Anthem EPO - ES Represented Sunnyvale - Benefits
Anthem EPO - ES Represented Sunnyvale - Benefits
Anthem EPO - ES Represented Sunnyvale - Benefits

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
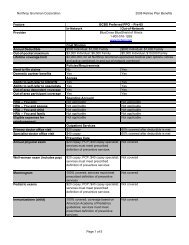
Northrop Grumman Health Plan<strong>Benefits</strong> Summary - Plan Year 7/1/11 - 6/30/12Plan Facts<strong>Anthem</strong> <strong>EPO</strong> - <strong>ES</strong> Rep <strong>Sunnyvale</strong>Web sitewww.anthem.com/caMember services 1-866-504-9638Domestic partner benefitsYesAdditional commentsSee SPD or check with Plan for detailsCost<strong>Anthem</strong> <strong>EPO</strong> - <strong>ES</strong> Rep <strong>Sunnyvale</strong>You onlyYou and spouseYou and child(ren)You and familyEligible expenses for reimbursementContact NGBCContact NGBCContact NGBCContact NGBCNot applicableAnnual deductible$0 Individual; $0 FamilyPrimary doctor office visit$10 copaySpecialist office visit$20 copayOut-of-pocket maximum$0 Individual; $0 FamilyLifetime coverage limitLimit does not applyHospital copay100% coveredHospital semi-private room100% covered
Inpatient lab and X-ray100% coveredInpatient surgery100% coveredInpatient physician and surgeon services100% coveredOutpatient surgery100% coveredOutpatient laboratory services100% coveredOutpatient X-ray100% coveredEmergency room (not followed by admission)100% covered after $100 copay; per ER visit; waivedif admittedUrgent care clinic visitPaid at level of services billed; $20 copay if billed asoffice visit; ER visit level if billed as ER visitOutpatient cardiac rehabilitation$20 copay; limited to Phase 1 and Phase 2 carePrescription drug vendorExpress ScriptsPrescription drug Web sitewww.express-scripts.comPrescription drug member services 1-800-655-1971Annual prescription deductible$0 Individual; $0 Family
Annual Rx out-of-pocket maximum$1,500 Individual; $3,000 FamilyRetail generic$5 copay or 10% coinsurance whichever is greater; 30day supplyRetail formulary brand$20 copay or 10% coinsurance whichever is greater;30 day supplyRetail nonformulary brand$40 copay or 10% coinsurance whichever is greater;30 day supplyMail order generic $5 copay or 10% coinsurance whichever is greater; 90day supplyMail order formulary brand$20 copay or 10% coinsurance whichever is greater;90 day supplyMail order nonformulary brand$40 copay or 10% coinsurance whichever is greater;90 day supplyOral contraceptivesRetail and mail order available; applicable prescriptiondrug copay applies; check with Plan for detailsFertility drugsCovered under MedicalCoverage<strong>Anthem</strong> <strong>EPO</strong> - <strong>ES</strong> Rep <strong>Sunnyvale</strong>Annual physical exam100% covered; services must meet prescribeddefinition of preventive services; check with Plan fordetailsWell-woman exam (includes pap)100% covered; services must meet prescribeddefinition of preventive services; check with Plan fordetailsMammogram100% covered; services must meet prescribeddefinition of preventive services; check with Plan fordetailsColonoscopy100% covered; services must meet prescribedf f f
definition of preventive services; check with Plan fordetailsCancer screenings100% covered; services must meet prescribeddefinition of preventive services; check with Plan fordetailsCardiovascular screenings100% covered; services must meet prescribeddefinition of preventive services; check with Plan fordetailsAllergy tests and treatments100% covered; injections; $10 copay PCP/$20 copayspecialist for physician testingFertility services100% covered; after applicable copays; limited to$25,000 per lifetime including prescription drugsIn vitro fertilization100% covered; after applicable copays; limited to$25,000 per lifetime for all fertility services combinedincluding prescription drugsArtificial insemination100% covered; after applicable copays; limited to$25,000 per lifetime for all fertility services combinedincluding prescription drugsFemale tubal ligation100% covered; in or outpatient hospital setting; $10copay PCP/$20 copay specialist in office setting;applicable prescription drug copays applyMale vasectomy100% covered; in or outpatient hospital setting; $10copay PCP/$20 copay specialist in office setting;applicable prescription drug copays applyOffice visit: Pre/postnatal$10 copay initial visit only; PCP; $20 copay specialistinitial visit only; a copay may apply to subsequentvisits due to complicationsIn-hospital delivery services100% coveredNewborn nursery services100% covered
