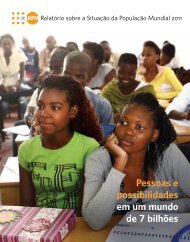
FOCUS ONDemographic trends for adolescents:Ten key factsFigure 2.1: Adolescent population (10–19 years) by region, 2009Industrializedcountries118 millionLatin Americaand Caribbean108 millionCEE/CIS58 millionEastern andSouthern Africa91 millionWest andCentral Africa94 millionMiddle East andNorth Africa84 million• In 2009, there were 1.2 billion adolescents aged 10–19 in the world,forming 18 per cent of world population. Adolescent numbers havemore than doubled since 1950.• The vast majority of adolescents – 88 per cent – live in developingcountries. The least developed countries are home to roughly 1 inevery 6 adolescents.• More than half the world’s adolescents live in either the South Asiaor the East Asia and Pacific region, each of which contains roughly330 million adolescents.East Asia and Pacific329 millionSouth Asia335 million• On current trends, however, the regional composition of adolescentsis set to alter by mid-century. In 2050, sub-Saharan Africa is projectedto have more adolescents than any other region, marginally surpassingthe number in either of the Asian regions.Source: United Nations, Department of Economic and Social Affairs,Population Division, World Population Prospects: The 2008 Revision,, accessed October 2010.Figure 2.2: Trends in the adolescent population, 1950–2050Population in millions1400120010008006004002000World1950 1960 1970 1980 1990 2000 2010 2020 2030 2040 2050Developing countriesSource: United Nations, Department of Economic and Social Affairs,Population Division, World Population Prospects: The 2008 Revision,, accessed October 2010.Least developed countriesIndustrialized countries• India has the largest national population of adolescents (243 million),followed by China (207 million), United States (44 million), Indonesiaand Pakistan (both 41 million).• Adolescents account for only 12 per cent of people in the industrializedworld, reflecting the sharp ageing of Europe and Japan in particular. Incontrast, adolescents account for more than 1 in every 5 inhabitants ofsub-Saharan Africa, South Asia and the least developed countries.• Adolescent boys outnumber girls in all regions with data available,including the industrialized countries. Parity is closest in Africa, with995 girls aged 10–19 for every 1,000 boys in Eastern and SouthernAfrica and 982 girls per 1,000 boys in West and Central Africa, whilethe gender gap is greatest in both Asian regions.• At the global level, adolescents’ share of the total populationpeaked in the 1980s at just over 20 per cent.• Although adolescent numbers will continue to grow in absolute termsuntil around 2030, adolescents’ share of the total population is alreadydeclining in all regions except West and Central Africa and will steadilydiminish all over the world through 2050.• One trend that will continue to intensify in the coming decades isthat ever more adolescents will live in urban areas. In 2009, around50 per cent of the world’s adolescents lived in urban areas. By 2050,this share will rise to almost 70 per cent, with the strongest increasesoccurring in developing countries.See References, page 78.20THE STATE OF THE WORLD’S CHILDREN 2011
are a regular threat in urban areas, and rising affluence –with attendant increases in traffic volume – may accountfor the higher road fatalities recently seen in Asia and theeastern Mediterranean. Boys are more prone than girlsto injury and death from such accidents as well as fromviolence stemming from chance encounters or organizedgang conflict. Because the rate of urbanization is mostrapid in the poorest regions of sub-Saharan Africa andSouth Asia – which are also the areas with the greatestshare of adolescents in the population – averting injuriesin the second decade of life must become a major internationalhealth objective. 4Tobacco consumption and drug and alcohol use aregrowing health risks for adolescentsIn part, injuries arise from a propensity to take risks thatis a common feature of adolescence, connected with thepsychological need to explore boundaries as part of thedevelopment of individual identity. Such readiness to takerisks leads many adolescents to experiment with tobacco,alcohol and other addictive drugs without sufficient understandingof the potential damage to health or of other longtermconsequences of addiction, such as being drawn intocrime to pay for a habit.The most common addiction is cigarette smoking, a habit thatalmost all tobacco users form while in their adolescent years.It is estimated that half the 150 million adolescents who continuesmoking will in the end die from tobacco-related causes. 5Risky behaviours often overlap: A 2007 UNICEF report onchild poverty in Organisation for Economic Co-operation andDevelopment (OECD) countries indicated that adolescentswho smoke are three times more likely to use alcohol regularlyand eight times more likely to use cannabis. 6Nutritional statusAdolescent females are more prone to nutritionaldifficulties than adolescent malesIn early childhood (0–4 years), the available internationalevidence suggests that differences in nutritional statusbetween girls and boys are statistically negligible in allregions except South Asia. 7 As the years pass, however,girls run a greater risk than boys of nutritional difficulties,notably anaemia. Data from 14 developing countries showa considerably higher incidence of anaemia among femaleadolescents aged 15–19 as compared to their male counterpartsin all but one country. 