Autoantibodies in Systemic Autoimmune Diseases - (GFID) eV
Autoantibodies in Systemic Autoimmune Diseases - (GFID) eV
Autoantibodies in Systemic Autoimmune Diseases - (GFID) eV

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
AUTOANTIGENS,AUTOANTIBODIES,AUTOIMMUNITYEdited by: K. Conrad (Dresden, Germany)U. Sack (Leipzig, Germany)Vol. 2, second Edition – 2007AuthorsDr. Karsten ConradInstitute for ImmunologyMedical Faculty of the Technical University DresdenFetscherstrasse 7401307 Dresden, GERMANYPhone: +49 (0) 351-458-6540Fax: +49 (0) 351-458-6308E-mail: K Conrad@mail.zih.tu-dresden.deDr. Werner SchößlerRathenaustr. 1216341 Panketal, GERMANYFax: +49 (0) 30-983-119-94E-mail: Dr.Schoessler@arcor.deProf. Dr. Falk HiepeCharité University HospitalDepartment of Rheumatology & Cl<strong>in</strong>ical ImmunologySchumannstraße 20/2110117 Berl<strong>in</strong>, GERMANYPhone: +49 (0) 30-450-513012Fax: +49 (0) 30-450-51392E-mail: Falk.Hiepe@charite.deMarv<strong>in</strong> J. Fritzler, MD, PhDProfessor of Medic<strong>in</strong>eArthritis Society ChairFaculty of Medic<strong>in</strong>eUniversity of CalgaryCalgary, Alberta, CANADAPhone: +01 403-220-3533Fax: +01 403-283-5666E-mail: Fritzler@ucalgary.ca
ContentsPreface, 2 nd edition ................................Preface, 1 st edition.................................XVXVINotesfortheUseofthisBook.......................... 1<strong>Autoantibodies</strong> — Def<strong>in</strong>itions and Characteristics ............. 3<strong>Autoantibodies</strong> <strong>in</strong> the Diagnosis of <strong>Autoimmune</strong> <strong>Diseases</strong> ........ 4Part 1<strong>Autoantibodies</strong> <strong>in</strong> <strong>Systemic</strong> <strong>Autoimmune</strong> <strong>Diseases</strong>Alanyl-tRNA (tRNA Ala )SynthetaseAntibodies .............. 10Alpha-Act<strong>in</strong><strong>in</strong>Antibodies .......................... 10Alpha-EnolaseAntibodies .......................... 10Alpha-Fodr<strong>in</strong>Antibodies .......................... 12Am<strong>in</strong>oacyl-tRNASynthetaseAntibodies ................. 13Annex<strong>in</strong>VAntibodies ............................ 15Ant<strong>in</strong>eutrophilCytoplasmicAntibodies(ANCA)............. 16Ant<strong>in</strong>uclearAntibodies(ANA) ....................... 19ASE-1Antibodies ............................... 21Asparag<strong>in</strong>yl-tRNA (tRNA Asp )SynthetaseAntibodies........... 21AssemblyosomeAntibodies ......................... 22Azurocid<strong>in</strong>Antibodies ............................ 22Beta-Fodr<strong>in</strong>Antibodies............................ 24Beta-2 Glycoprote<strong>in</strong> I (β2-GPI)Antibodies ................ 24BPIAntibodies ................................ 27C1DAntibodies ................................ 28C1qAntibodies ................................ 28CADM-140Antibodies ............................ 30Calpastat<strong>in</strong>Antibodies ............................ 31Calreticul<strong>in</strong>Antibodies............................ 32cANCA(C-ANCA).............................. 33
VICONTENTSCardiolip<strong>in</strong>Antibodies ............................ 34Catheps<strong>in</strong>GAntibodies ........................... 37CCPAntibodies................................ 38CD16Antibodies ............................... 39CENP-BAntibodies.............................. 40CENP-CAntibodies.............................. 40CENP-EAntibodies ............................. 41CENP-FAntibodies.............................. 42CentrioleAntibodies ............................. 44CentromereAntibodies............................ 44Centrophil<strong>in</strong>Antibodies ........................... 47CentrosomeAntibodies ........................... 47Chromat<strong>in</strong>Antibodies ............................ 49ChromoAntibodies.............................. 50Citrull<strong>in</strong>atedProte<strong>in</strong>/PeptideAntibodies.................. 51Coil<strong>in</strong>Antibodies ............................... 53CollagenAntibodies ............................. 54CRPAntibodies................................ 56Cryoglobul<strong>in</strong>s ................................. 56CytoplasmicL<strong>in</strong>kerProte<strong>in</strong>170(CLIP-170)Antibodies ......... 57DEKAntibodies................................ 58Double-StrandedDNA(dsDNA)Antibodies ............... 59EEA-1Antibodies ............................... 62EF1AAntibodies................................ 63EJAntibodies ................................. 64ElastaseAntibodies .............................. 64ENAAntibodies................................ 64EndothelialCellAntibodies ......................... 65EPCRAntibodies ............................... 66ExosomeAntibodies ............................. 67FerAntibodies................................. 67Ferrit<strong>in</strong>Antibodies .............................. 67Fibrillar<strong>in</strong>Antibodies............................. 68Fibrill<strong>in</strong>1Antibodies ............................. 69FibroblastAntibodies............................. 70Filaggr<strong>in</strong>Antibodies ............................. 70Glutam<strong>in</strong>yl-tRNA (tRNA Glu )SynthetaseAntibodies ........... 71Glycyl-tRNA (tRNA Gly )SynthetaseAntibodies .............. 71GM1Antibodies ............................... 72GolgiApparatusAntibodies ......................... 72GuAntibodies................................. 74GWBAntibodies ............................... 74
CONTENTSVIIHeatShockProte<strong>in</strong>(Hsp)Antibodies ................... 76Histidyl-tRNA (tRNA His )Synthetase(HRS)Antibodies......... 77HistoneAntibodies .............................. 77HMGAntibodies ............................... 79HsEg5Antibodies............................... 805-HT4ReceptorAntibodies ......................... 80HumanNeutrophilElastase(HNE)Antibodies .............. 80IFI16Antibodies ............................... 81IgA<strong>Autoantibodies</strong> .............................. 82Isoleucyl-tRNA (tRNA Ile )SynthetaseAntibodies ............. 83JaAntibodies.................................. 83Jo-1Antibodies ................................ 83Kerat<strong>in</strong>Antibodies(AKA).......................... 85KiAntibodies ................................. 86K<strong>in</strong>ect<strong>in</strong>Antibodies.............................. 87KJAntibodies ................................. 87KSAntibodies................................. 88KuAntibodies................................. 88L5/5S Antibodies ............................... 90L7Antibodies ................................. 91L12Antibodies................................. 91Lactoferr<strong>in</strong>Antibodies ............................ 91Lam<strong>in</strong>Antibodies............................... 92La/SS-BAntibodies.............................. 92LECellFactor ................................. 95LEDGF(LensEpithelialDerivedGrowthFactor)Antibodies ...... 96Leucyl-tRNA (tRNA Leu )SynthetaseAntibodies.............. 97Lipoprote<strong>in</strong>Lipase(LPL)Antibodies.................... 97LupusAnticoagulant(LA) .......................... 98LysosomeAntibodies............................. 100LysozymeAntibodies............................. 101Lysyl-tRNA (tRNA Lys )SynthetaseAntibodies............... 101M3mAchR(M3R)Antibodies........................ 101MasAntibodies ................................ 101MBLAntibodies................................ 102MCVAntibodies ............................... 102Mi-2Antibodies................................ 103MidbodyAntibodies ............................. 105MMPAntibodies ............................... 107Mpp1Antibodies ............................... 107Mpp10Antibodies............................... 108MSAAntibodies................................ 108
