OD BaraySantuk, OD Kampong Thom, ODStoung, OD Ankor Chey, ODChhouk, OD Kampong Trach, ODKampot, OD Ang Snoul, RHKampong Speu, RH KampongThom, RH Kampot, RH Kandal.Chief accountant, accountant,and cashier from OD Ken Svay,OD Koh Thom, OD Khsac Kandal,OD Muk Kompol, OD Ponhea Leu,OD Saang, OD Ta Khmao, ODKratie, OD Chloung, OD Cheung,OD Kandal, OD Tbong, OD Lech,OD Kamchay Mear, OD KampongTabek, RH Kratie, RH Prey Veng,RH Phnom Penh.Chief accountant, accountant,and cashier fromOD Ken Svay, OD Kos Thom, ODKhsac Kandal, OD Muk Kompol,OD Ponhea Leu, OD Saang, ODTakhmao, OD Kratie, ODChhloung, OD Cheung, ODKandal, OD Tbong, OD Lech, ODKamchay Mear, OD KampongTrabek, RH Kratie, RH PhnomPenh.35 16 5135 13 4835 13 4834 19 5334 17 5188
731 May-04June58 07-11 June 59101130 June –01 July02 August– 05August201016 August– 19August2010244BasicAccounting& InternalControlBudget &CashManagementBudgetCosting andCash FlowManagementBudgetCosting andCash FlowManagementBudgetCosting andCash FlowManagementKratieSiemReapDBFOfficeSiemReapSihanoukChief accountant, accountant,and cashier from OD Mesang, ODNeak Leung, OD Bakan, ODSampove Meas, OD PresSihanouk, OD Steung Treng, ODChi Pou, OD Romeas Hek, ODSvay Rieng, OD Kep, OD Pailin, ODBoribo, PRH Pursat, PRH PreahSihanuouk, PRH Steung Treng,PRH Svay Rieng, PRH Kept, PHRPailin, RTC Kampong Cham, RTCKampot, RTC Steung Treng, RTCBattambang.Chief accountant, accountant,and cashier from OD Mesang, ODNeak Leung, OD Bakan, ODSampove Meas, OD PresSihanouk, OD Chi Pou, ODRomeas Hek, OD Svay Rieng, ODKep, OD Pailin, OD Boribo, RHPursat, RH preas sihanouk, RHSteung Treng, RH Svay Rieng, RHKep, RH Paillin, Rh Prey Veng, RTCBattambong, RTC steung Treng,RTC Kampong Cham, and RTCkampot.Khut Thavary, Ang Vannak, MokMoeun, So Serey, Nuth Hak, SoNary, Moy Phally, Hy Sotheary,Lay Heng, Ly Sinthean, Khat Kea,To Sophorn, Keut Meakdaren,Pok ChindaChief accountant, accountant,and cashier from PHD Koh Kong,PHD Takeo, PHD OrdorMeanchey, OD Samroang, ODSmach Meanchey, OD Sre Ambel,OD Prey Kabas, OD Bati, OD DaunKeo, OD Ang Roka, OD Kirivong,PRH Koh Kong, PRH Takeo, PRHOrdor MeancheyChief accountant, accountant,and cashier from PHD Siem Reap,PHD Kampong Cham, OD ChoengPrey, OD Chamkar Leu, OD PreyChor, OD Siem Reap, OD SothNikum, OD Angkor Chum, ODKralanh, OD Memut, OD PonheaKrek, PRH Kampong Cham, PRHSiem Reap.39 21 6039 24 6311 4 1529 13 4228 11 3989
1213141506September– 09September201020September– 23September201017November– 18November201022December-24December20104433BudgetCosting andCash FlowManagementBudgetCosting andCash FlowManagementFinancialAccountingManuals-Training <strong>of</strong>Trainerspreparationfor rolloutBasicAccounting& InternalControl,BudgetCosting andCash FlowManagementSihanoukSiemReapDBF,MoHDBF,MoHChief accountant, accountant,and cashier from OD TbengMeanchey, OD Sen Monorom, ODBan Lung, OD Peareang, ODPreah Sdach, PRH Modul Kiri, PRHPreah Vihea, PRH Ratanak Kiri,PRH Prey Veng, PHD Modul Kiri,PHD Preah Vihea, PHD RatanakKiri, PHD Prey Veng.Chief accountant, accountant,and cashier from PHD BanteayMeanchey, PHD Battambang,PHD Kompong Chhnang, PHDKompong Speu, PHD KompongThom, PHD Kompot, PHD Kandal,PHD Kratie, PHD Phnom Penh,PHD Pursat, PHD Preah Sihanouk,PHD Stung Treng, PHD SvayRieng, PHD PailinStaff from planning and Finance<strong>of</strong>fice, Supply <strong>of</strong>fice, andLiquidation Office, DBF <strong>of</strong> MoHStaff from planning and Finance<strong>of</strong>fice and Supply <strong>of</strong>fice (DBF).25 10 3528 14 4212 5 172 1 3Total participants for Modules 1& 2 Basic accounting and Internal Control 141Total participants for Modules 3& 4 Budget and Cash Management 143Total participants for Budget Costing and Cash Flow Management 123Total participants for Training <strong>of</strong> Trainer 12Workshop 29 November 2010 Consultative Workshop on MOH Financial Accounting ManualsD. Cadre taskE. Midwives incentivesImplementation <strong>of</strong> Midwife incentives supported by Royal Government provides 60,000 Riel forMidwifery Staff at HCs, and 40,000 Riel for Midwifery Staff at RHs for live births. Theseincentives continue to be the main factors contributing to the increase in deliveries by healthstaff at health facilities from 44% in 2009 to 50.2% in 2010.90
NoRTCsTotalNo.<strong>of</strong>TrainedAsso-Sex 2nd 2nd 2nd 2ndPrimary PrimaryNurseDentalM F Nurse midwife dentist Nurse Midwife Nurse midwifeOther1 RTC Battambang 590 205 385 314 146 39 29 622 RTC Kg Cham 746 277 469 318 154 128 47 31 683 RTC Kampot 586 190 396 315 149 32 30 604 RTC Stung Treng 353 146 207 176 98 36 43Total 2,275 818 1,457 1,123 547 128 79 39 126 2334.2 STAFF DISTRIBUTION A ND RETE NTION, W ITH PRIORITY TO PE RSONNEL ESSENTIA L TOHEALTH SECTOR PRIORITIE SSTAFF DEPLOYMENTThe Annex contains a detailed table <strong>of</strong> the deployment <strong>of</strong> all MOH staff in the health system bycategory and by key locations (departments, national programs, provinces, etc.4.3 STAFF T RA INING AT RTC SNo Indicators Quarter 1 Quarter 2 Quarter 3 Quarter 4 ANNUALTarget Ach Target Ach Target Ach Target Ach Target Ach1# <strong>of</strong> Midwifery preceptorsreceived ToT training25 25 0 0 0 0 0 0 50 25course2% <strong>of</strong> 3 year curriculumcontents and guideline are 25% 20% 25% 20% 25% 50% 25% 10% 100% 100%developed3% <strong>of</strong> clinical checklist forADNM is reviewed25% 0% 25% 0% 25% 10% 25% 0% 70% 10%4% <strong>of</strong> exit examquestionnaires for ADM is 0% 0% 30% 0% 20% 0% 0% 0% 50% 0%developed5% <strong>of</strong> exit examquestionnaires for ADNM 0% 0% 25% 20% 50% 50% 25% 0% 70% 70%is reviewed6% <strong>of</strong> exit examquestionnaires for PNM is 0% 0% 40% 0% 10% 40% 30% 30% 70% 70%reviewed7% <strong>of</strong> Bachelor <strong>of</strong> Science inMidwifery curriculum is 0% 0% 40% 0% 40% 30% 20% 10% 40% 40%developed8# <strong>of</strong> supervision onmidwifery pre-servicetraining at RTCs1 0 2 2 4 0 4 0 4 291
No Indicators Quarter 1 Quarter 2 Quarter 3 Quarter 4 ANNUALTarget Ach Target Ach Target Ach Target Ach Target Ach9% <strong>of</strong> <strong>Health</strong> Workforce<strong>Plan</strong> reviewed50% 0% 30% 0% 0% 0% 0% 0% 80% 0%10% <strong>of</strong> exit exam guidelinefor ADN program is0% 0% 50% 20% 50% 80% 50% 0% 70% 100%reviewed11# <strong>of</strong> CECs attendeddatabase training course 10 0 10 0 20 0 20 0 40 0at Department <strong>of</strong> HRD12# <strong>of</strong> CECs attendeddatabase management 10 10 10 8 10 6 30 32 100 56training course at RTCs13# <strong>of</strong> National meeting onstrengthening the quality<strong>of</strong> training for health1 1 1 1 1 1 1 0 4 3CONSTRAINTSIn quarter 1, Department and Regional Training Centers were busy with conducting exitexamination for Nursing and Midwifery program and also recruitment <strong>of</strong> new intakesfor Regional Training Centers.In quarter 4, HRD was busy with the preparation <strong>of</strong> national entry exam <strong>of</strong> MedicalDoctor, Pharmacist, Dentist and Bachelor <strong>of</strong> Science in Nursing for both Public andPrivate Universities.Also recruitment <strong>of</strong> new intakes for Nursing and Midwifery courses and exit exam <strong>of</strong>Associate Degree <strong>of</strong> Nursing students in all RTCs were conducted.NEXT STEPSAll activities in Annual Operational <strong>Plan</strong> <strong>of</strong> HRD 2011 will be completely implemented in 20114.4 PE RFORMA NCE MA NA GEME NT SYSTEMPERSONNEL DEPARTMENT<strong>Monitoring</strong> IndicatorsNoIndicators1 Number <strong>of</strong> provinces and municipalitiestrained on Personnel Management2 Number <strong>of</strong> provinces and municipalitiesSupervised on personnel ManagementQuarter 1 Quarter 2 Quarter 3 Quarter4 ANNUALT A T A T A T A T A2 1 0 0 2 1 2 0 6 27 7 7 7 7 7 3 2 24 233 Number <strong>of</strong> SOA received incentives 30 24 6 4 2 2 0 0 30 304 Number <strong>of</strong> staff recruited to be civilservants0 0 850 810 32 32 8 8 850 85092
CONSTRAINTS AND NEXT STEPS Personnel department has no enough human resource to implement all newdepartment functions on SOA and PMAS implementation Activity plan not implemented in 2010 will be implemented in 2011Meeting/Workshop Activities ReportTotalType <strong>of</strong> Meetings and Workshops Number <strong>of</strong>SexFunded ByParticipants M F Pooled DiscreteMeeting on the determination <strong>of</strong> number<strong>of</strong> civil servant to be recruit with PHDs 42 36 6 $3,356Workshop on the DeploymentImprovement &Personnel Management 76 73 3 $6,885Commentscontinue tonext yearcontinue tonext yearTotal 118 109 9 $10,24193
