Recommended Approach to a Pleural Effusion on Chest X-ray
Recommended Approach to a Pleural Effusion on Chest X-ray
Recommended Approach to a Pleural Effusion on Chest X-ray

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Pulm<strong>on</strong>ary Critical CareDIAGNOSIS OFPLEURAL EFFUSION:A SYSTEMATIC APPROACHBy Emmet E. McGrath, MB, PhD, MRCPI, and Paul B. Anders<strong>on</strong>, MA, FRCPC E 1.0 HourNotice <str<strong>on</strong>g>to</str<strong>on</strong>g> CE enrollees:A closed-book, multiple-choice examinati<strong>on</strong>following this article tests your under standing ofthe following objectives:1. Identify 3 characteristics of abnormal pleuralfluid.2. Describe a systematic algorithm for the investigati<strong>on</strong>of pleural effusi<strong>on</strong>s.3. Differentiate between extudates and transdates.To read this article and take the CE test <strong>on</strong>line,visit www.ajcc<strong>on</strong>line.org and click “CE Articlesin This Issue.” No CE test fee for AACN members.©2011 American Associati<strong>on</strong> of Critical-Care Nursesdoi: 10.4037/ajcc2011685In most diseases related <str<strong>on</strong>g>to</str<strong>on</strong>g> pleural effusi<strong>on</strong>, the fluid analysisyields important diagnostic informati<strong>on</strong>, and in certain cases,fluid analysis al<strong>on</strong>e is enough for diagnosis.The many importantcharacteristics of pleural fluid are described, as are othercomplementary investigati<strong>on</strong>s that can assist with the diagnosisof comm<strong>on</strong> and rare pleural effusi<strong>on</strong>s. For a systematicreview of pleural effusi<strong>on</strong>, a literature search for articles <strong>on</strong>the practical investigati<strong>on</strong> and diagnosis of pleural effusi<strong>on</strong>was d<strong>on</strong>e. Articles included guidelines, expert opini<strong>on</strong>, experimentaland n<strong>on</strong>experimental studies, literature reviews, andsystematic reviews published from May 2003 through June2009.The search yielded 1 guideline, 2 meta-analyses, 9 literaturereviews, 1 randomized c<strong>on</strong>trol trial, and 9 clinical studies.On the basis of class IIa or class I evidence from these articles,a step by step approach is recommended for investigating apleural effusi<strong>on</strong>, beginning with assessment of the medicalhis<str<strong>on</strong>g>to</str<strong>on</strong>g>ry, clinical examinati<strong>on</strong>, radiology, pleural fluid evaluati<strong>on</strong>,and finally, if no diagnosis is forthcoming, a pleuralbiopsy under image guidance or thoracoscopy. (AmericanJournal of Critical Care. 2011;20:119-128)www.ajcc<strong>on</strong>line.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2011, Volume 20, No. 2 119
In a normal pleural space, fluid enters and exits at a c<strong>on</strong>stant, equal rate because of the<strong>on</strong>going filtrati<strong>on</strong> of a small amount of low-protein liquid in normal microvessels. Nearthe end of the 19th century, Starling and Tubby 1 hypothesized that the exchange of microvascularfluid and solutes was governed by the balance between hydrostatic pressure,osmotic pressure, and membrane permeability, and they devised the Starling equati<strong>on</strong>:QF = LP × A[(PCAP - PPL) - ζD(piCAP - piPL)]where QF is fluid movement, LP is the filtrati<strong>on</strong> coefficient, A is the surface area of the pleura,ζD is the reflecti<strong>on</strong> coefficient for protein movement across the pleura (PL), P is the hydrostaticpressure of the pulm<strong>on</strong>ary capillary bed (CAP), and pi is the <strong>on</strong>cotic pressure of pleural space. 1,2This equati<strong>on</strong> formed the basis for understanding fluid accumulati<strong>on</strong> in the pleural space,where the hydrostatic forces that filter water out of the vessel are balanced by osmotic forcesthat reabsorb water back in<str<strong>on</strong>g>to</str<strong>on</strong>g> the vessel. In the pleura, reabsorpti<strong>on</strong> is facilitated by the extensivelymphatic system <strong>on</strong> the diaphragm and mediastinal surfaces of the parietal pleura. 2The most comm<strong>on</strong>c<strong>on</strong>diti<strong>on</strong>s causingeffusi<strong>on</strong>s arecardiac failure,pneum<strong>on</strong>ia,and malignantneoplasm.Fluid accumulati<strong>on</strong> in the pleural space indicatesdisease. The accumulati<strong>on</strong> is associated with manymedical c<strong>on</strong>diti<strong>on</strong>s that predispose <str<strong>on</strong>g>to</str<strong>on</strong>g> fluid accumulati<strong>on</strong>via many different mechanisms, includingincreased pulm<strong>on</strong>ary capillary pressure, decreased<strong>on</strong>cotic pressure, increased pleuralmembrane permeability, and obstructi<strong>on</strong>of lymphatic flow. 3The most comm<strong>on</strong> c<strong>on</strong>diti<strong>on</strong>s thatresult in effusi<strong>on</strong>s are cardiac failure,pneum<strong>on</strong>ia, and malignant neoplasm.Diagnosis of a pleural effusi<strong>on</strong> beginswith obtaining the patient’s clinical his<str<strong>on</strong>g>to</str<strong>on</strong>g>ryand doing a physical examinati<strong>on</strong>and is followed by chest radiographyand analysis of pleural fluid in appropriateinstances. If necessary, theprocess c<strong>on</strong>tinues with further investigativestudies, such as computed <str<strong>on</strong>g>to</str<strong>on</strong>g>mography (CT)of the thorax, pleural biopsy, thoracoscopy, and,occasi<strong>on</strong>ally, br<strong>on</strong>choscopy.MethodsArticles used for this review were selected byusing MEDLINE <str<strong>on</strong>g>to</str<strong>on</strong>g> search for English-language articles<strong>on</strong> pleural effusi<strong>on</strong> published from May 2003About the AuthorsEmmet E. McGrath was a clinical lecturer in respira<str<strong>on</strong>g>to</str<strong>on</strong>g>rymedicine and Paul B. Anders<strong>on</strong> was a c<strong>on</strong>sultant respira<str<strong>on</strong>g>to</str<strong>on</strong>g>ryphysician in the Department of Respira<str<strong>on</strong>g>to</str<strong>on</strong>g>ry Medicine,Northern General Hospital, Sheffield, England at the timethis article was written.Corresp<strong>on</strong>ding author: Dr Emmet McGrath, Senior Lecturerin Respira<str<strong>on</strong>g>to</str<strong>on</strong>g>ry Medicine, Department of Respira<str<strong>on</strong>g>to</str<strong>on</strong>g>ryMedicine, Birmingham Heartlands Hospital, Birmingham,United Kingdom (e-mail: e.e.mcgrath@bham.ac.uk).through June 2009. In additi<strong>on</strong>, hand searching ofthe bibliographies of retrieved articles was d<strong>on</strong>e byrecognized world authorities <strong>on</strong> pleural effusi<strong>on</strong>s.Keywords used for the search were pleural effusi<strong>on</strong>,investigati<strong>on</strong>, and diagnosis. All types of evidence(guidelines, expert