VIIICONTENTSMyeloperoxidaseAntibodies......................... 110Myos<strong>in</strong>Antibodies .............................. 113Nedd5Antibodies............................... 113NMDAReceptorAntibodies......................... 114NOR-90Antibodies.............................. 115NucleolarAntibodies ............................. 117Nucleol<strong>in</strong>Antibodies ............................. 118Nucleophosm<strong>in</strong>Antibodies ......................... 119NucleosomeAntibodies ........................... 120NuMAAntibodies............................... 122OJAntibodies ................................. 124oxLDLAntibodies............................... 124pANCA(P-ANCA).............................. 126PCNAAntibodies............................... 128PDGFReceptor(PDGFR)Antibodies ................... 129Per<strong>in</strong>uclearFactors(PNF) .......................... 130PhosphatidicAcid(PA)Antibodies..................... 130Phosphatidylchol<strong>in</strong>e(PC)Antibodies.................... 131Phosphatidylethanolam<strong>in</strong>e(PE)Antibodies ................ 132Phosphatidyl<strong>in</strong>ositol(PI)Antibodies.................... 133Phosphatidylser<strong>in</strong>e(PS)Antibodies..................... 134Phospholipid(PL)Antibodies........................ 135PL-7Antibodies................................ 139PL-12Antibodies ............................... 140PM-1Antibodies................................ 141PMS1Antibodies ............................... 142PM/SclAntibodies .............................. 142PM/Scl-75Antibodies ............................ 145PM/Scl-100Antibodies ............................ 145Poly(ADP-Ribose)Polymerase(PARP)Antibodies............ 145ProteasomeAntibodies............................ 146Prote<strong>in</strong>ase3Antibodies............................ 147Prote<strong>in</strong>CAntibodies ............................. 149Prote<strong>in</strong>SAntibodies ............................. 150Prothromb<strong>in</strong>Antibodies ........................... 151RA33Antibodies ............................... 152ReplicationProte<strong>in</strong>A(RPA)Antibodies .................. 155RheumatoidFactors(RF) .......................... 156RibosomalAntibodies ............................ 157RibosomalPProte<strong>in</strong>(RPP)Antibodies................... 159RibosomalRNAProcess<strong>in</strong>g(Rrp)Prote<strong>in</strong>Antibodies .......... 161RNAAntibodies................................ 162
CONTENTSIXRNAHelicaseIIAntibodies ......................... 163RNAHelicaseA(RHA)Antibodies..................... 163RNAP-IAntibodies.............................. 164RNAP-IIAntibodies ............................. 164RNAP-IIIAntibodies ............................. 164RNAPolymerase(RNAP)Antibodies.................... 164Ro52Antibodies................................ 166Ro60Antibodies................................ 167Ro/SS-AAntibodies.............................. 16728SrRNAAntibodies............................. 172S10Antibodies................................. 172SaAntibodies ................................. 172SAPAntibodies ................................ 173SCAntibodies................................. 173Scl-70Antibodies ............................... 173S<strong>in</strong>gle-StrandedDNA(ssDNA)Antibodies ................ 176Sip1Antibodies ................................ 177SmAntibodies................................. 177snoRNPAntibodies.............................. 179snRNPAntibodies .............................. 179SRProte<strong>in</strong>Antibodies ............................ 182SRPAntibodies ................................ 182SS-56Antibodies ............................... 184SS-AAntibodies................................ 185SS-BAntibodies................................ 185ssDNAAntibodies............................... 185Threonyl-tRNA (tRNA Thr )SynthetaseAntibodies ............ 185Th/ToAntibodies ............................... 185Thrombomodul<strong>in</strong>Antibodies ........................ 186TopoisomeraseIAntibodies ......................... 187TopoisomeraseIIAntibodies......................... 187Trimethylguanos<strong>in</strong>eAntibodies ....................... 188U1-RNPAntibodies.............................. 188U2-RNPAntibodies.............................. 189U4/U6-RNPAntibodies ........................... 189U5-RNPAntibodies.............................. 190U7-RNPAntibodies.............................. 190U11-RNPAntibodies ............................. 190
XCONTENTSPart 2<strong>Systemic</strong> <strong>Autoimmune</strong> <strong>Diseases</strong> – Syndromes, Diagnostic Criteria,Symptoms“Abortion,spontaneous ............................ 192Acidosis,renal-tubular ............................ 192Acro-Osteolysis ................................ 192Addison’sdisease ............................... 192Adrenocorticalfailure ............................ 192Aldolase,elevated<strong>in</strong>plasma ......................... 192Alopecia .................................... 192Alveolitis.................................... 193Amaurosisfugax ............................... 193ANCA-associatedvasculitis ......................... 193Anemia .................................... 193Anti-Jo-1syndrome ............................. 194Antiphospholipidsyndrome(APS) ..................... 194Anti-SRPsyndrome ............................. 197Anti-Synthetasesyndrome.......................... 197Arthralgia ................................... 198Arthritis .................................... 198Behçetdisease................................. 199Bronchialasthma ............................... 199Budd-Chiarisyndrome ........................... 200Butterfly rash ................................. 200Calc<strong>in</strong>osiscutis ................................ 200Cardiomyopathy ............................... 200Catastrophic”APS .............................. 201Cavernouss<strong>in</strong>usthrombosis ........................ 202Cerebral<strong>in</strong>farction .............................. 202Cerebralischemia............................... 202Chorea ..................................... 202Churg-Strausssyndrome(CSS) ....................... 203Claudicationofextremities ......................... 203Claudicationofmasticatorymuscles .................... 204Cogan’ssyndrome .............................. 204Congenitalheartblock ............................ 204Conjunctivitis ................................. 204Connectivetissuediseases .......................... 205Creat<strong>in</strong>ek<strong>in</strong>ase,elevated<strong>in</strong>plasma..................... 205CRESTsyndrome .............................. 205Cryoglobul<strong>in</strong>emia .............................. 206Cryoglobul<strong>in</strong>emicnephropathy ....................... 206