CHAPTER 5: HEALTH INFORMATION SYSTEMThe new HIS database at the HIS Bureau (design <strong>of</strong> which was supported by HSSP2 through theservices <strong>of</strong> an international short term HIS consultant) was <strong>of</strong>ficially launched in July, 2009 afterrevision <strong>of</strong> the HIS forms at each level <strong>of</strong> the MOH. Subsequently, HIS staff at central, provincial,OD, and health facility levels were trained by the HIS Bureau in the use <strong>of</strong> the new database.Trend data from the old database have been transferred to the new database. All PHDs andODs in the country now possess and use the computerized database system and send theirmonthly reports to the MOH in electronic format (either through electronic mail or throughcourier), and HSSP2 is providing additional support for computerization <strong>of</strong> RH and HCinformation systems through the provision <strong>of</strong> computer equipment at health facility level.One <strong>of</strong> the problems encountered in 2009 during the transition continued to be tackled duringthis reporting period. Since previous years’ data are all in the old Excel tables format, theBureau continued to devote considerable time and resources to converting them to a usableformat for the new Access based system.Also, during this period, URC’s IT team began to collaborate with the Bureau in developing aweb-based HIS database that will enable IUs (provincial, OD and health facility levels) to uploadand download data as required. The team met on a weekly basis with Bureau staff to design thefeatures <strong>of</strong> the new web site. HSSP2 M&E Adviser also participated in some <strong>of</strong> the meetings toensure that the design team incorporates all HSP2 indicators (core and annual) and includesappropriate trend graphs, charts, and tables linked to the data. When ready, it is expected thatdata from 2006 onward will be available for trend analysis at PHD, OD and health facility levelas required. As <strong>of</strong> the end <strong>of</strong> April, 2011 the web site was still under development, and was notaccessible.Population denominators continue to pose challenges to determining accurate values for keyutilization and coverage indicators in the health sector. Population projections from the 2008Census are only available for succeeding years at the national, provincial, and administrativedistrict levels, but not for operational districts and health facility catchment areas which may ormay not coincide with administrative district and commune boundaries. Recently, the HISBureau has begun using population estimates from the commune database (CDB) forcatchment populations up to the provincial level (national totals continue to be based onCensus 2008 projections). The CDB is housed at the <strong>Ministry</strong> <strong>of</strong> Interior under whose remitCommune Councils fall, and consists <strong>of</strong> total population figures for each commune aggregatedupwards to each administrative district and province, as collected from the CCs themselves. Theissue for the MOH is that even if the sub-national total population figures are accurate, targetpopulation figures are less likely to be, since the proportions on which they are based arethemselves outdated e.g., the Census 2008 did not produce a crude birth rate estimate, as aresult <strong>of</strong> which an older estimate is being used, leading to overestimates <strong>of</strong> target populationssuch as “expected pregnancies” (more properly “expected births,” since it is derived from thecrude birth rate).As an example, the table below shows a comparison <strong>of</strong> the 2010 population totals taken fromthe HIS and those contained in the annual contracts between PHD Commissioners and SOAs. Ascan be seen in some cases there are significant differences that inevitably have implications forcalculation <strong>of</strong> valid and reliable performance achievements. 2011 contract figures are also94
listed; these will be compared with the HIS 2011 figures once the HIS database is madeavailable.KampongChamSOA Populations from HIS and Contracts for 2010 and 20112010 2010 Contract 2011 Contract(HIS)(PHD-SOA)(PHD-SOA)Prov RH 1,769,862 1,753,147 1,753,147Chamkar Leu-Stueng Trang 163,856 163,856 164,561Choeung Prey-Batheay 213,128 199,816 200,675Memut 135,668 136,554 137,141Ponhea Krek-Dambae 200,745 216,132 216,132Prey Chhor-Kang Meas 187,959 187,959 187,767Koh Kong Prov RH 119,568 58,615 59,667Smach Mean Chey 55,011 58,615 58,615Srae Ambel 64,557 64,557 62,094MondulkiriPreahVihearProv RH 62,819 62,818 66,802Sen Monorom 62,819 62,818 66,802Prov RH 183,718 183,718 190,350Tbeng Meanchey 183,718 183,718 190,350Prey VengPearaing 201,710 201,710 201,730Preah Sdach 119,180 119,180 119,192Ratanakiri Prov RH 164,848 164,848 172,270Balong 164,848 164,848 172,546Siem ReapProv RH 1,220,308 942,236 966,075Kralanh 115,509 127,104 118,431Siem Reap 314,375 303,383 331,237Sot Nikum 585,720 292,860 300,268Angkor Chhum 204,704 218,889 216,000TakeoProv RH 939,223 948,858 955,120Ang Rokar 135,659 139,231 140,150Bati 192,907 198,970 200,283Daun Keo 219,515 219,515 220,964Kirivong 229,475 229,475 230,990Prey Kabass 161,667 161,667 162,734OtdarMeancheyProv RH 154,762 219,316 201,669Samraong 154,762 218,791 201,60995
CHAPTER 6: HEALTH SYSTEM GOVERNANCE6.1 HA RMONIZ ATION A ND ALIGNMENT W ITH IN THE MOH AND AC ROSS THE HE A LTH SECTORThis reporting period witnessed a consultation on increasing harmonization and alignment <strong>of</strong>existing support for health systems strengthening from the Joint <strong>Health</strong> System FinancingPlatform partners during the week <strong>of</strong> 31 May, 2010. The partners include the GAVI alliance,World Bank, Global Fund, and WHO. Based on discussions, the MOH has welcomed theparticipation <strong>of</strong> both GAVI and GFATM in the upcoming JAPR and Mid Term Review <strong>of</strong> HSP2. Inaddition, further work will be undertaken to streamline indicators required to be reported tothe partners so as to reduce the burden on the MOH from multiple formats for reporting.However, GAVI and GFATM will both continue as non-pooling donors. The Debriefing Noteprepared by the partners was circulated to all TWG-H members for information.As already reported elsewhere in the report, further steps were taken to increase H&A <strong>of</strong>Program and MOH systems. Quarterly review reports from IUs now adhere to the MOH format,with some additional information regarding training, workshops and meetings conducted alsocollected. Following agreement between JPIG partners and MOH top management on movingplanning and monitoring functions to the Department <strong>of</strong> <strong>Plan</strong>ning and <strong>Health</strong> Information, thesecretariat has been working extensively on aligning planning and reporting with the existingMOH system. Currently, the planning function (except for the mid-year review <strong>of</strong> the budget)has been fully integrated at all levels, which has reduced the role <strong>of</strong> secretariat in convertingthe approved plans into the Program approved format and budget lines, following the HSSP2financial management system. The recent updated Program monitoring framework also is nowfully aligned with the HSP2 frame work, except for a few indicators required by the WorldBank’s portfolio projects.6.2 PU BLIC-PRIVA TE PA RTNE RSHIPSPublic-private partnerships were strengthened during this reporting period through the furtherexpansion <strong>of</strong> internal contracting arrangements, and the close involvement <strong>of</strong> local andinternational NGOs in the implementation <strong>of</strong> HEFs, either as HEF implementers or HEFoperators. Further details on both appear elsewhere in the report.6.3 INSTITU TIONAL DEV ELOPMENT6.3.1 POLICY DEVELOPMENT AND IMPLEMENTATIONDuring this reporting period, the National <strong>Health</strong> Congress/Joint Annual Performance Reviewwas conducted on 14-15 March, 2011 to review progress made against the 2010 AOP and t<strong>of</strong>inalize and disseminate health sector priorities for the preparation <strong>of</strong> the 2012 AOP.In December, 2009 the RGC terminated the MBPI, PMG, and other salary supplement andincentive schemes pending introduction <strong>of</strong> a unified, more equitable and sustainable scheme in2010. Subsequently, during this reporting period, the RGC announced the launching <strong>of</strong> thePriority Operating Cost (POC) scheme that would strengthen equity and sustainability <strong>of</strong>incentive systems. The POC scheme is expected to be launched in the second semester, 2011.96