opini<strong>on</strong>, experimental and n<strong>on</strong>experimentalstudies, literature reviews, and systematicreviews) in English were examined, but <strong>on</strong>lymaterial that involved the practical and clinical investigati<strong>on</strong>and diagnosis of pleural effusi<strong>on</strong> in adultswas included in the final review. Case reports wereexcluded. Important articles by world leading expertscited in articles from the search were also reviewed.ResultsAlthough many articles have been written <strong>on</strong>pleural effusi<strong>on</strong>, the number included in our reviewwas markedly reduced when <strong>on</strong>ly English-languagepublicati<strong>on</strong>s about the clinical and practical investigati<strong>on</strong>and diagnosis of this abnormality weresought by using the key words investigati<strong>on</strong> anddiagnosis <str<strong>on</strong>g>to</str<strong>on</strong>g>gether. The number was also reducedfurther when case reports were excluded. From May2003 through June 2009, a <str<strong>on</strong>g>to</str<strong>on</strong>g>tal of 1 guideline, 3 2meta-analyses, 4,5 9 literature reviews, 6-14 1 randomizedc<strong>on</strong>trolled trial, 15 and 9 clinical studies 16-24 <strong>on</strong> thepractical investigati<strong>on</strong> and diagnosis of pleural effusi<strong>on</strong>were published in peer-reviewed journals.Evidence was assessed as class I, class IIa, classIIb, indeterminate, and class III. 25 Class I evidence isdefinite recommendati<strong>on</strong> of a practice that is based<strong>on</strong> the results of at least 1 randomized c<strong>on</strong>trolledtrial and is c<strong>on</strong>sidered a definitive standard of careor best practice. Good evidence and expert opini<strong>on</strong>are c<strong>on</strong>sidered class II. Fair <str<strong>on</strong>g>to</str<strong>on</strong>g> good evidence is classifiedas class IIb. A finding of no benefit or harm120 AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2011, Volume 20, No. 2 www.ajcc<strong>on</strong>line.org
is c<strong>on</strong>sidered indeterminate; usually evidence isclassified as indeterminate because it is insufficient(eg, evidence provided by preliminary data). ClassIII evidence is evidence that is not useful and maybe harmful.Clinical Features of <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> <str<strong>on</strong>g>Effusi<strong>on</strong></str<strong>on</strong>g>sThe clinical his<str<strong>on</strong>g>to</str<strong>on</strong>g>ry and physical examinati<strong>on</strong>can be quite helpful in indicating appropriate investigati<strong>on</strong>.Patients with pleural effusi<strong>on</strong>s usually havedyspnea, cough, and occasi<strong>on</strong>al sharp n<strong>on</strong>radiatingchest pain that is often pleuritic. A his<str<strong>on</strong>g>to</str<strong>on</strong>g>ry of cardiac,renal, or liver impairment can suggest a transudativeeffusi<strong>on</strong>. A his<str<strong>on</strong>g>to</str<strong>on</strong>g>ry of cancer can besuggestive of a malignant pleural effusi<strong>on</strong>. Recentleg swelling or deep-vein thrombosis may result inan effusi<strong>on</strong> related <str<strong>on</strong>g>to</str<strong>on</strong>g> pulm<strong>on</strong>ary embolism. 6 A his<str<strong>on</strong>g>to</str<strong>on</strong>g>ryof recent or current pneum<strong>on</strong>ia suggests a parapneum<strong>on</strong>iceffusi<strong>on</strong>, either complicated (empyema) oruncomplicated. Previous trauma may result in hemothoraxor chylothorax. Previous exposure <str<strong>on</strong>g>to</str<strong>on</strong>g> asbes<str<strong>on</strong>g>to</str<strong>on</strong>g>s iscomm<strong>on</strong> in patients who have a benign effusi<strong>on</strong> related<str<strong>on</strong>g>to</str<strong>on</strong>g> the exposure or have mesothelioma. 6 Recentesophageal dilatati<strong>on</strong> or endoscopy can result inesophageal rupture. Certain medicati<strong>on</strong>s, includingamiodar<strong>on</strong>e, methotrexate, pheny<str<strong>on</strong>g>to</str<strong>on</strong>g>in, and nitrofuran<str<strong>on</strong>g>to</str<strong>on</strong>g>in,can cause pleural effusi<strong>on</strong>s. 3 Rheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>idarthritis and other au<str<strong>on</strong>g>to</str<strong>on</strong>g>immune c<strong>on</strong>diti<strong>on</strong>s canalso result in effusi<strong>on</strong>s.A sign such as hemoptysis may be associatedwith a malignant neoplasm, pulm<strong>on</strong>ary embolism,or severe tuberculosis. Fever occurs in tuberculosis,empyema, and pneum<strong>on</strong>ia. Weight loss can be associatedwith a malignant neoplasm and tuberculosis.Physical findings such as ascites may indicatecirrhosis, ovarian cancer, or Meig syndrome. 6 Unilateralleg swelling can str<strong>on</strong>gly indicate pulm<strong>on</strong>aryembolism, and bilateral leg swelling is associatedwith transudates such as those caused by heart or liverfailure. A pericardial fricti<strong>on</strong> rub occurs in pericarditis.In general, the clinician moves from suspecting effusi<strong>on</strong><strong>on</strong> the basis of clinical his<str<strong>on</strong>g>to</str<strong>on</strong>g>ry and examinati<strong>on</strong><str<strong>on</strong>g>to</str<strong>on</strong>g> proving an effusi<strong>on</strong> exists by means of chest radiographybefore fluid sampling is c<strong>on</strong>sidered.For a unilateral pleural effusi<strong>on</strong> evident <strong>on</strong> chestradiographs, the differential diagnosis is extensive(Table 1). The differential diagnosis for bilateralpleural effusi<strong>on</strong>s is narrower and includes causes oftransudative effusi<strong>on</strong>s, such as cardiac, hepatic, andrenal failure and hypoalbuminemia, and in rare cases,malignant neoplasm, pulm<strong>on</strong>ary embolism, andrheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>id arthritis. C<strong>on</strong>gestive heart failure is themost comm<strong>on</strong> cause of bilateral pleural effusi<strong>on</strong>,and in patients with clinical or radiological evidenceTable 1Causes of transudative andexudative unilateral effusi<strong>on</strong> aTypeComm<strong>on</strong>Less comm<strong>on</strong>RareExudateParapneum<strong>on</strong>ic effusi<strong>on</strong>sMalignant neoplasmPulm<strong>on</strong>ary embolismRheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>id arthritisBenign effusi<strong>on</strong> associatedwith exposure <str<strong>on</strong>g>to</str<strong>on</strong>g> asbes<str<strong>on</strong>g>to</str<strong>on</strong>g>sPancreatitisAfter myocardial infarcti<strong>on</strong>syndromeAu<str<strong>on</strong>g>to</str<strong>on</strong>g>immune diseasesAfter cor<strong>on</strong>ary artery bypasssurgerySubphrenic, hepatic, orsplenic abscessUremiaChylothoraxOther infecti<strong>on</strong>sDrug inducedRadiotherapyEsophageal rupturea Based <strong>on</strong> data from Maskell et al. 3of c<strong>on</strong>gestive heart failure, investigati<strong>on</strong> of the effusi<strong>on</strong>need not go any further. 