Pseudoasbestos Bodies and Fibers in Bronchoalveolar Lavage of ...
Pseudoasbestos Bodies and Fibers in Bronchoalveolar Lavage of ...
Pseudoasbestos Bodies and Fibers in Bronchoalveolar Lavage of ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Pseudoasbestos</strong> <strong>Bodies</strong> <strong>and</strong> <strong>Fibers</strong> <strong>in</strong> <strong>Bronchoalveolar</strong><strong>Lavage</strong> <strong>of</strong> Refractory Ceramic Fiber UsersPASCAL DUMORTIER, INGRID BROUCKE, <strong>and</strong> PAUL DE VUYSTChest Department, Hôpital Erasme, Université Libre de Bruxelles, Brussels, BelgiumRefractory ceramic fibers (RCF) are widely used to replace asbestos<strong>in</strong> applications requir<strong>in</strong>g high heat resistance. Ferrug<strong>in</strong>ousbodies mimick<strong>in</strong>g asbestos bodies (ABs) have been detected <strong>in</strong> thelungs <strong>of</strong> RCF production workers. This raises the question abouttheir presence <strong>in</strong> other occupational groups <strong>and</strong> whether “typicalABs” still reflect past asbestos exposures <strong>in</strong> all sett<strong>in</strong>gs. An ABcount<strong>in</strong>g by phase-contrast light microscopy <strong>and</strong> a screen<strong>in</strong>g testby analytical electron microscopy were systematically performedon all bronchoalveolar lavage fluids (BALF) submitted to our laboratory<strong>in</strong> 1992 through 1997 (n 1,800). When RCF were detected<strong>in</strong> electron microscopy, the structures considered as “typicalABs” were marked under light microscopy <strong>and</strong> prepared forfurther chemical <strong>and</strong> structural analysis. Pseudo-ABs on RCF weredetected <strong>in</strong> samples from n<strong>in</strong>e subjects (0.5%). All <strong>of</strong> them hadworked either as foundry workers, steel workers, or welders. Inthese subjects, alum<strong>in</strong>o-silicate fibers compatible with RCF accountedfor 42% <strong>of</strong> the core fibers analyzed, other nonasbestos fibersfor 28%, <strong>and</strong> asbestos fibers for 30%. ABs thus rema<strong>in</strong> a validmarker <strong>of</strong> asbestos retention but attention must be paid to a possibleoccurrence <strong>of</strong> pseudo-asbestos bodies on RCF <strong>and</strong> other nonasbestosfibers <strong>in</strong> end-users <strong>of</strong> refractory fibers.Keywords: asbestos; refractory ceramic fibers; biopersistence; bronchoalveolarlavage fluid; transmission electron microscopyInhaled particles <strong>and</strong> fibers deposited <strong>in</strong> the lungs are usuallyphagocytized by alveolar macrophages. Ferrug<strong>in</strong>ous bodiesresult from the deposition <strong>of</strong> an iron-rich prote<strong>in</strong> layer at thecell–particle <strong>in</strong>terface <strong>of</strong> biopersistent fibers or particles that aretoo large to be completely phagocytized. Ferrug<strong>in</strong>ous bodiesmostly form on particles larger or fibers longer than 10 m (1,2). They may occur on a wide variety <strong>of</strong> materials, <strong>in</strong>clud<strong>in</strong>gasbestos fibers, sheet silicates, diatomaceous earth, coal particles,metal compounds, <strong>and</strong> silicon carbide (3–5). The mechanismslead<strong>in</strong>g to ferrug<strong>in</strong>ous bodies formation are not fullyunderstood. Experimental evidence suggests that they couldbe formed by an exocytotic activity <strong>of</strong> macrophages or giantcells (6). In rodents, coated fibers can be detected <strong>in</strong> light microscopypreparations 2 to 3 mo after exposure (2).Coated asbestos fibers are referred to as asbestos bodies(ABs). In light microscopy the central core <strong>of</strong> a “typical” ABis a th<strong>in</strong>, straight, transparent, <strong>and</strong> colorless fiber. The fiber iscovered by a regularly segmented or cont<strong>in</strong>uous golden yellowto red brown coat<strong>in</strong>g. Some branched or curved forms can beobserved (1, 3, 7). The validity <strong>of</strong> this def<strong>in</strong>ition is supported(Received <strong>in</strong> orig<strong>in</strong>al form December 5, 2000 <strong>and</strong> <strong>in</strong> revised form April 10, 2001)This work was partly supported by Grant 3.4525.97 from the Fonds de la RechercheScientifique Médicale. I. Broucke was supported by a grant from the FondationErasme.Correspondence <strong>and</strong> requests for repr<strong>in</strong>ts should be addressed to P. Dumortier,Chest Department, CUB Hôpital Erasme, Route de Lennik 808, B1070 Brussels,Belgium. E-mail: pdumorti@ulb.ac.beThis article has an