Endotracheal Intubation
Endotracheal Intubation
Endotracheal Intubation

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
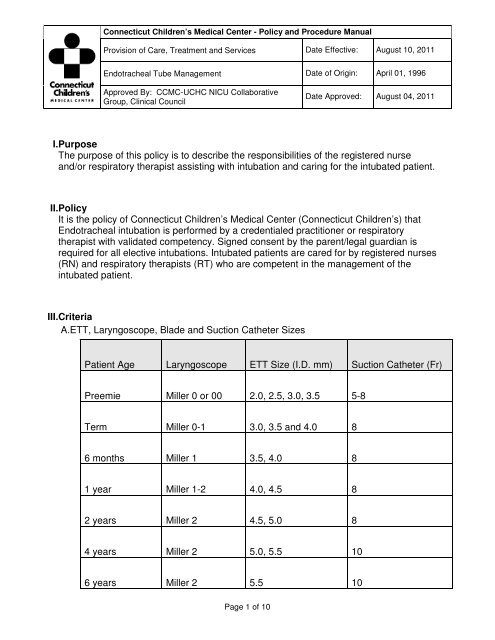
Connecticut Children’s Medical Center - Policy and Procedure ManualProvision of Care, Treatment and Services Date Effective: August 10, 2011<strong>Endotracheal</strong> Tube Management Date of Origin: April 01, 1996Approved By: CCMC-UCHC NICU CollaborativeGroup, Clinical CouncilDate Approved: August 04, 2011B.Equipment/Supplies1.<strong>Endotracheal</strong> Tube (ETT)2.Laryngoscope handle and blade3.Stylet (optional) (available in adult and pediatric sizes)4.End Tidal CO Detector5.Magill Forceps (optional)6.12 ml syringe (optional)7.Tape8.Scissors9.2” x 2” gauze10.Tincture of Benzoin (optional)11.Disposable gloves12.Self inflating bag, anesthesia bag, or T-piece resuscitator and appropriate sizedmask13.PEEP valve, if patient needs PEEP > 5 cm H 2 O14.Suction set-up with catheters and/or Yankauer (optional)15.O 2 flowmeter with nipple connected to oxygen source16.Stethoscope17.Oral airway (optional)18.NG tube19.Tape measure20.Patient monitors (Pulse Oximetry, Cardiorespiratory)21.For patients in the Neonatal Intensive Care Unit (NICU): Hydrocolloid dressing orother barrier and securing device22.Personal protective equipment23.Sterile saline for catheter clearanceIV.GuidelinesA.<strong>Intubation</strong>1.Explain the procedure to the patient and/or family, if appropriate. Engage ChildLife Specialist when appropriate.2.Verify that suction equipment and oxygen source are available and in workingorder.3.Assemble supplies and equipment. Assure patient is on appropriate monitors.4.Refer to the table above under criteria when selecting ETT, Laryngoscope, Bladeand Suction Catheter Sizes. (When a cuffed tube is requested, consider using ahalf-size smaller than what would otherwise be selected.5.Attach blade to laryngoscope handle and snap blade into functioning position toensure battery and fiberoptic light source function.Page 3 of 10
Connecticut Children’s Medical Center - Policy and Procedure ManualProvision of Care, Treatment and Services Date Effective: August 10, 2011<strong>Endotracheal</strong> Tube Management Date of Origin: April 01, 1996Approved By: CCMC-UCHC NICU CollaborativeGroup, Clinical CouncilDate Approved: August 04, 20116.Prepare the ETT. Person performing intubation may choose cuffed or uncuffedETT depending on patient needs. To test the integrity of the cuffed ETT, inflatethe cuff with air, depress both the pilot balloon and cuff to test for any leakage,then remove all the air from the ETT cuff.7.Insert the stylet, if appropriate. Keep the end of the ETT inside the sterilepackaging to maintain sterility. Be sure the end of the stylet does not protrude fromthe tip of the ETT (end inserted into patient)8.Prepare tape strips (hydrocolloid barrier/securing device) to secure the ETT onceinserted. Strips should be long enough to reach across the child’s face from onecheek to the other.9.Prepare Tincture of Benzoin.10.Administer pain medication and/or sedation as ordered. This may includeadministration of a neuromuscular blocking agent (paralytic).11.Ventilate with positive pressure ventilation using anesthesia bag, self-inflating bag,or T-piece resuscitator and O 2 to maintain adequate saturation, heart rate andcolor.12.Pre-suction the patient’s airway prior to intubation, if indicated. Assist theintubating practitioner in positioning the child’s head, and handing equipment andsupplies during ETT insertion.13.Monitor the patient’s heart rate, respiratory rate, and oxygen saturations duringintubation. Notify intubating practitioner of any significant changes.14.Once the ETT has been placed, with manual ventilation in progress, one personholds the ETT in position, while the other person auscultates to confirm bilaterallyequal breath sounds, and visualizes to ensure symmetrical chest rise.15.An exhaled carbon dioxide (CO 2) detector is used to confirm that the ETT is in thetrachea and not in the esophagus. A CO detector is attached between the ETTand the anesthesia, self inflating bag, or T-piece resuscitator. The patient ismanually ventilated with several breaths. A device specific color change indicatesplacement in the trachea. A pediatric CO 2 detector is used for patients under15kg. The end tidal CO 2 detector is less reliable for extremely low