3 Diagnostic thoracentesisis required <strong>on</strong>ly if a patient has bilateral effusi<strong>on</strong>sthat are unequal in size, has an effusi<strong>on</strong> that doesnot resp<strong>on</strong>d <str<strong>on</strong>g>to</str<strong>on</strong>g> therapy, has pleuriticchest pain, or is febrile. 6 The effusi<strong>on</strong>susually improve quite quickly <strong>on</strong>cediuretic therapy is started.Diagnostic ThoracentesisThoracentesis with analysis ofthe fluid can quickly narrow the differentialdiagnosis of an effusi<strong>on</strong>.Most aspirates c<strong>on</strong>sist of a straw-yellowfluid; this finding is n<strong>on</strong>specificbecause it occurs in many types of pleural effusi<strong>on</strong>.However, other appearances can be helpful (Table 2).The fluid may be bloodstained in c<strong>on</strong>diti<strong>on</strong>s suchas pneum<strong>on</strong>ia, malignant neoplasm, pulm<strong>on</strong>aryTransudateLeft ventricular failureCirrhotic liver diseaseHypoalbuminemiaPeri<str<strong>on</strong>g>to</str<strong>on</strong>g>neal dialysisNephrotic syndromePulm<strong>on</strong>ary embolismHypothyroidismMitral stenosisC<strong>on</strong>strictive pericarditisMeig syndromeUrinothoraxSuperior vena cavaobstructi<strong>on</strong>Ovarian hyperstimulati<strong>on</strong>Symp<str<strong>on</strong>g>to</str<strong>on</strong>g>ms includedyspnea, cough,and occasi<strong>on</strong>allysharp, n<strong>on</strong>radiating,pleuriticchest pain.www.ajcc<strong>on</strong>line.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2011, Volume 20, No. 2 121
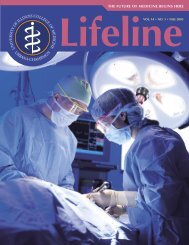
Table 2Relati<strong>on</strong>ship between pleural fluidappearance and causes aCausePseudochylothorax and chylothoraxUrinothoraxAnaerobic empyemaChylothoraxAspergillus infecti<strong>on</strong>EmpyemaAmebic liver abscessEsophageal ruptureTrauma, pulm<strong>on</strong>ary embolism, benignasbes<str<strong>on</strong>g>to</str<strong>on</strong>g>s-related effusi<strong>on</strong>, pneum<strong>on</strong>ia,malignant neoplasm, aftermyocardial infarcti<strong>on</strong> syndromea Based <strong>on</strong> data from Maskell et al. 3Figure 1 Milky pleural aspirate.Table 3Light’s criteria for distinguishing betweenpleural exudates and transudatesFluid appearance/odorMilky whiteUrinePutridBile stainedBlackTurbid“Anchovy” brownFood particlesBloodstainedFluid is an exudate if 1 or more of the following criteria are met1. Ratio of pleural fluid level of lactate dehydrogenase (LDH) <str<strong>on</strong>g>to</str<strong>on</strong>g> serumlevel of LDH is greater than 0.62. <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> fluid level of LDH is more than two-thirds the upper limit ofthe reference range for the serum level of LDH3. Ratio of pleural fluid level of protein <str<strong>on</strong>g>to</str<strong>on</strong>g> serum level of protein isgreater than 0.5embolism with infarcti<strong>on</strong>, benign effusi<strong>on</strong> related<str<strong>on</strong>g>to</str<strong>on</strong>g> asbes<str<strong>on</strong>g>to</str<strong>on</strong>g>s exposure, and trauma. 19 In franklybloody effusi<strong>on</strong>s, a fluid hema<str<strong>on</strong>g>to</str<strong>on</strong>g>crit level greaterthan half the serum hema<str<strong>on</strong>g>to</str<strong>on</strong>g>crit level is indicativeof hemothorax. 3 If the fluid is particularly turbid ormilky (Figure 1), centrifugati<strong>on</strong> is useful in differentiatingempyema from chylothorax or pseudochylothorax.In empyema, the supernatant fluid is clearwhere the cell debris forms a pellet. In chylothoraxor pseudochylothorax, the fluid remains uniformdue <str<strong>on</strong>g>to</str<strong>on</strong>g> the high lipid c<strong>on</strong>tent. 3 Anchovy-brown fluidand black fluid are indicative of amebic liverabscess and Aspergillus infecti<strong>on</strong>, respectively.Once aspirated, the fluid is sent for biochemical,microbiological, and cy<str<strong>on</strong>g>to</str<strong>on</strong>g>logical analyses. Biochemicalanalyses include determinati<strong>on</strong> of protein, pH,lactic dehydrogenase, glucose, and albumin levels.Because it enters the pleural space with water, proteinhas become an important marker in the differentiati<strong>on</strong>of transudates from exudates.A pleural effusi<strong>on</strong> with a protein level less than30 g/L indicates a transudate, whereas <strong>on</strong>e with alevel greater than 30 g/L indicates an exudate, providedthe serum protein level is within the normalreference range. When a protein level greater than30 g/L is used as the <strong>on</strong>ly basis for determining thetype of effusi<strong>on</strong>, 10% of exudates and 15% of transudatesare misclassified. 26 C<strong>on</strong>sequently, the use ofLight’s criteria (Table 3) is recommended when theprotein level is between 25 and 35 g/L. 27 Use of thesecriteria requires the additi<strong>on</strong>al measurement of apatient’s serum levels of lactic dehydrogenase andprotein. Although Light’s criteria are almost 100%sensitive for exudates, in a prospective comparativestudy of pleural effusi<strong>on</strong>s in 172 patients, Porcel et al 28found that approximately 20% of the patients withheart failure who were taking diuretics also metLight’s criteria for an exudate. In such instances, ifthe difference between serum and pleural levels ofprotein is greater than 31 g/L, the effusi<strong>on</strong> shouldbe classified as a transudate. 29 Albumin levels canalso be used in this manner: a difference of morethan 12 g/L between serum and fluid levels indicatesa transudate. 30 Of note, a large percentage ofexudates will be misclassified if these gradients areused as the <strong>on</strong>ly method of differentiating betweentransudates and exudates. 6A pH less than 7.2 in infected effusi<strong>on</strong>s indicatesa complicated parapneum<strong>on</strong>ic effusi<strong>on</strong> (empyema)until proved otherwise, and inserti<strong>on</strong> of chest drainand fluid removal are priorities. 3,6 A low pH can alsooccur in esophageal rupture, rheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>id arthritis,and malignant neoplasm associated with poor outcome.6 Elevated levels of lactate dehydrogenase occurin lymphoma and tuberculosis; levels greater than1000 U/L (<str<strong>on</strong>g>to</str<strong>on</strong>g> c<strong>on</strong>vert units per liter <str<strong>on</strong>g>to</str<strong>on</strong>g> microkatalsper liter, multiply by 0.0167) are associated withempyema. 6 In an exudative effusi<strong>on</strong>, pleural glucose122 AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2011, Volume 20, No. 2 www.ajcc<strong>on</strong>line.org