onl<strong>in</strong>e data supplement, which is accessible from this issue’stable <strong>of</strong> contents onl<strong>in</strong>e at www.atsjournals.orgAm J Respir Crit Care Med Vol 164. pp 499–503, 2001Internet address: www.atsjournals.orgby numerous electron microscopy analyses which have demonstratedthat 95 to 98% <strong>of</strong> the core fibers <strong>of</strong> structures correspond<strong>in</strong>gto this def<strong>in</strong>ition are <strong>in</strong>deed asbestos fibers (1, 8).Most ABs are built on amphibole asbestos fibers <strong>and</strong> the ABburden correlates with the amphibole content <strong>of</strong> the lung (9).ABs on chrysotile have been observed <strong>in</strong> subjects recently exposedto this type <strong>of</strong> fiber despite its shorter biopersistence(7). Concentrations above 1 AB/ml <strong>in</strong> bronchoalveolar lavagefluid (BALF) or above 1,000 AB/g dry lung tissue <strong>in</strong>dicatenontrivial asbestos exposure, <strong>and</strong> the concentrations <strong>of</strong> ABs <strong>in</strong>BALF <strong>and</strong> lung tissue are correlated (10).Typical ABs can usually be dist<strong>in</strong>guished from other ferrug<strong>in</strong>ousbodies. The latter have brown to black cores or broadtransparent to yellow cores, usually with an irregular coat<strong>in</strong>g(3). The terms “ferrug<strong>in</strong>ous body” <strong>and</strong> “pseudo-asbestos body”are equally used for these atypical structures. In this article,we will use the term “ferrug<strong>in</strong>ous body” for atypical structureseasy to dist<strong>in</strong>guish from ABs <strong>in</strong> rout<strong>in</strong>e phase-contrast lightmicroscopy <strong>and</strong> restrict the term “pseudo-asbestos body”(pseudo-AB) to structures that look like typical ABs but arebuilt on nonasbestos core fibers.Pseudo-ABs form at least on erionite (11) <strong>and</strong> on refractoryceramic fibers (RCF) (12, 13). Because erionite exposureis limited to a few villages <strong>in</strong> Cappadocia (Turkey), pseudo-ABs on erionite do not really <strong>in</strong>terfere with evaluation <strong>of</strong> occupationalasbestos exposures.Pseudo-ABs on RCF have been occasionally described <strong>in</strong>BALF (13) <strong>and</strong> lung tissue (12) <strong>of</strong> RCF production workers.RCF are man-made vitreous fibers produced from a meltedmixture <strong>of</strong> Al 2 O 3 <strong>and</strong> SiO 2 or from calc<strong>in</strong>ed kaol<strong>in</strong> clay. Otheroxides, such as ZrO 2 , B 2 O 3 , TiO 2 , <strong>and</strong> Cr 2 O 3 , can be added <strong>in</strong>order to change the fiber properties. They are used to replaceasbestos <strong>in</strong> high-temperature <strong>in</strong>sulation such as <strong>in</strong>sulation <strong>of</strong>furnaces <strong>and</strong> kilns; high-temperature filtration; <strong>and</strong> refractoryblankets, papers, felts, <strong>and</strong> textiles. Production <strong>of</strong> RCF wasuncommon before the 1970s. RCF represent 1 to 2% <strong>of</strong> thecurrent total production <strong>of</strong> man-made vitreous fibers. BesidesRCF, refractory fibers made <strong>of</strong> crystall<strong>in</strong>e alum<strong>in</strong>um oxide orcrystall<strong>in</strong>e zirconium oxide are also produced (14).The <strong>in</strong>creas<strong>in</strong>g use <strong>of</strong> RCF raises the question whether “typicalABs” still reflect asbestos exposures <strong>in</strong> all sett<strong>in</strong>gs. Thisstudy concerns the occurrence <strong>of</strong> RCF <strong>and</strong> other refractory fibers<strong>in</strong> rout<strong>in</strong>e electron microscopy analyses.METHODSEach year, approximately 300 BALF samples from cl<strong>in</strong>ical or medicolegalcases are referred to our laboratory for fiber or particle analysis.For each sample the referr<strong>in</strong>g chest physician is requested to fill <strong>in</strong>a questionnaire on cl<strong>in</strong>ical data, occupational <strong>and</strong> environmentalbackground, <strong>and</strong> the type <strong>of</strong> particles that must be searched for. Becausethe questionnaire is rarely fully completed, we have developeda rout<strong>in</strong>e analytical procedure to m<strong>in</strong>imize the possibility to overlookunsuspected exposures. It <strong>in</strong>cludes an AB <strong>and</strong> uncovered fiberscount<strong>in</strong>g by light microscopy <strong>and</strong> a quick evaluation <strong>of</strong> the particulateburden through a screen<strong>in</strong>g test by analytical transmission electronmicroscopy.