birth weightinfants who have small tidal volumes, and is less reliable in patients incardiopulmonary arrest. For these situations alternate confirmation methods maybe indicated.16.Apply benzoin to both cheeks; let dry until it becomes tacky. Secure the ETT inposition using tape strips. In the NICU: Place thin hydrocolloid on cheeks; applybenzoin only to hydrocolloid—avoid direct use on skin whenever possible. Utilizesecuring device to stabilize ETT when appropriate.17.Measure the ETT from the end of the tube where the adapter is attached to thepatient’s lip or securing device. Record measurement on the patient’s flow sheet.Alternatively, make note of the ETT marking that appears at the patient’s lip, ifvisible, and document.18.Approximate insertion depth, in centimeters from midtrachea to lip:Page 4 of 10
Connecticut Children’s Medical Center - Policy and Procedure ManualProvision of Care, Treatment and Services Date Effective: August 10, 2011<strong>Endotracheal</strong> Tube Management Date of Origin: April 01, 1996Approved By: CCMC-UCHC NICU CollaborativeGroup, Clinical CouncilDate Approved: August 04, 20114.Unless the tapes need changing, loosen only the tapes securing the ETT (not thecord clamp).5.Advance or withdraw the ETT as ordered. Verify placement by comparingmeasurements of ETT. .6.Apply benzoin to the ETT and re-secure tapes.7.Assess the patient’s breath sounds. Placement should be confirmed by X-ray.C.Care of the Patient with an ETT1.All intubated patients are monitored with oxygen saturation and cardio-respiratorymonitors. Monitor for complications, such as pneumothorax or other air leak,atelectasis, pneumonia or malpositioned ETT.2.All ventilator settings shall be checked and documented hourly. Assess vital signsand respiratory status in accordance with Connecticut Children’s policy, unlessotherwise ordered(refer to unit specific policy). Monitor and document patientresponse to ventilator changes.3. Assess abdomen for distention when vital signs are performed.4.Placement of a nasogastric or orogastric tube may be indicated to relieve gastricdistention and assist ventilation.5.Institute supportive measures/positioning to promote comfort, respiratoryexcursion, and gas exchange.D.Suctioning with Closed Suction System1.See Closed Suction System policy.2.Note: Suctioning an ETT is performed as a sterile procedure (sterile suctioncatheter and sterile gloves).3.Suctioning is performed as needed for increased peak inspiratory pressures,adventitious breath sounds, increased work of breathing, decreased O 2saturations, etc, unless otherwise ordered,.4.Explain the procedure to the patient/family as appropriate.5.Generally, two caregivers (RN, RT, credentialed practitioner) should perform theprocedure to ensure safety and to maintain sterility of equipment. Hyperoxygenationbefore and in between suction passes may be indicated if the patientis known to have significant desaturations with ETT suctioning. May use manualbreaths from the ventilator, self inflating bag, anesthesia bag, or T-pieceresuscitator.6.Normal saline drops should only be instilled if the patient has thick, tenacioussecretions, and previous attempts to remove secretions without saline have beenunsuccessful. (Instillation of normal saline solution to facilitate secretion removal isnot evidence based.)7.Determine the proper catheter level for suctioning:a)Approximate the length of the ETT from the proximal adapter to the tip.Page 6 of 10
Connecticut Children’s Medical Center - Policy and Procedure ManualProvision of Care, Treatment and Services Date Effective: August 10, 2011<strong>Endotracheal</strong> Tube Management Date of Origin: April 01, 1996Approved By: CCMC-UCHC NICU CollaborativeGroup, Clinical CouncilDate Approved: August 04, 2011b)Correlate this length to a point on the suction catheter.c)Sterilely insert the suction catheter into the ETT ensuring that catheter does notreach more than 0.5-1 cm beyond this lengthd)Apply suction and hold while withdrawing the catheter in a quick, smooth motionfor no longer than 10 seconds per passE.Note: Closed Suctioning System allows the above procedure above (D.4a.throughDf.) to be performed without disconnecting the patient from the ventilator. The systemitself is sterile. Caregiver hands should be washed thoroughly before the procedure,but sterile gloves are not required.F.Determine the proper