CONTENTSXICryoglobul<strong>in</strong>emicpurpura ......................... 206Cryoglobul<strong>in</strong>emicvasculitis ......................... 206Cutaneousleukocytoclasticvasculitis.................... 207Dementia,multi-<strong>in</strong>farct ........................... 207Dermatomyositis ............................... 207Dermatomyositis,amyopathic ........................ 208Discoidlupuserythematosus(DLE) .................... 208Drug-<strong>in</strong>ducedlupus(DIL).......................... 209Eos<strong>in</strong>ophilia .................................. 210Epilepsy .................................... 210Episcleritis ................................... 210Erythema ................................... 210Esophagealdysfunction ........................... 210Evanssyndrome ............................... 211FacialParesis ................................. 211Felty’ssyndrome ............................... 211F<strong>in</strong>gertipnecrosis............................... 212Giantcellarteritis............................... 212Glomerulonephritis ............................. 212Glomerulosclerosis .............................. 213Goodpasture’sdisease ............................ 213Gottron’ssign ................................. 213Guilla<strong>in</strong>-Barré syndrome .......................... 213Headache ................................... 213Hemianopia .................................. 214Hemorrhagicalveolitis ............................ 214Henoch-Schönle<strong>in</strong>purpura ......................... 214Hepatic<strong>in</strong>farction .............................. 215Hepatomegaly ................................. 215Horton’sdisease................................ 215Hypereos<strong>in</strong>ophilia .............................. 215Hypergammaglobul<strong>in</strong>emia ......................... 216Hypersensitivityvasculitis .......................... 216Hypertension ................................. 216Hypocomplementemicurticarialvasculitissyndrome(HUVS) ..... 217IgAnephropathy ............................... 218Intest<strong>in</strong>alnecrosis .............................. 218Intracardiacthrombus ............................ 218Juvenilechronicarthritis(JCA) ....................... 218Juvenileidiopathicarthritis(JIA) ...................... 222Juvenilerheumatoidarthritis(JRA) .................... 222Juvenilescleromyositis ............................ 222
XIICONTENTSKawasakisyndrome.............................. 222Leukocytopenia ................................ 223Leukocytosis ................................. 223Libman-Sacksendocarditis ......................... 224Lilacr<strong>in</strong>gs ................................... 224Livedoreticularis/racemosa ......................... 224Lymphadenopathy .............................. 224Lymphocytopenia .............................. 225Malabsorption ................................ 225Mechanic’shands ............................... 225Membranousnephritis/nephropathy(MN) ................ 225Men<strong>in</strong>gitis,aseptic .............................. 226Mesenteric<strong>in</strong>farction............................. 226Microscopicpolyangiitis(MPA)....................... 226Microstomia.................................. 226Migra<strong>in</strong>e,atypical .............................. 227Mixedconnectivetissuedisease(MCTD) ................. 227Moschkowitz’ssyndrome .......................... 229Mucocutaneouslymphnodesyndrome .................. 230Muscleweakness ............................... 230Muscularatrophy ............................... 230Myalgia .................................... 230Myocardial<strong>in</strong>farction............................. 231Myoglob<strong>in</strong>,elevated<strong>in</strong>plasma ....................... 231Myositis,idiopathic.............................. 231Myositisoverlapsyndromes ......................... 231Neonatallupuserythematosus(NLE) ................... 231Neonatallupussyndromes ......................... 232Nephritis ................................... 232Neuropathy .................................. 233Organicbra<strong>in</strong>syndrome ........................... 233Otitisexterna ................................. 233Otitismedia .................................. 233Overlapsyndromes.............................. 234Pancreatic<strong>in</strong>farction ............................. 234Pancreatitis .................................. 234Panniculitis .................................. 234Parotitis .................................... 234Pericardial effusion .............................. 234Pericarditis .................................. 235Peritonitis ................................... 235Photosensitivity ................................ 235
CONTENTSXIIIPleuritis .................................... 235Polyarteritisnodosa ............................. 236Polymyalgiarheumatica(PMR) ...................... 237Polymyositis(PM)/Dermatomyositis(DM) ................ 237Polymyositis/sclerodermaoverlap ..................... 239Polyneuritis,cranial ............................. 240PrimarySjögren’ssyndrome......................... 240Prote<strong>in</strong>uria .................................. 240Pseudocaverns ................................ 240Psychosis ................................... 240Ptosis ..................................... 241Pulmonary fibrosis .............................. 241Pulmonaryhemorrhage ........................... 241Pulmonaryarterialhypertension(PAH) .................. 241Pulmonary <strong>in</strong>filtrates ............................. 242Pulselessness ................................. 242Purpura .................................... 242Raynaud’sphenomenon ........................... 242Relaps<strong>in</strong>gpolychondritis .......................... 243Ret<strong>in</strong>itis .................................... 243Ret<strong>in</strong>alischemia ............................... 244Rheumatoidarthritis ............................. 244Rheumatoidnodules ............................. 245Rh<strong>in</strong>itis..................................... 246Rhupus .................................... 246Saddlenose .................................. 246Scleritis/Episcleritis.............................. 246Sclerodactyly ................................. 246Scleroderma .................................. 246Scleroderma/myositisoverlap ........................ 247Sclerodermaspectrumdisorder ...................... 247Sclerosiss<strong>in</strong>escleroderma .......................... 247SecondarySjögren’ssyndrome ....................... 248Sensor<strong>in</strong>euralhear<strong>in</strong>gloss .......................... 248Sharpsyndrome ............................... 248S<strong>in</strong>usve<strong>in</strong>thrombosis ............................ 248S<strong>in</strong>usitis .................................... 248Sjögren’ssyndrome(SjS)........................... 249Sneddon’ssyndrome ............................. 252Sp<strong>in</strong>al<strong>in</strong>farction ............................... 252Splenomegaly ................................. 252Still’sdisease ................................. 253
XIVCONTENTSStroke ..................................... 253Subacutecutaneouslupuserythematosus(SCLE) ............ 253<strong>Systemic</strong>lupuserythematosus(SLE) .................... 253<strong>Systemic</strong>sclerosis(SSc) ........................... 255<strong>Systemic</strong>vasculitides ............................. 257Takayasuarteritis ............................... 258Teleangiectasia ................................ 259Temporalarteritis............................... 259Thrombocytopenia .............................. 259Thrombocytopenicthromboticpurpura(TTP) ............. 260Thrombocytosis ............................... 260Thrombosis .................................. 260Thyroiditis .................................. 260Tolosa-Huntsyndrome ........................... 260Transitoryischemicattacks(TIA)...................... 260Transversemyelitis .............................. 261Ulcers ..................................... 261Undifferentiatedconnectivetissuedisease(UCTD) ........... 261Urticaria .................................... 262Valvularheartdisease ............................ 262Vertigo ..................................... 262Wegener’sgranulomatosis(WG) ...................... 263Xerostomia .................................. 264Abbreviations ................................... 265Appendices..................................... 267