500 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 164 2001Additional <strong>in</strong>formation about BALF sampl<strong>in</strong>g, preparation, <strong>and</strong>exam<strong>in</strong>ation by light <strong>and</strong> electron microscopy is available <strong>in</strong> the onl<strong>in</strong>edata supplement.If RCF were detected as pseudo-ABs core or uncoated fibers dur<strong>in</strong>gthe electron microscopy screen<strong>in</strong>g test, the light microscopy slideswere reexam<strong>in</strong>ed. Some typical ABs were r<strong>and</strong>omly selected, exam<strong>in</strong>ed<strong>in</strong> natural light at a higher magnification (400 to 1,250),marked with a high-precision object marker (15), <strong>and</strong> photographed.These marked bodies were transferred to electron microscopy grids<strong>and</strong> their core fiber was analyzed by energy-dispersive spectrometry <strong>and</strong>measured. This allowed us to determ<strong>in</strong>e the percentage <strong>of</strong> true <strong>and</strong>pseudo-ABs conta<strong>in</strong>ed <strong>in</strong> a BALF <strong>and</strong> to compare their morphologic<strong>and</strong> optical characteristics.The concentration <strong>of</strong> ABs, pseudo-ABs, <strong>and</strong> fibers <strong>and</strong> their size(width, length, <strong>and</strong> aspect ratio) are presented as geometric mean(GM) (geometric st<strong>and</strong>ard deviation [GSD] 95% confidence <strong>in</strong>terval;[CI]). Mann-Whitney U tests were used to compare fiber sizes.RESULTSPatientsBetween January 1, 1992 <strong>and</strong> December 31, 1997, BALF samplesfrom 1,800 patients were exam<strong>in</strong>ed. AB counts were 1AB/ml BALF <strong>in</strong> 617 (34%) patients <strong>and</strong> 5 AB/ml BALF <strong>in</strong>310 (17%). The electron microscopy screen<strong>in</strong>g test revealedalum<strong>in</strong>o-silicate fibers compatible with RCF as pseudo-ABscores or uncovered fibers <strong>in</strong> the BALF <strong>of</strong> n<strong>in</strong>e <strong>of</strong> 1,800 patients.Demographic, occupational, <strong>and</strong> cl<strong>in</strong>ical data <strong>and</strong> the<strong>in</strong>dication for the m<strong>in</strong>eralogical analysis <strong>of</strong> BALF are reported<strong>in</strong> Table 1. The n<strong>in</strong>e patients had all been work<strong>in</strong>g <strong>in</strong>foundries, steelworks, or as welders. All patients were stillwork<strong>in</strong>g <strong>in</strong> possible contact with RCF when BALF was performed,except Patient 6 who had worked as a radiology technicianfor 9 yr. Exposure to RCF was never reported <strong>in</strong> the occupationalhistory given by the referr<strong>in</strong>g physician.BALF AB, Pseudo-AB, <strong>and</strong> Ferrug<strong>in</strong>ous Body ContentTable 2 summarizes the results <strong>of</strong> the m<strong>in</strong>eralogical analyses.All 9 patients had more than 1 typical AB/ml <strong>in</strong> BALF <strong>and</strong>seven had more than 5 typical AB/ml. Altogether, 257 structures(237 typical ABs <strong>and</strong> 20 uncovered fibers) were marked<strong>and</strong> analyzed (Figures 1 <strong>and</strong> 2). Several types <strong>of</strong> nonasbestoscore fibers were identified. They were distributed <strong>in</strong>to six categories(Si Al, Al Si, Si, Al, Fe, no signal) accord<strong>in</strong>g tothe major peaks detected <strong>in</strong> the chemical spectra. Amorphousalum<strong>in</strong>o-silicate fibers accounted for 42% <strong>of</strong> the body coresanalyzed, other nonasbestos fibers for 28%, <strong>and</strong> asbestos for30%. Nonasbestos core fibers accounted for 50% or more <strong>in</strong>five <strong>of</strong> the n<strong>in</strong>e patients. Although electron diffraction <strong>in</strong>dicatedthat the