catheter level for suctioning:1.Ensure the tip of the Y adaptor touches a marked whole centimeter number on theETT (e.g., 18 cm on the ETT).2.Add 5.5 cm to the whole number in the previous step for the correct catheterlength (e.g., 18 cm + 5.5 cm = 23.5 cm) or match the number or color on thesuction catheter with the number on the ETT.3.Advance the catheter until the calculated number is aligned with the lavage port.4.Apply suction and hold while withdrawing the catheter in a quick, smooth motionfor no longer than 10-15 seconds per pass.5.Closely observe the patient’s oxygen saturation, heart rate, and color during theprocedure.6.Repeat the procedure only until the ETT has cleared of secretions. Avoidunnecessary repeated passes, since suctioning can cause damage to the trachealmucosa, and suctioning causes acute alveolar hypoxia which may result in anincrease in pulmonary vascular resistance.7.Observe and document color, character and volume of secretions.G.Patient Safety1.ETT position and security is confirmed at minimum every 4 hours. This is doneeither by visualizing ETT marking appearing at the patient’s lip, or measuring thedistance from the patient’s lip to the end of the ETT. Findings are compared tothose previously documented to determine whether the tube has migrated in orout. If a discrepancy is noticed, discuss plan with credentialed practitioner.2.If the credentialed practitioner orders that the tube be moved in or out, suctionoropharynx to remove pooled secretions, deflate cuff if present, and reinflate oncenew position is achieved. Secure as above, confirm placement, and documentprocedure and new measurement or marking.Page 7 of 10
Connecticut Children’s Medical Center - Policy and Procedure ManualProvision of Care, Treatment and Services Date Effective: August 10, 2011<strong>Endotracheal</strong> Tube Management Date of Origin: April 01, 1996Approved By: CCMC-UCHC NICU CollaborativeGroup, Clinical CouncilDate Approved: August 04, 20113.The tape securing the ETT should be replaced as needed to keep the tube incorrect position. Changing the tape is a two-person procedure. The credentialedpractitioner may order sedation and/or paralytics in order to avoid unintentionalremoval of ETT during the procedure. Verify that all settings are sufficient toadequately ventilate while patient is sedated or paralyzed. Adjust settings asordered.4.Caregivers must take every measure to prevent unintentional removal of the ETT,including adequate sedation, positioning to alleviate tension on the tube, restraintsper credentialed practitioner order, assisting ancillary personnel with procedures,i.e., CXR. Care must be taken to prevent ventilator tubing from becoming kinked,tangled or snagged by other tubes or equipment used in the management of thepatient.5.Skin assessment under and around the tape and ETT is done with mouth care.Consider repositioning or retaping the ETT if skin is reddened or if tube hasremained in the same position for several days. Thin hydrocolloid dressing or otherbarrier may be applied under tape for protection of skin.H.Ventilator Associated Pneumonia Prevention1.Intubated patients should receive mouth care every 2 - 4 hours.2.Moisten oral mucosa and lips as needed.3.Intubated patients should have the head of bed at 30-45 o (15-30 o for patients < 1year of age, 12-15° in the NICU) unless contraindicated.4.Ventilator tubing should be maintained in a dependent position to prevent “rainout”from flowing backward toward the patient and down the ETT. If excess wateror condensation exists do not drain back into the humidifier, considerdisconnecting tubing briefly, emptying water, and removing additional tubing thatmay be collecting water (ex: Cold foot segment of Fisher Paykel circuit).5.Reposition patient at a minimum of every 2 hours (NICU, per unit protocol)6.Maintain strict sterility of any equipment connected to or used in the care of theendotracheal tube.7.Maintain separate suction set-ups for endotracheal and oral/nasal suctioning.8.Suction the mouth before suctioning the ETT to prevent oral secretions from beingaspirated when ETT is suctioned.9.Follow hand washing guidelines.I.Extubation1.Ensure credentialed practitioner order has been received and documented prior toextubation.2.Evaluate sedative and narcotic doses and consider caffeine loading for neonatesprior to extubation.3.Explain procedure to patient/family as appropriate.4.Elevate the head of bed.Page 8 of 10