6.4 STRE NGTHE N MOH HEALTH SECTOR STEWARD SH IP TH ROU GH DECENTRALIZA TION A NDDECONCE NTRA TIONIn 2009, the National Committee on Decentralization and Development was renamed as theNational Committee for Democratic Development (NCDD) with a focus on implementingdemocratic decentralization initiatives at sub-national levels. In January 2009, the MoH wasincluded as a member <strong>of</strong> the NCDD, and per the instructions <strong>of</strong> the MOI, a working group wascreated within the MOH with a Secretary <strong>of</strong> State as chair to liaise with NCDD; a budget <strong>of</strong>$20,000 was provided by NCDD for conducting two workshops, field visits to 7 provinces tostudy constraints and challenges, and to pay for <strong>of</strong>fice equipment and supplies, and incentivesfor 3 <strong>of</strong>ficials.Later in the year, a joint mission <strong>of</strong> UNDP and GTZ which are supporting NCDD was conductedto the ministries <strong>of</strong> health, education, social welfare and rural development. The findings <strong>of</strong> themission on the health sector was that while the two workshops had been conducted (one forprovincial <strong>of</strong>ficials and one for central and national program staff), along with site visits to 7provinces, there was little understanding or appreciation <strong>of</strong> the concepts <strong>of</strong> decentralizationand deconcentration, with some misgivings regarding how the initiative would actually beimplemented especially with respect to deployment <strong>of</strong> staff. The mission also found verylimited involvement <strong>of</strong> pr<strong>of</strong>essional associations and NGOs in the process, particularly inconducting the review <strong>of</strong> functions, responsibilities and task that is required as part <strong>of</strong> theprocess. The mission recommended that the membership <strong>of</strong> the D&D working group beexpanded to include more representatives from the sub-national levels, national programs, civilsociety organizations, and health partners. A second recommendation was that a functionalanalysis be carried out to identify core functions <strong>of</strong> the MOH, and those that could potentiallybe transferred to sub-national levels. It also suggested that the MOH prepare a roadmap forimplementing D&D, after consultation with all relevant stakeholders in the health sector,identifying short-term, medium-term, and long-term activities for implementation. The MOHaccepted the recommendations to expand the working group, and to conduct furtherdiscussions with departments and national programs to determine which functions, tasks andresponsibilities could be transferred to local levels. In principle it was agreed that in the future,health centers will be managed by District Councils and referral hospitals by Provincial Councils.With regard to the deployment <strong>of</strong> staff, the state secretariat <strong>of</strong> public function is examining theissue and will present its recommendations in due course which will be in line with the MEF’spublic financial management reform initiative.During this reporting period, a number <strong>of</strong> concrete steps have been taken by the working groupso as to follow through on the recommendations <strong>of</strong> the UN-GTZ Joint Review Mission. The D&Dworking group has now been expanded to include DHRD, DSH and DDF as representing thecentral MOH departments, CENAT, NCHADS and NMCHC as representing the nationalprograms, the PHDs <strong>of</strong> Banteay Meanchey, Battambang, Siem Reap, Prey Veng, and KampongThom, UNICEF, GTZ, WHO, and JPIG as representatives <strong>of</strong> health development partners, alongwith MEDICAM. Directors <strong>of</strong> each <strong>of</strong> the central departments and PHDs will act as focal points,with their deputies as alternates. The formulation <strong>of</strong> a D&D strategic framework for the healthsector and mapping <strong>of</strong> functions for D&D have also been initiated. The core group for thesetasks includes the DG/A&F, Director/DPHI and DD/DBF. Based on the identified need fortechnical assistance for examining the question <strong>of</strong> SOAs under D&D, the future relationshipbetween the OD and the administrative district, and lessons learned from international97
experience, TORs have been agreed and UNICEF will initiate the recruitment <strong>of</strong> a short termconsultant.6.5 STRE NGTHE NING COMMU NITY ENGA GEME NT<strong>Monitoring</strong> Indicators for <strong>Health</strong> PromotionNo12345678910IndicatorsQuarter 1 Quarter 2 Quarter 3 Quarter 4 ANNUALTarget Ach Target Ach Target Ach Target Ach Target AchIn theTime No <strong>of</strong> Spot mediaprocessTV5 Station campaign 270procuremeon ANCnt270 270 180 180 180 180 630 630In theTime number <strong>of</strong>process12Karaokeprocureme12 12 8 8 8 8 28 28ntIn theTime No <strong>of</strong> Spot mediaprocessBayon Station campaign 270procuremeon ANCnt270 270 135 135 0 0 405 405In theTime No <strong>of</strong> Karaoke 12processprocureme12 12 8 8 0 0 20 20ntNo <strong>of</strong> monitoring andsupervision on BCC/IPC 4 5 4 3 4 2 4 6 16 16in RHNo <strong>of</strong> WS ondevelopment studybook <strong>of</strong> elderly2 2 NA NA NA NA NA NA 2 2promotionNo <strong>of</strong> WS ondevelopment lessonplan <strong>of</strong> elderly2 0 NA NA NA NA NA 1 2 1promotionNo <strong>of</strong> monitoring andevaluation tobacco and 3 3 2 2 2 2 2 2 9 9health activityNo <strong>of</strong> technical workinggroup meeting on1 0 1 0 1 0 1 1 4 1alcoholNo <strong>of</strong> awareness ontobacco harmful andsmoke free work placeNA NA 3 3 2 2 NA NA 5 5declaration workshopNo <strong>of</strong> WS on harmful <strong>of</strong>alcohol useNA NA 1 1 NA NA NA NA 1 1No <strong>of</strong> training on smokefree policyNA NA 1 1 2 2 NA NA 3 3No <strong>of</strong> T shirts to be usedon CR-PR campaign500 500 NA NA NA NA NA NA 500 500No <strong>of</strong> hats to be usedon CR-PR campaign500 500 NA NA NA NA NA NA 500 500No <strong>of</strong> banners to beused on CR-PR40 40 NA NA NA NA NA NA 40 4098
NocampaignIndicatorsQuarter 1 Quarter 2 Quarter 3 Quarter 4 ANNUALTarget Ach Target Ach Target Ach Target Ach Target Ach11No <strong>of</strong> technical supporton provider behaviorchange intervention(PBCI)9 10 12 8 14 11 15 10 50 3912 Number <strong>of</strong> WS developposter on smoke freehomeNumber <strong>of</strong> WS developT shirt on smoke freehomeNumber <strong>of</strong> Pre- Test <strong>of</strong>13 Poster and T shirt onSmoke free homeNumber <strong>of</strong> CR-PR14campaignCommunity involved incommunitiesNumber <strong>of</strong> TOT onprovider behavior15change intervention(PBCI)Number develop bookstraining <strong>of</strong> trainer <strong>of</strong>16 <strong>Health</strong> CenterManagementCommitteeNumber developcurriculum training <strong>of</strong>17 trainer <strong>of</strong> <strong>Health</strong> CenterManagementCommitteeNumber training <strong>of</strong>trainer for <strong>Health</strong>18 Center ManagementCommittee incommunityNA NA 1 NotyetdoneNotNA NA 1 yetdoneNotNA NA 2 yetdoneNA NA NA 1 1 1NA NA NA 1 1 1NA NA NA 1 2 1NA NA 1 1 NA NA NA NA 1 1NA NA 1200 1700 1200 ###NA NA 1 1 1 1 NA NA 2 2NA NA 1 1 NA NA NA NA 2 1NA NA 2 1 NA NA NA NA 1 1NA NA NA NA NA NA 2 2 2 2CONSTRAINTSDifficult to travel from PHD to HC and Villages for conduct monitoring and supervisionBudget for provide to VHSG, VHV,TBA involve in Campaign training and launching is notfit to the real expenseKnowledge <strong>of</strong> VHSG, VHV ,TBA and village chief is limited for provide keys message <strong>of</strong>campaign to community peopleNo gifts ( soap) to give to community people during campaign implementation is makepeople did not want to participationLess incentive for VHSG for conducted campaign activitiesIEC Materials for use in campaign limited99
NEXT STEPSOn Air for CFC CampaignCampaign on CR_PR Duties, ANC and CFC3-Training and technical support training activities such as PBCI, C_IMCI, MPA, CR_PRand HygienePHC activitiesTobacco activitiesAlcohol activities<strong>Monitoring</strong> and Supervision on health promotion activities such as ANC, CFC and CR{PRCampaign, integrated monitoring, etc.100
CHAPTER 7: PROGRAM MANAGEMENT AND IMPLEMENTATION7.1 KEY PROGRA M MA NA GEME NT AND IMPLE MENTA TION ISSUE S7.1.1 EXTERNAL AUDITSExternal audits have been conducted for 2010 on a quarterly basis. Complete quarterlyauditor’s reports have been reported to the Program for Q1, Q2, and Q3 (both FinancialStatement Report and Internal Control Report). For Q4, the auditor has submitted FinancialStatement Report but not yet submitted the Internal Control Report on the reporting period.The overall findings from the quarterly external audit reports for year 2010 is there are stillsome issues with weaknesses in internal controls. These weaknesses have been addressedthrough consultative meetings, and have been clarified with agreed actions by all IUs asindicated in the Annex for each quarter.7.1.2 LEGAL COVENANTSWill be updated in Final Report7.1.3 JOINT QUARTERLY MEETINGSJoint quarterly meetings <strong>of</strong> the Joint Program Management Group were regularly held duringthis reporting period, one <strong>of</strong> which coincided with the Joint Supervision Mission <strong>of</strong> JPIGpartners. Key outcome and output indicator data for the national and provincial levels werepresented and reviewed, along with the performance <strong>of</strong> individual SOA/SDGs and ODs receivingdiscrete funds. Quarterly Interim Financial Reports were presented for review. Key actions forfollow-up were listed with appropriate deadlines to be monitored, and regular monthlymeetings were held to follow up on actions taken.7.1.4 INDIGENOUS PEOPLES FRAMEWORKWith regard to indigenous peoples, current internally contracted districts possess largemajorities <strong>of</strong> ethnic minority indigenous people. Staff working at health centers and healthposts in ethnic minority areas generally have been selected locally, and are conversant in, andcan communicate in those languages. Enhanced activities targeted at indigenous peoples willbe carried out through efforts on community participation through innovative interventionsthat the Program intends to pilot, such as community score cards, recruitment <strong>of</strong> staff fromethnic minority groups, health equity funds established to target ethnic minority areas, etc. Thecommunity scorecard is being developed jointly with the DPHI and is planned to be piloted inRatanakiri province.7.1.5 GOOD GOVERNANCE FRAMEWORKThe matrix detailing the progress <strong>of</strong> implementation <strong>of</strong> the Good Governance Framework is inAnnex. In general, there has been satisfactory progress on implementation <strong>of</strong> the FrameworkGGF which can be summarized as follows:101