silicon-, alum<strong>in</strong>um-, <strong>and</strong> iron-rich fibers had acrystall<strong>in</strong>e structure, <strong>in</strong>terpretable electron diffraction patternscould not be obta<strong>in</strong>ed.No dist<strong>in</strong>ction could be made between the different core fibersdur<strong>in</strong>g rout<strong>in</strong>e phase-contrast light microscopy analysis. Someiron-rich core fibers could, however, be discrim<strong>in</strong>ated ow<strong>in</strong>g totheir reddish-brown color when exam<strong>in</strong>ed under natural light athigher magnification (1,000) with oil immersion objectives.Dur<strong>in</strong>g the period covered by the study, two other patientspresented with pseudo-ABs on crystall<strong>in</strong>e silica <strong>and</strong> on crystall<strong>in</strong>eiron oxide core fibers, but no RCF. They had bothpseudo-AB concentration greater than 5/ml <strong>of</strong> BALF. Interest<strong>in</strong>gly,these two patients were respectively work<strong>in</strong>g as agr<strong>in</strong>der <strong>and</strong> as a trimmer <strong>in</strong> two different foundries.Pseudo-AB Size ParametersCore fibers <strong>of</strong> pseudo-ABs were thicker, shorter, <strong>and</strong> hadlower aspect ratios than those <strong>of</strong> true ABs from our database(Table 3). When comparisons were performed accord<strong>in</strong>g toasbestos fiber type, pseudo-ABs core fibers are thicker <strong>and</strong>longer than crocidolite <strong>and</strong> chrysotile core fibers (p 0.005),shorter than amosite core fibers (p 0.005), but have diametersimilar to amosite (GM [GSD; 95% CI]:0.24 m [1.92; 0.22to 0.26]; p 0.23) <strong>and</strong> tremolite (0.31 m [2.09; 0.29 to 0.34];p 0.079) <strong>and</strong> length similar to tremolite (33.6 m [1.57; 31.9to 35.4]; p 0.136) core fibers. Among pseudo-ABs, 50% <strong>of</strong>the core fibers were longer than 30 m <strong>and</strong> th<strong>in</strong>ner than 0.5 m.Most pseudo-ABs fibers (71%) were th<strong>in</strong>ner than 0.4 m <strong>and</strong>few (10%) were thicker than 1 m.Quantitative chemical analysis <strong>of</strong> fibers <strong>and</strong> other observationsmade on the BALF <strong>of</strong> these patients are reported <strong>and</strong>discussed <strong>in</strong> the onl<strong>in</strong>e data supplement.DISCUSSIONWe report the presence <strong>of</strong> coated <strong>and</strong> uncoated RCF <strong>in</strong> BALF.It was not possible to make a dist<strong>in</strong>ction between pseudo-ABsTABLE 1. EXPOSURE AND CLINICAL DATA OF THE PATIENTS WITH RCF IN BALF SAMPLESCaseNo.Age(yr)ReportedOccupationDuration(yr) Cl<strong>in</strong>ical Data* Suspected Exposure1 37 Gr<strong>in</strong>der <strong>in</strong> a foundry 9 N Asbestos, metalsBlowlamp operator load<strong>in</strong>g 5<strong>and</strong> unload<strong>in</strong>g <strong>of</strong> furnaces2 25 Gr<strong>in</strong>der <strong>in</strong> steelworks 3 N Asbestos, ‡ metals3 42 Furnace clean<strong>in</strong>g <strong>in</strong> a foundry 20 Progressive massive fibrosis Asbestos, silica4 54 Furnace worker 14 N Asbestos5 37 Furnace mason 10 Pleural effusion Asbestos6 39 Furnace <strong>in</strong>stallation <strong>and</strong> 6 Pulmonary <strong>and</strong> pleural Asbestos, coal, silicadismantl<strong>in</strong>gfibrosis <strong>of</strong> upper zonessecondary to radiationtherapy for Hodgk<strong>in</strong>’slymphoma7 50 Concrete preparator 1 Pleural plaques † Asbestos, coal, alum<strong>in</strong>um, rock woolFurnace worker <strong>in</strong> steelworks 3Foundry worker 1Boiler welder 288 40 Welder 25 Pleural effusion Asbestos9 52 Furnace worker <strong>in</strong> steelworks 27 Pleural plaques † Asbestos* N No detectable pulmonary or pleural abnormality.†Confirmed by CT scan.‡Possible environmental exposure to tremolite asbestos <strong>in</strong> Turkey until the age <strong>of</strong> 19.