Preface, 2 nd editionThe determ<strong>in</strong>ation of autoantibodies has become an <strong>in</strong>tegral part of the diagnosisand differential diagnosis, as well as the estimation of the prognosis and developmentof autoimmune diseases. Furthermore, because many disease-associatedautoantibodies are detectable <strong>in</strong> precl<strong>in</strong>ical stages, they have assumed a potentialrole <strong>in</strong> the very early diagnosis or risk assessment of disease development. Thegrow<strong>in</strong>g knowledge about the pathogenic and diagnostic value of autoantibodies<strong>in</strong> systemic diseases, and the discovery of novel autoantibodies and changes <strong>in</strong>classification criteria necessitated the publish<strong>in</strong>g of a revised and supplemented2 nd edition. Besides the cl<strong>in</strong>ically relevant autoantibodies also antibodies that mayserve as tools <strong>in</strong> molecular, cell and tumor biological studies have been <strong>in</strong>cluded.However due to the rapid development, the alphabetical catalogue of relevant orpotential relevant autoantibodies is <strong>in</strong>complete. Therefore, the authors appreciatehelpful comments for future editions.Karsten ConradMarv<strong>in</strong> J. FritzlerFalk HiepeWerner Schößler
Preface, 1 st editionAmong the challenges fac<strong>in</strong>g the new millennium physician are tremendouschanges <strong>in</strong> biomedical and <strong>in</strong>formation technologies that are rapidly chang<strong>in</strong>g thenature and complexity of cl<strong>in</strong>ical practice. S<strong>in</strong>ce the discovery of the LE cell over50 years ago, there has been a logarithmic <strong>in</strong>crease <strong>in</strong> the description and cl<strong>in</strong>icalapplication of autoantibodies <strong>in</strong> an ever-widen<strong>in</strong>g spectrum of diseases. <strong>Systemic</strong>rheumatic diseases are among the most complex of these diseases because thecl<strong>in</strong>ical presentation and constellation of f<strong>in</strong>d<strong>in</strong>gs are <strong>in</strong> part reflected by thespectrum of autoantibodies found <strong>in</strong> these conditions. The litany of autoantibodyacronyms, designations and descriptors <strong>in</strong>clude Sm, dsDNA, SS-A/Ro, ‘ SS-B/La,U1RNP, Jo-1, topo-I, CENP, Ku, Ki, Sa, and ribo P, to name a few. This antibodyalphabet soup’ has threatened to move cl<strong>in</strong>ical diagnostics <strong>in</strong>to a literal Tower of‘Babel.It is important to appreciate how the antibody alphabet soup’ can be useful <strong>in</strong>the diagnosis and management of systemic rheumatic diseases. The applicationsare as varied and rich as are the multiplicity of the autoantibody specificities. Certa<strong>in</strong>ly,autoantibody test<strong>in</strong>g is not required to make a diagnosis <strong>in</strong> a woman whopresents with a photosensitive sk<strong>in</strong> rash, pericarditis, glomerulonephritis, anemiaand psychosis. This patient clearly has SLE and the detection of autoantibodiesconfirms the obvious.What may not be as clear is that the presence of anti-dsDNAcould correlate with nephritis and the presence of anti-ribo P may <strong>in</strong>dicate manifestationsof central nervous system lupus <strong>in</strong> the presence of confound<strong>in</strong>g factorssuch as <strong>in</strong>fections and drug use. In addition, not all patients present “with classicaltextbook” features of systemic rheumatic diseases. Unfortunately, <strong>in</strong> many casesthe time <strong>in</strong>terval from the onset of symptoms to a confirmed diagnosis and meet<strong>in</strong>gestablished criteria for the classification of disease,can be measured <strong>in</strong> decades.Thus, when there is limited (forme fruste) disease or a s<strong>in</strong>gle disease manifestation,the detection of serum autoantibodies can play an important role <strong>in</strong> rais<strong>in</strong>g thesuspicion of evolv<strong>in</strong>g disease and forecast<strong>in</strong>g prognosis. A good example is theuse of autoantibodies <strong>in</strong> the <strong>in</strong>itial evaluation of Raynaud’s phenomenon. If theANA and other autoantibody tests are negative, the likelihood that his patient hasprimaryRaynaud’sdiseaseislikelyandtheconcernthatthecl<strong>in</strong>icalcoursewilltransform <strong>in</strong>to systemic rheumatic disease is lessened. On the other hand, ample
PREFACE,1 ST EDITIONXVIIcl<strong>in</strong>ical studies have shown that the presence of anti-topo-I (Scl-70) is a harb<strong>in</strong>gerof diffuse scleroderma, antibodies to CENP are more predictive of the limitedform of the disease, and the presence of anti-PM/Scl, <strong>in</strong>dicates a sclerodermapolymyositisoverlap syndrome. There many other examples of the cl<strong>in</strong>ical utilityof autoantibody test<strong>in</strong>g <strong>in</strong> isolated cl<strong>in</strong>ical scenarios such as polyarthritis, myositis,neuropathies, cytopenias, and vasculopathies that are characteristic, but notspecific for, any s<strong>in</strong>gle systemic rheumatic disease. In many of these <strong>in</strong>stances ‘thepresence of one or more alphabet soup’ antibodies can be a prologue to diseasesthatarelikelytoevolvedur<strong>in</strong>gpatientfollow-up.While the diagnosis of forme fruste diseaseisanimportantuseofautoantibodytest<strong>in</strong>g,another valuable use is that they provide an understand<strong>in</strong>g of the pathogenesis.This has been clearly illustrated with the subsets of disease such as neonatallupussyndrome,subacutecutaneouslupus,homozygousC2deficiency, <strong>in</strong>terstitiallung disease, granulocytopenia, and Sjögren’s syndrome that are strongly associatedwith anti-SS-A/Ro. Compell<strong>in</strong>g evidence shows that anti-SS-A/Ro b<strong>in</strong>ds withthe cognate antigen <strong>in</strong> the fetal heart and <strong>in</strong> kerat<strong>in</strong>ocytes exposed to ultravioletlight. On the other hand, it is not clear how or if the same antibody participates<strong>in</strong> the development of keratoconjunctivitis sicca. The demonstration that ribosomalP prote<strong>in</strong>s and other autoantigens are found on the surface of some normaland apoptotic cells may provide an important clue to their potential pathogenicrole. The notion that some autoantibodies may be f<strong>in</strong>gerpr<strong>in</strong>ts <strong>in</strong>crim<strong>in</strong>at<strong>in</strong>g acauseoretiologyofthediseasearealsobe<strong>in</strong>gclarified. For example, antibodiesto fibrillar<strong>in</strong> (U3-RNP) are <strong>in</strong>duced <strong>in</strong> certa<strong>in</strong> stra<strong>in</strong>s of mice by heavy metal exposureand systemic sclerosis patients with these autoantibodies have high levelsof ur<strong>in</strong>ary mercury.The future of autoantibody test<strong>in</strong>g can be cast <strong>in</strong>to at least four arenas. First,the rapid advancement of new technologies (autoantigen arrays, microfluidics andnanotechnology) will change the complexion of the autoantibody test<strong>in</strong>g by provid<strong>in</strong>ga wealth of serological <strong>in</strong>formation that will almost certa<strong>in</strong>ly challengecurrent paradigms and cl<strong>in</strong>ical associations. It is now possible to use a drop ofblood to analyze serum for the presence of over 100 different