ElementsElement 1:ProcurementElement 2: FinancialManagementElement 3: DisclosureElement 4: Civilsociety roleElement 5:Complaints handlingand remedyElement 6: Code <strong>of</strong>Ethical ConductElement 7: SanctionsElement 8: ProgramSpecificStatus <strong>of</strong>Compliance1a: SC; 1b: AB; 1c:SC; 1d: SC; 1e: FC;1f: SC.2a: SC; 2b: SC; 2c:SC; 2d: SC; 2e:AB; 2f: SC; 2g:ANS; 2h: SC; 2j:SC; 2k: SC; 2l: SC;2m: SC; 2n: AS3a: SC; 3b: PC;Substantialcompliance (SC)Substantialcompliance (SC)PartialCompliance (PC)PartialCompliance (PC)8a: ANS; 8b: PC;8c: FC; 8d: AS;Key Progress/ConstraintsDelay in approval <strong>of</strong> AOP resulted in delay inpreparation <strong>of</strong> procurement plan. It is expected thatthe procurement plan for 2010 will be submitted forapproval by first week <strong>of</strong> April, 2010.Two counterpart staff were appointed by the MOHin September, 2009 and since then, one has joinedthe Program procurement team.The Financial Management Manual was adopted bythe MOH and approved by the WB by 31 December,2009.Submission <strong>of</strong> IFR Q1 was on time, but there was alittle delay in submittal <strong>of</strong> audit report Q1, 2010.Audit recommendations have been taken intoconsideration and report <strong>of</strong> implementationprogress is attached to this report.Internal Audit Advisor will be in place in August2010.Training plan for 2010 is included in quarterly plan.Will recruit a training coordinator to assist DPHI inpreparing training plan for 2011.Many Program documents have been disclosed.MOH is preparing Program information fordisclosure on website from Q4.Two CSOs, CMA and Medicam, have been selectedby the MEF to attend agreed selected procurementevents. They were invited to observe agreedselected procurement events, and attended 4bid/proposal openings on 25 March, 26 May, 30June, and 14 July, 2010.Complaints mechanism has been established.The Code <strong>of</strong> Ethical Conduct has been introduced toall relevant staff, and included in all consultantcontracts.Sanctions policy has been introduced.Program manuals have been translated anddisseminated to local levels for distribution by theend <strong>of</strong> Q1, 2010. English versions <strong>of</strong> the SDG Manual,FMM, and Operational Manual were disseminated atthe Program launch workshop in Q1, 2009 and theKampong Cham workshop in Q2, 2009, and s<strong>of</strong>tcopies were sent to all IUs by email as well.Translation by contracted pr<strong>of</strong>essional translators (atthe rate <strong>of</strong> 2 pages per day per extant contract) was102
ElementsStatus <strong>of</strong>ComplianceKey Progress/Constraintscompleted in December, 2009 and review and editsby Secretariat staff was completed in March, 2010and the Khmer versions disseminated to all IUs byend March, 2010.Per the MOH’s decision, the scope <strong>of</strong> the InternalContracting <strong>Monitoring</strong> Group has been broadenedto cover monitoring <strong>of</strong> both internally contractedPHDs and non- contracted PHDs. The name <strong>of</strong> thegroup has been changed to the Service Delivery<strong>Monitoring</strong> Group (SDMG), and 5 teams <strong>of</strong> 6members each drawn from senior central level andnational program staff have been established. Theterms <strong>of</strong> reference for the broadened scope <strong>of</strong> theSDMG as well as monitoring tools and schedule <strong>of</strong>visits is currently under finalization.Schedule E – Performance Indicators <strong>of</strong> Annex 12(Service Delivery Management Contract) – havebeen revised based on extensive discussions amongthe MOH, Program staff, and WB during Q4, 2009and Q1, 2010 and was presented at the next SDMGmeeting in May, 2010.7.1.6 SOCIAL SAFEGUARDSSocial safeguards policies have been distributed to all implementing units during launchingworkshops and the documents have been circulated to all provinces. The <strong>Ministry</strong> <strong>of</strong> <strong>Health</strong>’shealth equity funds provide increased access to public health services by the poor, and thisscheme is being expanded. Outreach activities have been implemented in all villages: thesehelp to promote public health services for both prevention and cure, and bring some specificservices such immunization and nutrition directly to the communities. In particular, the newinternal contracting modality includes community participation as a means to promote healthservice utilization and coverage, and this has been implemented by all internally contractedODs, the results <strong>of</strong> which will be monitored through regular quarterly meetings. In the secondquarter <strong>of</strong> 2011, the MOH expects to launch a pilot <strong>of</strong> the Community Score Card interventionwhich will strengthen community involvement and feedback in the health system.7.1.7 ENVIRONMENTAL SAFEGUARDSHospital Waste Management Guidelines for hospital waste management have been developedand implemented. The Department <strong>of</strong> Hospital Services <strong>of</strong> the <strong>Ministry</strong> is responsible forimplementing these guidelines, and has conducted several training workshops for hospital staffin the country. The Building Briefs for CPA and MPA service packages include the provision <strong>of</strong>hospital waste management facilities, and these will be incorporated into the civil worksconstruction and renovation plan.103
Incinerators for disposal <strong>of</strong> hospital waste are provided to all health facilities depending ontheir needs. The design <strong>of</strong> incinerators has been approved through a wide consultative process,and this has been applied at all health facilities.Only pesticide products with WHO pre-qualification, such as Abate and BTI, are purchased forthe Program through WHOPES. Use <strong>of</strong> these products has been monitored by respectiveimplementing units (e.g., Dengue Control Program) with assistance from WHO experts. TheSecretariat has been working closely with the WHO <strong>of</strong>fice to confirm documentary evidence onWHO pre-qualifications.The MOH will enforce efforts to address any concerns relating to water supply provided athealth facilities and carry out remedial measures where required and educate communitymembers in situations where elevated arsenic levels are discovered in sources <strong>of</strong> water supply.Budget for this is included in the civil works budget plan.Sanitation at health facilities have also been discussed and agreed to allocate budget forupgrading the facilities.7.1.8 INVOLUNTARY RESETTLEMENTA resettlement policy (A Framework for Land Acquisition Policy and Procedures) laying out theprocesses in case land acquisition is required was prepared at the time <strong>of</strong> HSSP2 design. Whileno civil works have begun as yet, it is necessary that all relevant MOH <strong>of</strong>ficials gain fullknowledge and understanding <strong>of</strong> the requirements contained in the resettlement policy whichis not currently the case. The Framework needs to be appropriately disseminated and fullyexplained to all concerned staff. Also, the current version <strong>of</strong> the Program Operational Manualdoes not include any information on the resettlement policy as framed, and this needs to beadded. During the next Joint Review Mission the MOH will provide partners with recordsdocumenting that infrastructure investments will occur on public land or, in case <strong>of</strong> new landacquisition, copies <strong>of</strong> land acquisition reports are made available as well. When civil works arelaunched, resettlement policies as agreed to and framed by the RGC will be applied withoutexception. Currently, these policies are being implemented in other sectors, and are beingmanaged through the Inter-Ministerial Resettlement Committee.7.1.9 PROCUREMENTProcurement <strong>of</strong> Consulting Firms and NGOs 2011HSSP2Pooled Fund1. SSS – Extension <strong>of</strong> PwC Contract - External Audit Services HSSP1 (2010, 2011) & HSSP2(Q1, 2011) with an estimated cost <strong>of</strong> USD 15,928 (evaluation in process).2. SSS - Extension <strong>of</strong> SKY Contract – Linkage <strong>of</strong> CBHI and HEF in Kampot Province (2011)(Re-submission <strong>of</strong> Work <strong>Plan</strong> 2011)3. IPA: QCBS – Recruitment <strong>of</strong> firm – Design/Design Review and Detail Engineering forHSSP2 CWs Program with the estimate cost <strong>of</strong> USD 750,000.00 (Bank’s approval on104