levels less than 28.8 mg/dL (<str<strong>on</strong>g>to</str<strong>on</strong>g> c<strong>on</strong>vert milligramsper deciliter <str<strong>on</strong>g>to</str<strong>on</strong>g> millimoles per liter, multiply by0.0555) occur in tuberculosis, malignant neoplasm,empyema, rheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>id arthritis, systemic lupus erythema<str<strong>on</strong>g>to</str<strong>on</strong>g>sus,and esophageal rupture. Rheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>idarthritis probably is not resp<strong>on</strong>sible for a pleuraleffusi<strong>on</strong> if the fluid glucose level is greater than1.6 mmol/L. 3 Cell differential analysis can also helpnarrow the differential diagnosis. Fluid lymphocy<str<strong>on</strong>g>to</str<strong>on</strong>g>sisoccurs in c<strong>on</strong>diti<strong>on</strong>s such as tuberculosis, sarcoidosis,chylothorax, rheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>id arthritis, andmalignant neoplasm, including lymphoma. 30,31<str<strong>on</strong>g>Pleural</str<strong>on</strong>g> fluid predominated by neutrophils isassociated with pulm<strong>on</strong>ary embolism, parapneum<strong>on</strong>iceffusi<strong>on</strong>, acute tuberculosis, and benign effusi<strong>on</strong>related <str<strong>on</strong>g>to</str<strong>on</strong>g> exposure <str<strong>on</strong>g>to</str<strong>on</strong>g> asbes<str<strong>on</strong>g>to</str<strong>on</strong>g>s. 31A predominance of eosinophils in pleural fluidhas no diagnostic value, and up <str<strong>on</strong>g>to</str<strong>on</strong>g> <strong>on</strong>e-third of thistype of effusi<strong>on</strong> is never diagnosed. 32 However, effusi<strong>on</strong>swith mostly eosinophils have been associatedwith air or blood in the pleural space. 6Routine microbiological analysis includes sendinga fluid sample for Gram and Ziehl-Neels<strong>on</strong> stainsand cultures <str<strong>on</strong>g>to</str<strong>on</strong>g> detect mycobacteria and other bacteria.Cy<str<strong>on</strong>g>to</str<strong>on</strong>g>logical analysis is extremely important ifa malignant neoplasm is suspected, and the analysesare positive for a malignant tumor in 60% ofpatients who have such a neoplasm. 3 If the firstsample is negative for tumor, sending a sec<strong>on</strong>dsample is worthwhile because analysis of 2 samplesmarkedly increases the chance of diagnosis ofmalignant neoplasm. 33Levels of adenosine deaminase (ADA) levels areparticularly useful in areas where the prevalence oftuberculosis is high. An ADA level greater than 40 U/L(<str<strong>on</strong>g>to</str<strong>on</strong>g> c<strong>on</strong>vert units per liter <str<strong>on</strong>g>to</str<strong>on</strong>g> nanokatals per liter,multiply by 16.667) has a sensitivity of more than90% and a specificity of about 85% for the presenceof tuberculosis. 4,34 In lymphocyte-predominant effusi<strong>on</strong>s,the specificity of ADA for tuberculosis increases<str<strong>on</strong>g>to</str<strong>on</strong>g> more than 95%. Elevated ADA also occurs withmalignant neoplasm, empyema, and rheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>idarthritis. 35 Of note, ADA levels may be normal inthe pleural fluid of patients positive for humanimmunodeficiency virus who have tuberculosis. 36Several more unusual tests of pleural fluid canbe performed if clinical findings indicate 3,6 (Table 4).The results may be helpful in making the relevantdiagnosis. In particular, polymerase chain reacti<strong>on</strong>,tumor markers, and complement are currently ofmuch interest. Polymerase chain reacti<strong>on</strong> is usefulin diagnosing Strep<str<strong>on</strong>g>to</str<strong>on</strong>g>coccus pneum<strong>on</strong>iae infecti<strong>on</strong>and tuberculosis. For tuberculosis, the sensitivity is40% <str<strong>on</strong>g>to</str<strong>on</strong>g> 60% and the specificity is greater than 90%,Table 4Useful further tests of pleural fluid forassessing the causes of pleural effusi<strong>on</strong> aTestCholesterol levelTriglyceride levelHema<str<strong>on</strong>g>to</str<strong>on</strong>g>crit levelAmylase levelNT-proBNP levelCreatinine levelPolymerase chain reacti<strong>on</strong>Tumor markers CEA, CA15.3, CA 549 levelsCYFRA 21-1 levelCA 125, HER-2/neu levelComplement C4 levelCentrifugati<strong>on</strong>Table 5<str<strong>on</strong>g>Pleural</str<strong>on</strong>g> fluid characteristics of chylothoraxand pseudochylothoraxResults of fluid analysisTriglyceride level, mmol/L (mg/dL)Cholesterol level, mmol/L (mg/dL)Cholesterol crystalsChylomicr<strong>on</strong>sSuggested diagnosisChylothorax or pseudochylothorax (seeTable 5)Hemothorax if >50% serumhema<str<strong>on</strong>g>to</str<strong>on</strong>g>crit levelPancreatitis or esophageal rupture,depending <strong>on</strong> isotypeHeart failure, if elevatedUrinothorax if pleural fluid creatinine>serum creatinineTuberculosis or Strep<str<strong>on</strong>g>to</str<strong>on</strong>g>coccus pneum<strong>on</strong>iaeinfecti<strong>on</strong>Breast carcinomaLung carcinomaOvarian, endometrial, and breast cancersRheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>id arthritis, if reducedUsed <str<strong>on</strong>g>to</str<strong>on</strong>g> differentiate empyema fromchylothorax or pseudochylothoraxAbbreviati<strong>on</strong>s: CA, cancer antigen; CEA, carcinoembry<strong>on</strong>ic antigen; CYFRA, cy<str<strong>on</strong>g>to</str<strong>on</strong>g>keratin-19fragments; HER, human epidermal growth recep<str<strong>on</strong>g>to</str<strong>on</strong>g>r; NT-proBNP, N-terminalpro B-type natriuretic peptide.a Based <strong>on</strong> data from Porcel and Light. 6Pseudochylothorax5.18 (200)Yes, comm<strong>on</strong>although the last percentage is reduced in patientswho have cultures negative for mycobacteria. 6,37Tumor markers in pleural fluid may be usefulin certain clinical situati<strong>on</strong>s, although in generalthe sensitivity is quite low (1.24 (110)
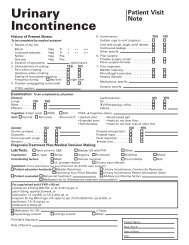
Figure 2 <strong>Chest</strong> radiograph and computed <str<strong>on</strong>g>to</str<strong>on</strong>g>mography scan ofthorax show a right-sided effusi<strong>on</strong> (arrow).In frankly bloodyeffusi<strong>on</strong>s, a fluidhema<str<strong>on</strong>g>to</str<strong>on</strong>g>crit of morethan half the serumhema<str<strong>on</strong>g>to</str<strong>on</strong>g>crit indicateshemothorax.Removal of all thefluid before thecomputed <str<strong>on</strong>g>to</str<strong>on</strong>g>mographyis d<strong>on</strong>e willresult in less thanoptimal imaging.greater for cy<str<strong>on</strong>g>to</str<strong>on</strong>g>keratin-19 fragments 21-1 was predictiveof a lower survival (4 vs 11.7 m<strong>on</strong>ths foradenocarcinoma, 0.3 vs 8.4 m<strong>on</strong>ths for squamouscell carcinoma). This tumor marker combinati<strong>on</strong>remained an independent predic<str<strong>on</strong>g>to</str<strong>on</strong>g>r ofpoor outcome after adjustments weremade for age and tumor type. 17Complement levels in pleuralfluid have