Pediatric exams100% covered; services must meet prescribeddefinition of preventive services; check with Plan fordetailsImmunizations (child)100% covered; cov based on American Academy ofPediatrics guidelines; services must meet prescribeddefinition of preventive services; check with Plan fordetailsMental Health: Combined with substance abuseNot applicableMental Health: Outpatient coverage$10 copay; preauthorization is required for additionalservices beyond 12 visitsMental Health: Inpatient coverage100% covered; preauthorization requiredBehavioral health member servicesBehavioral health vendorBehavioral health Web siteSame as medical planSame as medical planSame as medical planDetox: Outpatient coverage$10 copay; preauthorization is required for additionalservices beyond 12 visitsDetox: Inpatient coverage100% covered; preauthorization requiredRehab: Outpatient coverage$10 copay; preauthorization is required for additionalservices beyond 12 visitsRehab: Inpatient coverage100% covered; preauthorization required
Dental implantsNot coveredAccidental injury to teeth100% covered; limitations apply; see SPD or checkwith Plan for detailsSurgical removal of tumors, cysts, and impacted teeth100% covered; limited to surgical removal of tumorsand cysts; removal of impacted teeth not coveredRoutine vision exams$10 copay; limited to PCP screening only; limited toone exam per benefit plan yearRegular lenses and framesNot coveredContact lensesNot coveredHearing evaluations100% covered; applicable copay applies to examHearing aids100% covered; limited to 2 hearing aids per benefitplan year; applicable copay applies to examAcupuncture$20 copay; limited to 20 visits per benefit plan year;acupuncture and acupressure combinedChiropractic$20 copay; limited to 40 visits per calendar yearOutpatient physical therapy$20 copay; limited to 50 visits per benefit plan year;not combined with any other therapy
Outpatient speech therapy$20 copay; limited to 50 visits per benefit plan year;not combined with any other therapyOutpatient occupational therapy$20 copay; limited to 50 visits per benefit plan year;not combined with any other therapyNoncustodial home health care100% covered; limited to 120 visits per benefit planyearPrescribed care in noncustodial skilled nursing facility100% covered; limited to 120 days per benefit planyearHospice care100% coveredAmbulance servicesProsthetic devices100% covered100% covered; must be medically necessaryAccessOut-of-area dependent coverageOut-of-area participant coverageDomestic partner benefitsEase of UseAbility to self-refer to OB/GYNAbility to self-refer to specialistsMember Satisfaction<strong>Anthem</strong> <strong>EPO</strong> - <strong>ES</strong> Rep <strong>Sunnyvale</strong>YesYesYes<strong>Anthem</strong> <strong>EPO</strong> - <strong>ES</strong> Rep <strong>Sunnyvale</strong>YesYes<strong>Anthem</strong> <strong>EPO</strong> - <strong>ES</strong> Rep <strong>Sunnyvale</strong>Health plan averageNational averageNot availableNot available
Health plan averageNational averageNot availableNot availableHealth plan averageNational averageNot availableNot availableHealth plan averageNational averageNot availableNot availableCare Management: Education and Assistance<strong>Anthem</strong> <strong>EPO</strong> - <strong>ES</strong> Rep <strong>Sunnyvale</strong>Asthma care managementCancer care managementDiabetes care managementHeart disease care managementHypertension care managementSmoking cessation programWeight control programPrenatal care managementYesNoYesYesNoNoNoNoThe comparison charts are compiled using information that applies to a large number of health plan users andis commonly reported by the health plans. Depending on the chart type, such as charts for dental and visionplans, certain information and/or sections won't appear because the necessary data isn't available. If you havequestions about a topic that isn't covered in the charts, refer to the plan's SPD or contact the health provider'smember services department for additional information. Also, keep in mind that the information on access andquality of care is provided by the health plans. Neither Northrop Grumman nor Hewitt Associates is responsiblefor the accuracy of this information. If there is a discrepancy between the information displayed on thesecharts and the official plan documents, the official plan documents will control. Northrop Grumman reservesthe right to amend, suspend, or terminate the plan(s) or program(s) at any time.