Procurement <strong>Plan</strong> 2011). The TOR is now being revised to reflect the change in scope <strong>of</strong>work.4. IPA: QCBS – Recruitment – Construction Supervision for <strong>Health</strong> Facilities in Preah Vihearand Phnom Penh with the contract amount <strong>of</strong> USD 99,594.00 (contract signed)5. IPA: QCBS – Recruitment <strong>of</strong> firm – Integrated Financial and Technical Audit 2011 – 2013with an estimated cost <strong>of</strong> USD 500,000.00 (MOH’s approval on RFP, 21 st Jan 2011).AFD1. SSS - Extension <strong>of</strong> SRC Contract – Institutional Capacity Building in Takeo Province withcost <strong>of</strong> USD 214,731.00 (Negotiation process).2. SSS - Extension <strong>of</strong> SKY Contract – Micro <strong>Health</strong> Insurance with estimate cost <strong>of</strong> USD631,142 (Negotiation process).3. SSS – Selection <strong>of</strong> PwC – Financial Audit for SRC Takeo with estimate cost <strong>of</strong> USD6,500.00 (AFD’s approval).BTC2. QCSB – Recruitment <strong>of</strong> NGO for Administration & Management Cost for HEF – Cluster10 with the contract amount <strong>of</strong> USD 108,792.08.3. QCSB – Recruitment <strong>of</strong> NGO for Administration & Management Cost for HEF – Cluster11 with the contract amount <strong>of</strong> USD 109,600.88.4. QCSB – Recruitment <strong>of</strong> NGO for Administration & Management Cost for HEF – Cluster12 with the contract amount <strong>of</strong> USD 118,826.81.5. QCSB – Recruitment <strong>of</strong> NGO for Administration & Management Cost for HEF – Cluster13 with the contract amount <strong>of</strong> USD 98,626.00.HSSP1ADB/GMS-CDC1. QCS – Recruitment – GMS-CDC1 End <strong>of</strong> Project <strong>Evaluation</strong> with the contract amountUSD 176,116.57GAVI1. QCS – Recruitment – Assessment <strong>of</strong> 24 Hours MPA and <strong>Health</strong> System Strengtheningwith the contract amount <strong>of</strong> USD 31,240.00.2. Extension <strong>of</strong> PwC Contract – External Audit Service 2010 with the estimate cost <strong>of</strong> USD12,375.00 (Negotiation process).Recruitment <strong>of</strong> Individual Consultants105
2010:HSSP2: The consultants have been engaged and extension contracts in 2010 were: (i) ChiefProgram Administrator, (ii) Pooled Fund Management Officer, (iii) Discrete AccountsManagement Officer, (iv) NRHP Program Assistant, (v) M&E Advisor, (vi) FinancialManagement Advisor, (vii) Procurement Advisor, (viii) Chief Procurement Officer, (ix)M&E Officer (2 Positions), (x) Management Assistant, (xi) Chief FinancialManagement Officer, (xii) Senior Discrete Financial Management Officer, (xiii) SeniorPooled Fund Accounts Financial Management Officer, (xiv) Discrete AccountsFinancial Management Officer, (xv) Pooled Fund Accounting Assistant (1 Position),(xvi) Discrete Account Assistant (6 positions), (xvii) Management Assistant, (xviii)Senior Secretary, (xix) Administrative Officer, (xx) Midwifery Associate, (xxi) OfficeClerk, (xxii) Infrastructure Development, (xxiii) International Advisor to Internal AuditDepartment, (xxiv) Drivers (13 positions)HSSP1:BTC:AHI:GAVI:GMS:AFD:The consultants have been engaged in 2010 were: National Construction SupervisionEngineer (2 Positions)The consultants have been engaged and contract extension in 2010 were: TA-<strong>Health</strong>Equity Funds (2 Positions), TA Contract Management (2 Positions), TA-Development<strong>of</strong> District <strong>Health</strong> Systems, TA-Office Administrator, TA Financial ManagementCapacity Building, Drivers (4 Position).The consultant had contract extension in 2010 was: Project AccountantExtension contract <strong>of</strong> M&E OfficerThe consultants who had contracts extension in 2010 were: Project Assistant,Outbreak and Hospital Preparedness expert, Community-based Vector Control, M&EExpert, Project Accountant, Procurement Assistant, Accounting Assistant, Secretary,Drivers (3 Position)<strong>Health</strong> Financing AdvisorUNFPA: Emergency Obstetric & Newborn Midwifery Skills Enhancement Coordinator for NMCH.2011:HSSP2New Contract: The following individual consultants have been engaged in 2011: (i)IT/Communication Officer, (ii); Internal Contracting <strong>Monitoring</strong> Officer; (iii) AdministrativeOfficer; (iv) Senior Secretary/Logistic; (v) Procurement Advisor (under evaluation process); (vi)Chief Procurement Officer (Re-advertisement); (vii) Training Management Officer (underprocessing); Procurement Assistant (2 Positions).Contract Extension: Contract Extension <strong>of</strong> HSSP2 Consultants including International Advisor toInternal Audit Department, Chief Program Administrator, Pooled Fund Management Officer,Discrete Accounts Management Officer, NRHP Program Assistant, M&E Officer (2 Positions),Management Assistant, Chief Financial Management Officer, Senior Discrete Financial106
Management Officer, Senior Pooled Fund Accounts Financial Management Officer, DiscreteAccounts Financial Management Officer, Pooled Fund Accounting Assistant, Discrete AccountAssistant , Drivers (13 positions)BTC consultant contracts extension: (i) TA. Contract Management; (ii) TA DDHS-KC; (iii) TA HEF-KC; (vi) TA-OA-KC; (v) TA-CM-SR; (vi) TA-FMCB-SR; (vii) TA-HEF-SR; (viii) Drivers (4 Positions)HSSP1 consultant contracts extensions: National Construction Supervision Engineer (2Position)GAVI: New Contract: Financial and Administrative Officer (advertisement)AFD: New Contract: NGO Capacity Building OutcomesGMS/CDC2 New Contract: In the effort <strong>of</strong> harmonization and alignment and to effectively use<strong>of</strong> technical assistants, the procurement unit is also responsible for procurement underGMS/CDC2. The Grant effective on 27 March 2011 and the following consultants have beenengaged: (i) Contract <strong>of</strong> GMS2 Consultants; (ii) Project Assistant Manager; (iii) M&E Expert; (iv)Procurement Office; (v) Project Accountant; (vi) Accounting Assistant; (vii) AdministrativeAssistant/Secretary; (viii) Drivers (4 Position).Procurement <strong>of</strong> GoodsShopping:1. Shopping <strong>of</strong> Air-conditioner (14 units) for CDC with total contract amount <strong>of</strong> USD8,988.00 (Delivered).2. Shopping <strong>of</strong> Furniture (7 items) for CDC with total contracts amount <strong>of</strong> USD 8,404.00(Delivered).3. Shopping <strong>of</strong> USB Modem (35 units) for CDC with total contract amount <strong>of</strong> USD 7,925.00(Delivered).4. Shopping <strong>of</strong> Audio Visual Equipment (Digital Video Camera 2 units and Digital Camera 34units) for CDC (On process <strong>of</strong> bidding document).5. Shopping <strong>of</strong> Procurement <strong>of</strong> Oxygen Cylinder Flow Regulator with Humidifier bid No.HSSP2/10/PF/G/06/Shopping6. Shopping <strong>of</strong> Mini Diesel Generator (3 sets) for Ratanakiri Province with contract amount<strong>of</strong> USD 3,480.00 (Delivered)7. Shopping <strong>of</strong> Furniture (Meeting Table 7 units for Ratanakiri, Metal Cupboard 3 units &Metal bookshelves 2 units for DIC with total contract amount <strong>of</strong> USD 1,321.00(Delivered)8. Shopping <strong>of</strong> Urine Pregnancy Test Strip (500 boxes) & Urine Test Strip for Glucose &Protein (250 boxes) with total contract amount <strong>of</strong> USD 4,775.00 for NRHP (on process,contract signed on 21 Apr. 11).9. Shopping <strong>of</strong> Printing (flipchart 3,000 copies & Leaflet 50,000 sheets) with contractamount <strong>of</strong> USD 6,450.00 for DHP Department (Delivered)10. Shopping <strong>of</strong> Printing (4 items: Banner, T-Shirt, Raincoat & Bag) for NMCH and (Jacket)for CDC with total contract amount <strong>of</strong> USD 13,022.00 (Delivered)11. Shopping <strong>of</strong> Security Camera 16 units and DVR Recorder 1 unit (on process <strong>of</strong> BiddingDocument)12. Prepared the process for vehicles insurance for year 2011 (Completed)107
National Competitive Bidding (NCB)1. NCB <strong>of</strong> Printing documents (23 items) for NMCH with total contract amount <strong>of</strong> USD76,440.00 (Delivered)2. NCB <strong>of</strong> Office Equipment (Photocopy 3 units, LCD Projector 9 units, External HD 16 units,USB Flash 20 units & Fax Machine 1 unit) under HSSP2 with total contract amount <strong>of</strong> USD19,839.00 (Delivered)3. NCB <strong>of</strong> audio visual equipment ( Digital Video Camera 7 units, Digital Camera 23 units, TV32”5 units, DVD player 5 units, Microphone 10 units, Amplifier 5 units & Loud Speaker 20units) under HSSP2 with estimate total contract amount <strong>of</strong> USD 27,374.00 (under process <strong>of</strong>bid evaluation)4. Process <strong>of</strong> TV and Radio spots (Mease Vaccination Campaign) broadcasting for NMCH withtotal contract amount <strong>of</strong> USD 73,368.00 (complete)ICB to be carried out by IPAInvolvement <strong>of</strong> HSSP Secretariat in procurement <strong>of</strong> ICB document is to prepare and get Bank’sapproval on procurement plan, prepare technical specifications, organize PRC meeting forreviewing and endorsing bidding documents, negotiate contracts, and manage and monitorcontract implementations. The ICB contract and/or package is:1. CB – Medical Equipment for Svay Rieng Referral Hospital CPA3 (Cost estimate process).108