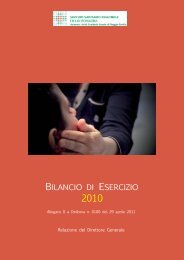
Dumortier, Broucke, <strong>and</strong> De Vuyst: Pseudo-asbestos <strong>Bodies</strong> on RCF 501TABLE 2. CONCENTRATION OF FIBERS AND BODIES IN BALF SAMPLES OF PATIENTS IN WHOM RCFs WERE DETECTEDCaseNo.TypicalAB/mlLight MicroscopyUF/mlElectron MicroscopyNumber<strong>of</strong> Typical % with% <strong>of</strong> Each Type <strong>of</strong> Nonasbestos Core Fiber §AtypicalFB/mlABsAnalyzedNonasbestosCore Fiber Si Al Al Si Si Al Fe No signal1 † 29 11 20 105 97.1 23.8 19 29.5 4.8 202 22 1.9 3 33 84.8 33.3 30.3 3 18.23 41 5.3 3.6 19 84.2 47.4 10.5 15.8 5.3 5.34 8.2 16 ND 12 83.3 66.7 16.75 1.2 116 ND 20* 50* 20* 30*6 8.7 11 ND 15 26.7 6.7 207 ‡ 28 20 0.3 21 28.6 14.3 4.8 9.58 6.8 1.6 ND 16 12.5 12.59 2.5 0.16 ND 16 12.5 12.5Mean 53.3 24.8 15.6 5.9 3.1 2.8 1.1Def<strong>in</strong>ition <strong>of</strong> abbreviations: AB asbestos body, FB ferrug<strong>in</strong>ous body, ND not detected; UF = uncovered fiber longer than 10 m.* The number <strong>of</strong> typical ABs was low, <strong>and</strong> analyses were performed on 20 uncovered fibers located <strong>and</strong> marked under light microscopy.†Mean concentration from three BAL samples (second <strong>and</strong> third samples obta<strong>in</strong>ed, respectively, 32 <strong>and</strong> 47 mo after the first one).‡Mean concentration <strong>of</strong> two samples (second sample obta<strong>in</strong>ed 13 mo after the first one).§Categories def<strong>in</strong>ed accord<strong>in</strong>g to the ma<strong>in</strong> peaks <strong>in</strong> energy-dispersive X-ray spectrometry.on RCF <strong>and</strong> true ABs when apply<strong>in</strong>g the morphologic or opticalcharacteristics rout<strong>in</strong>ely used for light microscopy ABcount<strong>in</strong>g. Indeed, the various types <strong>of</strong> pseudo-ABs would nothave been detected <strong>in</strong> the absence <strong>of</strong> the systematic electronmicroscopy screen<strong>in</strong>g test performed on all the BALF samplesexam<strong>in</strong>ed <strong>in</strong> our laboratory. For the period exam<strong>in</strong>ed (1992through 1997), significant amounts <strong>of</strong> pseudo-ABs on RCF<strong>and</strong> other refractory fibers were observed <strong>in</strong> respectively 0.5%<strong>of</strong> all the patients exam<strong>in</strong>ed, 1.5% <strong>of</strong> those with 1 AB/ml,<strong>and</strong> 2.3% <strong>of</strong> those with 5 AB/ml BALF. Moreover, pseudo-ABs formed only on other types <strong>of</strong> nonasbestos core fibers(crystall<strong>in</strong>e silica <strong>and</strong> crystall<strong>in</strong>e iron oxide) were detected <strong>in</strong>two additional patients. All cases were revealed as a result <strong>of</strong>the abundance <strong>of</strong> pseudo-ABs or <strong>of</strong> RCF. The sensitivity <strong>of</strong>the electron microscopy screen<strong>in</strong>g test to detect bodies <strong>and</strong> fibersis much lower than that <strong>of</strong> light microscopy. In particular,when true ABs largely outnumber pseudo-ABs or if there areonly a few bodies, the presence <strong>of</strong> pseudo-ABs is more likelyto rema<strong>in</strong> undetected. It is thus possible that there were additionalcases to those reported <strong>and</strong> that the forego<strong>in</strong>g percentagesare underestimated.There are no data about the presence <strong>of</strong> pseudo-ABs on RCF<strong>and</strong> other refractory fibers <strong>in</strong> the lungs <strong>of</strong> patients exam<strong>in</strong>ed beforethe end <strong>of</strong> 1991. Accord<strong>in</strong>gly, it is not possible to concludeon any time trends <strong>in</strong> the occurrence <strong>of</strong> such fibers <strong>in</strong> BALF, buttheir relative occurrence <strong>in</strong> comparison with asbestos fibers willprobably <strong>in</strong>crease with <strong>in</strong>creas<strong>in</strong>g replacement <strong>of</strong> asbestos byRCF <strong>in</strong> <strong>in</strong>dustrial sett<strong>in</strong>gs where high heat resistance is required.The patients were exposed as end-users or by work<strong>in</strong>g <strong>in</strong>the vic<strong>in</strong>ity <strong>of</strong> sources <strong>of</strong> refractory fibers <strong>and</strong> were never employed<strong>in</strong> the production <strong>of</strong> these fibers. Interest<strong>in</strong>gly, all thesubjects had been exposed <strong>in</strong> foundries, steelworks, or aswelders. Exposure to refractory fibers had not been suspected,<strong>and</strong> a confusion with asbestos exposure <strong>in</strong> the occupationalhistory reported <strong>in</strong>itially by the patients or the referent physiciansis obvious (Table 1). This reflects the similar applications<strong>of</strong> these two k<strong>in</strong>ds <strong>of</strong> fibers <strong>and</strong> the lack <strong>of</strong> <strong>in</strong>formation aboutthe actual exposure conditions <strong>of</strong> patients us<strong>in</strong>g RCF.Figure 1. Light (A) <strong>and</strong> transmissionelectron microscopy (B)views <strong>of</strong> the same pseudo-ABon a RCF. Energy-dispersiveX-ray spectrometry chemicalcomposition spectrum (C) wasobta<strong>in</strong>ed from the fiber segment<strong>in</strong>dicated by an arrow.