autoantibodies <strong>in</strong> as<strong>in</strong>gle test that can be completed and reported with<strong>in</strong> m<strong>in</strong>utes. Second, it is anticipatedthat autoantibody test<strong>in</strong>g will be a critical part of monitor<strong>in</strong>g and evaluat<strong>in</strong>gpatients placed on a variety of the newer biological therapeutics. For example, it is<strong>in</strong>creas<strong>in</strong>gly clear that <strong>in</strong>terferon and tumor necrosis factor blockade therapies areassociated with the <strong>in</strong>duction of autoantibodies and, <strong>in</strong> some cases, full blown disease.Interest<strong>in</strong>gly,theseobservations fall on the historical evidence that drugs suchas proca<strong>in</strong>amide and hydralaz<strong>in</strong>e can <strong>in</strong>duce autoantibodies and lupus syndromes.Third, it is likely that autoantibody test<strong>in</strong>g will replace more <strong>in</strong>vasive and costlydiagnostic techniques such as the salivary gland biopsy for Sjögren’s syndrome,the small bowel biopsy for coeliac disease, the nerve and sk<strong>in</strong> biopsy for vasculitis,the muscle biopsy for myositis, and many others. Fourth, carefully designed
XVIIIPREFACE,1 ST EDITIONstudies that assess the cost effectiveness of autoantibody test<strong>in</strong>g are required. Onone hand, there is the notion that <strong>in</strong> many patients, <strong>in</strong>clud<strong>in</strong>g the woman withunequivocal features of SLE described above, that even the relatively <strong>in</strong>expensiveautoantibody test is superfluous and not cost effective. However, the implicationsof longer term health care costs of miss<strong>in</strong>g an early diagnosis <strong>in</strong> a patient withforme fruste disease must also be carefully considered. A cost-effective and rationalapproach to autoantibody test<strong>in</strong>g algorithms and cl<strong>in</strong>ical practice guidel<strong>in</strong>esare overdue. Cl<strong>in</strong>ical studies to address these issues will prove worthwhile and savepatients from needless, expensive and <strong>in</strong>vasive tests, and missed diagnosis that canlead to significant morbidity and mortality.This book and reference guide is <strong>in</strong>tended to assist the physician understandand <strong>in</strong>terpret the variety of autoantibodies that are be<strong>in</strong>g used as diagnostic andprognostic tools for patients with systemic rheumatic diseases. Although the landscapeof autoantibody test<strong>in</strong>g cont<strong>in</strong>ues to change,this <strong>in</strong>formation will be a usefuland valuable reference for many years to come.Marv<strong>in</strong> J. Fritzler
Notes for the Use of this BookThis reference book on the serological diagnosis of systemic autoimmune diseasesis divided <strong>in</strong>to two ma<strong>in</strong> sections. The autoantibodies observed <strong>in</strong> autoimmunediseases are described <strong>in</strong> alphabetical order <strong>in</strong> Part 1, and autoimmune disordersas well as symptoms that <strong>in</strong>dicate the possible presence of an autoimmune diseaseare listed <strong>in</strong> Part 2. Guide marks (the symbol “”) were <strong>in</strong>serted to ensure fastand easy cross-reference between symptoms, a given autoimmune disease andassociated autoantibodies. Bibliographic references were omitted due to the broadscope of the subject matter. Only the first authors of historical or some importantrecent publications have been “named.With some exceptions (e.g.,ant<strong>in</strong>uclear antibodies) the prefix anti-”was omittedfor better clarity of alphabetization. Anticentromere antibodies, for “example,are listed as centromere antibodies”. In as far as they were known to the authors,synonyms or alternative names for the antibodies were also listed. Obsolete term<strong>in</strong>ologyis <strong>in</strong>dicated as such, and the names preferred by the authors are used <strong>in</strong>the alphabetical <strong>in</strong>dex.The autoantibody description section beg<strong>in</strong>s, <strong>in</strong> some cases, with a brief <strong>in</strong>troductionor historical account. This is followed by <strong>in</strong>formation on the targetstructures (autoantigens), detection methods, cl<strong>in</strong>ical relevance, and <strong>in</strong>dicationsfor test<strong>in</strong>g of the autoantibody.The authors’ rat<strong>in</strong>g of the cl<strong>in</strong>ical relevance of each autoantibody listed <strong>in</strong> thebook is <strong>in</strong>dicated us<strong>in</strong>g variable color<strong>in</strong>g and letter<strong>in</strong>g.White Letters onGreen BackgroundThese are autoantibodies of high diagnostic relevance (markers for diagnosis,prognosis or monitor<strong>in</strong>g) that can usually be determ<strong>in</strong>ed <strong>in</strong> all laboratories.
2 INTRODUCTIONBlack Letters onMedium Green BackgroundThese are diagnostically relevant autoantibodies that are not measurable <strong>in</strong> alllaboratories and therefore are determ<strong>in</strong>ed <strong>in</strong> specialized laboratories only.Black Letters onLight Green BackgroundThe cl<strong>in</strong>ical relevance of these antibodies is (still) unclear due to their verylow frequency of detection, discrepancies between the f<strong>in</strong>d<strong>in</strong>gs of different studies(lack of comparability due to differences <strong>in</strong> study design, methodology, ethnic differences,etc.), methodological problems, or prelim<strong>in</strong>ary nature of study f<strong>in</strong>d<strong>in</strong>gs.Black Letters onWhite BackgroundThese autoantibodies are currently not cl<strong>in</strong>ically relevant, are no longer cl<strong>in</strong>icallyrelevant, or are cl<strong>in</strong>ically relevant only <strong>in</strong> isolated cases. This can also <strong>in</strong>cludedisease-specific autoantibodies if their test<strong>in</strong>g does not provide any added diagnosticadvantages over other parameters.
Part 1<strong>Autoantibodies</strong> <strong>in</strong> <strong>Systemic</strong><strong>Autoimmune</strong> <strong>Diseases</strong>
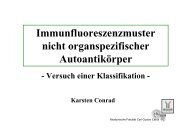
GWB ANTIBODIES 75GWB AntibodiesSynonym: Anti-GW bodies also referred to as mammalian process<strong>in</strong>g (P) bodies.AutoantigensGWB autoantigens <strong>in</strong>clude a group of 3 GW prote<strong>in</strong>s referred to as GW182, GW2and GW3 as well as other components such as Ago2, Ge-1/Hedls and RAP55. Theyare localized to discrete cytoplasmic structures that are <strong>in</strong>volved <strong>in</strong> mRNA process<strong>in</strong>g.The GW antigens were so-named because they conta<strong>in</strong> numerous glyc<strong>in</strong>e (G)and tryptophan (W) repeats and have a calculated molecular mass of 182 kDa)and they b<strong>in</strong>d to mRNA as well as Ago2, and are key components of the RNA <strong>in</strong>terferencesilenc<strong>in</strong>g complex (RISC) (reviewed <strong>in</strong> Jakymiw et al., 2007). The mostcommon target antigen of GWB antibodies is Ge-1/Hedls followed by GW182(Bhanji et al., 2007).Detection Methods• IIF us<strong>in</strong>g monolayers of tissue culture or tumor cells, e.g., HEp-2 cells (Fig.12).21Figure 12. IIF pattern on HEp-2 cells (Immuno Concepts Ltd, Sacramento, USA) of ananti-GWB antibody positive serum: dist<strong>in</strong>ctive cytoplasmic dots vary<strong>in</strong>g <strong>in</strong> number fromzero<strong>in</strong>mitoticcells(1)tomorethan30<strong>in</strong><strong>in</strong>terphasecells(2).