CHAPTER 8: PROGRAM MONITORING AND EVALUATION8.1 PROGRAM MONITORING ACTIV ITIESNo IUs.Central toPHDCentral toODCentral toRHCentral toHC<strong>Plan</strong> Ach <strong>Plan</strong> Ach <strong>Plan</strong> Ach <strong>Plan</strong> AchNational Programs1 NNP 76 70 76 70 50 37 252 3212 NRH 24 20 N/A N/A N/A N/A 69 693 PMTCT N/A N/A N/A N/A 3 4 20 21Comments4 NIP 111 26 156 95 134 5 Team busy with other taskssuch as AH1N1campaign6 NCHP 21 21 21 22 50 39 24 267 DengueProgram8 HelminthsControlProgram25 25 25 25 6 6 26 2613 13 12 12 12 12 Budget gap between requestand approval, and mountainousareas were difficult to accessTotal 270 175 290 224 109 86 537 480Departments10 DPHI 83 74 43 34 81 67 0 0 Implementation processcomplicated leading toimplementation starting delayand transportation barriers;Limitation in accessing to ODwhich is located far fromprovince capital11 DBF 96 82 0 0 0 0 0 0 No car for transportation andsome staff busy with their dutyat the <strong>of</strong>fice12 HSD 93 90 29 28 189 185 10 10 Difficulty on transportation toprovinces for monitoringbecause, we haven’torganization car and gasoline.Mission by bus is difficult toreach target at health centerlevel13 DPM 0 0 0 0 0 0 102 85 We have difficulty using publictransportation, HSSP2 coverstravel costs only from PhnomPenh to provinces, but does notcover from PHDs to ODs, HCsand communities14 DP 0 0 0 0 0 0 0 0 Extra overload <strong>of</strong> work likecensus and Personneldepartment has not enoughhuman resource to implementall new department functionson SOA and PMASimplementation109
No IUs.Central toPHDCentral toODCentral toRHCentral toHCComments<strong>Plan</strong> Ach <strong>Plan</strong> Ach <strong>Plan</strong> Ach <strong>Plan</strong> Ach15 DDF 198 198 65 75 65 89 160 243 Lack <strong>of</strong> means <strong>of</strong> transportationto perform the activitiesespecially from capital <strong>of</strong>province to district orcommunes16 CDC 150 94 115 94 72 54 150 132 No transport for the spotchecksand supervision for thecentral teams; ad hoc activitiesproposed by developmentpartners and not in the plan;and lack <strong>of</strong> human resources17 Admin 48 48 76 38 40 20 0 0 Public transport cannot reachHCs and far ODs18 HRD (HRDto RTCs)4 2 0 0 0 0 0 0 During 1st quarter, Departmentand Regional Training Centerswere busy with conducting exitexamination for Nursing andMidwifery program and alsorecruitment <strong>of</strong> new intakes forRegional Training Centers andthere were many publicholidays in 2nd quarter.19 DIC 96 62 0 0 0 0 0 0 No means <strong>of</strong> transportationthus difficult to monitor NGOprojects and shortage <strong>of</strong> staff interms <strong>of</strong> number, capacity, andcommitment (DIC is requestingmore staff)20 IAD 11 11 15 15 11 11 14 14 Lack <strong>of</strong> car and petrol21 CMS 0 0 0 0 0 0 0 0Total 779 661 343 284 458 426 436 4848.2 SE RVICE DE LIVERY MONITORING GROUPDuring this reporting period, a number <strong>of</strong> activities were conducted to improve monitoring <strong>of</strong>service delivery in the sector. The MOH established 5 <strong>Monitoring</strong> Teams <strong>of</strong> 6 members eachconsisting <strong>of</strong> senior and mid-level managers from the MOH and national programs to conductquarterly monitoring <strong>of</strong> both SOA and non-SOA provinces. Two consultation workshops wereconducted during this period. The first consultative workshop was conducted on 28 May, 2010in Phnom Penh and wasattended by SDMG membersand PHD representatives underthe chairmanship <strong>of</strong> HE Pr<strong>of</strong>.Tan Vuoch Chheng, UnderSecretary <strong>of</strong> State, MOH andchair <strong>of</strong> the SDMG. Based ondiscussions at the workshop alist <strong>of</strong> action points with clearresponsibilities and deadlineswas formulated for furtheraction. The second consultativeSDMG Team 4 conducting a monitoring visit to a health center inMondulkiri from 27 September to 2 October, 2010.110
workshop was conducted from 22-23 June, 2010 at Preah Sihanouk. The main objectives <strong>of</strong> theworkshop were to draft monitoring tools for each level, finalize TORs for the SDMG, draftmonitoring schedules for the <strong>Monitoring</strong> Teams, decide on reporting formats by PHDs and SOAsand begin discussions on the bonus formula and criteria for release for SDG/SOA. Binders withexisting tools and reference and resource materials prepared by the M&E unit/HSSP2 weredistributed to participants along with the revised list <strong>of</strong> M&E indicators for internal monitoring.Further meetings <strong>of</strong> the SDMG were conducted in October and December, 2010 and March,2011 to address key issues such as target setting methods, procurement, financial reporting,new contracts, bonus payments, methods <strong>of</strong> verification, etc. Details are available in the sectionon SOAsAll <strong>Monitoring</strong> Teams, which began their visits from 15 August, 2010 have conducted field visitsduring this period accompanied on occasion by JPIG members, and at least one team hasalready conducted 3 provincial visits. It is expected that the next SDMG meeting will beconducted in the second week <strong>of</strong> May, 2011.SDMG <strong>Monitoring</strong> Team Visits 2010-11ProvinceDate VisitQuarter 3, 2010Team 1 Kampong Cham 13-17 Sep 2010Team 2 Prey Veng 26 Sep to 1 Oct 010Team 3 Takeo 13-17 Sep 2010Team 4 Mondulkiri27 Sep to 2 Oct2010Team 4 Koh Kong 18-23 Oct 2010Team 5 Ratanakiri 15-21 Aug 2010Team 5 Preah Vihear 22-29 Aug 2010Team 5 Siem Reap26 Sep to 1 Oct2010Team 5 Siem Reap 3-7 Oct 2010Team 5 Kampong Thom11-16 Oct 2010,Non SOAQuarter 1, 2011Team 1 Kampong Cham 28 Feb to 3 March 2011Team 2 Prey Veng 30 Jan to 3 Feb 2011Team 3 Takeo 21-25 Feb 2011Team 4 Mondulkiri 23-26 Feb 2011Team 4 Koh Kong 28 Feb to 5 March 2011Team 5 Ratanakiri 6-12 Feb 2011Team 5 Siem Reap 13-18 Feb 2011Team 5 Preah Vihear 7-12 March 2011111
SDMG Team 1 conducting monitoring visit to Kampong Cham PHD in February 2011.112
ANNEXESANNEX A. A GREED ACTIONS TA KEN ON INTE RNAL CONTROL BA SED ON EXTERNA L AUD IT RE PORTS FOR QUARTE RS I, II & III 2010Quarter I, 20101. CASH AND BANKNo. Funding Issues Implementing Units Action Taken1.1 Petty cash kept in safebox is over thethreshold (US$1,000)1.2 Lack <strong>of</strong> petty cashmanagement in safeboxKg Cham- AHRDHE“Poor Family DevelopmentOrganization”This NGO is newly recruited to implementthe HEF. We had instructed them to followthe financial manual.This NGO is new to the program. We willinstruct to “Poor Family DevelopmentOrganization” not to mix personal cash withprogram cash2. ADVANCES3. EXPENDITURE2.1 Long outstandingadvances2.2 Advance register is notproperly prepared andupdated2.3 Late checking andposting <strong>of</strong> advanceliquidation3.1 Signature on per diempayment sheet andattendant list notproperly controlled3.2 Mission orders, travelvouchers and invoicesare not properlycontrolledAll relevant implementingunitsWe had instructed all implementing units tostrictly follow the guidelines. We will includereport <strong>of</strong> status/with reason <strong>of</strong> outstandingin quarterly reportHSSP2 FMG HSSP has implemented since August 2010HSSP2 FMG HSSP has implemented since August 2010Kampong Thom ProvinceBanteay Meanchey, KgThom, Preah VihearInstructed to refund the amountThe procedure is included in FinancialManual. We will instruct them to follow thefinancial manual.113
No. Funding Issues Implementing Units Action Taken3.3 Overstated payment onuser fees and per diemBanteay Mean Chey PHDand Action for <strong>Health</strong>Banteay Meanchey PHD refunded on 22July 2010 and Action for <strong>Health</strong> will berefunded on 3 September 2010.3.4 Room rental charge forworkshop or seminar3.5 Duplication <strong>of</strong> prenumbereddisbursement vouchersHSSP-FMGNMCH and Poor FamilyDevelopmentWe will issue a letter to MCHC to refundthis amount to programWe will instruct NMCH and Poor FamilyDevelopment to use the single referencevoucher number and which can verify thepayment voucher against the generalledger3.6 Finger print are madeonly when makingpaymentPoor Family DevelopmentWe will issue a formal letter to Poor FamilyDevelopment to follow the auditor’srecommendation.4. TAX ISSUES3.7 Reports onmanagement meetingon the allocation <strong>of</strong>incentive package werenot properly preparedand approved4.1 Tax not deducted onstaff’s salaryAll SOAsWe will instruct to all SOAs to keep theproper meeting minutes in everymanagement meetings.All individual consultant contracts whichhad been approved by the donors andMoEF have no provision <strong>of</strong> salary taxesand on the other hand the salary tax cannotbe paid from the donor funds. If salary taxis required it should have clearly mentionedthat this shall be paid from the counterpartfunds.5. COMPLIANCE6. FIXED ASSETS5.1 Recruitment <strong>of</strong> anInternal Audit Advisornot yet completed6.1 Fixed assets should betaggedPreah VihearThe international Internal audit advisorstarted his services on 18th August 2010.We will instruct to Preah Vihear and followup checking will be made during nextsupervision mission <strong>of</strong> FMG group114