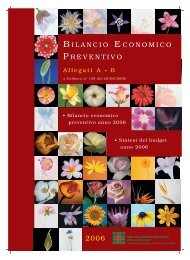
502 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 164 2001Figure 2. Light (A) <strong>and</strong> transmissionelectron microscopy (B)views <strong>of</strong> the same pseudo-ABon a crystall<strong>in</strong>e iron compoundfiber. Energy-dispersive X-rayspectrometry chemical compositionspectrum (C) was obta<strong>in</strong>edfrom the fiber segment<strong>in</strong>dicated by an arrow.The detection <strong>of</strong> refractory fibers <strong>in</strong> the lungs confirms therelease <strong>of</strong> respirable fibers <strong>in</strong> the work environment <strong>of</strong> the patients.Mean airborne fiber concentrations measured dur<strong>in</strong>g<strong>in</strong>stallation or removal <strong>of</strong> RCF furnace <strong>in</strong>sulation are close to1 fiber/ml air (16), but concentrations as high as 23 f/ml havebeen detected (17). This contrasts with the current fiber concentrationsat workplace <strong>in</strong> RCF production plants whichrarely exceed 1 fiber/ml (16, 18, 19). Similarly, the heaviest exposures<strong>and</strong> the highest number <strong>of</strong> asbestos-exposed workerswere also not necessarily found <strong>in</strong> the production <strong>of</strong> asbestosor <strong>of</strong> asbestos-conta<strong>in</strong><strong>in</strong>g products.On the other h<strong>and</strong>, the variety <strong>of</strong> fiber types observed <strong>in</strong>the BALF <strong>of</strong> our patients, <strong>in</strong>clud<strong>in</strong>g asbestos, silica-rich, <strong>and</strong>iron-rich fibers together with various refractory fibers, <strong>and</strong> thepresence <strong>of</strong> elevated concentrations <strong>of</strong> nonfibrous particles,reflects the complexity <strong>of</strong> mixed exposures <strong>in</strong> foundries, steelworks,<strong>and</strong> weld<strong>in</strong>g. The most probable hypotheses for silicarich,alum<strong>in</strong>um-rich, <strong>and</strong> iron-rich fibers are respectively siliconcarbide (5) or silica, alum<strong>in</strong>um oxide refractory fibers, <strong>and</strong>iron oxide (20) fibers released at workplace.Although RCF are reported to be fibrogenic <strong>and</strong> carc<strong>in</strong>ogenic<strong>in</strong> animal experiments (21), there is no evidence <strong>in</strong> epidemiologicstudies on RCF production workers <strong>of</strong> an associationbetween workplace exposure <strong>and</strong> an <strong>in</strong>creased risk <strong>of</strong>lung fibrosis, lung cancer, or mesothelioma (18, 22, 23). Thismust nevertheless be <strong>in</strong>terpreted with caution, because <strong>of</strong> thesmall number <strong>of</strong> exposed workers <strong>in</strong> the cohorts [n 628 forthe European study (18) <strong>and</strong> n 652 for the U.S. study (23),respectively], the relatively short surveillance period, <strong>and</strong> theaverage low levels <strong>of</strong> exposure ( 1 fiber/ml air). Consequently,it is not yet possible to draw def<strong>in</strong>itive conclusions on the riskssuch exposures may cause for exposed workers. In addition tothe observations from production workers, cohorts data areneeded concern<strong>in</strong>g end-users who may be exposed to higherfiber levels <strong>and</strong> to mixtures <strong>of</strong> dusts.Radiologic studies have shown a possible association betweenexposure to RCF <strong>and</strong> pleural plaques (22, 23), althoughthis has not been confirmed by computed tomographic (CT)scan studies. The occurrence <strong>of</strong> pleural plaques after low-dosecumulative exposures to RCF is, however, plausible, by analogywith what has been observed with asbestos. In our series,however, the two patients with typical pleural plaques (Patients7 <strong>and</strong> 9) had a majority <strong>of</strong> asbestos fibers as body cores.The chest X-ray <strong>of</strong> Patient 3 show<strong>in</strong>g a progressive massive fibrosiswith large opacities was more