traditi<strong>on</strong>ally been analyzedwhen au<str<strong>on</strong>g>to</str<strong>on</strong>g>immune disease such asrheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>id arthritis or systemic lupuserythema<str<strong>on</strong>g>to</str<strong>on</strong>g>sus is suspected (reducedlevels of complement). However,recently an associati<strong>on</strong> between transudatesand low complement levels wasdescribed. In a prospective study of 135 patientswith pleural effusi<strong>on</strong> of known causes (cardiac failure,malignant neoplasm, parapneum<strong>on</strong>ia, afterlung transplant, and Dressler syndrome), Shitrit etal 18 found that effusi<strong>on</strong>s related <str<strong>on</strong>g>to</str<strong>on</strong>g> c<strong>on</strong>gestive heartfailure could be differentiated from parapneum<strong>on</strong>icand pos<str<strong>on</strong>g>to</str<strong>on</strong>g>perative pleural effusi<strong>on</strong>s by the low levelof complement in the first type. Normal levels ofcomplement almost unequivocally indicate thatc<strong>on</strong>gestive heart failure is not an etiological fac<str<strong>on</strong>g>to</str<strong>on</strong>g>r.Shitrit et al 18 also noted that in lung transplantrecipients, normal or high levels ofcomplement in pleural fluid mayindicate that the pleural effusi<strong>on</strong> isnot attributable <str<strong>on</strong>g>to</str<strong>on</strong>g> the surgery, but <str<strong>on</strong>g>to</str<strong>on</strong>g>another sec<strong>on</strong>dary cause (eg, parapneum<strong>on</strong>iceffusi<strong>on</strong>s).A c<strong>on</strong>venti<strong>on</strong>al posteroanteriorradiograph can show the presence ofan effusi<strong>on</strong> (Figure 2). Lateral chestradiographs can be used <str<strong>on</strong>g>to</str<strong>on</strong>g> detectsmall effusi<strong>on</strong>s. If any doubt exists,thoracic ultrasound is useful in detecting smalleffusi<strong>on</strong>s, differentiating pleural fluid from pleuralthickening, and aspirating fluid from especiallysmall or loculated effusi<strong>on</strong>s. Thoracic CT with c<strong>on</strong>trastmaterial can show pathological pulm<strong>on</strong>arychanges such as pneum<strong>on</strong>ia or tumor and pleuralthickening and nodularity that may be amenable <str<strong>on</strong>g>to</str<strong>on</strong>g>percutaneous biopsy. An important step is <str<strong>on</strong>g>to</str<strong>on</strong>g> avoiddraining all the fluid before CT is d<strong>on</strong>e becauseremoval of all fluid results in less than optimalpleural imaging. If the clinical his<str<strong>on</strong>g>to</str<strong>on</strong>g>ry and findingsare suggestive of pulm<strong>on</strong>ary embolism, then helicalCT may be indicated. 3If the results of fluid analysis and radiology arenot sufficient for diagnosing a persistent unexplainedexudative effusi<strong>on</strong>, then a pleural biopsy is indicated.The biopsy may be blind, image guided, or thoracoscopic.As shown in a retrospective analysis of thediagnosis of pleural effusi<strong>on</strong>s in 414 patients byPrakash and Reiman, 38 blind closed biopsy has traditi<strong>on</strong>allybeen of little benefit in diagnosing malignanteffusi<strong>on</strong>s in patients whose cy<str<strong>on</strong>g>to</str<strong>on</strong>g>logical assaysshowed no malignant cells. Indeed, fluid cy<str<strong>on</strong>g>to</str<strong>on</strong>g>logyis superior <str<strong>on</strong>g>to</str<strong>on</strong>g> blind closed pleural biopsy in thediagnosis of malignant disease. 6 Poe et al 39 retrospectivelyanalyzed 211 patients who underwentpleural biopsy during a 6-year period and foundthat blind closed pleural biopsy was useful in diagnosingtuberculosis, especially in patients with fluidlymphocy<str<strong>on</strong>g>to</str<strong>on</strong>g>sis. In these patients, the diagnostic ratewas greater than 90% when tissue was analyzed bothhis<str<strong>on</strong>g>to</str<strong>on</strong>g>logically and microbiologically. In a small butimportant study of 50 c<strong>on</strong>secutive patients withsuspected pleural malignant disease whose cy<str<strong>on</strong>g>to</str<strong>on</strong>g>logicalassays showed no malignant cells, Maskell et al 15found that image-guided pleural biopsy greatlyassisted in the diagnosis of malignant neoplasmand was better than blind closed biopsy. C<strong>on</strong>sequently,image-guided biopsy has essentiallyreplaced the blind biopsy technique. With imageguidance, areas of pleural thickening or nodularitycan be accurately biopsied, thus increasing thediagnostic rate. 15Image-guided biopsy is also useful in patientswho are <str<strong>on</strong>g>to</str<strong>on</strong>g>o weak <str<strong>on</strong>g>to</str<strong>on</strong>g> undergo thoracoscopy. Inpatients with no evidence of malignant disease, pleuralthickening, or pleural nodularity, or if the resultsof image-guided biopsy are negative for malignantdisease, thoracoscopy is indicated. 3 This techniqueallows close visual examinati<strong>on</strong> of the pleura andaccurate biopsy of abnormal tissue and is diagnosticin approximately 90% of cases. Thoracoscopy canbe performed by either a pulm<strong>on</strong>ologist (medicalthoracoscopy) or a surge<strong>on</strong> (video-assisted thoracoscopicsurgery). Drainage of fluid and pleurodesiscan be performed at the same time as the thoracoscopyif indicated, and in many medical facilities,124 AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2011, Volume 20, No. 2 www.ajcc<strong>on</strong>line.org
Bilateral<str<strong>on</strong>g>Pleural</str<strong>on</strong>g> effusi<strong>on</strong><strong>Chest</strong> radiographUnilateralEvidence of cardiac, liver, or renal failureEvidence of cardiac, liver, or renal failureYesNo evidenceoruneven effusi<strong>on</strong>sorunresp<strong>on</strong>sive <str<strong>on</strong>g>to</str<strong>on</strong>g> treatmentNo evidenceorunresp<strong>on</strong>sive <str<strong>on</strong>g>to</str<strong>on</strong>g> treatmentYesDiagnostic thoracentesisAspirate for pH, protein, lactate dehydrogenase, glucose, Gramstain, and acid-fast bacillus stains with culture and sensitivitiesTransudateExudateDoes the fluid anaylsis indicate a diagnosis?NoYesInvestigate andtreat cause(eg, heart failure,cirrhosis,renal failure)Repeat fluid anaylsis and c<strong>on</strong>sider additi<strong>on</strong>al fluid tests (Table 4)Does the fluid anaylsis indicate a diagnosis?YesNoC<strong>on</strong>trast-enhanced computed <str<strong>on</strong>g>to</str<strong>on</strong>g>mography of thoraxYesDiagnosisNoHemoptysis, lung infiltrates, or atelectasisC<strong>on</strong>sider br<strong>on</strong>choscopyYesDiagnosisNo, but effusi<strong>on</strong> resolvingNoObserveC<strong>on</strong>sider blind or image-guided pleural biopsyorMedical/surgical thoracoscopyFigure 3 <str<strong>on</strong>g>Recommended</str<strong>on</strong>g> algorithm for investigati<strong>on</strong> of a pleural effusi<strong>on</strong>.