No. Funding Issues Implementing Units Action Taken6.2 Fixed assets countshould be performedregularlyPreah VihearWe will instruct to Preah Vihear, to conductphysical verification <strong>of</strong> fixed assets byindependent person at least once a yearand keep the evidence <strong>of</strong> verificationdocuments and approval <strong>of</strong> managementon verification result properlyQuarter II, 20101. CASH AND BANK1.1 Duties <strong>of</strong> accountantand cashier notproperly segregatedKratieWe will instruct to Kratie province to followthe petty cash box control system strictlyaccording to auditor’s recommendation.1.2 Blank cheques shouldnot be pre-signed1.3 Petty cash kept in safebox is over thethreshold (US$1,000)1.4 Cheque not used forthe payment over USD2001.5 Stamp “Cancelled” notused for wrong chequeSiem ReapTakeo BFHTakeo BFHSihanoukville BFHWe will instruct to Siem Reap to follow theAuditor’s recommendation.We will instruct to Takeo BFH strictly followthe Financial Manual.We will instruct to Takeo BFH strictly followthe Financial Manual.We will instruct to Sihanouk Ville BFHstrictly follow the Financial Manual.2. ADVANCES2.1 Long outstandingadvanceHead Office, Kg Thom,Kampot, Battambang, SvayRieng, Kg Cham, Kg Speu,MCH and CNMWe will remind to those provinces strictlyfollow the Financial Manual to releaseadvance payment for subsequent activitiesafter submission <strong>of</strong> document <strong>of</strong> theprevious advance.2.2 Advance clearancedate should not be thesame as the date <strong>of</strong> theadvance requestKandal, Siem Reap, TakeoPHD Siem Reap. Takeo and Kandalconfirmed they have recorded the date <strong>of</strong>advance request as the date <strong>of</strong> advancereconciliation in the SOE. Management hasinformed and instructed these threeprovinces on this mistake and asked toavoid repeating in future.115
3. EXPENDITURENo. Funding Issues Implementing Units Action Taken3.1 Signature on per diempayment sheet andattendant list notproperly controlledKanda, Kg Chhnang, KgSpeuWe instructed all IUs to respect financialpolicy during 3rd quarter 2010 jointsupervision mission meeting. This practiceis not applicable from 2011 onward. Therepeat mistake will be refunded.3.2 Mission orders, travelvouchers and invoicesare not properlycontrolledSvay Rieng, Kandal, Kratie,Kg Speu, Takeo, NMCHStated in the Financial Manual aboutmission orders, travel vouchers, invoices.We will instruct to them to follow thefinancial manual strictly. Svay Rieng PHD,Kandal and Kratie are local staff withouttravel mission. This participant-instructorsshall have at least a nomination-invitationletter to attend the session. For Kg Speu,it was confirmed the activities wereconducted beyond the duration specified inthe mission order. For NMCH, it was thestaff from OD to join the activities carriedout by NMCHC. Since this had not beenwell informed in advance to OD, themission order was produced very late.Takeo , refund has been made.3.3 Correction on missionorders should not beaccepted3.4 Quotations notobtained for allpurchases <strong>of</strong> overUS$100Kg Thom, Svay Rieng,Kandal, Kg Speu, SiemReap OD, Reproductive<strong>Health</strong> Association.All concern departments.In future , this correction withoutmanagement recognition (no signature) istreated as misconduct. RHAC: we willdiscuss the issue with <strong>Health</strong> Equity FundImplementer and suggest them to postcheck and verify the case.We will remind them to follow this issue notto happen again in future.116
No. Funding Issues Implementing Units Action Taken3.5 Employment contractshould be properlypreparedSamrong ODWe instructed to Samrong OD to prepareproper employment contract. Procurementguideline for SOA is being developed andwill be finalized within Q1 2011.3.6 Disbursement vouchersshould be prenumberedwith unique,sequential referencenumbers3.7 Reports on training orworkshops were notproperly preparedSamrong OD and Action for<strong>Health</strong>Kg Thom, Kg Speu,Smarong OD anf NMCHCWe will remind them to follow this issue notto happen again in future.We have instructed all IUs to submit thereport and at least 2 pictures. HSSPfinance team has included theserequirements in the supervision check list.3.8 Pre-signed andstamped approvals ontravel vouchers shouldnot be accepted3.9 Staff evaluation formsshould be properlymonitored3.10. Expenditures should beproperly calculatedbefore making payment3.11 OperationalDocument’s (OPD)patient listing shouldclearly state theamount <strong>of</strong> payment3.12 Filing systemprocedures forsupporting documentsshould be improved3.13 Adjustments should beproperly adjusted in thecorrect period4. INFORMATION TECHNOLOGY AND GENERAL CONTROLKg ThomSamrong OD and SotnikumODAction for <strong>Health</strong>Organization<strong>Health</strong> Equity FundImplementers and PoorFamily Development.Buddhist for <strong>Health</strong> andTakeo.RHACwe instructed to Kg Thom to follow theissue and ensure not to happen again infuture.we instructed to those provinces to preparestaff performance evaluation forms properlyin the future, SDMG will check on thisevaluation.We instructed Action for <strong>Health</strong> to refundthe overpaid amount.<strong>Health</strong> equity Fund Implementer will checkand verify the cases.We have instructed them to follow theauditor's commentWe will instruct RHAC to record allexpenditure within the reporting period.117
5. TAX ISSUESNo. Funding Issues Implementing Units Action Taken4.1All relevant ImplementingPassword procedureunitsregarding changes andminimum length shouldbe established4.2Procedure to back updata and up date antivirusshould beestablished5.1 Withholding tax onsalary should bedeclared to the taxdepartmentAll relevant ImplementingunitsWe will develop a more comprehensive ITpolicy within the project. HSSP will appointa new IT expert to resolve all IT issuesstarting in 2011We instructed to those provinces to followthe recommendations. HSSP will appoint anew IT expert to resolve all IT issuesstarting in 2011All individual consultant contracts whichhad been approved by the donors andMoEF have no provision <strong>of</strong> salary taxesand on the other hand the salary tax cannotbe paid from the donor funds. If salary taxis required it should have clearly mentionedthat this shall be paid from the counterpartfunds.6. FIXED ASSETS6.1 Fixed asset should betaggedHSSP secretariatFMG will check all fixed assets quarterly inorder to ensure that they are taggedproperly according to respective fundedprogram6.2 Fixed assets count isnot performed regularlyHSSP secretariatWe issued instruction to follow the auditor'srecommendation immediately andsupervise accordingly.Quarter III, 20101. ADVANCES118
No. Funding Issues Implementing Units Action Taken1.1 Long outstandingadvancesHead Office, Kampot,Battambang, Svay Rieng,Kg Cham, Takeo, NMCH,Malaria, BanteayMeanchet, Per vengFor central level could be mitigatedthrough: (1) delegating the activities toprovinces as much as possible;(2) if thereis more than one activity to be conductedone immediately after another, than needto have different persons appointed forclearing advances (3) trying to scheduleactivities with enough time interval forclearing advances; in this case notproviding second advance, if first one is notyet clear.2. EXPENDITURE2.1 Internal control overmission orders andtravel vouchersSvay Rieng, Takeo, Sreambel, Smach Meanchey,Malaria, BanteayMeanchey, PrevengThe Double mission orders were refunded2.2 Pre-signed andstamped approvals ontravel vouchers2.3 Corrections on missionordersMalariaKg Thom, Svay Rieng,BFH, Takeo, CHHRANot permitted to Pre-signed mission orderIn future, this correction withoutmanagement recognition (no signature) istreated as misconduct.2.4 Disbursement vouchersshould be prenumberedwith unique,sequential referencenumbers2.5 Filing systemprocedures forsupporting documentsPoor Family DevelopmentSvay Rieng, BFH, Kirivong,Poor Family Development,Prey Veng.Reminded them not to happen again infuture.Instructed to follow auditor's comments.2.6 Quotations notobtained for allpurchases <strong>of</strong> overUS$100Svay Rieng, Kg Cham,Takeo, Malaria,Reminded them not to happen again infuture.119
No. Funding Issues Implementing Units Action Taken2.7 Reports on training orworkshops were notproperly preparedSmach Meanchey, BTMeanchey, Prey Veng, KohKongWe have instructed all IUs to submit thereport and at least 2 pictures. HSSPfinance team has included theserequirements in the supervision check list.2.8 Expenditures should beproperly calculatedbefore making paymentBFH, KirivongReminded to check before makingpayment. The overstated payment will berefunded.2.9 Control over existenceand accuracy <strong>of</strong>training or workshopsHead <strong>of</strong>fice.Program has requested the Internal Auditorto review the non-existence and this hasbeen confirmed. The payment was madeonly one day workshop. Management willassign staff to spot check some trainingactivities.3. FIXED ASSETS2.10. Employment contractshould be properlyupdatedFixed asset listingshould be properlyupdatedFixed assets should betaggedSre AmbelPreah Vihear ODReproductive <strong>Health</strong>Association <strong>of</strong> Cambodia.We will instruct them to review theemployment contract when it is expired.Informed them to update the fixed assetslisting on quarterly basis.Informed them to tag the fixed assetsbased on the Financial Manual.4.TAX ISSUESWithholding tax onsalary should bedeclared to the TaxDepartmentAll individual consultant contracts whichhad been approved by the donors andMoEF have no provision <strong>of</strong> salary taxesand on the other hand the salary tax cannotbe paid from the donor funds. If salary taxis required it should have clearly mentionedthat this shall be paid from the counterpartfunds.120