consistent with the diagnosis<strong>of</strong> silicosis than <strong>of</strong> asbestosis or idiopathic lung fibrosis.In Patient 8, benign asbestos-<strong>in</strong>duced pleural effusion wasconsidered as the most probable diagnosis. Other studies haveTABLE 3. DIMENSIONS OF THE CORE FIBERS OF TRUE AND PSEUDO-ABsPseudo-asbestos<strong>Bodies</strong>Asbestos <strong>Bodies</strong>(All types)Mann-Whitneyp ValueNumber <strong>of</strong> core fibers analyzed 125 1,081Diameter, mGM (GSD; 95% CI) 0.27 (2.6; 0.23–0.32) 0.14 (2.8; 0.13–0.15) 0.0001Range 0.01–2.0 0.01–1.65Length, mGM (GSD; 95% CI) 35.4 (1.9; 32.2–39.0) 31.8 (1.74; 30.8–32.9) 0.01Range 6–338 5–276Aspect ratioGM (GSD; 95% CI) 136 (2.8, 113–163) 219 (2.6; 207–232) 0.0001Range 15–2,300 15–6,300
Dumortier, Broucke, <strong>and</strong> De Vuyst: Pseudo-asbestos <strong>Bodies</strong> on RCF 503also <strong>in</strong>dicated a possible promot<strong>in</strong>g effect <strong>of</strong> RCF on airwaysobstruction <strong>in</strong> smokers (18).Last but not least, despite the widespread use <strong>of</strong> glass wool,rock wool, <strong>and</strong> slagwool for <strong>in</strong>sulation, we were unable to detectferrug<strong>in</strong>ous bodies on such fibers <strong>in</strong> the whole series <strong>of</strong>1,800 electron microscopy screen<strong>in</strong>g tests. Only one alteredrock wool structure was detected. This is largely <strong>in</strong> accordancewith the hypothesis that those materials ma<strong>in</strong>ly release nonrespirablefibers or that these fibers are not biopersistent (24).ConclusionsAB count<strong>in</strong>g <strong>in</strong> BALF or lung tissue rema<strong>in</strong>s <strong>in</strong> most cases avalid marker <strong>of</strong> asbestos exposure but attention must be paidto a possible occurrence <strong>of</strong> ferrug<strong>in</strong>ous bodies on nonasbestosfibers <strong>in</strong> end-users <strong>of</strong> RCF. Targeted electron microscopic fiberanalysis <strong>in</strong> BALF is helpful if exposure to such fibers issuspected. The RCF detected <strong>in</strong> BALF showed size characteristicssimilar to those <strong>of</strong> amphibole asbestos fibers. Occupationalgroups at risk <strong>of</strong> exposure to RCF should be identified<strong>and</strong> airborne fiber measurements need to be performed toevaluate exposure levels <strong>in</strong> these groups. Preventive protectionmeasures must be taken to m<strong>in</strong>imize the exposure <strong>of</strong>these workers.References1. Churg AM, Warnock ML. Asbestos <strong>and</strong> other ferrug<strong>in</strong>ous bodies; theirformation <strong>and</strong> cl<strong>in</strong>ical significance. Am J Pathol 1981;102:447–456.2. Morgan A, Holmes A. The enigmatic asbestos body: its formation <strong>and</strong>significance <strong>in</strong> asbestos-related disease. Environ Res 1985;38:283–292.3. Churg A, Warnock ML, Green N. Analysis <strong>of</strong> the cores <strong>of</strong> ferrug<strong>in</strong>ous(asbestos) bodies from the general population: II. True asbestos bodies<strong>and</strong> pseudoasbestos bodies. Lab Invest 1979;40:31–38.4. De Vuyst P, V<strong>and</strong>e Weyer R, De Coster A, March<strong>and</strong>ise FX, DumortierP, Ketelbant P, Jedwab J, Yernault JC. Dental technician’s pneumoconiosis.Am Rev Respir Dis 1986;68:131–140.5. Dufresne A, Loosereewanich P, Armstrong B, Infante-Rivard C, PerraultG, Dion C, Massé S, Bég<strong>in</strong> R. Pulmonary retention <strong>of</strong> ceramic fibers<strong>in</strong> silicon carbide (SiC) workers. Am Ind Hyg Assoc J 1995;56: 490–498.6. Koerten HK, de Bruijn JD, Daems WT. The formation <strong>of</strong> asbestos bodiesby mouse peritoneal macrophages: an <strong>in</strong> vitro study. Am J Pathol1990;137:121–134.7. De Vuyst P, Dumortier P, Moul<strong>in</strong> E, Yourassowsky N, Yernault J. Diagnosticvalue <strong>of</strong> asbestos bodies <strong>in</strong> bronchoalveolar lavage fluid. AmRev Respir Dis 