8In nine countries – all, aside from India, in West and CentralAfrica – more than half of girls aged 15–19 are anaemic. 9India also has the highest underweight prevalence amongadolescent girls among the countries with available data,at 47 per cent. The implications for adolescent girls in thisFigure 2.3: Anaemia is a significant risk for adolescentgirls (15–19) in sub-Saharan Africa and South AsiaPrevalence of anaemia among adolescent girls aged 15–19 in asubset of high-prevalence countries with available data80Figure 2.4: Underweight is a major risk for adolescentgirls (15–19) in sub-Saharan Africa and South AsiaPercentage of adolescent girls aged 15–19 who are underweight*in a subset of high-prevalence countries with available data50706050406866635957 5652 51 51494030474035 34 34333029 282730202010100MaliSenegalGhanaBeninCongoIndia*The horizontal line at the 40 per cent mark represents the threshold atwhich anaemia is considered a severe national public health issue.Source: DHS and national surveys, 2003–2009.BurkinaFasoGuineaSierraLeoneUnited Republicof Tanzania0IndiaEritreaBangladeshNigerSenegalEthiopiaNamibia* Defined as a body mass index of 18.5 or less.Source: DHS and other national surveys, 2002–2007.ChadCambodiaBurkinaFasorealizing the rights of adolescents 21
- Page 2 and 3: © United Nations Children’s Fund
- Page 4 and 5: AcknowledgementsThis report was pro
- Page 7 and 8: THE STATE OF THE WORLD’S CHILDREN
- Page 9: GLobal challenges for adolescents 1
- Page 12 and 13: large cohort of unemployed youth, w
- Page 14 and 15: FOCUS ONEarly and late adolescenceR
- Page 16 and 17: ment and active participation. Disa
- Page 18 and 19: age at which individuals are legall
- Page 20 and 21: the rights of adolescents or to pro
- Page 22 and 23: The Convention was sufficiently ins
- Page 24 and 25: Adolescents are often consideredthe
- Page 26 and 27: HALLENGES ANDRealizing the rights o
- Page 30 and 31: country are particularly serious, g
- Page 32 and 33: Gathering accurate data on adolesce
- Page 34 and 35: sexes, there is still a considerabl
- Page 36 and 37: PERSPECTIVEFacing the challenge:Rep
- Page 38 and 39: FOCUS ONInequality in childhood and
- Page 40 and 41: ADOLESCENT VOICESAct responsibly:Nu
- Page 42 and 43: past decade, though not all of them
- Page 44 and 45: Yet other initiatives against child
- Page 46 and 47: PERSPECTIVEChernobyl 25 years later
- Page 48: Adolescents are deeply concernedabo
- Page 51 and 52: OPPORTUNITIESrisk of climate change
- Page 53 and 54: Poverty, unemploymentand globalizat
- Page 55 and 56: PERSPECTIVEThe effects of climate c
- Page 57 and 58: high-level competencies that are in
- Page 59 and 60: a window for possible economic deve
- Page 61 and 62: ADOLESCENT VOICESReclaim Tijuana:Pu
- Page 63 and 64: are exacerbating those risks, inclu
- Page 65 and 66: sentencing wherever possible, inclu
- Page 67 and 68: e stranded in poverty by conflict o
- Page 70 and 71: HALLENGES ANDOver the course of the
- Page 72 and 73: gated by age, disability, sex, ethn
- Page 74 and 75: FOCUS ONPreparing adolescents for a
- Page 76 and 77: the Ministry of Education, in colla
- Page 78 and 79:
exactly ‘youth participation’ l
- Page 80 and 81:
spaces as part of Aprendiz, the ‘
- Page 82 and 83:
PERSPECTIVEAdolescent girls:The bes
- Page 84 and 85:
ADOLESCENT VOICESFrom victims to ac
- Page 86 and 87:
ReferencesCHAPTER 11United Nations,
- Page 88 and 89:
19United Nations Children’s Fund,
- Page 90 and 91:
STATISTICAL TABLESEconomic and soci
- Page 92 and 93:
Under-five deaths (millions)Region
- Page 94 and 95:
STATISTICAL TABLESapproach is not t
- Page 96 and 97:
TABLE 1. BASIC INDICATORSCountries
- Page 98 and 99:
TABLE 1. BASIC INDICATORSUnder-5mor
- Page 100 and 101:
TABLE 2. NUTRITIONCountries and ter
- Page 102 and 103:
TABLE 2. NUTRITIONCountries and ter
- Page 104 and 105:
TABLE 3. HEALTHCountries and territ
- Page 106 and 107:
TABLE 3. HEALTH% of populationusing
- Page 108 and 109:
TABLE 4. HIV/AIDSCountries and terr
- Page 110 and 111:
TABLE 4. HIV/AIDSEstimatedadult HIV
- Page 112 and 113:
TABLE 5. EDUCATIONCountries and ter
- Page 114 and 115:
TABLE 5. EDUCATIONPrimary schoolNum
- Page 116 and 117:
TABLE 6. DEMOGRAPHIC INDICATORSCoun
- Page 118 and 119:
TABLE 6. DEMOGRAPHIC INDICATORSPopu
- Page 120 and 121:
TABLE 7. ECONOMIC INDICATORSCountri
- Page 122 and 123:
TABLE 7. ECONOMIC INDICATORSCountri
- Page 124 and 125:
TABLE 8. WOMENCountries andterritor
- Page 126 and 127:
TABLE 8. WOMENCountries andterritor
- Page 128 and 129:
TABLE 9. CHILD PROTECTIONChild labo
- Page 130 and 131:
TABLE 9. CHILD PROTECTIONChild labo
- Page 132 and 133:
Summary indicatorsAverages presente
- Page 134 and 135:
TABLE 10. THE RATE OF PROGRESSCount
- Page 136 and 137:
TABLE 10. THE RATE OF PROGRESSUnder
- Page 138 and 139:
TABLE 11. ADOLESCENTSCountries and
- Page 140 and 141:
TABLE 11. ADOLESCENTSAdolescents po
- Page 142 and 143:
TABLE 12. EQUITYCountries andterrit
- Page 144 and 145:
TABLE 12. EQUITYBirth registration
- Page 146 and 147:
AcronymsAIDSCEDAWDHSFGM/CGDPHIVIUCW
- Page 148:
United Nations Children’s Fund3 U