76 AUTOANTIBODIES IN SYSTEMIC AUTOIMMUNE DISEASESNOTE: The frequency of detection of anti-GWB depends on the cell l<strong>in</strong>e andtissue that is used for the assay because GWB are most highly expressed <strong>in</strong>rapidly proliferat<strong>in</strong>g cells and <strong>in</strong> testis and a subset of neural cells. In addition,anti-GWB may be obscured by high titer anti-cytoplasmic antigens such asanti-mitochondrial antibodies.• IIF us<strong>in</strong>g monoclonal anti-GW182 for co-localization• IB us<strong>in</strong>g whole cell extracts or purified GWB fractions.• EIA or ALBIA us<strong>in</strong>g recomb<strong>in</strong>ant GW, Ago2, Ge-1/Hedls and RAP55 prote<strong>in</strong>s.• IP of recomb<strong>in</strong>ant prote<strong>in</strong> produced by <strong>in</strong> vitro transcription and translationof cDNA of respective antigens.Cl<strong>in</strong>ical Relevance• Moderate to high titers of anti-GWB are found <strong>in</strong> ∼ 0.4 % of rout<strong>in</strong>e screen<strong>in</strong>gus<strong>in</strong>g HEp-2 cells (St<strong>in</strong>ton et al., 2004). They are primarily associated with Sjögren’s syndrome, ataxia and other neuropathies, systemic lupus erythematosus(SLE), primary biliary cirrhosis (Bloch et al., 2005) and also found <strong>in</strong>other systemic autoimmune rheumatic diseases.• A systematic study of cohorts of various autoimmune diseases is needed nowthat rapid and sensitive array technology (e.g. ALBIA) is available.• It is important to note that the detection of anti-GWB may be masked by otherautoantibodies (i.e. antimitochondrial antibodies <strong>in</strong> primary biliary cirrhosis)or overlooked <strong>in</strong> the presence of strong ANA.IndicationsNone currently established.Comments: If the typical cytoplasmic discrete speckled pattern is found dur<strong>in</strong>gscreen<strong>in</strong>g with HEp-2 cells, serological follow-up to rule out reactivity with othercytoplasmic antigens that give a similar pattern (i.e. EEA-1, lysosome) is required.This can be partly accomplished by co-localization studies. However, it shouldbe noted that GWB are quite heterogeneous with respect to content of any oneof the components. Thus, analyses of autoantibodies with multiplexed array technologiesare preferred once the dist<strong>in</strong>ctive sta<strong>in</strong><strong>in</strong>g pattern is identified. At thecl<strong>in</strong>ical <strong>in</strong>terface, exam<strong>in</strong>ations should be performed, e.g., to detect the potentialdevelopment of connective tissue disease (Sjögren’s syndrome) and neurologicalconditions such as ataxia and sensory/motor neuropathies. Cooperation with aresearch laboratory can be useful, e.g., for determ<strong>in</strong>ation of the specificity andfurther evaluation of the potential cl<strong>in</strong>ical relevance of these antibodies.
HISTIDYL-TRNA (TRNA HIS )SYNTHETASE (HRS) ANTIBODIES 77Heat Shock Prote<strong>in</strong> (Hsp) AntibodiesCollective term for all autoantibodies directed aga<strong>in</strong>st heat shock prote<strong>in</strong>s/heatstress prote<strong>in</strong>s (Hsp).AutoantigensVarious heat shock prote<strong>in</strong>s (heat-stress-<strong>in</strong>duced prote<strong>in</strong>s) like Hsp60, Hsp70 andHsp90.Detection Methods• WB us<strong>in</strong>g cell extracts after one- or two-dimensional separation.• EIAus<strong>in</strong>gbiochemicallypurified or recomb<strong>in</strong>ant heat shock prote<strong>in</strong>s.Cl<strong>in</strong>ical RelevanceHsp antibodies occur <strong>in</strong> a number of autoimmune and non-autoimmune diseases(especially <strong>in</strong>fections) as well as <strong>in</strong> healthy <strong>in</strong>dividuals.IndicationsNone related to systemic autoimmune diseases. The use of Hsp antibodies fordiagnosis of arteriosclerosis and autoimmune diseases of the <strong>in</strong>ner ear is be<strong>in</strong>gevaluated.Histidyl-tRNA (tRNA His )Synthetase (HRS) AntibodiesSee Jo-1 antibodies, Am<strong>in</strong>oacyl-tRNA synthetase antibodies.Histone AntibodiesSynonym: Anti-histone antibodies (AHA).
78 AUTOANTIBODIES IN SYSTEMIC AUTOIMMUNE DISEASESHistory: Histone antibodies appear to be <strong>in</strong>volved <strong>in</strong> the LE cell phenomenon thatwas first described <strong>in</strong>1948. H2A-H2B antibodies and, more recently, H1antibodieshave been implicated <strong>in</strong> this phenomenon, which was an important milestone <strong>in</strong>the discovery of autoantibodies associated with SLE ( LE cell factor).AutoantigensHistones can be found <strong>in</strong> almost all eukaryotic cell nuclei. The histone familyconta<strong>in</strong>s the follow<strong>in</strong>g five basic prote<strong>in</strong>s: H1 (26.5 kDa), H2A (14 kDa), H2B(13.8 kDa), H3 (15.3 kDa) and H4 (10.2 kDa). Histones form complexes withdouble-stranded DNA, called nucleosomes. The DNA thereby wraps arounddimeric H2A-H2B and H3-H4, while H1 b<strong>in</strong>ds to DNA on the surface of thenucleosome. The bead-like nucleosomes help bundle the DNA <strong>in</strong>to a morecompact chromat<strong>in</strong> structure. All histones and histone complexes can be targetedby autoantibodies.Detection Methods• IIF us<strong>in</strong>g HEp-2 cells: Chromat<strong>in</strong> can be visualized like the pattern producedby dsDNA antibodies (homogeneous sta<strong>in</strong><strong>in</strong>g of <strong>in</strong>terphase nuclei and of thechromat<strong>in</strong>region<strong>in</strong>mitoticcells).NOTE: Anegativeimmunofluorescence does not exclude the presence of AHA.• EIA, ALBIA and LIA us<strong>in</strong>g isolated histones or histone mixtures.• RIA us<strong>in</strong>g isolated histones or histone mixtures.• WB.Comments: The conformational epitopes may be altered or destroyed due to solidphase b<strong>in</strong>d<strong>in</strong>g (EIA) and/or the use of SDS-polyacrylamide gel electrophoresis(WB).Cl<strong>in</strong>ical Relevance• With the possible exception of anti-H1, AHA are not specificforanyonedisease,but can be detected <strong>in</strong> a number of autoimmune diseases, especially rheumaticdisorders: <strong>Systemic</strong> lupus erythematosus (SLE; 50–80 %), drug-<strong>in</strong>ducedlupus (DIL; 92–95 %), rheumatoid arthritis (RA; up to 11%), RA vasculitis(up to 75 %), Felty’s syndrome (up to 79 %), juvenile idiopathic arthritis(JIA; up to 51%), systemic sclerosis (SSc; up to 30 %), ANA positive undifferentiatedconnective tissue diseases (up to 90 %), primary biliary cirrhosis (up to55 %), autoimmune hepatitis (up to 35 %). Furthermore,AHA are detectable <strong>in</strong>patients with neoplastic diseases,subacute sensoric neuropathies and <strong>in</strong>fections.
HMG ANTIBODIES 79• High titers of AHA are found almost exclusively <strong>in</strong> patients with SLE and DIL.The detection of high AHA titers <strong>in</strong> the absence of SLE marker antibodies ischaracteristic of drug-<strong>in</strong>duced lupus.• AHAcanbeoftheIgG,IgMorIgAisotype.IgGAHAappeartoberelatedtothe disease activity of lupus.• In patients with SSc, AHA are associated with lung, heart and kidney <strong>in</strong>volvement(Hesselstrand et al., 2003). A strong correlation of AHA with the numberof morphea lesions and the number of <strong>in</strong>volved areas of the body have beendescribed <strong>in</strong> patients with localized sclerodema (Takehara et al., 2005).Indications1. Suspicion of drug-<strong>in</strong>duced lupus (especially after proca<strong>in</strong>amide, hydralaz<strong>in</strong>e,isoniazid, chlorpromaz<strong>in</strong>e, methyldopa, beta blockers, anticonvulsant, sulfasalaz<strong>in</strong>eor captopril use).NOTE: To establish the diagnosis of drug-<strong>in</strong>duced lupus, the potential presenceofSLEmarkerantibodies(i.e., dsDNA and Sm antibodies) must be ruledout us<strong>in</strong>g the appropriate tests.Antihistone antibodies tend to disappear with<strong>in</strong>one year of discont<strong>in</strong>u<strong>in</strong>g the causative drug.2. Differential recognition of ant<strong>in</strong>uclear antibodies <strong>in</strong> sera present<strong>in</strong>g a typicalchromat<strong>in</strong> fluorescence pattern.HMG AntibodiesAutoantigensChromosomal high mobility group (HMG) prote<strong>in</strong>s. The prote<strong>in</strong>s HMG-1, -2, -14and -17 have been described as target prote<strong>in</strong>s of autoantibodies <strong>in</strong>volved <strong>in</strong> systemicautoimmune diseases. Furthermore, antigens with HMG motifs (HMG-boxprote<strong>in</strong>s such as Sp100, SOX13) can be targeted by antibodies from autoimmunepatients (Fida etal., 2002).Detection Methods• WB us<strong>in</strong>g cell extracts or HMG preparations.• EIAus<strong>in</strong>gbiochemicallypurified HMG.