1987;136:1219–1224.8. Dumortier P, De Vuyst P, Strauss P, Yernault J. Asbestos bodies <strong>in</strong>bronchoalveolar lavage fluids <strong>of</strong> brake l<strong>in</strong><strong>in</strong>g <strong>and</strong> asbestos cementworkers. Br J Ind Med 1990;47:91–98.9. Warnock ML, Isenberg W. Asbestos burden <strong>and</strong> the pathology <strong>of</strong> lungcancer. Chest 1986;89:20–26.10. De Vuyst P, Karjala<strong>in</strong>en A, Dumortier P, Pairon J, Monso E, BrochardP, Teschler H, Tossava<strong>in</strong>en A, Gibbs A. Guidel<strong>in</strong>es for m<strong>in</strong>eral fiberanalyses <strong>in</strong> biological samples: report <strong>of</strong> the ERS work<strong>in</strong>g group. EurRespir J 1998;11:1416–1426.11. Sebastien P, Gaudichet A, Bignon J, Baris Y. Zeolite bodies <strong>in</strong> humanlungs from Turkey. Lab Invest 1981;44:420–425.12. Roggli VL. Rare pneumoconiosis: metalloconiosis. In: Saldana M, editor.Pathology <strong>of</strong> pulmonary disease. Philadelphia: JB Lipp<strong>in</strong>cott; 1994.p. 411–422.13. Sébastien P, Vergnon J, Blanchard O, Wastiaux A, Emonot A. Durability<strong>of</strong> ceramic fibers <strong>in</strong> the human lung: prelim<strong>in</strong>ary results. Ann OccupHyg 1994;38(Suppl 1):723–730.14. De Vuyst P, Dumortier P, Swaen GMH, Pairon JC, Brochard P. Respiratoryhealth effects <strong>of</strong> man-made vitreous (m<strong>in</strong>eral) fibres. EurRespir J 1995;8:2149–2173.15. Dumortier P, De Vuyst P. Object mark<strong>in</strong>g, a bridge between light <strong>and</strong>analytical electron microscopy for particle characterization. J ElectronMicrosc Techn 1988;8:229–230.16. Maxim LD, Kelly WP, Walters T, Waugh R. A multiyear workplacemonitor<strong>in</strong>gprogram for refractory ceramic fibers. Regul ToxicolPharmacol 1994;20:S200–S215.17. Strubel G, Faul L. Pollutant load caused by ceramic fibers <strong>and</strong> new resultsabout their behaviour <strong>of</strong> recrystallization. Ann Occup Hyg 1994;38(Suppl 1):713–722.18. Trethowan WN, Burge PS, Rossiter CE, Harr<strong>in</strong>gton JM, Calvert IA.Study <strong>of</strong> the respiratory health <strong>of</strong> employees <strong>in</strong> seven European plantsthat manufacture ceramic fibres. Occup Environ Med 1995;52:97–104.19. Rice CH, Lockey JE, Lemasters GK, Lev<strong>in</strong> LL, Staley P, Hansen KR.Estimation <strong>of</strong> historical <strong>and</strong> current employee exposure to refractoryceramic fibers dur<strong>in</strong>g manufactur<strong>in</strong>g <strong>and</strong> related operations. Appl OccupEnviron Hyg 1997;12:54–61.20. Dodson R, O’Sullivan M, Corn C, Garcia J, Stocks J, Griffith D. Analysis<strong>of</strong> ferrug<strong>in</strong>ous bodies <strong>in</strong> bronchoalveolar lavage from foundryworkers. Br J Ind Med 1993;50:1032–1038.21. Hesterberg TW, Hart GA, Chevalier J, Miiller WC, Hamilton RD,Bauer J, Thevenaz P. The importance <strong>of</strong> fiber biopersistence <strong>and</strong> lungdose <strong>in</strong> determ<strong>in</strong><strong>in</strong>g the chronic <strong>in</strong>halation effects <strong>of</strong> X607, RCF1, <strong>and</strong>chrysotile asbestos <strong>in</strong> rats. Toxicol Appl Pharmacol 1998;153:68–82.22. Lemasters G, Lockey J, Rice C, McKay R, Hansen J, Lu J, Lev<strong>in</strong> L,Gartside P. Radiographic changes among workers manufactur<strong>in</strong>g refractoryceramic fiber <strong>and</strong> products. Ann Occup Hyg 1994;38(Suppl1):745–751.23. Lockey J, Lemasters G, Rice C, Hansen K, Lev<strong>in</strong> L, Shipley R, Spitz H,Wiot J. Refractory ceramic fiber exposure <strong>and</strong> pleural plaques. Am JRespir Crit Care Med 1996;154:1405–1410.24. McDonald JC, Case BW, Enterl<strong>in</strong>e PE, Henderson V, McDonald AC,Plourde M, Sébastien P. Lung dust analysis <strong>in</strong> the assessment <strong>of</strong> pastexposure <strong>of</strong> man-made m<strong>in</strong>eral fiber workers. Ann Occup Hyg 1990;34:427–441.