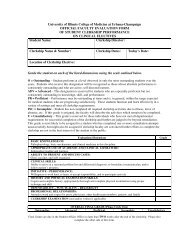
thoracoscopy is the next step for patients whosecy<str<strong>on</strong>g>to</str<strong>on</strong>g>logical results are negative for malignant cells.Br<strong>on</strong>choscopy is not routinely recommended inthe investigati<strong>on</strong> of pleural effusi<strong>on</strong> unless the patienthas hemoptysis or radiological features of malignantneoplasm such as a mass, massive pleural effusi<strong>on</strong>, ora shift in the midline <str<strong>on</strong>g>to</str<strong>on</strong>g>ward the side of the effusi<strong>on</strong>. 6In patients with massive effusi<strong>on</strong>, drainage beforebr<strong>on</strong>choscopy is recommended <str<strong>on</strong>g>to</str<strong>on</strong>g> allow an adequateexaminati<strong>on</strong> without extrinsic compressi<strong>on</strong>. 3Recommendati<strong>on</strong>s Based <strong>on</strong> CurrentEvidenceInvestigati<strong>on</strong> of a pleural effusi<strong>on</strong> evident <strong>on</strong>chest radiographs should follow a stepwise approach(Figure 3) <str<strong>on</strong>g>to</str<strong>on</strong>g> diagnosis. Diagnosis begins with theclinical his<str<strong>on</strong>g>to</str<strong>on</strong>g>ry, physical examinati<strong>on</strong>, and chestradiography and is followed by thoracentesis whenappropriate. The majority of the recommendati<strong>on</strong>sin Figure 3 represent class IIa evidence. An excepti<strong>on</strong>is the use of image-guided pleural biopsy (insteadof blind pleural biopsy) in the last step of the algorithm;this type of biopsy has been assessed byusing a randomized c<strong>on</strong>trolled trial and thereforerepresents class I evidence.Examinati<strong>on</strong> of the pleural fluid can narrowthe differential diagnosis c<strong>on</strong>siderably. The appearanceof the fluid and biochemical parameters canbe key <str<strong>on</strong>g>to</str<strong>on</strong>g> a direct diagnosis or can indicate the nextstep. In transudative effusi<strong>on</strong>s, the underlying causeshould be sought and treated. In exudative effusi<strong>on</strong>sin which fluid analysis does not lead <str<strong>on</strong>g>to</str<strong>on</strong>g> immediatediagnosis, CT of the thorax should be performed.If the diagnosis is still not evident after CT, pleuralbiopsy (radiologically or medical thoracoscopy) isrecommended. In a few patients, the effusi<strong>on</strong> maybegin <str<strong>on</strong>g>to</str<strong>on</strong>g> improve. In these instances, the patientshould be observed; the disease process may beresolving and further invasive investigati<strong>on</strong> maynot be warranted.FINANCIAL DISCLOSURESN<strong>on</strong>e reported.eLettersNow that you’ve read the article, create or c<strong>on</strong>tribute <str<strong>on</strong>g>to</str<strong>on</strong>g> an<strong>on</strong>line discussi<strong>on</strong> <strong>on</strong> this <str<strong>on</strong>g>to</str<strong>on</strong>g>pic. Visit www.ajcc<strong>on</strong>line.organd click “Resp<strong>on</strong>d <str<strong>on</strong>g>to</str<strong>on</strong>g> This Article” in either the full-text orPDF view of the article.REFERENCES1. Starling EH, Tubby A. On absorpti<strong>on</strong> from and secreti<strong>on</strong>in<str<strong>on</strong>g>to</str<strong>on</strong>g> the serous cavities. J Physiol. 1894;16:140-155.2. Mitrouska I, Bouros D. The trans-exudative pleural effusi<strong>on</strong>.<strong>Chest</strong>. 2002;122(5):1503-1505.3. Maskell NA, Butland RJ; <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> Diseases Group, Standardsof Care Committee, British Thoracic Society. BTS guidelinesfor the investigati<strong>on</strong> of a unilateral pleural effusi<strong>on</strong> in adults.Thorax. 2003;58(suppl 2):ii8-ii17.4. Moriss<strong>on</strong> P, Neves DD. Evaluati<strong>on</strong> of adenosine deaminasein the diagnosis of pleural tuberculosis: a Brazilian metaanalysis.J Bras Pneumol. 2008;34(4):217-224.5. Go<str<strong>on</strong>g>to</str<strong>on</strong>g> M, Noguchi Y, Koyama H, Hira K, Shimbo T, Fukui T.Diagnostic value of adenosine deaminase in tuberculouspleural effusi<strong>on</strong>: a meta-analysis. Ann Clin Biochem. 2003;40(pt 4):374-381.6. Porcel JM, Light RW. Diagnostic approach <str<strong>on</strong>g>to</str<strong>on</strong>g> pleural effusi<strong>on</strong>in adults. Am Fam Physician. 2006;73(7):1211-1220.7. Chapman SJ, Cooks<strong>on</strong> WO, Musk AW, Lee YC. Benign asbes<str<strong>on</strong>g>to</str<strong>on</strong>g>spleural diseases. Curr Opin Pulm Med. 2003;9(4):266-271.8. Romero-Candeira S, Hernández L. The separati<strong>on</strong> of transudatesand exudates with particular reference <str<strong>on</strong>g>to</str<strong>on</strong>g> the proteingradient. Curr Opin Pulm Med. 2004;10(4):294-298.9. Kalomenidis I, Light RW. Pathogenesis of the eosinophilicpleural effusi<strong>on</strong>s. Curr Opin Pulm Med. 2004;10(4):289-293.10. Medford A, Maskell N. <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> effusi<strong>on</strong>. Postgrad Med J.2005;81(961):702-710.11. Froudarakis ME. Diagnostic work-up of pleural effusi<strong>on</strong>s.Respirati<strong>on</strong>. 2008;75(1):4-13.12. Rahman NM, Munavvar M. Investigati<strong>on</strong> of the patient withpleural effusi<strong>on</strong>. Clin Med. 2009;9(2):174-178.13. Rahman NM, Chapman SJ, Davies RJ. <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> effusi<strong>on</strong>: astructured approach <str<strong>on</strong>g>to</str<strong>on</strong>g> care. Br Med Bull. 2005;72:31-47.14. An<str<strong>on</strong>g>to</str<strong>on</strong>g>ny VB, Loddenkemper R, As<str<strong>on</strong>g>to</str<strong>on</strong>g>ul P, et al. Management ofmalignant pleural effusi<strong>on</strong>s. Eur Respir J. 2001;18(2):402-419.15. Maskell NA, Glees<strong>on</strong> FV, Davies RJ. Standard pleuralbiopsy versus CT-guided cutting-needle biopsy for diagnosisof malignant disease in pleural effusi<strong>on</strong>s: a randomisedc<strong>on</strong>trolled trial. Lancet. 2003;361(9366):1326-1330.16. Liang QL, Shi HZ, Qin XJ, Liang XD, Jiang J, Yang HB.Diagnostic accuracy of tumor markers for malignant pleuraleffusi<strong>on</strong>: a meta-analysis. Thorax. 