Connecticut Children’s Medical Center - Policy and Procedure ManualProvision of Care, Treatment and Services Date Effective: August 10, 2011<strong>Endotracheal</strong> Tube Management Date of Origin: April 01, 1996Approved By: CCMC-UCHC NICU CollaborativeGroup, Clinical CouncilDate Approved: August 04, 20115.Ensure that the equipment for the desired mode of post-extubation oxygendelivery or CPAP is set-up and functional.6.Have suction and oxygen available, with necessary supplies (self inflating,anesthesia bag, or T-piece resuscitator, mask, suction catheters). If the child hasa cuffed ETT, obtain an empty 3-10 ml syringe to deflate the cuff prior to ETTremoval.7.Suction the mouth, nose, and ETT prior to removal. Chest Physiotherapy may bebeneficial. Deflate the ETT cuff, if appropriate. Consider hyper-oxygenation of thepatient for several minutes prior to extubation.8.Holding the ETT in position, gently loosen and remove the tape from the child’sface.9.Disconnect the ETT from the ventilator, and quickly and smoothly remove the ETTfrom the patient’s airway.10.Position patient for optimal airway capacity.11.Encourage the patient to cough and to take deep breaths if cognitively able tofollow commands.12.Gently suction the oropharynx/nasopharynx as needed.13.Establish new mode of support, per credentialed practitioner order (e.g., hood,nasal cannula, face-mask, nasal CPAP).J.Post-extubation Monitoring1.Assess vital signs, color, respirations, breath sounds, work of breathing, andoxygen saturation immediately following extubation.2.Monitor respiratory effort, rate, and presence of stridor. Evaluate the patient’scolor, perfusion, activity, and oxygen saturation closely for several hours until thepatient is stable.3.A post-extubation blood gas is typically sent 1 hour after extubation and thenrepeated based on the patient’s condition.4.Consider using transcutaneous CO 2 or non-invasive ETCO 2 monitoring.5.Turn and reposition patient every 2 hours (2-4 hours in the NICU) if the patient isnot moving him/herself to promote drainage and prevent stasis of secretions.Suction as needed.6.If atelectasis is present, the patient should be encouraged to take deep breathsevery 2-4 hours while awake. This can be done with an incentive spirometer,blowing bubbles or other breathing techniques. Alternately, Intermittent PositivePressure Breathing (IPPB), Intrapulmonary Percussive Ventilation (IPV), and/orchest physiotherapy may be indicated for those patients who cannot comply with acoughing and deep breathing regime.7.For post extubation stridor, notify the credentialed practitioner, position patient foroptimal airway capacity. Administer inhaled racemic epinephrine as ordered.K.DocumentationPage 9 of 10
Connecticut Children’s Medical Center - Policy and Procedure ManualProvision of Care, Treatment and Services Date Effective: August 10, 2011<strong>Endotracheal</strong> Tube Management Date of Origin: April 01, 1996Approved By: CCMC-UCHC NICU CollaborativeGroup, Clinical CouncilDate Approved: August 04, 20111.Document procedure (intubation or extubation) and patient’s response in theProgress Notes.2.Record ventilator settings, and any changes in settings, as well as tube positionconfirmations on the patient flow sheet and/or RT ventilator sheets.3.Document response to changes in therapy in the progress notes. .4.Record all vital signs and assessments on the flow sheet.5.Record medications on the MAR.6.Record each time the patient is suctioned on the flow sheet; document volume andcharacteristics of secretions.7.Record all blood gas results on the flow sheet.8.Document interventions performed in oral care, and those for promotion of skinintegrity and comfort in the medical record.V.ReferencesAACN Procedure Manual for Pediatric Acute and Critical Care, Saunders (Elsevier),2008, pp 5-34.VI.Related DocumentsClosed Suction SystemChest Physiotherapy (CPT)Oxygen Management in the NICUOxygen Therapy ProcedureMedication Administration and DocumentationNasal or Oral Enteral Tube Insertion and UseNeuromuscular Blocking AgentsPain Assessment and ManagementSkin Integrity and Wound Risk AssessmentUse of Restraint for the Protection of Invasive DevicesVentilator-Associated Pneumonia Reduction Strategies GuidelineVital Signs Policy- NICUAssessment and Reassessment of PatientsPage 10 of 10