Part 2<strong>Systemic</strong> <strong>Autoimmune</strong> <strong>Diseases</strong> –Syndromes, Diagnostic Criteria,Symptoms
192 SYSTEMIC AUTOIMMUNE DISEASES — SYNDROMES,DIAGNOSTIC,SYMPTOMSAbortion, spontaneousRecurrent spontaneous abortions that generally occur after the 10 th week of gestation(caused by thrombotic events <strong>in</strong> the placenta) are a characteristic sign of antiphospholipid syndrome.Acidosis, renal-tubularRenal manifestation of Sjögren’s syndrome.Acro-OsteolysisOccurs as a typical feature of systemic sclerosis and is a reflection of a severeacral microcirculatory disorder.Addison’s diseaseMay be due to thrombosis of the blood vessels of the adrenal glands as a rarecomplication (
ALVEOLITIS 193AlopeciaDiffuse (alopecia diffusa) or localized alopecia (alopecia areata) may occur <strong>in</strong> cutaneouslupus erythematosus (ANA negative!) or systemic lupus erythematosus.AlveolitisInterstitial lung <strong>in</strong>volvement occurs <strong>in</strong>: <strong>Systemic</strong> lupus erythematosus, Sjögren’s syndrome, Polymyositis/dermatomyositis, <strong>Systemic</strong> sclerosis, Scleroderma/myositis overlap syndrome, Microscopic polyangiitis (hemorrhagic alveolitis is a feared complication!).Typical feature of: Anti-Jo-1 syndrome or anti-synthetase syndrome.See also hemorrhagic alveolitis.Amaurosis fugaxReversible, mostly unilateral bl<strong>in</strong>dness due to ret<strong>in</strong>al circulatory disorder. Rareophthalmologic manifestation of antiphospholipid syndrome (<strong>in</strong> 5 %). Alsosymptom of giant cell arteritis (temporal arteritis).ANCA-associated vasculitisGroup of primary systemic vasculitides associated withANCA ( cANCA/prote<strong>in</strong>ase3antibodies, pANCA/myeloperoxidase antibodies): Wegener’sgranulomatosis(WG), Microscopic polyangiitis (MPA), Churg-Strauss syndrome (CSS).
194 SYSTEMIC AUTOIMMUNE DISEASES — SYNDROMES,DIAGNOSTIC,SYMPTOMSAnemiaAnemia may occur <strong>in</strong> all <strong>in</strong>flammatory diseases and is associated with the degreeof <strong>in</strong>flammatory activity. Coombs-positive autoimmune hemolytic anemia mayoccur <strong>in</strong> systemic lupus erythematosus and rarely <strong>in</strong> other connective tissuediseases. Coombs-positive hemolytic anemia occurs <strong>in</strong> about 9 % of patients with antiphospholipid syndrome.Anti-Jo-1 syndromeOrig<strong>in</strong>al name for anti-synthetase syndrome.Antiphospholipid syndrome(APS)Synonyms: Hughes syndrome, anticardiolip<strong>in</strong> syndrome, phospholipid antibodysyndrome, cardiolip<strong>in</strong> antibody syndromeAPS is one of the most common autoimmune diseases. Its cl<strong>in</strong>ical picture is extremelyvariable, and the complications aris<strong>in</strong>g from the disease may be m<strong>in</strong>imalto life-threaten<strong>in</strong>g. The features of APS <strong>in</strong>clude venous and arterial thrombosis,recurrent spontaneous abortions, neurological complications and phospholipidantibody expression. APS may occur as an isolated disease entity (formerly primaryantiphospholipid syndrome) or <strong>in</strong> comb<strong>in</strong>ation with another autoimmunedisease, especially systemic lupus erythematosus (formerly secondary antiphospholipidsyndrome). Sneddon’s syndrome and Budd-Chiari syndrome are partially attributableto APS. The catastrophic antiphospholipid syndrome is a rare form of APScharacterized by extensive vascular occlusions <strong>in</strong> multiple organ systems, lead<strong>in</strong>gto renal failure and malignant arterial hypertension, severe CNS manifestations,acrocyanosis and gangrene.A workshop, preced<strong>in</strong>g the Eleventh International Congress on antiphospholipidantibodies (aPL) <strong>in</strong> Sydney, Australia, considered revisions to the <strong>in</strong>ternationalclassification criteria for APS.
ANTIPHOSPHOLIPID SYNDROME (APS) 195Revised classification criteria for the APS[accord<strong>in</strong>g to MIYAKIS et al., 2006]Cl<strong>in</strong>ical criteria1. Vascular thrombosis*Oneormorecl<strong>in</strong>icalepisodesofarterial,venous,orsmallvesselthrombosis.Thrombosis must be confirmed by objective validated criteria(i.e.unequivocal f<strong>in</strong>d<strong>in</strong>gs of appropriate imag<strong>in</strong>g studies or histopathology).For histopathologic confirmation, thrombosis should be presentwithout significant evidence of <strong>in</strong>flammation <strong>in</strong> the vessel wall.2. Pregnancy morbiditya) One or more unexpla<strong>in</strong>ed deaths of a morphologically normalfetusatorbeyondthe10 th week of gestation, with normal fetal morphologydocumentedbyultrasoundorbydirectexam<strong>in</strong>ationofthefetus, orb) One or more premature births of a morphologically normal neonatebefore the 34th week of gestation because of (i) eclampsia or severepreeclampsia def<strong>in</strong>ed accord<strong>in</strong>g to standard def<strong>in</strong>itions, or (ii) recognizedfeatures of placental <strong>in</strong>sufficiency, orc) Three or more unexpla<strong>in</strong>ed consecutive spontaneous abortions beforethe 10th week of gestation, with maternal anatomic or hormonalabnormalities and paternal and maternal chromosomal causes excluded.In studies of populations of patients who have more than onetype of pregnancy morbidity, <strong>in</strong>vestigators are strongly encouragedto stratify groups of subjects accord<strong>in</strong>g to a, b, or c above.Laboratory criteria**1. Lupus anticoagulant (LA) present <strong>in</strong> plasma, on two or more occasionsat least 12 weeks apart, detected accord<strong>in</strong>g to the guidel<strong>in</strong>es ofthe International Society on Thrombosis and Haemostasis (ScientificSubcommittee on LAs/phospholipid-dependent antibodies) (Brandt etal., 1995, Wisloff et al., 2002). See Lupus anticoagulant.2. Anticardiolip<strong>in</strong> (aCL) antibody of IgG and/or IgM isotype <strong>in</strong> serum orplasma, present <strong>in</strong> medium or high titer (i.e. > 40 GPL or MPL, or >the 99 th percentile), on two or more occasions, at least l2 weeks apart,measured by a standardized EIA (T<strong>in</strong>cani et al.,2001; Harris et al.,2002;Wong et al., 2004). See Cardiolip<strong>in</strong> antibodies.