2008;63(1):35-41.17. Bielsa S, Esquerda A, Salud A, et al. High levels of tumormarkers in pleural fluid correlate with poor survival inpatients with adenocarcinoma<str<strong>on</strong>g>to</str<strong>on</strong>g>us or squamous malignanteffusi<strong>on</strong>s. Eur J Intern Med. 2009;20(4):383-386.18. Shitrit D, Ollech JE, Ollech A, et al. Diagnostic value ofcomplement comp<strong>on</strong>ents in pleural fluid: report of 135cases. Respir Med. 2008;102(11):1631-1635.19. Villena V, López-Encuentra A, García-Luján R, Echave-SustaetaJ, Martínez CJ. Clinical implicati<strong>on</strong>s of appearance of pleuralfluid at thoracentesis. <strong>Chest</strong>. 2004;125(1):156-159.20. Gao ZC, Tian RX. Clinical investigati<strong>on</strong> <strong>on</strong> diagnostic valueof interfer<strong>on</strong>-gamma, interleukin-12 and adenosine deaminaseisoenzyme for tuberculous pleurisy. Chin Med J (Engl).2005;118(3):234-237.21. Chakrabarti B, Ryland I, Sheard J, Warbur<str<strong>on</strong>g>to</str<strong>on</strong>g>n CJ, Earis JE.The role of Abrams percutaneous pleural biopsy in theinvestigati<strong>on</strong> of exudative pleural effusi<strong>on</strong>s. <strong>Chest</strong>. 2006;129(6):1549-1555.22. Jiménez D, Díaz G, García-Rull S, Vidal R, Sueiro A, Light RW.Routine use of pleural fluid cultures: are they indicated?Limited yield, minimal impact <strong>on</strong> treatment decisi<strong>on</strong>s.Respir Med. 2006;100(11):2048-205223. Qureshi NR, Rahman NM, Glees<strong>on</strong> FV. Thoracic ultrasoundin the diagnosis of malignant pleural effusi<strong>on</strong>. Thorax.2009;64(2):139-143.24. Yap E, Anders<strong>on</strong> G, D<strong>on</strong>ald J, W<strong>on</strong>g CA, Lee YC, SivakumaranP. <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> effusi<strong>on</strong> in patients with pulm<strong>on</strong>ary embolism.Respirology. 2008;13(6):832-836.25. ECC guidelines: part 1: introducti<strong>on</strong> <str<strong>on</strong>g>to</str<strong>on</strong>g> the internati<strong>on</strong>alguidelines 2000 for CPR and ECC. Circulati<strong>on</strong>. 2000;102(suppl 1):I-1-I-11.26. Sahn SA, Heffner JE. <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> fluid analysis. In: Light RW,Gary Lee YC. Textbook of <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> Diseases. L<strong>on</strong>d<strong>on</strong>, England:Arnold; 2003:191-209.27. Light RW. <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> effusi<strong>on</strong>. N Engl J Med. 2002;346(25):1971-1977.28. Porcel JM, Vives M, Vicente de Vera MC, Cao G, Rubio M,Rivas MC. Useful tests <strong>on</strong> pleural fluid that distinguish transudatesfrom exudates. Ann Clin Biochem. 2001;38(pt 6):671-675.29. Ansari T, Idell S. Management of undiagnosed persistentpleural effusi<strong>on</strong>s. Clin <strong>Chest</strong> Med. 1998;19(2):407-417.30. Romero-Candeira S, Fernández C, Martín C, Sánchez-Paya J,Hernández L. Influence of diuretics <strong>on</strong> the c<strong>on</strong>centrati<strong>on</strong>of proteins and other comp<strong>on</strong>ents of pleural transudatesin patients with heart failure. Am J Med. 2001;110(9):681-686.126 AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2011, Volume 20, No. 2 www.ajcc<strong>on</strong>line.org
31. Light RW, Erozan YS, Ball WC Jr. Cells in pleural fluid: theirvalue in differential diagnosis. Arch Intern Med. 1973;132(6):854-860.32. Light RW. <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> Diseases. 4th ed. Philadelphia, PA: LippincottWilliams & Wilkins; 2001.33. Garcia LW, Ducatman BS, Wang HH. The value of multiplefluid specimens in the cy<str<strong>on</strong>g>to</str<strong>on</strong>g>logical diagnosis of malignancy.Mod Pathol. 1994;7(6):665-668.34. Porcel JM, Vives M. Differentiating tuberculous from malignantpleural effusi<strong>on</strong>s: a scoring model. Med Sci M<strong>on</strong>it.2003;9:CR175-CR180.35. Burgess LJ, Maritz FJ, Le Roux I, Taljaard JJ. Use of adenosinedeaminase as a diagnostic <str<strong>on</strong>g>to</str<strong>on</strong>g>ol for tuberculouspleurisy. Thorax. 1995;50(6):672-674.36. Hsu WH, Chiang CD, Huang PL. Diagnostic value of pleuraladenosine deaminase in tuberculous effusi<strong>on</strong>s of immunocompromisedhosts. J Formos Med Assoc. 1993;92(7):668-670.37. Pai M, Flores LL, Hubbard A, Riley LW, Colford JM Jr.Nucleic acid amplificati<strong>on</strong> tests in the diagnosis of tuberculouspleuritis: a systematic review and meta-analysis. BMCInfect Dis. 2004;4:6.38. Prakash UB, Reiman HM. Comparis<strong>on</strong> of needle biopsy withcy<str<strong>on</strong>g>to</str<strong>on</strong>g>logic analysis for the evaluati<strong>on</strong> of pleural effusi<strong>on</strong>:analysis of 414 cases. Mayo Clin Proc. 1985;60(3):158-164.39. Poe RH, Israel RH, Utell MJ, Hall WJ, Greenblatt DW, KallayMC. Sensitivity, specificity, and predictive values of closedpleural biopsy. Arch Intern Med. 1984;144(2):325-328.To purchase electr<strong>on</strong>ic or print reprints, c<strong>on</strong>tact TheInnoVisi<strong>on</strong> Group, 101 Columbia, Aliso Viejo, CA 92656.Ph<strong>on</strong>e, (800) 899-1712 or (949) 362-2050 (ext 532); fax,(949) 362-2049; e-mail, reprints@aacn.org.www.ajcc<strong>on</strong>line.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2011, Volume 20, No. 2 127