ANNEX B. RE CORD OF CONTRAC TS FROM CKPNo Description Contract Number ContractorContractdateAmount <strong>of</strong>ContractPerformanceSecurityAmount <strong>of</strong>PerformanceSecurityExpiry DateFor HSSP1HSSP1-CKP-10-ICB-G-001(Lot-4)Europ Continent22 Feb.2011$155,614.17 FTB $15,561.4118 June20111MedicalEquipmentHSSP1-CKP-10-ICB-G-001(Lot-1)HSSP1-CKP-10-ICB-G-001(Lot-2)Envisioning Co., LtdEnvisioning Co., Ltd21 Feb.201104 Feb.2011$87,095.35 ACLEDA Bank Plc $8,709.53$254,558.72 ACLEDA Bank Plc $25,455.8701 Jun.201109 June2011HSSP1-CKP-10-ICB-G-001(Lot-3)Envisioning Co., Ltd04 Feb.2011$540,262.82 ACLEDA Bank Plc $54,026.2809 June2011For HSSP21MannequinEquipmentHSSP2-CKP-10-NCB-G-008Europ Continent04 Jan.2011$27,613.00 FTB $2,761.3005 May20112MedicalEquipmentHSSP2-CKP-10-ICB-G-005DRC International B.V09 Feb.2011EUR290,342.53Deutsche BankEUR29,034.2630 June2012121
No Description Contract Number ContractorContractdateAmount <strong>of</strong>ContractPerformanceSecurityAmount <strong>of</strong>PerformanceSecurityExpiry Date(Lot-1 & lot-2) $8,096.90 $809.693MedicalEquipmentHSSP2-CKP-10-ICB-G-011Envisioning Co., Ltd31 Mar.2011$203,273.00 ACLEDA Bank Plc $20,327.30 01 July 2011HSSP2-CKP-10-ICB-G-007(Lot-1)Medicom Co., Ltd04 Apr.2011$15,112.97 Mekong Bank $1,512.00 31 July 20114MedicalEquipmentHSSP2-CKP-10-ICB-G-007(Lot-2)Europ Continents04 Apr.2011$62,489.00 FTB $6,248.90 4 July 2011HSSP2-CKP-10-ICB-G-007(Lot-3)Medicom Co., Ltd04 Apr.2011$24,641.02 Mekong Bank $2,465.00 31 July 2011515 units <strong>of</strong>AmbulanceHSSP2-CKP-10-ICB-G-009Automotive ExportSupplies LTD(AESKJAER)04 Apr.2011$409,650.006Material forTeaching &Equipment forTraining/Practice for Calmet,SoviethospitalHSSP2-CKP-10-ICB-G-010(Lot-1)HSSP2-CKP-10-ICB-G-010Dynamic Pharma Co.,LtdComin Khmere Co., Ltd04 Apr.201104 Apr.2011$23,714.00 UCB $2,400.00 29 July 2011$13,936.00 UCB $1,393.00 30 July 2011122
No Description Contract Number ContractorContractdateAmount <strong>of</strong>ContractPerformanceSecurityAmount <strong>of</strong>PerformanceSecurityExpiry Date(Lot-2)HSSP2-CKP-10-ICB-G-010(Lot-3)Envisioning Co., ltd04 Apr.2011$27,402.30 ACLEDA Bank Plc $2,740.23 04 July 20117Text BooksHSSP2-CKP-11-NCB-G-014HSSP2-CKP-11-NCB-G-014Pidana Co., LtdEnvisioning Co., Ltd22 Apr.201122 Apr.2011$72,087.00 ACLEDA Bank Plc $7,208.70 21 July 2011$18,565.95 ACLEDA Bank Plc 1,856.59 18 July 20118OfficeEquipmentHSSP2-CKP-10-ICB-G-012(Lot-1&2)Te Aik Hong OfficeMachine Supplies Co.,Ltd22 Apr.2011$75,681.00 &$42,282.00123
AccountantANNEX C. ADMINISTRA TION OFFICIAL CA D RE IN 2010InstitutionTotalPercentage Dentist(%) DoctorDentist PHD <strong>of</strong> Medical MedicalAssistant Pharmacist Assist DoctorInstitutionTotalPercentage Dentist Dentist PHD <strong>of</strong> Medical Medical Specialist Non-<strong>Health</strong>Others(%) Doctor Assistant Pharmacist Assist Doctor Doctor pr<strong>of</strong>essionalNon-TechnicalStaffPharmacist PharmacistAssistantPhysiotherapistPrimaryDentistPrimaryLabTechnicianPrimaryMidw ifePrimaryNursePrimaryPharmacist Pr<strong>of</strong>essorSecondaryLabTechnicianSecondaryMidw ifeSecondaryNurseX-RayTechnicianIT1. Central1. Central ++4565 24.94 97 15 5 374 11364565 24.94 97 15 5 374 1136 11 184 5 156 225 48 48 0 16 28 183 11 28 242 340 1363 1 23 26MunicipalityMunicipalityMoH 490 2.68 17 2 1 49 135 MoH 490 2.68 17 2 1 49 135 0 76 1 32 84 9 0 0 0 0 4 0 3 2 12 42 0 10 11LeaderLeader16 0.03 5 16 0.03 5 1LevelLevel2 Cabinet 5 0.03 1 2 Cabinet 5 0.03 1 2 1 13 AD 31 0.17 2 1 6 3 3 AD 31 0.17 2 1 6 3 8 4 1 2 2 24 DBF 75 0.41 4 2 4 DBF 75 0.41 4 2 29 18 3 1 4 3 1 105 CDC 66 0.36 10 22 5 CDC 66 0.36 10 22 2 1 1 29 16 DDF 78 0.43 1 1 6 DDF 78 0.43 1 1 7 1 3 62 37 DPHI 35 0.19 5 17 7 DPHI 35 0.19 5 17 9 1 1 28 HSD 50 0.27 3 5 30 8 HSD 50 0.27 3 5 30 7 2 1 1 19 HRD 24 0.13 1 7 11 9 HRD 24 0.13 1 7 11 1 1 1 210 IAD 23 0.13 1 1 8 10 IAD 23 0.13 1 1 8 1311 DIC 11 0.06 6 11 DIC 11 0.06 6 1 1 1 212 PD 24 0.13 2 8 12 PD 24 0.13 2 8 3 2 2 1 2 1 2 113 PMD 28 0.15 9 1 3 11 13 PMD 28 0.15 9 1 3 11 1 1 1 1DG/AdminiDG/Admini14 stration & 6 0.03 2 14 stration & 6 0.03 2 3 1FinanceFinanceDG/TechniDG/Techni1517 0.09 4 5 1517 0.09 4 5 3 1 2 1 1cal <strong>Health</strong>cal <strong>Health</strong>DG/InspectDG/Inspect1611 0.06 1 1 4 1611 0.06 1 1 4 2 3ionsionsNationalNational2151 11.75 35 6 1 119 5502151 11.75 35 6 1 119 550 10 33 1 50 36 9 34 0 5 4 65 2 14 101 135 938 1 0 2HospitalHospitalCalmeteCalmete1514 2.81 1 1 18 127 1514 2.81 1 1 18 127 6 9 11 8 1 6 2 1 4 3 32 48 235 1HospitalHospitalMittapheaMittapheap Khmer-p Khmer-2562 3.07 10 2 41 143 2562 3.07 10 2 41 143 2 11 1 15 11 4 9 3 24 2 4 26 57 197SovietSovietHospitalHospitalKunthakKunthak3 Bopha 182 0.99 7 22 3 Bopha 182 0.99 7 22 1 1 3 3 6 3 9 3 124HospitalHospitalNationalNational4 Pediatric 376 2.05 2 9 87 4 Pediatric 376 2.05 2 9 87 5 9 7 3 5 9 2 20 1 217HospitalHospitalPreahPreah5 Angduong 139 0.76 15 2 1 8 52 5 Angduong 139 0.76 15 2 1 8 52 1 7 1 1 1 1 8 1 5 3 32HospitalHospitalPreahPreah6 Kosamak 378 2.07 7 1 36 119 6 Kosamak 378 2.07 7 1 36 119 1 6 8 6 10 2 14 1 9 23 133 2HospitalHospitalCentralCentral1279 6.99 32 2 3 100 3481279 6.99 32 2 3 100 348 0 71 2 63 87 24 13 0 8 1 34 4 11 121 104 233 0 11 7LevelLevelCambodiaCambodia1 n Red 20 0.11 2 3 1 n Red 20 0.11 2 3 1 12 1 1CrossCross2 CMS 35 0.19 7 2 2 CMS 35 0.19 7 2 5 7 9 2 2 1NationalNationalTB &TB &3167 0.91 17 51 3167 0.91 17 51 5 5 6 3 3 1 1 2 19 54LeprocyLeprocyCentreCentreNationalNational4 AIDS 124 0.68 11 61 4 AIDS 124 0.68 11 61 6 7 3 2 1 6 4 21 2CentreCentre5 NAA 26 0.14 3 14 5 NAA 26 0.14 3 14 5 1 1 1 16National<strong>Health</strong>Promotion50 0.27 9 25 6National<strong>Health</strong>Promotion50 0.27 9 25 5 1 2 1 5 1 17NationalBloodBankCentre40 0.22 2 7 7NationalBloodBankCentre40 0.22 2 7 2 3 2 2 13 98NationalMalariaCentre95 0.52 8 34 8NationalMalariaCentre95 0.52 8 34 4 1 6 5 2 1 1 13 209NationalTraditionalMedication Centre33 0.18 1 5 7 9NationalTraditionalMedication Centre33 0.18 1 5 7 3 2 9 3 1 2124
10 NIPH 84 0.46 4 23 10 NIPH 84 0.46 4 23 9 2 6 1 2 29 5 3Lab <strong>of</strong>Lab <strong>of</strong>DrugDrug11 Quality 39 0.21 2 1 11 Quality 39 0.21 2 1 6 1 17 3 1 3 4 1ControllinControllingg12 NMCH 326 1.78 1 25 70 12 NMCH 326 1.78 1 25 70 12 12 10 3 20 1 15 90 66 1PasteurPasteur1331 0.17 1 10 1331 0.17 1 10 2 5 3 1 5 4InstituteInstitute14 TSMC 84 0.46 2 11 14 TSMC 84 0.46 2 11 3 1 4 10 3 10 10 28 215 UHS 125 0.68 32 1 4 29 15 UHS 125 0.68 32 1 4 29 7 2 7 1 1 4 1 9 7 13 5 2MunicipalitMunicipality 645 3.52 13 5 106 103645 3.52 13 5 106 103 1 4 1 11 18 6 1 3 23 80 5 18 89 150 2 6y2.2. Provincial13737 75.06 92 49 0 713 1003 Provincial13737 75.06 92 49 0 713 1003 9 117 18 730 239 54 80 21 67 1787 3176 16 0 182 1523 3792 11 11 47LevelLevelBanteayBanteay1 Meanchey 898 4.91 7 5 39 51 1 Meanchey 898 4.91 7 5 39 51 2 69 7 1 1 1 10 97 222 1 12 110 255 6 2PHDPHDBattambanBattamban21387 7.58 7 4 72 68 21387 7.58 7 4 72 68 3 130 24 5 4 3 20 122 267 2 12 222 422g PHDg PHDBattambanBattamban347 0.26 1 347 0.26 1 3 1 1 1 13 27g RTCg RTCKampong4Cham PHD 1387 7.58 11 1 68 103 4 Kampong1387 7.58 11 1 68 103 14 42 20 3 12 1 1 194 281 14 153 459 1 1 8Cham PHDKampongKampong526 0.14 3 1 1 526 0.14 3 1 1 1 1 6 12 1Cham RTCCham RTCKampongKampong6 Chhnang 530 2.9 3 2 26 33 6 Chhnang 530 2.9 3 2 26 33 2 11 13 4 4 2 2 89 173 1 5 51 108 1PHDPHDKampongKampong7714 3.9 3 2 38 83 7714 3.9 3 2 38 83 1 2 14 14 4 8 1 1 62 250 1 13 58 156 1 1 1Speu PHDSpeu PHDKampong8Thom PHD 626 3.42 4 1 24 40 8 Kampong626 3.42 4 1 24 40 12 91 12 2 2 101 150 1 15 54 115 1 1Thom PHDKampotKampot9808 4.41 7 2 39 46 9808 4.41 7 2 39 46 3 3 85 15 3 6 2 1 89 140 1 12 108 243 1 2PHDPHDKampotKampot1044 0.24 1 5 1044 0.24 1 5 1 2 1 7 27RTCRTCKandalKandal111070 5.85 10 11 62 124 111070 5.85 10 11 62 124 2 24 15 63 31 9 9 3 3 132 175 3 19 111 261 2 1PHDPHDKoh KongKoh Kong12167 0.91 2 1 11 18 12167 0.91 2 1 11 18 5 6 3 1 2 16 21 1 4 23 49 1 1 2PHDPHD13 Kratie PHD 503 2.75 1 1 28 14 13 Kratie PHD 503 2.75 1 1 28 14 2 16 9 1 1 84 147 2 52 143 2Kep VilleKep Ville1494 0.51 2 4 12 1494 0.51 2 4 12 2 2 5 2 9 23 1 11 21PHDPHDPailin VillePailin Ville15133 0.73 1 14 15 15133 0.73 1 14 15 2 16 1 1 10 32 12 29PHDPHDMondulkiriMondulkiri16169 0.92 3 13 7 16169 0.92 3 13 7 2 12 1 1 1 33 39 1 10 44 2PHDPHDOddorOddor17225 1.23 1 19 15 17225 1.23 1 19 15 1 3 1 1 28 75 2 19 59 1MeancheyMeancheyPreah18Vihea PHD 263 1.44 6 14 18 Preah263 1.44 6 14 4 10 4 1 3 61 56 3 1 23 75 2Vihea PHDPrey VengPrey Veng191020 5.57 8 3 89 68 191020 5.57 8 3 89 68 1 6 55 11 2 7 1 183 346 13 47 173 1 6PHDPHDPursatPursat20532 2.91 1 4 22 33 20532 2.91 1 4 22 33 10 2 22 9 2 11 46 63 1 6 105 191 1 3PHDPHDRattanakRattanak21280 1.53 1 1 7 16 21280 1.53 1 1 7 16 1 1 12 4 2 56 91 3 13 68 4Kiri PHDKiri PHDSiem ReapSiem Reap22729 3.98 3 1 32 65 22729 3.98 3 1 32 65 4 15 17 7 14 8 95 140 1 5 106 211 1 4PHDPHDPreahPreah23292 1.6 4 2 16 34 23292 1.6 4 2 16 34 1 8 11 1 1 25 45 6 43 94 1SihanoukSihanoukSteung24Treng PHD 259 1.42 1 5 9 24 Steung259 1.42 1 5 9 2 1 17 1 1 53 65 1 31 71 1Treng PHDSteungSteung2523 0.13 1 2523 0.13 1 1 1 1 3 16Treng RTSTreng RTSSvay RiengSvay Rieng26484 2.64 3 2 24 47 26484 2.64 3 2 24 47 7 8 3 4 2 1 64 183 6 30 98 2PHDPHD27 Takeo PHD 1027 5.61 8 3 53 81 27 Takeo PHD 1027 5.61 8 3 53 81 1 7 19 17 5 4 4 137 190 28 102 365 3Total 1 + 2 18302 100 189 64 5 1087 2139 Total 1 + 2 18302 100 189 64 5 1087 2139 20 301 23 886 464 102 128 21 83 1815 3359 27 28 424 1863 5155 12 34 73TotalTotal82998299WomenWomenTotal Men 10003 Total Men 10003125
ANNEX D. IND ICA TOR BY PROV INCE AND OD (NUMERATORS ONLY)126
127
128
129
130
131
132
133