196 SYSTEMIC AUTOIMMUNE DISEASES — SYNDROMES,DIAGNOSTIC,SYMPTOMS3. Anti-β 2 glycoprote<strong>in</strong> I antibody of IgG and/or IgM isotype <strong>in</strong> serumor plasma (<strong>in</strong> titer > the 99 th percentile), present on two or moreoccasions, at least 12 weeks apart, measured by a standardized EIA,accord<strong>in</strong>g to recommended procedures (Reber et al., 2004). See β2glycoprote<strong>in</strong> I antibodies.Def<strong>in</strong>ite APS is considered to be present if at least one of the cl<strong>in</strong>icalcriteria and one of the laboratory criteria are met.It must be po<strong>in</strong>ted out that the classificationofAPSshouldbeavoidedif less than 12 weeks or more than 5 years separate the positive aPL testand the cl<strong>in</strong>ical manifestation.∗ Coexist<strong>in</strong>g<strong>in</strong>heritedoracquiredfactorsforthrombosisarenotreasonsforexclud<strong>in</strong>gpatients fromAPS trials.However,two subgroups of APS patients shouldbe recognized, accord<strong>in</strong>g to: (a) the presence, and (b) the absence of additionalrisk factors for thrombosis. Indicative (but not exhaustive) such cases <strong>in</strong>clude:age (> 55 <strong>in</strong> men,and > 65 <strong>in</strong> women),and the presence of any of the establishedrisk factors for cardiovascular disease (hypertension, diabetes mellitus, elevatedLDL or low HDL cholesterol, cigarette smok<strong>in</strong>g, family history of premature cardiovasculardisease,body mass <strong>in</strong>dex ≥ 30 kg m –2 , microalbum<strong>in</strong>uria,estimatedCFR < 60 ml m<strong>in</strong> –1 ), <strong>in</strong>herited thrombophilias, oral contraceptives, nephroticsyndrome, malignancy, immobilization, and surgery. Thus, patients who fulfilcriteria should be stratified accord<strong>in</strong>g to contribut<strong>in</strong>g causes of thrombosis.∗∗ Investigators are strongly advised to classify APS patients <strong>in</strong> studies <strong>in</strong>to oneof the follow<strong>in</strong>g categories: I, more than one laboratory criteria present (anycomb<strong>in</strong>ation); IIa, LA present alone; IIb, aCL antibody present alone; IIc, anti-β2 glycoprote<strong>in</strong> I antibody present alone.Features associated with APS but not <strong>in</strong>cluded <strong>in</strong> the revised criteria:• heart valve disease (Libman-Sacks endocarditis; rheumatic fever and septic endocarditishave to be excluded)• livedo reticularis• thrombocytopenia• nephropathy• neurological manifestations (cognitive dysfunction, transient cerebral ischemiaand stroke, dementia, transverse myelopathy, seizure)• IgA aCL• IgA anti-β 2GPI• antibodies aga<strong>in</strong>st phosphatidylser<strong>in</strong>e• antibodies aga<strong>in</strong>st phosphatidylethanolam<strong>in</strong>e
ANTI-SRP SYNDROME 197• antibodies aga<strong>in</strong>st prothromb<strong>in</strong> alone• antibodies to the phophatidylser<strong>in</strong>e-prothromb<strong>in</strong> complex<strong>Autoantibodies</strong>: Phospholipid antibodies (see also appendix VI)Anti-SRP syndromeA subtype of idiopathic myositis (see Polymyositis).Characteristic features:• Predom<strong>in</strong>antly occurs <strong>in</strong> women of black African descent• Acute/subacute onset with severe polymyositis• Cardiac <strong>in</strong>volvement frequently occurs• Severe myonecrosis with only m<strong>in</strong>imal <strong>in</strong>flammation• Responds poorly to immunosuppressive therapy; very poor prognosis (5-yearmortality of 75 %!)Comment: In rare cases atypical cl<strong>in</strong>ical manifestations may occur <strong>in</strong> the presenceof necrotiz<strong>in</strong>g myopathy (Dimitri et al., 2007).<strong>Autoantibodies</strong>: SRP antibodies serve as diagnostic marker. Ro52 antibodiescan be found but did not have any diagnostic or prognostic relevance.Anti-Synthetase syndromeSynonym: Anti-Jo-1 syndrome.Subtype of idiopathic myositis (see Polymyositis) characterized by the additionaloccurrence of arthralgia/arthritis and <strong>in</strong>terstitial lung <strong>in</strong>volvement (alveolitis,pulmonary fibrosis) and the detection of autoantibodies that react with tRNAsynthetases (especially Jo-1).Major criteria of the anti-synthetase syndrome1. Polymyositis2. Polysynovitis (arthralgia, arthritis, tenosynovitis)
198 SYSTEMIC AUTOIMMUNE DISEASES — SYNDROMES,DIAGNOSTIC,SYMPTOMS3. Interstitial lung disease (fibros<strong>in</strong>g alveolitis)4. Am<strong>in</strong>oacyl-tRNA synthetase antibodiesAdditional associations• Rhagades and keratoses of the hands (“mechanic’s hands”)• Raynaud’s phenomenon• Acrosclerosis• Sicca symptoms• Dermatomyositis-like sk<strong>in</strong> manifestations<strong>Autoantibodies</strong>: Am<strong>in</strong>oacyl-tRNA synthetase antibodies are diagnostic markers.Among these, Jo-1 antibody is the most common detectable biomarker. Ro52 antibodies are found at high frequencies but without aid <strong>in</strong> diagnos<strong>in</strong>gthis type of autoimmune myositis.ArthralgiaCommon feature of all degenerative and <strong>in</strong>flammatory rheumatic diseases; frequentlyoccurs as a manifestation of systemic and organ-specific autoimmunediseases.<strong>Autoantibodies</strong>: Patients suspicious for <strong>in</strong>flammatory rheumatic disease shouldbe screened for ant<strong>in</strong>uclear antibodies (ANA), ant<strong>in</strong>eutrophil cytoplasmic antibodies(ANCA), CCP/citrull<strong>in</strong>ated prote<strong>in</strong>/peptide antibodies and rheumatoidfactor (RF).ArthritisCharacteristic feature of <strong>in</strong>flammatory jo<strong>in</strong>t diseases: HLA-B27 associatedspondylarthropathia, juvenile chronic arthritis (JIA), rheumatoid arthritis(RA).Common symptom of systemic autoimmune diseases: Connective tissuediseases, systemic vasculitides, relaps<strong>in</strong>g polychondritis, hypocomplementemicurticarial vasculitis syndrome.<strong>Autoantibodies</strong>: Patients suspicious for <strong>in</strong>flammatory rheumatic diseases shouldbe screened for ant<strong>in</strong>uclear antibodies (ANA), ant<strong>in</strong>eutrophil cytoplasmic