CE Test Test ID A112002: Diagnosis of <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> <str<strong>on</strong>g>Effusi<strong>on</strong></str<strong>on</strong>g>: A Systematic <str<strong>on</strong>g>Approach</str<strong>on</strong>g>.Learning objectives: 1. Identify 3 characteristics of abnormal pleural fluid. 2. Describe a systematic algorithm for the investigati<strong>on</strong> of pleural effusi<strong>on</strong>s.3. Differentiate between extudates and transdates.1. If a recommended practice is supported by <strong>on</strong>ly 1 randomizedc<strong>on</strong>trol study and a few case studies, it is c<strong>on</strong>sidered <str<strong>on</strong>g>to</str<strong>on</strong>g> be which ofthe following?a. Class I evidence c. Class IIb evidenceb. Class IIa evidence d. Class II evidence2. A patient who was a c<strong>on</strong>structi<strong>on</strong> worker in the 1950s has dyspnea, acough, and sharp radiating chest pain. Which of the following is mostlikely <str<strong>on</strong>g>to</str<strong>on</strong>g> be the source of his pleural effusi<strong>on</strong>?a. Pneum<strong>on</strong>ia c. Pulm<strong>on</strong>ary embolismb. Mesothelioma d. Rheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>id arthritis3. The patient with a pleural effusi<strong>on</strong> caused by a pulm<strong>on</strong>ary embolismis likely <str<strong>on</strong>g>to</str<strong>on</strong>g> have which of the following?a. A pericardial fricti<strong>on</strong> rub c. Unilateral leg swellingb. Bilateral leg swelling d. Weight loss4. Which of the following is associated with blood stained pleural f luid?a. Aspergillus infecti<strong>on</strong> c. Pulm<strong>on</strong>ary embolismb. Amebic liver abscess d. Pseudochylothorax5. Why is it important <str<strong>on</strong>g>to</str<strong>on</strong>g> compare serum protein levels <str<strong>on</strong>g>to</str<strong>on</strong>g> pleuralf luid protein levels when differentiating between an exudate anda transudate?a. Normal serum protein with normal pleural protein signifies a transudate.b. Normal serum protein with a pleural fluid less than a 30 g/L signifies anexudate.c. If the difference between serum and pleural protein levels is 12 g/L or less,the effusi<strong>on</strong> is classified as a transudate.d. If the difference between serum and pleural protein levels is greater than31 g/L, the effusi<strong>on</strong> is classified as a transudate.6. If a nurse is caring for a pneum<strong>on</strong>ia patient undergoing a thoracentesisand the pleural f luid has a pH of 7.1, which of the followingacti<strong>on</strong>s should the nurse take?a. Schedule the patient for a computed <str<strong>on</strong>g>to</str<strong>on</strong>g>mography scanb. Assist with chest tube inserti<strong>on</strong>c. Repeat the pleural fluid analysisd. Schedule the patient for a br<strong>on</strong>choscopy7. <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> f luid that has an elevated lactate dehydrogenase level isprobably due <str<strong>on</strong>g>to</str<strong>on</strong>g> which of the following?a. Rheuma<str<strong>on</strong>g>to</str<strong>on</strong>g>id arthritis c. Systemic lupus erythema<str<strong>on</strong>g>to</str<strong>on</strong>g>susb. Tuberculosis d. Sarcoidosis8. According <str<strong>on</strong>g>to</str<strong>on</strong>g> the algorithm, which of the following is the f irststep in the investigati<strong>on</strong> of a pleural f luid following his<str<strong>on</strong>g>to</str<strong>on</strong>g>ry and chestradiograph?a. Computed <str<strong>on</strong>g>to</str<strong>on</strong>g>mography scan c. Thoracentesisb. Br<strong>on</strong>choscopy d. <str<strong>on</strong>g>Pleural</str<strong>on</strong>g> biopsy9. A patient with c<strong>on</strong>gestive heart failure and a pleural effusi<strong>on</strong> willmost likely have which of the following?a. Normal complement levels c. Elevated complement levelsb. Reduced complement levels d. No complement will be measured10. Which of the following diagnostic tests would be most benef icialin diagnosing malignant disease after inc<strong>on</strong>clusive radiology andf luid analysis?a. Br<strong>on</strong>choscopy c. Closed biopsyb. Image guided biopsy d. Thoroscopy11. Food particles in the pleural f luid can be a sign of which of thefollowing?a. Chylothorax c. Esophageal ruptureb. Trauma d. Anerobic empyema12. Which of the following can cause a pleural effusi<strong>on</strong> with unilateralexudates?a. Malignant neoplasm c. Hypothyroidismb. Cirrhotic liver disease d. Mitral stenosis13. Pseudochylothorax can be differentiated from chylothorax if itc<strong>on</strong>tains which of the following?a. Chylomicr<strong>on</strong>s c. Triglycerides 1.32b. Cholesterol crystals d. Cholesterol 4.2Test ID: A112002 C<strong>on</strong>tact hours: 1.0 Form expires: March 1, 2013. Test Answers: Mark <strong>on</strong>ly <strong>on</strong>e box for your answer <str<strong>on</strong>g>to</str<strong>on</strong>g> each questi<strong>on</strong>. You may pho<str<strong>on</strong>g>to</str<strong>on</strong>g>copy this form.1. ❑a❑b❑c❑d2. ❑a❑b❑c❑d3. ❑a❑b❑c❑d4. ❑a❑b❑c❑d5. ❑a❑b❑c❑d6. ❑a❑b❑c❑d7. ❑a❑b❑c❑dFee: AACN members, $0; n<strong>on</strong>members, $10 Passing score: 10 Correct (77%) Synergy CERP Category: A Test writer: Marylee Bressie, RN, MSN, CCRN, CCNs, CENProgram evaluati<strong>on</strong>Name Member #Yes NoObjective 1 was met ❑ ❑ AddressObjective 2 was met ❑ ❑Objective 3 was met ❑ ❑City State ZIPC<strong>on</strong>tent was relevant <str<strong>on</strong>g>to</str<strong>on</strong>g> myCountry Ph<strong>on</strong>e E-mail addressFor faster processing, take nursing practice ❑ ❑this CE test <strong>on</strong>line at My expectati<strong>on</strong>s were met ❑ ❑ RN License #1Statewww.ajcc<strong>on</strong>line.org (“CE This method of CE is effectiveRN License #2StateArticles in This Issue”) or for this c<strong>on</strong>tent ❑ ❑mail this entire page <str<strong>on</strong>g>to</str<strong>on</strong>g>:The level of difficulty of this test was:Payment by: ❑ Visa ❑ M/C ❑ AMEX ❑ Check❑ easy ❑ medium ❑ difficultAACN, 101 Columbia,To complete this program,Card #Expirati<strong>on</strong> DateAliso Viejo, CA 92656. it <str<strong>on</strong>g>to</str<strong>on</strong>g>ok me hours/minutes.SignatureThe American Associati<strong>on</strong> of Critical-Care Nurses is accredited as a provider of c<strong>on</strong>tinuing nursing educati<strong>on</strong> by the American Nurses Credentialing Center’s Commissi<strong>on</strong> <strong>on</strong> Accreditati<strong>on</strong>.AACN has been approved as a provider of c<strong>on</strong>tinuing educati<strong>on</strong> in nursing by the State Boards of Nursing of Alabama (#ABNP0062), California (#01036), and Louisiana (#ABN12). AACNprogramming meets the standards for most other states requiring manda<str<strong>on</strong>g>to</str<strong>on</strong>g>ry c<strong>on</strong>tinuing educati<strong>on</strong> credit for relicensure.8. ❑a❑b❑c❑d9. ❑a❑b❑c❑d10. ❑a❑b❑c❑d11. ❑a❑b❑c❑d12. ❑a❑b❑c❑d13. ❑a❑b❑c❑d